
Annual report for 2018
Published 30 April 2019

© Crown copyright 2019
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/raib-annual-report-published-2019/annual-report-for-2018
Our Purpose:
We independently investigate accidents to improve railway safety, and inform the industry and the public.
1. Chief Inspector’s review of 2018
Last year was the 11th successive year in which no passenger was killed in a derailment or train collision on the national network. I am pleased to note that the overall levels of risk to those who travel and work on the UK’s railways have continued to drop in the 13 years since the RAIB started investigating rail accidents. However, the death of a track worker at Stoats Nest Junction on 6 November was a sad reminder of the continuing risk to people maintaining our railways. Moving trains continue to present a hazard when staff or passengers are in close proximity to them. Typically this includes the platform-train interface, level crossings and engineering work activities. December saw the tragic death of a passenger who died after being struck by a branch whilst leaning out of a train window near Bath.
Safety of track workers
Prior to the accident at Stoats Nest Junction, it had been nearly five years since a track worker was struck and killed by a train. However, in that time there have been too many near misses in which workers have had to jump for their lives at the last moment. In the case of the near miss at Egmanton in October 2017 (report 11/2018), a multi-fatality accident was only avoided with two seconds to spare.

View from forward facing CCTV showing trackerworkers moving into the left-hand cess at Egmanton. A crossing is in the foreground and OLE is visible
The number and type of near misses in recent years is hugely disappointing given the efforts made to address track worker safety during that time. Every near miss, however caused, should be viewed as a failure of the system to deliver safety. I am concerned that, despite much effort and many initiatives, we are not seeing the hoped-for improvements in safety for track workers - in the last two years we have published three investigation reports and four safety digests covering narrowly avoided collisions between trains and track workers. Our class investigation into the safety of track workers, published in April 2017, took data from over 70 incidents, including near misses and operational irregularities, which happened in a single year.
We recently met with the Office of Rail and Road (ORR) and Network Rail to review experience to date. Although there can be no doubting the determination of the industry to address the underlying causes of near misses and accidents involving track workers, a clear improvement strategy has still to emerge. For RAIB’s part, we are assisting by collating the learning from our investigations over the last 13 years, and the resultant recommendations. The idea is to provide an evidence-based summary of the key safety issues as an input to the important decisions that need to be made by the rail industry to improve the safety of track workers.
Learning lessons from the Croydon tram crash
I am aware that considerable work has already been carried out to address the 15 recommendations we made following our investigation into the tragic accident at Sandilands on the morning of 9 November 2016, which led to the death of 7 passengers and serious injuries to many others. It is good that a number of substantive safety improvements have already been implemented (these are summarised in section 4). I am particularly encouraged that the Light Rail Safety and Standards Board has now been established in response to our recommendation 1, and is now fully funded. This will enable collaborative work across the tramway sector to share safety data, better understand tramway risk and develop new standards. It is also pleasing to note the progress made by the Croydon tramway with the implementation of our recommendations – this has already led to a major review of operational risks and a number of substantive safety measures, such as the installation of improved signage, step-down speed restrictions and the installation of a system to monitor and detect the onset of fatigue or distraction involving tram drivers. We also note with interest the work undertaken by TfL London Trams to manufacture and test several prototype windows that are designed to provide additional containment. This research was supported by Tram Operations Ltd and has led to the installation of enhanced strength window film. All of these actions, combined with the recent announcement that London Trams is now installing a system to automatically apply tram brakes in case of overspeeding at high risk locations, indicate a real determination to prevent the circumstances that led to so many deaths and injuries.
I recognise that a number of our recommendations will take time to fully address and that there are a number of ongoing work streams which are considering how and when the recommendations should be implemented. Levels of progress vary according to the recommendation, and between different tramways. Although this is understandable, our preliminary analysis of the information provided to us by the ORR suggests that there remains work to be done. This is particularly true for the recommendation which relates to the improvement of containment provided by windows and doors, across all UK tram fleets. For this reason I urge the tramway sector to dedicate the resource and imagination that is needed to address all of the issues highlighted by the Sandilands accident.
Corporate knowledge and organisational culture
The disastrous collision at Clapham Junction on 12 December 1988, in which 35 people died and 484 were injured, was a turning point in the history of Britain’s railways. The immediate cause of the accident was poor working practice by a signalling technician, and the subsequent public inquiry into the accident highlighted serious deficiencies in the management of safety, particularly around the design, modification, testing and commissioning of signalling systems. Putting in place the recommendations of the inquiry fundamentally changed several aspects of how the railway is run, and for signal engineers one of the most important was the approach to routine tasks, such as testing alterations to signalling installations. It was therefore concerning for RAIB to discover, during our investigation of the collision at Waterloo in August 2017, that some of these important changes were not reflected in the way that signalling modifications were being undertaken.
Some of the people involved in the signalling work connected with upgrading Waterloo station and its approach tracks did not keep proper records of temporary works, or ensure that additional temporary wiring was shown on the design documents. Leaving that temporary wiring in place when it should have been removed led to a passenger train being diverted onto a blocked line and colliding with wagons. Compliance with the existing standards, developed since Clapham, would have provided the controls needed to stop temporary wiring being installed and used in the uncontrolled manner which resulted in this accident.
These symptoms of a deep-seated problem should give us all pause for thought. How can organisations ensure that lessons from events that happened outside the personal experience of present-day railway people are taught and retained? Compliance with a standard comes more naturally to people when they understand the purpose of the requirement, and the consequences that may arise from disregarding it.
We are recommending that Network Rail takes action to reinforce the attitudes and depth of understanding needed for signal designers, installers and testers to safely apply their technical skills and knowledge. This should include the establishment of processes to educate present and future staff about how and why the standards have been developed. It’s also important to equip our engineers and technicians with the cognitive and social skills that are needed to work safely, both by themselves and as part of a team.
I believe that this accident at Waterloo starkly demonstrates why the lessons of Clapham should never be forgotten.
Managing the risk of change
Like any railway professional, I am excited by the potential for technology to transform our industry. Tomorrow’s digital railway will create the opportunity to run more trains with greater reliability over existing infrastructure. I also recognise that changes to organisation and business processes are necessary if the railway is to adapt to the demands of the modern world.
Technological and organisational change is both inevitable and essential. However, a number of our recent investigations have demonstrated how well intentioned changes can result in unintended unsafe outcomes. Examples of such outcomes that featured in reports published during 2018 included the introduction of power operated gates at user worked crossings (Frognal Farm, report 12/2018) and the design of electrical traction control equipment on refurbished trains (Guildford, report 05/2018). An example of poor implementation of a new business process was identified in the investigation into a track worker near miss incident at South Hampstead (report 20/2018). This found that a new track safety role, the ‘Person in Charge’, had been introduced in a way that lacked clarity, which led to misinterpretation of the related procedure and confusion on site.
The rail industry is frequently criticised for implementing change too slowly, or for being risk averse and overly bureaucratic. This is sometimes an unfair criticism - the operating railway is not the right place to test unproven products and processes without suitable risk mitigation measures in place. There is clearly a need for the railway industry to think carefully about how to bring about change whilst controlling the risk to the existing railway. This should also include consideration of the particular challenges associated with designing, validating and commissioning new computer based train signalling systems (see our interim report on the loss of speed restrictions on the Cambrian line (interim report IR01/2018)).
Private level crossings
I have already referred to the accident at Frognal Farm level crossing (report 12/2018). This accident, which came very close to killing a motorist, has shown up some significant weaknesses in the way that some level crossings have been managed over many years. User-worked level crossings, where the user is responsible for operating gates themselves, are usually on rural, private roads. They are a legacy of agreements between railway companies and landowners, made at the time the railways were built in the nineteenth century. Today’s trains are more frequent and travel faster than the Victorian railway builders could ever dream of, and the risk to crossing users and people on trains at these level crossings is now one of the most significant that the railway has to manage.
The nineteenth-century approach to managing the use of private level crossings revolved round the concept of the authorised user, the person occupying the land or premises that the crossing gave access to. They were considered to be responsible for making sure that anyone who had a valid reason to visit them and needed to use the crossing was aware of how to cross safely. It is doubtful whether this concept was ever really effective, and in today’s world of parcel deliveries by multiple couriers it just doesn’t work. The risk associated with these crossings, and particularly the need for a fresh approach to giving information and instructions to users who are unfamiliar with them, is one of the themes from 2018 which can be found in Section 5.
Managing the risk of accidents at the interface between platform and train
Since it was set up in 2005, RAIB has investigated 15 events in which door systems have not detected objects trapped in the closed and locked doors of a departing train or tram. In every case, a digit, limb, an item of clothing or a bag has become caught in the doors and the train has departed, sometimes resulting in very serious injuries.
Over a period of two weeks in August and September 2018 we published no less than four different reports into ‘trap and drag’ events. In the most serious of these a passenger became trapped in the doors of a tube train and was dragged a short distance into the tunnel at Notting Hill Gate station in London. Although she survived this terrible accident she suffered serious injuries. The other incidents involved potentially dangerous occurrences on trams in Nottingham and Bury and on a main line train at Bushey. September 2018 also saw us launch an investigation into a dangerous train dispatch at Elstree & Borehamwood station, in which the dog of an intending passenger was trapped in the closing doors and dragged to its death.
Although every such event is different, it is striking how often we encounter a dependence on the door interlock and a belief that modern door systems can always be relied upon to detect a trapped object. This misconception appears still to be prevalent across all rail sectors and all types of train dispatchers. These incidents reinforce the absolute importance of the final safety check after the doors are detected as closed and before a tram or train continues with its journey. This is a safety message that applies equally to trams and trains.
Safe train dispatch requires drivers to maintain high levels of concentration. For this reason our investigation into the accident at Notting Hill Gate examined the extent to which the nature of the driving task can result in drivers not consciously processing the available information when dispatching their train, and the need to think hard about how to reduce the risk of train operators losing attention and awareness while operating trains that are driven automatically. The need for this fundamental thinking is vital given the likelihood that more and more elements of the driving task will be automated in the years to come.
Management of operating incidents
Minor technical faults on trains are a daily reality on the railways, but sometimes these minor events, if not identified and dealt with effectively, can quickly develop into a potential safety incident. One such example was the evacuation of passengers from a train at Peckham Rye in south London. Our investigation (report 16/2018) revealed that misunderstandings and confusion resulted in passengers being told to leave the safety of a train, climb down vertical steps above a live electric rail, and walk in darkness along an overgrown path to a station. About eighty people went through this before the evacuation was stopped, and it is very fortunate that no-one was hurt.
When dealing with this type of incident, a train driver has many tasks to perform, and as we all know ourselves stress can sometimes affect our ability to function properly. Unfortunately, over recent years there have been a number of incidents on the railway in which train drivers have not been adequately supported when managing a difficult situation in unfamiliar circumstances. It is essential that on these occasions the signaller, train driver, any other involved staff (whether on the train or on the ground) and the various control rooms all work together to coordinate their activities to meet the needs of passengers, and the train driver is supported to ensure that the incident is effectively and efficiently resolved.
Our recently published investigation into the self-detrainment of passengers from stranded trains at Lewisham (report 02/2019) also highlights how quickly an operating incident on a busy urban railway can become a potentially dangerous situation without quick and effective intervention by signallers and operations controllers. I believe that there is an urgent need for the railway industry to improve the effectiveness of its existing arrangements for the management of operating incidents, particularly in areas controlled from large signalling centres.
Disseminating good practice
A highlight of the year for me was the 2018 Rail Industry Good Practice seminar we hosted in Birmingham on 14 November. This was the second year that we have run such an event and it was great to be joined by 140 fellow investigators from across the rail industry. I believe that it is very important that everyone in the industry who is involved in the investigation of accidents and incidents is given an opportunity to ‘network’, to discuss the lessons that they have learned and to exchange ideas in such a forum. It was also good that we were able to run a similar event in Belfast on 27 November with colleagues from Northern Ireland and the Irish Republic.

Three RAIB staff in high visibility standing in a position of safety as a train passes by.
…and finally
I would like to thank my colleagues at the RAIB for their support, good humour and sheer professionalism over the last year. I would never have expected that in the 36th year of my railway career I would still be learning so much. The reward for their work is the quality of the safety learning, the clarity of the information we provide, and the continued good reputation of the Branch.
Simon French
Chief Inspector of Rail Accidents
April 2019
2. Annual report 2018 and priorities for 2019
This is the Rail Accident Investigation Branch’s (RAIB) Annual Report for the calendar year 2018. It is produced in accordance with the Railways (Accident Investigation and Reporting) Regulations 2005 (SI1992) and meets the requirement of the European Railway Safety Directive (2004/49/EC).
Further information about us, our role and the legislation which governs our operations can be found at: www.gov.uk/raib.
Our Priorities
For 2019/20, our priorities are:
- continued delivery of high quality investigations and the dissemination of timely and effective safety learning
- working with other railway accident investigators in the UK to share good practice and to help improve the quality of investigations throughout the industry
- the active exploration of new ways of working with the other transport accident investigation branches to promote improvements to our effectiveness, efficiency and resilience, whilst also safeguarding our functional independence in the selection and conduct of investigations
- to review and revise our documented working arrangements with British Transport Police and the Office of Rail and Road
- implementing a new computer tool for the management of investigation data
- continuing to explore ways of communicating RAIB safety learning in a way that better meets the needs of our stakeholders (including the use of social media)
- working to improve information exchange with railway accident investigation bodies in Europe and beyond
- forging new working relationships with the rail industry and academia
- a fresh examination of the way we recruit and develop our talent so as to promote greater inclusion, and improve the diversity of our team
3. Operational activity
Activities started in 2018
Our regulations require the railway industry to report certain accidents and incidents to us. We received 376 notifications of railway accidents and incidents between 1 January and 31 December 2018. Of these, 61 were of sufficient importance to warrant the RAIB carrying out a ‘preliminary examination’ of the evidence in order to determine the most appropriate response.

Infographic describing RAIB activities which commenced during 2018 in response to 61 preliminary examinations which were started.
Letters to involved parties are sent in cases where, following our preliminary examination, we do not believe that there is sufficient potential safety learning to justify either further investigation or the production of a digest. We may then share the evidence that we have collected with the industry parties involved, to assist them with their own investigations into the event. We may review industry investigations to inform ourselves about the quality of the investigation or technical aspects of the event that it relates to.
Activities completed in 2018
We completed and published 20 full investigation reports in 2018 and the average time taken to publish was 9.2 months. We completed and published 12 safety digests in 2018 and the average time taken to publish was 2.9 months.
During 2018 we also issued one interim report and three urgent safety advice notices. RAIB also wrote to Coroners following three preliminary examinations at the site of fatal accidents.
You can read more about safety digests and urgent safety advice at Appendices B and C of this report.
Northern Ireland and the Channel Tunnel
Although we did not carry out any investigations in Northern Ireland or the UK part of the Channel Tunnel during 2018, we maintain contact with the respective infrastructure manaqers and railway undertakings. We also liaise as appropriate with the safety authorities for Northern Ireland and the Channel Tunnel system. These are:
- Department for Infrastructure (Northern Ireland)
- Intergovernmental Commission (Channel Tunnel)
Classification of accidents and incidents that have to be notified to the European Agency for Railways (ERA) 2014 - 2018
We have a duty to investigate all railway accidents in the UK that are classified as ‘serious’ in the Railways (Accident Investigation and Reporting) Regulations 2005 (the 2005 Regulations). This definition covers all derailments and collisions of rolling stock which result in the death of one person, serious injuries to five or more persons or extensive damage to the rolling stock, the infrastructure or environment. We also have a similar duty for those incidents and accidents which, under slightly different circumstances, could have resulted in serious accidents, and which have an obvious impact on railway safety regulation or the management of safety.
The 2005 Regulations transpose the requirements of the EU Directive 2004/49/EC into UK law.
The European Union Agency for Railways has published guidance to promote consistent categorisation of investigations in accordance with the Directive. We use this to classify our investigations according to Articles 19(1) and 19(2) of the Directive.
- Article 19(1) - a ‘serious’ accident where the investigation is mandatory
- Article 19(2) - an accident or incident, which under slightly different conditions might have led to a serious accident (eg a narrowly avoided ‘serious’ accident)
Table 1 shows the breakdown of accidents and incidents that we have investigated between 2014 and 2018 as classified according to Articles 19(1) and 19(2). The figures have been collated according to the date of occurrence and not publication of the report.
Table 1 – Investigations by category sorted by Articles 19(1) and 19(2)[footnote 1].
| Basis for Investigations by the European Railway Safety Directive category | 2014 | 2015 | 2016 | 2017 | 2018 | Total |
|---|---|---|---|---|---|---|
| Article 19(1) | 2 | 1 | 5 | 4 | 3 | 15 |
| Article 19(2) | 17 | 20 | 14 | 14 | 16 | 81 |
| Total | 19 | 21 | 19 | 18 | 19 | 96 |
Appendix A includes details of the investigations commenced and completed in 2018 and the legal basis for the investigation.
Figure 1 gives a breakdown of the total number of investigations and bulletins/safety digests started, by type of accident, for the five year period 2014 – 2018.
RAIB investigations and safety digests 2014-2018
| Full investigations | Bulletins / Safety digests | |
|---|---|---|
| Level crossing accidents and near misses | 9 | 7 |
| Events involving moving trains (staff) | 13 | 10 |
| Freight train derailments | 8 | 2 |
| Events involving moving trains (passengers and members of the public) | 15 | 3 |
| Passenger train derailments | 5 | 6 |
| Collision with an obstacle | 10 | 7 |
| Infrastructure failures | 8 | 0 |
| Collisions with other trains | 7 | 2 |
| Runaway incidents | 6 | 3 |
| Signals passed at Danger | 3 | 1 |
| Class investigations | 3 | 0 |
| Train defects | 5 | 1 |
| Fires on rolling stock | 3 | 1 |
| Near misses | 1 | 3 |
| Unauthorsed train movements | 3 | 1 |
| Other | 3 | 0 |
4. Recommendations
The recommendations in our investigation reports are made with the objective of improving railway safety. Recommendations are either intended to reduce the chance of a similar accident recurring or to mitigate the consequences were such an event to occur again. Occasionally we also make recommendations related to the way incidents and accidents are managed.
We direct recommendations to the organisation we think is best placed to implement the changes required (the ‘end implementer’). This includes railway, non-railway, private and public sector bodies.
Each recommendation is also addressed to the appropriate safety authority[footnote 2] . If a recommendation relates to an organisation that is not regulated by the railway industry’s safety authority it can be addressed to any other public body (eg the Health and Safety Executive).
On receipt of an RAIB recommendation, the safety authority is legally required to ensure that the ‘end implementers’ properly consider the recommendations, and where appropriate, act on them, as required by the Regulations. The Regulations give the safety authority the power to require end implementers to provide full details of the measures they intend to take, or have taken, to implement the recommendation.
The safety authority is also required to inform us, within a period not exceeding 12 months, of the measures taken in response to the recommendation, or the reasons why no implementation measures are being taken.
We have no statutory powers to enforce the implementation of recommendations. However, the actions taken may be considered as part of any subsequent investigation.
In the 20 reports published in 2018 we made a total of 55 recommendations.
We maintain an Index of RAIB recommendations which shows the latest status of each recommendation (as reported to us by the relevant safety authority or public body). Each entry is linked to a recommendation status report that provides the full text of each recommendation.
These status reports are compiled from information provided to us by the relevant safety authority, or other public body. All responses are categorised as follows:
i. Implemented – all actions to deliver the recommendation have been completed.
ii. Implemented by alternative means – the intent of the recommendation has been satisfied in a way we did not identify during the investigation.
iii. Implementation ongoing – work to deliver the intent of the recommendation has been agreed and is in the process of being delivered.
iv. Progressing – the relevant safety authority has yet to be satisfied that an appropriate plan, with timescales, is in place to implement the recommendation; and work is in progress to provide this.
v. Non-implementation – recommendation considered and no implementation action is to be taken.
If we are still awaiting an initial report from the relevant safety authority or public body on the status of the recommendation we categorise it as ‘Awaiting Response’.
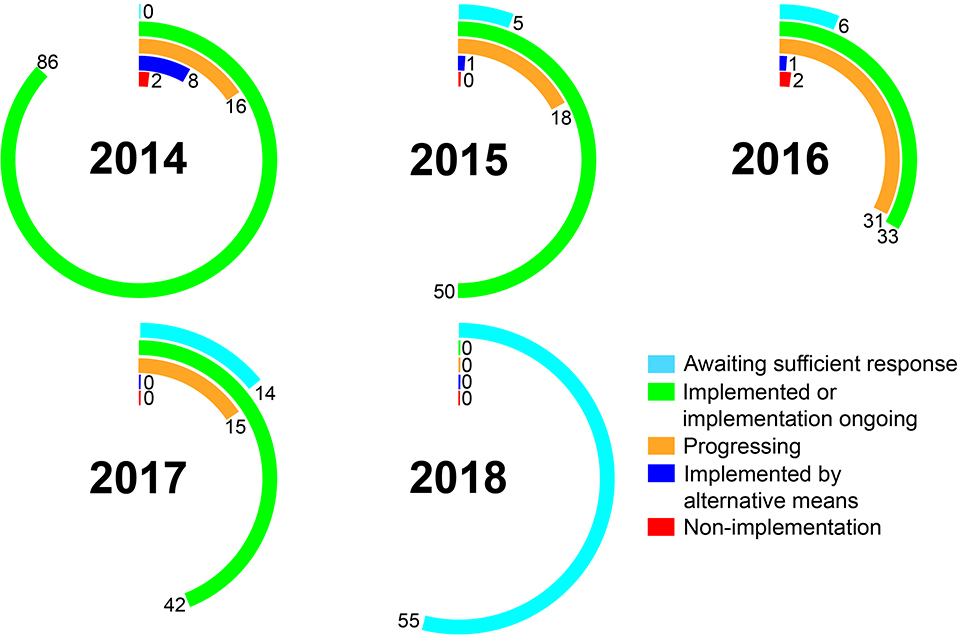
Five multicoloured radial graphs representing the years 2014 - 2018. These illustrate the status of recommendations by year according to the Office of Rail and Road (at 31 December 2018)
ORR reports to the RAIB indicate that 82% of all RAIB recommendations made since 2005 have been implemented, or were in the process of being implemented (as of 31 December 2018). Another 2% have been implemented by alternative means. In the case of 3% of our recommendations the duty holder proposed no action and ORR considers it be closed (ie non-implementation). The remaining 13% of recommendations remain open because ORR has yet to receive a sufficient response, or because ORR is still in the process of evaluating the adequacy of the duty holders’ response (ie progressing).
Sometimes, based on our understanding of the risk, we have concerns over the way that an organisation has responded to a recommendation or information provided to us by the safety authority. When this happens we will raise these concerns with the relevant safety authority. The responses are highlighted with a coloured triangle in the Index.
The meaning of the coloured triangles is as shown below:
Red - We have particular concerns that no actions have been taken in response to a recommendation.
Blue - We are concerned that the actions taken are inappropriate or insufficient to address the risk identified during the investigation.
White - We note that substantive actions have been reported but we still have concerns.
We may also add our own comments which will appear in the recommendation status report.
The status of some recommendations has changed in 2018.
In a number of instances we have concerns about the response. These are:
Table 2 – Summary of recommendations of RAIB concern
| Report No. | Investigation name | Rec No. | Triangle colour | Intent of recommendation | RAIB’s residual concern |
|---|---|---|---|---|---|
| 06/2011 | Track worker struck by a train at Cheshunt Junction (this recommendation was previously reported as ‘Implemented’ in 2013, but was re-opened in 2015 after the Hest Bank investigation (08/2015) highlighted that Network Rail had not delivered what had been promised) | 2 | Blue | Improved safe systems of work to cover activities at locations with extended sighting | Network Rail’s responses to date appear contradictory. It is therefore unclear how Network Rail intends to address the risk (of delayed warnings) that was identified in the Cheshunt and Hest Bank investigations. Network Rail has yet to provide clear guidance/instructions and therefore appear to be continuing to rely on work teams applying local and unofficial working practices |
| 07/2013 | Dangerous occurrence involving track workers near Roydon station | 2 | White | Improved methods by which planners assess the suitability of ‘Red Zone working’ when selecting an appropriate safe system of work | The risk identified by the RAIB could be addressed, at least in part, by the new track safety standard (019). However, the RAIB has doubts about the implementation of this standard so it is too early to judge whether the intent of the recommendation has been met |
| 20/2013 | Track worker struck by train at Bulwell | 1 | White | Providing information to planners about which safe systems of work are considered appropriate for specified sections of the line | Although actions are reported to have been taken to improve the selection of a safe system of work, the specific intent of the recommendation has yet to be addressed |
| 21/2013 | Fatal accident involving a track worker at Saxilby | 1 | Blue | Identifying and implementing suitable controls to assure the adequate performance of agency staff in safety leadership roles or reducing its dependence on such staff | The evidence provided to RAIB neither demonstrates that Network Rail has reduced its reliance on agency staff in safety leadership roles nor explains how the performance of agency staff in these roles is to be assured |
| 16/2017 | Track worker near miss incidents at Camden Junction South | 2 | Blue | Improved presentation of information in the Weekly Operating Notice to reduce the risk of confusion when arranging protection of engineering possessions (including the use of diagrams) | Network Rail has reviewed the recommendation and concluded that no change is required. This is surprising given the need to present such information clearly to those implementing pre-planned blockages of the line. RAIB is seeking evidence that the risk has been understood and properly addressed |
| 07/2017 | Class investigation into accidents and near misses involving trackworkers | 1 | Blue | Equipping safety leaders on site to recognise and deal effectively with circumstances not encompassed by their ‘safe system of work (local risk management) | RAIB has yet to understand how the specific intention of the recommendation has been addressed |
| 07/2017 | Class investigation into accidents and near misses involving trackworkers | 3 | Blue | Reviewing the competence requirements for safety leaders who are responsible for implementing safe systems of work on lines that are already open to traffic (including local knowledge) | The response provided to RAIB does not address the need for local geographic knowledge, which is one of the basic intentions of the recommendation |
| 07/2017 | Class investigation into accidents and near misses involving trackworkers | 5 | White | Improvements to the way that Network Rail collects, analyses and reports information on incidents and accidents to track workers (in order to provide a better understanding of the risks of each method of protection) | The response refers only to a risk assessment of the existing hierarchy, and makes no mention of the use of incident data to inform this assessment. It is therefore unclear how the intention of this recommendation has been addressed |
Recommendations in reports published in 2018
Recommendations made in 2018 were targeted at the following organisations (in some cases they were made to more than one implementer):
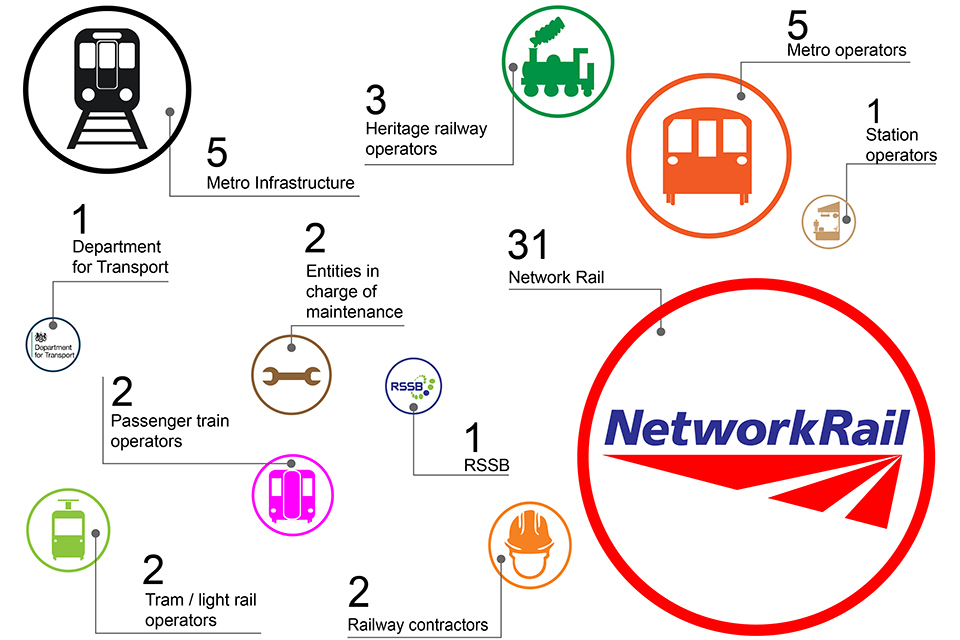
Graphic describing the organisations to which RAIB recommendations published in 2018 were directed. the larger the icon for that group or organisation, the more recommendations
Response to RAIB recommendations made in the Sandilands junction (Croydon tram) investigation
On 9 November 2016 a tram overturned on a sharp curve at Sandilands junction, Croydon. Seven passengers were killed and many more seriously injured. The anniversary of the publication of our report into this tragic accident occurred on 7 December 2018. Our report included 15 recommendations intended to improve tramway safety. These were addressed to the ORR as the Safety Authority for railways and tramways in Britain. In accordance with normal process, the ORR then passed 13 of these recommendations to the relevant duty holder for action. Two of the recommendations related to the ORR itself were addressed in accordance with the ORR’s own internal review process.
The ORR is required to ensure that all recommendations are duly taken into consideration and where appropriate acted upon, and to report to RAIB within twelve months of the recommendation being issued what action has been taken. We received that report on 4 December 2018 and it is published in full on the ORR website. We are grateful for the work that the ORR has undertaken with the tramway sector to help facilitate a coordinated response, and for the detailed report it has provided to us. The table below summarises the ORR’s current assessments of the status of the response to every recommendation, as reported to the RAIB by 31 December 2018. In some cases the nature and extent of actions reported to have been taken by the Croydon tramway are different from those reported for other tramways. For this reason the status of actions taken by Croydon is shown separately from the status of actions taken by others.
| REC | Subject | Croydon tramway | Other tramways | ORR |
|---|---|---|---|---|
| 1 | Industry safety body | IG | ||
| 2 | Industry review of risk | IG | IG | |
| 3 | Automatic speed control | IG | P | |
| 4 | Vigilance devices | IG | P | |
| 5 | Visual cues | IG | IG | |
| 6 | Passenger containment | P | P | |
| 7 | Emergency lighting | P | P | |
| 8 | Evacuation | P | P | |
| 9 | Regulatory framework | IG | ||
| 10 | Independent risk review | IG | ||
| 11 | Driver fatigue | IG | ||
| 12 | Organisational culture | I | ||
| 13 | Response to safety related reports | I | ||
| 14 | On-tram CCTV | I | ||
| 15 | Maintenance and testing documentation | I |
| Status | Explanation |
|---|---|
| I - Implemented | All actions to deliver a recommendation have been completed. |
| IG – Implementation ongoing | ORR is content with the proposed action plan to implement the recommendation and the timescale for delivery that has been presented by the end implementer. |
| P - Progressing | ORR is satisfied that the end implementer is taking suitable action to consider and address a recommendation, but a formal completion date has not yet been provided. |
Summary of the status of actions taken in response to the RAIB’s recommendations (as reported by ORR before 31 December 2018)
Since the end of 2018 further progress has been reported by the industry and the ORR has updated its assessment of the status of actions taken in response to the RAIB’s recommendations. Shown below is an updated summary table based on information provided by ORR to RAIB on 5 April 2019.
| REC | Subject | Croydon tramway | Other tramways | ORR |
|---|---|---|---|---|
| 1 | Industry safety body | I | ||
| 2 | Industry review of risk | IG | IG | |
| 3 | Automatic speed control | I | P | |
| 4 | Vigilance devices | IG | P/IG (see note 1) | |
| 5 | Visual cues | I | IG | |
| 6 | Passenger containment | P (see note 2) | P | |
| 7 | Emergency lighting | IG | P/I (see note 3) | |
| 8 | Evacuation | P | P | |
| 9 | Regulatory framework | I | ||
| 10 | Independent risk review | I | ||
| 11 | Driver fatigue | IG | ||
| 12 | Organisational culture | I | ||
| 13 | Response to safety related reports | I | ||
| 14 | On-tram CCTV | I | ||
| 15 | Maintenance and testing documentation | I |
Summary of the status of actions taken in response to the RAIB’s recommendations (as reported by ORR on 5 April 2019).
Note 1 - ORR has reported that Edinburgh Trams and West Midlands Metro/Transport for West Midlands are reviewing the setting of their existing driver vigilance systems.
Note 2 - RAIB has been informed that TfL London Trams/Tram Operations Ltd have now completed installation of film with enhanced strength to the windows of all trams operating on the Croydon system. Testing has shown that the containment provided by the windows will be improved.
Note 3 - Transport for Greater Manchester/Manchester Metrolink Ltd have included emergency lights that operate independently of the tram power supply in the specification of the new Metrolink fleet.
Examples of significant learning
Some of our investigations have contributed to enhancing industry’s understanding of specific areas of risk. We have made a number of wide ranging recommendations this year which have the potential to reduce that risk. Examples include:
- The investigation into the derailment of a freight train at Lewisham (report 04/2018) revealed some important learning concerning the processes that Network Rail uses to identify and manage risks associated with vertical track geometry features following track renewal and heavy maintenance and the design of modular switch and crossing layouts. These issues were addressed by RAIB’s recommendations.

Winter view of the derailment at Lewisham showing one vehicle on its side to the left and two vehicles upright but standing in the ballast.
- Our investigation into a collision between a car and the back of a stationary freight train that was standing on a level crossing at Stainforth Road level crossing near Doncaster (report 08/2018) revealed that the level crossing barriers lifted and the road traffic signals stopped showing despite the presence of the train. This happened because the level crossing controls, which dated back to the original installation in 1974, did not detect that the train was foul of the crossing. We recommended that Network Rail review the risks at other crossings with such controls and identify suitable risk mitigation measures to address them.
- Our investigation into the derailment of a passenger train after hitting a landslip at Loch Eilt (report 10/2018), in north-west Scotland led to a recommendation to take snow melt into account when assessing the risk of earthwork failures.

The two-car derailed train on the moors at Loch Eilt showing the submerged line and landslide.
- Following a collision between a train and a delivery van on a private crossing at Frognal Farm (report 12/2018) we identified the need for Network Rail to review and revise the information offered at private level crossings so as to enable their safe use by first time users. We also highlighted a need for a change in the law to allow signage to be improved and consideration of the role of the ‘authorised users’.

View of the approach to Frognal Farm user worked crossing showing a red and white Stop sing, the crossing phone and gate. A number of railworkers in high visibility clothing are on the scene.
- The investigation into the trap and drag accident at Notting Hill Gate (report 14/2018) led to a recommendation for London Underground to consider how the design of the task, equipment and training can influence train operators’ attention and awareness.

Platform CCTV of passengers at Notting Hill Gate underground station. The departing train is on the right of the image with a passenger and their clothing trapped in the doors.
- Our investigation into the detrainment of passengers from a London Overground train onto a line with live conductor rail, at Peckham Rye (report 16/2018) found that the railway industry’s control and command structures did not provide the support that the driver needed to safely manage the consequences of a train failure away from a station platform. We concluded that operations control and signalling staff had not been adequately prepared to safely manage stranded trains, and that the railway industry had placed too little emphasis on the need for practical training for those involved in such events.
- The collision and derailment just outside Waterloo station (report 19/2018) highlighted the extent to which some essential safety practices established after the Clapham junction disaster were not applied when signalling equipment was being altered and tested. RAIB recommended that Network Rail take steps to ensure the competence of signalling staff and to promote the attitudes and depth of understanding that is needed to properly appreciate the importance of applying all design, installation and testing processes.

The derailed train at Waterloo in blue, yellow and red livery after striking the barrier vehicles. Railway staff in high visibility clothing are in attendance
- The investigation into a narrowly avoided collision between a group of track workers and a train at South Hampstead (report 20/2018) revealed that the confused implementation of important new track safety rules contributed to the cause of the accident, as did the absence of signage at the access point (which has been the subject of previous RAIB recommendations).
5. Identification of important issues highlighted during 2018
While it is not intended to be a comprehensive list, the following topics were either prominent during 2018, or of particular concern to us:
- Design and operation of user worked level crossings
- Managing the risk at the platform-train interface (including trap and drag)
- The safe management of abnormal train operating events
- Protection of track workers from moving trains
Each of these topics is summarised below.
5.1 Design and operation of user worked level crossings
Overview
Where private roads, which lead to houses, farms or other commercial premises, cross the railway on the level, it is normally necessary for crossing users to operate the crossing gates or barriers themselves. Such crossings are referred to as user worked crossings (UWC). In many cases, it is not possible to obtain sufficient warning of approaching trains by looking along the line, and telephones are provided for users to contact the railway signaller to obtain permission to cross.
When someone with a vehicle wants to use a crossing, the signaller may give them permission to cross, if there is sufficient time for the user to do so before the next train will arrive at the crossing. In some circumstances, such as when the user has a slow vehicle or a number of animals, the signaller will stop any trains approaching the crossing until the user has reported that they have crossed over safely and are clear of the line.
Each crossing is provided with signs explaining how to use it. To supplement the signs, the authorised users, who have legal rights to pass along the road or track over the crossing, are given information by the railway about how to use the crossing. They should make arrangements, as far as possible, to pass this information on to their employees and other people who may have to visit the premises served by the crossing.
Most members of the public are unfamiliar with this type of level crossing, and it may not be possible for authorised users to brief people such as delivery drivers before they encounter the crossing for the first time. Safety in such circumstances relies firstly on the user understanding the signs and contacting the signaller before going over the crossing, and then acting on the information given to them. It is also vital that the signaller has adequate information available to assist them to make the correct decision when they are asked for permission to cross.
Some statistics
Number of accidents/incidents at UWCs investigated by the RAIB (full reports and Safety Digests)
| On Network Rail infrastructure | On other infrastructure | ||
|---|---|---|---|
| Number of investigations | Since October 2005 | 16 | 3 |
| In the last 5 years | 9 | 1 |
Important areas of safety learning
The key topics of concern to the RAIB that were highlighted or reinforced during 2018, and the associated areas for improvement, are summarised in the table below:
| Topics of particular concern to RAIB | Areas for improvement indentified by RAIB | Linked reports |
|---|---|---|
| Reliance on the authorised user briefing first time users of the UWC is no longer a credible means of risk control (in this era of multiple delivery agencies calling at properties) | Review the role and duties of the authorised user | 3, 7 |
| Design all UWCs such that they are suitable for use by first time users | 1, 3, 7 | |
| Regulations mandate potentially misleading signage that is not adapted to every type of UWC | Updating of the current regulations, the Private Crossings (Signs and Barriers) Regulations 1996, to enable the installation of more suitable signage | 3, 7 |
| At user worked crossings with telephones, a high reliance is placed on the signaller’s judgement when deciding if it is safe for road vehicles to cross | Better enable safe operation of UWCs with telephones by:
|
2, 4, 5 |
| Signallers are heavily dependent on the road user’s judgement of their vehicle type and the time it will take to cross | The need for improved communications protocols for signallers when dealing with road vehicle users | 4, 5 |
| Clarification of the method of operation for heavy and long vehicles at UWCs | 5 | |
| The potential for human errors at UWCs with power operated gates (POGOs) has not been sufficiently addressed | Improvements to signage and control systems associated with power operated gates at UWCs | 1, 3 |
5.2 Managing the risk at the platform-train interface (including trap and drag)
Overview
Every day, there are up to 20 million crossings of the platform-train interface as people get on and off trains and trams at stations and tram stops. Although the vast majority of these movements across the interface happen safely, there are several ways in which they can go wrong: people can be trapped in doors and dragged along, or fall onto the track and be struck by a train. The consequences of such events are often very serious.
The main risk that the operator is able to control is that from trap and drag incidents. Checking that everyone and everything is clear before the train/tram departs is crucial, but it can be challenging to manage the consequences of the way people behave, and the sheer numbers of people on platforms can make it hard for staff to see all the doors.
Some statistics
Number of accidents at the platform-train interface investigated by the RAIB (full reports and Safety Digests)
| Trap and drag in train doors | Other PTI accidents | ||
|---|---|---|---|
| Total number of investigations | Since October 2005 | 15 | 6 (includes 1 fatal accident) |
| In the last 5 years | 11 | 2 |
Important areas of safety learning
The key topics of concern to the RAIB that were highlighted or reinforced during 2018, and the associated areas for improvement, are summarised in the table below:
| Topics of particular concern to RAIB | Areas for improvement identified by RAIB | Linked reports |
|---|---|---|
| Door control systems are not always capable of detecting thin objects trapped in closed and locked doors | Enhancing the ability of door control systems to detect the presence of a trapped object (eg sensitive edges and/or anti-drag systems) | 1, 4, 5 |
People involved in train/tram dispatch:
|
Measures to address the risk of over-reliance on the door control system to detect trapped objects, and reinforcing the need for the final safety check by those involved with dispatch | 1, 2, 3, 4, 5 (and numerous previous investigations) |
| Measures to enhance the quality of the view of the interface between the platform and train/tram (particularly in crowded conditions) | 1 | |
| Loss of attention by drivers due to the repetitive nature of the task | Measures to support train and tram drivers in maintaining attention and awareness (particularly when associated with automatic train operations) | 1 |
| Research and development of technology to assist the dispatcher to determine that passengers are clear of the train | 5 | |
| Lack of passenger understanding of how train doors operate – some imagine that they will reopen like a lift door if obstructed | Research to better understand the way that passengers interact with rail vehicle/tram doors | Various |
5.3 The safe management of abnormal train operating events
Overview
Minor technical faults on trains are a daily reality on the railways, but sometimes these minor events, if not identified and dealt with effectively, can quickly develop into a potential safety incident.
When trains stop between stations, passengers can soon become worried or impatient. In some cases people may decide to make their own way out of the train and continue their journey on foot. In doing so they put themselves at risk and cause an escalation of the delay, as other trains have to be stopped and electric power may have to be turned off until the tracks are confirmed to be clear.
Dealing with such situations can be very challenging for train crew, as they may have technical tasks to perform as well as responding to the needs of the passengers. There can be particular problems on local and suburban trains which do not have toilet facilities, and may also be very crowded with standing passengers. It is therefore important that proper support is available for staff when trains are stranded, and that there are suitable, up-to-date and adequately rehearsed plans in existence for recovering the situation.
Some statistics
Number of investigations into the management of abnormal train operating events
| Number of investigations | Since October 2005 | 7 |
|---|---|---|
| In the last 5 years | 7 |
Important areas of safety learning
The key topics of concern to the RAIB that were highlighted or reinforced during 2018, and the associated areas for improvement, are summarised in the table below:
| Topics of particular concern to RAIB | Areas for improvement indentified by RAIB | Linked reports |
|---|---|---|
| Drivers only encounter train stranding/failure events very rarely and sometimes receive insufficient support | Improved support provided to drivers when dealing with out-of-course events such as SPADs and train failures | 1, 2, 3 |
| Poorly managed interfaces between different trains, signallers, and control offices | Improved communication and coordination between different railway companies’ command and control functions | 2, 3, 4 |
| The time taken for operators to recognise that a situation involving a stranded train is potentially dangerous and needs to be managed (early recognition) | Measures to help operating staff recognise that an incident involving a stranded train on a busy urban railway will rapidly become a ‘safety incident’ and that decisive action is needed to manage the situation | 3, 4 |
| The stranding of trains remote from stations | Measures to ensure that stranded trains are routed to locations where passengers can be safely evacuated, whenever possible (eg Emergency Permissive Working) | 4 |
| Ineffective management of train stranding incidents by signallers and operations controllers | Improved planning, and enhanced training and practice, to enable operating staff to effectively manage incidents where one or more trains are stranded | 3, 4 |
| Ineffective communications between drivers, signallers and controllers during an abnormal event | The need for clear safety critical voice communications between train drivers and signallers | 1, 2, 3, 4 |
| Insufficient preparedness for winter conditions, particularly in areas of third rail electrification | Reviewing the adequacy of existing measures (eg increasing the deployment of conductor rail heating in urban areas) | 4 |
5.4 Protection of track workers from moving trains
Overview
Before the accident at Stoats Nest Junction, it had been nearly five years since a track worker was struck and killed by a train. However, in that time there have been too many near misses in which workers have had to jump for their lives at the last moment.
Work involving inspection and maintenance of the railway’s track, structures and signalling equipment, must take place on and around the line. If this work is to be done while trains are running, automatic warning systems or human lookouts can be used to give warning of approaching trains. To protect a work site, the person in charge can arrange with the signaller for the line to be blocked to trains for short periods. For major planned works, the engineering staff can take possession of the line, blocking it to trains for a longer time.
When engineering possessions are set up, staff have to go onto the line to place boards and detonators to mark the limits of the protected site, and must return at the end of the work to remove this protection. In areas where the lines are electrified on the third rail system, two people are required to be present to carry out these duties.
Whatever the arrangements for protection, this type of work often involves small groups working without direct management supervision. Accurate planning, discipline, continuous vigilance and adherence to rules are vital to keep people safe.
Some statistics
Number of accidents/incidents involving track workers and moving trains that were investigated by the RAIB (full reports and Bulletins/Safety Digests)
| On Network Rail Infrastructure | On other infrastructure | |||
|---|---|---|---|---|
| Planned work on lines open to traffic (or unprotected) | Planned work on lines blocked to traffic | |||
| Total number of investigations | Since October 2005 | 23 | 15 | 2 |
| In the last 5 years | 11 | 11 | 1 | |
| Investigations into fatal accidents | Since October 2005 | 5 | 2 | 0 |
| In the last 5 years | 1 | 1 | 0 |
Important areas of safety learning
The key topics of concern to the RAIB that were highlighted or reinforced during 2018, and the associated areas for improvement, are summarised in the table below:
| Topics of particular concern to RAIB | Areas for improvement indentified by RAIB | Linked reports |
|---|---|---|
| The quality of leadership on site | Selecting and training leaders with the right qualities, and equipping them to manage the hazards and local conditions that they actually encounter on site | 2, 3, 4, 6, 8, 12 |
| The way that information is presented to track workers (signs and documentation) and to signallers | Measures to ensure that track workers are provided with concise, accurate and relevant information (including documents, and signs at site access points) to facilitate safe decision making | 4, 6, 10, 11, |
| Improved presentation of information in notices issued to signallers (eg Weekly Operating Notices), particularly in cases where one possession spans multiple work stations | 1, 11 | |
| Poor standards of lookout protection on lines that are still open to traffic | Developing the skills of those that plan and implement lookout protection, and the information available to them | 4, 8, 12 |
| Selecting the right people, with commensurate local knowledge, to lead work activities on lines that are still open to traffic | ||
| Managing the risk at locations with extended sighting times | ||
| The role and supervision of staff who install possession protection measures (boards and detonators) | Measures to ensure better management of the risk associated with the activities of possession protection staff | 7, 9, 10 |
| Management and supervision of contingent labour | Measures to ensure that ‘zero hours’ staff are suitably supervised and monitored (particularly in relation to hours of work) | 7, 13 |
| An unwillingness of staff, particularly those on zero hour contracts, to challenge unsafe practice | Promoting a just culture in which it’s OK to challenge unsafe working practices (regardless of the type of employment contract) | 3, 13 |
| Steps to mitigate the potentially adverse effect that client-contractor relationships can have on the willingness of contract workers to challenge unsafe systems of work | 3, 6 | |
| Ineffective planning | Use of clever and coordinated planning to minimise the work that is undertaken on lines that are open to traffic | 4, 8 |
| Introduction of the new ‘Person in Charge’ role – change management | Promoting a clearer understanding of the responsibilities in the revised track safety standard, NR/L2/0HS/019 (including those of the person in charge and the responsible manager) | 6 |
| Reviewing the way that important changes to track safety rules are managed |
6. Other activities and information about RAIB
International issues
During 2018 RAIB continued to be an active participant in the work of the EU Network of National Investigation Bodies (NIBs) and regularly attended its plenary meetings. This network has been established to further compliance with the legal obligation of NIBs to work together to conduct an active exchange of views and experience (as required by EU Directive 2004/49/EC). The RAIB has contributed to the establishment of a peer review regime for EU NIBs.
The RAIB has also strengthened its contacts with the National Transportation Safety Board in the USA and other non-EU investigation bodies throughout the world. In furtherance of these international contacts the Chief Inspector attended the annual meeting of the International Transport Safety Association in Baku and other international forums.
RAIB has maintained its good bi-lateral relations with each of the investigation bodies on the UK railway industry’s international borders, the Bureau d’Enquêtes sur les Accidents de Transport Terrestre, in France, and the Rail Accident Investigation Unit, in Ireland.
Rail accident investigators’ good practice seminar
In November we hosted our second seminar for accident investigators working in the UK heavy rail industry. More than 140 industry professionals attended to hear presentations on investigation techniques. Speakers from RAIB, the Healthcare Safety Investigations Branch, RSSB and Transport for London were able to share experiences and insight into the world of accident investigations.
We also held a similar event in Belfast on 27 November with colleagues from Northern Ireland Railways and Irish Rail to share experiences of investigative knowledge and lessons learned.
Working with the other Accident Investigation Branches
During 2018 the RAIB has continued to work closely with the other two transport accident investigation branches (Air and Marine). The three Chief Inspectors strongly believe that closer co-operation will benefit all of the branches. It was for this reason that the year saw the creation of a formally constituted Tri-branch Management Board to promote improvements to the three AIBs’ effectiveness, efficiency and resilience, whilst also safeguarding their functional independence in the selection and conduct of investigations. It was also good to welcome Sir Richard Garwood as the newly appointed part-time non-executive Chair of the board.
RAIB’s own safety record
We provide an operational response to railway accidents and incidents, which vary in nature, scale and environment. As part of this work, our staff can face significant health and safety risks. We have developed our own Safety Management System which includes our health and safety policy and arrangements for how we manage risk. It also sets out a system for the real-time assessment of risk by means of a process known as Dynamic Risk Assessment.
We monitor our own health and safety performance as an integral part of our management and governance process. This process also includes a Health, Safety and Welfare committee which is chaired by the Chief Inspector.
Six minor injuries to our staff were reported during 2018. Each of these was recorded and investigated.
Funding
Our operating budget for the 2018-19 financial year was £4.8m. The following graph shows this in relation to the last five financial years.
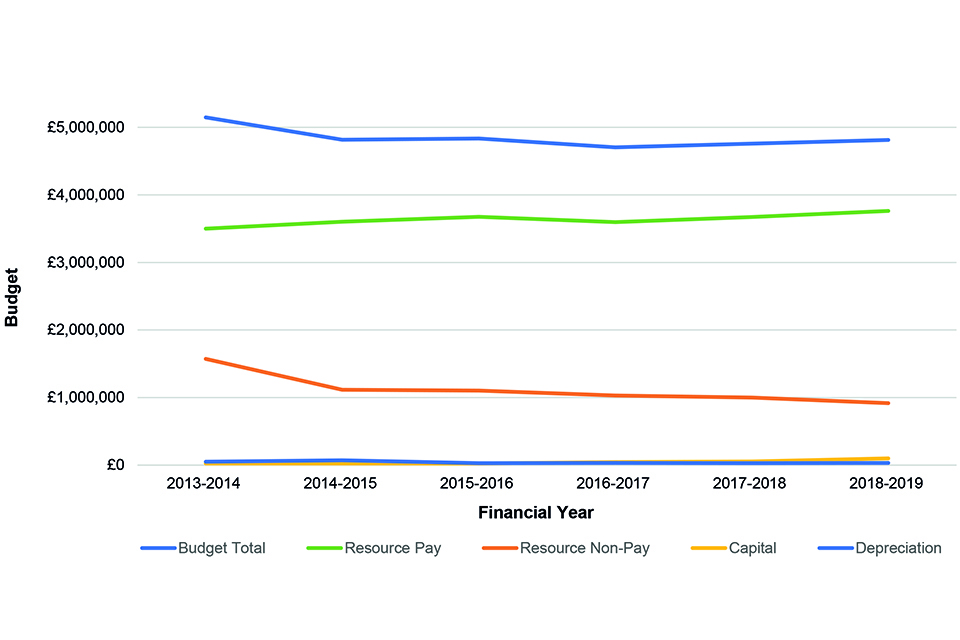
Line graph describing the RAIB budget across the financial years 2013 - 2019
7. Appendices
7.1 Appendix A – Investigations completed and commenced in 2018
Table A1 provides details of all RAIB investigations published during 2018. Details of all investigations started by RAIB during 2018 are provided in table A2.
We classify our investigations according to Article 19 of guidance published by ERA. This guidance promotes consistent categorisation of investigations in accordance with the Directive. The classifications are:
- Article 19(1) - a serious accident where the investigation is mandatory
- Article 19(2) - an accident or incident, which under slightly different conditions might have led to a serious accident, ie a narrowly avoided serious accident
In both tables, all investigations started under article 19(2) were undertaken on the basis of the potential or actual seriousness of the accident or incident; the schedule 19(1) threshold was not reached.
You can read summaries of all of our current investigations.
Table A1 – Full investigations completed in 2018
| Report Number | Event date | Publication date | Title of the investigation (location) | Occurrence type | Basis for investigation |
|---|---|---|---|---|---|
| 01/2018 | 17/10/2017 | 11/01/2018 | Runaway of a maintenance train near Markinch, Fife | Runaway incident | 19(2) |
| 02/2018 | 22/06/2017 | 30/01/2018 | Child nearly falling through missing toilet floor, South Devon Railway | Train defects | 19(2) |
| 03/2018 | 28/05/2017 | 19/02/2018 | Trailer runaway near Hope, Derbyshire | Runaway incident | 19(2) |
| 04/2018 | 24/01/2017 | 28/02/2018 | Freight train derailment at Lewisham, south-east London | Freight train derailment | 19(2) |
| 05/2018 | 07/07/2017 | 20/03/2018 | Explosion inside an underframe equipment case at Guildford | Train defects | 19(2) |
| 06/2018 | 28/07/2017 | 09/05/2018 | Passengers struck by a flying cable at Abergavenny station | Infrastructure failure | 19 (2) |
| 07/2018 | 01/06/2017 | 21/05/2018 | Fatal accident at Trenos footpath crossing near Llanharan, Rhondda Cynon Taf, South Wales | Level crossing fatality | 19(1) |
| 08/2018 | 11/01/2018 | 19/07/2018 | Collision at Stainforth Road level crossing | Level crossing minor damage | 19(2) |
| 09/2018 | 14/08/2017 | 02/08/2018 | Freight train derailment at Ely West Junction | Freight train derailment | 19(2) |
| 10/2018 | 20/01/2018 | 07/08/2018 | Landslip and derailment at Loch Eilt, north-west Scotland | Passenger train derailment | 19(2) |
| 11/2018 | 05/10/2017 | 09/08/2018 | Near miss with a group of track workers at Egmanton level crossing | Staff hit by train (near miss) | 19(2) |
| 12/2018 | 23/10/2017 | 23/08/2018 | Collision at Frognal Farm User Worked Crossing | Level crossing injury | 19(2) |
| 13/2018 | 21/02/2018 | 28/08/2018 | Near miss with track workers at Pelaw North Junction | Staff hit by train (near miss) | 19(2) |
| 14/2018 | 31/01/2018 | 03/09/2018 | Passenger trapped and dragged at Notting Hill Gate station | Train movement accidents inv pax/pedestrians | 19(2) |
| 15/2018 | 15/12/2017 | 10/09/2018 | Pushchair trapped in tram doors and dragged, Nottingham | Near miss (non level crossing) | 19(2) |
| 16/2018 | 07/11/2017 | 09/10/2018 | Detrainment of passengers onto electrically live track near Peckham Rye station | Electric shock (near miss) | 19(2) |
| 17/2018 | 30/10/2017 | 16/10/2018 | Extensive track damage between Ferryside and Llangennech, Carmarthenshire | Train defects | 19(2) |
| 18/2018 | 15/03/2018 | 12/11/2018 | Runaway hand trolley at Ramsbottom, East Lancashire Railway | Runaway incident | 19(2) |
| 19/2018 | 15/08/2017 | 19/11/2018 | Collision at London Waterloo | Collision with other train | 19(2) |
| 20/2018 | 10/03/2018 | 18/12/2018 | Near miss with track workers and trolleys at South Hampstead, London | Staff hit by train (near miss) | 19(2) |
Table A2 – Full investigations commenced in 2018
| Event date | Title of the investigation (location) | Occurrence type | Basis for investigation |
|---|---|---|---|
| 11/01/2018 | Collision at Stainforth Road level crossing | Level crossing collision (Minor damage) | 19(2) |
| 22/01/2018 | Landslip and derailment at Loch Eilt, north-west Scotland | Passenger train derailment | 19(2) |
| 31/01/2018 | Passenger trapped and dragged at Notting Hill Gate station | Train movement accident involving a passenger | 19(2) |
| 21/02/2018 | Near miss with track workers at Pelaw | Staff hit by train (near miss) | 19(2) |
| 02/03/2018 | Stranding of trains and self-detrainments at Lewisham | Train movement accident involving passengers | 19(2) |
| 10/03/2018 | Near miss with track workers and trolleys at South Hampstead, London | Staff hit by train (near miss) | 19(2) |
| 16/03/2018 | Runaway hand trolley at Ramsbottom, East Lancashire Railway | Runaway incident | 19(2) |
| 08/06/2018 | RRV runaway at Bradford Interchange | Runaway incident | 19(2) |
| 20/07/2018 | Track worker near miss at Peterborough | Staff hit by train (near miss) | 19(2) |
| 17/08/2018 | Safety incident at Bagillt user worked crossing | Level crossing near miss | 19(2) |
| 01/09/2018 | Train door incident, Jubilee Line (Finchley Road) | Train defects | 19(2) |
| 04/09/2018 | Collision between a freight train and a utility vehicle in Dollands Moor yard | Staff hit by train (Injury) | 19(2) |
| 07/09/2018 | Train door accident at Elstree & Borehamwood station | Train movement accident involving a passenger | 19(2) |
| 11/09/2018 | Collision between a tram and a pedestrian, Edinburgh (Saughton) | Train movement accidents involving a pedestrian | 19(1) |
| 19/09/2018 | Collision between road-rail vehicles near Cholmondeston | Collision with other train | 19(2) |
| 19/10/2018 | Overspeeding at Sandy | Near miss (non-level crossing) | 19(2) |
| 06/11/2018 | Fatal accident at Stoats Nest Junction | Staff hit by train (fatality) | 19(1) |
| 01/12/2018 | Fatal accident involving a passenger on a train at Twerton near Bath | Train movement accident involving a passenger | 19(1) |
| 02/12/2018 | Near miss with track worker near Gatwick Airport station | Staff hit by train (near miss) | 19(2) |
7.2 Appendix B – safety digests commenced in 2018
Table B1 Safety digests commenced or completed in 2018
| Event date | Publication date | Digest number | Title of the investigation (location) |
|---|---|---|---|
| 06/11/2017 | 07/02/2018 | D01/2018 | Derailment of a passenger train near Wimbledon, south-west London |
| 17/01/2018 | 06/03/2018 | D02/2018 | Near miss with staff at Clapham Junction, London |
| 02/03/2018 | 23/05/2018 | D03/2018 | Near miss with a train driver at Stafford station |
| 08/04/2018 | 18/06/2018 | D04/2018 | Operational incident following signal passed at danger, Bethnal Green |
| 25/02/2018 | 26/06/2018 | D05/2018 | Passenger train striking rail on the track at Cradlehall, near Inverness |
| 10/06/2018 | 25/07/2018 | D06/2018 | Derailment of a passenger train near Clogwyn y Gwin South foot crossing, Welsh Highland Railway |
| 26/03/2018 | 29/08/2018 | D07/2018 | Passenger trapped in train doors and dragged at Bushey station |
| 30/05/2018 | 10/09/2018 | D08/2018 | Passenger trapped in tram doors and dragged at Bury tram stop, Greater Manchester |
| 07/07/2018 | 11/09/2018 | D09/2018 | Near miss at Plain Moor user worked crossing, Barton-le-Willows, North Yorkshire |
| 19/07/2018 | 28/09/2018 | D10/2018 | Tram overspeeding on a curve, Sheffield |
| 10/07/2018 | 19/10/2018 | D11/2018 | Near miss with track workers at Dundee |
| 25/07/2018 | 22/10/2018 | D12/2018 | Runaway of two coaches at Bitton, Avon Valley Railway |
| 29/10/2018 | 31/01/2019 | D01/2019 | Derailment at Dunkeld |
| 12/12/2018 | n/a | n/a | Near miss with track workers at Sundon |
| 21/12/2018 | 18/04/2019 | D04/2019 | Derailment of locomotive at Doncaster |
7.3 Appendix C – Urgent Safety Advice issued in 2018
We can issue urgent safety advice at any stage during an investigation when we believe there is a need to provide immediate information to the relevant industry bodies about the wider safety issues we have identified.
If the issue affects other European member states we report the safety advice to ERA via their safety information system (SIS); this action alerts all member states to the advice.
During 2018 we issued urgent safety advice on three occasions.
| Event date | Event | Urgent service advice | Date of USA |
|---|---|---|---|
| 15/12/2017 | Pushchair trapped in tram doors and dragged, Nottingham | Checking that tram doors are safe before departing from tram stops | 07/02/2018 |
| 25/02/2018 | Passenger train striking rail on the track at Cradlehall, near Inverness | Safety of the line after engineering work | 19/03/2018 |
| 19/10/2018 | Overspeeding at Sandy | Driver awareness of emergency speed restrictions | 29/11/2018 |
-
Figures do not include class investigations (which address more general safety issues). ↩
-
The safety authority is a body responsible for regulating railway safety; for Great Britain this is the Office of Rail and Road (ORR); for the Channel Tunnel it is the Intergovernmental Commission and for Northern Ireland it is the Department for Infrastructure. ↩