
Passenger train striking rail on the track at Cradlehall, near Inverness, 25 February 2018
Published 26 June 2018

© Crown copyright 2018
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/safety-digest-052018-cradlehall/passenger-train-striking-rail-on-the-track-at-cradlehall-near-inverness-25-february-2018
1. Important safety messages
The incident demonstrates the importance of:
- The Person in Charge making sure that suitable arrangements are in place to confirm that the line is clear and safe for the passage of trains, and that these arrangements are properly implemented
- Maintaining the same levels of supervision and discipline for all work sites, whether they be complex or simple, as this incident shows how an omission at a site of work with a perceived low risk can still result in a potentially catastrophic outcome
2. Summary of the incident
On 25 February 2018 at about 09:47 hrs, train 1E17, the 09:40 hrs service from Inverness to London, travelling at about 53 mph (85 km/h), struck the end of a 130 metre long section of rail. The rail had been left between the two running rails (in the four-foot) with one end resting on the left-hand rail of the up line, following an overnight engineering possession at Smithton, near Cradlehall, a short distance south of Inverness.
The train pushed the whole length of rail from the four-foot into the cess (beside the line) but did not derail. Had circumstances been slightly different there is little doubt that the impact from the rail could have derailed the train, resulting in a far more serious accident.

Image from Forward Facing CCTV of train 1E17 showing the rail just prior to impact (image courtesy Virgin Trains East Coast)
3. Background
The track maintenance work that took place during the night before the incident had been planned by Network Rail’s Scotland Route. The work was being carried out in preparation for the later replacement of rails, and comprised renewal of rail fastening components, including sleeper pads, rail clips and associated components. An earlier planning visit to the site had also identified eight new lengths of rail awaiting installation that needed to be moved, as they were seen as potential tripping hazards for the planned work. The rails were to be moved using a crane attachment on a road/rail vehicle (RRV).
The work was to take place within a planned overnight possession near Cradlehall from 23:15 hrs on Saturday 24 February 2018, until 09:35 hrs on Sunday 25 February. The site was approximately 2 km (1.25 miles) long, and the planned work was straightforward, involving the dropping of materials and movement of rails.
The staff undertaking the work consisted of a person in charge of the possession (PICOP), an engineering supervisor (ES) and two controllers of site safety (COSS), who were managing the two separate work groups working within the possession. One COSS was acting as a machine / crane controller supervising a machine operator operating a road/rail vehicle. The other COSS was tasked with supervising a group of track workers who were clearing the ballast around the sleepers and rail clips.
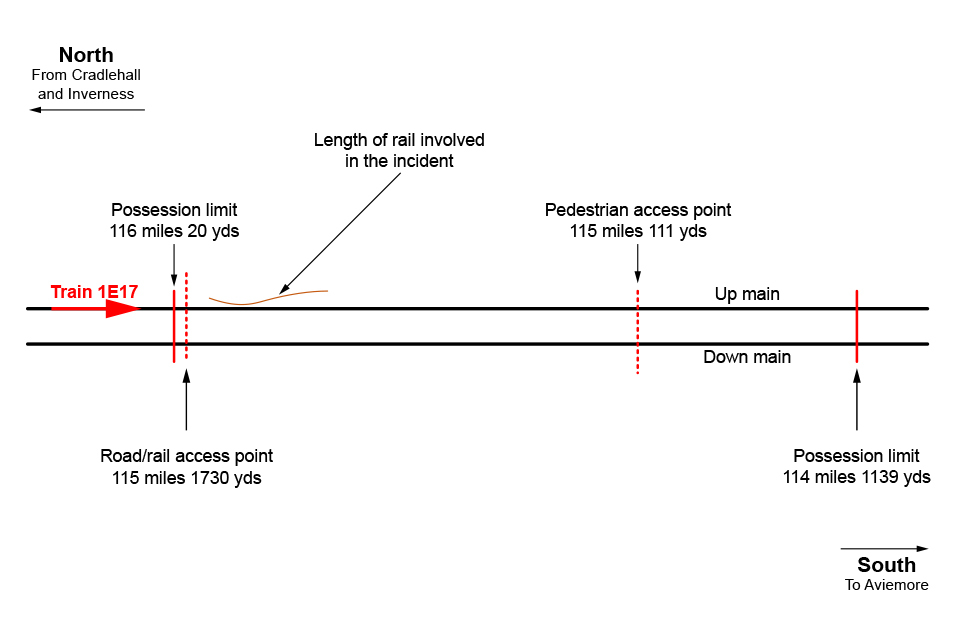
Diagram of location (not to scale)
The start of the possession was delayed by two hours because a signal post replacement key for a protecting signal for the possession limits could not be found, and the possession was eventually granted at 01:30 hrs.
At approximately 01:45 hrs the ES contacted each COSS to allow the track workers and RRV to access the sites of work, via the road/rail access point located close to the 116 milepost. Both the PICOP and ES then joined the work groups.
The machine controller / COSS and machine operator on-tracked the RRV and travelled to the southern end of the possession, where they were instructed by the PICOP to move two of the eight new rails from the four-foot of the up main line to the four-foot of the down main line. The PICOP then instructed the COSS and machine operator to help the other track workers, who were clearing the ballast from the areas around the track clips, and offloading the track clipping components from the trailer attached to the RRV to be dropped into the cess along the whole length of the possession. After a period, they were asked to leave the other trackworkers and form a separate work group to move the remainder of the new rails. The RRV and trailer travelled north to the road/rail access point, where the trailer was detached from the RRV.
There is conflicting evidence as to if, and when, a conversation took place between the PICOP and the machine controller and operator, regarding the movement of the rail that was later struck by the train. This rail had not been included in the original eight which the PICOP had planned to be moved. It was located in the down cess (the space alongside the track), near to the north end of the possession. The PICOP and ES have stated that they both believed this rail needed to be moved further away from the running rail, and instructed the machine controller and operator to move it, but that it should remain in the cess.
After moving this rail, the machine controller and machine operator then took their RRV south, and moved the remaining six new rails from the four-foot of the down line to the four-foot of the up line.
While this work was taking place, the other group of track workers were still working northwards through the possession, clearing the remaining ballast from the areas where the track clipping components were to be replaced. At some point during the night the two work groups passed each other.
At approximately 05:50 hrs towards the end of the shift, the machine controller and operator, who had now dropped the materials and moved the rails, met with the PICOP and ES and confirmed that they had completed their work and asked if they could go home. This was agreed and they both travelled back to the road/rail access point at 115 miles 1730 yards, off-tracked the RRV and departed from the site. Some of the remaining track workers continued working northwards but did not see that the incident rail was foul of the line, and the PICOP and ES later left the possession by the pedestrian access gate (at 115 miles 111 yards), where they were picked up by a road vehicle and travelled back to the road/rail access point. On his arrival at the access point the PICOP observed that the RRV and trailer had been off-tracked. He contacted the signaller and handed back the possession at 06:30 hrs. At about 09:47 hrs, train 1E17 travelling from Inverness to London struck the end of a piece of rail at about 53 mph (85 km/h).
The train driver checked the train but did not identify any damage. He contacted the signaller and the train was authorised to continue its journey. When the train called at Dunkeld and Birnam, the train driver undertook another visual check of the train, at the request of the train operator’s maintenance controller. The train driver then reported that the lifeguard had been damaged. The train was authorised to continue to Perth, where the passengers were transferred to another train. The damage to the lifeguard shows that it had struck the end of the rail at an angle and deflected the rail to the left, and pushed the whole length of rail from the four-foot into the cess as the train slowed to a stand. The impact had sheared one of the two bolts that retains the lifeguard in place.

The rail after being struck by the train

(Left-hand image) the end of the rail, showing the impact mark and (right-hand image) the damaged lifeguard
4. Cause of the incident
The delay at the start of the possession affected the task briefing of the safe work pack. Witness evidence shows the briefings were ad-hoc and were probably undertaken by various members of staff (team leaders and other depot technicians who had some awareness of the site). Witnesses also indicate that this confused staff as to who was actually in charge and what roles they were each performing.
There is conflicting evidence about whether the PICOP instructed the machine controller, also acting as a COSS, and the machine operator to move the incident rail away from the running line. Witness evidence indicates that the machine controller and machine operator decided not to move the rail further into the cess because they believed it would compromise an axle counter (a piece of equipment that is used to detect the presence of trains) in the vicinity. They decided instead to move the rail into the four-foot. Photographic evidence shows that an axle counter was present, but its location would not have prevented the rail being safely moved into the cess.
Having made the decision to move the rail to a different location, the machine controller did not tell anyone else what had been done. The machine controller and machine operator did not fully check the site after they moved the rail.
Witness evidence shows that the machine controller, who was acting as the COSS for this two person workgroup, believed that it was not his responsibility to check the site was safe for running trains, as this was the responsibility of the ES. However, the ES believed that the work site was too long for it to be his responsibility to check it, and that this was the sole responsibility of the COSS who was also acting as the machine controller.
Both the ES and PICOP felt sure that the site was safe to hand back, as they had, albeit at different times during the night, seen the whole length of the possession and the activities that had taken place. Materials that had been dropped were in safe positions, and rails that were considered to be tripping hazards had been moved. They therefore believed a final walk through the whole possession was not required.
When the PICOP and ES returned to the road/rail access point by road, the end of the incident rail was only 90 metres away, but it was dark, there was insufficient lighting to illuminate a wide area, and the rail was not visible. The ES and PICOP both believed the section of rail they had asked to be moved was still in the cess of the down line.
Section 4.14 of Network Rail’s standard NR/L2/OHS/019 module 02 ‘Planning and working within a possession’ (standard 019), states that when work is completed, the Person in Charge shall check that everyone they are responsible for is clear of the line, and that the site is left in a safe state. In this case the role of Person in Charge had been allocated to the PICOP by the planner, although the PICOP was not aware of this as the planner had not advised him, and having to deal with the delays at the start of the shift meant that he had not read the safe work pack properly.
The Rule Book, GE/RT8000/HB12, Handbook 12 ‘Duties of the engineering supervisor (ES) or safe work leader (SWL) in a possession’ says that when a COSS has signed the work site certificate to confirm that they no longer need the ES’s protection, the ES must contact the PICOP and ask for permission to remove the work site marker boards once the line is clear of all engineering trains or on-track plant such as RRVs.
After the PICOP at Cradlehall had agreed with the machine controller and operator that they could leave the site, there was no opportunity for further discussion of the work they had undertaken. Likewise, the machine controller believed that the once the PICOP had verbally agreed to his request to leave the worksite, in the presence of the ES, he did not need to contact the ES or the PICOP again.
The off-tracking of the RRV and trailer led the ES and PICOP to the view that the machine controller and operator, and all of the equipment, were clear of the line and the work was complete.
Handbook 12 states that the ES must tell the PICOP that the line is safe and clear, for the work site to be given up. The PICOP was subsequently advised by the Engineering Supervisor that the protection was no longer required, and the possession was handed back safe for the passage of trains at 06:50 hrs with a piece of rail lying across the head of the running rail.
5. Previous similar occurrences
On 6 October 2014, a passenger train was damaged when it struck a cabinet door in Watford tunnel, Hertfordshire. The RAIB investigated the incident, and concluded that the COSS had advised the ES and PICOP that the line was safe for the passage of trains, without checking that the cabinet door had been properly secured after work had been carried out in the tunnel during the night. As a consequence the RAIB made the following recommendation:
‘Network Rail should implement a means to meet the rule book requirement for the designated person (Engineering Supervisor or Safe Work Leader) to confirm to the PICOP that the railway is safe and clear for the passage of trains when that designated person is not present on site.’
See RAIB report 12/2015.
The intention of this recommendation was for Network Rail to make explicit its processes for handing back a work site so as to reduce the risk arising from the railway not being safe and clear for the passage of trains.
In 2017 Network Rail reported to the Office of Rail and Road (ORR) that it had implemented the recommendation through the introduction of the role of Person in Charge in the latest version of standard 019, to manage risks during work on the track. The Person in Charge is responsible for all aspects of safety during and on completion of the work. The revised standard is intended to provide greater clarity about who is responsible for the safety of the task.
In June 2017 staff at the delivery unit in Inverness were given a short briefing on the role of the Person in Charge and the changes within standard 019. The briefing was given at the depot prior to the start of a possession. Witness evidence indicates that the staff did not fully understand the significance of the change, and the role and responsibilities of the Person in Charge.
On 18 June 2015, a passenger train struck a wooden sleeper on the line near Somerleyton, Suffolk. The previous day, the sleeper had fallen from a trailer which had been used to collect scrap material from the lineside. The RAIB bulletin reinforced the need for clarity on who is responsible for ensuring the safety of the line at the conclusion of engineering work. See RAIB bulletin 03/2015.
On Northern Ireland Railways infrastructure on 4 February 2016, a passenger train travelling from Belfast Great Victoria Street to Portadown collided with an excavator bucket which had been left on the track near Knockmore Junction. The bucket had been detached from an excavator undertaking track maintenance work during the previous night when regular train services were not running. There was no effective process for checking that the track was clear of obstructions before the line was reopened to regular services. See RAIB report 20/2016.
The RAIB made two recommendations addressed to Northern Ireland Railways. The first related to introducing a formalised process for checking that lines are safe after engineering work is complete and before the line is reopened to regular traffic. The second recommended a review and possible modifications to the formalised communication arrangements used by engineering supervisors controlling access to the railway.
On 15 May 2017, an on-track machine leaving an engineering possession near Kirkham, Lancashire, encountered a large tubular steel pile obstructing the line on which it was travelling. The pile had been left on the track during engineering work earlier in the night, and was overlooked when the work site was handed back. The RAIB safety digest emphasised the importance of having a formal, well briefed process for checking that a site of work is clear of materials and equipment before notifying the engineering supervisor that the line is safe for the passage of trains. See RAIB safety digest 11/2017.
At East Somerset Junction, near Frome, on 13 May 2018, a passenger train struck an object on the track. The train did not derail. The driver examined the train and advised that the cab steps were missing from the train along with some damage to the flange of the leading wheelset. Investigations into the incident revealed that a rail skate belonging to a welding team had been struck and was badly damaged. It was also established that the rail skate had been used during an overnight engineering possession between Blatchbridge Junction and Bruton, which included the blockage of the Westbury lines. The possession had been handed back at 05:42 hrs.
At Primrose Hill on 11 March 2018, a group of track workers narrowly avoided being struck by a passenger train as it passed between South Hampstead station and Primrose Hill tunnels, travelling towards London Euston on the up fast line.
The track workers, who believed that they were working on the up slow line, heard shouted warnings from other workers who had become aware of the sound of the train’s warning horn and saw the headlights of the approaching train. They immediately began to get out of the way and removed two trolleys that they had placed on the track. The track workers and trolleys were clear of the approaching train around two seconds before the train passed.
The RAIB is investigating this incident. The investigation will consider the adequacy of Network Rail’s processes for ensuring the safety of staff and review the extent to which the role of Person in Charge was understood and implemented by those involved.
6. Urgent Safety Advice
Following the incident at Cradlehall, and in the light of the other incidents listed above, the RAIB issued urgent safety advice (USA 02/2018) to Network Rail on 19 March 2018. The company was advised to take urgent steps to review the effectiveness of the actions it had taken to address the risk of objects being left on the line after engineering work, and to implement measures to ensure the safety of the line.
You can print this safety digest.