Adult social care monthly statistics, England: April 2022
Published 14 April 2022
Applies to England

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/statistics/adult-social-care-in-england-monthly-statistics-april-2022/adult-social-care-monthly-statistics-england-april-2022
Main points
COVID-19 testing in care homes
ln the week ending 22 March 2022:
- there were 17,646 positive lateral flow test results among staff which is the highest number recorded since the start of the pandemic, surpassing figures recorded in the previous peak in the week ending 4 January 2022 (17,555)
- there were 3,207 positive tests results among residents, which is also higher than the previous peak in the week ending 4 January 2022 (2,411)
Since the beginning of March 2022, the number of positive tests returned from both lateral flow devices and PCR tests has increased substantially for both staff and residents, following the previous decline in January and February. These trends may be partially influenced by the changes to testing guidance in care homes, however the overall number of tests conducted only slightly increased this month.
COVID-19 and flu vaccination in social care settings
As of week ending 22 March 2022, the proportions who had received a first booster dose of the COVID-19 vaccine were:
- 89.7% of total residents and 53.1% of total staff of older adult care homes
- 81.0% of total residents of younger adult care homes
- 49.0% of total staff of younger adult care homes and 44.8% of total domiciliary care staff
As of week ending 22 March 2022, the proportions who had received their flu vaccination for the 2021 to 2022 season were:
- 84.5% of total residents and 26.8% of total staff of older adult care homes
- 74.6% of total residents of younger adult care homes
- 25.4% of total staff of younger adult care homes and 19.1% of total domiciliary care staff
Infection control measures in care homes
In the week ending 22 March 2022:
- 88.3% of care homes in England were able to accommodate residents receiving visitors. This was a slight decrease compared to the previous week, following a period of substantial increase from the end of January 2022 through to mid-March 2022
- 81.6% of care homes who had staff required to self-isolate paid those staff their full wages while self-isolating. This proportion has remained consistent since mid-December 2020
- 69.0% of care homes had no staff members working in another health or social care setting. This proportion has been stable since the end of November 2021, after a period of gradual decline from April 2021
Staff absences due to COVID-19
In the week ending 22 March 2022:
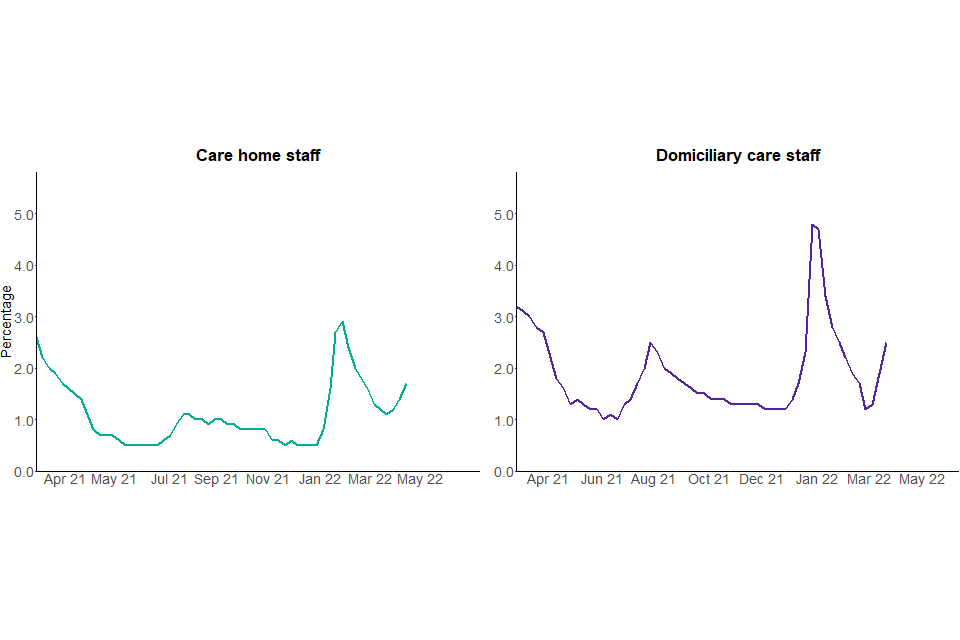
- 1.7% of care homes staff and 2.5% of domiciliary care staff were absent due to COVID-19 related reasons
These proportions have been increasing since the week ending 8 March 2022, following a period of decline between mid-January and the start of March 2022.
Introduction
This is a monthly publication by the Department of Health and Social Care (DHSC) of statistics on adult social care in England. This statistical bulletin provides an overview on a range of information on social care settings, with a focus on the impact of COVID-19.
This report provides newly published information on:
-
selected infection prevention control (IPC) measures in care homes at national, regional and local authority level
-
staffing levels in care homes at national, regional and local authority level
-
staff absence rates due to COVID-19 in care home and domiciliary care at national, regional and local authority level
-
personal protective equipment (PPE) availability in care homes and domiciliary care at national, regional and local authority level
-
testing for COVID-19 in care homes at national, regional and local authority level
-
flu vaccination for the 2021 to 2022 flu season in adult social care settings at national, regional and local authority level
This report also includes previously published statistics on uptake of first, second and booster doses of COVID-19 vaccinations in adult social care settings.
For more information and links to other published sources of adult social care data see the ‘About this data’ section below.
Publication updates
Updates on this month’s report
This month’s report includes the national estimates for availability of PPE in domiciliary care, which had been suppressed in previous months due to data quality issues with figures from the London region. The updated national figure in this report excludes the data from providers in the London region and no data from local authorities in the London region are presented in the data tables.
This is because of incomparable data between London and other regions. For a number of providers in London, responses are collected via the London Association of Directors of Adult Social Services (ADASS) before being uploaded to Capacity Tracker in bulk. Due to differences in the interpretation of the wording of the questions asked by London ADASS about specific items of PPE stock, the data collected via this channel is not comparable to the data collected directly via Capacity Tracker. Work is currently being undertaken to review the data collection on availability of PPE across regions.
Updates on future reports
The next publication will be published on 12 May 2022. Dates for future publications will be pre-announced on the GOV.UK publication release calendar.
On 21 February 2022, DHSC published new guidance on Living with COVID, which outlines the government’s plan for removing the remaining legal restrictions while protecting people most vulnerable to COVID-19 and maintaining resilience.
On 31 March 2022, DHSC published new infection prevention and control guidance on managing specific infections and a supplement that sets out how to reduce the spread of COVID-19 in adult social care settings in England, which both apply from 4 April 2022.
In light of this new guidance and the end of the Adult Social Care Infection Control Fund on 31 March 2022, data items within Capacity Tracker, which is the adult social care COVID-19 data collection tool, are undergoing a review, in partnership with care providers, the Care Quality Commission (CQC), and local government. As an important proportion of this publication relies on this data collection, substantial changes to the publication might occur from May 2022.
The Adult Social Care Infection Control Fund was first introduced in May 2020, to support adult social care providers in England to reduce the rate of COVID-19 transmission and was then extended in September 2021 until the end of March 2022. During this period, providers received funds expected to be spent on infection prevention and control measures including ensuring that staff who are isolating receive their normal wages and limiting staff movement between settings, among other measures.
From the end of March 2022, the government will not provide any further funding for COVID-19 positive social care staff to stay away from work and the staff movement restrictions will be lifted, allowing pressure on workforce to be alleviated. As a result, the data on these 2 measures ceased on 4 April 2022, therefore the timeseries for these 2 metrics will end on 29 March 2022. The end of the timeseries will be presented in the May 2022 publication data tables but these tables will no longer feature in subsequent publications.
In addition, as the seasonal flu vaccination campaign comes to an end, the collection of data on flu vaccination will be temporarily ceased. The timeseries for flu vaccination will end on 29 March 2022 and the data tables will feature in the May 2022 publication, but not in subsequent publications, until data is collected again next winter.
Since 4 April 2022, providers are asked to record spring booster vaccinations in Capacity Tracker. Data on spring boosters will be published in future reports.
The changes listed above do not, however, affect this month’s report. The data included in this report goes up to 22 March 2022, whereas these changes took effect on 4 April 2022.
More information on the adult social care COVID-19 data collection tool can be found in the background quality and methodology note.
COVID-19 and flu vaccination in adult social care settings
How the data can be used
This data can be used for:
-
comparing vaccination rates across local authorities and regions in England as self-reported by care providers for the:
- first, second and booster doses of the COVID-19 vaccine
- flu vaccinations for the 2021 to 2022 season
-
monitoring vaccination rates over time for the:
- first, second and booster doses of the COVID-19 vaccine
- flu vaccinations for the 2021 to 2022 season
This data cannot be used for:
- estimating the number of social care staff or residents who have not been vaccinated
- estimating the number of social care staff or residents who have been vaccinated abroad
- comparing with vaccination rates in other countries of the UK
- directly comparing vaccination take up rates between different types of care home staff (directly employed and agency staff)
- estimating the number of vaccinations delivered each day
Booster rates do not distinguish between those who are eligible for a booster, given the recommended gap between second dose and first booster dose.
The total number of staff and residents for each social care setting as well as the number reported to be vaccinated for COVID-19 and flu are self-reported by the care provider and local authorities. As a result, the rates in this publication refer to the percentage of staff and residents reported to be vaccinated by care providers. This means that the number of individuals who have not received the vaccine cannot be directly derived from data published in these statistics as there is a number of individuals for whom the vaccination status is unknown to the care provider.
The dates in this section refer to the dates on which vaccinations were reported by care providers as opposed to the dates on which vaccinations were administered.
Some care providers have reported the total number of staff or residents but not the numbers vaccinated. As a result of this, vaccination rates are affected by response rates. This is particularly prominent for vaccination rates for second doses in staff employed in other settings and first boosters and flu for all staff and resident groups. This is because these groups have a lower response rate and as a result, second dose vaccination rates may be underestimated.
For data relating to 9 November 2021 and before, response rates may have been underestimated, particularly for first boosters and flu vaccination. This is because the default value in the underlying data is set to zero, so any zero values submitted will appear to be non-responses. From 9 November 2021 onwards, care providers are required to select that they have reviewed their responses to confirm the data submitted is accurate, therefore increasing the accuracy of response rates.
Among care home staff, there is a substantial difference in reported vaccination rates for COVID-19 and flu vaccinations between staff directly employed by care homes and staff employed by agencies operating within care homes. This could be due to, for example but not exclusively, different uptake rates, vaccination status not being known to the care provider, or the nature of employment and information available to the care homes.
For data relating to 31 August 2021 onwards, a small number of social care staff who had their vaccination outside of the UK are excluded from the numbers vaccinated.
For more information, see the background quality and methodology note.
COVID-19 vaccinations
The NHS started administering vaccinations for COVID-19 in England on 8 December 2020. Social care staff and residents of care homes were prioritised for the vaccine according to the Joint Committee on Vaccination and Immunisation (JCVI) recommendation. For more information see Priority groups for coronavirus (COVID-19) vaccination: advice from the JCVI.
From 11 November 2021, all people working or volunteering in care homes were required to be fully vaccinated against COVID-19, unless exempt. As Omicron, which is intrinsically less severe, replaced Delta as the dominant variant, DHSC consulted on revoking this requirement. Over 90,000 responses were received and 90% supported the removal of vaccination as a condition of deployment. Following the publication of this consultation, the Secretary of State for Health and Social Care announced in a written ministerial statement the revocation of the legislation to take effect from 15 March 2022.
Although it is no longer a legal requirement for staff in adult social care to be vaccinated to be deployed, adult social care staff and residents are still encouraged to get their COVID-19 booster vaccination after receiving their second dose.
More details can be found at COVID-19 vaccination: a guide to booster vaccination.
On 21 February 2022, the JCVI issued advice on an additional COVID-19 spring booster dose, around 6 months after the last vaccine dose, for:
- adults aged 75 years and over
- residents in a care home for older adults
- individuals aged 12 years and over who are immunosuppressed, as defined in the COVID 19 healthcare guidance Green Book
The spring booster programme began on Monday 21 March 2022. Invitations are being sent to eligible people and visits offered to older adult care homes by local NHS teams.
Since 4 April 2022, providers are asked to record spring booster vaccinations in the Capacity Tracker. Data on spring boosters will be published in future reports. This report only presents data on first booster doses, which were introduced in autumn 2021.
COVID-19 vaccinations in older adult care homes
99.4% of older adult care homes have provided data on the number of staff and residents who received a first COVID-19 booster dose, as of week ending 22 March 2022. This means the first and second dose rates, and the number of staff and residents receiving a first booster dose may be underestimated compared with the true value.
For full response rates, see the accompanying ‘COVID-19 vaccination response rates, April 2022: data tables’ on the ASC monthly statistics page.
Residents of older adult care homes
As of week ending 22 March 2022, in older adult care homes:
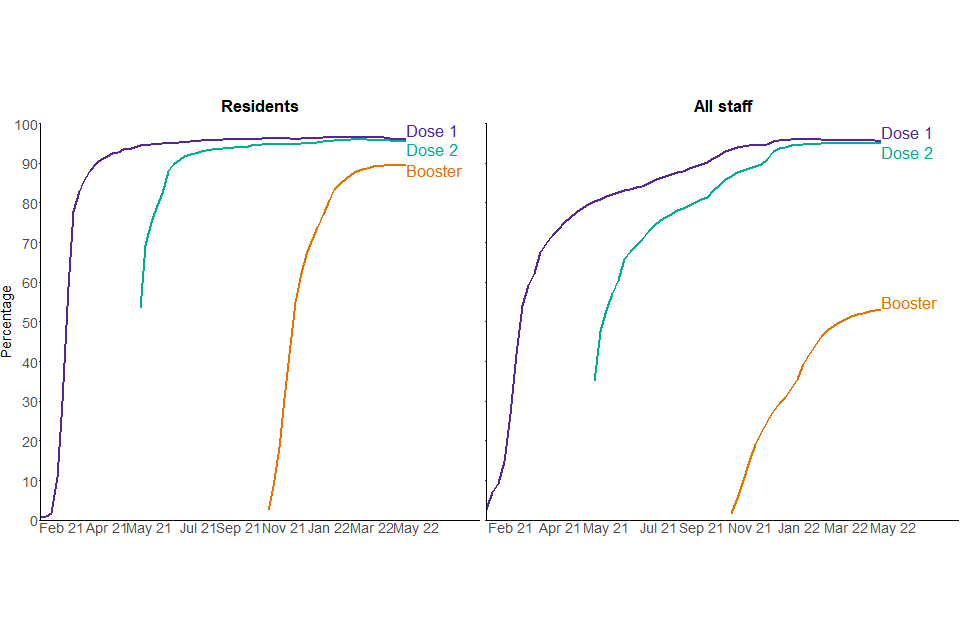
- 95.4% of residents have been reported to have received 2 doses
- 89.7% of residents have been reported to have received their first booster dose
First booster vaccination rates increased steeply between mid-October 2021 and January 2022 and have stabilised since the end of January 2022.
There is some variation in reported first booster doses administered regionally, with the East of England region having the largest uptake with 91.6% of residents vaccinated, compared with the lowest uptake in London with 87.6%.
Staff of older adult care homes
As of week ending 22 March 2022, in older adult care homes:
- 95.0% of staff have been reported to have received 2 doses
- 53.1% of staff have been reported to have received their first booster dose
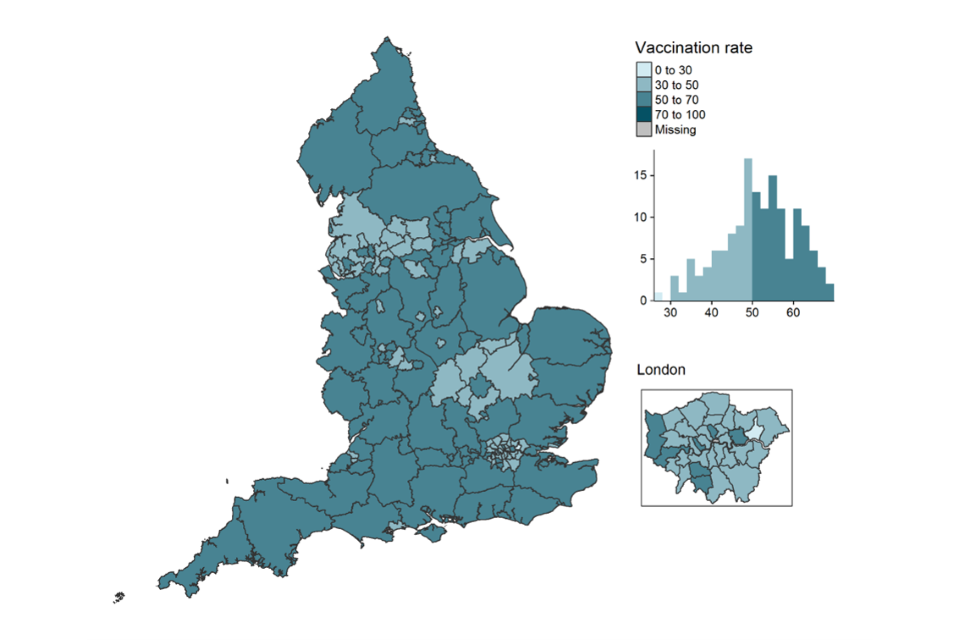
Reported booster vaccination rates continued to increase across all regions throughout February and March, although not as steeply as in January. There is large regional variation in rates, with the North East having the highest uptake with 59.1%, and London having the lowest at 42.7%.
Vaccination as a condition of deployment (VCOD) required individuals to be fully vaccinated against COVID-19 with a primary course (2 doses). Boosters were not required in order to comply with the regulations, but all staff were and continue to be encouraged to take up their offer of a booster dose.
Figure 1: percentage of staff and residents of older adult care homes who have received the first, second and booster doses of the COVID-19 vaccination, cumulative rate, 15 December 2020 to 22 March 2022, England
Reported booster vaccination rates are starting to stabilise for residents and continue to increase for staff in older adult care homes.
Source: Capacity Tracker
Figure 2: percentage of older adult care home staff who have received their booster dose of the COVID-19 vaccination by local authority, as of 22 March 2022, England
The majority of local authorities have a reported booster vaccination rate of between 50% and 70% for staff in older adult care homes.
Source: Capacity Tracker
Data from figures 1 and 2 can be found in tables 1 and 2 of the accompanying ‘COVID-19 vaccination statistics, April 2022: data tables’ on the ASC monthly statistics page, in addition to data by region and local authority.
Notes:
- data is reported by care providers
- data is based on date of reporting rather than date of vaccination
COVID-19 vaccinations in staff working in domiciliary care, younger adult care homes and other settings
Data for staff working in other settings (including non-registered providers and local authority employed) after August 2021 does not include Surrey as this data is no longer collected by the local authority.
The following proportions of social care staff have been reported to have received their COVID-19 vaccination doses:
In younger adult care homes as of week ending 22 March 2022:
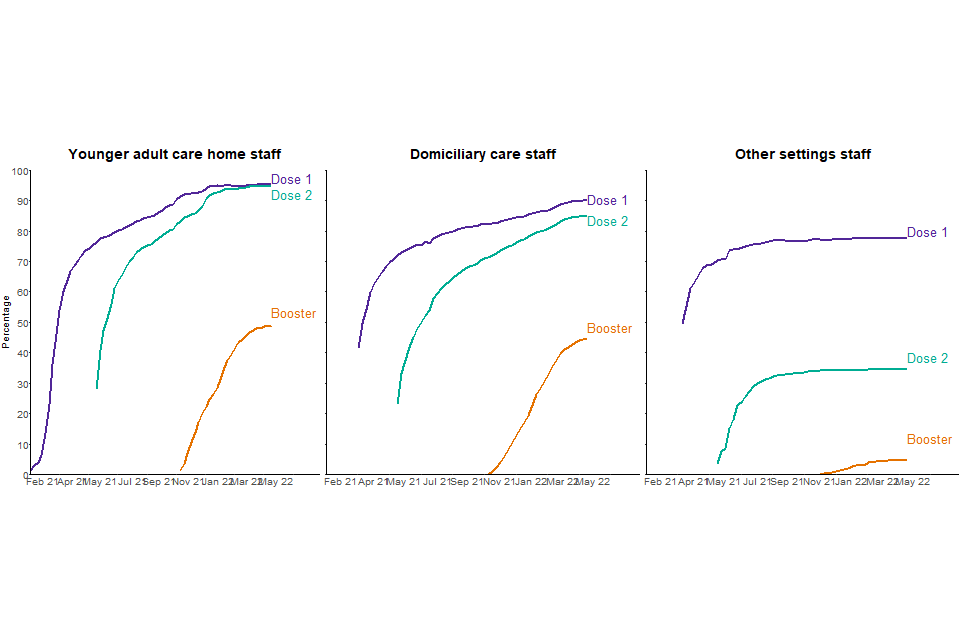
- 94.7% of staff have been reported to have received 2 doses
- 49.0% of staff have been reported to have received their first booster dose
For domiciliary care staff as of week ending 22 March 2022:
- 85.1% of staff have been reported to have received 2 doses
- 44.8% of staff have been reported to have received their first booster dose
Among staff working in other settings as of week ending 22 March 2022:
- 34.7% of staff have been reported to have received 2 doses
- 4.8% of staff have been reported to have received their first booster dose
As data is self-reported by care providers, COVID-19 vaccination rates are affected by response rates. An overview of response rates is in the table below.
Table 1: percentage of providers that have provided data on the number of staff vaccinated at least once as of 22 March 2022
| Dose | Younger adult care home providers on behalf of their staff | Domiciliary care providers on behalf of their staff | Local authorities on behalf of staff working in other settings |
|---|---|---|---|
| Provided data on second dose | 99.1 | 94.5 | 63.8 |
| Provided data on first booster dose | 98.9 | 92.7 | 26.3 |
Notes:
- due to these response rates, the number of staff and residents, particularly for boosters, will be underestimated compared with the true value. For full response rates see the accompanying ‘COVID-19 vaccination response rates, April 2022: data tables’ on the ASC monthly statistics page
- there is regional variation for all staff groups – see table 2 for further details
Figure 3: percentage of staff in younger adult care homes, domiciliary care settings and other care settings who have received the first, second and booster dose of the COVID-19 vaccination, cumulative rate, 15 December 2020 to 22 March 2022, England
Reported booster vaccination rates for staff are starting to stabilise across all settings.
Source: Capacity Tracker
This data can be found in tables 6, 9 and 10 of the accompanying ‘COVID-19 vaccination statistics, April 2022: data tables’ on the ASC monthly statistics page, in addition to data by region and local authority.
Table 2: percentage of younger adult care home and domiciliary care staff reported to have received a first booster dose of the COVID-19 vaccine, up to 22 March 2022 by region, England
| Region | Younger adult care home staff | Domiciliary care staff | Staff working in other settings |
|---|---|---|---|
| East Midlands | 50.6 | 45.6 | 12.1 |
| East of England | 49.8 | 48.9 | 0.8 |
| London | 46.4 | 28.5 | 0.6 |
| North East | 63.2 | 52.9 | 9.0 |
| North West | 46.7 | 43.0 | 5.4 |
| South East | 46.8 | 49.2 | 3.4 |
| South West | 49.3 | 53.3 | 1.8 |
| West Midlands | 49.9 | 43.5 | 3.9 |
| Yorkshire and the Humber | 47.5 | 48.8 | 13.3 |
COVID-19 vaccinations for residents of younger adult care homes
Residents of younger adult care homes were not part of a single priority group for the COVID-19 vaccine. However, the conditions for which they reside in care homes are likely to make them more vulnerable to COVID-19 and they were therefore likely to be part of priority groups 3 to 9. First booster dose roll out, however, is dependent on the recommended time gap between second dose and booster dose rather than specific priority groups.
As of week ending 22 March 2022, in younger adult care homes:
- 92.3% of residents have been reported to have received 2 doses
- 81.0% of residents have been reported to have received their first booster dose
Flu vaccination in adult social care settings
The national influenza (flu) immunisation programme aims to provide direct protection to those who are at higher risk of influenza associated morbidity and mortality. Groups eligible for NHS influenza vaccination are based on the advice of the JCVI. More details can be found in the National flu immunisation programme 2021 to 2022 letter.
This report covers cumulative flu vaccination rates for the 2021 to 2022 season in the below adult social care groups:
- residents in older adult care homes
- staff directly employed by older adult care homes
- agency staff working in older adult care homes
- staff directly employed by younger adult care homes
- agency staff working in younger adult care homes
- domiciliary care staff registered to independent CQC providers
- social care staff working in other settings (including non-registered providers and local authority employed)
- residents of younger adult care homes
Guidance on flu vaccination for social care workers was updated on 9 September 2021. For more information, see the background quality and methodology note.
Data is self-reported by care providers and local authorities, who may submit their resident and staff numbers but not the number receiving the flu vaccination, resulting in a lower reported percentage vaccinated. An overview of response rates for the numbers vaccinated is in the table below.
As the seasonal flu vaccination campaign has come to an end, the collection of flu vaccination data from providers will be temporarily suspended until next winter. As a result, the timeseries for flu vaccination will end on 29 March 2022 and the data tables will feature in the May 2022 publication, but not in subsequent publications, until data is collected again.
Table 3: percentage of providers that have provided data on the number of staff or residents who received a flu vaccination for the 2021 to 2022 season, as of 22 March 2022
| Older adult care home providers on behalf of their staff | Younger adult care home providers on behalf of their staff | Domiciliary care providers on behalf of their staff | Local authorities on behalf of staff working in other settings | |
|---|---|---|---|---|
| Percentage who provided flu data at least once | 99.4 | 98.9 | 92.6 | 19.7 |
For full response rates see the accompanying ‘COVID-19 vaccination response rates, April 2022: data tables’ on the ASC monthly statistics page.
Older adult care homes
As of week ending 22 March 2022, the proportions of those who had received a flu vaccination in older adult care homes were:
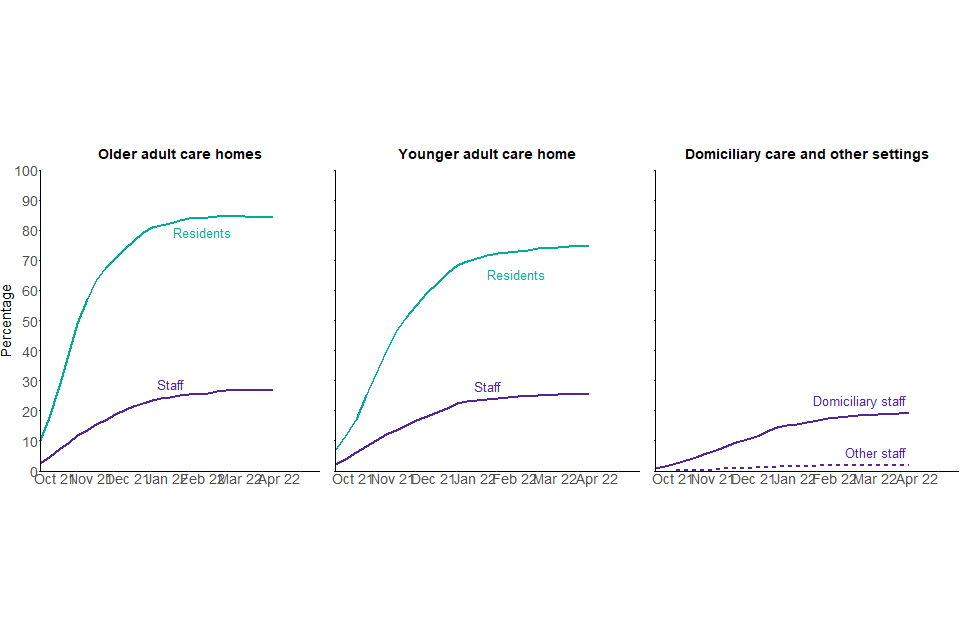
- 84.5% of residents
- 26.8% of all staff
Younger adult care homes
As of 22 March 2022, the proportions of those who had received a flu vaccination in younger adult care homes were:
- 74.6% of residents
- 25.4% of all staff
Domiciliary care staff and staff working in other settings
As of 22 March 2022, the proportions of staff who work in domiciliary care and other settings who had received a flu vaccination were:
- 19.1% of domiciliary care staff
- 1.9% of staff working in other settings
Figure 4: percentage of social care staff and residents who have received the flu vaccination, cumulative rate, 28 September 2021 to 22 March 2022, England
The reported flu vaccination rates are highest among older adult care home residents.
Source: Capacity Tracker
This data can be found in tables 1, 2, 5, 6, 9 and 10 of the accompanying ‘Flu vaccination statistics, April 2022: data tables’ on the ASC monthly statistics page, in addition to data by region and local authority.
There is regional variation in reported flu vaccination uptake among each of the adult social care groups. The variation is most pronounced among staff and residents of younger adult care homes. Regional variation among all groups is summarised in table 4.
Table 4: percentage of each social care group reported to have received a flu vaccination up to 22 March 2022 by region, England
| Region | Older adult care home residents | Older adult care home staff | Younger adult care home residents | Younger adult care home staff | Domiciliary care staff | Other settings staff |
|---|---|---|---|---|---|---|
| East Midlands | 84.3 | 27.3 | 68.4 | 21.4 | 19.0 | 5.0 |
| East of England | 84.8 | 23.6 | 75.2 | 25.2 | 19.6 | 0.3 |
| London | 83.6 | 19.9 | 77.6 | 24.9 | 14.0 | 0.2 |
| North East | 84.7 | 28.2 | 77.5 | 35.7 | 24.2 | 4.0 |
| North West | 83.9 | 27.3 | 73.0 | 28.3 | 18.3 | 3.2 |
| South East | 84.9 | 26.0 | 75.9 | 24.5 | 21.1 | 1.6 |
| South West | 86.0 | 30.0 | 71.8 | 25.1 | 21.7 | 0.5 |
| West Midlands | 83.3 | 29.5 | 76.3 | 25.9 | 18.6 | 2.3 |
| Yorkshire and the Humber | 84.6 | 28.5 | 76.2 | 24.5 | 20.0 | 2.9 |
Infection prevention control measures
How the data can be used
This data can be used for:
- estimating the number and proportion of care homes that indicate they:
- are accommodating COVID-safe visits within the care homes in line with government guidance
- are paying full wages to the majority of their self-isolating staff
- restrict staff movement across settings
- monitoring trends over time
- comparisons across local authorities and regions in England
This data cannot be used for:
- estimating the number of visitors in care homes and their infection or vaccination status
- comparing with other countries of the UK
- linking staff movement across settings to positivity rates
Until 31 March 2022, the Adult Social Care Infection Control and Testing Fund provided funding from local authorities to ensure that infection prevention control (IPC) measures were in place to curb the spread of COVID-19. This publication provides data on how providers were implementing the following measures:
- limitation of staff movement across different social care settings
- accommodating COVID-19 safe visitation in care homes in line with government guidance
- payment of full wages when care home staff were isolating due to COVID-19
On 31 March 2022, the Adult Social Care Infection Control Fund reached the end of its extension period. The end of the fund means that, among other implications, the government will no longer provide funding for COVID- positive social care staff to stay away from work and staff movement restrictions will be lifted, allowing pressure on workforce to be alleviated.
As a result, among other data collected about infection prevention control measures, the data on staff pay and staff movement will cease to be collected from 4 April 2022 and therefore the last data point in the timeseries for these 2 metrics will be the 29 March 2022. The end of the timeseries will be presented in the May 2022 publication data tables but these tables will no longer feature in subsequent publications.
The April publication includes data up to 22 March 2022, before the collection ceased on 4 April 2022. The question on COVID-safe visitation in care homes will remain but might be modified in upcoming weeks, as part of the data collection tool review.
More details on the data collection, coverage and quality of this data can be found in the ‘About this data’ section below.
Accommodating COVID-safe visitation in care homes
There are currently no restrictions on visiting in care homes under normal circumstances. However, during periods of outbreak or when a resident is COVID-positive, visits inside a care home should be limited to one named visitor only. From 4 April 2022, visitors will no longer be required to test before the visit, unless they are providing personal care. However, this change does not affect the data in this publication as the last data point included is 22 March 2022.
The guidance on allowing care home residents to have visitors has changed since December 2020 and is summarised in the table below.
Table 5: changes in visiting guidance since December 2020
| Date | Guidance |
|---|---|
| From 4 April 2022 | No restrictions on visitation in care homes. Every care home resident should have one visitor who can visit in all circumstances (including during periods of isolation and outbreak) Visitors are no longer required to test before a visit, unless providing personal care. Visitors providing personal care will not need to test more than twice a week. |
| From 31 January 2022 to 3 April 2022 | No limits on the number of named visitors, with testing and guidance to support safe visiting in place |
| From 15 December 2021 to 30 January 2022 | Residents are permitted to have 3 named visitors for regular visits with testing in place |
| 19 July 2021 to 14 December 2021 | No limits on the number of named visitors, with testing and guidance to support safe visiting in place |
| 17 May 2021 to 18 July 2021 | Residents are permitted to have 5 named visitors for regular visits with testing in place |
| 12 April 2021 to 16 May 2021 | Residents are permitted to have 2 named visitors for regular visits with testing in place |
| 8 March 2021 to 11 April 2021 | Residents are permitted to have 1 named visitor for indoor visits with testing in place |
| 6 January 2021 to 7 March 2021 | No indoor visits permitted due to the national lockdown |
| 1 December 2020 to 5 January 2021 | Indoor visits permitted with testing in place (from 19 December 2020 – no indoor visits permitted in tier 4 areas) |
Note: timelines for guidance are accurate as of 14 April 2022.
More information on the current visiting guidance can be found in the COVID-19 supplement, which accompanies the Infection prevention and control in adult social care settings. DHSC have also published a summary of changes to COVID-19 guidance for adult social care providers which provides details on the recent changes to the visiting guidance.
This report covers care homes that were accommodating visitation in line with the previous guidance, before 4 April 2022. This could cover visitation in care homes premises, either indoors or outdoors, or also visits off premises, either for the day or overnight. The new guidance took effect on 4 April 2022, which was after the latest data point included in this report.
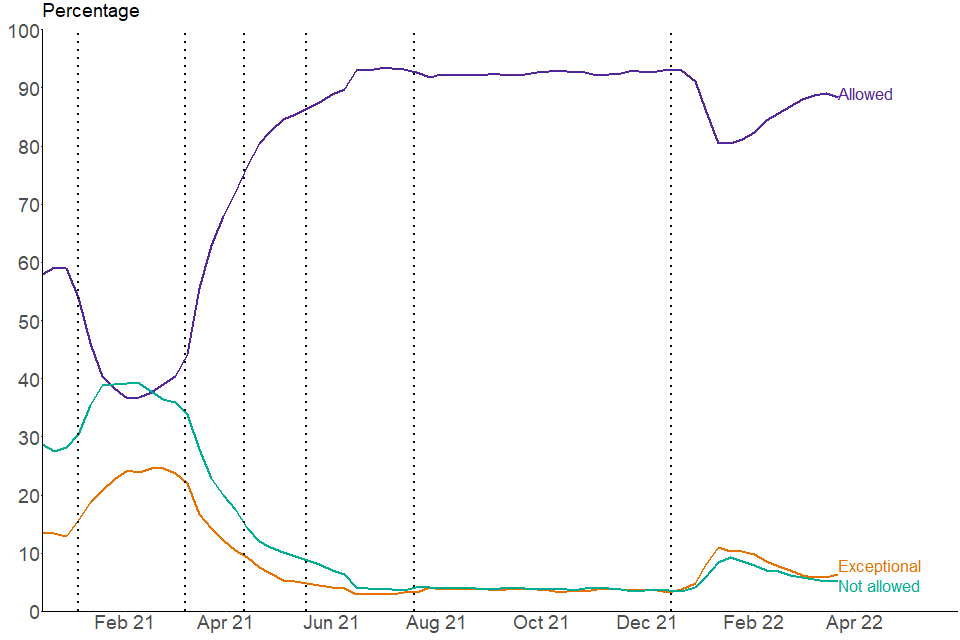
In the week ending 22 March 2022:
- 88.3% of care homes in England were able to accommodate residents receiving visitors within care homes in all circumstances. This proportion had gradually increased throughout February 2022, following the removal of restriction on the number of visitors per resident, but it decreased slightly in the week ending 22 March 2022
- a further 6.3% were able to accommodate visits in exceptional circumstances, which is a slight increase compared to the previous week. This figure had progressively declined since mid-January 2022. Exceptional circumstances are individually defined by each care home but are generally thought to be considered when residents are palliative
- there has been substantially less variation across regions in March 2022 compared to mid-January 2022. 89.9% of care homes accommodated visiting in the South East compared to 85.5% in the East Midlands in the week ending 22 March 2022
Figure 5: percentage of care homes accommodating or limiting visits for residents, 15 December 2020 to 22 March 2022, England
The proportion of care homes accommodating visiting for residents has decreased slightly after a period of increase between mid-January 2022 and mid-March 2022.
Source: Capacity Tracker
This data can be found in table 1 of the accompanying ‘Infection control, PPE and workforce statistics, April 2022: data tables’ on the ASC monthly statistics page, in addition to data by region and local authority.
Payment of care home directly employed staff while self-isolating due to COVID-19
Up to 31 March 2022, the infection control funds could be used to ensure staff who were self-isolating along with government guidance were paid their full wages. This included:
-
staff isolating while waiting for a test
-
isolating after having tested positive or after a positive test in their household
-
staff required to quarantine prior to receiving certain NHS procedures
Employers who do not pay their staff their full wages while self-isolating must pay their staff at least Statutory Sick Pay (SSP) when the employee meets the following criteria:
- is classed as an employee and has done some work for their employer
- earns an average of at least £120 per week
- has been ill or is self-isolating for at least 4 days in a row (including non-working days)
Care home staff who do not meet the criteria may not be eligible and as a result not paid to self-isolate. For more information, see guidance on Statutory Sick Pay.
After 31 March 2022, the government will no longer provide funding for COVID-positive social care staff to stay away from work. The data collection on whether care homes pay their staff full wages when self-isolating ceased on 4 April 2022. This means that the last data point in the timeseries for staff pay will be the 29 March 2022. The end of the timeseries will be presented in the May 2022 publication data tables but the table will no longer feature in subsequent publications.
This publication includes data up to 22 March 2022, before the collection ceased on 4 April 2022.
The figures in this report refer to care homes which had staff required to self-isolate in the relevant week. This means care homes who had no staff needing to self-isolate will be excluded from the rates for the relevant week. There may be several care providers who may use a combination of payment options for staff wages. In these situations, providers should report the option they use for the majority of their staff.
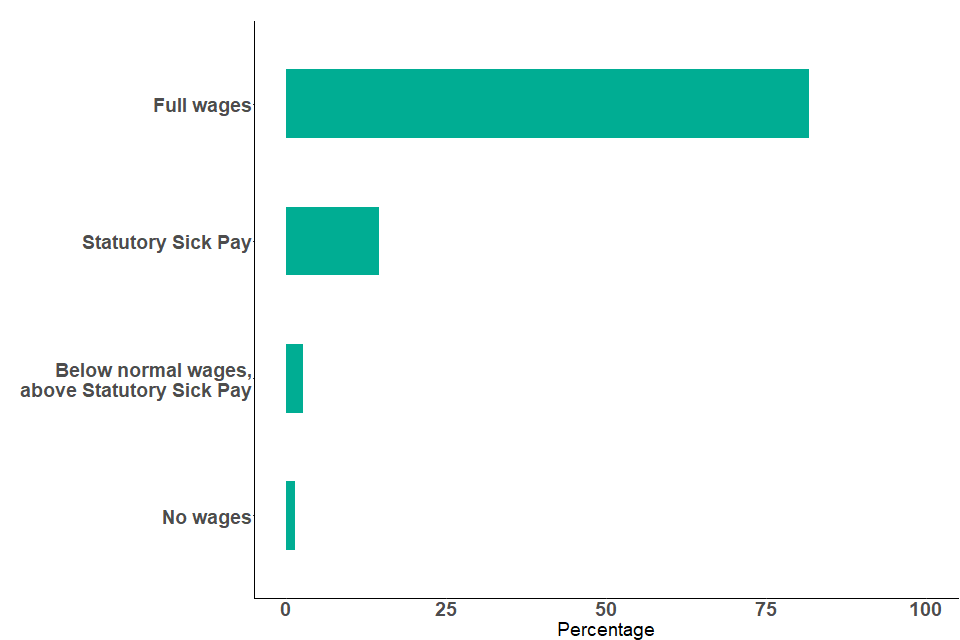
In the week ending 22 March 2022:
- 81.6% of care homes who had directly employed staff needing to self-isolate paid staff their full wages. This proportion has remained consistent since mid-December 2020
- there is substantial regional variation with 88.6% of providers in the North East paying their staff full wages compared with 76.4% in the East Midlands
Figure 6: percentage of care homes with staff self-isolating by wages paid, week ending 22 March 2022, England
More than 8 in 10 care homes reported paying their staff full wages when self-isolating.
Source: Capacity Tracker
This data can be found in table 2 of the accompanying ‘Infection control, PPE and workforce statistics, April 2022: data tables’ on the ASC monthly statistics page, in addition to data by region and local authority.
Limiting staff movement between care settings
Up to 31 March 2022, infection control funding could be used to reduce the need for staff movement between health or social care settings to limit the spread of infection. For example, it could be used to recruit additional staff to enable staff to only work across one care home.
As part of the Living with COVID policy changes, the new COVID-19 infection prevention and control resource for adult social care guidance, which applies from 4 April 2022, includes the relaxation of staff movement restrictions between health or social care settings which will allow pressure on workforce to be alleviated.
The data collection on care homes staff movement across settings ceased on 4 April 2022. This means that the last data point in the timeseries for staff movement will be the 29 March 2022. The end of the timeseries will be presented in the May 2022 publication data tables but the table will no longer feature in subsequent publications.
This publication includes data up to 22 March 2022, before the collection ceased on 4 April 2022.
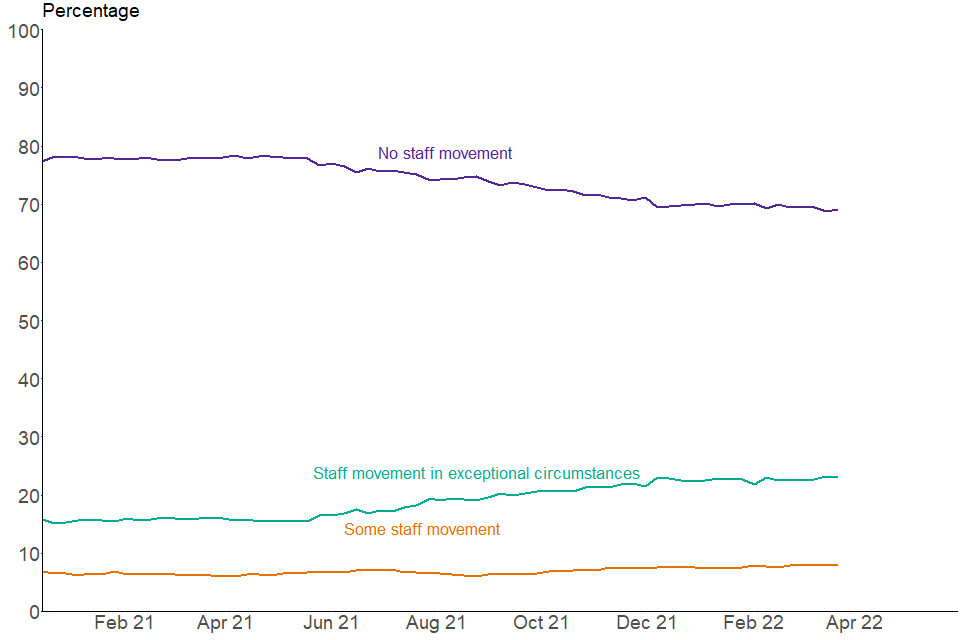
In the week ending 22 March 2022:
- 69.0% of care homes had no staff members working in another health or social care setting. This figure has remained broadly consistent since December 2021, following a period of gradual decline from April 2021
- 8.0% of care homes had some staff additionally working in another health or social care setting
- a further 23.0% of care homes had some staff additionally working in another health or social care setting due to exceptional circumstances. This number has remained broadly consistent since December 2021, following a period of gradual increase between May 2021 and November 2021. Exceptional circumstances are defined as the care home having exhausted all other reasonable steps to ensure there are sufficient staffing levels
- there is substantial regional variation with 78.7% of providers in the North East having no staff working in another health or social care setting in the week ending 22 March 2022, in comparison with 63.5% in the South East
Figure 7: percentage of care homes by staff working across additional health or social care settings, 15 December 2020 to 22 March 2022, England
The proportion of care homes reporting having no staff working in another setting has gradually decreased since May 2021 but has remained broadly similar since December 2021.
Source: Capacity Tracker
This data can be found in table 3 of the accompanying ‘Infection control, PPE and workforce statistics, April 2022: data tables’ on the ASC monthly statistics page, in addition to data by region and local authority.
Care home staffing levels
How the data can be used
This data can be used for:
- estimating the number and proportion of care homes that indicate they are operating within their agreed staffing ratios
- monitoring trends over time
- comparisons across local authorities and regions in England
This data cannot be used for:
- identifying the reasons for care home staff shortages and absences
- linking staff shortages and the number of positive cases among care home staff
- comparing with other countries of the UK
In order to measure the workforce pressures on providers during the pandemic, each provider is asked to assess their workforce pressures based on their agreed staffing ratios. More details on how staffing ratios are agreed can be found within the CQC guidance on staffing.
An additional adult social care workforce report providing more information on the pressures faced by the adult social care workforce, received through an ad hoc survey, was published as part of this collection on 17 December 2021. The survey covers more detailed insight into current workforce pressures faced compared to 6 months previously. This includes issues relating to recruitment, retention, staff morale and use of agency staff.
This survey complements the regular collection by providing the opportunity to have a deeper exploration of workforce issues which is possible in an ad hoc survey but would be too burdensome for the regular collection.
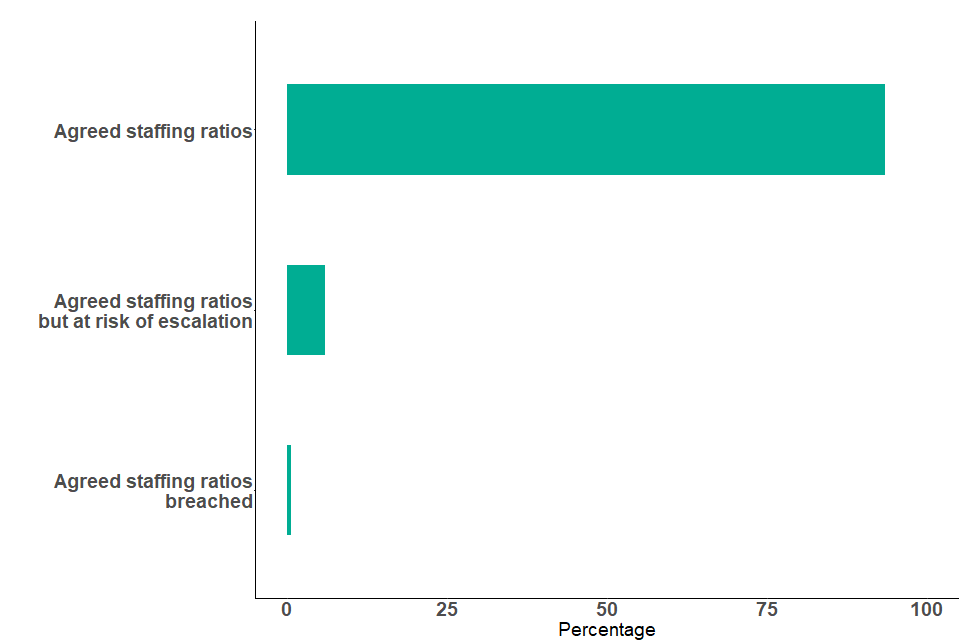
In the week ending 22 March 2022:
- 0.6% of providers flagged that their agreed staffing ratios had been breached. This has been stable throughout February and March, following a period of decrease since to the week ending 4 January 2022 when it reached a peak of 0.8%. The proportion of providers flagging a breach of their staffing ratios has consistently remained lower than 1%
- 5.9% flagged that they were operating within the agreed staffing ratios but there is a significant risk of escalation in the coming days. This proportion has also been stable throughout February and March 2022, after a period of decrease since a peak of 6.7% in the week ending 11 January 2022
- 93.5% were operating within their agreed staffing ratios, which is similar to proportions seen throughout February and March 2022. This proportion had reached its lowest point of 92.5% in the week ending 11 January 2022
If a care home’s staffing ratio has been breached, then business continuity measures may be put in place.
Figure 8: percentage of care homes operating within agreed staffing ratios, week ending 22 March 2022, England
More than 9 in 10 care homes report operating within their agreed staffing ratios.
Source: Capacity Tracker
This data can be found in table 4 of the accompanying ‘Infection control, PPE and workforce statistics, April 2022: data tables’ on the ASC monthly statistics page, in addition to data by region and local authority.
Staff absence rates
How the data can be used
This data can be used for:
- estimating the number and percentage of staff absent because of COVID-19 related reasons
- monitoring trends over time
- comparisons across local authorities and regions in England
This data cannot be used:
- as a sole indicator of all workforce pressures faced by the social care sector, since they only cover COVID-19 related absence
- to directly compare absence rates related to COVID-19 between domiciliary care and care home staff
- for comparing with other countries of the UK
- for linking COVID-19 related absence rates with test positivity rates
Absence rates related to COVID-19 are calculated using the reported number of staff employed and the reported number of staff out of work that day because of COVID-19 related reasons. Both the number of total staff employed, and the number of staff absent might be affected by provider response rates as only numbers reported by providers in the last 7 days are included in the total counts.
Absence data started to be reported by care providers in Capacity Tracker from December 2020. However, low response rates in the first few months of collection mean that the workforce data is incomplete, which affects the accuracy of the absence data during that period.
Providers who are the least likely to respond are likely to be those experiencing the most pressures on delivery due to high levels of staff absence. For this reason, data from December 2020 to the start of February 2021 for care homes, and from December 2020 to the start of March 2021 for domiciliary care providers, are not presented in this publication.
COVID-19 related absences cannot be directly linked to staff test positivity rates. This is because absences related to COVID-19 can cover a wide range of reasons, including but not restricted to staff:
- testing positive to COVID-19
- self-isolating
- caring for someone who has tested positive to COVID-19
- suffering from illness related to COVID-19
For more information, see the background quality and methodology note.
Absence rate statistics presented in this section were added for the first time in February 2022, following growing general interest in workforce pressures from various sources. They complement the statistics on staffing ratios presented in the previous section.
The staffing ratios statistics have not presented substantial variation over the past year, with the exception of the last few months. In the adult social care workforce survey published in December 2021, however, care providers have reported facing pressures on staffing levels. This suggests that the staffing ratio statistics may not accurately illustrate these workforce pressures.
COVID-19 related absence rate statistics alone are still not sufficient to give a full picture of workforce pressures faced by the sector, however they may provide more insight on some of the challenges. Additional statistics, such as general absences, retention or recruitment could provide a more complete picture.
In care homes
Data on care home staff absences related to COVID-19 is available from 9 February 2021.
In the week ending 22 March 2022, 1.7% of care home staff were absent because of COVID-19 related reasons. Absence rates started to increase again since the start of March 2022, following a period of substantial decrease from 2.9% in the week ending 11 January 2022 to 1.1% in the week ending 1 March 2022.
Variation across regions has increased throughout March 2022. In the week ending 22 March, 2.5% of staff were absent because of COVID-19 related reasons in the South West, compared with 0.7% in London. In the week ending 1 March 2022, there was less regional variation, with 1.3% of staff absent because of COVID-19 related reasons in the South West, compared with 0.7% in London.
The data suggests that the size of the care home workforce has been gradually declining since April 2021. This may however be partly driven by a change in response rates over the period. A reduction in the care home workforce size is another indication of pressures faced by the sector to deliver care.
Data on workforce counts and response rates can be found in tables 5 and 10, respectively, of the accompanying ‘Infection control, PPE and workforce statistics, April 2022: data tables’ on the ASC monthly statistics page.
More information about other sources of adult social care workforce data can be found in ‘Other sources of adult social care COVID-19 data’ (in the ‘About this data’ section below).
In domiciliary care
Data on domiciliary care staff COVID-19 related absences is available from 2 March 2021. Absence rates in domiciliary care settings are not directly comparable with those in residential care homes.
Domiciliary staff COVID-19 absence rates started to increase again from early March 2022, reaching 2.5% in the week ending 22 March 2022, following a period of gradual decline between early January 2022 and the end of February 2022. This figure still remains substantially lower than the peak of 4.8% seen in week ending 4 January 2022, which was the highest level seen since the start of the timeseries in March 2021.
There has been some variation across regions, especially during periods of high absences. Throughout March 2022 variation across regions has started to increase again slightly. In the week ending 22 March 2022, 3.8% of domiciliary care staff were absent due to COVID-19 related reasons in London, compared with 1.7% in the West Midlands. London has consistently shown substantially higher COVID-19 related absence rates compared with other regions and peaked at 7.0% in the week ending 4 January 2022.
Similarly to care homes, the data suggests that the domiciliary care workforce size has been gradually declining during the last year. This may however be partly driven by a change in response rates over the period.
Data on workforce counts and response rates can be found in tables 6 and 12 of the accompanying ‘Infection control, PPE and workforce statistics, April 2022: data tables’ on the ASC monthly statistics page.
More information about other sources of adult social care workforce data can be found in ‘Other sources of adult social care COVID-19 data’ (in the ‘About this data’ section below).
Figure 9: percentage of staff absent due to COVID-19 related reasons, up to week ending 22 March 2022, England
Absence due to COVID-19 related reasons has recently started to increase again after a period of substantial decrease in January and February 2022, in both care homes and domiciliary care settings.
Source: Capacity Tracker
Note: the proportion of staff absent due to COVID-19 reasons is not comparable across care settings.
This data can be found in tables 5 and 6 of the accompanying ‘Infection control, PPE and workforce statistics, April 2022: data tables’ on the ASC monthly statistics page, in addition to data by region and local authority.
PPE availability in care settings
How the data can be used
This data can be used for:
-
estimating the number and proportion of care homes and domiciliary care providers who are experiencing PPE shortages in the next 48 hours, and comparing across local authorities and regions in England
-
monitoring trends over time
This data cannot be used for:
- predicting PPE shortages in the coming weeks
- comparing with other countries of the UK
- linking PPE shortage to positivity rates
All care homes and domiciliary care providers are responsible for ensuring safe systems of work and have duties concerning the provision and use of PPE in the workplace.
The COVID-19 supplement, which accompanies the Infection prevention and control in adult social care settings, sets out the PPE recommendations for adult social care services in England. The government will continue to provide free PPE to the adult social care sector until the end of March 2023, or until guidance is withdrawn or substantially amended.
This publication covers the availability of the following 5 items of PPE:
-
aprons
-
eye protection
-
gloves
-
hand sanitiser
-
face masks
In care homes
In the week ending 22 March 2022, 0.2% of care homes in England had either no supply or were expecting to experience a shortage in the next 48 hours of at least one item of PPE. This gradually decreased from late September 2020 when 1.1% of care homes were experiencing a shortage and has remained relatively unchanged since March 2021.
In domiciliary care
In the week ending 22 March 2022, 1.2% of domiciliary care providers in England, excluding London, reported having no supply or were expecting to experience a shortage in the next 48 hours of at least one item of PPE. This proportion has gradually decreased since July 2021.
This figure does not include figures from local authorities in the London region and therefore is not a complete picture of the national situation. This is due to incomparable data across London and other regions. For a number of providers in London, responses are collected via the London Association of Directors of Adult Social Services (ADASS) before being uploaded to Capacity Tracker in bulk. Due to differences in the interpretation of the wording of the questions asked by ADASS about specific items of PPE stock, the data collected via this channel is not comparable to the data collected directly via Capacity Tracker. Work is currently being done to harmonise the data across regions.
Local figures for the London region and London local authorities have therefore been suppressed from the data tables. Data for other regions and local authorities outside of London can be found in table 8 of the accompanying ‘Infection control, PPE and workforce statistics, April 2022: data tables’ on the ASC monthly statistics page.
This publication only presents figures from the week ending 6 July 2021, when the wording of the question in the collection tool was changed, which resulted in the incomparability of the data between London and other regions. Data prior to July 2021 can be found in previous editions of the publication. The last edition to present data prior to July 2021 is the Adult social care in England, monthly statistics: March 2022.
COVID-19 testing in adult care homes
How the data can be used
This data can be used for:
- estimating the number of PCR and rapid lateral flow tests taken and positive results returned in care homes, and comparing across local authorities and regions in England
- estimating trends in prevalence and positivity rates for COVID-19 in care homes based on trends in positive tests
This data cannot be used for:
- calculating positivity rates for COVID-19 in care homes due to routine and repeat testing of individuals
- linking positivity rates in care homes to lower vaccination rates in care homes
- estimating the number of people tested and positive cases in care homes as people can take more than one test
For more information on:
- the rollout of the testing programme in care homes, see the ‘About this data’ section below
- testing kits used, see the ‘Terminology’ section below
Number of tests conducted and positive tests returned in adult care homes
The number of positive rapid lateral flow tests returned during March 2022 increased substantially for both residents and staff, reaching similar levels to those recorded during the previous peak in January 2022. This steep increase follows a previous period of rapid decline seen throughout February 2022. The number of positive PCR tests also increased this month, for both residents and staff.
Overall, the number of tests conducted increased slightly when compared to the previous month.
Recent changes to testing guidance in care homes have affected the number of PCR and rapid lateral flow tests conducted among staff and residents. An overview of the changes to the testing guidance in care homes since June 2022 is presented in table 6 below.
From 4 April 2022 the requirement of care home staff to complete pre-shift rapid lateral flow tests is replaced by twice weekly rapid lateral flow tests, and asymptomatic testing for residents is removed. Additionally, symptomatic testing is now done with rapid lateral flow tests instead of PCR tests. DHSC published a summary of changes to testing and other IPC measures. These changes do not impact the data published this month as the time series only includes data up to the week ending 22 March 2022. However, this change in guidance will impact data in future publications.
Table 6: changes in testing guidance in care homes since June 2020
| Date | Chnages in guidance |
|---|---|
| From 4 April 2022 | Staff – 2 rapid lateral flow tests per week If symptomatic 2 rapid lateral flow tests taken 48 hours apart Residents – no testing If symptomatic 2 rapid lateral flow tests taken 48 hours apart Visitors – no testing unless providing personal care |
| From 16 February 2022 to 3 April 2022 | Staff – pre shift rapid lateral flow tests |
| From 11 January 2022 | Staff and residents – removal of confirmatory PCR test following a positive rapid lateral flow test |
| 15 December 2021 to 15 February 2022 | Staff – weekly PCR and 3 rapid lateral flow tests per week |
| 7 June 2020 to 14 December 2021 | Staff – weekly PCR and 2 rapid lateral flow tests per week Residents – monthly PCR PCR tests for staff and residents if symptomatic Visitors – required to take a rapid lateral flow test before each visit (tests are free) |
To see the latest testing regime guidance for care homes, see the COVID-19 testing in adult social care guidance and the Infection prevention and control in adult social care settings. DHSC have also published a summary of changes to COVID-19 guidance for adult social care providers which provides details on the recent changes to the testing guidance.
Care home staff
Rapid lateral flow tests
In the week ending 22 March 2022, there were 17,646 positive tests returned from rapid lateral flow test kits in care home staff. This number increased throughout March and surpassed figures recorded in the previous peak in early January 2022. This increase follows a period of rapid decline seen throughout February 2022.
The number of rapid lateral flow tests conducted in care home staff, which includes positive, negative and void tests, increased slightly throughout March 2022. This increase follows a period of decline in February 2022. Despite this, the number of tests conducted remains lower than in mid-January 2022 (903,409 tests) with 724,449 in the week ending 22 March 2022.
The increase in March may have partly been driven by the change in testing guidance on 16 February 2022, when pre-shift rapid lateral flow tests replaced thrice weekly rapid lateral flow tests. Further changes to the guidance took effect on 4 April 2022, which will further affect the trends in the data in future publications.
PCR tests
The overall number of PCR tests conducted – including positive, negative and void tests – in care home staff increased in the week ending 22 March 2022 compared to the previous week. This is the first increase recorded after a period of decrease since the end of February, following the removal of weekly asymptomatic PCR testing in the guidance on 16 February 2022.
Due to the recent changes in testing guidance for care home staff, PCR test results are now less relevant than rapid lateral flow test results in measuring COVID-19 prevalence in care homes.
Care home residents
The testing regime for staff is more frequent than for residents. As a result, the total number of staff tests is higher than the total number of resident tests. For more information, see the ‘About this data’ section.
Rapid lateral flow tests
In the week ending 22 March 2022, there were 3,207 positive tests returned from rapid lateral flow test kits in care home residents. The number of positive rapid lateral flow tests returned during March 2022 increased substantially, surpassing levels recorded during the previous peak in the week ending 4 January 2022 (2,411). This recent steep increase follows a previous period of decline seen throughout February 2022.
The number of rapid lateral flow tests conducted in care home residents, which includes positive, negative and void tests, increased slightly throughout March 2022 following a period of decrease in January and February. In the week ending 22 March 2022 there were 37,720 tests conducted, which remains substantially lower than the 77,197 tests conducted in the week ending 4 January 2022.
PCR tests
The number of PCR tests conducted – including positive, negative and void tests – in care home residents also increased slightly throughout March 2022, following a period of decease. Despite this, figures remain substantially lower than in mid-January 2022.
The previous period of decrease in the overall number and number of positive PCR tests in care home residents followed the removal of a confirmatory PCR test after receiving a positive rapid lateral flow test result from 11 January 2022.
From 4 April 2022, as asymptomatic testing is removed for care home residents, residents will only take PCR tests in the event of an outbreak, prior to discharge from hospital or on new admissions to a care home. This change in guidance will affect the data in future publications.
Figure 10: number of tests conducted in care home staff and residents, 2 September 2020 to 22 March 2022, England
The number of tests conducted among staff and residents has increased slightly throughout March 2022 for both rapid lateral flows and PCR tests, following a period of rapid decrease.
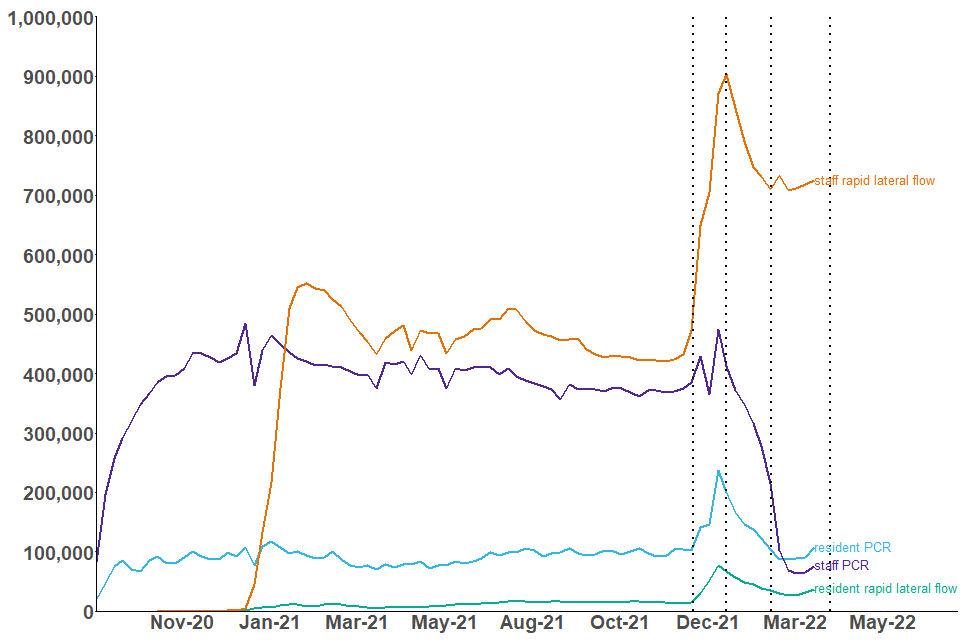
Source: NHS Test and Trace
Note: the dotted lines in this chart represent the implementation of the 4 most recent changes in care home testing guidance. See table 6 for a breakdown of the specific changes.
This data can be found in tables 1 and 2 of the accompanying ‘COVID-19 testing statistics, April 2022: data tables’ on the ASC monthly statistics page, in addition to data by region and local authority.
Figure 11: number of positive test results in care home staff and residents, 2 September 2020 to 22 March 2022, England
The number of positive test results returned in care home staff and residents rapidly increased throughout March 2022.
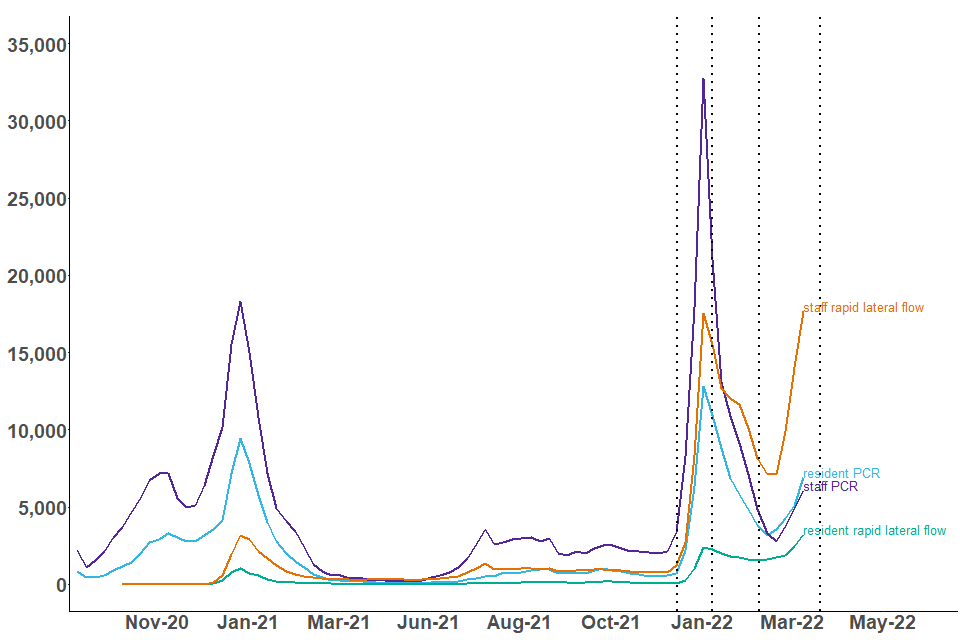
Source: NHS Test and Trace
Note: the dotted lines in this chart represent the implementation of the 4 most recent changes in care home testing guidance. See table 6 for a breakdown of the specific changes.
This data can be found in tables 1 and 2 of the accompanying ‘COVID-19 testing statistics, April 2022: data tables’ on the ASC monthly statistics page, in addition to data by region and local authority.
Staff and residents have different testing regimes as outlined in the ‘About this data’ section below. As a result, the number of positive test results returned are expected to be of a different scale between staff and residents.
Visitors
The number of positive tests returned in both care home visitors and visiting professionals has increased in March 2022, following a period of decrease.
In the week ending 22 March 2022 there were:
- 690 positive rapid lateral flow tests and 78 positive PCR tests returned in care home visitors
- 107 positive rapid lateral flow tests and 4 positive PCR tests returned among visiting professionals to care homes
The number of rapid lateral flow tests conducted – including positive, negative and void tests – among visitors decreased slightly in March 2022. In the week ending 22 March 2022, there were 85,926 rapid lateral flow tests conducted among visitors compared to 93,014 at the start of the month. This follows a period of increase from mid-January to mid-February, which coincided with the relaxation of visiting restrictions allowing more visitors per resident in care homes.
Additionally, there were 8,934 rapid lateral flow tests conducted among visiting professionals to care homes in the week ending 22 March 2022. This has been broadly stable since early January 2022.
Terminology
Care home: facilities providing residential care. The data in this bulletin refers to Care Quality Commission (CQC) registered care homes.
Older adult care homes: care homes serving any older people (aged 65 and over) as identified from the latest CQC data on care homes in the ‘older people service’ user band. A small number of residents within care homes serving older people may be aged under 65.
Younger adult care homes: care homes not serving any older people (aged 65 and over) as identified from the latest CQC data on care homes in the ‘older people service’ user band.
Domiciliary care: services providing personal care for people living in their own homes. The data in this bulletin refers to domiciliary staff employed by independent CQC registered providers.
Staff: unless specified, staff can refer to staff directly employed by a provider and/or through an agency.
Staff employed by other settings: this includes non-registered providers and local authority employed: all other eligible frontline social care staff working in close and personal contact with people clinically vulnerable to COVID-19 (as defined by the Joint Committee on Vaccination and Immunisation (JCVI) priority groups) who need care and support irrespective of where they work or who they are employed by, for example, local government, NHS, private sector or third sector.
Agreed staffing ratios: the agreed number of residents for any given member of staff. This is determined by individual providers to ensure there is safe levels of staffing for care to be delivered. This can be subject to inspection by the CQC. See Regulation of staffing for more information.
PCR (polymerase chain reaction) tests: PCR tests check for the genetic material of the coronavirus in the sample, which is taken using a swab and is processed in a lab via a polymerase chain reaction (PCR). These are predominantly used in care homes for people who experience symptoms, and for routine asymptomatic testing for staff and residents.
Rapid lateral flow tests: often referred to as ‘rapid tests’, or lateral flow device, these test for the presence of proteins called ‘antigens’ which are produced by the virus. They are swab tests that give results in 30 minutes or less, without the need for processing in a laboratory. These tests are primarily used in care homes for routine asymptomatic testing for staff, residents and visitors.
PPE (personal protective equipment): equipment worn by staff or visitors in care homes to reduce transmission of COVID-19. This publication refers to supplies of aprons, eye protection, gloves, hand sanitiser and face masks in care homes.
About this data
These statistics are being published as a part of a wider landscape of statistics on adult social care. The Government Statistical Service (GSS) compiles a UK adult social care database of official statistics on adult social care across the 4 nations of the UK. This is updated on a monthly basis.
The UK Statistics Authority (UKSA) conducted a review of adult social care statistics in England which called for:
-
better leadership and collaboration across different organisations publishing official statistics. This publication has been produced in collaboration with other statistics providers of COVID-19 adult social care data and DHSC will endeavour to work with various stakeholders as more data is published through this publication
-
addressing of gaps in available data, particularly in privately funded care. This bulletin aims to plug some of that gap by including data on residents privately funding their care in addition to those funded by local authorities
-
improving existing official statistics. These statistics are being badged as experimental statistics and more data will be added iteratively based on user needs
Other sources of adult social care COVID-19 data
COVID-19 vaccinations
NHS England and Improvement (NHSEI) also publish data on vaccinations in adult social care settings as part of their broader statistical release on COVID-19 vaccination, using the same methodology and the same data source as this publication but there are differences in the:
-
reporting period; data in this publication reports data collected up to 11:59pm on a Tuesday whereas NHSEI use data collected up to 11:59pm on a Sunday
-
a small amount of data may be collected after the respective reporting periods
-
regional breakdowns; data in this publication uses the administrative regions of England and NHSEI use NHS regions
COVID-19 testing
DHSC also publishes care home testing data in the weekly NHS Test and Trace statistics (England) at national level. This publication uses the same data source but has a different methodology for presenting testing in care homes and differences in the figures will occur due to the following reasons:
-
differences in which tests from different routes are included. Both methodologies include the number of tests registered from kits sent directly to care homes, but this publication additionally includes care home staff or residents tested via other routes such as regional or local test sites. As a result, figures in this report will be substantially higher for PCR tests conducted in care home staff due to the current guidance recommending staff with symptoms to be tested outside of the care home (see coronavirus (COVID-19) testing in adult care homes for more information). This also means that changes in the guidance for the wider population might affect the trends differently across both publications
-
different reporting periods. This publication uses the start time of the test in comparison to the Test and Trace statistics which use the date on which the test result was received by the individual taking the test
-
different times of extracting the data
For more details on the NHS Test and Trace programme and the statistics see the NHS Test and Trace methodology document.
Adult social care workforce size and absence statistics
Skills for Care publishes yearly and monthly estimates of the number of adult social care filled posts as a measurement of the size of the adult social care workforce. Differences in data sources and methodology mean that these statistics are not comparable with those published in this report.
Skills for Care’s monthly tracking data on staffing is based on the unweighted responses of a relatively small cohort of providers who have updated records in the Adult Social Care Workforce Data Set (ASC-WDS) in each respective month. This data may not be representative of the sector as a whole and therefore may only be indicative of general trends. Skills for Care use a wider definition of ‘domiciliary care’ than is used in Capacity Tracker and include other services delivered in the user’s own home, such as supported living and extra care housing.
Skills for Care also publishes monthly estimates of the average number of days lost due to sickness, which are not comparable with the absence rates published in this report. This is because of similar reasons explained above and due to the nature of Skills for Care’s estimate which is not specific to COVID-19 related absences.
In December 2021, an additional workforce report providing more information on the pressures faced by the adult social care workforce has been published as part of this data collection. This information was received through an ad hoc survey, and has been published as part of this collection as a one-time event. See the adult social care workforce survey: December 2021 report.
The workforce survey complements the regular collection by providing the opportunity to have a deeper exploration of workforce issues which is possible in an ad hoc survey but would be too burdensome for the regular collection.
Data sources
COVID-19 vaccination, infection prevention control (IPC), PPE availability, absence rates and staffing levels
Data in this publication is taken from self-reported data submitted by care providers in England through a data collection and insight tool called Capacity Tracker.
Up until 4 April 2022, care providers were expected to submit data on IPC compliance on a weekly basis while data on vaccinations, PPE availability, staff absences and staffing levels is expected to be updated on a daily basis. After 4 April 2022, all data fields are expected to be updated weekly, to reduce the burden on providers.
Infection control data for each reporting week refers to data up to 2pm on the date stated as the ‘week ending’ and the 7 days prior. For PPE, absence rates and staffing-levels, data relates up to 11:59pm on the date stated as the ‘week ending’. The reporting week usually ends on a Tuesday but occasionally no data is available for this date, in these situations the ‘week ending’ date will be the nearest available date.
This bulletin presents the proportion of staff and residents vaccinated out of the total number of staff and residents as self-reported by care providers. Only individuals who have not tested positive for COVID-19 in the last 28 days are eligible to receive the vaccine. Data on the number of staff and residents of older adult care homes eligible for the vaccination over time can be found in the accompanying COVID-19 vaccination tables on the ASC monthly statistics page.
For more information, see the ‘Data Sources’ section of the accompanying background quality and methodology note.
COVID-19 testing data
Testing data is collected from management information generated during the operation of the NHS Test and Trace service.
For more information, see the ‘Data Sources’ section of the accompanying background quality and methodology note.
Data coverage and quality
All data in this publication refers to adult social care settings in England only.
Data submitted by providers reflects the current priorities to monitor the COVID-19 pandemic in social care settings. Data collection could be subject to change based on changes to the priorities and therefore the reporting in this publication will be adapted accordingly.
IPC, PPE availability, absence rates and staffing levels
Providers are expected to submit data on IPC measures on a weekly basis while staffing levels and PPE availability data are expected to be submitted on a daily basis. Any providers who have not submitted data within the last 7 days are excluded from the relevant analysis for the associated time period where no response was received. The full response rates for all data points are available in tables 9 to 12 of the accompanying ‘Infection control, PPE and workforce statistics data tables’ on the ASC monthly statistics page. From 4 April 2022, the expectation for all data fields changed to weekly, to reduce the burden on providers.
COVID-19 vaccinations
Data on total number of staff and residents as well as those vaccinated is self-reported by care providers and local authorities. Providers are expected to update their vaccination data on a daily basis. There may be a time lag between individuals receiving the vaccine and the week they are reported in the statistics depending on when providers have updated their vaccination data. From 4 April 2022, the expectation for all data fields changed to weekly, to reduce the burden on providers.
COVID-19 testing
This report includes the number of tests conducted on care homes residents, staff and visitors who were tested by:
-
PCR and rapid lateral flow test kits sent directly to the care home for regular testing, which were registered through the National Testing Programme digital infrastructure
-
PCR and rapid lateral flow test kits conducted at another testing site such as a regional or local test site or a mobile testing unit or tests that were registered
The figures in this report are only deduplicated to report on the number of individual tests taken, not the number of people tested. Because people can have more than one test, the data should not be compared with prevalence rates or case positivity rates.
This report does not contain data on those tested through pillar 1.
Data for each reporting period relates to the day an individual took their test.
To see the latest testing regime guidance for care homes see the COVID-19 testing in adult social care guidance and the Infection prevention and control in adult social care settings guidance.
The guidance for testing in care homes changed on 4 April 2022, but these changes do not affect the trends presented in this report. From 4 April 2022, staff are expected to take rapid lateral flow tests twice a week, and asymptomatic testing for residents is removed. Additionally, symptomatic testing is now done with rapid lateral flow tests instead of PCR tests. On 31 March 2022, DHSC published a summary of changes to testing and other IPC measures.
As of the week ending 22 March 2022, which is the latest data point included in this publication, the regular testing regime in place was as follows:
Care home staff testing:
- before each shift, with a rapid lateral flow test
- immediately if they develop symptoms, with a PCR test taken at home or at a testing site
Care home residents testing:
- monthly, using PCR test kits
- as soon as they join a care home, if they are new, with a PCR test
- immediately if they develop symptoms, with a PCR test
Care home visitors testing:
- visitors should receive a negative lateral flow test result and report it on the day of their visit, either by conducting the test at home or when they arrive at the care home
Visiting professionals to care homes:
- NHS professionals should provide proof of a negative test taken 72 hours in advance of the visit
- CQC inspectors regularly take weekly PCR tests but should additionally take rapid lateral flow test on the day of visiting a care home
- other professionals should be tested with a rapid lateral flow test on arrival
Different testing regimes apply when there is an outbreak of COVID-19 in a care home. See the COVID-19 testing in adult social care guidance for more details.
Revisions
Any revisions to past publications will be in line with DHSC’s revision policy and highlighted in future publications accordingly.
Feedback
For feedback and any further questions, contact asc.statistics@dhsc.gov.uk.