From harm to hope: A 10-year drugs plan to cut crime and save lives
Updated 29 April 2022

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/from-harm-to-hope-a-10-year-drugs-plan-to-cut-crime-and-save-lives/from-harm-to-hope-a-10-year-drugs-plan-to-cut-crime-and-save-lives
Forward
The Prime Minister
It’s that much harder to level up a community while criminals are dragging it down. After all, to thrive and succeed in life we need to feel safe on our streets and secure in our homes. And if we’re going to make that the daily reality for most people in this country then we’re going to have to do more to tackle illegal drugs.
That’s what this strategy is all about, a new approach to the problem that will reduce crime and improve people’s lives.
The financial cost of drug misuse is absolutely staggering. It currently costs society almost £20 billion a year, something like £350 for every man, woman and child in England.
But the human toll is incalculably larger, measured not in pounds lost but in lives shattered.
The vulnerable victims of the vile county lines gangs, dragged into the world of organised crime from as young as seven. The innocent families whose homes are broken into by addicts seeking to feed their habits, and whose neighbourhoods are blighted by the criminals who supply them. The small business owner who endures repeated shoplifting and anti-social behaviour on their high street. The almost 3,000 people who lose their lives to illicit drugs each year, and the grieving loved ones they leave behind.
It’s clear that the old way of doing things isn’t working. So this plan is different. It’s not a short-term fix but a long-term, 10-year strategy, one that treats drug abuse not just as a law enforcement issue but as a problem for all of society that all of government must deal with.
There are more than 300,000 heroin and crack addicts in England who, between them, are responsible for nearly half of all burglaries, robberies and other acquisitive crime. These serial offenders should be properly punished for the crimes they commit, crimes which cause misery in communities across the country. But they should also be given the chance to get off drugs and turn their lives around. Because if we can turn around the lives of addicts, the communities in which they live will experience lower crime, lower disorder and less violence. That is our goal.
We will also crack down on the supply chains that deliver misery to so many neighbourhoods. Children will receive a comprehensive education about the dangers of drugs. Interventions will happen earlier to stop young people getting dragged into a life of drugs and crime.
And there will be no implicit tolerance of so-called recreational drug users. We cannot allow the impression to be given that occasional drug use is acceptable. It isn’t. So there will be new penalties for drug users.
Because drugs cause crime and crime ruins innocent lives. If we’re going to succeed in levelling up this country then we have to break the cycle of violence and abuse that blights so many communities, bring hope to those who have long since lost it and help rebuild the lives shattered by the illegal drug trade.
With this strategy, that’s exactly what this government will do.
Rt Hon Boris Johnson, MP Prime Minister
The Secretary of State for Health and Social Care, the Secretary of State for the Home Department and the Combating Drugs Minister
This ten-year plan, the most ambitious for a generation, sets out how this Government will combat illegal drug use – reducing crime, saving lives, and challenging the very notion of ‘recreational drug use’, which fuels a violent and exploitative market.
This is the first ever Drugs Strategy that commits the whole of government and our public services to work together and share responsibility for creating a safer, healthier and more productive society. Illegal drug use is a complex issue that has evolved over many years, so we must harness all of our energy and expertise as we respond.
The worrying trends of recent years, exposed by the excellent reviews led by Dame Carol Black, mean that failing to act is not an option.
Drugs have a ruinous effect on our society, leaving a trail of misery in their wake. They drive half of all homicides and nearly 3,000 people tragically lost their lives through drug misuse deaths in England and Wales last year. Not only that, the most deprived areas face the most drug-driven crime and health harms.
Drugs destroy lives, they shatter families and they plague neighbourhoods around the country, fuelling violence and acquisitive crime. Enough is enough. We must turn the tide.
This government will reverse these problems within the next decade. We will make our neighbourhoods safer for decades to come through an uncompromising confrontation of the illegal drug market, reducing harm to individuals and communities, through treatment and recovery from addiction, and by reducing demand for drugs.
We will make crime an unattractive option that doesn’t pay. Justice will be served to drug dealers thanks to tough enforcement and world-class intelligence. We are committed to bring the full force of government to bear in a relentless and uncompromising attack on every phase of the drugs supply chain.
We’re also giving the prison service the capability and technology to disrupt the supply and use of drugs in prison protecting prisons from being academies of crime. All prisons must have a zero-tolerance approach to drugs, making sure that treatment is available so prisoners can make lasting change towards drug-free life to prevent them reoffending.
We will also ensure that there is early intervention for young people and families at the greatest risk and make sure all children are provided with high quality education on health and relationships to help prevent the use of drugs.
We will offer more support to people with drug addiction. Addiction is a chronic condition that requires earlier and better treatment, and sustained support. That will be combined with more funding to give more people better quality treatment, support for those who are in need of housing, and employment support to help people find a job that’s right for them.
Drug dependence often co-exists with other health disparities, like poor mental health and homelessness, so we’re making sure the physical and mental health needs of people with drug addictions are addressed, to reduce harm and support recovery.
We’re also boosting the sector’s health professional workforce, so they’re well equipped to deliver the treatments needed to succeed. As well as this, we’ll work with the NHS and the third sector to expand and improve evidence-based treatments and interventions, for example talking therapies, inpatient detoxification and residential rehabilitation, needle and syringe programmes, and a full range of medicines that can support recovery.
The strategy also shows how we’ll keep expanding the provision of the life-saving heroin antidote naloxone to drive down drug-related deaths and explore the rollout of the potentially revolutionary buprenorphine, to drive down drug deaths.
And for adults taking recreational drugs, who are too often sheltered from the serious violence, human exploitation, severe addiction and crime of the drugs trade, there will be tougher consequences which will be felt more strongly than today. A White Paper next year will consider a series of escalating sanctions such as curfews or the temporary removal of a passport or driving licence, and increased fines.
To deliver this ambitious strategy, we are investing almost £900 million of additional funding over the next three years and developing a new framework of national and local accountability. This will deliver 54,500 more treatment places, prevent nearly 1,000 deaths, and close over 2,000 more county lines. We will reverse the rising trend in drug use within a decade, with an ambition to reduce overall use towards a historic 30-year low.
The government will be relentless in our tenacity, to utilise every tool at our disposal to drive drugs out from our cities, towns, and villages. Our strategy is designed to save lives and reduce crime, in turn helping to level up our country. The stakes could not be higher, and we are utterly determined to deliver the change that is so badly needed.
The Rt Hon Priti Patel MP Home Secretary
The Rt Hon Sajid Javid MP Health Secretary
The Rt Hon Kit Malthouse MP Combating Drugs Minister
Executive summary
Our 10-year UK Government plan to combat illegal drugs sets out how we are doing more than ever to cut off the supply of drugs by criminal gangs and give people with a drug addiction a route to a productive and drug-free life [footnote 1]. Underpinned by record investment of over £3 billion in the next three years, we will reduce drug-related crime, death, harm and overall drug use.
National and local partners will focus on delivering three strategic priorities:
Break drug supply chains – Home Office and Ministry of Justice
Within a decade the UK will be a significantly harder place for organised crime groups (OCGs) to operate. We will step up our response to the supply of the most harmful drugs, attacking all stages of the supply chain, reducing the associated violence and exploitation, and protecting prisons from being academies of crime. We will achieve this by:
1. restricting upstream flow – preventing drugs from reaching the country
2. securing the border – a ring of steel to stop drugs entering the UK
3. targeting the ‘middle market’ – breaking the ability of gangs to supply drugs wholesale to neighbourhood dealers
4. going after the money – disrupting drug gang operations and seizing their cash
5. rolling up county lines – bringing perpetrators to justice, safeguarding and supporting victims, and reducing violence and homicide
6. tackling the retail market – so that the police are better able to target local drug gangs and street dealing
7. restricting the supply of drugs into prisons – technology and skills to improve security and detection
Deliver a world-class treatment and recovery system – Department of Health and Social Care, Ministry of Justice, Department for Levelling Up, Housing and Communities, and the Department for Work and Pensions
Within a decade, we will deliver a world-class treatment and recovery system in England. An additional £780 million over three years will be committed to begin to take this forward, implementing Dame Carol Black’s key recommendations [footnote 2]. We will treat addiction as a chronic health condition, breaking down stigma, saving lives, and substantially breaking the cycle of crime that addiction can drive by:
1. delivering world-class treatment and recovery services – rebuild local authority commissioned substance misuse services, improving quality, capacity and outcomes
2. rebuilding the professional workforce – develop and deliver a comprehensive substance misuse workforce strategy
3. ensuring better integration of services – making sure that people’s physical and mental health needs are addressed to reduce harm and support recovery, and ongoing delivery of Project ADDER to join up treatment, recovery and enforcement [footnote 3]
4. improving access to accommodation alongside treatment – access to quality treatment for everyone sleeping rough and better support for accessing and maintaining secure and safe housing
5. improving employment opportunities – employment support rolled-out across England and more peer support linked to Jobcentre Plus services
6. increasing referrals into treatment in the criminal justice system – specialist drug workers to support treatment requirements as part of community sentences so offenders engage in drug treatment
7. keeping prisoners engaged in treatment after release – improved engagement of people before they leave prison and better continuity of care into the community
Achieve a generational shift in demand for drugs – Home Office, Department for Education, Department of Health and Social Care, Ministry of Justice, Department for Culture, Media and Sport, Department for Levelling Up Housing and Communities
We will take bold steps to change attitudes in society around the perceived acceptability of illegal drug use. We will achieve this by:
1. building a world-leading evidence base – ambitious new research backed by a cross-government innovation fund to test and learn and drive real-world change
2. applying tougher and more meaningful consequences – decisive action to do more than ever to target more people in possession of illegal drugs and a white paper next year with proposals to go further
3. delivering school-based prevention and early intervention – delivering and evaluating mandatory relationships, sex and health education to improve quality and consistency, including a clear expectation that all pupils will learn about the dangers of drugs and alcohol during their time at school
4. supporting young people and families most at risk of substance misuse – investing in a range of programmes that provide early, targeted support, including the Supporting Families Programme
By the end of 2024/25 we expect this whole-of-government mission to have:
- prevented nearly 1,000 deaths, reversing the upward trend in drug deaths for the first time in a decade
- delivered a phased expansion of treatment capacity with at least 54,500 new high-quality treatment places – an increase of 20% – including:
- 21,000 new places for opiate and crack users, delivering 53% of opiate and crack users in treatment
- at least 7,500 more treatment places for people who are either rough sleeping or at immediate risk of rough sleeping – a 33% increase on the current numbers
- a treatment place for every offender with an addiction
- contributed to the prevention of three-quarters of a million crimes including 140,000 neighbourhood crimes through the increases in drug treatment
- closed over 2,000 more county lines through our relentless and robust action to break the model and bring down the gangs running these illegal lines
- delivered 6,400 major and moderate disruptions – a 20% increase – against activities of organised criminals, including arresting influential suppliers, targeting their finances and dismantling supply chains
- significantly increase our denial of criminal assets, taking cash, crypto-currency and other assets from the hands of criminals involved in drug trafficking and supply
Over the course of the 10-year strategy, we will reverse the rising trend in drug use, with an ambition to reduce overall use towards a historic 30-year low. This will support the government’s levelling up mission with people living longer, healthier lives, in safe and productive neighbourhoods.
Accountability and delivery
As Combating Drugs Minister, Kit Malthouse MP, has overarching accountability for the strategy and delivery of the ambitions and commitments, and will present an annual report to Parliament to monitor progress. Each relevant secretary of state has accountability for delivery of the elements within their department’s remit, with a relentless focus on better outcomes for citizens and neighbourhoods set out through a new national outcomes framework.
Local delivery partners will be held to account through a local outcomes framework and wider measures set out in chapter 5. We will engage with delivery partners to develop and publish both frameworks in April 2022, identifying accountable owners within local areas. Success relies on a wide range of local partners working together toward the long-term ambitions of the strategy.
To support delivery across England we are:
- requiring each local area to have a strong partnership that brings together all the relevant organisations and key individuals, and developing guidance to support the new Integrated Care Systems (ICS)
- developing and implementing a commissioning quality standard to support transparency and accountability between all partners and layers of government
Delivering a safe, healthy and more productive country
Addressing the complex relationship between drugs, crime, health outcomes and deprivation means we will make a substantial contribution to the government’s defining mission of levelling up.
In some areas people experience greater harm because of where they live: the impact of higher levels of drug addiction and drug-related crime disproportionately blight their neighbourhoods.
We will level up our response to drugs through increasing our support, targeting first those neighbourhoods which suffer the most, and ensuring we reach every local authority over the next three years. To help us do this, we will take learning from our flagship Project ADDER, with a sharp focus on delivery for citizens.
Chapter 1 – Overview and approach
The chronic and entrenched nature of drug use in this country and around the world means we need to take a long-term approach if we are to be successful in turning this around. This 10-year plan is an evidence-based and modern approach to addressing the demand for, and supply of, drugs.
This is essential to prevent problems from resurfacing or worsening. Over the next decade we will turn the tide on drug crime, reduce the harm drugs cause to individuals and society, and save lives for this generation and the next. This will be underpinned by nearly £900 million of additional investment over the next three years, taking the total cross-government funding to more than £3 billion, national and local system reform, and a set of ambitious outcomes and goals to which government and local partners will be held accountable for delivery.
The challenge of illegal drug use
Drugs are a global problem, causing considerable harm around the world. Drug use and harms have been rising, blighting neighbourhoods and holding them back from levelling up to their full potential. Since the last drugs strategy was published in 2017, it has become clear that we need to step back and understand why things have continued to head in the wrong direction.
Dame Carol Black was commissioned to carry out a two-part review of drugs policy. Part one was a broad assessment of the evidence on illegal drug supply into the UK and how criminals meet the demand of users, and part two made specific recommendations for improving prevention, treatment and recovery [footnote 4].
These reviews set out the stark reality. An estimated 1,716 OCGs are involved in supplying drugs in the UK, including within the prison estate [footnote 5]. County lines are driving increased violence in the drugs market, as well as exploitation of young people and vulnerable drug users. In 2020 alone referrals of children suspected to be victims of county lines increased by 31% [footnote 6]. The UK is among the countries in Europe most affected by drugs and demand for them across the population is too high: over three million adults reported using drugs in England and Wales in the last year and one in three 15-year-olds said they took drugs in 2018, up from one in four in 2014.
Over three million adults reported using drugs in England and Wales in the last year and one in three 15-year-olds said they took drugs in 2018 [footnote 7].
The capacity of the treatment system is insufficient to meet the need for support and half of people with an addiction to the most harmful drugs – opiate and crack cocaine – are not engaged in treatment. The level of unmet need for other drugs is even higher. A number of countries have been experiencing their highest levels of drug-related deaths over recent years, and in the UK, there has been an 80% increase since 2012, with the number of heroin-related deaths doubling in that time [footnote 8].
Some people experience multiple and complex needs, with drug addiction co-occurring with a range of health inequalities such as mental ill health, homelessness and rough sleeping, and contact with the criminal justice system. In England, over a quarter of a million people each year experience at least two out of three across homelessness, substance misuse and involvement in the criminal justice system, and at least 58,000 people have contact with all three [footnote 9]. The likelihood of suffering from these disadvantages varies widely depending on where a person lives, with high numbers concentrated in northern cities and some seaside towns. Reduced drug use will mean that people live longer, healthier lives and suffer less crime in their neighbourhoods.
Our 10-year strategic approach
This strategy is underpinned by a clear recognition that illegal drugs damage society. Our collective ambition is to achieve a generational shift in the country’s relationship with drugs and to reduce overall drug use towards a historic 30-year low. We will also reduce the harms that drug addiction and supply cause to individuals and neighbourhoods.
Over 300,000 people are addicted to heroin and crack cocaine in England. This is the biggest section of the illegal drugs market with an estimated value of £5.1 billion a year. The addiction, harms and deaths that these drugs cause, and the violence associated with their supply, result in the vast majority of the cost to individuals, neighbourhoods and society [footnote 10]. Addiction to these drugs is thought to be linked to around half of all theft, burglary and robbery with, on average, people with an addiction using drugs on 251 days of the year at a cost of £12,538 [footnote 11].
For these reasons, we will focus in the immediate term on efforts to combat the supply of heroin and crack cocaine, and on getting those suffering from addiction the treatment and support they need.
At the same time, we will retain a sharp focus on pursuing the illegal supply of all drugs and on delivering high-quality treatment for addiction to other drugs. The addiction they cause can and does ruin lives. Over half of the additional people receiving drug treatment over the next three years will be supported into long-term recovery from a range of substances including cannabis, powder cocaine, alcohol and synthetic drugs, , including GHB and similar substances often involved in ‘chemsex’.
We will also do more to reduce non-dependent, so-called ‘recreational’ drug use. For example, users of cocaine, who on average take drugs 30 days of a year, may think their use is harmless, but it feeds a criminal market worth around £2 billion that is reliant on an exploitative and violent supply chain, both at home and abroad [footnote 12]. Legal consequences for this use have not been sufficiently applied across all levels of society, with the Commission on Race and Ethnic Disparities highlighting the disproportionate effect of possession laws, particularly for Class B drugs, on young black people [footnote 13]. We will improve our methods for identifying ‘recreational’ drug users and roll-out a system of tougher penalties aimed at this.
Decriminalisation is often suggested as a simple solution to many of the problems caused by illegal drugs. This is not the case. It would leave organised criminals in control while risking an increase in drug use. What is required is the whole system approach recommended by Dame Carol Black and, in implementing all of the key recommendations of her review, that is what this strategy seeks to do: cutting off the supply of drugs, preventing and reducing drug use, and world-class treatment and recovery support for those battling addiction.
Addressing the increase in overall drug use requires a generational and attitudinal shift so that in 10 years fewer people take drugs or feel drawn towards taking them. Investing in the education and resilience of children and young people will help us to level up the whole country, particularly for those families at higher risk of drug use or harm, so that no matter where someone is born or lives, they can excel and prosper in those places.
Our strategic priorities require different approaches and will have differing impacts across demographics and local areas. We will monitor impacts across the strategy’s whole system approach to track progress towards better outcomes and avoid any unintended consequences, such as widening inequalities. The following table summarises our three strategic priorities and our plan against each.
Our plan on a page - Drug Strategy strategic priorities
| Priority | Break drug supply chains | Deliver world-class treatment and recovery services | Achieve a shift in the demand for recreational drugs |
|---|---|---|---|
| Why? | Drug supply chains are violent and exploitative, degrading neighbourhoods across the country and internationally | Drug addiction harms individuals and society: deaths have risen to record levels and almost half of acquisitive crime is linked to addiction | Use of recreational drugs has grown over a decade, particularly among young people, risking individual harm and fuelling dangerous markets |
| How? | We will continue to roll up county lines and strengthen our response across the drug supply chain, making the UK a significantly harder place for organised crime groups to operate | We will invest a further £780 million to rebuild drug treatment and recovery services, including for young people and offenders, with new commissioning standards to drive transparency and consistency | We will strengthen the evidence for how best to deter use of recreational drugs, ensuring that adults change their behaviour or face tough consequences, and with universal and targeted activity to prevent young people from starting to take drugs |
| Who? | Home Office and MoJ, working with international and intelligence partners, NCA, Border Force, police, courts, prison and probation | DHSC, DLUHC, DWP and MoJ working with NHSE, local authorities, treatment providers and people with lived experience | DfE, DHSC, Home Office and MoJ, working with local authorities, police, education providers, secure facilities and youth services |
| What? | Within three years: close over 2,000 more county lines, disrupt 6,400 OCG activities and deny more criminal assets | Within three years: prevent nearly 1,000 deaths, deliver 54,500 new high-quality treatment places and prevent a quarter of a million crimes | Reduce overall drug use to a new historic 30-year low over the next decade |
Putting evidence at the heart of this approach
These priorities are underpinned by Dame Carol Black’s landmark review. This recommended a new long-term approach, with large-scale investment and changes to oversight and accountability, delivered by the whole of government. The review set out the compelling evidence based on the benefits to society of investment in high-quality drug treatment and recovery.
Through this strategy, we will deliver all of the key recommendations from part two of the review.
The record national investment that this government committed to this year gives a solid foundation for our ambitious strategic approach. The drug treatment, recovery and criminal justice workforces have responded with drive and innovation to deliver new treatment places and recruit and train a new generation. Across enforcement, we have built a powerful set of policies in co-operation with police and operational partners with encouraging results.
Through Project ADDER, local partners are demonstrating the success we can have by bringing enforcement, treatment and recovery efforts together in areas of the greatest need.
We will become world-leading in our approach, with evidence-led and data-driven interventions, and a commitment to build the evidence base where necessary. We will work across government, with delivery partners, experts and advisers, those with lived experience, and those who work in our public services to get this right.
Our mission is to be at the forefront of international co-operation, working with our international partners to shape the global debate on drugs, respond to new threats and share evidence and best practice through our global networks. These networks include the Five Eyes, the United Nations Commission on Narcotic Drugs and the United Nations Office on Drugs and Crime. Combating illegal drugs is a global challenge and, as such, we look to our partners across the world in evolving our approach.
Levelling up our neighbourhoods
Combating drugs use and harm is a priority for all of government. This strategy sets out commitments across the Home Office [footnote 14], the Department of Health and Social Care (DHSC) [footnote 15], the Ministry of Justice (MOJ) [footnote 16], the Department for Work and Pensions (DWP) [footnote 17], the Department for Levelling Up, Housing and Communities (DLUHC) [footnote 18], and the Department for Education (DfE) [footnote 19]. This will mean police officers, drug treatment and recovery staff, housing officers, prison and probation officers, mental health service staff, youth offending staff, family key workers, employment support workers and teachers joining forces in a way that has never been done before.
Confronting the drug threat is at the heart of this government’s ambition to level up the country. This strategy takes us further and helps us to deliver the commitments to protect victims and make streets safer, as set out in the Beating Crime Plan. The Beating Crime Plan demonstrated that neighbourhoods blighted by the presence of highly damaging Class A drugs cannot prosper and provide the happy, healthy environment that their citizens deserve. The most deprived areas face the highest prevalence of drug-driven crime and health harms associated with drug use. They also experience more of the harms caused by illegal drug markets.
People face multiple disadvantage in every local authority – drug addiction, homelessness and contact with the criminal justice system are often experienced in combination. But in some places, particularly some northern cities and seaside towns, there is a higher prevalence of this multiple disadvantage, as shown in the maps of England below. This strategy will deliver for the whole nation, investing first in these areas of greatest need. Our approach will empower local leaders and communities to help address these challenges, giving people more opportunities to develop skills and increase the prosperity of the areas they live in.
Application across the United Kingdom
Combating illegal drug use and harm is a priority for the whole of the UK. Many elements of drugs policy are devolved but this does not mean that we, together with our colleagues in the devolved administrations, are any less determined in our effort to confront this issue right across the UK.
While this strategy applies to matters reserved to the UK Government, we are fully committed to building a UK-wide approach so that we further embed collaboration, share practice with each other and collectively develop the evidence base on a wide range of drugs issues [footnote 20].
Map of England showing local authorities ranked by opiate and crack cocaine use
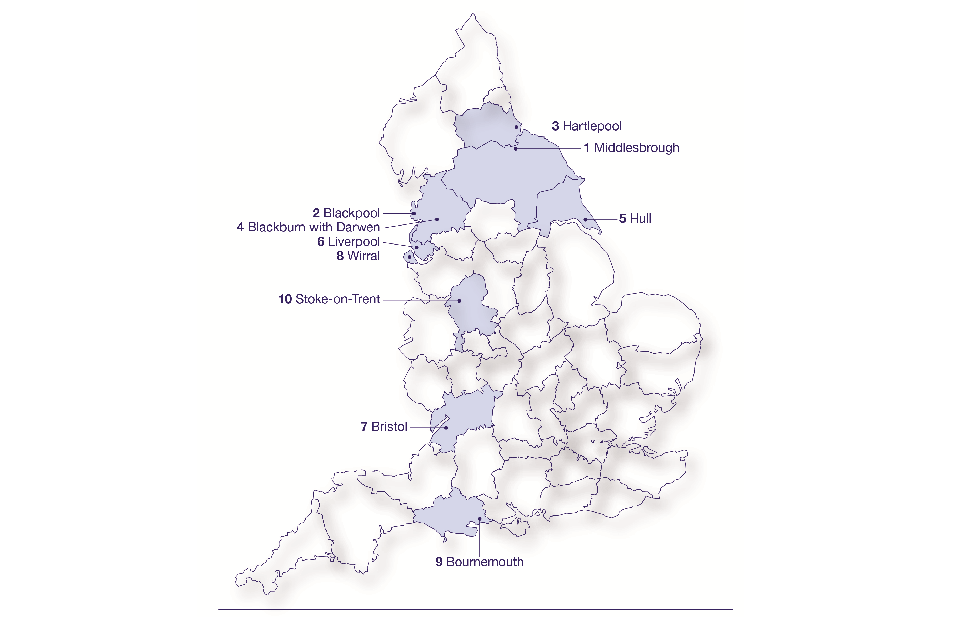
Map of England showing local authorities ranked by opiate and crack cocaine use
Opiate and crack use ranked by local authority (per 1,000 population)
- Middlesbrough 25.51
- Blackpool 23.45
- Hartlepool 20.63
- Blackburn and Darwen 18.84
- Hull 18.15
- Liverpool 17.06
- Bristol 15.66
- Wirral 15.63
- Bournemouth 15.05
- Stoke-on-Trent 14.67
Map of England showing local authorities ranked by multiple and complex needs
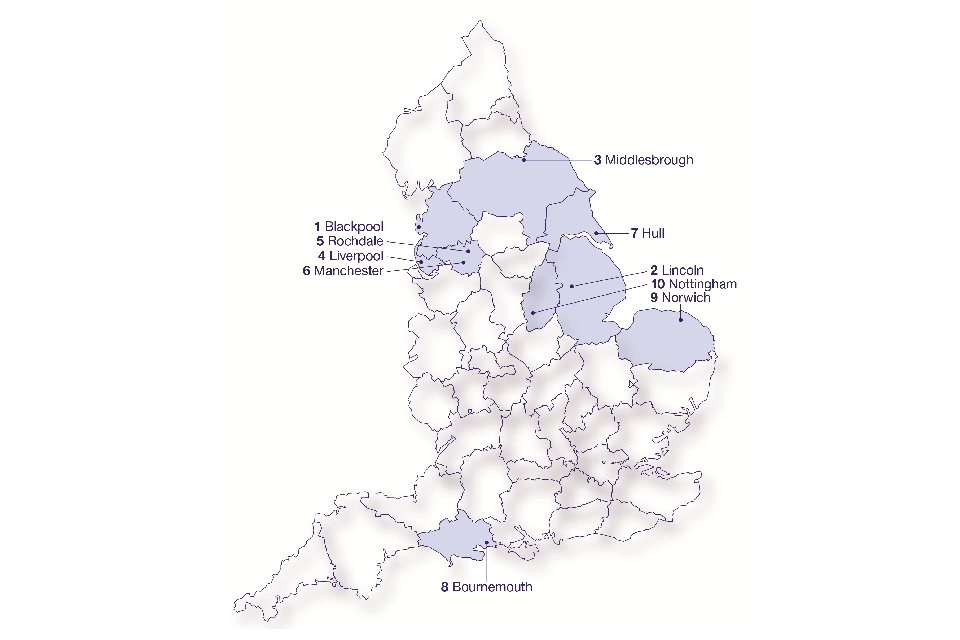
Map of England showing local authorities ranked by multiple and complex needs
Number with multiple and complex needs ranked by local authority (per 1,000 of working age adults)
- Blackpool 17.3
- Lincoln 16.2
- Middlesbrough 15.9
- Liverpool 13.4
- Rochdale 12.7
- Manchester 12.7
- Hull 12.7
- Bournemouth 12.4
- Norwich 12.3
- Nottingham 12.0
UK-wide sharing programme
In this strategy we have set out where we share objectives, as well as areas in which we are working together or learning from one another. We are committed to implementing a strong UK-wide sharing programme which will enable us to work closely with counterparts in the devolved administrations.
In October 2021, the UK Government Sponsor Minister for Combating Drugs chaired a summit in Belfast with ministers from across the UK and experts in the field to discuss a range of drugs issues. This was our third UK-wide drugs summit and there was a strong recognition that we all benefit from working together to address shared challenges. The Scottish Government, Welsh Government and Northern Ireland Executive have set out their own strategies – described below – to tackle the harms from drug use in areas where responsibility is devolved.
Scotland
Following further record rises in the number of drug-related deaths, in January 2021 the Scottish Government set out a national mission to improve and save lives. While it has an immediate focus on reducing drug deaths, the purpose of the mission is also to get more people into the form of treatment right for them, to reduce harms and to enhance recovery. Additional funding of £250 million over five years (from 2021) was announced to support this mission.
Since the announcement in January additional funding has been made available to alcohol and drug partnerships, national organisations as well as community and grass-roots organisations to support service improvement, support children and families affected by problem substance use, and increase capacity for residential rehabilitation.
The Scottish Drug Deaths Taskforce continues to lead work to address the unique challenges in Scotland by identifying evidence-based strategies that will make a difference to those most at risk. Through the taskforce the Scottish Government have: published a set of Medication Assisted Treatment standards to improve the delivery of drug treatment across Scotland; funded a wide range of projects, initiatives and research to further reduce the levels of drug deaths; worked with partners, including Police Scotland and the Scottish Ambulance Service, to massively increase the distribution of naloxone; and investigated the role of the criminal justice system in a public health response to problem substance use.
Wales
The Welsh Government published a revised Substance Misuse Delivery Plan (2019-22) in January 2021 in response to COVID-19 [footnote 21].
Harm reduction continues to be a key part of the Welsh Government’s approach and has been for 10 years. The Welsh Government sees substance misuse as a health issue and funding to substance misuse services, which are predominantly provided by local Area Planning Boards, has been increased over recent years and maintained, highlighting the support for the sector.
A range of prevention and treatment work is undertaken and a key part of the Welsh Government’s harm reduction approach has been the distribution of naloxone to prevent overdose deaths. A recently completed peer-to-peer naloxone pilot was very successful in increasing access to the medicine this is currently being rolled out across Wales.
Northern Ireland
Following two years of extensive consultation and production, the Northern Ireland Executive’s new Substance Use Strategy ‘Preventing harm & empowering recovery: a strategic framework to tackle substance use’ was launched in September 2021 [footnote 22].
Their 10 year strategy has five key outcomes covering: prevention, early intervention, and alternative approaches; harm reduction; treatment and support; recovery; and joined up implementation. Enforcement is one element of the overall response, to ensure that illegal drugs or illicit prescription drugs cannot find their way into circulation.
Problem solving justice is an international model being developed in Northern Ireland aimed at tackling the root causes of offending behaviour and reducing harmful behaviour within families and the community. A Problem-Solving Justice Five-Year Strategic Plan was developed during 2020 to enable evidence-based decisions about the future of pilot projects and to facilitate a strategic and structured roll-out. Building on this work a new Adult Restorative Justice Strategy is being developed by the Department of Justice.
Chapter 2 – Breaking drug supply chains
Our vision is to level up our neighbourhoods by ridding them of drugs, making them safe and secure places and enabling all areas to prosper and grow. To achieve this, we will prioritise cutting off the drug supply that is causing the most harm. Given the scale of the threat and the rise of the violent county lines distribution model, breaking drug supply chains and ‘rolling up’ county lines is a priority for the whole of government, the police and all law enforcement partners.
We are committed to bring the full force of government to bear in a relentless and uncompromising attack on every phase of the drugs supply chain. This means using all of our law enforcement capability, diplomatic, programmatic and intelligence community levers. Our innovative supply attack plan will target the most violent and exploitative elements of the drugs trade, boost the police and law enforcement response and provide a shared, end-to-end strategic approach to drugs across the system.
Over the next 10 years, we will make all parts of the UK significantly harder places for organised crime groups (OCGs) to operate in. We will deliver the Prime Minister’s goal of ‘rolling up’ the county lines model, protecting the most vulnerable from exploitation and trafficking by criminal gangs and reducing associated levels of violence and homicide. We will also focus on security to disrupt the supply of drugs into the prison estate. Our prisons provide tough punishment for organised criminals. They must be a place where prisoners can never participate in drug-related crime.
What is the problem?
The global availability of drugs is higher than ever before, fuelling rises in the purity of heroin and crack cocaine [footnote 23]. The UK is now Europe’s largest heroin market and a target for international drug trafficking gangs. Concerted action to combat this abhorrent trade is more critical than ever.
As the threat from drugs has continued to evolve, so has the diversification and adaptability of OCGs, with the emergence of synthetic substances and a rise in the prevalence of online markets. OCGs seek to take advantage of our border and operate a wholesale ‘middle market’ distributing drugs across the country. The organised criminality behind the drugs trade makes our neighbourhoods less safe: heroin and crack cocaine addiction is linked to almost half of all acquisitive crime, including burglary, robbery and theft [footnote 24], and drugs contribute to almost half of all homicides [footnote 25].
Growth in drug supply has also driven an increase in county lines, the most violent and exploitative distribution model yet seen. Gangs criminally exploit and traffic children and vulnerable young people, coercing them into becoming ‘runners’ to transport Class A drugs and money around the country. These children and young people often struggle to get out as a result of drug debt and threats against themselves and their families. ‘Cuckooing’ is a tactic where drug dealers use violence and coercion to occupy a property and use it as a base for dealing. Dealers often target those who are the most vulnerable, including those experiencing drug addiction, mental ill health or learning disabilities.
The scourge of the drugs market continues into our prison system, where illicit drugs are far too readily available. Serious and organised crime dominates the drug economy in prisons and is part of a web which includes drug supply outside. There are several enablers of this, including the illicit use of mobile phones within prisons to co-ordinate crime and fuel high levels of violence as offenders vie for control of the internal market and enforce drug debts.
How this strategy will change things for the better
We are already delivering real impact. In the past two years our County Lines Programme has closed down more than 1,500 deal lines, made over 7,400 arrests, seized over £4 million in cash as well as significant quantities of drugs, and safeguarded more than 4,000 vulnerable people. The latest National County Lines Co-ordination Centre (NCLCC) assessment shows a reduction in the total number of potentially active lines per month, with numbers across England and Wales reported to have fallen from between 800 and 1,100 in 2019-20 to 600 in 2020-21 [footnote 26].
But we know that OCGs are reactive and resilient and will continue to adapt how they supply drugs. That is why, supported by £300 million of investment over three years, we will mobilise robust and innovative supply interventions through an ‘end-to-end’ plan which includes sustained investment across the supply chain. Across all pillars we will continue to build our evidence base to determine what works best in disrupting the drug supply chain and trial innovative interventions, as set out below.
Break the supply chain summary plan
| Priority | Method |
|---|---|
| Restricting upstream flow | – extending the NCA’s Near Europe Taskforce which focuses on the response upstream – supporting the NCA’s International Liaison Officer network and Border Force international work to stop drugs from coming to the UK in the first place – responding to the changed situation in Afghanistan by pivoting operational capabilities along this drug supply route and continuing to disrupt key actors |
| Securing the border | – trialling innovative approaches, led by the NCA and Border Force, to secure the border and tackle drug supply |
| Targeting the‘middle market’ | – making sure our dedicated organised crime partnerships continue to receive support and investment, targeting the disruptive ‘middle market’ – leveraging the recruitment of 20,000 more police officers to grow Regional Organised Crime Units and London equivalents, allowing them to bear down on the enablers of drug supply, including illicit firearms and money laundering |
| Rolling up county lines | – strengthening our flagship County Lines Programme to tackle the most violent and exploitative distribution model yet seen |
| Tackling the retail market | – continuing Project ADDER for a further two years up until March 2025, trailblazing a whole system approach |
| Going after the money | – recruiting more financial investigators, strengthening the NCA’s National Economic Crime Centre and bolstering our engagement with international partners |
| Prison security | – utilising technology and skills to improve security and detection and rid our prisons of drugs |
By bearing down across the supply chain in this way, we will deliver significant progress, including:
- a reduction in drug-related crime and homicide
- over 2,000 more county lines closed and an increase in both drug trafficking convictions and the number of vulnerable children and adults safeguarded [footnote 27]
- 6,400 major and moderate disruptions against activities of organised criminals (an increase of 20%) [footnote 28]
- significantly increase our denial of criminal assets, taking cash, crypto-currency and other assets from the hands of criminals involved in drug trafficking and supply
- enhanced testing in prisons, to drive towards drug-free prisons
Rolling up the county lines model
We will dismantle the county line distribution model that is exploiting children and vulnerable adults and devastating our neighbourhoods. Building on the success of our recent investment we will move county lines from a low-risk, high-reward to a high-risk, high-consequence criminal activity, with continued disruption and arrests of the criminal gangs responsible, increased seizures of cash and drugs, and less harm done to children and vulnerable adults.
We will make up to £145 million of funding available for our ambitious County Lines Programme in the first three years alone, which will build on over £65m invested since 2019. This will include funding the NCLCC to provide strategic oversight for all county lines disruption activity, promote best practice among police forces, target the illicit finances associated with county lines and support innovative use of civil and criminal orders.
The programme will support a concentrated law enforcement response, focusing on key exporting forces and targeting the most harmful gangs and lines, including those running in and out of Scotland and Wales. We have established dedicated county lines taskforces in the three largest exporter areas – London, Merseyside and the West Midlands – piloting a range of operational tactics to establish the best methods for long term disruption. We are also funding specific operations with local forces to identify and tackle county lines from importing areas, focusing on those causing the most harm to their local area.
We will grip the transport network through the extension of a dedicated British Transport Police (BTP) County Lines Taskforce. This will make the rail network a high risk for county lines distribution and we are also targeting the road network through investment in crucial automatic number plate recognition (ANPR) technology to maximise the use of analytical capability and enable better identification of vehicles involved.
County lines activity online will be disrupted, focusing on investigation, disruption and enforcement work against specific gang targets. Funding for specialist support for criminally exploited and trafficked young people and their families will help them to exit their involvement from county lines activity and break their association with criminal gangs.
Case study: Co-ordinated national law enforcement protects the most vulnerable in society from county lines
BTP assisted the Metropolitan Police Service with a missing person inquiry involving a child, who was thought to have left London and forced to work for a county lines gang to clear their debt. The young person was already the subject of a modern slavery investigation in ‘County A’ having previously been located at a ‘cuckooed address’ [footnote 29].
As the young person was believed to be travelling by train, BTP’s County Lines Taskforce conducted enquiries and identified that the young person had travelled to ‘County B’ and was being held at a local Class A drug user’s address. A search of the address by BTP found not only the child, but also a significant quantity of Class A drugs and a mobile phone deemed to be operating a county line.
BTP’s investigation resulted in three people being arrested for human trafficking and drug supply, supported by a statement from the young person about their experience and exploitation. The child has since been actively engaged with social services and is no longer involved in county lines. The registered occupier of the ‘cuckooed’ address in ‘County B’ was also safeguarded as a vulnerable adult.
Restricting upstream flow
Addressing international drug trafficking requires a comprehensive approach. Alongside a strong law enforcement response, we must also leverage our diplomatic and overseas policy networks to unlock political support from other governments and build our partners’ capacity to address the critical enablers of drug supply such as corruption and illicit finance. A concerted focus on prevention overseas is key to managing potential risks emanating from law enforcement responses.
We are working with international partners to leave no safe spaces for criminals and their associates. The National Crime Agency (NCA)’s international liaison officer network directly targets the highest harm offenders overseas to prevent drugs from coming to the UK. They work with Border Force to build and strengthen enforcement capacity in countries that export drugs and those through which drugs travel in transit. This upstream operational work by the NCA has so far this year resulted in the seizure of over 123 tonnes of cocaine. In addition to at-source and transit activity, Europe is a critical nexus point for drugs bound for the UK. In 2021, we established the Near Europe Taskforce, a team of NCA and Border Force officers focusing on upstream supply, port security, corruption, and intelligence and information sharing to identify and disrupt offenders, making it more difficult for OCGs to transport drugs to the UK. This collaborative effort has led to the seizure of almost five tonnes of Class A drugs so far this year.
We will strengthen our upstream response and reinforce the work of our overseas networks. We will deploy more international liaison officers in significant source and transit countries, enabling us to work more widely with key partners to disrupt and prosecute those who supply illegal drugs. The changing situation in Afghanistan – the source of 95% of heroin in the UK – has highlighted the importance of remaining agile against emerging threats upstream [footnote 30]. We have pivoted our focus to prioritise sustained investment in multi-disciplinary capabilities along key narcotics supply routes from the region to the UK.
We will address the underlying drivers and enablers of drug production and trafficking upstream including strengthening our prevention work and increasing the resilience of people to avoid a life of crime by improving socio-economic conditions and local service delivery.
Securing the border
Strengthening the UK border is key to intervening against drug supply. Over time, we have experienced increasingly sophisticated criminal methodologies that seek to exploit border vulnerabilities and bring social and economic disruption to the UK. We have pivoted quickly to meet these new threats and challenges.
Law enforcement agencies including the NCA and Border Force are working closely together to share intelligence and increase our ability to detect and disrupt OCGs trafficking illegal drugs through the border. This includes the corruption of those in trusted positions in ports who facilitate drug trafficking. This work is already seeing results. Last year, Border Force seized approximately four tonnes of cocaine and two tonnes of heroin [footnote 31].
We know that drugs can enter the country in a variety of ways such as being hidden in freight containers, carried by individuals on passenger transportation, or via post and parcels. We are working to develop a more comprehensive understanding of the risks that these modes present, including investing in systematic risk testing and analysis to direct workforce and assets to the right threats. Investment in data analytics and intelligence capabilities will enhance our enforcement activity to counter threats to the UK border more effectively. We are developing Cerberus, a new multi-mode data gathering, analysis and targeting system, which will contain all relevant border data by 2026, allowing us to use sophisticated analytics to build a rich intelligence picture of the traffic crossing the border.
Our ambition is to implement further targeted activity, continuing to trial innovative approaches which use the full range of law enforcement tactics. We will continue to bring agencies together to pool intelligence on drugs crossing our border, addressing vulnerabilities and creating a ‘ring of steel’ around key ports.
Case study: UK Government approach leads to the largest ever cocaine seizure in Montenegro
In June 2021, Border Force signed a memorandum of understanding with Montenegro to prevent drugs and other illicit goods at the border and in transit to Europe and the UK. This led to the provision of drug detection technology and training of Montenegrin customs and police funded by our Official Development Assistance and Conflict Stability and Security Fund programmes.
The NCA built the capacity of the investigative team by providing vehicles, IT surveillance equipment and training and developed intelligence sharing methods. In parallel, diplomatic lobbying resulted in Montenegro’s commitment to amend legislation to allow increased surveillance measures against international OCGs.
Using UK intelligence, Montenegro’s authorities made their largest cocaine seizure of 1.4 tonnes in 2021. This seizure is significantly attributed to the Border Force-led capacity building support and the joined-up approach from partners across government.
Targeting the ‘middle market’
OCGs operate a wholesale ‘middle market’ between the large-scale importation of drugs through the border and dealing that takes place in our neighbourhoods. Criminals operate across multiple local areas and may be connected to regional, national and international networks involved in trafficking, money laundering and wider organised crime. We are targeting drug supply and distribution – from highly sophisticated OCGs involved in large-scale importation, through to middle tier offenders and drug supply networks in our neighbourhoods – at every tier of policing.
Regional Organised Crime Units (ROCUs) play a pivotal role in tackling the ‘middle market’ threat as the principal interface between the NCA and policing in England and Wales, providing expertise, specialist technology and investigative capability. They are key in countering the harm from the ‘middle market’ in respect of enforcement, intelligence development and confiscating or denying access to assets. In the last 12 months, we estimate this joint working has removed three tonnes of Class A and B drugs.
The NCA also targets those criminals who operate at the highest levels of offending and present the highest risk. The NCA and police forces work closely, sharing intelligence and pooling resources to target the highest harm organisations through ROCUs and organised crime partnerships (OCPs). OCPs have been established in London, Merseyside and Scotland to stop the flow of firearms and drugs into criminal markets and county lines networks. In April 2021, Class A drugs with a street-value of more than £10 million were seized in a single joint operation led by the London OCP. At a local level, some forces such as the Metropolitan Police Service deploy specialist crime proactive teams, economic crime teams and reactive teams daily, successfully disrupting OCG activity and seizing significant quantities of drugs.
We will build on these successful partnerships and encourage further collaboration across all law enforcement partners to investigate and disrupt high value targets. It is also critical that we support the improvement and development of cutting-edge tools and techniques to allow law enforcement and national security partners to keep pace with the rapidly changing ways that criminals can communicate with each other.
We will prioritise an allocation from the recruitment of 20,000 more police officers to grow capacity and capability in all ROCUs and London equivalents to confront ‘middle market’ drug supply. Investment in officers will support regional tier policing to bear down on the enablers of drug supply, including illicit firearms and money laundering.
Going after the money
We want to make the UK the hardest place to launder cash and remove the profitability of the drugs market. To do this, we must improve our understanding of how best to restrict OCGs’ ability to launder their proceeds of crime and increase seizures of cash and assets.
In every tier of policing, reducing the profitability of the drugs trade remains a priority and we are seeing success across the system. New pilot programmes are being trialled, in collaboration with the NCA and other law enforcement agencies, to better understand the methodologies undertaken by OCGs to launder illicit finances in relation to drugs.
The proceeds of the drugs trade represent a significant proportion of criminal cash circulating within the UK. The National Economic Crime Centre’s Project PLUTUS aims to make it harder for criminals in the UK to launder the proceeds of their crime by adding friction and cost to the laundering process. The NECC brings together a cross-government, law enforcement and financial sector response with objectives including making the UK a harder place for criminals to launder cash and deterring the use of criminal proceeds, such as those from the supply of illicit drugs. We are also strengthening the capability and capacity of the NCA and policing, making sure that they have the data, technology, and investigative tools they need to target these criminals, both domestic and international.
ROCUs and the NCA played a leading role in co-ordinating the policing response to Operation VENETIC, removing harmful criminals from our streets and seizing drugs, firearms, criminal assets and cash. Between April 2020 and July 2021, the ROCUs alone were responsible for seizures of £33.6 million of cash and over 1.5 tonnes of cocaine and heroin. We will also invest in cutting-edge technical capability to support regional tier policing to confront drugs supply and seize the profits from drugs. To make sure that there is no easy money in crime, we are growing regional policing’s response to high-harm fraud, including the laundering of drug profits, by establishing a dedicated network of 30 regional fraud investigators this year.
Additionally, we have published our three-year Economic Crime Plan to strengthen the UK’s resilience to illicit finance and cement its position as a world-leader in the global fight against economic crime [footnote 32].
UK criminals involved in drug trafficking are often incentivised to engage in criminality through the ease of money laundering to overseas jurisdictions where they can enjoy their profits, further fuelling harm to UK citizens. That is why, as well as going after the money at home, we will also adopt a broader international approach. We will enhance progress to date and bolster our engagement with international partners, increase the number of trained financial investigators, and strengthen the NECC.
Tackling the retail market
The impact of drugs is felt in our neighbourhoods and it is critical that we continue to disrupt supply chains at a local and regional level. Street-level retail supply is the point where drugs are mostly sold for personal use and the online supply of drugs to individual users has become increasingly prominent. It is the responsibility of local police forces to address this and we must make sure that this is a top priority for our police forces.
Individual police forces in England and Wales are operationally independent, with the National Police Chiefs Council providing co-ordination to ensure the consistent enforcement of drugs policy and supporting forces to work together, and with other law enforcement partners, to confront the drugs threat.
We have already invested £59 million in Project ADDER, a programme that demonstrates the benefit of a whole-system approach to addressing drug addiction in some of the hardest hit local authorities across England and Wales. Over the next three years, we will continue our investment and strengthen our evidence base through evaluation of the programme. This learning will be vital in informing our future strategic direction.
To enhance this response, we will look at opportunities to incentivise the whole policing system to focus on drugs, including the National Policing Framework, the Strategic Policing Requirement, engagement with police and crime commissioners, the inspection framework and training and professional practice.
The government has also published its draft Online Safety Bill – a world-leading and much-needed law which will make the UK the safest place to be online, with the sale of illegal drugs being a priority harm that it aims to address [footnote 33].
Prison security
We have already invested significantly in the security of our prisons in England and Wales. The government’s £100 million investment into the Security Investment Programme, funded innovative multi-agency approaches to better tackle high-harm crime, along with new equipment and technologies in parts of the prison estate. This will better disrupt the supply of illicit items, including drugs, into prison and prevent serious organised criminals from running their networks while in custody.
This investment saw 74 X-ray body scanners rolled out across the entire male closed estate, enhanced gate security, mimicking airport screening, with metal detecting portals, increased use of drug detection dogs and other technology installed at our highest priority sites. All new build prisons will be equipped with this enhanced security and X-ray body scanners as standard. To build on these gains, police forces, prisons, probation and partners will strengthen collaboration to better identify and stop organised crime and career criminals from continuing to offend and running their drug networks in prisons. These criminals disrupt the delivery of safe, decent and secure regimes and cause harm in the community.
UK-wide collaboration
Border Force and the NCA work to combat drug supply across the UK. For example, the NCA have established an organised crime partnership with Police Scotland. The partnership aims to confront a range of serious and organised crime threats, including drugs and firearms supply into Scotland. In Northern Ireland the NCA is also a key partner in the Organised Crime Task Force, Paramilitary Crime Task Force and Joint Agency Task Force structures.
OCGs are misusing pill press machinery to manufacture harmful drugs such as ‘street’ benzodiazepines. These are being sold across the UK and causing significant harm, particularly in Scotland where they were implicated in 66% of drug-related deaths in 2020 [footnote 34]. The government is working with the NCA and partners in Scotland to increase our understanding of the scale of the threat and explore ways to address the supply of these pills.
Thanks to engagement with the NCLCC and the County Lines Programme pilot forces (West Midlands, Merseyside and Metropolitan Police), we are aware of county lines running to and from Scotland and have conducted a number of joint operations with Police Scotland. Forces will continue to work together to remove this threat.
North Wales is one of the key importing areas for Merseyside county lines networks, with Class A drugs imported via road and rail. Merseyside Police is working closely with North Wales Police as part of our County Lines Programme to close down the lines and prevent the gangs responsible from causing further harm.
Chapter 3 – Delivering a world-class treatment and recovery system
The foundations of this chapter are based on Dame Carol Black’s landmark independent review of drugs. Our vision is for an ambitious 10-year transformation programme which shows our commitment to delivering the key recommendations made in her review and going further. Tough enforcement action must be coupled with a high-quality treatment and recovery system to break the cycle of addiction.
Within a decade, we will have a world-class drug and alcohol treatment and recovery system across England, delivered via a highly trained and motivated workforce offering a full range of evidence-based interventions. This will be available to anyone experiencing substance addiction, from entrenched heroin users and people struggling with cocaine, cannabis, and alcohol, to young people using psychoactive substances.
We will create a system where no one falls through the gaps, where there is no stigma attached to addiction and it is treated as a chronic health condition, and where people who need it are provided with long-term support. It will be a system where individuals and families experience the full positive impact of this transformation programme, and where those local areas with the highest need receive the most support. This system will promote equality and meet the needs of all communities, particularly, those who have often not received an effective service in the past, including people from ethnic minority backgrounds and women.
By putting the individual at the centre of everything we do, and by underpinning services with extensive and robust evidence, we can save lives, reduce harm and crime, and stop the ‘revolving door’ in and out of prison. While many aspects of treatment and recovery are devolved, we are committed to working with the devolved administrations to learn from each other on shared challenges.
What is the problem?
Dame Carol Black’s independent review of drugs set out the scale of the challenge for the treatment and recovery system. In summary, the review found that:
- an estimated 300,000 people in England use opiates and or crack cocaine
- disinvestment in adult treatment with an even greater reduction in funding for young people’s specialist substance misuse services and a growing level of unmet need
- there is a lack of oversight and accountability at a local and national level with the re-introduction of incentives and levers, alongside locally held joint responsibility and accountability, needed to regenerate and revitalise the system
- prolonged shortage of funding has depleted the workforce resulting in a loss of skills, expertise and capacity from this sector
- caseloads have grown too high reducing the quality of treatment
- there is a lack of specialist services, including inpatient detoxification and residential rehabilitation
- recovery support has ben underfunded, including housing and employment support, and recovery communities
- there are high levels of physical and mental health need, without sufficient focus on drugs and alcohol within NHS and mental health services or within the workforce, and links with drug treatment are far too weak
- more than a third of people in prison are there due to crimes relating to drug use
- too few offenders are in treatment to make lasting change to their behaviour
This is a stark set of findings and since the review was published deaths related to drug misuse in England and Wales have increased to 2,966 in 2020, the highest number since records began in 1993 [footnote 35].
How this strategy will change things for the better
The government is committed to transforming the lives of those affected by drug addiction. An additional £780 million will fund the first three years of an ambitious, decade-long transformation of drug treatment and wider recovery support in England [footnote 36]. This marks the largest ever increase in treatment and recovery funding, taking the total treatment and recovery spend to more than £2.8 billion. The new investment will be ringfenced so that the money is spent only on this agenda.
We will deliver the key recommendations in part two of Dame Carol Black’s review, using a whole system approach, and going further with a 10-year commitment. We will invest in expanding treatment capacity, re-building the workforce, strengthening skills and increasing our mix of professionals. We will empower local leaders to deliver on this commitment, while ensuring that they are held accountable for this spend and for putting in place strong partnerships at the local level between education providers, local authorities, the NHS and criminal justice agencies.
By investing across a range of joined-up services, we can deliver life-saving support and improve the safety and productivity of local areas by reducing the harms that drug addiction can cause and maximising long-term recovery. This will provide local areas with effective substance misuse treatment, mental and physical healthcare, housing and employment. This includes clear referral pathways for offenders into treatment, reducing the risk of reoffending, and we will see a steep reduction in acquisitive crime (such as burglary, robbery and theft) and drug-related violence.
We will address mental and physical health system gaps by working with the NHS to introduce effective pathways and better integration, including improving the skills of the workforce in relation to drugs and alcohol. We will also extend effective joint commissioning arrangements to serve populations in and out of drug and alcohol treatment services for those who suffer from both mental health conditions and drug and alcohol use.
We will start this transformation by prioritising the local areas that have the highest need for drug treatment and recovery, with full national coverage across England by the end of 2024/25. This will significantly contribute towards the government’s commitment to levelling up.
We will carefully monitor progress to make sure that this investment delivers significant and tangible improvements. Success will be measured against national and local outcomes frameworks to achieve the following by the end of 2024/25:
- nearly 1,000 deaths prevented, and lives saved
- a phased expansion to deliver at least 54,500 new high-quality drug and alcohol treatment places, a 19% increase on current numbers
- treatment contributing to around 740,000 crimes prevented, of which 140,000 are neighbourhood crimes such as burglary, robbery and theft
- 21,000 new treatment places for opiate and crack users, 53% of opiate and crack users in treatment
- 30,000 new treatment places for non-opiate users, including a further 5,000 more young people in treatment
- at least 7,500 more treatment places for people who are either rough sleeping or at immediate risk of rough sleeping – a 33% increase on the current numbers
- a treatment place for every offender with an addiction
- 24,000 more people in long-term recovery from substance dependency
- increased referrals from police, courts and probation into drug treatment
- more people recovering from addiction in sustained employment
- more people recovering from addiction in stable and secure housing
Achieving all that means our NHS will reduce unnecessary burden and be able to redirect resources into other areas of need. Our prisons will not be a revolving door for those whose offending is linked to addiction. Our neighbourhoods will benefit from reduced crime and rough sleeping and more children will be protected from the harms of drugs in their families or neighbourhoods. Our economy will benefit from substantial savings to policing, health and justice and an increased workforce.
Increased accountability and transparency
We will improve consistency and transparency of service delivery in England, so that people everywhere can expect the same quality of service, and local areas can be held to account at a national level.
- By March 2022 we will have developed a new national commissioning quality standard to increase transparency, ensure consistency, promote effective joint-working, enhance improvement support and accountability.
- The national commissioning quality standard will be developed with local areas, including the Local Government Association (LGA) and the Association of Directors of Public Health (ADPH), and will set out the full range of treatment and recovery interventions that local areas should provide for their population based on an assessment of need, including having due regard to the public sector equality duty and meeting the needs of different demographics. We will share learning from the development and implementation of the commissioning quality standard with colleagues across the UK.
- Starting this year, DHSC has made it a condition of grant funding that a local authority must “have regard to the need to improve the take up of, and outcomes from, its drug and alcohol misuse treatment services, based on an assessment of local need and a plan which has been developed with local health and criminal justice partners”. We will ensure that local areas maintain their existing investment in drug and alcohol treatment in 2022/23 and beyond.
- The Office for Health Improvement and Disparities (OHID) will lead on monitoring local areas and, from 2022/23, this will include an annual publication of key national and local indicators to show progress.
Treatment
We will invest £533 million over three years to rebuild local authority commissioned substance misuse treatment services in England. This is additional to the current annual public health grant spend (£670 million in 2019/20), which we expect local authorities will continue to invest in drug and alcohol services going forward.
The £533 million will be broken down into the following:
| Funding | 2022/23 | 2023/24 | 2024/25 | 3-year total |
|---|---|---|---|---|
| Current additional funding | £80m | £80m | £80m | £240m |
| Place-based additional funding | £20m | £81m | £192m | £293m |
| Total above existing spend | £100m | £161m | £272m | £533m |
Continuation of additional funding made available in 2021/22
In 2021/22, £80 million (in addition to the existing public health grant) was made available to enhance drug treatment in England. This has delivered a wide range of successful interventions that reduce drug-related death and improve access to treatment for offenders. All local authorities will continue to get at least this level of investment over the next three-years.
This will enable them to invest in a wide range of evidence-based interventions to meet the needs of their local population, focusing on reducing drug-related death rates and bringing more offenders into treatment. This will also support the commissioning of inpatient detoxification services and increase treatment capacity for those with entrenched use and complex needs.
Place-based additional funding
Over the next three years, £293 million of additional funding will be made available to reduce harm and improve recovery rates significantly. This will implement all of the key recommendations made by Dame Carol Black, including an increase in treatment quality and capacity, strengthening the skills and professional mix of the workforce, making sure that a full range of treatment and harm reduction interventions are available and investing in recovery communities.
All local authorities in England will receive enhanced treatment funding over the course of the next three years. We will use a targeted approach, prioritising those places experiencing the highest harm (rate of drug deaths, deprivation, opiate and crack cocaine prevalence, and crime), learning and evaluating as we go. In 2022/23, we will invest in the 50 local areas with the highest needs, followed by the next 50 in 2023/24, and the final 50 in 2024/25, leading to England-wide coverage.
Levelling up is at the core of this approach. The level of deprivation in the local authorities with higher need is twice that of those in those with lower levels of need, and there is a strong correlation with local authorities in the North East and Yorkshire. Using this approach, just under half of opiate and crack cocaine users and half of offenders whose crimes are drug-related will be offered support in 2022/23.
We will construct grant agreements and reporting mechanisms to set the areas of spend for which the money is being allocated and safeguard existing spend on substance misuse services through the public health grant. We will support local areas to ensure that the additional funding means a full range of evidence-based interventions are available in every area and that the system is responding to new and promising innovations, such as forms of long-acting buprenorphine. We will also consider how incentives can be used to support the delivery of the government’s priorities, to monitor and evaluate performance and to include a claw back mechanism should money not be spent for the purposes for which it has been provided.
The following measures will ensure that this additional funding is used effectively.
- We will support local areas to expand and improve the quality of a full range of evidence-based harm reduction and treatment interventions. Both the NHS and third sector providers will have vital roles in this. This will include interventions to reduce harm and save lives, such as the overdose antidote naloxone, and needle and syringe programmes; effective talking therapies or psychosocial interventions, to support people to understand their addiction, make changes and develop coping strategies; and the full range of medicines to reduce harm and support detoxification including new medicines, such as long-acting buprenorphine.
- We will work with local authorities and stakeholders, including the Local Government Association (LGA) and the ADPH to develop and implement a commissioning quality standard to support transparency and accountability between partners and government. We will offer improvement support including sector-led improvement.
- We will develop and implement mechanisms to make sure that there is adequate provision of inpatient detoxification and residential rehabilitation in all areas of the country.
- We will offer improvement support to local authorities, working with the LGA, focussing on areas with poorer outcomes, to make sure that there is the capacity and capability to deliver the transformation needed.
- We will provide data, guidance, and support to local areas to fully understand and meet the needs of underserved groups and people with protected characteristics, including women and people from ethnic minority backgrounds.
- Support substance misuse commissioners and sexual health commissioners to work together to improve pathways between services for those who use drugs in a ‘chemsex’ context. This will include a review of the current model sexual health service specification as well as consideration for the needs of this group in the substance misuse commissioning quality standards and the workforce strategy.
Young people’s treatment and support for families
Young people who have drug problems often have complex needs. This often involves poor mental health and self-harm, and sometimes experience of criminal or sexual exploitation. These young people need a combination of specialist treatment and wider health and social care services. Services need to be trauma-informed and treatment should be family-based if necessary, particularly for those whose parents are themselves dependent on drugs or alcohol.
Addiction also has a devastating impact on families. Families can support and aid recovery, but they also have their own support needs. Specific support is required for families with parental substance misuse treatment needs which must be co-ordinated at a local level.
Over the next three years we will make sure that:
- 50% more young people receive specialist substance misuse interventions, preventing longer term use into adulthood
- outcomes frameworks, commissioning quality standards and workforce development initiatives consider the needs of families and young people and support local areas to assess and meet their needs effectively
Strengthening the skills and the professional mix of the workforce
A strategy focused on retention and recruitment of a high-quality drug treatment workforce will be key to attracting the best people into the sector to make it their career. We need to rebuild the sector’s health professional workforce (including psychiatrists, doctors, nurses and psychologists) and improve the level of skill and training among drug workers and peer recovery workers, so that they are all well equipped to deliver the psychosocial and health interventions that drug users in treatment require to succeed. This workforce will also be better able to address the trauma and mental health problems which can underpin a lot of drug addiction, and will be agile in responding to the needs of different populations, including women, people who are LGBT, and people from ethnic minority backgrounds.
Staff will have lower caseloads and the skill to deliver more evidence-based psychological interventions. This will improve recovery rates for all people in drug treatment but will be particularly valuable for non-opiate users and recently initiated heroin users.
By the end of 2024/25, we will make funding available for:
- 800 more medical, mental health and other professionals
- 950 additional drug and alcohol and criminal justice workers
- adequate commissioning and co-ordinator capacity in every local authority
Further funding and support will be provided by DHSC to:
- work with Health Education England to implement a comprehensive strategy to expand the workforce through effective recruitment and retention
- work with Health Education England to define and improve the training and skills of all sections of the drug treatment workforce, including registered health professionals, drug and alcohol workers and peer supporters
- engage collaboratively with the wider Mental Health Workforce Strategy which includes specialist training for, and accreditation of, frontline staff working with people with co-occurring mental health and substance misuse issues
- work with the Royal Colleges and groups of professionals, peer workers, service providers and service users to create a Centre for Addiction for everyone working within substance misuse services
- develop guidance and relevant standards to support a reduction in case load sizes to enable staff to deliver high quality interventions and pursue career and professional development
Better integrated services
People with drug addiction often have physical and mental health needs which must be met to enable a successful outcome from treatment. Mental health problems and trauma are often central to an individual’s dependency on drugs and alcohol, and all too often people fall through the gap between services. We will transform the system so that providing trauma informed care becomes the norm, and complex needs (such as homelessness) are recognised and responded to. We will:
- work with NHS England to explore opportunities for better commissioning to make sure that there is locally joined-up service provision between specialist mental health services and substance misuse services for people with co-occurring issues including those experiencing rough sleeping
- make sure the next phase of the Integrated Care System development includes leadership on drugs and alcohol to integrate physical and mental health care with substance misuse services
- build on learning from the Changing Futures Programme to improve access to treatment and support for adults experiencing multiple disadvantage – including combinations of homelessness, addiction, mental ill health, domestic abuse and contact with the criminal justice system [footnote 37]
Recovery
Promoting recovery from drug addiction is a key aspect of our approach. There is significant investment underpinning the strategy which includes funding for accommodation and employment support, which will be rolled out with our the investment in treatment. Recovery is a process that often takes time to achieve, and effort to maintain – people need something meaningful to do, somewhere safe to live and a support system in the community.
Improved access to accommodation
Homelessness and rough sleeping can be both a cause and a consequence of substance use. A rough sleeping questionnaire carried out in 2020 found that at least 43% of respondents who had a drug need, developed their dependency prior to first sleeping rough, and 17% afterwards [footnote 38]. Alongside our ambitious commitment to end rough sleeping, we will work to break the cycle of homelessness and addiction across England. We know that having a secure home is key to recovery and that treatment is less likely to be effective without this, with a much higher chance of relapse. We will extend our work to provide specialist treatment and recovery services to people sleeping rough and offer help to people whose ability to engage in treatment is hampered by their need for support with their housing.
To do this we will continue investment in the rough sleeping drug and alcohol treatment grant (RSDATG) to improve services for people who sleep rough or are at risk of sleeping rough, building on substantial funding invested in 2020/21 and 2021/22, including a further investment of at least £15 million to expand this over the next three -years. RSDATG will provide at least 7,500 more people who are either rough sleeping or at immediate risk of rough sleeping with treatment, a 33% increase on the current numbers who are experiencing housing problems in treatment [footnote 39].
We will invest £53 million over the next three years to fund a menu of housing support options which will improve the recovery outcomes for people in treatment and reduce the flow of people into homelessness and rough sleeping – including funding housing support workers to work within treatment services. Alongside this investment, we will build the evidence base on the housing related need for people dependent on drugs and alcohol and the most effective interventions.
Improved employment opportunities
Dame Carol Black’s review highlighted that, alongside treatment, meaningful activity makes an important contribution to sustaining recovery from drug use. There is considerable evidence that employment can improve treatment outcomes, reduce the frequency and severity of relapse, and reduce re-presentations to services [footnote 40].
To support recovery and the movement from treatment into work, we will invest a further £21 million to roll out Individual Placement and Support (IPS) for those in treatment for drug or alcohol use across England by the end of 2024/25. This brings the total funding for this new programme to over £39 million across the next three years. Commissioned by DWP and managed by OHID, IPS offers intensive, individually tailored support to help individuals in treatment find the right job, with in-work support for the employee and employer to ensure that work is sustained. Previously trialled in seven local authority areas, IPS is already being expanded to cover 46 local authority areas in 2021/22. This additional investment will secure full coverage across England by the end of 2024/25.
We will also provide support which enables individuals to disclose their substance use safely, move into recovery and move closer to work. This includes investing over £8 million in support including a new peer mentoring programme in England, Wales and Scotland, where mentors will work in partnership with Jobcentre Plus and treatment staff [footnote 41]. They will and use their lived experience of substance use, treatment and recovery to act as advocates and visible symbols of recovery to support people into employment.
Case study: Individual Placement and Support for people with a drug addiction
OC accessed IPS alongside community drug and alcohol treatment. Her use of cocaine had brought her into contact with criminal gangs, and she was coerced into prostitution, becoming dependent on a gang for access to drugs.
She moved away from the area where the gang operated but she had little confidence and had regarded paid employment as unrealistic. Her IPS specialist worked with her to build her up and allow her to see her strengths. They made sure she understood how part-time work alongside Universal Credit would be a viable option.
The IPS specialist brokered an interview with a local business. OC took the lead throughout the interview, with the IPS specialist assisting by suggesting areas where it would be helpful to say more. OC was offered the job, with a role being ‘carved’ that fitted the employer’s needs and her circumstances.
On starting work, the IPS specialist provided OC with the most practical support. Despite living in the area for several years, she had never been to the neighbouring town where her new job was based. The IPS specialist accompanied her to work while OC became more confident in making the journey.
Having started working only a few hours per week, OC is successful in this job and has gradually increased her hours to full time and has remained substance-free.
Communities of recovery
Social support and networks help people to recover. Local authorities in England will be expected to use this additional investment to make sure that that peer-based recovery support services and communities of recovery are linked to and embedded in every drug treatment system.
Mutual aid organisations such Al-Anon, Alcoholics Anonymous, Cocaine Anonymous, Families Anonymous, Narcotics Anonymous and SMART Recovery also have a vital role to play and can support the drug and alcohol treatment system, helping people to achieve and maintain recovery. We will make sure that treatment services support people to use mutual aid wherever possible.
Recovery networks are highly valued by people who use them and can significantly enhance the work of treatment services, harnessing the commitment and energy of people with lived experience. However, peer supporters should not be left to do the work of professionals without appropriate training, pay or support. To support this, we will develop standards and guidance for the recovery sector and local areas, working with the government’s Recovery Champion Dr Ed Day [footnote 42]. We will support local areas to involve people with lived experience of drug dependence as peer supporters and recovery coaches and, at a national level, encourage the development of a flexible and innovative network of recovery organisations.
Research
Despite the huge societal damage and cost of £19 billion a year caused by addiction to illegal drugs, there is limited clinical or public health innovation. Our Life Sciences Vision seeks to take a vaccines taskforce-type approach to complex health problems, bringing together the right partners with the right leadership to make rapid progress. There needs to be a sharp focus on what government, the NHS, local authorities, regulators, companies, medical research charities, academia and philanthropy must do to create the environment in which we can accelerate research breakthroughs in the UK, so patients and society receive a real benefit.
This new mission will be focused on addiction, one of the biggest health problems of our generation, and it will be delivered alongside the other missions on obesity, cancer, dementia and mental health that were announced in the Life Science Vision. This mission will help to create capacity to test and trial innovative new approaches in this area. Currently there is not a rich evidence base to underpin the development of new psychopharmaceuticals or novel digital therapeutics and technologies, nor is there much existing capability to draw on within academia and private companies. This mission, with a call for proposals, will seek to stimulate the creation of such evidence and collaboration, and understand the efficacy of technological interventions when paired with public health and clinical approaches. We will also explore funding mechanisms which will reward those who create innovations that address the problem.
Improving the criminal justice system response
Reducing crime and reoffending is a fundamental part of this strategy and the government’s levelling up agenda. There are high rates of drug addiction among offenders, and our ambition is to support them to become drug free. Treatment works to reduce reoffending so addressing drug dependency is crucial to preventing further crime [footnote 43]. From the moment that an offender comes into contact with the criminal justice system, we will be focused on their rehabilitation and recovery from drug misuse.
In addition to the investment in treatment and recovery outlined above, an additional £120 million for the MoJ over the next three years will be invested to make sure that offenders fully engage with recovery-focused treatment services, to complement the DHSC investment in England outlined earlier in this chapter, including increased provision of treatment for offenders in the community via HMPPS in Wales.
This includes mandatory and voluntary testing regimes in prison, support for prisoners to engage with community treatment ahead of their release and increasing the use of intensive drug rehabilitation requirements for those on community sentences. We will be learning from existing good practice, both in the UK and internationally. Our goal is to ensure that appropriate and high-quality treatment is available to all offenders with an addiction so that they can work towards drug-free living, and also to ensure that drug treatment, housing and employment support is available for every prisoner subject to probation supervision upon release.
Community sentences
We must focus on treatment whilst offenders are in the community, which is a genuine opportunity to support recovery from dependency while monitoring their compliance. Taking forward commitments made in the Beating Crime Plan, we will expand and improve the use of drug testing on arrest so that we are taking every chance to identify offenders who use drugs. This will enable us to make sure that they get directed to treatment and can turn away from a life of crime – for example, as a requirement of a community sentence. Police will pass on information from a positive drug test to NHS Liaison and Diversion services who work at police stations and courts to identify offenders with drug treatment and other needs such as poor mental health and refer them onwards to treatment. We are completely clear that crimes that meet the threshold for prison will be punished using custodial sentences; this is not an alternative but is a clear and effective plan for making sure treatment is required where needed for those who would be sentenced in the community as a proportionate sentence.
We want to see greater use of tough and effective community sentences with drug rehabilitation requirements, which require offenders to commit to treatment and regular drug testing, this includes the use of combined community sentences for those with a dual diagnosis of poor mental health. We are investing in additional specialist drug workers to work with police, courts and probation to assess offenders, and give sentencers confidence that they can make greater use of these kinds of sentences, because they will know that treatment will be available.
We are also piloting new problem-solving ‘substance misuse courts’ where the offender is seen regularly by the same judge who oversees their progress with treatment and other interventions, tailored to their needs [footnote 44]. The judge will be able to use a system of incentives and sanctions to encourage compliance, and – following legislative changes in the Police, Crime, Sentencing and Courts Bill – to impose new brief temporary custodial penalties for non-compliance [footnote 45].
Treatment in prison
We will focus on rehabilitation and recovery for all prisoners with a substance misuse problem from the day they arrive in custody. We must ensure that all prisoners make best use of their custodial sentence to make meaningful progress towards recovery.
To do this, all prisons must have a zero-tolerance approach to drugs, investing in security and intelligence to prevent their supply, and making sure that treatment is available to ensure prisoners can make lasting change to prevent them reoffending. All prisoners receive a comprehensive health screening within their first week to identify drug misuse and related health needs and agree a plan for recovery-focused treatment, tailored to the length of their sentence. Regular drug testing also enables us to respond quickly, punish and disrupt supply and identify drug misuse so that prisoners can be referred to treatment. From 2023, a new drug testing contract will facilitate testing for more and different types of drugs, including emerging and psychoactive substances, as well as testing for the abuse of prescribed medication.
Based on these personalised treatment plans, we will make sure that all prisoners can access high-quality treatment, which includes integrated mental health services where there is a dual diagnosis, that enables them to recover from their addiction as quickly as possible, in a meaningful and lasting way. The full range of evidence-based treatment interventions will be available to address the variety of drug needs presented by people in custody, including abstinence-based interventions to support recovery from drug dependency. We are exploring the benefit of making long-acting buprenorphine available to prisoners, to assess the impact on engagement with treatment, protection from overdose and relapse after release. We will also supply life-saving naloxone medication to staff in prisons and approved premises to administer to those who have suffered from an opiate overdose, preventing unnecessary deaths.
Tackling drug misuse in prison is wider than healthcare alone. Our aim is for all prisons to be recovery focused and training for prison officers as well as drug strategy leads in key prisons will support this. We will establish a key performance indicator to monitor all prisons’ progress in ensuring that recovery is the focus and share local good practice around the estate. HMP Holme House, the drug recovery prison, provides an innovative whole prison approach, with investment in security, a wide range of health services and support for prisoners to live drug free. Peer support and the wider environment is crucial, and we are expanding the use of recovery-focused areas in prisons, including incentivised substance-free living units. These are a ‘safe space’ away from drugs which support prisoners either to stop using drugs, or remain drug free, whilst undertaking voluntary drug testing and engaging with treatment. Early outcomes have identified a reduction in violence and substance misuse, and a link to increased employment opportunities on release.
Case study: HM Prison Holme House
The following is the testimony of an anonymous prisoner sentenced to custody at HMP Holme House following offending linked to their use of drugs.
“It is only since coming to this establishment I have been able to fully understand my actions and the reasons why I was once acting in the manor [sic] I did. When I have arrived at other prisons there has always been set people coming asking if I want to buy drugs or other items of contraband. This was just becoming a normality for me and for a very long time I was not straight headed and constantly in trouble for numerous different things. When I arrived here due to what security have done on the battle of drugs in prison, I have not only been able to focus on what’s really important but also it has helped me conquer a demon myself…The drug scene at HH is very minimum. I personally think this is how prisons should be, as it has benefited me in more ways than you can imagine. I have been able to mend two broken down relationships as a result of me realising that drugs was my downfall. I have learnt to accept, acknowledge and deal with my issues… Since my arrival here I have reached enhanced status, gained employment … and also had numerous positive ‘incentives and earned privileges’.”
Ensuring prisoners stay engaged in treatment after release
Preparation for release must begin as soon as a prisoner arrives in custody, with treatment plans focused on long-term recovery and continuity in the community. We plan to introduce a resettlement passport in England and Wales, which will bring together the key information and services to support prison leavers to address their drivers of repeat offending and ensure a smooth transition into the community. Drug misuse treatment services will form a key part of this, alongside wider resettlement services such as support to secure accommodation and employment.
We will also ensure continuity in the treatment provided in prison and in the community so that the transition is as seamless as possible. The additional funding provided in this year – £80 million for local authorities in England to invest in treatment – has delivered more specialist drug treatment staff to work with prisoners as they leave prison and help them to re-enter the community and start treatment. This includes people with lived experience, who are often more able to secure engagement in those vital first few days. As set out earlier in this chapter, this funding will continue for at least the next three years, with further investment and support to maximise recovery and prevent reoffending.
Making sure that offenders engage with treatment in the community is crucial to reducing the likelihood of them reoffending. The NHS RECONNECT service provides prisoners, including people with drug addiction and who also have other health needs, with a dedicated point of contact to make referrals and supports them to prepare for, and turn up to, appointments [footnote 46]. We are also investing to expand the use of video call technology, which is already in place in 86 prisons, enabling prisoners to have virtual initial meetings with community-based treatment providers before they are released, to build relationships and make it more likely that the prisoner will want to keep their appointments.
It is vital that the Probation Service works closely with healthcare services to make sure that offenders continue to access treatment. To support closer partnership working, OHID will publish an interactive single point of contact resource to facilitate communication between probation and treatment services in custody and the community. We have piloted the role of Health and Justice Partnership Co-ordinators who liaise between prisons, probation and treatment providers, to co-ordinate services more effectively. We will be expanding this role to cover all regions and share best practice more widely. This role will support new integrated care systems giving, for the first time, prisons and probation a seat at the table when commissioning discussions are taking place. Regional teams will support in sharing data on offenders needs to ensure that services meet their specific needs. This will make sure that treatment in prison and the community is joined up, so that offenders’ treatment plans are consistent.
Accommodation, education and employment are vital to both support recovery from drug misuse and reduce reoffending. Lack of somewhere to live when leaving prison is a major barrier to engaging in treatment. Without stable accommodation, prison leavers are almost 50% more likely to reoffend [footnote 47]. We need to make sure that prisoners receive the education and employment support they need to move out of prison into gainful employment, reducing the risk of reoffending. The interventions below will improve support across these vital areas.
-
Building on the investment in prison leaver rehabilitation announced earlier this year, £200 million a year will be invested by the end of 2024/25 to improve prison leavers’ access to accommodation, employment support and substance misuse treatment and to introduce further measures for early intervention to tackle youth offending.
-
As announced in the government’s Beating Crime Plan, a new Community Accommodation Service was launched in five probation areas in July 2021 to provide temporary housing and support.
-
Housing specialists in prisons will be recruited to help strengthen the partnership working between prisons, probation and local authorities to increase the likelihood of prison leavers securing accommodation in the community before they leave.
-
The government has increased the number of prison work coaches offering employment support. The new dedicated Universal Credit telephone line provides quick access for prison leavers to the benefit system, ensuring the financial stability needed to look for and stay in work. DWP is working with prisons to develop local agreements to enhance co-ordination and ensure continuity of support on release, building on the published National Partnership Agreement with MoJ.
UK-wide collaboration
The latest national clinical guidelines on treating drug misuse and dependence are UK-wide and were co-produced by clinical and other experts from across the UK.
The UK Government and the devolved administrations agreed that we need to review legislation to make naloxone (a drug that reverses the effects of an opioid overdose) more easily available to people who use drugs and are at-risk. A joint consultation on widening access to naloxone closed on 28 September 2021. The consultation was launched and developed with the UK Government and devolved administrations and future legislative changes would apply across the United Kingdom.
DHSC and OHID work with the devolved administrations in collating UK data on drug-related deaths, drug-related infectious diseases, and drug treatment, among other indicators for sharing with international agencies such as the United Nations Office on Drugs and Crime.
MoJ’s pilot problem-solving courts will align with the model currently operating in Scotland, with a primary focus on treatment, regular drug testing and court reviews of progress.
Chapter 4 – Achieving a generational shift in the demand for drugs
Our vision is to bring about a generational shift in the use of drugs across society so that, within 10 years, fewer people take drugs or feel drawn toward taking drugs, and today’s children and young people grow up in a safer and healthier environment. We will work with experts to encourage people to change their attitudes and behaviour by making sure that drug users are fully aware of the significant risks they are running, including the harms that their use is causing to themselves and others.
For those who nevertheless choose to continue with their drug use, there will be swift, certain and meaningful consequences which will be felt more strongly than today and will escalate for those who continue to offend. Drugs are harmful to society and no one is above the law. We will also step up activity aimed at protecting vulnerable children and young people so that they are less likely to ever start taking drugs.
What is the problem?
Around three million people in England and Wales report using drugs each year, putting themselves at risk and driving a violent and exploitative supply chain including through so-called ‘recreational’ drug use. Prevalence of cocaine use amongst adults in the UK is second only to the USA [footnote 48]. Cannabis is even more widely used than cocaine, with 7.8% of 16 to 59 year olds (2.6 million people) and 18.7% of 16 to 24 year olds (1.2 million people) reporting use in 2019/20 [footnote 49].
Most ‘recreational’ users are sheltered from the social consequences of the drugs trade – the serious violence, human exploitation, severe addiction and crime – which are often felt by those living in more deprived parts of our country or overseas. This is part of a harmful cycle where drug use is normalised; adults using drugs socially often live relatively typical and otherwise healthy lives and may not recognise their role in fuelling the drugs trade or influencing and damaging the behaviour of others, including children. They may also feel that they are not at risk of experiencing any consequences themselves from their drug use. This should not be the case.
Drug use among children and young adults is particularly concerning. Following fifteen years of sustained decline in the use of drugs, since 2012 there has been an increase in the proportion of 16 to 24-year olds reporting use of both cannabis and Class A drugs [footnote 50]. Drug use by young people risks worse immediate and long-term outcomes, including health, educational attainment and involvement in criminal activity.
How this strategy will change things for the better
Reduced demand for drugs will have positive impacts on degrading violent supply chains and will have wider benefits on quality of life. To get there we need a whole-of-society effort, and we must pursue a range of activities focused on:
- building a world-class evidence base
- reducing the demand for drugs among adults
- preventing and reducing use among children and young people.
Building a world-leading evidence base
We will develop a world-leading evidence base on how to tackle drug use amongst adults. This will address the insufficient international knowledge for how to change drug-related attitudes and behaviours at a population level.
As a first step, we are commissioning a comprehensive domestic and international research project on reducing drug use across society, the first component of which will make initial policy recommendations in spring 2022 with an ongoing programme of work.
The evidence base for how to prevent drug use among children and young people is more developed. We know that a focus on risk and resilience factors is important. Good outcomes can be achieved by building resilience through skills-based education, as well as through multi-component programmes involving parenting interventions and support for individuals and families [footnote 51]. We will keep implementing this and improving our understanding further to respond to concerning trends in drug use. The Advisory Council on the Misuse of Drugs will also use their significant expertise to commence further work with a review on prevention of vulnerable groups falling into drug use. Liverpool John Moores University have been commissioned to conduct primary research to understand the causes of the recent increased prevalence of drug use among young people. This will report in early 2023, with emerging findings during 2022, and will inform a further programme of work.
The people who influence and effect change and behaviours are varied – peers, families, teachers, social media influencers and the wider media are just a few. We will therefore convene a drug summit in Spring 2022 to bring together independent experts, employers and representatives of relevant sectors including education, law enforcement and the night-time economy, with partners from across government to help us better understand the challenges and potential solutions.
We will draw upon the insights and recommendations from the summit and research projects as we work towards our long-term ambition. A new £5 million three-year cross-government innovation fund will allow us to test and learn, realise our ambition to reverse the rising trend in drug use and reduce overall use towards a historic 30-year low within a decade.
Reducing the demand for drugs among adults
The strategy is unashamedly clear on our position: illegal drug use is wrong and unlawful possession of controlled drugs is a crime. We must take quick and decisive action to reduce the use of drugs ‘recreationally’. A new and bold approach – supported by an additional investment of £25 million – will be rolled out within three years to set the framework for the next decade and drive down rates of illegal drug use.
The bold new approach will deliver more meaningful, fairer and tougher consequences for those who use drugs ‘recreationally’ and will make sure that anti-social behaviour impacting on the quality of life of people and neighbourhoods is a priority and dealt with robustly. It has two phases of action: taking decisive action now, and then a white paper to be even bolder in achieving tougher and more meaningful consequences for illegal drug use. This framework will target those who currently feel, perhaps because of where they live or socialise, that they are not at risk of facing legal consequences from their use. We will make it clear to such people that they must change their behaviour, or they will face a range of escalating sanctions that will drive impositions on their lifestyles far greater than are felt today. Insights and evidence from our evaluation and research alongside this will inform future investment.
A framework for change
This programme of work is targeted at interventions that, in combination, address different aspects of the same problem. The police already come into contact with drug users in a range of contexts, but by rapidly expanding the use of drug testing on arrest we are enabling the identification of a greater number of drug users. At the same time by bringing a tough consequences scheme to a number of police force areas and adding to existing pioneering schemes, we are ensuring that the model for assessment, referral and applying sanctions to those caught in possession of drugs is rolled out at scale.
While doing this we are supporting forces to take a consistent national approach to sending clear and impactful messages to those who buy drugs from dealers and whose contact details are found in vast numbers when dealers’ phones are seized up and down the country. Further work will test the kinds of messages and support which are most likely to result in sustained changes in attitudes and behaviours and will provide evidence for future communications campaigns. As a result of all of these initiatives, drug users will increasingly become known to law enforcement, forced to face up to their behaviour, and the set of flexible but escalating interventions will begin to shift the dial on drug use.
Taking decisive action now
We are aware of seven police forces currently operating out-of-court disposal schemes and at least double this number will be operating such schemes by the end of 2024/25. With an additional £3 million per year allocated in the Spending Review, a total of £9 million, we will support police forces to introduce, or expand, a tough consequences out-of-court disposals scheme from Summer 2022 which will make sure that more people using illegal drugs receive a relevant and proportionate consequence. Criminal charges will remain the final step for those who continue to offend.
The new investment will deliver an expansion in the capacity of forces to deal with drug possession offenders, ensuring that more people face the consequences of their use through a consistent, swift and certain approach to drug possession. Sanctions will be proportionate and relevant to the circumstances. For example, those who are caught in possession of drugs for the first time may be required to attend a drugs awareness course, so they have the opportunity to understand the harms of drugs and change their behaviour. In some cases, an individual may need more than one opportunity to make this change in their lifestyle, and police forces will have discretion to support this. For those who don’t engage or who continue to offend, the police will be able to impose further requirements, including levying a fine or, requiring them to do work in their community or agree to undertake drug treatment for this pattern of drug use. Ultimately, they could receive a caution or face prosecution.
This will mean that so-called ‘recreational’ drug use doesn’t go without punishment, but it also allows the police to focus their attention on the ruthless pursuit of the criminal gangs supplying drugs and driving the highest harm. We believe that police officers will welcome the opportunity to direct adults who use drugs into a range of tough and meaningful interventions which will cause them to think about their drug use and the choices they are making, and in many cases will help people to decide to stop using drugs. The projects will be designed with police forces and will aim both to address the disproportionate way in which certain groups, such as young black men, are sanctioned by the criminal justice system for drug possession (as highlighted in the March 2021 Commission on Race and Ethnic Disparities report) and, at the same time, deliver a set of tougher consequences for everyone who breaks the law.
A £15 million expansion of drug testing on arrest through police forces across England and Wales will be rolled out from April 2022. All forces will have the technology to test people arrested for trigger offences, such as acquisitive crimes (such as burglary, robbery and theft), for cocaine and for certain opiates. We are also funding a number of forces to expand drug testing on arrest outside of trigger offences, as part of efforts to explore new approaches for targeting wider cohorts of users. When people test positive, they may be subject to an assessment of their drug use and referral to drug awareness, drug treatment or other interventions aimed at changing their behaviour.
Separately, we are legislating within the Police, Crime, Sentencing and Courts Bill to expand powers initially within problem solving ‘substance misuse’ courts pilots to enable drug testing of offenders serving community sentences which meet a certain criterion. At the moment, we can only test those who agree to undergo drug treatment. This new power will give judges the ability to order drug testing of anyone whose offending is related to their use of drugs, whether they agree to it or not. If they test positive, they could be in breach of their order and liable to be resentenced to a custodial sentence. This will form part of a package of incentives and sanctions available to the judge to incentivise compliance.
In addition, when we seize drug dealers’ phones, we will use the information held on them to contact their customers with a range of messages to discourage their drug use and direct them to support. This will help to make sure that no one is, or feels, anonymous when they buy drugs. We want to learn from this, and so will support an expansion under a project called Operation Mercury, working closely with the National Police Chiefs Council and police forces.
We want to drive behaviour change to reduce the demand for drugs before it gets to this stage. Our next step is further research and testing messaging through an evidence-based, targeted behaviour change initiative, initially aimed at students in further and higher education to be rolled out in autumn 2022.
Existing evidence tells us that communications campaigns work best when they are tailored and targeted to the audience and are integrated with support interventions, such as brief sessions on the harms of drugs, information and advice. The trial of messaging in universities will be delivered alongside increased capacity to deliver these interventions and ensure access to treatment services for those with an appropriate level of need. In choosing locations we will consider where there is need in terms of the level of drug use and where there are existing well-established local drug treatment services or young people services that, if funded, could partner with universities to expand and enhance their services.
We will robustly test and evaluate the impact of different messages including whether people act on being exposed to the campaign, namely by seeking information or support as directed by the campaign message, and then whether they make different choices about drug use.
A white paper to be even bolder in achieving tougher and more meaningful consequences for illicit drug use
The government will publish a white paper in due course which will look at new measures to reduce demand and deter people from illegal drug use through a set of tougher sanctions. We will not hesitate to ensure repeat offenders face consequence. At this stage nothing is off the table; for repeat offenders we will explore options to change their behaviour via civil sanctions and court orders. This could include, where relevant and proportionate, curfews or the temporary removal of a passport or driving licence, measures that would escalate depending on the severity and frequency of the offences. We will also consider going further than before in fining people who break the law, including consulting on options to increase the level of fines to maximise the deterrent and dissuasion of financial penalties.
The white paper will also set out options to expand the use of drug testing on arrest, in particular to allow this tool to be targeted towards so-called ‘recreational’ users, which may involve looking at which offences are ‘trigger offences’, and also the drugs for which police can test. Our evaluation of the projects outlined in this section of the strategy will inform the white paper and our long-term future ambition.
Preventing the onset of drug use among children and young people
As stated in part two of Dame Carol Black’s review, preventing drug use is more cost-effective and socially desirable than dealing with its consequences. To sustainably reduce both ‘recreational’ and problematic drug use among adults in the long-term, we must take a whole-of-government approach to preventing use among children and young people now. In line with the evidence, this will involve a broad range of activities, most of which are not specific to addressing drug use but have many other benefits as well.
While the prevention interventions that the UK Government is responsible for are predominantly only in England, we will continue to work with the devolved administrations to share practice and learning.
School-based prevention and early interventions
The most effective and sustainable approach to reducing demand is building the resilience of young people through giving them a good start in life, the best education possible and keeping them safe, well and happy.
Drugs education is part of the compulsory health education curriculum for all state funded schools, following the introduction of statutory relationships, sex and health education in England in September 2020. In health education, there is a strong focus on mental wellbeing, including a recognition that mental wellbeing and physical health are linked. This includes teaching about the dangers of drugs and alcohol which teachers are supported to deliver with a package of teacher training modules. DfE is developing long-term monitoring of delivery across the whole of the new relationships, sex and health education requirement. This includes new quantitative and qualitative research, to understand the quality of implementation, including teacher confidence in teaching the statutory requirements, and identifying any further training and support needs.
As well as universal education, there are a range of programmes in schools to identify and support children with vulnerabilities including individual risk factors which also apply to drug use such as having difficulty managing emotions, coping with challenges, and exercising behavioural self-control. For example, multi-disciplinary specialist teams are working in alternative provision schools to provide wraparound support for those most at risk of involvement in serious violence and county lines.
Supporting young people and families most at risk of substance use
Young people at higher risk of using and experiencing harm from drugs include those taken into care, those with untreated mental health issues, those involved with gangs and those whose parents use drugs among other factors. We are stepping up investment over the next three-years in a range of programmes across government that provide early support to children and families, including families where the use of drugs is a risk to the child.
Supporting families and children across the country is a crucial part of the government’s ambition to level up. In addition to the £39 million already committed to champion family hubs, £300 million will be invested to transform ‘Start for Life’ services and create a network of family hubs in half of the council areas across England. This investment will provide thousands of families access to support, ensuring babies have the best start in life – supporting them to thrive and realise their potential. Family hubs are a way of joining up locally to improve access to services, the connections between families, professionals, services, and providers, and putting relationships at the heart of family help. Family hubs bring together services for children of all ages, with a great Start for Life offer at their core.
An additional £200 million is being invested over the next three years in the cross-government Supporting Families Programme, taking total planned investment to nearly £695 million. This funding will help up to 300,000 more families facing multiple, interconnected issues to access effective whole-family support and to improve their life outcomes. The most recent national evaluation of the Troubled Families Programme (which preceded Supporting Families) found that, in the year before starting on the programme, 15.6% of families had an individual dependent on drugs or alcohol [footnote 52]. By supporting these parents, we can help to reduce the incidence of substance use in the next generation.
For those children who cannot remain with their families and must be taken into care, making sure that care placements provide safe and secure homes that meet their needs is a priority. Over the next three years we will provide £259m to maintain capacity and expand provision in secure and open residential children’s homes. This will provide high quality, safe homes for some of our most vulnerable children and young people.
We know that children suffering from poor mental health are at higher risk of being drawn towards drug use or the exploitation linked to it. Making sure that children have access to mental health treatment is a key component of preventing those most at risk of experiencing harm from illicit drugs. As part of an additional £2.3 billion per year by 2023/24, an additional 345,000 children and young people will have access to mental health services each year by 2023/24. Additional NHS targeted interventions for the most vulnerable children and young people will strengthen provision around the child and intervene earlier to enable better outcomes.
Getting young people, particularly those who are more vulnerable, socially engaged and able to form strong relationships with their peers and trusted adults is vital in avoiding them being drawn in and damaged by illicit drugs and other dangerous activities. Grounded in the findings from the Youth Review, the Department for Culture, Media and Sport will invest £560 million of funding over three-years to build a new and improved youth offer. The Youth Investment Fund will be targeted at areas most in need and will provide investment in new safe spaces for young people, so they can access support from youth workers, and enjoy beneficial activities including sports and culture.
NHS England and Improvement are rolling out a framework for integrated care (SECURE STAIRS) across the children and young people secure estate. Children held in secure settings are amongst the most vulnerable in society. They are more likely than others to have additional healthcare needs, such as neurodevelopmental disorders, substance addiction and mental health disorders. Working collaboratively with co-commissioners and partners across the whole system (education, children’s services, public health, voluntary sector and youth justice) we will make sure that integrated, trauma-informed services are delivered to those who need them.
We also know that children have distinct needs from adults as a result of their age, and it is right that this is reflected in the way that the justice system treats children who have, or may have, offended. We must recognise the unique needs of children compared with adults and the vulnerabilities of those involved in drug crime. To be effective, we must address the underlying reasons for a child or young person’s offending and take a flexible and proportionate approach to addressing the criminal behaviour. This is ultimately how we see young offenders going on to lead crime-free lives. This is achieved by striking the right balance between prevention, support and sanction, addressing the causes of criminal behaviour, intervening early to provide support, and diverting children away from the formal justice system where possible.
Chapter 5 – Setting up for success: partnerships and accountability
Local government and delivery partners are the foundation of this strategy. They are best able to establish priorities and devise ways of working to address challenges quickly and effectively. Our vision is for this strategy to provide both the strategic objectives and the investment needed to make sure that local partners across England are empowered and resourced to deliver results.
New nationally set standards and outcomes will provide structure and oversight that will ensure consistently high-quality services, and that funding is prioritised around the commitments in this strategy. At the heart of our objectives will be effective multi-agency partnerships that bring to life the principles of comprehensive treatment and recovery alongside tough and effective enforcement and ambitious prevention to reduce drug use for the long term.
What is the problem?
The drivers of drug use and drug-related harm are complex and cut across the responsibilities of a range of different government departments and other organisations. The systems map below highlights the range of support that could be needed by an individual or a family, and potential pathways into the types of support they might need.
This needs to be co-ordinated to be effective but too often it is not, or the services are not in place to provide a journey to recovery. This undermines efforts to combat drugs and level up the country.
How this strategy will change things for the better
We are doing three main things to support communities to flourish and succeed:
- providing focused investment, targeted at the places with the greatest need – this will mean that areas with high levels of drug use, drug-related deaths and crime will be prioritised for aligned additional funding across treatment, justice, employment and accommodation support
- improving partnership working – we will set out what good partnership working looks like and who should be involved, using lessons from Project ADDER and other locally-based partnership initiatives such as Changing Futures to develop best practice and a learning network
- developing a system of national and local outcomes, frameworks and accountability that will drive a consistent and clear set of expectations across the next decade and ensure measurement of government against its promises
Systems map on the range of support that an individual with addiction might need to access
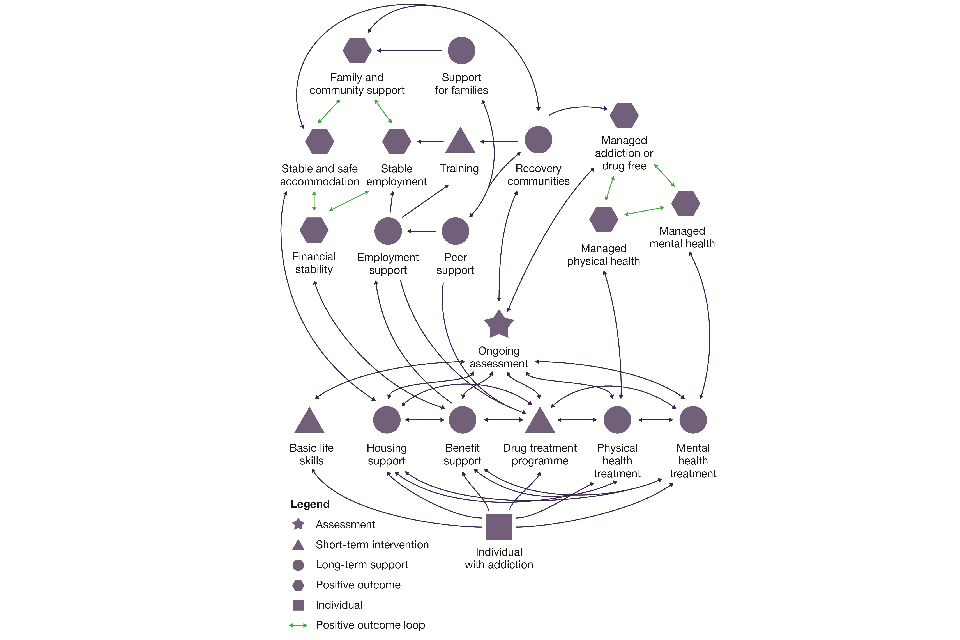
Systems map on the range of support that an individual with addiction might need to access
Focused investment, targeted at the areas of greatest need
The funding announced in this strategy will deliver ring-fenced additional support across treatment and recovery services, housing support, employment support, and support for offenders. This will be rolled out across the country over the course of this Parliament, starting with the areas of greatest need, supported by focused and uncompromising enforcement on supply chains and prevention of drug use [footnote 53].
Our existing flagship initiative, Project ADDER, has taken a local partnership approach to addressing drug use in some of the hardest-hit local authorities across England and Wales. These principles and learning will now be applied to a wider range of activity in more places. In addition, funding for Project ADDER is committed to for the next three years to enable us to maximise progress on combating drugs and feed learning to the national roll-out.
Case study: Learning from Project ADDER
In Project ADDER, partners designed delivery plans shaped around local needs and circumstances, taking into account the views of those with lived experience at every stage. Both the police and local authority are accountable to the shared ADDER outcomes, which include reducing drug use and drug-related deaths, as well as reducing reoffending by better supporting individuals in leading fulfilling lives away from a life of crime. This has motivated each organisation to play their part in order to gain help from others to deliver on their own individual objectives.
Although the local authority and police force are at the heart of each project, their approach is based on closer working across a broad range of organisations including probation, housing, employment, mental health services and social services. This enables the police to cut off supply whilst working in tandem with treatment providers to divert people away from offending and into enhanced treatment and recovery interventions, including housing and employment services, having a greater collective impact on levels of demand.
The Project ADDER Partnership Network allows us to share learning and good practice across the projects with the wider sector and the devolved administrations across the UK. We will use this learning, alongside other initiatives, to build frameworks into our long-term strategy that support and enable local leaders to work in partnership, and make sure that money is spent effectively across local services. This will drive clearer alignment between national outcome expectations and local delivery outcomes.
Improve partnership working
Multi-agency leadership
Senior leadership buy-in and support is essential to appropriate resource and priority being placed on combating drugs within a local area. This means supporting frontline practitioners including police or probation officers, doctors, nurses, drug workers, teachers, social workers or youth workers, to work together effectively.
We are requiring local areas in England to have a strong partnership that brings together all the relevant organisations and key individuals, and to provide a single point of contact for central government. This partnership could cover one local authority or several, but it must have proactive oversight of the implementation of all three strategic priorities of the strategy and make sure that local organisations work together and jointly agree provision and where they can improve. At a minimum, we would expect all the following organisations to be represented in a strategic partnership in England, with a nominated chair as the responsible owner:
- elected members
- local authority officials (including expertise in relevant areas to include substance misuse, housing, employment, education, social care and safeguarding)
- local NHS strategic leads (e.g. clinical commissioning groups, primary care networks and integrated care partnerships)
- NHS England and Improvement
- the Office for Health Improvement and Disparities region
- substance misuse treatment providers
- voluntary, community and social enterprise sector
- people affected by drug-related harm
- primary care representatives
- mental health treatment providers
- local schools and FE representatives
- Job Centre Plus
- police representatives
- Police and Crime Commissioners
- Probation Service
- the Youth offending service
- prisons and young offender institutions
Understanding the local situation and defining priorities
It is only by sharing data and conducting joint analysis that local areas can properly understand what their priorities are, and how to address them together. A key task of the local partnership will be to conduct a joint needs assessment through the review of local drug data and evidence and use this to agree a local drugs strategy and action plan, including developing data recording and sharing. We will provide guidance and templates to help partners plan co-ordinated, efficient activity to drive down all forms of harm related to drug use. The partnership should be informed by any existing evidence already collated by the local area on system performance and maturity.
We will engage on the detail of the structures and processes to be included in the guidance early in 2022, to be agreed and operational for the 2022/23 financial year. This will happen in tandem with the development of the new quality standards for commissioning substance misuse treatment and recovery services by OHID that was mentioned in chapter 4. This will make sure that action is integrated between all three of our strategic priorities.
Working across existing structures and partnerships
There are strong existing partnerships in many local areas. Multi-agency leadership of combating drug use could operate through an existing structure (such as a Community Safety Partnership, Health and Wellbeing Board, or Integrated Care Partnership) where the membership and principles of joined-up, outcome-focused working are in place.
Prevention of substance use is a key element of the government’s ambition to reduce the demand for drugs. We know that the factors placing young people at risk of substance use are complex and often inter-related. In 2017, significant reforms were introduced, requiring local authorities, clinical commissioning groups and chief officers of police to form multi-agency safeguarding partnerships. Multi-agency safeguarding arrangements (MASAs) were fully established in 2019, and we continue to work across government and with local partners to ensure that they are as effective as possible. With strategic oversight from health, policing and local authority leaders, MASAs can co-ordinate identification, protection and intervention for those at risk of harm in a way which best responds to local circumstances. Our draft guidance for a new Serious Violence Duty requires police, probation, and the NHS to work together with local authorities to prevent and reduce serious violence.
Our proposals for partnership working to address drug harms, with local flexibility alongside central guidance and support, are modelled on learning from this and other initiatives including Changing Futures and Project ADDER.
Developing a system of national and local outcomes, frameworks and accountability
National Outcomes Framework
To provide a clear and consistent focus on the long-term outcomes this strategy commits to, and to effectively track and measure progress, we are developing a new national outcomes framework. This will measure progress against our aims across England, enabling citizens to assess our performance.
The draft national outcomes framework is set out below and states our long term and intermediate outcomes and proposes a range of metrics that will allow us to assess progress towards these. We have built these around data that is readily available. The limitations of this approach are understood, and we will review and strengthen these counting mechanisms in the coming months. Once finalised, we will use these headline metrics as a continuous thread through the lifetime of the strategy.
We will engage and work with experts and stakeholders, including sharing expertise and best practice with colleagues across the devolved administrations, to identify further supporting measures to monitor:
- progress from delivery to outcomes, including measures to describe the impact we are having in protecting the public from organised crime gangs
- the health of the whole system and look for unintended consequences and behaviours, including differential impacts across protected groups
We will be looking at measures we can already assess, as well as:
- what can be enhanced and developed through improving data quality, data matching, and new data collection
- developing new measures focused specifically on drug use, alongside cross-cutting measures
- enhancing and developing surveys to measure qualitative outcomes, such as societal attitudes to drugs or ease of availability of drugs
In April 2022 we will publish these measures and the progress made against them in annual reports, providing updates to metrics and reporting against our commitment to expand and improve the evidence base on what works to combat drug use.
As part of our approach to developing new data, we will work with the cross-departmental Better Outcomes through Linked Data (BOLD) Programme to enhance the availability of information with the aim of improving services and outcomes for the most vulnerable adults in society. The programme will deliver better evidenced, joined-up and more effective cross-government interventions to support people at specific touchpoints in their interactions with government services, utilising timely linked anonymous data and evidence.
As Combating Drugs Minister, Kit Malthouse MP has overarching accountability for delivery of the ambitions and outcomes and will present an annual report to Parliament to monitor progress. Each relevant secretary of state has accountability for delivering the outcomes and commitments within their department’s remit, with a relentless focus on better outcomes for citizens and neighbourhoods.
Government departments will be accountable for progress against these outcomes and metrics to the Joint Combating Drugs Unit, and through existing departmental and government-wide accountability. We will also continue to evaluate and report on programmes within this strategy and on the success and challenges of the whole-of-government approach, to make sure that these continue to deliver value for money, and to identify and propagate good practice and track their progress against the national outcomes.
Long term strategic outcomes and headline metrics
Reduce overall drug use
Measured by:
- Drug use for 16-59 year olds, source ONS Crime Survey England and Wales
- Drug use for 16-24 year olds, source ONS Crime Survey England and Wales
- Drug use for 11-15 year olds, source NHS Digital Statistics on Dug Misuse
Reduce drug-related crime
Measured by:
- Drug-related reoffending rates, source MoJ Proven Reoffending Data
- Neighbourhood crime offences, source ONS Crime Survey England and Wales
- Number of drug related homicides, source ONS Homicide in England and Wales
Reduce drug related deaths and harms
Measured by:
- Death from drug misuse, source ONS Deaths related to drug poisoning England and Wales
- Volume of hospital admissions related to drug misuse (primary diagnosis), source NHS Digital Statistics on Dug Misuse
Intermediate outcomes
Reduce the levels of drug supply
Measured by:
- Volume of Class A drug seizures, source Home office
- Drug purity levels heroin / cocaine, source NCA
- Number of moderate / major disruptions, source NCA
Improve recovery outcomes
In consultation with stakeholders, we will develop a set of measures to assess wider recovery outcomes (in the community and prisons) this is likely to include measures around achieving long-term recovery, moving int stable accommodation, meaningful activity and mental health.
Increase engagement in treatment
Measured by:
- New quality and outcome measure (April 2022), source OHID (in development)
- Numbers in treatment (opiate / non-opiate), source, OHID Substance Misuse Treatment for Adults
These national metrics are currently collected and available to provide trend data to measure the strategic outcomes of the strategy. All have limitations and risks, but further work will be conducted to develop an improved set of supporting metrics and develop the data sources further.
Local outcomes frameworks
For this to succeed, there needs to be alignment between national outcome expectations and local delivery. We will therefore be introducing a local outcomes framework to sit alongside the National Outcomes Framework. Like its national equivalent, the local outcomes framework will cover all three strategic priorities.
As with the proposed local partnership structures, we will engage on potential metrics early in 2022, to ensure that they are agreed and operational for the 2022/23 financial year. As recommended by Dame Carol Black, the local outcomes framework will enable comparison with other similar areas and, in some cases, funding may be dependent on showing progress on these outcomes. The new national commissioning quality standards will support local areas to align services with the outcomes required.
Measurement in itself will not reduce the harm associated with illegal drugs without action. We will therefore expect local areas in England to produce their own annual report, analysing local performance and identifying appropriate next steps. Organisations must jointly identify how they will address their agreed priorities, allocate their respective resources to meet the joint objectives and identify where they need more support or where government can better enable action or remove barriers.
Appropriate support will be offered to local areas based on their performance and the steps identified in their reports. Where considerable improvement in partnership structures or service delivery is required, we will support local areas to analyse their local need, draw on best practice from elsewhere, and develop and monitor improvement plans.
Chapter 6 – A 10-year journey
This strategy demonstrates clear ambition to address the substantial harm that is currently experienced across our country due to the supply and use of illegal drugs. Record levels of investment and a clear whole-of-government commitment are solid foundations for success.
The commitment of the government cannot be judged only through words, but by action to deliver real change for citizens and neighbourhoods. Outcome frameworks and accountability are essential for this. We must also commit to transparency, openness and continuous improvement.
There are many areas that this strategy has not covered in detail. The full breadth of the government’s priorities on combating drugs spans a wide portfolio. This publication is just the first iteration of what will be a living document, and we will publish annual reports, which allows us to move our thinking forward year on year. We will use the reports, which will be laid before Parliament, to track progress against the National Outcomes Framework. We will work with experts, including the Advisory Council for the Misuse of Drugs and experts through experience, to assess emerging threats, review the latest evidence, monitor trends and identify new areas of focus.
Central oversight will be the responsibility of the new Joint Combating Drugs Unit, headed by cross-government Combating Drugs Minister Kit Malthouse MP. The unit which was created in July 2021, and is charged with monitoring implementation and success of the strategy and will lead on annual reporting.
Our ambition will be supported by our commitment to investing in research relating to supply, prevention, treatment, and recovery. Several components of this strategy contain commitments to innovate and improve by developing the evidence base, trialling new ideas, evaluating promising initiatives and embedding research into service delivery. We will promote greater innovation in research by offering incentives or rewards to companies or organisations whose developments prove beneficial in practice in the addiction field. We will also introduce an innovation fund, led by Chief Scientific Advisers in UK government departments. These commitments will allow us to test and learn against our goal to drive down overall drug use – striving to level up neighbourhoods and save lives.
This strategy is the start of a 10-year journey. Over the next decade, the government and its partners must continue to listen, learn and adapt as the context around us changes. In the next three years, and in the decade ahead, we will reduce drug-related crimes, deaths, harms and overall drug use, and level up the country.
Footnotes
-
Further detail on the geographical scope of the strategy is provided in chapter 1. ↩
-
Review of drugs part two: prevention, treatment, and recovery - GOV.UK (www.gov.uk) ↩
-
Project ADDER (Addiction, Diversion, Disruption, Enforcement and Recovery) is a comprehensive approach to tackling drug misuse and offending, bringing together local agencies, police, councils and health services in some of the areas most affected by drug misuse. This programme tackles drugs misuse through coordinated action combining targeted and tougher policing with enhanced treatment and recovery services. ↩
-
Review of drugs: Part One - GOV.UK (www.gov.uk); Review of drugs: Part Two - GOV.UK (www.gov.uk) ↩
-
National Strategic Assessment of Serious and Organised Crime 2020 (National Crime Agency) ↩
-
2020 NRM Referrals of under 17s, change on 2019 figures. There have been improvements in awareness and recording which have contributed to this increase in addition to increased prevalence. ↩
-
Drug misuse in England and Wales: year ending March 2020 (Office for National Statistics). Includes all drug types, including glue, aerosols and solvents. Cannabis is the most common. Smoking, drinking and drug Use among young people in England 2018 [NS] - NHS Digital ↩
-
Deaths related to drug poisoning in England and Wales: 2019 registrations (Office for National Statistics). ↩
-
‘Hard Edges: mapping severe and multiple disadvantage’ (Lankelly Chase Foundation, 2015) ↩
-
The report of the Commission on Race and Ethnic Disparities - GOV.UK (www.gov.uk) ↩
-
Responsible for UK drug legislation, UK borders and organised crime, policing and crime reduction in England and Wales. ↩
-
Responsible for drug treatment services in England, as well as wider health and social care services. This includes treatment in prisons. ↩
-
Responsible for courts, prisons and probation, and for reducing reoffending in England and Wales. ↩
-
Responsible for policies on employment support and social security in England and Wales and shares that responsibility in Scotland with the Scottish Government. In Northern Ireland, these areas are the responsibility of the Northern Ireland Executive. The Department for Communities in Northern Ireland and the Department for Work and Pensions in Great Britain seek to maintain similar social security systems. ↩
-
Responsible for levelling up, local authorities, housing and rough sleeping in England. ↩
-
Responsible for the welfare and safeguarding of all children in England, children’s mental health and wellbeing in education. ↩
-
The legal framework relating to the misuse of drugs, including the Misuse of Drugs Act 1971 and the Psychoactive Substances Act 2016, is reserved to the UK Government. Further, the NCA and Border Force conduct drug supply reduction activity across the UK. Other policy areas covered in the strategy such as healthcare, education, housing and social care only cover England. The areas relating to the work of the police and the criminal justice system apply to England and Wales. DWP’s Individual Placement and Support Programme covers England and the peer mentoring programme covers England, Scotland and Wales. ↩
-
Preventing Harm, Empowering Recovery - Substance Use Strategy, Department of Health (health-ni.gov.uk) ↩
-
The production of opium and cocaine doubled between 1998 and 2017. From 2013 to 2018 there was an increase from 36% to 76% in crack cocaine purity and an increase from 29% to 46% in heroin purity. Review of drugs: Part One - GOV.UK (www.gov.uk) ↩
-
Measuring the costs of drug-related crime in Understanding organised crime: estimating the scale and the social and economic costs (publishing.service.gov.uk) ↩
-
Homicide in England and Wales - Office for National Statistics (ons.gov.uk) ↩
-
NCLCC County Lines Strategic Assessment 20/21. The reduction in potentially active lines is believed to be linked to a change in reporting and enhanced operational activity. ↩
-
Figure is based on continuing to shut down open and reopened lines over the next 3 years and assumes investment at levels set out within this document. ↩
-
The NCA assesses the impact of interventions against drugs supply in terms of organised crime group disruptions. Over the last three years, law enforcement has delivered around 5,300 major and moderate disruptions against drugs OCGs, where a ‘major’ disruption reflects a significant or long-term impact on an OCGs ability to operate (such as the dismantling of an organised crime group through the conviction of key individuals or a series of large seizures), and ‘moderate’ represents a noticeable or medium term impact (such as a single large seizure). With this investment we will deliver 6,400 major and moderate disruptions of drugs OCGs over the next three years – a 20% increase. This represents a significant and sustained attack on criminals’ ability to bring drug-related harm to our communities. ↩
-
Case study anonymised to protect the identities of those involved. ↩
-
What Is the Future of UK Drugs Policy for Afghanistan? - Royal United Services Institute (rusi.org) ↩
-
Seizures of drugs, in England and Wales, financial year ending 2020 - GOV.UK (www.gov.uk) ↩
-
National Records of Scotland: Drug-related deaths in Scotland in 2020. ↩
-
Deaths related to drug poisoning in England and Wales: 2020 registrations (Office for National Statistics) ↩
-
The spilt of funding is set out in this chapter. This sum includes £8m of funding for a peer mentoring programme – which will cover England, Scotland and Wales – described in more detail later in this chapter. ↩
-
Changing Futures is working with 15 local cross-sector partnerships to test innovative approaches to more effective and co-ordinated support. ↩
-
Rough Sleeping Questionnaire: initial findings - GOV.UK (www.gov.uk) ↩
-
7,500 places is included in the headline 54,500 total figure. ↩
-
Black, C.M., 2016. An Independent Review into the Impact on Employment Outcomes of Drug or Alcohol Addiction and Obesity. Department for Work and Pensions. Henkel D. Unemployment and substance use: a review of the literature (1990-2010). Current drug abuse reviews. 2011 Mar 1;4(1):4-27. ↩
-
DWP is responsible for policies on employment support and social security in England and Wales and shares this responsibility in Scotland with the Scottish Government. ↩
-
PHE/MOJ 2017 Study ↩
-
A similar approach in Hawaii has seen successful outcomes. Managing Drug Involved Probationers with Swift and Certain Sanctions: Evaluating Hawaii’s HOPE - National Institute of Justice (ojp.gov) ↩
-
Community Performance Annual, update to March 2021 - GOV.uk (www.gov.uk) ↩
-
Drug misuse in England and Wales: year ending March 2020 (Office for National Statistics). ↩
-
Drug misuse in England and Wales: year ending March 2020 (Office for National Statistics). ↩
-
The international evidence on the prevention of drug and alcohol use: Summary and examples of implementation in England - GOV.UK (www.gov.uk) ↩
-
National evaluation of the Troubled Families Programme 2015-2020: family outcomes - national and local datasets part 4 (www.gov.uk) ↩
-
Funding for peer mentoring covers England, Wales and Scotland. Funding to support offenders will include provision of treatment via HMPPS in Wales ↩