
Annual Report for 2017
Published 17 May 2018

© Crown copyright 2018
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/raib-annual-report-published-2018/annual-report-for-2017
Our Purpose:
To independently investigate accidents to improve railway safety, and inform the industry and the public.
1. Chief Inspector’s review of 2017
The tram accident at Sandilands junction in Croydon on 9 November 2016 was a tragic and momentous event, and the Rail Accident Investigation Branch’s (RAIB) response to it has inevitably been the most significant part of our activities during 2017. In December we published the final report of our investigation into that overturning event, which resulted in the death of seven passengers, serious injuries to nineteen, and psychological trauma to many others. It was vital that the circumstances that led to this accident, and the factors that contributed to these levels of harm, were properly understood and the safety learning identified. To achieve this we undertook our most complex and extensive investigation to date. By February 2017 we had already issued two interim reports and during the summer of 2017 we notified the tram industry and the safety authority of the areas that were likely to feature in our recommendations.
Large parts of the investigation would not have been possible without the excellent cooperation of the other statutory bodies. Our investigation team quickly established good working relationships with their counterparts in British Transport Police and the Office of Rail and Road (ORR), and this enabled each body to fulfil its own legal duties without detriment to the work of the others. The tram industry organisations involved also cooperated freely with our investigation and provided technical support when needed.
We are particularly grateful to the families of those who so tragically lost their lives. All the families were supportive of our work and understood the reasons why we had to investigate every aspect of this accident. We were hugely impressed by their courage and dignity, and that of the people who were injured, when engaging with us in such distressing circumstances.
Our report makes 15 recommendations for the improvement of safety on tramways. Two themes that feature in many of these are the need for tramways to improve their understanding of risk, particularly in relation to events that are only likely to occur rarely, but will have very serious consequences; and the need to establish additional measures to control the likelihood of human failings leading to a catastrophic outcome of this type. Tram drivers are no different from the rest of us. As human beings, we are not well adapted to maintaining high levels of alertness when carrying out routine tasks which involve low levels of stimulation, such as driving a tram through a long straight tunnel. It is for this reason that the UK’s mainline railway has invested in technology that provides a warning, or intervenes, if a train approaches a high risk location, such as a tight curve, at too high a speed. We have produced a short video on our findings and recommendations from the Sandilands investigation.
A short video on our findings and recommendations from the Sandilands investigation.
I am encouraged by the positive response to our report and the recommendations. It is good to learn that the tramway sector has been in conversation with ORR and has already started work in many of the areas we have identified. I look forward to learning more about the outcomes in due course. It is also good to see that the mainline sector has shown an interest in the findings of the Sandilands investigation. The RSSB’s risk management forum in June 2018 will include a workshop on lessons from Sandilands for the heavy rail sector. We, together with Network Rail, will be holding a rail accident investigators’ seminar in November that will include discussions about the RAIB’s Sandilands investigation.
While we were working on the Sandilands investigation we also published 18 other investigations and 19 safety digests. Of these, the most significant in terms of potential consequences concerned the derailment of a passenger train just outside Watford Tunnel on 16 September 2016. The derailed train entered the tunnel and moved towards the adjacent line, where it was struck a glancing blow by a train travelling in the opposite direction.
The Watford Tunnel investigation once again highlighted the potential for very serious harm following a landslip, and the critical need to identify and properly manage earthworks, and their associated drainage systems. However, since it is unlikely that earthwork failures will be entirely eliminated in the foreseeable future, there is a need for infrastructure managers to continue to explore ways of predicting the areas that are most at risk following extreme weather events, and developing means of detecting failures before trains arrive.
Of particular note at Watford was the fact that the deviation of the derailed train from the track was limited because one rail engaged with a gap between different elements of the train’s underframe equipment. The gap was not designed for this purpose but, fortuitously, its presence almost certainly prevented a much more serious collision. This is why we have repeated an earlier recommendation that the rail industry (Rail Delivery Group and RSSB) considers the feasibility and safety benefit of providing guidance to derailed trains, either by features designed into the train or by the provision of special infrastructure at high risk locations. I am hopeful that this will lead to a much better understanding of reasonably practicable measures to keep trains in line should they derail.
A very unusual accident occurred at Twyford station in April 2016, when a teenager in a wheelchair, who was waiting with her mother to catch a train, found herself being blown along and across the station platform as a freight train passed through at speed. The wheelchair came into contact with three of the wagons, but by great good fortune its occupant was only slightly hurt. Our investigation found that passing trains can generate aerodynamic forces which can overcome the brakes of wheelchairs. We also found that users of wheelchairs and pushchairs have little awareness of the possible hazards from train slipstreams, and the railway industry could have done more to provide information and warnings to reduce the risk. I am glad that our work has produced information and recommendations which should help to make vulnerable members of society safer during their journeys by rail and note the work being undertaken by RSSB to address this risk.
Looking back over all the investigations that we have published or commenced during 2017, there are five major issues that stand out:
- how much the railway relies on signallers taking the correct action to ensure the safety of level crossing users when giving permission for road vehicles to cross a user worked crossing
- the danger to trains when earthworks and structures fail
- the number of narrowly avoided accidents involving track workers and moving trains
- the actual and potential consequences of the actions of fatigued railway workers
- the potential for serious accidents when errors are made during installation and commissioning of new infrastructure particularly when working under pressure
More detail on each of these is provided in section 4 .
Our ability to influence safety improvements relies greatly on how we are perceived by industry decision makers. We decided during the year to commission an independent market research consultancy, with extensive rail sector experience, to carry out a survey of our stakeholders across the railway industry.
You can read the results. For my part, I was pleased to see very high approval ratings against criteria such as professionalism. It was also good to note that 91% of the respondents believed that our investigations make an important contribution to improving railway safety - we were also seen to be performing well in respect of our independence and expertise.
Our recommendations are an important part of what we do since they are the primary means by which we can directly influence change. I was therefore particularly pleased to read that the majority of stakeholders surveyed are positive about our safety recommendations. The vast majority (almost 90%) of those surveyed consider them to be clear, well targeted, and well supported by evidence.

Average time taken to publish RAIB reports: 2014 - 12 months, 2015 - 11.3 months, 2016, 10.7 months, 2017 - 9.8 months
Given the value attached to the safety learning contained in our reports, it is natural that some stakeholders would like us to publish our reports more quickly, and 21% of those who responded to our survey thought that we performed badly in this respect. The graph shows the average elapsed time between the event date and the publication of our reports for each year between 2014 and 2017. We have reduced this by more than two months since 2014. Our average time to publication is now shorter than most of our counterparts elsewhere in the world. The graph excludes the small number of class investigations we have undertaken because they examine a number of incidents and accidents and do not have a single event date.
While acknowledging the desire for us to publish our reports earlier, I see little prospect of reducing our time to publish below that which we are currently achieving without there being a detrimental impact on quality. Therefore our focus in the future will be to find additional ways of communicating key safety information to a wider audience before our investigations are concluded. We already engage with affected parties throughout the investigation process, but we could do more to inform the public about emerging issues. One example of this is our recent decision to publish the urgent safety advice that is given to industry during an investigation at the time we issue it, rather than publishing it with the investigation report. We have also increased our use of interim reports when we feel there is a need to provide information about an accident to the industry and the public before we publish our final report (as for the Sandilands and Waterloo investigations).
We in the RAIB team are full time railway accident investigators. We believe we have learnt our trade and developed our expertise to a high standard, and we aim to work with others to help promote better accident investigation across the railway industry and to continue to learn from good practice elsewhere. I was therefore delighted that in October we were able to join with Network Rail in hosting a seminar involving many professionals in the railway industry who conduct or supervise investigations. The seminar featured a wide range of topics and ample opportunity for questions and lively debate. Since this event was well attended and the feedback from the participants was good, we intend to repeat the event in 2018 – I look forward to another opportunity to engage with fellow investigators.
In conclusion, I should like to thank my entire team for their dedication during 2017. I feel so privileged to work with such hard-working professionals, each of whom is committed to the improvement of safety on the UK rail and tram networks.
Simon French
Chief Inspector of Rail Accidents
17 May 2018
2. Operational activity
During the period from 1 January to 31 December 2017, we received 260 notifications of railway accidents and incidents from the industry. These resulted in 50 preliminary examinations.
As a result of the analysis of the information gathered, we started 19 full investigations and 14 safety digests.
We completed and published 19 full investigation reports in 2017. While our aim is to publish reports and safety digests within 12 months of the date of occurrence, the length of individual investigations can sometimes extend beyond this because of the complexity and scale of the investigation, late notification by the industry or the need to address complex issues raised during formal consultation. In 2017 the average time taken to publish reports was 9.8 months from the date of occurrence (as compared to 10.7 months in 2016). The shortest time taken was 7.5 months and the longest 12.7 months.
We also issued two interim reports, 19 safety digests and three urgent safety advice notices (more information on safety digests and urgent safety advice is provided later).
The figure below gives details of our investigation activity in 2017.
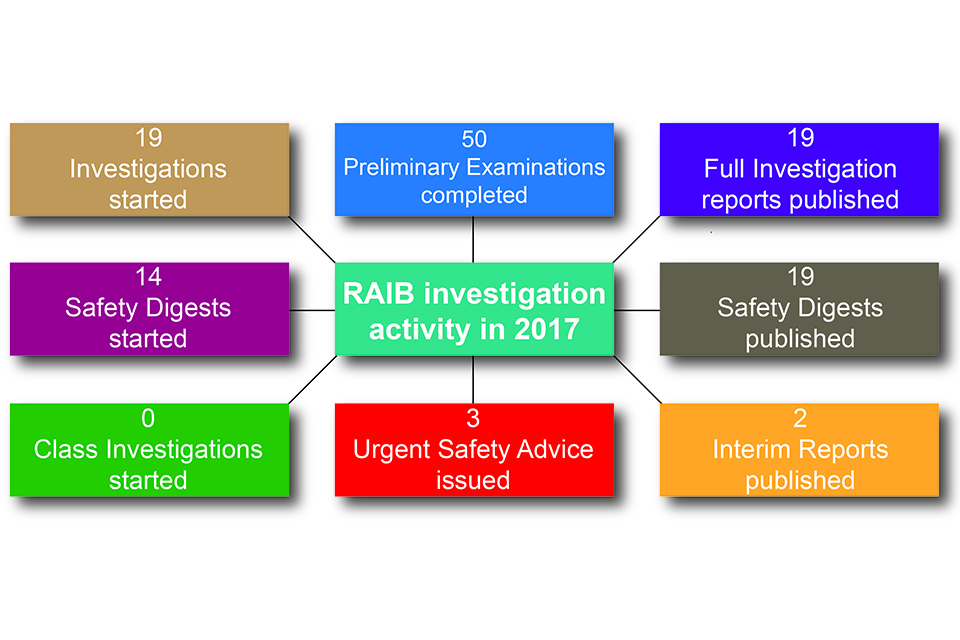
Investigation activity in 2017. 19 investigations started, 50 preliminary examinations completed, 19 full investigation reports published
2.1 Northern Ireland and the Channel Tunnel
During 2017, the RAIB did not carry out any investigations in Northern Ireland or the UK part of the Channel Tunnel. However we maintain contact with the two safety authorities (Department for Infrastructure and the Inter-Governmental Commission respectively).
2.2 Classification of accidents and incidents that have to be notified to the European Agency for Railways 2013 - 2017
We have a duty to investigate and to report to the European Agency for Railways (ERA) all railway accidents occurring in the UK that are classified in the Directive as ‘serious’[footnote 1]. We also have a similar duty for those incidents and accidents which, under slightly different circumstances, could have resulted in serious accidents, and which have an obvious impact on railway safety regulation or the management of safety.
ERA has published guidance to promote consistent categorisation of investigations in accordance with the Directive. We use this to classify our investigations according to Articles 19(1) and 19(2).
- Article 19(1) - a serious accident where the investigation is mandatory
- Article 19(2) - an accident or incident, which under slightly different conditions might have led to a serious accident, ie a near miss of a serious accident
Table 1 shows the breakdown of accidents and incidents that we have investigated between 2013 and 2017 as classified according to Articles 19(1) and 19(2). The figures have been collated according to the date of occurrence and not publication of the report.
Table 1 – Investigations by category sorted by Articles 19(1) and 19(2)[footnote 2]
| Basis for investigations by the European Railway Safety Directive category | 2013 | 2014 | 2015 | 2016 | 2017 | Total |
|---|---|---|---|---|---|---|
| Article 19(1) | 5 | 2 | 1 | 5 | 4 | 17 |
| Article 19(2) | 21 | 17 | 20 | 14 | 14 | 86 |
| Total | 26 | 19 | 21 | 19 | 18 | 103 |
Appendix B contains details of the investigations commenced and completed in 2017 and the legal basis for the investigation.
2.3 Safety digests
We began publishing safety digests in 2016. They are intended to share the key safety messages highlighted by a particular incident where we have decided not to publish a full investigation report.
We will publish a safety digest (and not a full investigation report) for any of the following reasons:
- the safety learning has already been (or will be shortly) covered by a safety recommendation in an investigation report
- the safety learning mainly relates to compliance with existing rules, procedures or standards
- the safety learning has a narrow application
During 2017, we started 14 safety digests and published 19 on our website. Details are included in Appendix C.
Chart 1 gives a breakdown of the total number of investigations and bulletins/safety digests started, by type of accident, for the five year period 2013 – 2017.
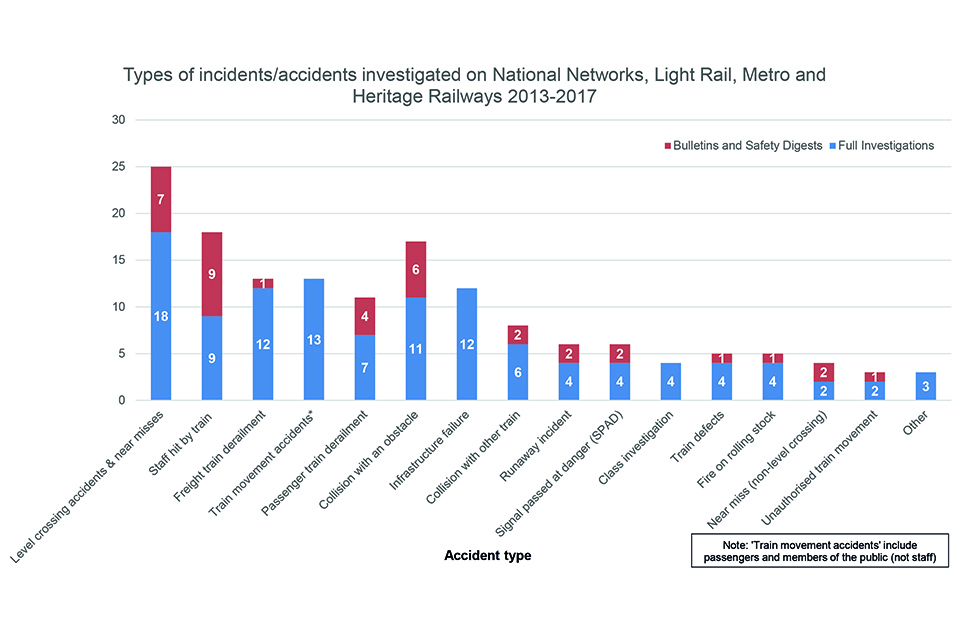
Bar graph showing number of full investigations and bulletins/safety digests started by type of accident
2.4 Urgent safety advice
We can issue urgent safety advice at any stage during an investigation when we believe there is a need to provide immediate information to the relevant industry bodies about the wider safety issues that have been identified. If the issue affects other European Union member states the safety advice is reported to ERA via their safety information system; this action alerts all member states to the advice. During 2017 we issued urgent safety advice on three occasions. All three were UK specific and therefore they were not sent to ERA.
Table 2 – Urgent safety advice issued by RAIB in 2017
| Incident date | Incident | Urgent safety advice | Date of USA |
|---|---|---|---|
| 01/04/2017 | Passenger collision with buffer stop at Preston station | Securing of refreshment trolley/disabled access ramp (See Appendix A of safety digest D10/2017) | 25/04/2017 |
| 28/07/2017 | Dangerous occurrence at Abergavenny station | Securing of overhead power cables at and around railway stations (See Appendix B of Report 06/2018) | 17/08/2017 |
| 23/10/2017 | Collision at Frognal Farm user worked level crossing | Signs at level crossings - Network Rail should urgently review the design and wording of the warning/instruction signs at user worked level crossings with power-operated gate opener equipment to ensure that the instructions are clear, and alert users to the nature and severity of the risks. | 07/11/2017 |
3. Recommendations
Our investigation reports make recommendations to improve safety and to prevent the reoccurrence of similar accidents.
In the 19 reports published in 2017, we made a total of 71 recommendations; the average number of recommendations per report was 4.
We direct recommendations to the organisation we think is best placed to implement the changes required (the ‘end implementer’). This includes railway, non-railway, private and public sector organisations. Each recommendation is sent to the appropriate safety authority[footnote 3] or public body.
The purpose of dealing with recommendations in this way is so that the safety authority can ensure that the ‘end implementers’ properly consider the recommendations, and where appropriate act on them, as the Directive and Regulations require. The Regulations give the safety authority (primarily ORR) the power to require end implementers to provide full details of the measures they intend to take, or have taken, to implement the recommendation.
The safety authority is also required to inform us, within a period not exceeding 12 months, of the measures taken, or the reasons why no implementation measures are being taken.
We have no statutory powers to follow up on the implementation of recommendations, unless it is necessary to do so as part of a subsequent investigation. However, ORR, other safety authorities, and other public bodies are required to report to us the actions taken.
Our website includes details of the response to our recommendations. These are contained in an Index of RAIB recommendations which captures the latest status of each recommendation (as reported to us by the relevant safety authority or public body). This also contains links to the full text of each recommendation.
A colour coded version of the index has also been produced to highlight the status of recommendations that were made or changed during 2017, or which remain open as at 31 December 2017.
These status reports are compiled from information provided to us by ORR, other safety authorities, or other public bodies, and the categories used are:
i. Implemented – all actions to deliver the recommendation have been completed
ii. Implemented by alternative means – the intent of the recommendation has been satisfied in a way we did not identify during the investigation
iii. Implementation ongoing – work to deliver the intent of the recommendation has been agreed and is in the process of being delivered
iv. Progressing – the relevant safety authority has yet to be satisfied that an appropriate plan, with timescales, is in place to implement the recommendation; and work is in progress to provide this
v. Non-implementation – recommendation considered and no implementation action to be taken
If we are still awaiting an initial report from the relevant safety authority or public body on the status of the recommendation we categorise it as ‘Awaiting Response’.
Chart 2 summarises the status of recommendations made between 1 January 2013 and 31 December 2017.
Chart 2 – Recommendation implementation status by year since 2013 (includes recommendations made to safety authorities and to public bodies).
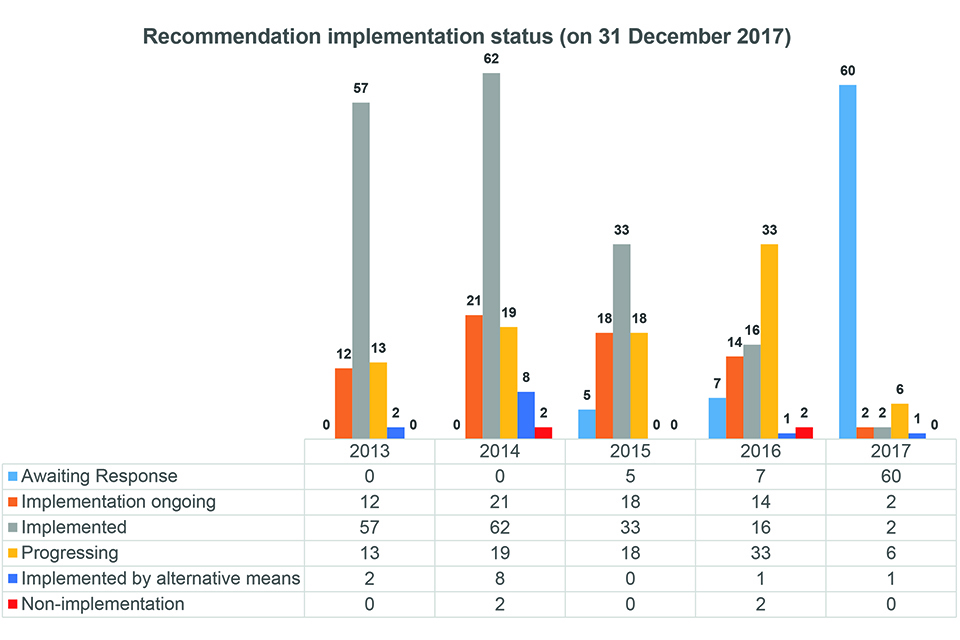
Bar chart showing status of recommendation for the years 2013, 2014, 2015, 2016 and 2017 as of 31 December 2017
Where we have concerns, based on risk, over the way that an organisation has responded to a recommendation, we raise these concerns with the relevant safety authority. The responses are marked with a coloured triangle in the Index. We may also add a comment and this will appear in the recommendation status report.
The triangles used are:
Red - We have particular concerns that no actions have been taken in response to a recommendation.
Blue - We are concerned that the actions taken are inappropriate or insufficient to address the risk identified during the investigation.
White - We note that substantive actions have been reported but we still have concerns.
Table 3 shows those recommendations where the status has changed during 2017, but we have concerns about the response.
Table 3 – Summary of recommendations of RAIB concern
| Investigation Name | Rec No | Topic | Concern | Triangle Colour |
|---|---|---|---|---|
| Track worker struck by train Grosvenor Bridge, London Victoria (19/2009). | 6 | Positions of safety for staff working on the live railway. | The recommendation, which is about track workers not using an adjacent line as a place of safety, has been closed on the basis of better decision-making by people with safety responsibility on site, especially safe work leaders. Therefore, the basis for closure is that selection and training of such personnel (who devise and implement safe systems of work) means it is less likely they will choose an inappropriate place of safety. Our view is that, to date, the evidence relating to safe work leaders does not strongly support this and it seems premature to close the recommendation, particularly as the safe work leader initiative is not being implemented as originally envisaged. | White |
| Accident to a track worker near Redhill (06/2015). | 3 | Actions to be taken by lookouts when their view towards approaching trains on one line is obscured by a passing train on another line. | This recommendation was concerned with a situation where a distant lookout, standing in the down side cess, had their view of any approaching up train obscured by a passing down train. It was not concerned with a situation where the distant and site lookouts had lost sight contact with each other. The Network Rail briefing material cited as addressing the recommendation appears to focus on this latter situation, rather than the former as the recommendation intended. | Blue |
| Tram collision with pedestrian near Market Street, Manchester (06/2016). | 1 | Improvement of the processes providng for the welfare of staff involved in potentially traumatic events. | The recommendation addressed apparent gaps in Metrolink’s procedures. In response, Metrolink reviewed its procedures, decided they were fit for purpose, and re-briefed them. However, the RAIB remains unconvinced that the existing procedures do address the gaps identified. | White |
3.1 Examples of significant learning
Some of our investigations have contributed to enhancing industry’s understanding of specific areas of risk. We have made a number of wide ranging recommendations (and identified a number of learning points) this year which have the potential to reduce that risk. Examples include:
- Our investigation of an incident at Twyford (01/2017) raised concerns about wheelchairs and pushchairs being moved by trains passing through stations at speed. We have recommended the identification of mitigation measures and the issue of suitable guidance
- The investigation into the collision at Hockham Road level crossing (04/2017) raised concerns about the risk of signaller error at user worked crossings where the signaller needs to give permission for users to cross. We have recommended that Network Rail improves information for signallers. This issue is further discussed in section 4
- The recommendations made in the investigation into the near miss at Dock Lane level crossing (08/2017) addressed the need for reviewing the risk management process for signallers controlling telephone operated level crossings and for ensuring that signaller workload is maintained at acceptable levels. This issue is further discussed in section 4
- A recommendation arising from the investigation into the fatal accident at Woodbourn Road (13/2017) addressed the need to look further into pedestrian detection technology for trams to reduce the risk of collision between a tram and a pedestrian
- A recommendation made in the report on the investigation into a serious irregularity at Cardiff East Junction (15/2017) addressed the need for improvement in the management of fatigue risk during major projects. This issue is further discussed in section 4
- Our investigation into two near misses at Camden Junction South (16/2017) raised concerns about the risk faced by track workers being on track to place or remove possession limit boards or detonators. We have recommended a review of the possession management process. This issue is further discussed in section 4
- A recommendation made in the report on the collapse of a cutting wall at Liverpool (17/2017) addressed the need for Network Rail to enhance examination and assessment processes for walls with high potential safety consequences in the event of failure
- Recommendations made in the report on the overturning of a tram at Sandilands (18/2017) addressed gaps in the understanding of risk associated with tramway operation (particularly low frequency/high consequence events). We have recommended that the industry develop suitable measures to automatically reduce excessive tram speeds and to develop a system that monitors and detects driver inattention
3.2 Recommendations and reports published in 2017
Recommendations made in 2017 were directed at the following organisations (in some cases they were made to more than one such organisation):
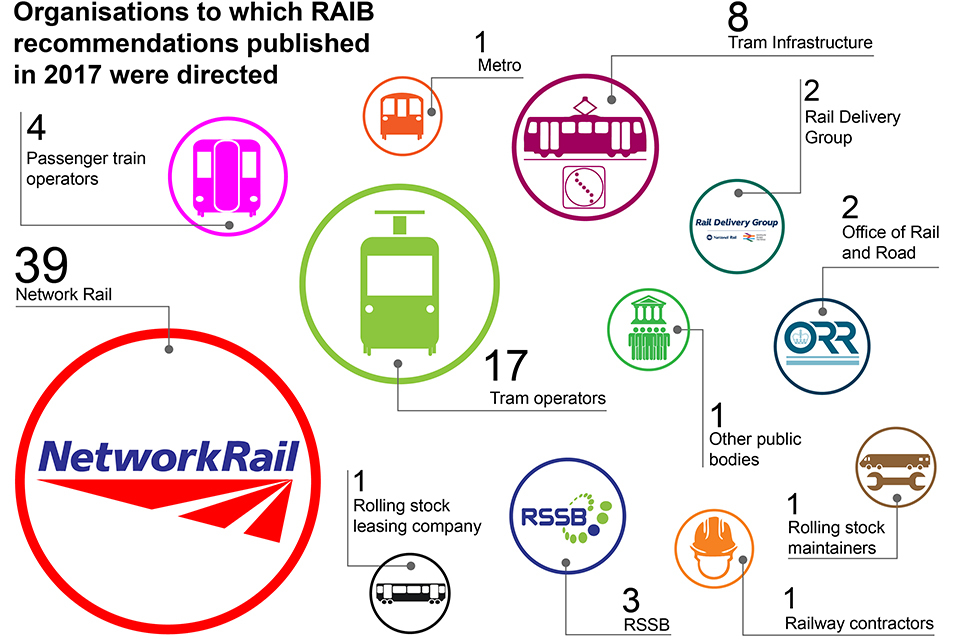
Recommendations and reports published in 2017. Organisations to which recommendations were directed are represented by differing sized circles.
4. Identification of important recurrent issues and areas of concern
The purpose of this section is to capture some important areas of safety learning that we identified during 2017. It is not intended to be comprehensive in scope but is focused on those areas which were either prominent during the year or of particular concern to us. The topics selected this year are:
- Reliance on signallers to ensure the safety of level crossing users
- Failures of structures and earthworks
- Safety of track workers
- Fatigue
- Errors during installation and commissioning of new infrastructure
4.1 Reliance on signallers to ensure the safety of level crossing users
Overview
The majority of accidents at level crossings are the consequence of misuse by members of the public. Misuse can be intentional (such as driving around closed barriers), or the result of a human lapse or mistake. It is encouraging to note the publicity campaigns that Network Rail has launched with the intention of making the public more aware of level crossing risk and encouraging safe behaviours, and the continued work of the British Transport Police to bring to justice those that deliberately flout the law.
However, a particular concern during 2017 has been the number of our investigations in which errors by signallers have been found to be causal. This illustrates that, despite the technology that protects train movements and the safety of users at many level crossings, there remains a risk that a single error by a signaller can still lead to a serious accident. In an environment where signal box control areas are becoming larger, and the number of crossings overseen by an individual signaller is increasing, there is a greater scope for signaller error unless the risk can be properly controlled. View a short video on the subject under the ‘details’ section.

Damage to the cab of the train involved at Hockham Road and the crossing at Thorney Marsh Lane. A quote from RAIB's press release is given in green text.
Relevant accidents
The reports published in 2017 into accidents/incidents involving staff error fell into two distinct sub-categories:
a. signallers authorising road vehicles to cross a user worked crossing when trains are approaching
b. signaller error when automatic crossings are not operating normally
Three investigations fell into the first sub-category:
- Hockham Road (04/2017), collision of train with tractor and trailer at a user worked crossing
- Dock Lane (08/2017), signaller authorised user to cross the line at a user worked crossing when a train was approaching
- Thorney Marsh Lane (D02/2017), signaller authorised user to cross the line at a user worked crossing when a train was approaching
Two investigations fell into the second sub-category:
- Broad Oak (D13/2017), signaller cleared signals for a train movement over an automatic half barrier crossing which was still under local control
- Magdalen Road (D14/2017), signaller forgot to restore the auto-raise function of a manually controlled crossing to manual operation when authorising a train to pass a signal at danger due to a track circuit failure
Issues
- when authorising users to cross the line at a user worked crossing, safety is dependent on signallers correctly judging that there is sufficient time available before arrival of the next train
- in order to judge whether it is safe to grant permission for users to cross the line, signallers are reliant on the information displayed to them by the control system, their local knowledge and high levels of concentration
- at some locations answering calls from members of the public asking for permission to cross the line is a substantial workload for signallers
- personal factors such as fatigue can give rise to incorrect judgements or lapses
- automatic warning systems at user worked crossings have been taken out of service due to incomplete safety validation
- the need for signallers to lead conversations when conversing with persons who are seeking permission to cross the line at user worked crossings
- the need for signallers to take special care when equipment at level crossings is not working correctly due to maintenance activities or malfunction
Areas of recommendation
- a review of measures for addressing user worked crossing risk, such as:
- improved information for signallers to facilitate good decision making when judging whether it is safe for users to cross the line
- increased use of automatic warning equipment
- closure/replacement of user worked crossings (04/2017)
- improved systems to ensure that signallers are sufficiently trained and familiar with signalling/control equipment to remain competent to supervise user worked crossings (04/2017)
- assessing and reducing the risk of human error at signal boxes where signallers are required to respond to large numbers of calls from user worked crossings (08/2017)
- assessing the risk of error by a signaller when identifying appropriate improvement options at user worked crossings (08/2017)
4.2 Failures of structures and earthworks
Overview
We continue to be concerned about the risk posed by unexpected failure of structures and earthworks. Since many of the country’s railway structures date from the Victorian era it is becoming ever more important to monitor how they are withstanding the passage of time and the inevitable wear and tear. The gradual degradation of assets can be managed by periodic inspection and maintenance. It is the sudden unexpected failures, often associated with extreme weather events, which give rise to the most concern because of their potential to derail trains. View a short video on the subject under the ‘details’ section.
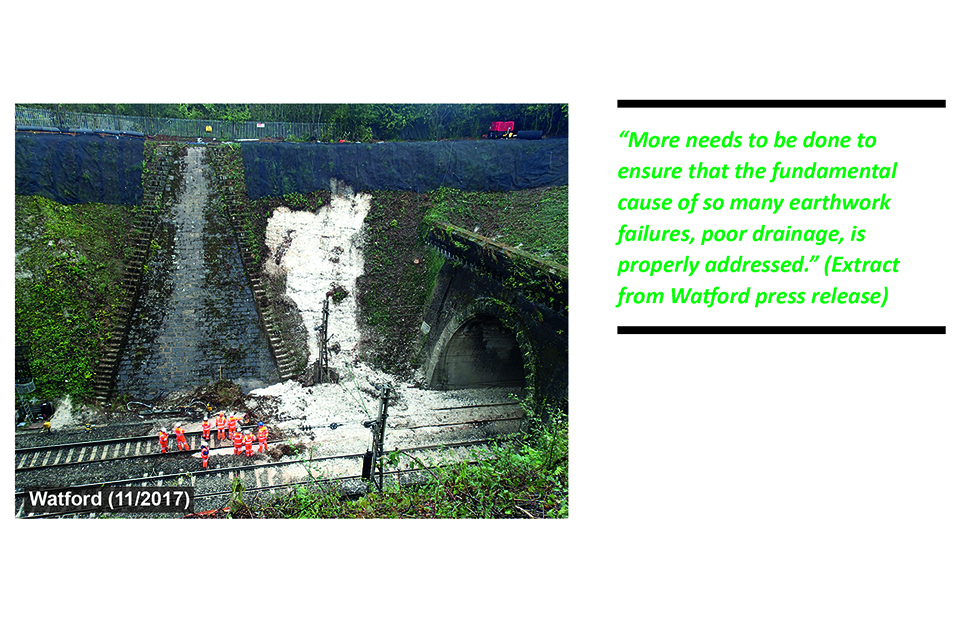
The collapsed embankment at Watford Tunnel, 2017 - Failures of structures and earthworks
Relevant accidents
The reports published in 2017 into accidents/incidents involving structural failure are:
- Barrow upon Soar (10/2017), damage to a water main which caused a partial collapse of an overline bridge onto a line that was open to traffic
- Liverpool (17/2017), collapse of a wall at the top of a rock cutting onto the track below
The reports published in 2017 into accidents/incidents involving earthwork failure are:
- Baildon (03/2017), train ran over unsupported track following washout of ballast
- Watford (11/2017), train struck landslip, derailed and was hit a glancing blow by a train in the opposite direction
Issues
- insufficient identification and maintenance of drainage affecting the stability of cutting slopes (loss of structures and earthworks asset knowledge)
- poor communications between operating staff following reports of infrastructure failure and the inability of controllers to quickly convert addresses and post codes reported by members of the public into railway locations
- poor management of risk associated with water mains on bridges over the railway
- construction activities of a neighbour creating additional surcharge on a railway structure
Areas of recommendation
- improved response to emergency phone calls, including measures to translate geographic information provided by members of the public into track location information, so enabling the effective direction of responders to emergencies such as earthwork failures (03/2017)
- steps to ensure that asset management teams, and people undertaking work activities on bridges, have sufficient competence and information to manage the risk to structures arising from damage to utilities such as water pipes (10/2017)
- improved processes for identifying localised water concentration features which can give rise to landslips (11/2017)
- completion of a comprehensive survey of drainage assets to provide sufficient asset knowledge to adequately manage the risk of earthwork failures (11/2017)
- identification of walls that have a potentially high safety consequence should they fail (17/2017)
- improved examination and assessment procedures for high risk walls, including checks of changes in adjacent land use and greater use of open source data such as Google images (17/2017)
4.3 Safety of track workers
Overview
The railway industry has come a long way in reducing the harm caused to those working on or near the line. It is now four years since a track worker was last killed by a moving train. The overall level of harm to track workers has been steadily dropping since the 1980s. Factors that have led to this improvement probably include the increased mechanisation of routine maintenance (so reducing the number of people working on or near the line), a reduction in number of activities that are undertaken ‘between trains’ and improved working practices.
However, in common with much of the industry, we remain concerned about the number of narrowly avoided collisions between trains and track workers. View a short video on the subject under the ‘details’ section.

In cab FFCCTV from Shawford and Raynes Park - Safety of track workers
Relevant accidents
The reports published in 2017 into accidents/incidents involving track workers are:
- Shawford (05/2017), narrowly avoided collision between a train and a track worker
- Class investigation (07/2017), into accidents and near misses involving track workers outside possessions
- Surbiton (D06/2017), narrowly avoided collision between a train and a track worker acting as lookout
- Great Chesterford (D12/2017), narrowly avoided collision between a train and track workers
- Dutton viaduct (D18/2017), narrowly avoided collision a express train and a group of track workers
- Raynes Park (D19/2017), lookout struck by passing train (causing minor injuries)
- Camden Junction South (16/2017), train signalled into a possession encountering two track workers who were in the process of placing boards and detonators
- Egmanton, narrowly avoided collision between a train and a group of track workers (5 October 2017, investigation ongoing)
Issues
- loss of safety discipline and vigilance on site
- distraction of those with safety duties by the work activity
- poor adaptation to circumstances that differ from the plan
- weak safety leadership on site and an unwillingness to challenge unsafe systems of work
- the dangers of adopting unauthorised systems of work
- the inappropriate use of generic systems of work covering long lengths of track to cover a single activity at a specific location
- the need for planning that is appropriate to the location and the task that is to be undertaken, including proper consideration of safe access routes
- the potentially catastrophic consequences of placing lookouts at the wrong location (eg with insufficient sighting of approaching trains)
- loss of information during the implementation of a possession that spanned more than one signalling workstation (processes for managing and communicating information associated with possessions are not optimised for modern, multi-panel signalling centres)
- the need for track workers with a safety critical role to have sufficient local knowledge to work safely
Areas of recommendation
- steps to ensure that excess work load and lack of resources do not compromise the safety of track workers (05/2017)
- a review of why gross non-compliances with systems for managing the safety of people working on or near the line were not detected by a Route’s audit and self-assurance systems (05/2017)
- improved processes for the implementation of possessions in signal boxes and control centres with multiple workstations, and a review of the way information is displayed in the Weekly Operating Notice (16/2017)
- a review of ways of reducing the need for staff to be on the track for the purpose of taking or giving back a possession (including consideration of technologies such as remotely operated track circuit operating devices) (16/2017)
- improvements in procedures and/or training for those in leadership roles to be able to adapt to changes in circumstances (07/2017)
- improvements to the training of track workers in non-technical skills (07/2017)
- changes in the competence requirements for people who lead track work in higher-risk situations, including knowledge of the location (07/2017)
- making location-specific photographic and video information more easily available to staff involved in planning and leading work on the track (07/2017)
- improvements in the collection, analysis and reporting of information on incidents involving track workers (07/2017)
We continue to urge that more be done to minimise the exposure of track workers to the risk of being struck by a train and are therefore supportive of existing initiatives to reduce the amount of work that is carried out on lines that are still open to traffic. However, sometimes there is no reasonable alternative to working on lines that are still open to traffic. For this reason we have recommended that, while continuing to work towards improving the planning of track engineering activities, it is also necessary for Network Rail to explore ways to better equip competent people to make safe decisions, within clearly defined guidelines, when the plan is no longer appropriate to the situation (07/2017).
4.4 Fatigue
Overview
Human fatigue is usually related to a lack of sleep. Although no one doubts the impact it can have on human performance in general, it can be very difficult to prove its role in any given accident. Nevertheless, it is identified as a possible factor in many of the accidents and incidents that we have investigated including the overturning of tram 2551 at Croydon on 9 November 2016.
Most people need seven to eight hours sleep each night, so the avoidance of fatigue is about having had enough good-quality sleep over a given period to get through to the end of the shift. The responsibility for managing this lies with both employers and employees.
Employers are required by law to manage the fitness of their staff who carry out safety critical work, and most companies who rely on shift work do this by having policies governing how work is scheduled, including limits on working hours, requirements for shift rotation and minimum times between successive shifts. Good fatigue management also gives employees training about fatigue, and encourages people to report if they feel unfit for duty because of fatigue.
Employees also have a responsibility to manage their own lives to minimise the risk of fatigue. This can be difficult when balancing the demands of family life and other commitments and interests beyond work. View a short video on the subject under the ‘details’ section.
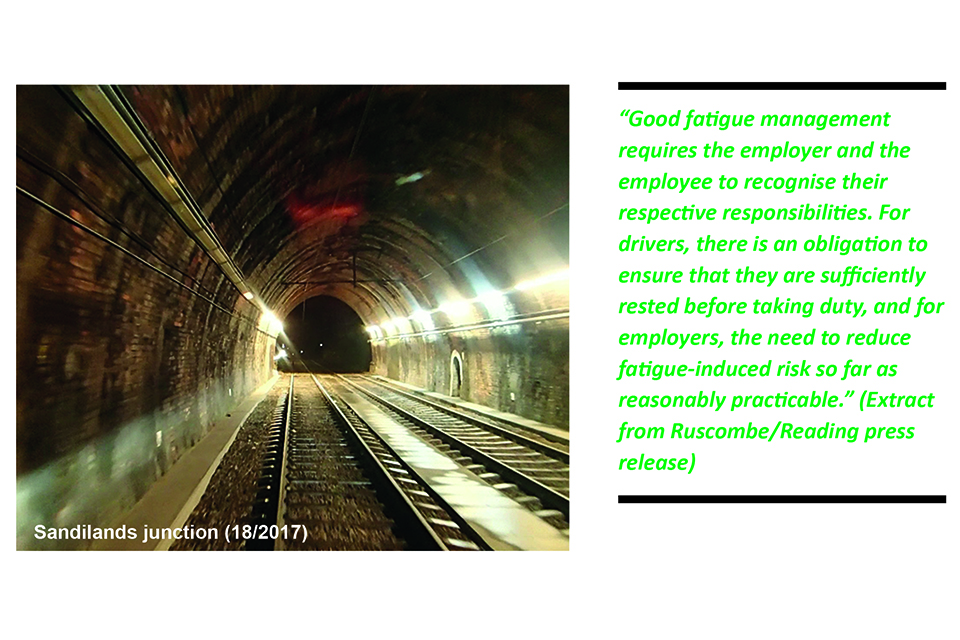
View of the two line inside the illuminated tunnel at Sandilands - Fatigue
Relevant accidents
The reports published in 2017 into accidents/incidents in which fatigue may have played a role include:
- Hockham Road (04/2017), collision of train with tractor and trailer at user worked crossing
- Shawford (05/2017), narrowly avoided collision between a train and track worker
- King’s Cross (D15/2017), buffer stop collision
- Cardiff East Junction (15/2017), points disconnected during commissioning of new signalling and track layout and left unsecured in the wrong position
- Camden Junction South (16/2017), train signalled into a possession encountering two track workers who were in the process of placing lights and detonators
- Sandilands junction (Croydon) (18/2017), tram entered a tight radius curve and overturned, killing seven and seriously injuring nineteen people
Issues
- during the year we have identified a number of factors that can contribute to impaired human performance due to fatigue:
- a series of long shifts on consecutive days
- inadequate sleep due to personal factors (such as family commitments) or inappropriate sleep patterns
- working a first night shift
- a long working hours culture associated with the installation and commissioning of a major project
- fatigue management systems that were not in line with published industry guidance
Areas of recommendation
- improvements to fatigue management systems for safety critical staff, including consideration of journeys before and after work (05/2017)
- improved management of fatigue risk during major projects (15/2017)
- improved management of fatigue risk, including enhanced guidance to staff on the steps they should take to reduce the risk of fatigue affecting their performance (18/2017)
4.5 Errors during installation and commissioning of new infrastructure
Overview
Major projects to upgrade the railway and improve the infrastructure are welcome and necessary to meet increasing demands for rail services. These projects can be complex, executed over long periods of time and sometimes need to take place alongside other parts of the railway that remain open to traffic. The nature of complex railway projects is that they generate additional risk for those who work on them (referred to in the section on fatigue) and for the operational railway that is affected by them. Such risk occurs both while the project is being undertaken and at the point where the project hands back upgraded infrastructure for normal operations. It is important that project risk is managed effectively and safe working practices are followed. We continue to be concerned about how such projects are managed and whether the lessons learned from the tragedies of the past are still being applied effectively on the railway.
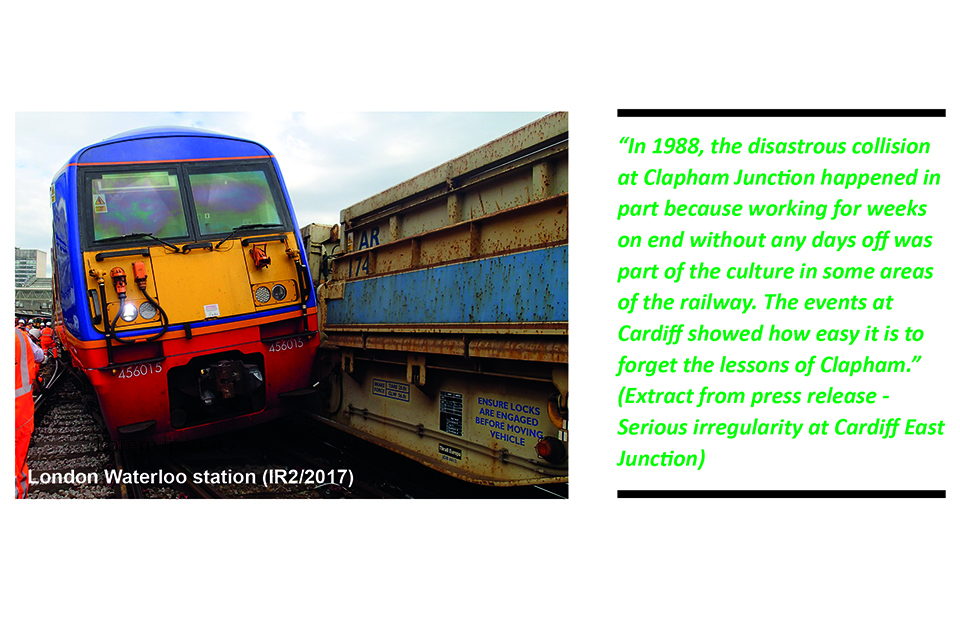
The derailed vehicle at London Waterloo station - Errors during installation and commissioning of new infrastructure
Relevant accidents
The reports published in 2017 into accidents/incidents relevant to the management of risk associated with the installation and commissioning of new infrastructure are:
- Cardiff East Junction (15/2017), points disconnected during commissioning of new signalling and track layout but left unsecured in the wrong position
- London Waterloo station (IR2/2017), route set and signal cleared for a departing train which then ran into the side of wagons protecting adjacent major engineering work
- Kirkham (D11/2017), a tamper leaving an engineering possession after completion of work encountered a large tubular steel pile obstructing the track
Issues
- insufficiently thorough project management arrangements and project governance
- where possible installing new infrastructure in accordance with the design intent
- the safety of the design process for modifications made during engineering works
- the effectiveness of the process for checking and identifying errors
- training, competence, working hours and fatigue management for designers, checkers, and testers
- management factors and organisational culture
- safety briefings, transfer of information and communication
- development of a suboptimal work group culture
Areas of recommendation
- steps to ensure that projects are appropriately held to account by the assurance process external to the project, and follow good practice throughout (15/2017)
- improved document management systems so that documents are easily identified, retrieved, traced and updated as necessary (15/2017)
- improvement to fatigue risk management in the project environment, particularly in relation to major projects (15/2017)
5. Other activities and information about RAIB
5.1 National Investigation Body Network
We continue to participate in the European Union (EU) network of National Investigation Bodies (NIB).
As a result of the recent changes to the Directive we are now working with a number of other NIBs to develop:
a) a peer review process
b) the improved sharing of knowledge between NIBs
In addition, we are working with the NIBs and ERA to improve the management of plenary meetings and to establish mechanisms for co-operation.
Some years ago we were also invited to participate in the Nordic regional grouping of NIBs and we continue to be an active member of this group too.
5.2 International Transport Safety Association conference
On 24-27 September 2017 our Chief Inspector attended the International Transport Safety Association conference in Japan. Representatives from 16 countries attended, including USA, Canada, Australia, Japan and South Korea.
The Association is composed of the independent investigation boards from countries around the world and its mission is to improve transport safety in each member country by sharing information and learning from the experience of others.
5.3 Rail accident investigators’ good practice seminar
In October we facilitated a seminar for accident investigators working in the UK heavy rail industry. The seminar was hosted by Network Rail at the Westwood development centre in Coventry and was attended by over 140 people. The day was made up of a number of presentations on topics such as fatigue, causal analysis, safety culture and report writing and also included discussions and the opportunity for delegates to propose ideas and raise problems they faced carrying out investigations.
Simon French, RAIB's Chief Inspector talking about Safety culture and SMS at the Rail accident investigators’ good practice seminar
5.4 Stakeholder survey
During October and November 2017 ComRes, the opinion research consultancy, undertook a stakeholder survey on our behalf. It primarily covered perceptions of us as an organisation and the value we provide to the railway industry. The survey comprised a questionnaire which was sent to a representative sample of railway industry managers who were judged to be either key decision makers, or likely to advise those making safety decisions. Responses to the survey were anonymous. Of the 223 stakeholders invited to take part, 118 responded.
The principal findings from the survey are described in the Chief Inspector’s review of 2017 at the beginning of this report. Read the full survey.
5.5 RAIB’s own safety record
We provide an operational response to railway accidents and incidents, which vary in nature, scale and environment. These operations often present significant health and safety risk to our staff and to people working alongside us. To counter this risk, we have developed and implemented our own Safety Management System (SMS). It includes our health and safety policy and arrangements for the management of risk. It also sets out a system for the ‘real-time’ assessment of risk by means of a process known as Dynamic Risk Assessment.
We monitor our own health and safety performance as an integral part of our management and governance processes. This includes a Health, Safety and Welfare committee which is chaired by the Chief Inspector. In 2017 we commenced the implementation of a trauma risk management process for our staff to ensure an effective post-incident response for those exposed to potentially traumatic events.
Four minor injuries to our staff were reported during 2017. Each of these were recorded and investigated.
5.6 Funding
For the 2017-18 financial year, our budget was £4.8m.
5.7 Chief Inspectors’ Board
This board was established in 2003 by the Secretary of State in the Department for Transport and consists of the three Chief Inspectors of accident investigation (Rail, Marine and Air). The Board meets at least quarterly to identify and develop common strategic issues to improve independent accident investigation in the UK.
This allows the Chief Inspectors to maintain operational independence and reporting of safety matters to the Secretary of State while benefiting from all three Accident Investigation Branches working together.
6. Appendices
6.1 Appendix A – Events that could have led to a serious train accident if circumstances had been slightly different
We consider that a multiple fatality accident was narrowly avoided in 3 events which were described in investigation reports published in 2017.
| Investigation name and event date | Report Number | Incident details |
|---|---|---|
| Partial bridge collapse onto open lines at Barrow-upon-soar, Leicestershire, 01/08/2016. | 10/2017 | A bridge over the Midland Main Line partially collapsed and a large volume of masonry fell onto the railway lines below. The bridge was closed to the public when the collapse occurred, but the railway lines below were open to traffic. |
| Derailment due to a landslip and subsequent collision, Watford, 16/09/2016. | 11/2017 | A southbound passenger train collided with a landslip and derailed at 70 mph (112 km/h). The derailed train continued into the tunnel, partly blocking the adjacent line. Less than one minute later, it was struck by a northbound train which did not derail. |
| Partial collapse of a wall onto open railway lines, Liverpool, 28/02/2017. | 17/2017 | Part of a wall at the top of a cutting above railway lines collapsed. Around 170 tonnes of masonry and other debris fell onto the tracks in the cutting. |
6.2 Appendix B – Full investigations completed and commenced in 2017
Details of all RAIB investigations published during 2017 are given in Table B1 and details of all investigations commenced during 2017 are included in Table B2.
The RAIB classifies its investigations according to Article 19 of guidance published by ERA to promote consistent categorisation of investigations in accordance with the Directive. The classifications are:
- Article 19(1) - a serious accident where the investigation is mandatory
- Article 19(2) - an accident or incident, which under slightly different conditions might have led to a serious accident, ie a narrowly avoided serious accident
In both tables, all investigations commenced under article 19(2) were undertaken on the basis of the potential or actual seriousness of the accident or incident; the schedule 19(1) threshold was not reached.
Summary details of open investigations can be can be found on our website under the link to ‘Current investigations’.
Table B1 – Full investigations completed in 2017
| Report Number | Event date | Publication date | Title of investigation (location) | Occurrence type | Basis for investigation |
|---|---|---|---|---|---|
| 01/2017 | 07/04/2016 | 19/01/2017 | Occupied wheelchair contacting a passenger train at Twyford station | Near miss rolling stock in motion | 19(2) |
| 02/2017 | 03/04/2016 | 13/02/2017 | Collision at Plymouth station | Train collision | 19(2) |
| 03/2017 | 07/06/2016 | 16/02/2017 | Trains passed over washed out track at Baildon, West Yorkshire | Structural failure | 19(2) |
| 04/2017 | 10/04/2016 | 14/03/2017 | Collision between a train & tractor at Hockham Road UWC | Train collision with an obstacle | 19(2) |
| 05/2017 | 24/06/2016 | 24/03/2017 | Near miss between a train and a track worker at Shawford | Near miss rolling stock in motion | 19(2) |
| 06/2017 | 15/08/2016 | 05/04/2017 | Fatal accident near David Lane tram stop | Accidents to persons caused by RS in motion | 19(2) |
| 07/2017 | 02/02/2016 | 13/04/2017 | Class investigation into accidents and near misses involving track workers outside possessions | Class investigation | |
| 08/2017 | 14/06/2016 | 03/05/2017 | Near miss at Dock Lane level crossing | Level crossing incident | 19(2) |
| 09/2017 | 07/08/2016 | 25/05/2017 | Fatal accident involving a train passenger near Balham | Accidents to persons caused by RS in motion | 19(1) |
| 10/2017 | 01/08/2016 | 06/06/2017 | Partial bridge collapse onto open lines at Barrow-upon-Soar, Leics | Structural failure | 19(2) |
| 11/2017 | 16/09/2016 | 10/08/2017 | Derailment due to a landslip and subsequent collision, Watford | Train collision with an obstacle | 19(2) |
| 12/2017 | 06/02/2017 | 21/09/2017 | Dangerous train door incident at Bank station on the Docklands Light Railway | Accidents to persons caused by RS in motion | 19(2) |
| 13/2017 | 22/12/2016 | 27/09/2017 | Fatal collision between tram and pedestrian at Woodbourn Road, Sheffield | Accidents to persons caused by RS in motion | 19(1) |
| 14/2017 | 05/10/2016 | 26/10/2017 | Fatal accident at Alice Holt footpath crossing, Hampshire | Level crossing accident | 19(1) |
| 15/2017 | 29/12/2016 | 30/10/2017 | Serious irregularity at Cardiff East Junction | Operational error | 19(2) |
| 16/2017 | 28/02/2017 | 27/11/2017 | Track worker near miss incidents at Camden Junction South | Near miss rolling stock in motion | 19(2) |
| 17/2017 | 28/02/2017 | 30/11/2017 | Partial collapse of wall onto open railway lines, Liverpool | Structural failure | 19(2) |
| 18/2017 | 09/11/2016 | 07/12/2017 | Overturning of a tram at Sandilands junction, Croydon | Tram overturning | 19(1) |
| 19/2017 | 20/03/2017 | 13/12/2017 | Freight train derailment at East Somerset junction | Train derailment | 19(2) |
Table B2 - Full investigations commenced in 2017
6.3 Appendix C – Safety digests completed or commenced in 2017
Safety digests are intended to share the key safety messages highlighted by a particular incident where we have decided not to publish a full investigation report. Table C1 includes all safety digests that were completed or commenced 2017.
Table C1 Safety digests completed or commenced in 2017
| Event date | Publication date | Digest number | Title of the investigation (location) |
|---|---|---|---|
| 30/10/2016 | 11/01/2017 | 01/2017 | Runaway and derailment of a locomotive at Toton sidings, Nottinghamshire |
| 26/11/2016 | 25/01/2017 | 02/2017 | Near miss at Thorney Marsh Lane level crossing, Castle Cary, Somerset |
| 07/12/2016 | 31/01/2017 | 03/2017 | Collision between a train and an engineering trolley, Stowe Hill Tunnel |
| 05/11/2016 | 23/02/2017 | 04/2017 | Charter train derailment near Southampton Eastern Docks |
| 29/11/2016 | 02/03/2017 | 05/2017 | Near miss with a pedestrian, Trinity Lane footpath crossing, Waltham Cross, Hertfordshire |
| 02/11/2016 | 06/03/2017 | 06/2017 | Near miss at Surbiton, south-west London |
| 16/02/2017 | 08/05/2017 | 07/2017 | Track workers struck by ballast near Chathill, Northumberland |
| 20/02/2017 | 18/05/2017 | 08/2017 | Trains struck a location cabinet door in Chipping Sodbury Tunnel |
| 06/04/2017 | 20/06/2017 | 09/2017 | Near miss with track workers at Ascot, Berkshire |
| 01/04/2017 | 21/06/2017 | 10/2017 | Passenger train collision with buffer stop at Preston station |
| 15/05/2017 | 08/08/2017 | 11/2017 | Near miss between a tamper and steel pile near Kirkham, Lancashire |
| 21/04/2017 | 09/08/2017 | 12/2017 | Near miss with track workers between Audley End and Great Chesterford |
| 29/06/2017 | 13/09/2017 | 13/2017 | Dangerous occurrence at Broad Oak level crossing near Canterbury, Kent |
| 09/08/2017 | 19/10/2017 | 14/2017 | Near miss at Magdalen Road level crossing |
| 15/08/2017 | 23/10/2017 | 15/2017 | Collision with buffer stops at King’s Cross station, London |
| 25/08/2017 | 01/11/2017 | 16/2017 | Collision between passenger train and trolleys near Clapham, North Yorkshire |
| 20/08/2017 | 22/11/2017 | 17/2017 | Passenger train derailment, London Paddington |
| 18/09/2017 | 04/12/2017 | 18/2017 | Near miss between train and workers on Dutton Viaduct, Cheshire |
| 22/08/2017 | 14/12/2017 | 19/2017 | Track worker struck by a train near Wimbledon, south-west London |
| 06/11/2017 | 07/02/2017 | 01/2018 | Derailment of a passenger train near Wimbledon station, South West London |
-
‘Serious accident’ refers to any train collision or derailment of trains, resulting in the death of at least one person or serious injuries to five or more persons or extensive damage to rolling stock, the infrastructure or environment, and any other similar accident with an obvious impact on railway safety regulation or the management of safety. ↩
-
Figures do not include class investigations (which address more general safety issues). ↩
-
The safety authority is the safety regulator; for Great Britain this is primarily ORR although there are some recommendations we made where the Health and Safety Executive has been the safety authority (for factors relating to accidents that were outside the control of the railway, and were the responsibility of other organisations to which the Health and Safety at Work etc Act 1974 applies); for the Channel Tunnel it is the Intergovernmental Commission and for Northern Ireland it is the Department for Infrastructure. ↩