
Collision between a passenger train and trolleys near Clapham, North Yorkshire, 25 August 2017
Published 1 November 2017

© Crown copyright 2017
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/safety-digest-162017-clapham/collision-between-a-passenger-train-and-trolleys-near-clapham-north-yorkshire-25-august-2017
1. Important safety messages
This accident highlights the importance of a COSS rebriefing the workgroup whenever there is a change to their system of work. As well as helping to ensure that the work group understands the change, the process of rebriefing provides an opportunity for the COSS to think carefully about the circumstances on site and for the work group to point out any mistakes the COSS may have made.
2. Summary of the accident
At 09:24 hrs on 25 August 2017 a passenger train collided with three engineering trolleys on the Settle Junction to Carnforth line between Giggleswick and Clapham, in North Yorkshire. The train, 2H08, the 08:18 hrs Northern service from Leeds to Morecambe was travelling on the Down branch line (referred to as the ‘down line’ in this safety digest) at 34 mph (55 km/h). Prior to the collision Network Rail staff had been working on both lines between Settle Junction and Carnforth, moving and positioning sleepers in the cess of the down line, ready for overnight track maintenance work.
The collision caused damage to the train, trolleys, sleepers and track. No staff, passengers or crew were injured.

View of the front of train after collision with the trolleys. The trolley is under the train. Railway staff in high visibility clothing are standing next to the train. a
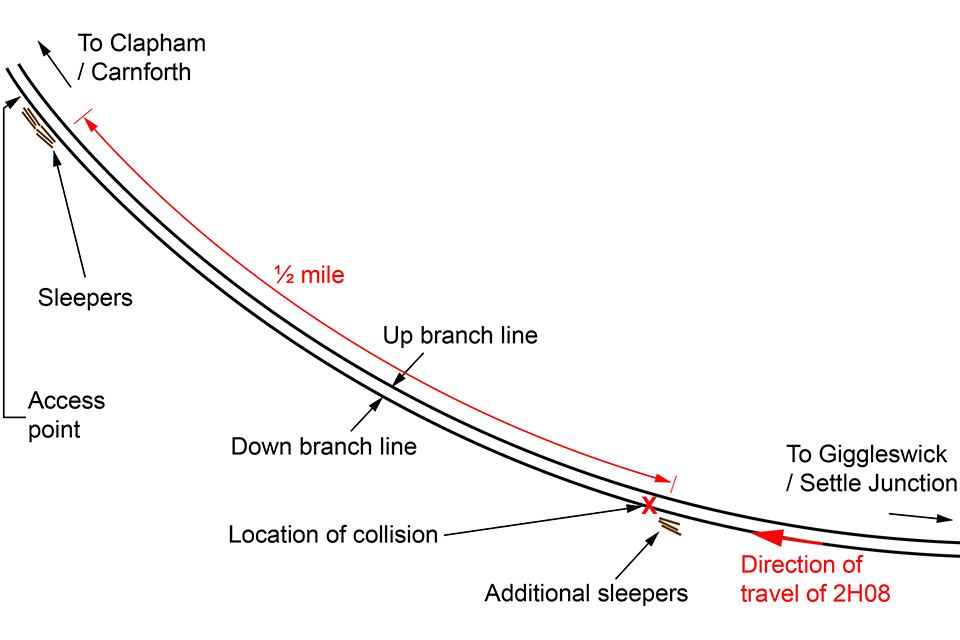
Schematic diagram of the area showing the locations of the access point and the point of collision. The path of train 2H08 is also marked.
3. Cause of the accident
The train struck the trolleys because the Controller of Site Safety (COSS) had an incorrect understanding of which of the two lines was the down line when he handed it back to the Protection Controller (PC), who was communicating with signallers to arrange protection for various works which were taking place on the route that morning.
On the day, Network Rail staff were to move and position sleepers in the cess of the down line. The safe system of work pack (SSOWP) for the work included two separate safe systems of work, namely a full line blockage on both lines; and a blockage of only the down line with a site warden protecting against straying towards the up line.
At 08:28 hrs the PC confirmed to the COSS that the signaller had granted a blockage of both lines and that detonator protection had been placed at the protecting signals. They agreed a call-back time of 09:10 hrs. The COSS noted that the down line would need to be handed back at that time, and the Up branch (referred to as the ‘up line’ in this safety digest) at 11:00 hrs.
The COSS briefed the workgroup on the safe system of work at the access point at Laneside, near Clapham, where they entered the railway. He decided that the trolleys would be placed on the down line to avoid having to carry sleepers the further distance across to the up line, even though this would require unloading and removal of the trolleys to allow trains to pass on the down line when it was handed back.
The group then proceeded towards Settle, picking up additional sleepers. At 09:05 hrs, after the work group had travelled ½ mile, the PC contacted the COSS as planned to arrange hand back of the down line. The line blockage was to remain on the up line. Although the COSS directed the workgroup to retire to the down cess, he did not instruct them to remove the trolleys from the line.
This configuration was not covered by either of the safe systems of work in the SSOWP. However, the level of protection offered was equivalent to one of the prescribed systems, and NR/L2/OHS/019 (Safety of people working on or near the line) allows a COSS to vary the arrangements as necessary to establish an appropriate safe system of work and implement it, as long as it offers at least the same level of protection as a planned safe system of work.
It is not clear whether the COSS informed the workgroup about which of the two lines he had handed back. Witness evidence suggests that he may have simply reported that a line was being handed back without making specific reference to the down line.
Having varied the arrangements to the prescribed safe systems of work, the COSS should have documented the changes on the Record of Arrangements and Briefing Form (RT9909), rebriefed the entire workgroup, checked their understanding and obtained their signatures on the RT9909 form.
For reasons that remain unknown, the COSS formed a belief that the trolleys were on the up line. He therefore handed the down line back to the PC, as requested. Because the other members of the workgroup had not been fully rebriefed, they were not in a position to correct the COSS. The COSS was familiar with the area and the naming of the two lines. The RAIB has concluded that his competence and knowledge did not contribute to this accident. Previous investigations demonstrate that even experienced workers can be become confused about which line is which when working on site.
There is no evidence that the limitations of the safe systems of work included in the SSOWP contributed either.
Having made sure that the sleepers on the trolleys were not foul of the adjacent line, the workgroup waited in the down cess. They expected the train to pass by on the clear up line 20 minutes later.
The train, a two-car class 142 with 28 passengers on board, approached the site of the trolleys on the down line at 58 mph (93 km/h). The driver sounded the train’s horn in response to a whistle board on the approach to a footpath crossing located about 178 metres from the trolleys.
Realising the potential for a collision, one of the track workers attempted to warn the train driver by signalling with his arms. The driver reacted by applying the train’s emergency brake. The speed of the train was reduced to 34 mph (55 km/h) at the point of collision.
The train struck the trolleys and sleepers. One trolley and several sleepers became wedged underneath the front of the train. The train came to a stop 108 metres beyond the point of collision.
4. Previous similar occurrences
The RAIB has in the past been notified of several incidents where engineering trolleys have been left on the line and struck by trains. It has investigated incidents in which COSS’s and other track workers have lost situational awareness while on the railway, in particular where confusion has arisen as to the line on which they were working. It has also investigated incidents that have arisen as a result of inadequate communications on site. However, none of the previously identified safety learning is directly relevant to the cause of this incident.
You can print this safety digest.