HPR volume 20 issue 5: news (28 May and 4 June 2026)
Updated 30 July 2026

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/health-protection-report-volume-20-2026/hpr-volume-20-issue-5-news-28-may-2026
Annual STIs and chlamydia screening data release (England)
The UK Health Security Agency (UKHSA) annual data release on sexually transmitted infections (STIs) in England shows that, overall, diagnoses fell by 8.3% between 2024 and 2025 (from 364,261 to 334,151), including infectious syphilis diagnoses in gay and bisexual men, which fell to their lowest level since 2016 (1).
The 2025 data also shows:
- a 13.5% overall decrease in infectious syphilis diagnoses — from 9,553 in 2024 to 8,262 in 2025
- a 10.9% decrease in gonorrhoea cases in all groups — from 71,766 in 2024 to 63,943 in 2025
- a 7.3% decrease in first episode genital warts in all groups — from 25,106 in 2024 to 23,282 in 2025
Despite the overall decrease in infectious syphilis, there was a 4.8% increase in diagnoses in heterosexual women — from 838 in 2024 to 878 in 2025.
The most commonly diagnosed STIs in 2025 were chlamydia (45.2% of all new STI diagnoses, 151,163), gonorrhoea (19.1%, 63,943), first episode genital herpes (8.6%, 28,779), and first episode genital warts (7.0%, 23,282) (see figure).
Breakdown of STI diagnoses in 2025 by disease type

Chlamydia screening
Among young women aged 15 to 24, who are recommended to be screened through the National Chlamydia Screening Programme, there was a 9.4% decrease in the number of chlamydia tests carried out, from 604,143 in 2024 to 547,308 in 2025, and a 13.6% decrease in chlamydia diagnoses, from 53,408 in 2024 to 46,122 in 2025.
The decline in chlamydia screening is a concern. Dr Hamish Mohammed, consultant epidemiologist at UKHSA, said: “Chlamydia can cause pelvic inflammatory disease and infertility if left untreated, so sexually active young women are encouraged to test for chlamydia after sex with a new partner or annually” (2).
References
1. UKHSA (2026). Sexually transmitted infections and screening for chlamydia in England: 2025 report
2. STIs fall with syphilis among gay and bisexual men lowest in a decade UKHSA website news story, 2 June 2026
Gastrointestinal infections: annual reports for 2025
UKHSA has published updated gastrointestinal infections data comprising annual reports on disease caused, in England, by 3 key pathogens: salmonella, campylobacter and cryptosporidium (1,2,3) and, in England and Wales, by Listeria monocytogenes (4) .
Non-typhoidal salmonella cases saw a modest year-on-year increase in 2025 (10,406 cases compared with 10,389 in 2024) but the annual report notes that cases in 2025 were at the highest level seen in a decade: a long-term trend indicating “a reversal of previous progress and suggesting renewed upward pressure on incidence” (1).
Campylobacter cases showed a year-on-year decline, in absolute numbers. However, campylobacteriosis remains the most commonly-reported bacterial gastrointestinal infection, with nearly 70,000 laboratory-confirmed cases reported in 2025 (2).
Cryptosporidium cases fell 27.2% year-on-year, from 5,703 in 2024 to 4,149 in 2025. The 2025 figures are in line with levels seen before the pandemic, reversing the higher numbers recorded in 2023 and 2024. However, the latest figures show that the number of outbreaks associated with farm settings and lamb-contact events remain high, with 18 outbreaks reported in 2025 (3).
Compared to other foodborne GI diseases, listeriosis cases are relatively rare, with only 181 cases reported in England and Wales in 2025. However, the infection can cause bacteraemia, meningoencephalitis or severe sepsis in the elderly, immunocompromised or those with underlying chronic conditions. Due to the severity of infection and high case fatality rate, listeriosis is an important public health concern (4).
References
1. UKHSA (2026). Non-typhoidal salmonella data 2016 to 2025
2. UKHSA (2026). Campylobacter data 2016 to 2025
3. UKHSA (2026). Cryptosporidium data 2016 to 2025
4. UKHSA (2026). Listeriosis in England and Wales: summary for 2025
Shigella sonnei and non-typhoidal salmonella clusters (ex-Cape Verde): second update
This is an update to the previously published Health Protection Report describing an outbreak of Shigella sonnei associated with travel to Cape Verde. In this report we provide updated case numbers within the Shigella sonnei outbreak and provide further details following the identification of Salmonella clusters which have also been linked to travel to Cape Verde.
Since 1 October 2025, 164 confirmed Shigella sonnei outbreak cases have been identified (see figure), with cases falling within a Single Nucleotide Polymorphism (SNP) single linkage cluster based on whole genome sequencing (WGS), designated t10.2052, suggestive of a common source. Cases in this cluster declined after peaking in late October 2025 but continued to be reported through late 2025 and early 2026. As of 17 April 2026, there have been no further reported cases in this cluster since 19 February 2026 (the latest sample submission date is 4 February 2026).
Trend over time of Shigella sonnei outbreak cases based on sample submission date at reference laboratory

S. sonnei outbreak cases were resident across all regions in England (n=137), Scotland (n=13), and Wales (n=14). Cases ranged in age from <1 year to 81 years with a median age of 53 years. The age group most affected were those aged 50 to 59 years (n=62, 38%). Across all age groups, 70% (n=114) were female.
Evidence gathered to date suggests that this outbreak was associated with travel to Cape Verde. Of the 164 confirmed cases reported since 1 October 2025, 127 cases reported international travel – of which 122 (96%) travelled to Cape Verde, the majority to the Santa Maria and Boa Vista areas. For the remaining cases, travel information was not known.
This strain of S. sonnei does not have any genomic resistance determinants against common antimicrobials used to treat traveller’s diarrhoea.
Activity within clusters of non-typhoidal salmonellosis associated with travel to Cape Verde
In addition to the above-mentioned outbreak of Shigella sonnei in UK travellers associated with travel to Cape Verde, UKHSA has identified increased reports within the following 3 clusters of non-typhoidal Salmonella, identified using WGS, that are associated with travel to Cape Verde.
Salmonella Enteritidis (t5.8449)
A total of 84 cases have been reported in the Salmonella Enteritidis t5.8449 cluster since 1 October 2025, with cases peaking in January 2026. Cases were resident across England (n=74), Scotland (n=6) and Wales (n=4). Cases ranged in age from <1 to 79 years with a median age of 51.5 years. The age group most affected were those aged 60 to 69 years (n=21, 25%). Across all age groups, 52% (n=44) were male.
Evidence gathered to date suggests that this cluster is associated with travel to Cape Verde. Of the 84 confirmed cases reported since 1 October 2025, 64 cases reported international travel. Sixty (94%) of these travelled to Cape Verde, the majority to the Santa Maria and Boa Vista areas. For the remaining cases, travel information was not known.
Salmonella Enteritidis (t5.8255)
There have been increased reports of cases in this cluster, with 11 cases reported since 1 October 2025. Cases were resident across England (n=10) and Wales (n=1). Cases ranged in age from 22 to 93 years with a median age of 66 years. The age group most affected were those aged 60 to 69 years (n=5, 46%). Across all age groups, 55% (n=6) were male.
Evidence gathered to date suggests that this cluster may be associated with travel to Cape Verde. Of the 11 confirmed cases reported since 1 October 2025, 7 cases reported international travel – all cases travelled to Cape Verde. For the remaining cases, travel information was not known.
Salmonella Virchow (t5.712)
A total of 4 cases were reported since 1 October 2025. All cases were resident in England. Cases ranged in age from 21 to 59 years with a median of 41 years, all cases were female.
Evidence gathered to date suggests that this cluster is associated with travel to Cape Verde. Of the 4 confirmed cases reported since 1 October 2025, 3 cases reported international travel – of which, all cases travelled to Cape Verde. For the remaining case, travel information was not known.
Further information
UKHSA continues to liaise with ABTA and Cape Verde public health authorities to share information regarding investigations of these clusters. UKHSA works closely with the National Travel Health Network and Centre (NaTHNaC) to ensure appropriate advice is in place for UK travellers.
Travellers seeking advice can visit the NaTHNaC website TravelHealthPro for up-to-date travel health guidance, including specific information for Cape Verde: NaTHNaC – Cape Verde. Advice on traveller’s diarrhoea can be found here: NaTHNaC – Travellers’ diarrhoea
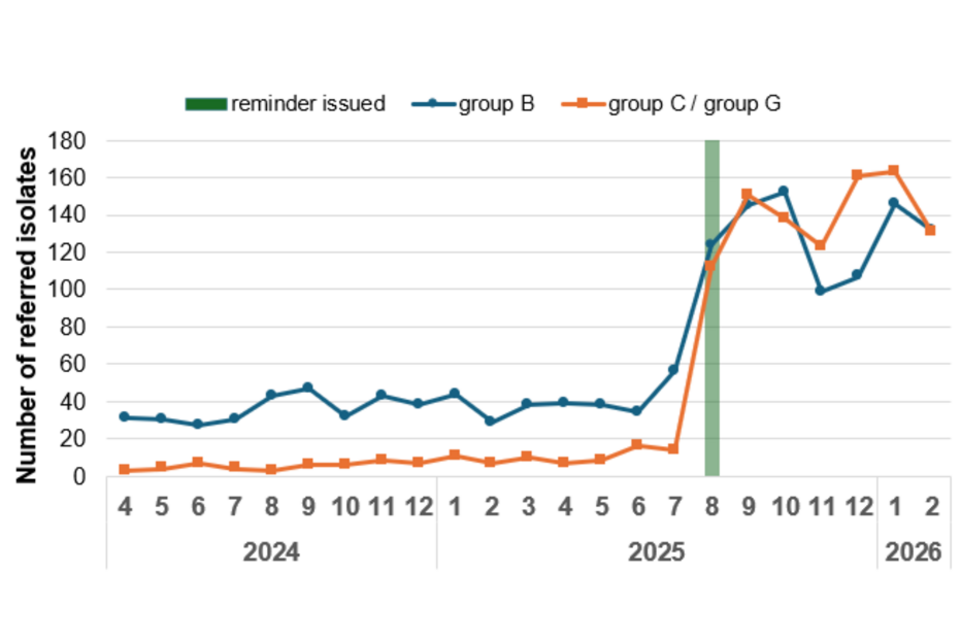
Referrals of beta-haemolytic streptococci isolates to UKHSA’s reference service
Following a UKHSA Briefing Note circulated to laboratories at the beginning of August 2025 reminding them of the recommendations (outlined in the Bacterial Reference Department manual) for referral of beta-haemolytic streptococci isolates from sterile sites, there has been a marked increase in the number of referrals to the UKHSA Staphylococcus and Streptococcus reference service (SSRS), Antimicrobial Resistance and Healthcare Associated Infections (AMRHAI) Reference Unit (1).
In the 6 months before the reminder was issued (February to July 2025) there was an average of 39 group B streptococcal (GBS) sterile site isolates referred per month, which increased by 234% to an average of 130 per month in the 6 months after (September 2025 to February 2026; see figure). Similarly, for group C/G streptococcal (GCGS) sterile site referrals, an average of 10 per month increased by 1,298% to 145 per month during the same time periods.
The collection and characterisation of these isolates aid:
- bacterial identification and typing
- genomic relatedness between isolates
- outbreak detection and management
- disease surveillance
- development of new vaccine targets and monitoring of future vaccine coverage.
The significant increase in referrals to UKHSA reference laboratories, prompted by the Briefing Note, was very welcome and the Agency acknowledges the importance of this and thanks laboratories for their engagement with the request.
Monthly group B and group C/G streptococcal sterile site referrals (England): April 2024 to February 2026
Prior to the UKHSA Briefing Note being issued, Group A streptococcal (GAS) sterile site isolate referral was routine for laboratories (1). However, GBS and GCGS sterile site referral had declined, motivating the reminder. Increasing the awareness of the recommendations, and of specimen referral rates, is particularly important as typing of isolates enhances surveillance, and informs outbreak detection, management and investigation. This is particularly important for GBS in the light of phase III GBS vaccine trials, and recent outbreaks of group B and group C/G streptococci in England (2,3).
The guidance highlighted within the UKHSA Briefing Note are:
- Bacterial Reference Department manual
- the UK Standards for Microbiology Investigations (UK SMI) ID4: Identification of Streptococcus species, Enterococcus species and morphologically similar organisms
- UK SMI B58: Detection of carriage of Group B Streptococci (Streptococcus agalactiae)
- the UK public health guidance for GAS in community and healthcare settings
In addition, GAS, GBS, and GCGS species exhibiting exceptional resistance phenotypes should be referred to the UKHSA Antimicrobial Resistance and Mechanisms Service, AMRHAI Reference Unit, for confirmation, that is, isolates that:
- are resistant to penicillin according to EUCAST clinical breakpoints v.15.0 (groups A, C/G: MIC >0.03 mg/L or zone diameter 0.125 mg/L or zone diameter <18mm)
- exhibit resistance to cephalosporins, vancomycin, teicoplanin, telavancin, dalbavancin, linezolid, tedizolid, quinupristin-dalfopristin or tigecycline
References
1. UKHSA (2025). ‘Referrals of group A, B, C and G streptococcal isolates to the Staphylococcus and Streptococcus Reference Section (SSRS)’ [internal document]
2. Collin SM, Lamb P, Jauneikaite E, le Doare K, Creti R, Berardi A, Heath PT and others (2019). ‘Hospital clusters of invasive Group B Streptococcal disease: a systematic review’ Journal of Infection: volume 79, number 6, pages 521 to 527
3. Guy RL, Rudman J, Broughton K, Moganeradj K, Mirfenderesky M, Brown C S, and Lamagni T (2025). ‘Descriptive analysis of incidence, hospital acquisition and health inequalities in invasive group C and G streptococcal infections England, 2016 to 2023’ Lancefield International Symposium on Streptococci and Streptococcal Diseases 2025, Brisbane Australia
Infection reports: seasonal GAS update; CPOs Q4/2025
Group A streptococcal infections: third update on seasonal activity in England, 2025 to 2026