NHS Infectious diseases in pregnancy screening programme handbook
Updated 30 June 2026
Applies to England

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/infectious-diseases-in-pregnancy-screening-programme-handbook/nhs-infectious-diseases-in-pregnancy-screening-programme-handbook
Guidance for local providers of infectious diseases in pregnancy screening.
1. Equality and diversity
The NHS screening programmes are population-based, meaning that screening tests are offered to everyone in a defined population group. The NHS Infectious Diseases in Pregnancy Screening (IDPS) programme offers and recommends screening for HIV, hepatitis B and syphilis in every pregnancy. The three conditions for which we offer screening disproportionately affect individuals from socioeconomically deprived backgrounds or those with any of the 9 protected characteristics, described in the 2010 Equality Act. The national screening programme and providers, therefore, have an important role to play in reducing health inequalities to:
- eliminate unlawful discrimination, harassment and victimisation and other conduct prohibited by the Act
- advance equality of opportunity between people who share a protected characteristic and those who do not
- foster good relations between people who share a protected characteristic and those who do not
Gender inclusive language in maternity services
While the term ‘woman’ is used in this document, this handbook is intended for every pregnant person, including women, trans men and those who identify as non-binary.
Trans and non-binary people face specific inequalities when accessing health care. Healthcare professionals should be aware that trans and non-binary people may have specific needs.
2. Introduction
This revised handbook replaces the previous version published in 2016. The programme handbook aims to inform and support best clinical practice in the delivery of the NHS IDPS programme.
The handbook covers all aspects of screening for HIV, hepatitis B and syphilis in pregnancy and provides an update of recent changes to the programme. It refers to supporting documents and national clinical guidance that providers should follow to ensure they deliver a high quality screening programme.
The programme handbook was developed with support of clinical stakeholders to provide consistent and seamless guidance from screening to clinical management of women with HIV, hepatitis B or syphilis.
Related documents
This handbook should be read in conjunction with NHS England screening guidance:
NHS population screening guidance explains the general principles of population screening.
Infectious diseases in pregnancy screening pathway requirements specification
Infectious diseases in pregnancy screening: care pathway
Infectious diseases in pregnancy screening programme: standards
Infectious diseases in pregnancy screening programme: laboratory handbook
Antenatal and newborn screening: identifying and reducing inequalities
Managing safety incidents in NHS screening programmes
NHS England serious incident framework
3. Programme overview
The UK National Screening Committee (UK NSC) recommends that systematic, population based screening for HIV, hepatitis B and syphilis in pregnancy is offered and recommended to all eligible women. The three infections are identified as viable and appropriate for screening as there are effective interventions that can be made in pregnancy, at delivery and postnatally to significantly reduce the risk of the infection being transmitted from a mother to her child, known as vertical transmission. Rates of the three infections in England are low, but screening is regarded as cost-effective because of the lifetime costs.
The UK NSC periodically reviews the three infections to ensure they remain appropriate and considers other infections that may be added to the programme. Information about the UK NSC review process can be found here.
The NHS IDPS programme aims to reduce the risk of vertical transmission of HIV, hepatitis B and syphilis by supporting high quality and accessible screening programmes throughout England which:
- ensure equal access to uniform and quality assured screening
- promote uptake of screening through understanding and awareness of the infections screened for
- ensure HIV, hepatitis B and syphilis are identified early in pregnancy to facilitate timely entry into specialist services for assessment and management
- ensure that neonatal management and follow up is appropriate and timely
Governance
The NHS IDPS programme is part of the Vaccinations and Screening directorate of NHS England who are responsible for the commissioning, operational and quality assurance of all the 11 national screening programmes.
4. Infections screened for
Human Immunodeficiency Virus (HIV)
In 2017 women made up one-third (31%, 28,669/93,385) of people living with HIV infection in the UK and a quarter (1,106/4,334) of new HIV diagnoses. 97% of women with diagnosed HIV were on treatment.
The number of new diagnoses in women who are pregnant, like the overall population of people living with HIV in the UK, has declined over the last decade particularly among women from sub-Saharan Africa. The number of pregnancies to women known to be living with HIV has also declined from a peak in 2006 to 2010 of over 1300 per year to below 1000 in the years since 2016.
Since 2016, approximately 90% of pregnancies have been to women who were aware of their HIV status before they became pregnant, compared to 72% in 2007 to 2011.
The success of testing and diagnosing HIV in women is due in part to the introduction of universal antenatal screening for HIV in 1999. Since then, coverage of screening in pregnancy has improved year on year, and in 2021 to 2022 in England it is 99.8% across all regions.
Clinical features
HIV is a retrovirus which attacks and destroys immune cells causing gradual failure of a person’s immune system over time. Eventually this leaves the body vulnerable to life threatening infections and cancers.
HIV transmission
HIV is transmitted through transfer of virus-containing bodily fluids. The main routes of transmission are through sexual intercourse, injecting drug use and vertical transmission.
The risk of vertical transmission when HIV is untreated in pregnancy is around 25% and before universal HIV screening in pregnancy, transmission rates were high. Since 1999, rates have declined significantly from 2.1% in 2000 to 2001 to under 0.4% since 2012 the impact of antenatal screening, high uptake of early and effective antiretroviral therapy (ART) and optimised clinical care before and during pregnancy, at birth and in the postnatal period.
HIV management in pregnancy
Management of HIV infection in pregnancy should be in line with the British HIV Association (BHIVA) Guidelines.
Suppression of HIV using ART is the main objective of HIV management. ART works by interrupting the life cycle of the HIV virus, disabling its ability to replicate in the human’s immune cells thereby allowing the immune system to recover. The fall in the level of virus in the blood stream and other parts of the body, including the genital tract, significantly reduces the risk of vertical transmission across the placenta during pregnancy or during exposure to maternal body fluids at delivery.
The aim of treatment is to reach full suppression, where the virus becomes undetectable in the blood. Regular viral load testing during pregnancy is used to monitor progress. For those not already on treatment, appropriate ART should be commenced early in pregnancy. This should happen soon after diagnosis and women are recommended to stay on treatment for life, which reduces the long-term risk of HIV related health problems and HIV transmission to others.
Where full viral suppression is achieved, the risk of HIV transmission during delivery is the same regardless of whether a woman has a vaginal delivery or a caesarean section and so for most women, HIV should not impact decisions about the method of delivery.
HIV is carried in breastmilk and can be transmitted through breastfeeding. HIV treatment can significantly reduce the risk of transmission, but this is yet to be quantified. For women on treatment with a consistently undetectable viral load, the risk is likely to be low, but it is not zero.
The British HIV Association (BHIVA) continue to advise that formula feeding is the safest feeding option as it eliminates the risk of HIV transmission following delivery. However, they highlight the importance of facilitating early discussion around infant feeding and advocate for women who are virologically suppressed to be supported if they wish to breastfeed. Support should include early planning and close monitoring by the perinatal infectious diseases multidisciplinary team (PID MDT) in line with BHIVA guidance on infant feeding.
Further Resources
HIV: explaining the screening result leaflet
Mentor Mothers at Positively UK: http://positivelyuk.org/pregnancy/
CHIVA – UK and Ireland (via referral from clinic or charity): https://www.chiva.org.uk/
5. Hepatitis B
Hepatitis B is a major public health problem and became the leading cause of infectious deaths globally in 2013, exceeding HIV, tuberculosis, and malaria. In 2019 it was estimated 296 million people (3.8% of the world’s population) were living with chronic hepatitis B. Hepatitis B is seen commonly in East Asia and Sub-Saharan Africa where between 5 and 10% of adults are chronically infected. Rates in Europe and North America are low at around 1%.
In 2021 the UK Health Security Agency (UKHSA) estimated the number of people living with chronic hepatitis B in England to be 206,000, equivalent to a prevalence estimate of 0.45% of the population.
The prevalence of hepatitis B in the pregnant population is lower and varies across England from 0.05% to 0.08% in some rural areas, rising to 1% or more in certain inner-city areas where populations with origins in endemic countries are higher.
The proportion of pregnancies to women living with hepatitis B has fallen over the last three years, from 3.89 per 1,000 eligible women in 2018 to 2019, to 3.38 per 1,000 eligible women in 2020 to 2021.
Clinical features
Hepatitis B is an inflammatory illness of the liver caused by the hepatitis B virus. Following acquisition, the virus infects human liver cells. Once inside it uses the cell’s machinery to replicate, creating copies of itself. The new virus then infects surrounding liver cells and repeats the process of replication.
It should be noted, that the process of viral replication does not itself damage the liver, instead, it is the individual’s own immune system, which detects the virus and mounts an attack which destroys both infected and surrounding non-infected liver cells.
A hepatitis B infection can result in two possible outcomes; an acute (short term) infection, or a chronic (life-long) infection where the body fails to clear the virus.
Acute hepatitis B infection
In around 90% of healthy adults who acquire hepatitis B their immune response can clear the virus within a few weeks or months. Many do not experience any symptoms, but where they do, it is usually between one and four months after infection and they are often mild including fever, fatigue, loss of appetite, nausea, vomiting and abdominal pain. Rarely, a life-threatening condition called ‘fulminant hepatitis’ can occur with an acute infection. This requires immediate medical attention as it can cause sudden liver failure resulting in the need for a liver transplant and can often be fatal.
Acute hepatitis B may last up to six months and individuals can easily pass the virus to others during this time. Those who successfully clear the virus make a full recovery and are then non-infectious to others and immune to reinfection. Those who do not clear the infection by six months have chronic Hepatitis B infection.
Chronic hepatitis B infection
Approximately 10% of adults who acquire hepatitis B do not clear the virus spontaneously within six months and are diagnosed with chronic hepatitis B. Spontaneous clearance of hepatitis B after this point is very rare and most individuals remain hepatitis B positive for life.
People with chronic infection have an increased risk of developing liver cirrhosis (permanent scarring of the liver) and liver cancer and management should be by a hepatologist or gastroenterologist. When clinically indicated, antiviral treatment can help to reduce the progression of liver disease and complications.
Hepatitis B transmission
Hepatitis B can be passed from person to person through unprotected sexual intercourse, vertically during pregnancy or childbirth and through direct contact with the blood of someone with the virus, including within the household or by sharing needles.
Hepatitis B in pregnancy
Without intervention to prevent transmission, the risk of infants acquiring the infection vertically can be as high as 90% for women with higher infectivity level, and between 10% to 40% for women with lower infectivity.
Whereas most adults who newly acquire Hepatitis B clear the virus, 90% of infants who acquire hepatitis B vertically will develop chronic infection. This chronic infection gives brings an increased lifetime risk of developing hepatocellular carcinoma.
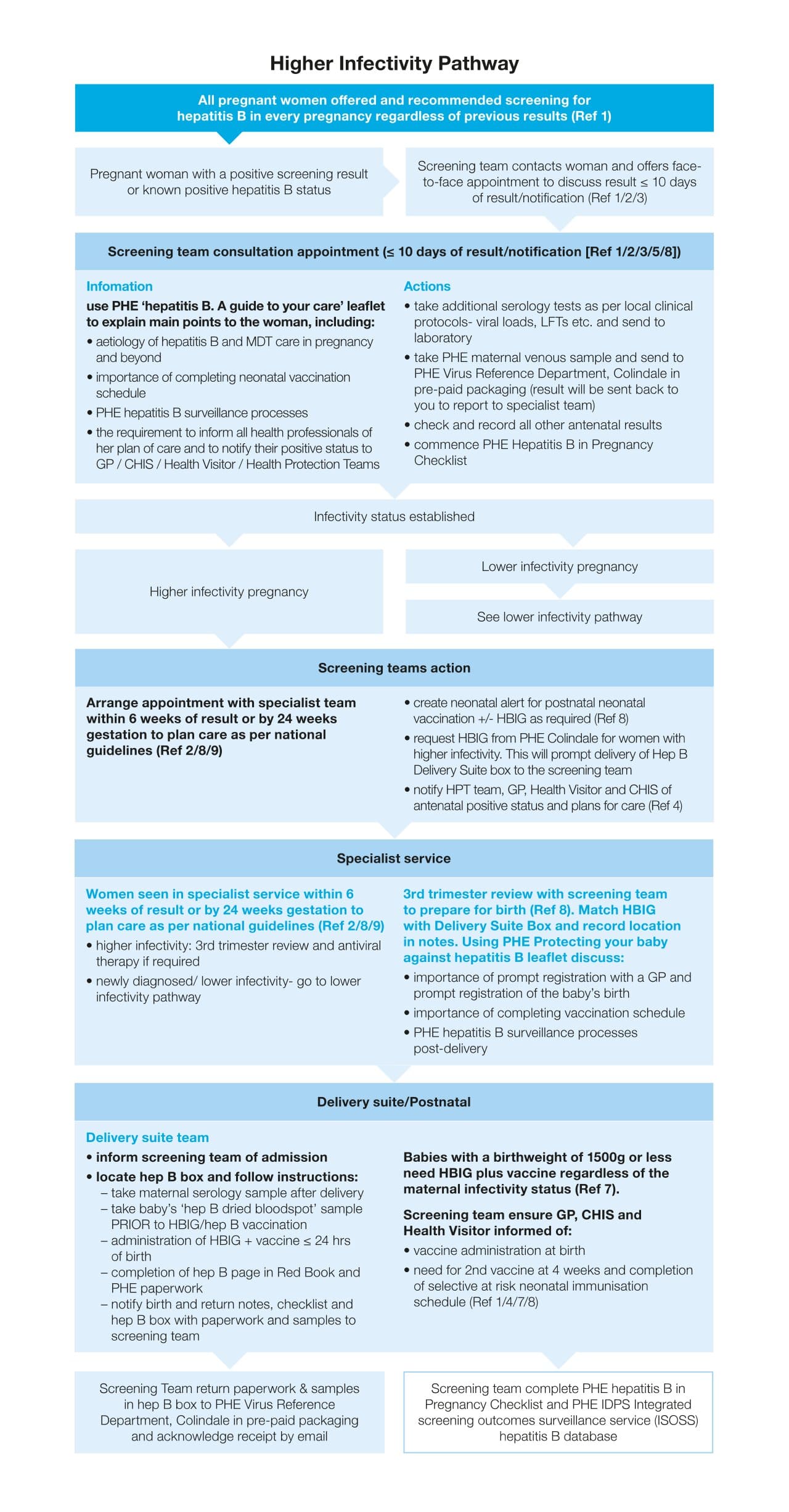
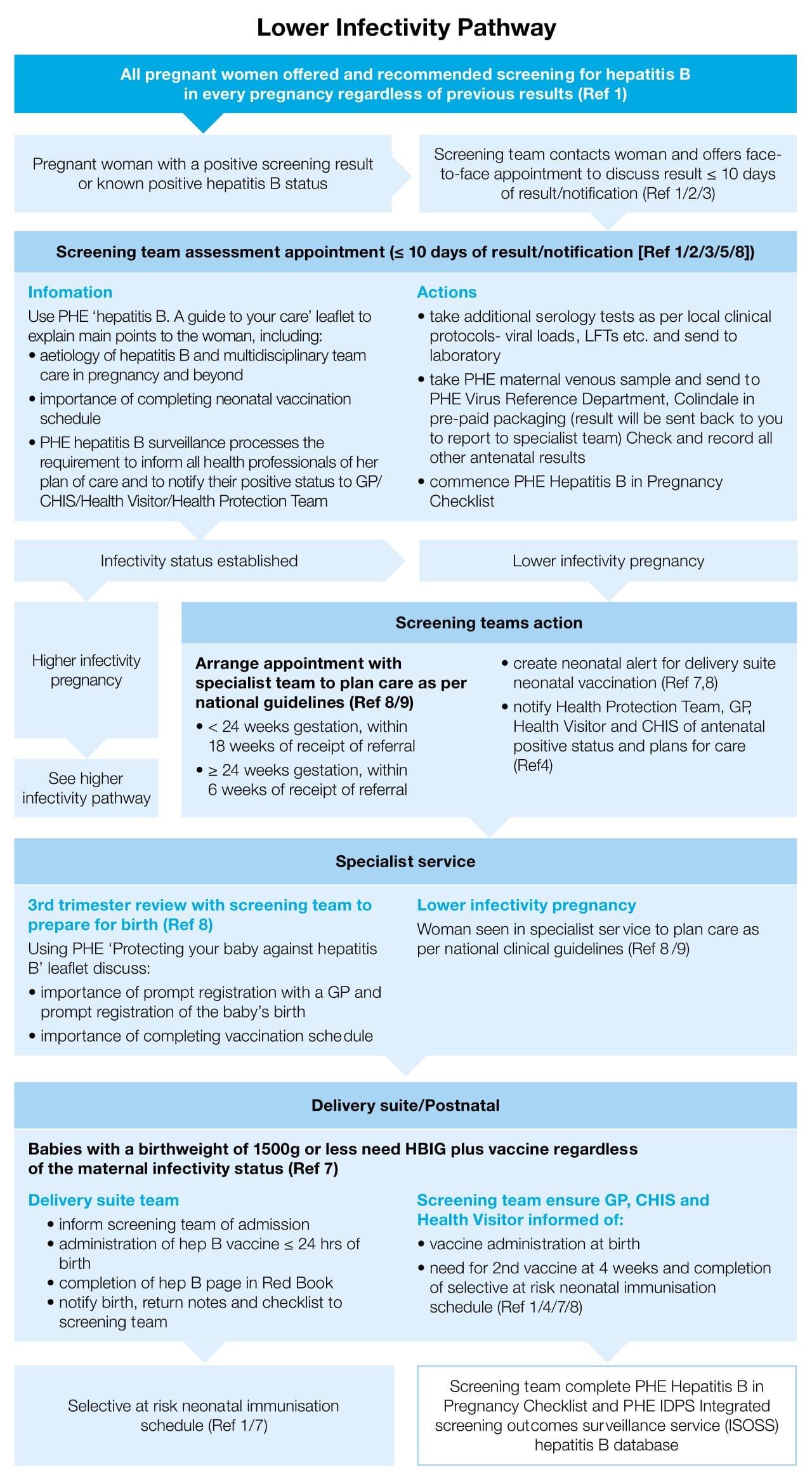
In June 2020 the IDPS programme launched the enhanced hepatitis B pathway with the aim of further reducing cases of vertical transmission by improving the management of hepatitis B in pregnancy and the uptake and completion of the neonatal immunisation schedule. High coverage of antenatal screening for hepatitis B and administration of a timely dose of birth vaccine in babies is the most effective method of preventing vertical transmission.
All infants born to women with hepatitis B should follow the selective neonatal hepatitis B immunisation programme for post exposure vaccination, starting with the birth dose. This is highly effective at preventing vertical transmission. Some infants will also require HBIG to give them the best protection.
Management in pregnancy
Management of hepatitis B infection in pregnancy should be in line with the British Viral Hepatitis Group (BVHG) and The green book: chapter 18 guidance.
Following a positive hepatitis B antenatal screening result, further serological tests are undertaken to determine the woman’s infectivity level (HBeAg and anti-HBe status and hepatitis B virus (HBV) DNA level (maternal viral load)), and which management pathway to commence.
All women with a new diagnosis of hepatitis B in pregnancy should be seen within 6 weeks regardless of their infectivity status.
Higher infectivity
Women with higher infectivity levels; a positive HBeAg, negative anti-HBe status, and/or a high HBV DNA Level, should be seen by specialist hepatitis B services within 6 weeks of the maternity service receiving their positive screening result in line with IDPS standard 6 and the higher infectivity pathway should be commenced.
{kind=link}
All babies born to women with higher infectivity require hepatitis B immunoglobulin (HBIG) in addition to the hepatitis B vaccine. For HBIG inclusion criteria according to maternal hepatitis B status see table 18.5 The Green Book on Immunisation - Chapter 18 Hepatitis B (publishing.service.gov.uk)
Women with an have elevated viral load (an HBV DNA level greater than or equal to 2x105 IU/ml) in pregnancy may be offered antiviral medication in the third trimester in order to reduce the amount of virus present in the maternal bloodstream at the time of delivery.
It should be noted that this is lower than the threshold for infants who require HBIG, meaning some women may require treatment in pregnancy but their infants will not require HBIG.
Lower infectivity
Women with lower infectivity; a negative HBeAg and positive anti-HBe status, with a viral load below 2x105 IU/ml, should follow the lower infectivity pathway and be seen by specialist hepatology services within 18 weeks of the maternity services receiving their positive result, in line with IDPS Standard 8. Babies born to women with lower infectivity require vaccination only.
{kind=link}
Please note, infants born to women with hepatitis B who have a birthweight of 1500 grams or less, should receive HBIG in addition to the vaccine, regardless of the infectivity status of the mother, as the benefit is high in this group of infants.
A woman’s hepatitis B status should not impact decisions about delivery or choice of infant feeding.
Further Resources
Guidance on the hepatitis B antenatal screening and selective neonatal immunisation pathway
Hepatitis B: screening and care in pregnancy and protecting your baby by vaccination
The Green Book: Immunisation against infectious disease: chapter 18 hepatitis B
6. Syphilis
The incidence of syphilis infection in the UK has increased since 2000. Although most infections still occur in men who have sex with men (70%), prevalence is increasing among heterosexual men and women which may in turn lead to a rise in the pregnant population.
Whilst there was only a slight increase in the number of syphilis infections in pregnancy in England from 1.39 screen positives per 1000 tested in 2017 to 2018 to 1.59 per 1000 tested in 2020 to 2021 continued vigilance is needed, highlighting the important role of the antenatal syphilis screening programme.
There are around 1000 cases of syphilis in pregnancy each year and just under half of those require treatment in pregnancy. This is a combination of women with newly diagnosed infections and those with a previous diagnosis that require treatment/re-treatment.
Clinical features
Syphilis is a complex, multistage disease caused by the bacterium Treponema Pallidum. Treponema pallidum is highly invasive and following transmission it spreads throughout the body via the venous and lymphatic systems within hours. This widespread dissemination can lead to a number of potential clinical presentations as the diseases progresses.
The varied clinical presentation of syphilis means it is not always correctly identified. While it is easily treatable with antibiotics, where early infection is missed and goes untreated, the infection can progress and result in severe cardiovascular, ocular and neurological complications.
The clinical presentation of syphilis is divided into stages: primary, secondary, latent and tertiary, and is most infectious in primary and secondary stages of infection.
Primary Stage
A single chancre marks the onset of the primary stage of syphilis, but there may be multiple sores. The chancre is usually (but not always) firm, round, and painless. It appears at the location where syphilis enters the body. These painless chancres can occur in locations that make them difficult to notice e.g. the vagina or anus. The chancre lasts 3 to 6 weeks and heals regardless of whether a person receives treatment. However, the infection will progress to the secondary stage if the person with syphilis does not receive treatment.
Secondary Stage
Secondary stage symptoms, which include skin rashes and/or mucous membrane lesions (sores in the mouth, vagina, or anus) are experienced in around 25% of cases. The development of a rash on one or more areas of the body:
- can appear when the primary chancre is healing or several weeks after the chancre heals
- does not usually cause itching
- may appear as rough, red, or reddish-brown spots on the palm of the hands and bottoms of the feet. However, rashes with a different appearance may occur on other parts of the body. Sometimes they resemble rashes caused by other diseases
- may be so faint they are hard to notice
Condyloma lata are large, raised, grey or white lesions. They may develop in warm, moist areas like the mouth, underarm or groin region.
In addition to rashes, signs and symptoms of secondary syphilis may include fever, swollen lymph nodes, sore throat, patchy hair loss, weight loss, muscle aches, fatigue and headaches.
The symptoms of secondary syphilis will go away with or without treatment. However, without treatment, the infection will progress to the latent and possibly tertiary stage of disease.
Latent Stage
The latent (hidden) stage of syphilis is a period where syphilis remains in the body but there are no visible signs or symptoms of the infection. Early latent syphilis is where infection was acquired within the past two years. Late latent syphilis is where infection was acquired more than two years ago. Latent syphilis of unknown duration is when there is not enough evidence to confirm initial infection was within the previous two years. Latent syphilis can last for years.
Tertiary Syphilis
Tertiary syphilis is rare and develops in a subset of untreated syphilis infections. It can appear 10–30 years after a person gets the infection, and it can be fatal. Tertiary syphilis can affect multiple organ systems, including the brain, nerves, eyes, heart, blood vessels, liver, bones and joints. Symptoms of tertiary syphilis vary depending on the organ system affected.
Syphilis transmission
The most common mode of syphilis transmission is sex including oral, vaginal and anal sex, by direct contact with infectious lesions of the primary or secondary stages. Transmission occurs when bacteria enter via tiny breaks in the skin or mucous membranes. Transmission can also occur through vertical transmission.
Syphilis in pregnancy
Syphilis can be transmitted vertically to the unborn baby during pregnancy resulting in congenital syphilis in the fetus. Congenital syphilis can cause miscarriage or late fetal loss, stillbirth and neonatal death. It is estimated that up to 40% of babies with congenital syphilis may be stillborn or die as a newborn. Where pregnancy results in a live birth, congenital syphilis can cause a variety of symptoms in the newborn, including low birth weight, jaundice, severe anaemia and neurological complications.
Management in pregnancy
A positive antenatal syphilis screening result cannot differentiate between a current syphilis infection and past syphilis infection which was successfully treated, therefore a comprehensive assessment must be carried out by sexual health services for all pregnant women with confirmed positive results, to make a clear maternal diagnosis and treatment plan.
The highest risk of transmission during pregnancy is in the third trimester. Congenital syphilis is more likely to occur when a woman has primary or secondary syphilis and is treated less than 30 days before delivery, therefore timely and effective treatment of maternal infection is vital.
Following diagnosis, syphilis should be treated with penicillin which is extremely effective (success rate of 98%) in preventing transmission to the baby.
Women treated for syphilis infection may be re-infected in pregnancy and so sexual health promotion and partner testing/treatment are vital.
Infant
All infants born to mothers treated for syphilis infection in the current pregnancy require a neonatal review at birth including a full physical examination and syphilis serology.
A baby born with congenital syphilis may not have any immediate signs or symptoms of disease. However, if treatment is not immediate, the baby may develop serious problems within a few weeks. Babies who do not receive treatment may have developmental delays, seizures, or die.
Infants diagnosed with congenital syphilis should be treated with penicillin without delay.
The IDPS programme launched a syphilis management pathway in May 2023. This guidance focuses on the management of infection following a positive screening result. Key objectives of the pathway are to improve timeliness of entry into specialist care for treatment and to ensure treatment and follow up of the women and her baby are completed.
The pathway formalises the existing activities undertaken by screening teams, clearly defining roles and responsibilities and setting timeframes for necessary actions. It also encourages effective collaborative working with sexual health services. Guidance is consistent with the British Association for Sexual Health and HIV (BASHH) syphilis guideline.
Further resources
Syphilis: managing infection in pregnancy
Syphilis: explaining the screening result leaflet
7. NHS Screening pathway requirements
The NHS offers and recommends screening tests for infectious diseases in every pregnancy, regardless of any past results or treatment. This also includes screening for women who present in labour having received no antenatal care, and those without documented evidence of a screening result in their current pregnancy. The Infectious diseases in pregnancy screening pathway requirements specification provides a step by step guide to the screening process.
Offer and recommend screening
All eligible women should be offered and recommended screening for HIV, hepatitis B and syphilis in every pregnancy, regardless of any past results or treatment. This includes women who are known to be living with HIV and/or hepatitis B to ensure:
- any change of infection status is identified
- they have access to the most up-to-date information about their condition
- there is a current result on the providers laboratory and maternity IT systems
- the antenatal screening team are aware, ensuring timely access to care from specialist services.
Screening is an individual choice and everyone must be given the opportunity to make a personal informed choice about whether or not to be screened. The decision must be based on an understanding of:
- the conditions for which screening is offered
- the benefits of screening for the three infections
- the screening test process the possible outcomes of the screening tests.
This discussion should be supported by information about screening tests offered during and after pregnancy and women should be made aware of how to access the digital version of Screening tests for you and your baby (STFYAYB).Those who are unable to access the digital version should be given a physical copy. Where required, women should be signposted to, or given, STFYAYB translations or STFYAYB easy guides. There should also be access to translation services if this is needed.
Immunisation in pregnancy
Midwives should discuss and promote vaccination against pertussis, influenza and COVID -19 (where eligible) in pregnancy. Women should also be advised to check their measles, mumps and rubella (MMR) status with their GP to ensure they have 2 documented administered doses of the MMR vaccination. As MMR is contraindicated in pregnancy, additional doses of MMR vaccine where required should be given postnatally. This information resource can used for pregnant women: Pregnancy: how to help protect you and your baby
Health professionals can find further information about pertussis vaccination in pregnancy here: https://www.gov.uk/government/collections/immunisation#pertussis-(whooping-cough)
Further information for health professionals about influenza vaccination in pregnancy can be found here: https://www.gov.uk/government/collections/annual-flu-programme
Further information for health professionals about COVID vaccination in pregnancy
Viral rash in pregnancy
Midwives must advise women to report any rash or rash-like illness to their midwife or GP as soon as possible to enable appropriate management of viral rash in pregnancy. The woman should be advised to avoid any clinical setting or other pregnant women until clinically assessed.
Screening offer accepted
When screening is accepted, blood samples should be taken without delay, ideally on the same day as the woman accepts the offer of screening. Taking of the screening sample should not be delayed to coincide with other appointments or scans as this can delay treatment and care that could significantly impact on vertical transmission of infection.
Blood samples must be sent to the laboratory for testing with the completed request forms (electronic and/or paper) as per local protocol, which should be clearly identifiable as an antenatal screening sample. The screening laboratory will perform testing in line with the testing algorithms in the NHS IDPS programme laboratory handbook and screening results should be reported by the laboratory and be available to maternity services within 8 working days.
Women who are known to be living with HIV or hepatitis B prior to pregnancy should have their positive status recorded in their maternity records and on the laboratory request form as ‘known positive’. The screening team at the maternity provider must then be informed, and an appointment arranged within 5 working days of either a confirmed screen positive result from the latest screening test, or her disclosure of positive status if she has declined screening.
It is important women are told when and how they will receive their results and that their contact details are checked to make sure they can be contacted to discuss their results if necessary.
Screening offer declined
If a woman chooses not to have screening for any or all of the three infections, the decision should be documented, and she should be informed that she will be contacted by a member of the screening team at the maternity provider for a further discussion.
A sample for any of the tests that are accepted should be taken the same day and sent to the laboratory with the request form clearly identifying which test has been declined.
A formal re-offer of screening must be made face-to-face by the maternity providers screening team by 20 weeks gestation. Women who book after 20 weeks gestation and decline screening must be re-offered screening within 2 weeks.
The purpose of the re-offer is to ensure the woman receives all the appropriate information and her decision is based on a good understanding of why screening is recommended. If the reoffer is accepted, screening samples should be taken the same day.
The reoffer is to facilitate informed choice and not to coerce women to accept screening. The discussion should be supportive and respectful of her right to choose.
Where the formal re-offer is declined, the reasons for this decision should be explored sensitively and any potential risk factors for infection identified such as high prevalence of infection(s) in the woman’s country of birth or partner’s country of birth, history of IV drug use or involvement in sex work.
All screening declines must be referred for discussion by the PID MDT. Any relevant history gained from the formal re-offer should be relayed to the PID MDT who are responsible for further review and management, in line with local and national clinical guidelines. PID MDT discussions/ risk assessment and any subsequent actions taken as a result should be documented in the woman’s maternity record.
Maternity providers must have a local protocol in place to support women who decline screening due to needle phobia. The use of dried blood spot or oral fluid samples as an alternative to a venous blood sample in needle phobic women is outside the scope of the IDPS pathway.
8. Management of screening results
Negative results
Negative screening results should be discussed with women and documented at their next routine antenatal appointment with the midwife or obstetric team.
Surveillance of infections in pregnancy has highlighted cases of infection acquired after an initial screen negative result at booking. All midwives involved in the provision of antenatal care should be encouraged to discuss sexual health with the women they care for. The ‘negative now’ message should be used when giving negative screening results to remind women that they are negative at the point of testing, and this does not confer protection throughout pregnancy.
Women should be advised about the availability of repeat testing and/or sexual health screening at any stage of pregnancy and be encouraged to report any symptoms or risks of exposure to infection(s) to their midwife. Midwives should also be vigilant for the need to recommend and facilitate repeat testing where a risk is identified.
Risks include where the woman:
- changes her sexual partner
- or her partner is sexually active with other people
- has a partner diagnosed with a sexually transmitted infection
- injects recreational drugs
- undertakes sex work
- is at risk of sexual exploitation.
Inconclusive results
Inconclusive screening results, more commonly seen in HIV and syphilis screening and less frequently encountered with HBV screening, are where the initial screening assay gives an equivocal or positive screening result which is not supported by the confirmatory tests. When this occurs, a repeat screen is needed to rule out the small possibility of a recent infection.
There must be a locally agreed process for the laboratory to inform the maternity providers screening team directly of all inconclusive results on the initial screening sample and request a repeat sample. The repeat sample should be taken a minimum of 2 weeks from the date of the initial sample.
For most women, the repeat sample will exclude recent infection as the serological markers will not have changed. To avoid unnecessary distress and anxiety referral to sexual health services is not recommended unless the repeat sample confirms an infection. Laboratories are advised to report clearly so that the maternity providers screening teams can confidently follow their recommendation.
Confirmed screen positive results
Maternity providers screening teams must be informed of all confirmed screen positive results by the laboratory and notification should be acknowledged by screening teams on receipt.
Women with a confirmed screen positive result should be offered an appointment to discuss their result in less than or equal to 5 working days of the maternity service receiving notification by the laboratory. The date the maternity service receive the confirmed screen positive result is counted as day 1.
Women who are living with HIV and hepatitis B and choose not to be-rescreened should be contacted and offered an appointment within 5 working days of the maternity services screening team being made aware of their status. This is an important opportunity to provide up to date information and ensure a consistent level of care and support for women, irrespective of their parity.
A face-to-face appointment should be offered, or appointments can be virtual if that is the woman’s choice and if it meets their individual needs.
Interpretation services must be provided if required and family members should not be used to interpret.
The appointment provides an opportunity for the maternity services screening team to:
- give up to date information about the infections and its relevance to the woman’s health and her pregnancy. For those who are already aware of their condition, to explore their understanding and address any gaps their knowledge.
- explain what to expect during pregnancy and following delivery, such as vaccination schedules and neonatal testing
- obtain a comprehensive history to aid onward referral to specialist services
- promote attendance to all appointments and ongoing maternal and infant engagement after the birth
- discuss communication with other health care professionals such as the general practitioner and community midwife (for HIV consent must be gained to share information)
- address any additional needs, complex social issues and potential barriers to engagement
- for hepatitis B inform Child Health Information Services (CHIS) to make sure a vaccination schedule can be set up following delivery as needed for the infant.
Verbal information should be supported by the HIV, hepatitis B and syphilis screening in pregnancy information leaflets which are available in 12 languages:
- HIV: explaining the screening result
- Syphilis: explaining the screening result
- Hepatitis B: screening and care in pregnancy and protecting your baby by vaccination
Women who have a disability, impairment or sensory loss should be provided with information they can easily read or understand in line with the Accessible Information Standard.
Information on the management of infections in pregnancy is available in easy read guides in the IDPS section of the STFYAYB easy guides.
9. Management of infections in pregnancy
Referral to specialist services
All women with a confirmed screen positive result must be referred to specialist services after receiving their results regardless of any past results or treatment.
For those who are living with HIV or hepatitis B and already engaged in care, this will ensure the service is aware of the current pregnancy and enable liaison between the two services to be initiated.
NHS IDPS programme management pathways for hepatitis B and syphilis The pathways provide step-by-step guidance for maternity service screening teams, outlining their responsibilities as the coordinator of the woman’s care.
It is recommended that maternity services screening teams share this guidance with colleagues in sexual health and hepatology services and use them to agree local roles and responsibilities.
Multidisciplinary working
Clinical associations such as BHIVA, BASHH and British Association for the Study of the Liver (BASL) endorse the MDT approach and recommend providers of HIV, sexual health and hepatology services have a nominated lead clinician for maternity referrals to support referral and ongoing liaison.
Management of the three infections in pregnancy involves several specialities and effective multidisciplinary working is important to ensure that the best possible care can be delivered. A multidisciplinary team approach will:
- ensure every woman with an infection in pregnancy is managed collaboratively, drawing on all the specialities to make well considered management plans and enabling ongoing liaison
- provide a forum to discuss and plan such as high-risk declines, women who do not or cannot engage, or where treatment has failed
- provide an established point of contact for managing urgent screening results.
All maternity providers should, have a maternity infectious diseases multidisciplinary team (PID MDT) which convenes to collaboratively review all women who screen positive for HIV, hepatitis B and syphilis. The maternity service screening team should coordinate the PID MDT and be the link between other members.
All women with a confirmed screen positive result for HIV, hepatitis B or syphilis should be added to the PID MDT caseload as soon as the maternity service screening team are made aware by the laboratory. This includes women who have screened positive but are not engaging with specialist services.
Membership of the PID MDT will vary locally and may include representation from the following:
- maternity service screening team/infectious diseases midwife
- sexual health services / genitourinary medicine
- HIV services
- hepatology / gastroenterology
- neonatology / paediatrics
- obstetrics
- laboratory services(microbiology/virology).
The laboratory team is integral to the delivery of the screening pathway and functions of the PID MDT. There should be a nominated lead for antenatal screening with representation on trust antenatal and newborn screening governance groups.
Where infection rates are low and it is not feasible to have a combined face to face MDT for the 3 infections, providers should consider alternative options of holding meetings to review all women with a screen positive result, such as:
- virtual meetings
- merging with existing forums such as HIV, hepatology, sexual health service or neonatal MDT meetings within which members will have well established working relationships
- creating joint or regional MDTs with other providers, enabling shared expertise and support.
Regardless of the number of women with screen positive results, every pregnancy should be discussed and managed collaboratively to ensure the provision of high quality, personalised care.
Care plans and neonatal alerts
Birth plans/checklists and neonatal alerts should be used to facilitate the transfer of key information between professionals regarding the woman’s treatment and the requirements for the baby at birth. These should be made available to obstetric and neonatal teams (delivery suite or IT system as per locally agreed process) as soon as the maternity service screening team receive them from the relevant service (HIV and syphilis).
- HIV birth plan
- hepatitis B Hepatitis B maternal and neonatal checklist
- syphilis BASHH syphilis Birth Plan or local equivalent.
Infants admitted to neonatal intensive care units
It is important that where a baby is admitted to the neonatal intensive care unit, the maternal birth plan, hepatitis B checklist and any other relevant information is shared by the maternity team with the neonatal team. The maternity service screening team should also be made aware that the infant is an inpatient so they can ensure all required interventions are undertaken (post exposure prophylaxis, serological testing, feeding support) and liaise with the PID MDT where necessary.
Addressing inequalities for women with a confirmed screen positive result
It is important to acknowledge the positive impact that continuity of care and expertise provided by screening midwives and infectious diseases specialists can have on this vulnerable population who often face health inequalities. The difference made by providing continuity of care to women who are screen positive was evident in both the syphilis and HIV clinical expert review panels (CERPs) (reviews of infants reported with vertical transmission of infection that look at clinical and social factors surrounding each case).
Core20PLUS5 is a national approach to support the reduction of health inequalities at both national and system level. The approach defines a target population cohort – the ‘Core20PLUS’ – and identifies ‘5’ focus clinical areas requiring accelerated improvement. One of these areas of focus is ‘Maternity care: ensuring continuity of care for 75% of women from Black, Asian and minority ethnic communities and from the most deprived groups.’
It also puts a focus on inclusion health groups which includes:
- people experiencing homelessness
- drug and alcohol dependence
- vulnerable migrants
- Gypsy, Roma and Traveller communities
- sex workers
- people in contact with the justice system
- victims of modern slavery other socially excluded groups.
10. NHS IDPS screening in other settings
Most antenatal infectious diseases screening will take place in maternity services and should be offered and carried out as early as possible, usually at the booking appointment. It may, however, be necessary to carry out screening in other settings and at other times during pregnancy. These include on admission to gynaecology wards, maternity assessment units or the delivery suite for women who present with no reliable documentation of their screening result from a United Kingdom Accreditation Service (UKAS) accredited laboratory.
Maternity providers must have a process in place to identify all eligible women, regardless of where and when they are screened, to ensure screening is completed and results actioned.
11. Transfers of care
If a woman changes care provider during her pregnancy it is not necessary to repeat the screening tests if the results can be accessed and are from a UKAS accredited laboratory. If the screening results are not available, it is recommended that the tests required are repeated as soon as possible.
Transfer of care is an opportunity to assess whether the woman may have been at risk of infection since her initial screening test and would therefore benefit from retesting.
Maternity providers must make sure that where a woman with a positive screening result transfers from or into their service, there is a process to ensure reliable transfer of information regarding her care, between services. A referral should be made to specialist services (HIV, hepatology, sexual health) in the receiving trust and if already available, birth plans should be put in place for delivery.
12. Pregnancy bookings after 20 weeks gestation
Women who present for antenatal care after 20 weeks gestation should have their screening expedited. The urgency is less acute than for unbooked women presenting in labour, but samples must be taken as soon as possible, and within 2 weeks of accessing antenatal care. A request for prompt testing and the reason must be made clear on the laboratory request form. Screening should be performed by the laboratory without delay, either on the day of receipt or next working day if received out of hours and results reviewed as soon as they are available from the laboratory.
Women with a confirmed screen positive result should be informed of their result and referred urgently to specialist services, requesting they be seen as soon as possible.
13. Miscarriage or termination of pregnancy after screening
A local protocol should be in place for women who miscarry or terminate their pregnancy after screening to make sure they receive their results and are followed up if required.
Negative results
Women should be informed of their results by telephone or letter. A template letter is available here.
Confirmed screen positive results
Women with a confirmed screen positive result should be contacted to discuss their result in less than or equal to 5 working days of the maternity service screening team receiving notification by the laboratory. The date the confirmed screen positive result is received is counted as day 1.
The screening team should then refer to the appropriate specialist services, ensuring the referral has been acknowledged before closing the maternity care episode.
Inconclusive results or inadequate samples requiring follow up
Women must be informed that their screening could not be completed and advised to contact their GP or local sexual health service for repeat testing.
14. Urgent screening for women admitted in labour or with a risk of labour (with no reliable evidence of a screening result in this pregnancy)
A locally agreed pathway must be in place to facilitate urgent screening for women admitted to the maternity unit either in labour or with a risk of labour, with no reliable laboratory evidence of screening results from a UKAS accredited laboratory. They should be given up to date information about the screening tests and screening should be recommended. Where consent is given, screening must be undertaken without delay.
To expedite testing, the maternity service must liaise directly with the laboratory, usually by telephone, to request urgent screening and make sure the laboratory has the necessary clinical information to aid prompt analysis. Maternity services must not rely on writing ‘urgent’ or similar on the request form or flagging ‘urgent’ on an electronic request.
The antenatal screening team must be informed of all women admitted to the labour and in-patient wards who were offered screening to allow appropriate tracking and follow-up of results and care.
Point of care tests must not be used either as the initial screen or as part of any confirmatory testing in the laboratory. The laboratory handbook algorithms largely follow the UK standards for microbiology investigations, and these do not include point of care tests.
Positive urgent screening results
There should be a robust process in place to support timely management of positive results so where required, interventions for the woman or baby may be initiated without delay.
All positive urgent screening results (confirmed and unconfirmed) must be communicated by the laboratory directly to the on-call obstetric team who will then consult with the paediatric team and relevant specialist service.
Unconfirmed positive results are where HIV, hepatitis B or syphilis is detected in the blood in the initial screening test, but the laboratory is unable to perform the confirmation test immediately. In this situation there needs to be an urgent clinician to clinician conversation. This should be between the laboratory clinician and the on-call obstetrician and paediatrician. This is the only circumstance in which an unconfirmed result can be given verbally and acted upon.
The reason results may be released provisionally is to enable therapy to be given to the baby, and to the woman if not yet delivered, to reduce the risk of vertical transmission before confirmatory tests are completed.
Every effort should be made to obtain urgent screening results before discharging the woman home. Where this is not possible a plan must be made for a named person to take responsibility for checking and communicating the results to the woman and to inform the screening team urgently in the event of a positive result.
15. Managing non-attendance
Maternity service screening teams must have systems in place to identify women who do not attend HIV, hepatitis B and sexual health service appointments (virtual or face-to-face) whilst pregnant.
When a woman does not attend a scheduled face-to-face appointment, or cannot be reached by telephone, this should be managed collaboratively by the screening team and specialist service in line with local guidelines. Efforts should be made to identify the reasons for non-attendance and support women wherever possible to attend appointments.
Ongoing non-engagement should be discussed by the PID MDT to agree a plan. Local safeguarding guidance maybe considered for women who are not engaged with healthcare services.
A referral to specialist services should still be made by the maternity screening team for women who have a screen positive result returned in labour or shortly following delivery. Non-attendance at this postnatal appointment must be managed in line with the specialist services local policy.
16. Education and training
Screening teams must ensure there is an ongoing educational programme for maternity staff to keep them informed and updated on important practical information.
Opportunities for teaching include meeting with new members of maternity staff, during mandatory or screening specific updates, or within maternity newsletters.
Key practice points include the need to:
- carry out screening early and avoid deferring screening to later appointments
- make women aware that they may need to be contacted about their results and check they have provided a working contact number
- referral of all women who decline one or more of the screening tests to the screening team
- discuss sexual health in pregnancy including a ‘negative now’ discussion when giving negative screening results
- be vigilant for risk factors and the need to offer retesting or referral to sexual health services
- know how to refer women to sexual health services
- check screening results at every contact during pregnancy including on admission to inpatient services
- know the process for urgent screening for women who present in labour or with a risk of labour with no screening results.
e-Learning resources
Maternity providers should encourage all healthcare professionals involved in antenatal and newborn screening to complete:
- Introduction to population screening
- Antenatal and newborn screening e-learning module.
These resources can be found on the e-Learning for Healthcare (eLFH) website.
Healthcare professionals involved in the management of infectious diseases in pregnancy should complete the advanced IDPS e-learning resource every 12 months to support the delivery of care to women.
There are also learning resources available for those working in neonatal and paediatric intensive care units and GPs.
17. Screening failsafes
Screening teams must make sure they have weekly failsafes in place to identify the eligible population, including women who book late or present unbooked in labour without screening results, to check that:
- all women who have accepted screening have a result
- samples not fit for purpose are repeated
- there is a record of all declines.
To support this process laboratories are required to produce and send screening teams a follow-up list of relevant results each week (or more frequently by local agreement).
The follow-up list must include all confirmed screen positive and inconclusive results and all samples which were not processed because the request is incomplete or the sample inadequate or insufficient.
There must also be a local process in plan to ensure:
- confirmed screen positive results have been communicated to the women
- referrals to specialist services have been made
- specialist appointments have been attended.
18. Data collection
NHS Screening standards
Screening standards provide a way of measuring how well screening programmes are performing in important areas. The revised screening standards for IDPS replace previous versions. They apply to data collected from 1 April 2023.
There are 8 IDPS standards for the three infections. The coverage standards: S01 S02 and S03 require matched cohort data and the follow up of any missed women.
Key performance indicators (KPIs)
KPIs are a subset of the screening standards and give a high-level overview of the quality of screening programmes at important points on the screening pathway.
The current IDPS KPIs reported quarterly are:
- coverage standard IDPS-S01: HIV (KPI ID1)
- coverage standard IDPS-S02: hepatitis B (KPI ID3)
- coverage standard IDPS-S03: syphilis (KPI ID4)
- diagnosis/intervention standard IDPS-S06: timely assessment of women with hepatitis B (KPI ID2).
The IDPS programme monitors rates of infection for HIV, hepatitis B and syphilis in the antenatal population, as well as rates of vertical transmission of infection using data submitted by providers.
Monitoring of screening outcomes is a core deliverable for all national screening programmes and a key objective for the programme teams. Within the NHS IDPS programme, the collation and analyses of screening outcome data is essential to:
- monitor the performance of the screening programme
- review all positive results to inform screening programme pathways, policies and standards
- identify areas for further audit, research and service improvements.
19. Integrated Screening Outcomes Surveillance Service (ISOSS)
ISOSS is part of the NHS IDPS programme, commissioned by NHS England to collect, analyse, and report obstetric and paediatric data on HIV, hepatitis B and syphilis in pregnant women and children. ISOSS assess the key outcomes of the IDPS Programme and its impact on:
- prevention of vertically acquired HIV, hepatitis B and syphilis
- protecting the health of women with HIV, hepatitis B and syphilis during and after pregnancy
- protecting the health of infants newly diagnosed with HIV, hepatitis B and congenital syphilis.
On behalf of NHS England, ISOSS collects data on all pregnancies with a diagnosis of HIV, hepatitis B and syphilis (including those diagnosed outside the screening programme such as sexual health services and A&E) via an online secure portal from all maternity providers in England. The team who delivers ISOSS can be contacted at the generic email address of isoss@ucl.ac.uk for any reporting queries and account issues including the set-up of new accounts.
Maternity services screening teams provide data to the ISOSS online portal at three different submission points:
- Green card – this is a quarterly submission of all pregnancies with a screen positive or known positive result for HIV, hepatitis B and syphilis.
- Antenatal notification form – this form is generated for each individual pregnancy and collects data on demographics, social background, screening and referral pathways and initial care during pregnancy.
- Pregnancy outcome form – this form is generated for all pregnancies where there has been a positive result or known positive status for HIV and hepatitis B. For syphilis, an outcome form is only generated for women who required treatment for syphilis in pregnancy and not all pregnancies with a positive syphilis screening result.
Follow-up care for infants born to women with HIV or syphilis is reported to ISOSS by colleagues from paediatric services via the same online portal. Outcome data on infants exposed to hepatitis B in pregnancy is shared by colleagues at the UK HSA.
Vertical transmissions
Any infant identified as having a suspected or confirmed vertical transmission of infection, including those born to women not known to have a positive result for HIV, hepatitis B or syphilis in pregnancy, must be promptly reported to ISOSS. Additional data collection around these transmissions will take place and the case reviewed by the CERP. Any learning from transmissions is fed back into the NHS screening programme in the form of guidance and pathway updates, and clinical care guidelines produced by BHIVA, BASHH and BASL.
ISOSS governance
ISOSS has Regulation 3 approval, meaning maternity services screening teams do not need to get permission from the women to submit data. Women cannot decline to have their data collected but can object to their data being used for further research purposes. If this is requested, the maternity services screening team must notify ISOSS who will mark the record as not to be used in research. Any research completed on the ISOSS data set goes through a rigorous application and approvals process through NHS England, with strict adherence to data protection processes.
ISOSS outputs
Data collected by ISOSS feeds into many essential work streams including:
- IDPS pathways and guidance
- clinical care guidelines produced by BHIVA, BASHH and BASL
- supporting 3rd sector organisations
- provision of NHS services
- wider public health surveillance activities.
Reports for the infections are produced annually and can be accessed here.
20. Quality Assurance
The NHS IDPS programme has a defined set of screening standards providers must meet to make sure local services are safe and effective.
The aim of quality assurance (QA) is to drive continuous improvement in the screening programme and ensure that these standards are being met by providers maintain. It covers the entire screening pathway, from identifying the eligible population, through to intervention and treatment. The screening quality assurance service (SQAS) undertakes the QA of the NHS screening programme.
Antenatal and newborn (ANNB) QA helps ensure all women and their babies have access to high quality screening wherever they live. ANNB QA lead quality assurance procedures for checking standards are met.
To help ensure services meet standards, all commissioners and service providers must comply with the NHS Infectious diseases in pregnancy screening pathway requirements specification which provides an overview of the screening programme and describes the actions required by providers at each stage of the screening pathway.
Quality assurance of laboratories (UKAS)
The NHS IDPS screening laboratories must:
- be accredited by the UK Accreditation Service (UKAS) to ISO 15189:2012 medical laboratories – requirements for quality and competence
- meet the IDPS laboratory QA evidence requirements mapped to ISO 15189:2012
- participate in external quality assurance (EQA) schemes accredited to ISO 17043:2010 conformity assessment – general requirements for proficiency testing
-
use reference laboratories accredited to ISO 15189:2012 for confirmation of screen positive results when this is not available in-house
- include an annual vertical audit of an antenatal screening sample in its laboratory audit schedule.
UKAS will review both ISO 15189 and the screening requirements on behalf of the screening quality assurance service (SQAS).
Screening Safety Incidents
A screening safety incident is any unintended or unexpected incident(s) that could have or did lead to harm to one or more persons who are eligible for NHS screening. This also applies to staff working in the screening programmes.
A screening safety incident can affect populations as well as individuals. It is an actual or possible failure in the screening pathway.
Providers should comply with the national guidance for the management of safety concerns and incidents in screening programmes and NHS England’s guidance for managing safety incidents in NHS screening programmes.
Laboratory services are expected to inform the Medicines and Healthcare Products Regulatory Agency (MHRA) of any adverse incidents.