NHS Test and Trace statistics (England): methodology
Updated 18 May 2022
Applies to England

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/nhs-test-and-trace-statistics-england-methodology/nhs-test-and-trace-statistics-england-methodology
The UK Health Security Agency (UKHSA) publishes weekly statistics on NHS Test and Trace (England). This document primarily sets out information on the data sources and methodology used to generate the statistics for testing in England. These statistics cover:
NHS Test and Trace bulletin, England
The bulletin includes the:
- number of people tested for coronavirus (COVID-19) in England
- number of people who tested positive for COVID-19 in England
- time taken for home and satellite test centres results to become available in England
Rapid asymptomatic testing bulletin, England
The bulletin includes the number of:
- lateral flow device (LFD) tests reported by test result
- LFD tests reported linked to education settings
- LFD and PCR tests reported in care homes
- LFD tests reported by NHS staff
- LFD tests reported in private and public sector workplaces
This document primarily sets out information on the data sources and methodology used to generate the statistics for testing in England.
UKHSA is consolidating where COVID-19 testing statistics are published to make it easier to find the latest data. From 17 December 2020, this publication no longer includes information on COVID-19 testing in the UK. This information can instead be found on the COVID-19 in the UK dashboard. Statistics on positive cases are published daily on the dashboard and weekly in the NHS Test and Trace publication.
These statistics have been produced quickly in response to developing world events. The Office for Statistics Regulation, on behalf of the UK Statistics Authority, has reviewed them against several important aspects of the Code of Practice for Statistics and regards them as consistent with the code’s 3 pillars of trustworthiness, quality and value.
NHS Test and Trace, England
This section covers the methodology for:
- NHS Test and Trace statistical bulletin
- NHS Test and Trace data tables
- demographic and regional information for people tested and testing positive
For information on PCR and LFD tests conducted and the rapid asymptomatic testing bulletin see the Tests conducted, England section below.
NHS Test and Trace in England was launched on 28 May 2020 to ensure that anyone who develops symptoms of COVID-19 could quickly be tested to find out if they have the virus. It then helped trace recent close contacts of anyone who tested positive for COVID-19 and, if necessary, notified them that they must self-isolate at home to help stop the spread of the virus. Routine contact tracing ended on 24 February 2022. The flow of how people have moved through the NHS Test and Trace service is shown in Figure 1.
UKHSA publishes weekly statistics on NHS Test and Trace. The purpose of this data is to provide a weekly update on the implementation and performance of NHS Test and Trace. Data collected for the Test and Trace programme is primarily for operational purposes and was not designed to track the spread of the virus. Studies into the spread of the virus in the UK are carried out by the Office for National Statistics (ONS). Further guidance can be found in comparing methods used in the COVID-19 Infection Survey and NHS Test and Trace, England.
A list of data sources relating to the COVID-19 pandemic in the UK can be found at COVID-19 statistics and analysis.
Figure 1: flowchart showing how people have moved through NHS Test and Trace
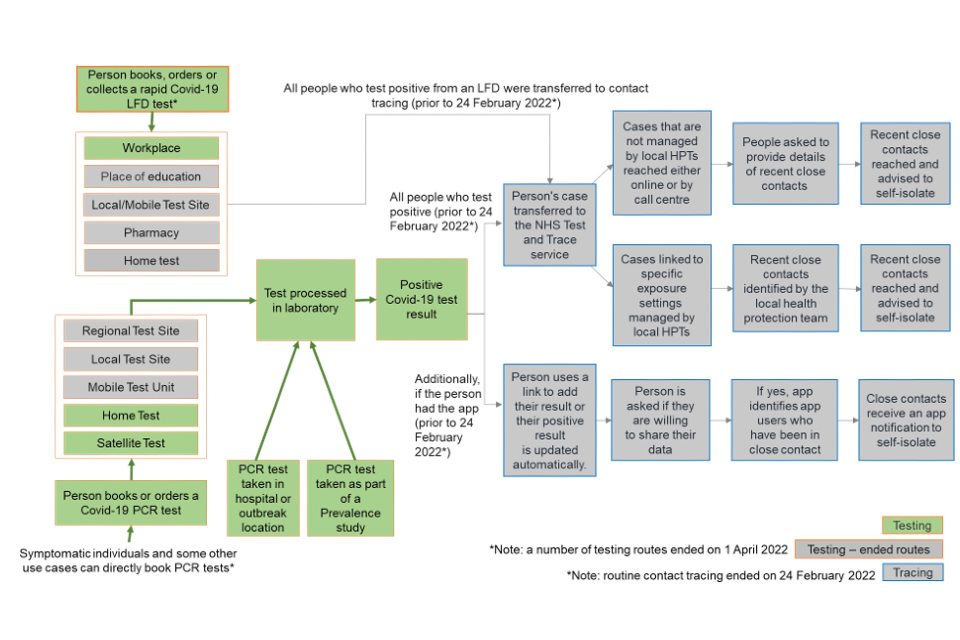
Figure 1 shows, in green, the remaining elements of NHS test and trace since contact tracing ended on 24 February 2022 and in-person testing routes ended on 1 April 2022. This includes either an LFD COVID-19 test within a workplace, or a PCR COVID-19 test at home or swab tests carried out at satellite testing centres.
Figure 1 shows, in grey, testing routes that have now ended and routine contact tracing that has now ended. Prior to the removal of free testing on 1 April 2022, for those taking LFD tests, they could collect their test from their workplace, pharmacy or local or mobile test site. They could also order a free LFD test to be delivered to their home.
Currently, booked PCR tests can be conducted at home via home test kits or at satellite test centres. PCR tests can also be taken in hospital or as part of a prevalence study. After tests have been taken, they are sent to a laboratory for processing. Once processed, a person will be emailed or texted their result. From 11 January 2022 in England, people who received positive LFD test results for COVID-19 were required to self-isolate immediately and were not required to take a confirmatory PCR test. Since 24 February 2022, the requirement to self-isolate has been removed. From 1 April 2022 booked PCR tests are no longer conducted at regional test sites, local test sites or mobile test units.
Prior to contact tracing ending on 24 February 2022, if a person had a positive COVID-19 test result, then their case was transferred to NHS Test and Trace and could be managed in one of two ways. First, cases not managed by local health protection teams (HPTs) were reached either online or by a call centre. They would then be asked to provide details of recent close contacts. These recent close contacts were then reached by NHS Test and Trace and advised to self-isolate. Second, cases linked to certain exposure settings were escalated to local HPTs who work to identify and reach recent close contacts and advise them to self-isolate. Additionally, if the person had the app and used the app to book their test, their positive result would be updated automatically. If they had the app but booked their test via a different route, they could use a link to add their positive result to the app. After entering their positive result into the app, the person would then have been asked if they are willing to share their data and if they said yes, the app would identify other app users who had been in close contact with the person who tested positive. Close contacts would then receive an app notification to self-isolate. On 24 February, routine contact tracing ended. Local health teams continue to use contact tracing and provide context-specific advice where they assess this to be necessary as part of their role in managing infectious diseases.
Since 1 April 2022, free LFD tests are no longer available to the public and individuals should only report the results of LFD tests they received prior to this date. In-person testing (at regional test sites, local test sites and mobile testing units) also ended on 1 April 2022.
Coverage
NHS Test and Trace is for England only. Therefore, the figures in this section are given for England only. Similar programmes are in place in Scotland, Wales and Northern Ireland but this data is not part of the NHS Test and Trace programme and is owned and managed by Public Health Scotland, the Welsh government and the Northern Ireland Public Health Agency respectively. Information is available at their statistics release pages:
Data sources
This data is collected from management information generated during the operation of the NHS Test and Trace service. The different data streams are collated centrally by UKHSA. Testing data is also collected by UKHSA and the time taken to receive a COVID-19 test result is taken from data collected and stored by commercial partners.
Timings and revisions
Figures given in previous releases are routinely revised each week going back to the start of Test and Trace.
The figures presented are based on a data cut taken several days after the end of the reporting period. This is to give time for data relating to the end of the 7-day period to be collected. Some data may continue to be collected after this period, and therefore may need to be revised over time.
Time series
Data is released as a time series of weekly data that is updated each week. Historic data may be revised if more accurate information is available later (see Timings and revisions above). This means that individual figures will not necessarily align with what was published earlier on GOV.UK.
Testing in England
NHS Test and Trace starts with an individual taking a swab test, either in pillar 1, pillar 2 or pillar 4. Those who go on to test positive[footnote 1] will have their case transferred to NHS Test and Trace for contact tracing. The majority of these are people who were tested under pillar 1 or pillar 2 of the government testing strategy:
- pillar 1: swab testing for the virus in UKHSA labs and NHS hospitals for those with a clinical need, and health and care workers
- pillar 2: swab testing for the virus in the wider population, through commercial partnerships[footnote 2], either processed in a lab or more rapidly via LFD tests
- pillar 3 testing: serology testing to show if people have antibodies from having had COVID-19
- pillar 4 testing: blood and swab testing for national surveillance supported by UKHSA, ONS and research, academic and scientific partners to learn more about the prevalence and spread of the virus and for other testing research purposes, more information is available at COVID-19 surveillance guidance[footnote 3]
There are several different types of COVID-19 tests available including PCR tests and LFD tests. In certain settings LAMP tests are also available. Details on each type of test are given in Types of COVID-19 testing in the section for Tests reported, England below.
It is a legal requirement that all positive cases are reported to UKHSA, irrespective of pillar or test type. As such, when pillar 4 research studies (for swab testing) identify positive cases, UKHSA is notified and this data flows into the surveillance system. This means that currently all positive cases identified by pillar 4 surveillance studies are captured under pillar 1 or 2 and are transferred to NHS Test and Trace. The same applies to those tested as part of the volunteer testing network: they are reported to UKHSA under pillar 1 and any positive cases are transferred to NHS Test and Trace. Pillar 3 (serology testing to show if people have antibodies from having had COVID-19) are not transferred to NHS Test and Trace.
Once conducted, tests are processed and the results are sent back to the individual through an email or an SMS.
Between 30 November 2020 and 26 January 2021, anyone who received a positive LFD result was instructed to take a confirmatory PCR test. The individual and their household were advised to self-isolate from the point of the positive LFD result being received. Contact tracing would then be initiated if a positive PCR was received. If a negative PCR was received after a positive LFD, the individual and their household were advised they no longer needed to self-isolate.
Between 27 January 2021 and 29 March 2021, a positive LFD test consequently initiated contact tracing without requirement for a confirmatory PCR test and the individual and their household were advised to self-isolate from the point of the positive LFD result being received.
From 30 March 2021 to 10 January 2022, the requirement to take a confirmatory PCR test was reinstated for all positive LFD tests. A positive LFD result continued to trigger contact tracing; however, NHS Test and Trace introduced improvements to automatically inform anyone self-isolating from a positive LFD to stop isolating if the confirmatory PCR was taken promptly and was negative. These individuals were then removed from contact tracing.
From 11 January 2022, the requirement to take a confirmatory PCR has been suspended, with a positive LFD test initiating contact tracing and the individual being required to self-isolate from the point of the positive LFD results being received. There are exceptions to the suspension and they are detailed in the following press release.
For more information on the types of test see the Types of COVID-19 testing section below.
People tested and people testing positive
For both pillars 1 and 2, data for England is provided by the NHS and UKHSA and the number of confirmed cases is collated to give the total number of confirmed cases over the reporting period. The headline figures reported in this publication for people tested and people testing positive include both LFD tests and polymerase chain reaction (PCR) tests, deduplicated for each reporting week.
More details about the data sources and methodology for pillar 1 and pillar 2 can be found in the section COVID-19 testing in the UK. Individuals with negative results from pooled tests are included in these figures. Individuals with positive results from pooled tests are excluded; however, the results from re-tests for those individuals are included.
From 9 April 2021, individuals who receive a positive LFD test result and subsequently a negative confirmatory PCR (within 72 hours) are removed from these figures. From 21 May 2021, individuals that receive a positive LFD test result and subsequently negative confirmatory PCR tests within 3 days that are all negative are removed from the underlying data used to produce these figures on a daily basis. More information on this methodology is given on the about the data page of the COVID-19 in the UK dashboard.
From 15 October 2020, the methodology for people tested and people testing positive has changed
Previously, the number of people newly tested and newly testing positive was reported, where the figures were deduplicated over the entirety of the pandemic so an individual would only appear once. This meant someone tested in March and again in September would only be counted in the March counts. This was progressively becoming less meaningful the longer the duration of the pandemic and meant that it was not appropriate to calculate a positivity rate from this data.
Figures are now reported as people tested and people testing positive at least once in the reporting week. People tested or testing positive are only counted once over the 7-day reporting period (Thursday to Wednesday), with a positive test being prioritised over a negative test. A person can be counted within more than one 7-day reporting period. If someone was tested more than once in different reporting weeks, they would be included in the count for all reporting weeks they were tested in.
For example, if a person was tested on Thursday and Friday of the same week, they would only be counted once in the reporting week. However, if someone was tested on Tuesday and Friday of the same week, that individual would be counted in 2 reporting periods, as the 2 tests fall into different 7-day reporting periods. If a person is tested under both pillar 1 and pillar 2 in the same reporting week, then only the pillar they were first tested under is counted, unless they were tested in both pillars on the same day, in which case, they are counted under pillar 2.
If someone had both a positive and a negative result in the same week, only the positive case would be counted, with the result being counted in pillar associated with the positive result. All previous reporting weeks have been backdated and revised with the new methodology.
When deduplicating within the reporting period, people have been matched using a fuzzy matching process. This involves using a combination of name, NHS number and date of birth to find duplicates and then remove them. Due to the nature of the matching, this will not always be a perfect match and there may sometimes be more people removed than necessary, for example, if someone has the same name and date of birth. However, this should only affect a small number of tests.
Demographic and regional data for people tested and people testing positive at least once in the reporting week is available in the weekly collection page. This data has been updated to account for the change in methodology for people tested and people testing positive. Demographic information is published for age, gender, UTLA and LTLA. For pillar 1, data is collected by the hospital, and is then enriched using patient records. For pillar 2, this data is collected when people register for a test and is voluntary, which means that people have the option not to provide their information. Note that for age, a person may fall into more than one age group if their age has changed between reporting weeks in which they were tested.
From 7 January 2021, this data will only be available for those tested using PCR tests (data also includes a small number of people tested using LAMP tests). This is to ensure the positivity rate remains comparable over time (see the Weekly positivity rate section for more information). Age and gender breakdowns for positive cases that include LFD and PCR tests can be found on the COVID-19 in the UK dashboard.
From 19 November 2020, regional information is derived using the person’s address recorded in the laboratory information systems at the time of testing. Before this, a person’s NHS Summary Care record was used. This change was applied to historical data since 1 September 2020 and has been revised. See COVID-19: comparison of geographic allocation of cases in England by lower-tier local authority for more information.
The totals provided for people tested and people testing positive in the demographic tables will not align with the total number of people tested and people testing positive given in the main publication. This is due to the exclusion of LFD tests in the demographic tables in addition to differences in when the data is taken, which means that one source may be more up to date than the other.
The cumulative number of people newly testing positive (deduplicated over the entirety of the pandemic) is available on the COVID-19 in the UK dashboard.
From 1 April 2021, the Northamptonshire upper tier local authority has been abolished and replaced with two new unitary authorities: North Northamptonshire and West Northamptonshire. The lower tier local authorities Corby, East Northamptonshire, Kettering and Wellingborough were incorporated into North Northamptonshire, and Daventry, Northampton borough and South Northamptonshire into West Northamptonshire. This change has been incorporated into the publication from the 15 April release onwards. Historic data for these abolished authorities is still available in previous releases.
For more information on local authority boundaries, see the Office for National Statistics Open Geography Portal.
Weekly positivity rate
It is no longer recommended that the headline figures for people tested and people testing positive are used to calculate a positivity rate. This is because it’s likely that LFD tests have a different positivity rate to PCR tests due to the use of LFDs in rapid testing. As the number of LFD tests reported is increasing over time, a consistent positivity rate cannot be calculated. From 7 January 2021, the weekly positivity rate has no longer been calculated as part of this publication but can instead be found on the COVID-19 in the UK dashboard for PCR only positive cases in England. As this is for PCR tests only, the positivity rate is comparable over time.
In addition, from 7 January 2021, the breakdown for the number of people tested and number of people testing positive in each reporting week, by age, gender and local authority (found on the weekly collection page) will only include those who have tested positive from a PCR test. This ensures the positivity rates calculated are consistent over time. Age and gender breakdowns for positive cases that include LFD and PCR tests can be found on the COVID-19 in the UK dashboard.
Note that these PCR-only positivity rates should not be used as a measure of prevalence for the general public as people tested using a PCR test is still not a random sample and is instead focused on people who may be more likely to have COVID-19. Additionally, it will not be an accurate measure of prevalence for the general public as some people will be asymptomatic and not all people who experience COVID-19 symptoms will get tested.
More information about the estimated number of people who have COVID-19 at a given time can be found in the UKHSA surveillance reports and ONS Coronavirus Infection Survey pilot.
Time taken to receive a COVID-19 test result
The time taken to receive a COVID-19 test result is included in the weekly NHS Test and Trace publication for both pillar 1 and pillar 2 testing in England.
For both pillar 1 and pillar 2 turnaround times, the total number of test results reported (and the time taken to do so) is not the same as the number of people tested.
For clinical reasons, some people are tested more than once. Therefore, the number of tests will be higher than the number of people tested. There are several valid reasons why some individuals may be tested more than once, including:
- regular testing of health and care workers
- individuals who have the virus, test positive, and have a subsequent test to see if they can return to work
- participation in early trials comparing healthcare professionals administered tests with self-administered tests, resulting in 2 results on the same day
- participation in research studies conducting routine tests on the same people each month
- some tests may come back as ‘void’ and a retest would be issued
- individuals with early symptoms who test negative, develop more symptoms and are retested and found to be positive
- regular testing required by the workplace
The data for the time taken to receive a COVID-19 test result has not been deduplicated. This means that the time taken to receive a COVID-19 test result is given for all tests that have been taken, including those tests that have been carried out on the same person more than once.
Pillar 1 testing turnaround times
Pillar 1 testing includes swab testing in UKHSA labs and NHS hospitals for those with a clinical need, and health and care workers. These tests are conducted in hospitals and outbreak locations. The data is recorded by UKHSA and NHS labs and covers England only, in line with the tracing data. The location is based on the laboratory site where the test was processed, which is usually an NHS hospital.
The time taken to receive a COVID-19 test result through pillar 1 is only available from 9 July 2020 due to differences in the reporting methodologies for NHS and UKHSA labs. Before this, data regarding the time taken to receive a COVID-19 result is not comparable across UKHSA and NHS labs. For consistency with other government publications, only comparable data has been included in order to give an overall picture for pillar 1.
There remains a small number of study samples and tests from private laboratories which are excluded from turnaround time figures as no timing data is available. Generally, these tests make up less than 5% of the tests reported and so their absence should not greatly affect the overall totals.
As some pillar 1 tests are provided to hospital patients, it is not practical for those administering the tests to record the exact time at which the test was taken. Therefore, the time taken to receive a COVID-19 test result is measured from the time that a test is received by a laboratory for processing to the time when the results are published to the Laboratory Information Management System (LIMS). The time taken to receive a COVID-19 test result is given as the number of tests results available within and after 24hrs of the test being received. This definition differs from those used for pillar 2 so the time taken to receive a COVID-19 test result cannot be compared across pillar 1 and pillar 2.
The number of tests included in the time taken to receive a COVID-19 test result is consistent with testing data published on the COVID-19 in the UK dashboard. The pillar 1 tests by nation on COVID-19 in the UK gives the pillar 1 tests for England daily and the sum of these over the given period will be consistent with the statistics provided here. However, the number of tests will not match exactly due to:
- the small number of study samples and tests from private laboratories that have been excluded from the time taken to receive a COVID-19 test result, but which are included in the pillar 1 tests by nation
- differences in when the data is taken, which means that one source may be more up to date than the other
Pillar 2 testing turnaround times
There are various routes for getting tested within pillar 2 (national swab testing). Data on the time taken to receive a COVID-19 test result for pillar 2 is presented for all routes combined and split up to reflect the different routes, as this impacts on the turnaround times. Note that this data does not include LFD tests. The current routes for taking a test through pillar 2 are:
- satellite test centres, which includes test kits provided directly to ‘satellite’ centres at places like care homes or hospitals that have a particularly urgent or significant need – the majority of tests from satellite test centres are care home tests
- home test kits, which are delivered to someone’s door so they can test themselves and their family without leaving the house
Previously, local test sites, regional test sites and mobile testing units were also included. However, these ended on 1 April 2022 and are no longer reported on.
From 4 March 2021, new satellite sub-channels have been included within the satellite test turnaround time data. These new sub-channels make up approximately 5% of the total number of satellite tests and includes satellite tests used by schools, hospices and within domiciliary care. From 18 March 2021, further sub-channels have been included to the satellite channel, making up 0.1% of the total number of satellite tests. This includes tests used in adult day-care centres and arrivals from red countries. Data previously published for satellite testing turnaround times has been revised to include these new routes.
From 18 March 2021, new sub-channels have been included within the home test turnaround time data. These new sub-channels make up approximately 8% of the total number of home tests and includes tests used in schools, for arrivals from amber countries and in vaccine trials. Data previously published for home testing turnaround times has been revised to include these new routes. From 11 November 2021, additional subchannels for vaccinated international arrivals, the events research program and dental patient testing were added to the home test turnaround data making up approximately 10% of the weekly number of home test kits.
The data for pillar 2 has been taken for England only.
For home testing and satellite test centres, people’s home addresses are used to assign the location of the person being tested. Note: this methodology has changed from using the location of the lab that processes the test, which was used until the start of August 2020. Previous figures have been revised to take into account the new methodology.
Testing turnaround times data does not include Randox tests, as these are handled through a different system. This will not affect the data for home test kits, but Randox tests made up a significant proportion of the tests reported in care homes, which form part of the satellite test centres. Until 16 July 2020, Randox tests made up just under 40% of the tests used in care homes. However, their use is being phased out and from 17 July 2020 these tests make up less than 5% of the tests reported in care homes.
The number of tests included in the time taken to receive a COVID-19 test result will not be the same as the total number of people tested for COVID-19. In addition to the general reasons stated in the Time taken to receive a COVID-19 test result section, there are a number of reasons for this:
- the source for the time taken to receive a COVID-19 test result is different – the number of people tested and testing positive for COVID-19 is taken from UKHSA, whilst the time taken to receive a COVID-19 test result is taken from commercial partners
- the data for the time taken to receive a COVID-19 test result has not been deduplicated – this means that the time taken to receive a COVID-19 test result is given for all tests that have been taken, including those tests that have been carried out on the same person more than once
- the time taken to receive a COVID-19 test result uses different metrics to segregate data for England from the UK
- the time taken to receive a COVID-19 test result is reported by the date the test was registered whereas people tested are reported against the specimen date
For pillar 2 satellite test centre and home test kits, the time taken to receive a COVID-19 test result is defined as the time from when a person completes a test registration (or the time a person indicates their test was taken for home testing kits) until the time that they receive a notification of the result of their test via an email or an SMS. Details are given below. From 27 August 2020, median turnaround times are reported in addition to the usual turnaround time windows, such as within 24 hours. For all measures the test is recorded against the date the test was registered.
For all measures of time taken to receive a COVID-19 test result, there are a number of test results that were not received. This covers any test where the results were not communicated, which may be because communication details (for example, phone number or email address) were not provided or were incorrect, or because the test was cancelled or abandoned, or no result was available. It also includes some tests that are still being processed. Some of these people may still have been passed into the contact-tracing system, but the data from the pillar 2 test does not show that their tests were complete. From 17 September 2020 the number of results not received was split to show those which were unsuccessful and those still in progress. Previously these were reported together.
Time taken to receive a COVID-19 test result from time of test
The time taken to receive a COVID-19 test result from time of test is measured from the time a person completes a test registration (or the time a person indicates their test was taken for home testing kits) until the time that they receive a notification of the result of their test via an email or an SMS. The time that a person completes their test registration should reflect the approximate time that the person took their test, but the accuracy of this will vary depending upon the route that they used to take the test.
For home testing kits, the start time is measured from the time a person inputs that they took their test (note that this process changed from the time a test was registered using a barcode scan, from July 2020 onwards). When a person registers their test, they are asked to give the time that their test was taken. This measure is self-reported but allows current and previous data to be measured using the same definition and allows for a more accurate end-to-end time to be calculated.
For satellite test centres, the time of test registration may not exactly align with the time that the test is taken. For example, a care home might complete registrations the night before they administer the tests. However, the start time used is consistent enough to provide comparable data on the time taken to receive a COVID-19 test result from the time of test for all mechanisms of testing. Satellite tests are predominantly used by care homes who need greater control and flexibility over when test kits are collected. For example, tests may be conducted over multiple days with a collection scheduled a few days later. Because of this, a lower proportion of test results will be available within 24 hours of the test being taken.
After someone takes a test, their test is transported to a laboratory for processing. There are normal fluctuations in this operational process which can sometimes cause the time taken to receive a test result to go over 24 hours, but still be turned around the next day. Where appropriate, the number of tests turned around the day after a test was taken are provided.
Tests reported, England
This section describes the methodology behind the data published in the ‘Tests reported’ data tables on the weekly collection page and the statistical bulletin on rapid asymptomatic testing.
Data sources
Several organisations supply data from multiple sources into the weekly statistics on testing. The different data streams are collated centrally by UKHSA. NHS Digital provides data for England and some data comes from commercial partners.
The data provided by the organisations mentioned above is provided under Data Sharing Agreements allowing the UKHSA access.
Coverage
For PCR tests, this data contains tests reported through the pillar 2 testing routes only (swab testing the wider population).
For the total number of LFD tests, this data includes those reported through the existing National Testing Programme digital infrastructure and doesn’t include LFD tests reported where the tests were not registered via this route. The following use cases for LFD tests are not reporting results digitally into Test and Trace systems, and therefore are excluded from the totals in this report:
- testing for the majority of NHS secondary care staff – these are reported separately in the publication
- testing for some staff in private sector industries
- testing for some hauliers – these are published separately at haulier COVID-19 testing
In these cases, test results should be reported directly to UKHSA.
An LFD test produces a result on the device almost immediately, without it being automatically recorded, therefore some results might not be captured. For settings where self-reporting LFD testing procedures are in place, it is likely that the number of tests that are reported in this publication are underreported. It is however their statutory duty to do so, and easier reporting tools are being rolled out to support these individuals to report their tests as quickly and efficiently as possible. It is possible that tests with a negative result are more likely to be affected, therefore it is not advisable to calculate a positivity rate with the data.
Timings and revisions
A snapshot of this data is taken for publication several days after the end of the reporting period to give time for tests reported at the end of the 7-day period to be captured. Figures given in previous releases are routinely revised as some tests may continue to be reported after this period.
Daily totals reflect actual counts reported for the previous day. Each day there may be corrections to previous reported figures. This means that previously published daily and weekly counts will not necessarily sum to the latest cumulative figure. It also means that today’s cumulative count may not match the previous day’s cumulative count plus today’s daily count.
Data is supplied daily from several different electronic data collection systems, and these can experience technical issues which can affect daily figures, usually resulting in lower daily counts.
If the quality of source data improves, there may be further revisions to historic time series. If this does occur, the rationale and impact of these revisions will be clearly highlighted.
Each weekly publication provides daily counts of tests reported from 28 May 2020; however, LFD tests were only made available from 21 October 2020. From 1 October 2020, the number of pillar 2 swab tests reported by lower-tier local authority (LTLA) was made available and from 10 December 2020, weekly breakdowns for LFD tests and PCR tests have been added. This includes whether the test was positive, negative or void and lower-tier local authority breakdowns.
Types of COVID-19 testing
Lab-based virus tests
These test for the presence of COVID-19 using a swab which is processed in a lab via PCR. They are carried out within pillar 1, pillar 2 and pillar 4. This type of test is predominantly used for:
- anyone who has symptoms
- to confirm a positive LFD test result
- regular asymptomatic testing in social care
In order to increase the capacity of the testing system to produce results, pooling of lab-based virus tests is being piloted within universities and adult social care from October 2020. Multiple swabs from individuals in the same household are grouped at point of swabbing and processed in the lab as one vial, a test result is then issued for all individuals that formed part of the pool. A negative result indicates that all individuals tested negative. A positive result indicates at least one individual is positive and all individuals are subsequently retested individually. Pooled tests are not currently included in the pillar 2 test turnaround time data.
Antibody tests
Antibody serology tests test for the presence of COVID-19 antibodies. These include pillar 3 tests and antibody tests undertaken within pillar 4.
Lateral flow device tests
LFD tests, often referred to as rapid tests, test for the presence of proteins called ‘antigens’ which are produced by the virus. They are swab tests that give results in 30 minutes or less, without the need for processing in a laboratory. These tests are primarily used for those who do not have symptoms.
LFDs were only made available from 21 October 2020 and were initially available in limited capacity except for areas where rapid testing pilots were reported. Since then their availability has expanded, initially to a broader range of settings and from 9 April 2021 to everyone in England.
Prior to 27 January 2021, if an individual received a positive LFD test result they were required to take a PCR test to confirm this. Between 27 January and 29 March 2021 this was no longer a requirement except for those self-reporting their test result. From 30 March 2021 the requirement to take a confirmatory PCR was reinstated for all positive LFD tests.
LFD tests are reported for England only and daily data for LFD tests has been made available from 21 October 2020 on the COVID-19 in the UK dashboard.
Other testing technologies
Relatively new types of tests are also being made available in certain settings. Similar to PCR tests, Loop-mediated isothermal amplification (LAMP) technology amplifies genetic material for the purpose of detecting viral RNA associated with the virus that causes COVID-19. Saliva based LAMP testing allows for self-collection of saliva unlike the swabbing of the nose and throat, required for PCR testing. LAMP testing is currently used for some NHS asymptomatic staff testing and allows for a greater number of tests to be completed in a shorter time frame.
Number of tests reported
The ‘number of tests reported’ counts all tests that have remained within the control of the programme (including PCR swab tests and LFD tests) and those that have been sent out and subsequently returned to be processed in a lab (such as satellite and home test kits). They are counted at the time they are processed. For a PCR test this is when the test is processed in a lab, for an LFD test this when the test was taken.
From 15 April 2021 there has been an improvement to the methodology for the number of PCR and LFD tests reported, whereby the data has been deduplicated to ensure an individual test is only counted once. Figures for previous weeks have been revised accordingly and a very small number of tests, less than 1% of the totals, have been removed.
The number of tests reported is reported by the 3 possible results of taking a test:
- positive
- negative
- unknown or void
Reasons for unknown or void tests include:
- the testing within the laboratory was unable to give an exact answer as the test gave an equivocal result (it was not clearly negative or positive)
- there was an issue with the sample when it is delivered to the laboratory making it impossible to return a result, such as the tube was damaged or leaked, the test could not be scanned, the instructions were not followed or the swab was not put in the tube. Due to the issue with the sample, some of these tests may not have been processed by the lab at all
- for LFD tests, an unknown or void test result is returned on the device if the test has not run correctly and individuals are advised to take another test
The number of PCR and LFD tests reported are also published by local tier local authority. An individual’s postcode of residence provided by the test subject is used to determine their local authority. Data for City of London and Hackney as well as Cornwall and Isles of Scilly have been combined due to their smaller population size.
From 1 April 2021, the Northamptonshire upper tier local authority has been abolished and replaced with two new unitary authorities: North Northamptonshire and West Northamptonshire. The lower tier local authorities Corby, East Northamptonshire, Kettering and Wellingborough were incorporated into North Northamptonshire, and Daventry, Northampton borough and South Northamptonshire into West Northamptonshire. This change has been incorporated into the publication from the 15 April release onwards.
Historic data for these abolished authorities is still available in previous releases. For more information on local authority boundaries, see the Office for National Statistics Open Geography Portal.
These figures are provisional, based on management information for testing. These figures will not align with those published on the COVID-19 in the UK dashboard as they are derived from a different data source with different associated methodology. The reasons for the differences are below:
- a cut of the data was taken at different points in time for each source
- this report uses the date a test was processed in the laboratory whereas the dashboard reports on the date reported by laboratories
- the LTLA is determined using the postcode of the person tested, the dashboard data is only available at a national level and this is determined by each of the individual devolved administrations
- daily data on the dashboard is not routinely revised figures whereas figures in this report are updated for previous dates when each data cut is taken
From 11 January 2022, individuals who received a positive LFD test are no longer required to take a confirmatory PCR. Further information can be found in the press release on confirmatory PCR testing.
Positive predictive value
The positive predictive value (PPV) represents the probability that a reported positive result from a COVID-19 test is a true positive. The PPV is calculated from the number of true positives divided by the sum of the number of true positives and the number of false positives.
The PPV of a test result will depend on the sensitivity and specificity of the test when used in a given setting and the level of virus prevalence in the population being tested.
Number of LFD tests reported in education settings
Primary schools and nurseries
Since 18 January 2021, on-site staff in primary schools, school-based nurseries, and state-maintained nurseries have been able to take an LFD twice weekly at home. From mid-March this was expanded to all private, voluntary and independent nurseries. Primary and nursery staff self-report their test result, therefore if an individual receives a positive result, they are then required to take a confirmatory PCR test. Primary school students are not currently being tested. This is because serious COVID-19-related illness is extremely rare in children and there is lower case rates and transmissions in younger children in comparison to secondary school children. Primary school aged children are likely to find repeated testing unpleasant and parents may find it challenging to repeatedly swab young children.
Secondary schools and colleges
LFD testing within secondary schools and colleges was implemented for on-site staff from 4 January 2021. Staff were expected to take a test once a week initially. However the guidance was updated at the start of the national lockdown to twice-weekly testing for those staff attending schools and colleges. Initially, secondary school staff testing was assisted via the use of an asymptomatic test site, however from 25 February they were encouraged to use home test kits. From the 8 March testing was expanded to all secondary school staff and students. On their return to school, students are required to take 3 tests (spaced 3 to 5 days apart) at their onsite asymptomatic test centre. Following this, they then begin twice weekly home testing. For more information see mass testing for secondary pupils.
Households and bubbles of school students and staff
From 1 March 2021 households, childcare and support bubbles of primary and secondary school students and staff are able to take an LFD test twice a week. Tests reported by these individuals are included within the figures for the school they are associated with. There are numerous ways these groups of individuals can receive a test. For more information see rapid lateral flow testing for households and bubbles of school pupils and staff.
Higher education
Rapid LFD testing was implemented by higher education providers from 27 November 2020 to support the safe travel of students over the winter break. Tests taken prior to this were part of testing pilots. In January twice weekly asymptomatic testing was introduced for staff and students accessing university facilities. This was delivered through supervised on-site asymptomatic testing sites. Asymptomatic testing has continued into the summer term and, from May, providers are able to set up LFD collection points to enable students and staff to test at home and self-report their result. All students returning to university from 17 May are encouraged to take 3 tests (3 to 4 days apart) at an on-site test facility, where available, before testing twice a week on-site or at home thereafter. For more information on testing in higher education please see the higher education COVID-19 guidance.
Number of LFD tests by phase of education and individual role
The number of LFD tests reported in the education sector are reported with a breakdown per phase of education and role (staff, student, household bubble and support bubble). LFD test result breakdowns are reported by the date the test result was communicated.
Primary school, schools-based nurseries and maintained nursery school data is collected from the self-reporting process. Secondary school and college data is identified from asymptomatic test sites linked to schools, and by linking information captured by the individuals when they self-report to data held for each institution. Secondary school and college figures also include tests not registered (see the section ‘data quality for testing in education’ below for more information). Data for higher education establishments is identified from tests reported at their asymptomatic test sites and from May also includes self-reported tests linked to the higher education providers.
For tests taken prior to 5 March, the individual role (staff or student) is determined using age as a proxy. An individual aged 20 or over is categorised as a staff member and under 20 a student. This method is not appropriate for colleges and higher education and therefore is not included. From 5 March, the self-test registration process will soon gathers this information and determines on whether someone is a staff member, student, part of a household, childcare or support bubble. The figures for tests taken by school household bubbles and school support bubbles are therefore only available from 5 March. Students and staff can also get tested at an asymptomatic test site (ATS), tests taken via this route continue to use age as proxy for staff and students.
The number of LFD tests reported by phase of education will not be directly comparable to the number of tests reported in England. There are a number of reasons for this:
- the source for the number of LFDs by phase of education is different
- the number of LFD tests by phase of education test result uses different metrics to segregate data for England from the UK
Data quality for testing in education
Testing in primary schools, schools-based nurseries, maintained nursery schools, secondary schools and colleges is carried out using self-report LFD tests, hence the level of data quality and accuracy is entirely reliant on subjects reporting the result of the LFD test and completing the testing journey.
For tests reported after 25 February, reference data from the Department of Education is used to determine the phase of education. For some tests where there is a lack of information captured, the test cannot be linked to a type of school. For the purposes of this report, these tests are reported separately as unidentified phase of education. In addition, a small number of secondary school tests prior to the 31 December 2020 have been excluded due to pilots not reporting digitally.
Age is used as a proxy for individual role for any tests prior to 5 March or where a test was taken at an ATS. Note, only students and staff are able to test at an ATS and not household or support bubbles.
Higher education reference data is used to determine which tests were reported in higher education providers. Given the decentralised site creation, there is no immediate visibility of new sites but these are incorporated into the data over time.
Tests not registered refers to tests which have been reported. However the individual has not digitally registered their test. This means these tests cannot be linked back to individuals in the system and a limited amount of information is captured. From 25 March the methodology has improved to identify which phase of education these tests belong to. Almost all tests not registered are attributed to secondary schools and colleges as they arise from on-site testing. The number of tests not registered are reported separately in the figures for secondary schools and colleges, and are included in the totals. The total tests for secondary schools and colleges for all previous weeks has been revised accordingly. A very small number of tests not registered belong to other phases of education and therefore these are not included.
Number of LFD and PCR tests reported in care home settings
The number of tests reported in care homes includes staff, residents and visitors tested via kits directly sent to the care home. It will not include care home staff, residents or visitors who are tested via a different route (for example, at a regional or local test site, mobile testing unit). The figures related to adult care homes and children’s care homes are excluded.
The number of LFD and PCR tests are counted on the day the test result was communicated. These figures only include tests which were registered, therefore if tests were reported but not registered online by the care home or individual then these will not be counted.
The number of tests reported is reported by type of test and by the individual role (staff, resident, visitor and visiting professional) which is captured when the test is registered. For some tests a limited amount of information is available therefore the individual role cannot be determined. These tests are reported separately in the data tables.
Due to the change in guidance issued on 23 December 2020 to increase testing in care home staff, the requirement for care home staff to register negative LFD test results was suspended between 31 December 2020 and 15 January 2021 inclusive. As a result, a proportion of LFD tests reported on care home staff will not be included for these dates.
Background on testing in care homes
Staff
Routine asymptomatic testing of care home staff began on 7 June 2020 with weekly PCR tests for staff. Enhanced testing began from 23 December 2020 with twice weekly rapid lateral flow tests for staff and rapid response testing in the event of a positive test result for 7 days.
From 16 February 2021, the rapid response testing was extended to cover daily rapid lateral flow testing for all staff until 5 days without a positive test result occur. Whole home PCR testing is undertaken in the event of an outbreak, first on day 1 and then again between day 4 to 7 of the outbreak.
The HPT can also use rapid lateral flow tests alongside PCRs for all staff at their discretion.
Residents
Routine testing of care home residents began on 7 June 2020 with monthly PCR tests for residents.
Whole home testing in the event of an outbreak was available from 22 January 2021, with PCR testing undertaken first on day 1 and then again between day 4 to 7 of the outbreak. From 16 February 2021 HPTs can also use rapid lateral flow tests alongside PCRs for all residents at their discretion.
Care home visitors
Rapid lateral flow tests were made available to some care homes for visitors to test on arrival for a visit from 2 December 2020. From 14 December 2020 this was rolled out to all care homes and all visitors were required to take an LFD test on arrival. Indoor visiting was suspended on 6 January 2021 in line with national lockdown restrictions. Throughout the period of national restrictions, visits were limited to outdoors, in visiting pods or with a substantial screen; as well as those in exceptional circumstances such as end of life.
From 21 June 2021, care homes residents can nominate 5 named visitors each, with 2 visitors being able to visit each day. These visitors should be tested using LFD tests on the day of every visit and produce a negative COVID test prior to their visit. Residents with the highest care and support needs can also have regular visits from an ‘essential care giver’ who will access the same testing arrangements as members of staff, that is a weekly PCR and (at least) twice weekly LFD.
Care home visiting professionals CQC inspectors
From 14 December 2020 CQC inspectors should take a weekly PCR test. From 22 March 2021 they should also conduct a lateral flow test prior to their inspection visit.
All other professionals
From 14 December 2020 all other professionals not already tested through regular NHS staff testing or CQC inspectors should be tested using an LFD test at the care home door immediately prior to a visit.
Additional information on testing in care homes
Following NHS guidance, issued on 16 February 2021, there is a window following a positive PCR result when care home staff, residents, and visiting professionals will not be tested. The window is 90 days from the onset of symptoms or, if asymptomatic when tested, 90 days after taking the positive test. This minimises additional positive results, which may be considered unnecessary as individuals are unlikely to be infectious. If the individual develops new symptoms during this window they will be immediately tested using PCR.
DHSC also publishes care home testing data in the monthly Adult social care in England statistics. This publication uses the same data source but has a different methodology for presenting testing in care homes and differences in the figures will occur due to the following reasons:
1.Differences in which tests from different routes are included
Both methodologies include the number of tests registered from kits sent directly to care homes, but the monthly Adult Social Care in England publication additionally includes care home staff or residents tested via other routes such as regional or local test sites. As a result, figures in this report will be substantially lower for PCR tests reported in care home staff due to the current guidance recommending staff with symptoms to be tested outside of the care home
2.Different reporting periods
This publication uses the date the test result was received in comparison to the Adult Social Care in England statistics which use the start time of the test
3.Different times of extracting the data
Number of LFD tests reported by NHS staff
Staff in primary care test at home using a self-test LFD kit twice weekly. They are required to report their result through the national testing programme digital infrastructure, using the online digital too. However, this is entirely dependent on the individual, therefore some underreporting is expected.
Staff in NHS trusts similarly self-test at home twice weekly but their test results are collated by their employer and not through the national testing programme digital infrastructure. The NHS trust then submits data for their staff to NHS Digital, which is separate to reporting through the National Testing Programme digital infrastructure. This separate reporting system was established this way as NHS secondary care providers began testing with LFDs before the NHS Digital reporting solution was built. Because of this, the figures for NHS trusts are not included in the national figures for the number of LFD tests reported via this route.
There are known differences in the completeness of the information provided by different NHS Trusts and the data collection process is dependent on the organisations submitting this information to NHS Digital. It is possible that there is some duplication of test results within the figures where NHS Trusts have reported the same results more than once in a given week. This is more likely to affect results up to 24 March 2021 before all NHS Trusts moved to a weekly submission through NHS Digital. However, where possible duplicates are identified and removed.
The timing of the weekly process of submission by NHS trusts means that data for the latest week is not available. Figures for tests reported by staff in NHS trusts are therefore published with an additional week’s lag in comparison to the rest of the data in this publication.
In addition, approximately 6,000 tests reported by staff in NHS trusts cannot be attributed to a test date or have a test date prior to the introduction of LFD testing, these are excluded from the figures. This is due to issues which arose during the data collection process from NHS trusts prior to 25 March.
Background information for NHS staff
NHS primary care staff
Primary care services provide the first point of contact in the healthcare system, acting as the ‘front door’ of the NHS. Primary care includes general practice, community pharmacy, dental and optometry (eye health) services. NHS staff in primary care were able to take an LFD test twice weekly since December 2020.
Staff in NHS trusts
NHS trusts include acute and specialist hospitals, community, mental health and learning disability and ambulance services. Staff in NHS trusts were able to get twice weekly LFD tests from November 2020.
Other NHS staff
Other NHS staff includes those working in the independent sector delivering NHS commissioned services or outside of primary care and NHS trusts. Staff in NHS-commissioned services in the independent sector were able to take twice weekly LFD tests from January 2021.
Number of LFD tests reported in workplace settings
The number of tests reported in private and public sector workplaces only includes tests which have been used and subsequently registered, either at an asymptomatic test site or via self-report at home. In addition, the number of tests reported in private sector workplaces only includes kits directly sent to private companies.
LFD tests reported in private and public sector workplace settings at an asymptomatic testing site are identified by the organisation’s Unique Organisation Number. Test reported via self-report as part of workplace testing are identified as users can declare the organisation for which they took the test.
Background on testing in private sector workplace settings
Since early November, staff in private and public sector workplace settings have been able to take an LFD test at an assisted testing site, however initially this was limited to staff in those organisations participating in testing pilots. Similarly, public sector staff began testing at home during a 5-week trial period in March, after which it was expanded to all government departments. From 6 April, at-home testing was rolled out to staff in private sector workplaces. Staff undertaking self-testing are asked to report their results through the national testing programme digital infrastructure, using the online digital tool. However, some underreporting is expected.
The figures in this report cover LFD tests registered through the National Testing Programme digital infrastructure, this includes on-site testing and self-testing, provided by NHS Test and Trace. Private sector companies can carry out testing using privately procured tests, these tests are reported via a different system and are not included in the figures. It is possible that some NHS tests may have been registered through this route and will therefore not be counted here, however, this is estimated to be a small proportion of all the tests reported.
Public sector workplaces refers to staff working in government departments. This includes organisations such as the Department for Transport, the Home Office, Ministry of Justice and Ministry of Defence. Initially, tests were made available via asymptomatic test sites, however from the beginning of March testing migrated to home LFD self-reporting. The majority of tests are taken by staff, however in some instances individuals affiliated with an organisation may also get tested. These figures do not include tests reported by haulier; they are published separately by the Department for Transport at Haulier COVID-19 testing.
Notes on interpreting weekly data
Each weekly update provides a snapshot of the testing within the 7-day period. The most recently reported week should be treated with some caution, as this data may be revised in the time series on the next release.
The statistics will be updated as more data becomes available and reportable. These are experimental statistics that are in the testing phase and not yet fully developed.
Notes on interpreting against other statistics
Historic figures for testing in the UK were available in the DHSC daily time series data but stopped being updated after 20 August 2020. Statistics on deaths, tests and cases are published daily in the UK COVID-19 dashboard.
Figures in the UK COVID-19 dashboard will be consistent with those published in the UKHSA Weekly Statistics for NHS Test and Trace reports. However, figures may not always exactly align due to the timing of data cuts. In addition, the dashboard reports positive cases deduplicated across the whole of the reporting period. The Weekly Statistics for NHS Test and Trace publication reports positive cases deduplicated across each weekly period. As a different methodology is used, these figures will not align.
Tests processed are published in this publication and tests reported are published on the dashboard. These will not align as tests processed counts all tests processed in a lab whereas tests reported includes all tests (swab, LFD and antibody tests), some of which are not processed in a lab.
Limitations
Given the importance of this service and the commitment of NHS Test and Trace to be open and transparent with the public it serves, these data are being released at the earliest possible opportunity. However, new IT systems and statistical outputs often take some time to bed in. This data should therefore be treated with caution while the system and our understanding of the data develops.
At this early stage, there is a risk of data entry errors or delay, which may require that data are revised and updated in subsequent publications. The process of finding and removing duplicate records may also need refining, which could result in revisions to the data.
Quality assurance
There are many stages of quality assurance in place to ensure the production process results in high quality outputs.
Input data
When the input data is received it is checked to ensure it is up to date, and there are no clear issues with it before the process begins.
The production code
All production code written in-house is rigorously tested and peer reviewed before used in the production process. When changes are made or new code this same process is followed before it is used.
Outputs
Tables are compared to previous outputs to check for larger revisions than should be expected and are also compared to other sources of similar information.
Text in the bulletin
Text changes in the bulletin are made by one person and are then checked and cleared by another person afterwards.
Related statistics
Testing statistics are also published in other places, including the COVID-19 in the UK dashboard, which is updated daily, and in the slides and data sets from the daily press conferences.
You can also view slides, datasets and transcripts from the press conferences at 10 Downing Street in response to COVID-19.
-
Between 30 November 2020 and 26 January 2021, those with a positive LFD test must have also had a positive confirmatory PCR test to trigger contact tracing. Between 27 January 2021 and 29 March 2021, confirmatory PCR tests were suspended and a positive LFD test triggered contact tracing. Between 30 March 2021 and 10 January 2022 the requirement to take a confirmatory PCR test was reinstated for all positive LFD tests. A positive LFD result continued to trigger contact tracing; however, NHS Test and Trace introduced improvements to automatically inform anyone self-isolating from a positive LFD to stop isolating if the confirmatory PCR was taken promptly and was negative. These individuals will then be removed from contact tracing. From the 11 January 2022 the requirement to take a confirmatory PCR was suspended with a positive LFD test triggering contact tracing. There are some exceptions to the suspension and they can be found on the following press release. ↩
-
The swab tests which are performed as part of the Vivaldi care home study whereby staff and residents undergo blood and swab testing, are captured under pillar 2. ↩