COVID-19 Winter Plan
Updated 2 December 2020

© Crown copyright 2020
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/covid-19-winter-plan/covid-19-winter-plan
Foreword from the Prime Minister
There can by now be no doubt about it – the scientific cavalry is almost here. The advances in vaccinations and treatments for COVID-19 are remarkable. In the hope and belief that they will be effective, the government has procured hundreds of millions of vaccine doses to be made available across the UK, the Crown Dependencies and Overseas Territories. We are preparing for a nationwide vaccination programme to be deployed at an enormous scale across the whole country from next month.
By the spring, these advances should reduce the need for economic and social restrictions. We should be able to render obsolete the very notion of a COVID-19 lockdown. We can now see the route out of this epidemic, provided the vaccines are approved and successfully deployed.
But the spring is still months away. We cannot just click our fingers, and inoculate the most vulnerable. It will take long and patient work, and a giant feat of logistics. That means we must be patient, and we must be realistic. There are still hard, cold months ahead – and in the meantime we must keep the virus under control.
January and February are traditionally the hardest months for the NHS, the depths of winter, when our hospital wards are under the greatest pressure. We cannot afford a third or even a fourth spike of the disease. And yet a new surge in the new year is exactly what will happen unless we fail to take adequate precautions.
So as we end our national restrictions on 2 December, they will not be replaced with a free for all. England will instead continue to use a sensible approach based on three tiers. And since the prevalence of the disease is, alas, still high, these tiers will remain tough.
Indeed they will be tougher than in October. No one wants to throw away the gains of lockdown. We must keep transmission down.
Even before the vaccine is here, we have a new tool at our disposal. We have new rapid turnaround tests that allow us to identify and isolate people who do not have symptoms but are unintentionally spreading the virus.
We are deploying these tests to NHS front-line staff, social care and other high-risk or critical settings. We are using them to help schools and universities to function and to drive down the outbreaks of the disease.
But it is also clear that there is another way of using these rapid tests – and that is to follow the example of Liverpool and test entire communities. In the weeks ahead we will be working with Local Authorities and communities to ensure that we offer this new tool in the areas that face the toughest restrictions, targeting testing at the areas that need it the most.
This system is untried. There are many unknowns. But if it works, we should be able to offer people who test negative the prospect of greater freedoms – to meet up in certain contexts with others who have tested negative. We will give support to those who have tested positive, to help them with isolation. But they will know that at the end of their isolation they too will have the prospect of greater freedoms.
And when towns, communities or regions can show that they have also engaged in community testing, they will have a much greater chance of reducing the restrictions under which they are living.
So, in the weeks to come we will be using these two scientific breakthroughs to fight the disease. We will be dispensing the vaccine as fast as we possibly can. But given that this will take time, we will simultaneously be using rapid testing to identify asymptomatic cases and to reduce transmission.
By keeping the virus under control this winter, the government hopes to enable friends and family to gather at Christmas. This will not, however, be a normal Christmas. Restrictions will remain, and there will continue to be a risk of transmission. But this is no longer an epidemic without end and I know that we have the resolve to see us through.
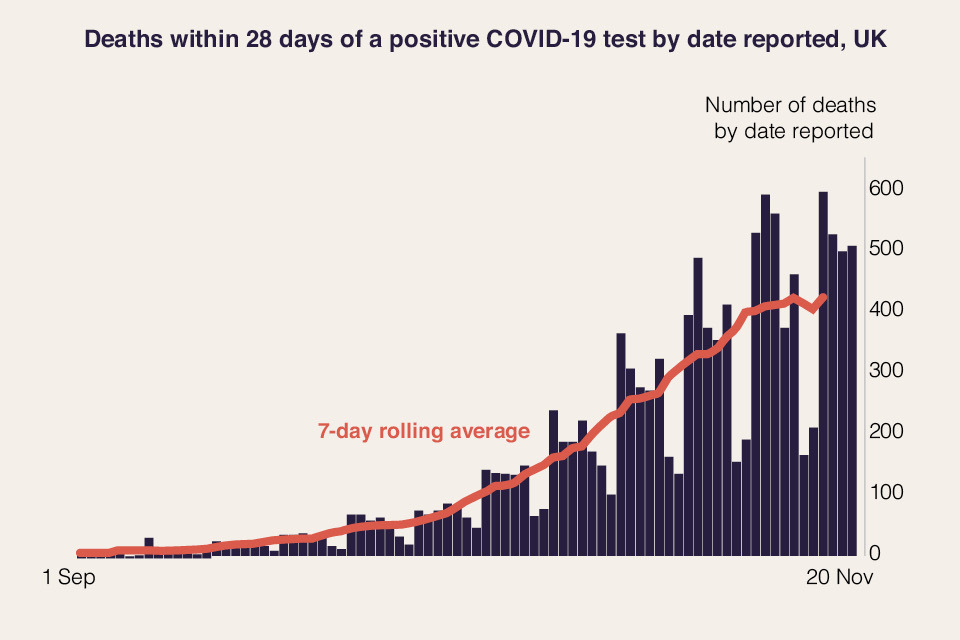
The public’s selflessness in following the rules is making a difference. The virus is not spreading nearly as quickly as it would if we were not washing our hands, maintaining social distance, wearing masks and so on. And in England, where national restrictions came into effect at the start of this month, the increase in new cases is flattening off.[footnote 1]
That would not have been possible without the public doing what has been asked of them.
Times have been tough. But the new year brings with it new hope – and, while there is still a long way to go, this plan shows how, together, we will get there.
1. Introduction
1. The UK Government’s COVID-19 Winter Plan presents a programme for suppressing the virus, protecting the NHS and the vulnerable, keeping education and the economy going and providing a route back to normality.
2. The UK Government’s overriding goal is to protect the lives and livelihoods of citizens across Scotland, Wales, Northern Ireland and England. It has worked closely with the devolved administrations on this shared goal. The government has procured vaccines for the whole of the UK, its testing capability serves all four nations of the UK and the government has carried out more tests than any other country in Europe. Significant quantities of Personal Protective Equipment (PPE) have been procured, manufactured and then distributed across England, Scotland, Wales and Northern Ireland. The Armed Forces have been invaluable in supporting communities and health services. HM Treasury has established an unprecedented package of support for businesses and individuals across the four nations of the UK. The coordinated approach of the UK authorities has been praised by the IMF as “one of the best examples of coordinated action globally - [that] has helped mitigate the damage, holding down unemployment and insolvencies”.
3. Vaccines are at the centre of the government’s plan. The global reach of the UK has put it in a strong position in the procurement of vaccines – with over 350 million doses secured by the UK Government for the benefit of all four nations.
4. Next month, the government will be ready for a UK-wide vaccination programme to begin, provided regulators approve the vaccines. Scientific advances in vaccination and treatments should reduce the need for economic and social restrictions from the spring.
5. Until that point, the government must rely on other tools to suppress the virus. The government will build upon the pilots in Liverpool and Merthyr Tydfil with wider community testing, allowing us to identify and isolate people who do not have symptoms but are unintentionally spreading the virus. In addition, the government will roll-out rapid testing nationally to NHS front-line staff, social care and other high-risk or critical settings. This strategy is backed by an additional £7 billion for NHS Test and Trace to increase testing and continue to improve contact tracing, taking the overall funding provided for Test and Trace this financial year to £22 billion.
6. This COVID-19 Winter Plan ensures the current national restrictions can be lifted on 2 December. This is only possible because everyone’s efforts during the current restrictions in England have slowed the spread of the virus and eased the pressure on the NHS. On 2 December, across all of England, regardless of tier:
a. The stay at home requirement will end, with domestic and international travel being permitted again subject to guidance in each tier.
b. Shops, personal care, gyms and the wider leisure sector will reopen.
c. Collective worship, weddings and outdoor sports can resume, subject to social distancing.
d. People will no longer be limited to seeing only one other person in outdoor public spaces - the rule of 6 will now apply as it did in the previous set of tiers.
7. However, the prevalence of the virus is still high and, without taking precautions, it could quickly run out of control before vaccines and large-scale community testing have had an effect. That would jeopardise the progress the country has made and once again risk intolerable pressure on the NHS, squeezing out non-COVID-19 patients from vital treatment.
8. England will therefore move back into the regional, tiered approach because it is right to target the toughest measures only in areas where the virus is most prevalent and where we are seeing sharper increases in the rate of infection. The previous tiered system had an impact on viral transmission but SAGE advised that stronger measures would be needed in some areas to prevent the epidemic from growing. The tiers therefore need to be strengthened to keep the virus under control:
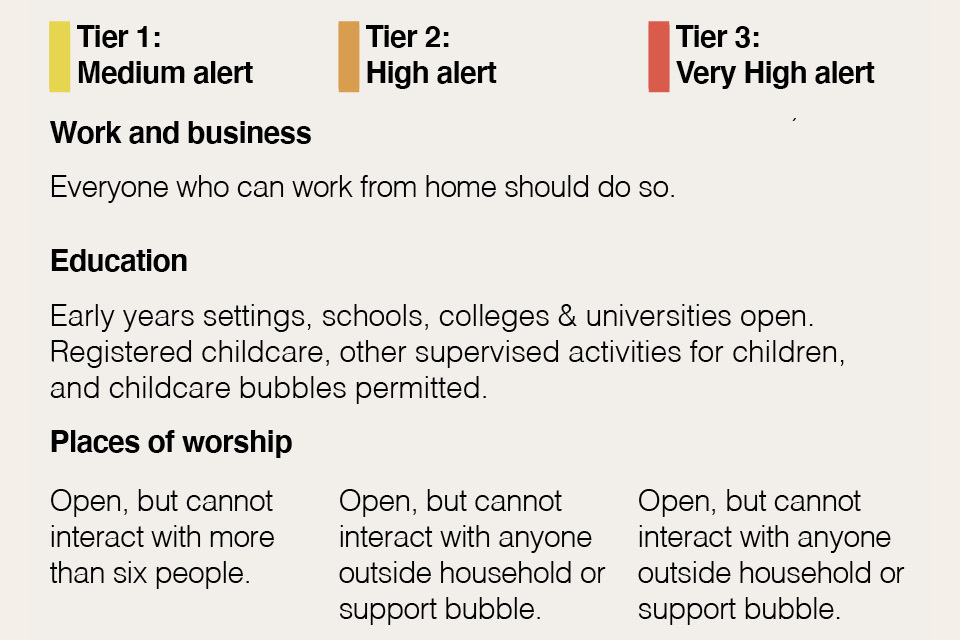
a. In tier 1, the government will reinforce the importance of working from home wherever possible.
b. In tier 2, pubs and bars must close unless they are serving substantial meals (like a full breakfast, main lunchtime or evening meal), along with accompanying drinks.
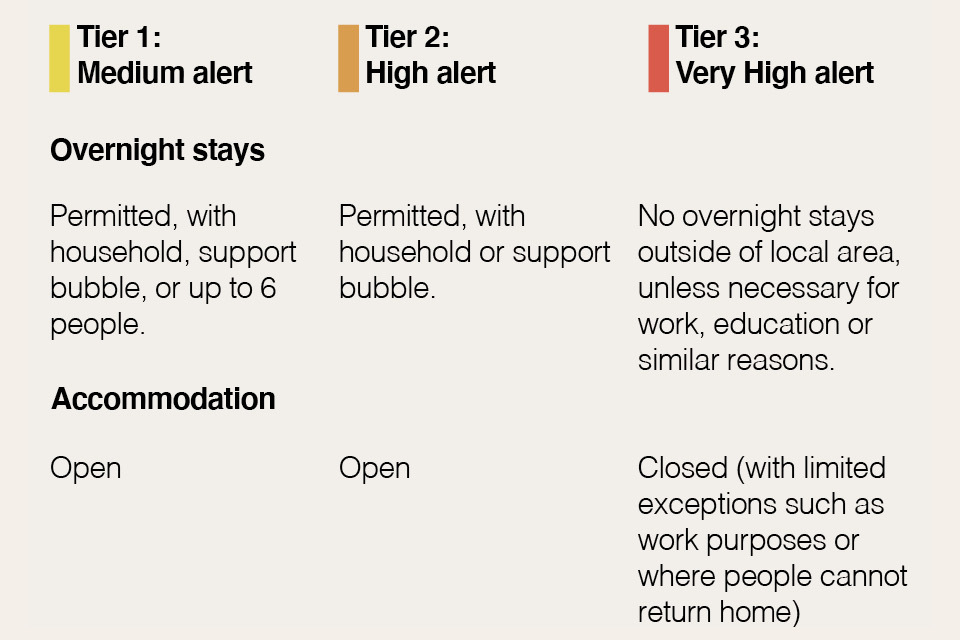
c. In tier 3, all hospitality will close except for delivery, takeaway and drive-through; hotels and other accommodation providers must close (except for specific exemptions, including people staying for work purposes or where they cannot return home); and indoor entertainment venues must also close.
9. These tiers are designed to reduce and keep R below 1 and therefore allow areas to move down the tiers, unlike the previous tiers which mostly slowed the increase, resulting in an epidemic that kept growing. The government is publishing the indicators which will help determine the tier each area will go into on 2 December and how areas move between tiers thereafter. The government will analyse the latest data and announce later this week the tiers each area will enter. Given the need to drive down prevalence further, more areas will go into the higher tiers.
10. The government will also refine the previous tiers:
a. The 10pm closing time for hospitality has been modified to last orders at 10pm and closing time at 11pm. This allows customers to depart gradually and provides greater flexibility.
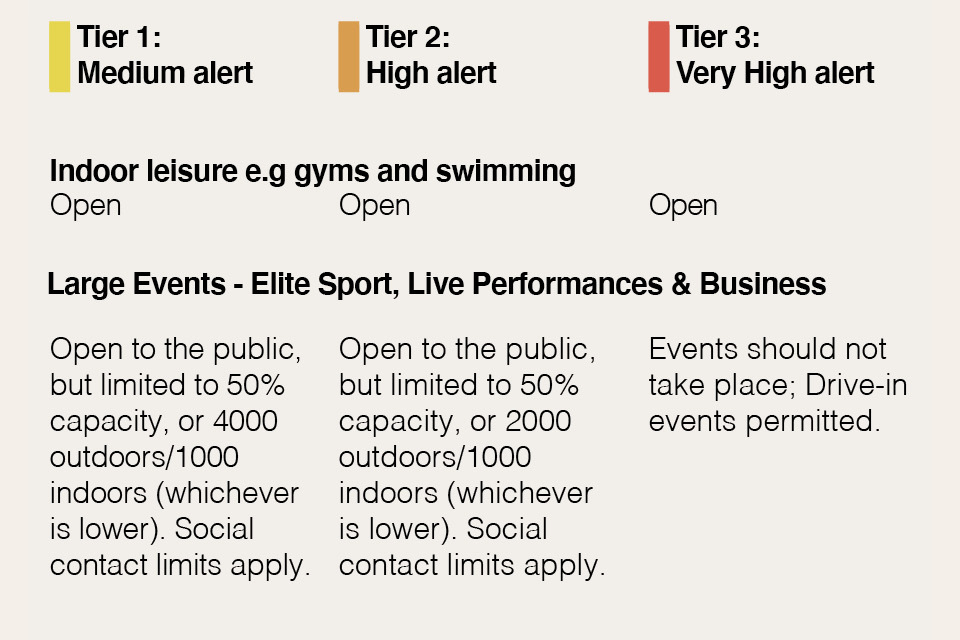
b. In tiers 1 and 2, spectator sport and business events can now resume inside and outside with tight capacity limits and social distancing, providing more consistency with indoor performances in theatres and concert halls.
c. The government is expanding eligibility of ‘support bubbles’[footnote 2]. This will help mitigate the impacts of the restrictions on parents of children aged under 1 (or under 5, but with a disability that necessitates continuous care) and for those households where a single adult cares for someone with a serious disability.
11. By keeping the virus under control through December, the government can enable everyone to see more of their family and friends over Christmas. The government is working to agree with the devolved administrations of Scotland, Wales and Northern Ireland a common approach to Christmas. It will be important to allow families and friends to meet in a careful and limited way, while recognising that this will not be a normal festive period and the risks of transmission remain very real. There is a shared objective to facilitate some limited additional household bubbling for a small number of days. The public will be advised to remain cautious. Wherever possible people should avoid travelling and minimise social contact. Work is continuing to finalise the arrangements, including relating to travel. The UK Government, Scottish Government, Welsh Government and Northern Ireland Executive hope to conclude this work this week, subject to agreement by each administration.
12. While less restrictive than the current national measures, the government recognises how tough these measures are for people and businesses that will be in tier 3, especially those parts of the country which have been under some form of restriction since the summer. The government will offer Local Authorities the opportunity to work together on whole community testing and more targeted testing to high risk settings, in addition to the scaled-up core testing regime. When accompanied by self-isolation of those testing positive, this substantial expansion of testing is a vital new tool to help areas get out of the toughest measures.
13. On 25 November, the government will be announcing the results of the Spending Review, which will set departmental spending plans for 2021-22. This will also provide the details of how departments will be funded for delivering this plan alongside other priorities.
14. In the medium term, as vaccines and community testing yield benefits, the need for restrictions should gradually reduce and life should begin to return closer to normal across the country.
1.1 International context
15. COVID-19 continues to be a global pandemic affecting all parts of the world. After a reduction in cases over the summer, the UK and most of Europe is now experiencing a second wave of the virus. The first wave was brought under control in most European countries in April, but in August, infections began to rise again. Between 18 August and 1 September cases in Spain rose 55%, France 123%, and Italy 161%. At first, many neighbouring countries appeared to keep infection rates low. However, through September and October, the infection began to spread in most European countries. There are now 12 countries in Europe with a weekly case rate over 400 per 100,000 of the population.[footnote 3]
16. Hospitalisations have risen and some health systems are under severe strain, notably France, where 90% of ICU beds are occupied.[footnote 4] In Belgium, the shortage of hospital beds is acute; from 2 November, 60% of beds were reserved for COVID-19 patients.[footnote 5]
17. Deaths across Europe have risen, with average daily COVID-19 related deaths currently at 612 in Italy, 595 in France and 169 in Belgium. However, the general increase in deaths has been far slower than the first wave.[footnote 6]
18. Governments across Europe have responded to that second wave with new, tighter restrictions which aim to suppress the spread of the virus. These restrictions look set to remain in place, and political leaders have suggested many measures will remain in force over the Christmas period.
Figure 1, COVID-19 deaths across Europe Impact of the second wave across European countries. Source: ECDC
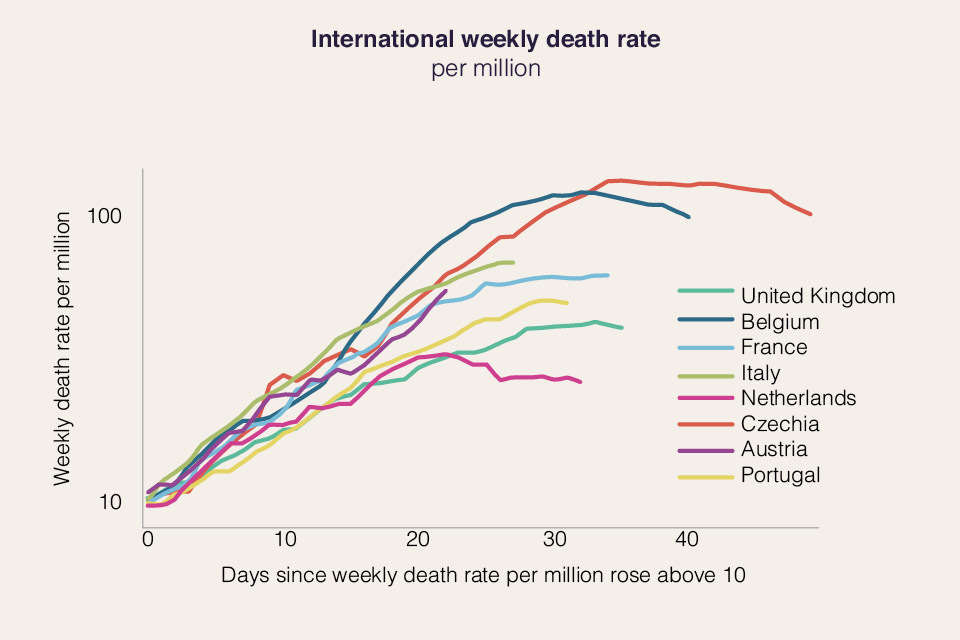
Figure 2 International COVID-19 hospital admissions A graph showing the impact of the second wave across selected international comparators. Source: ECDC.

1.2 The government’s objectives
19. The government’s strategy will be guided by three objectives.
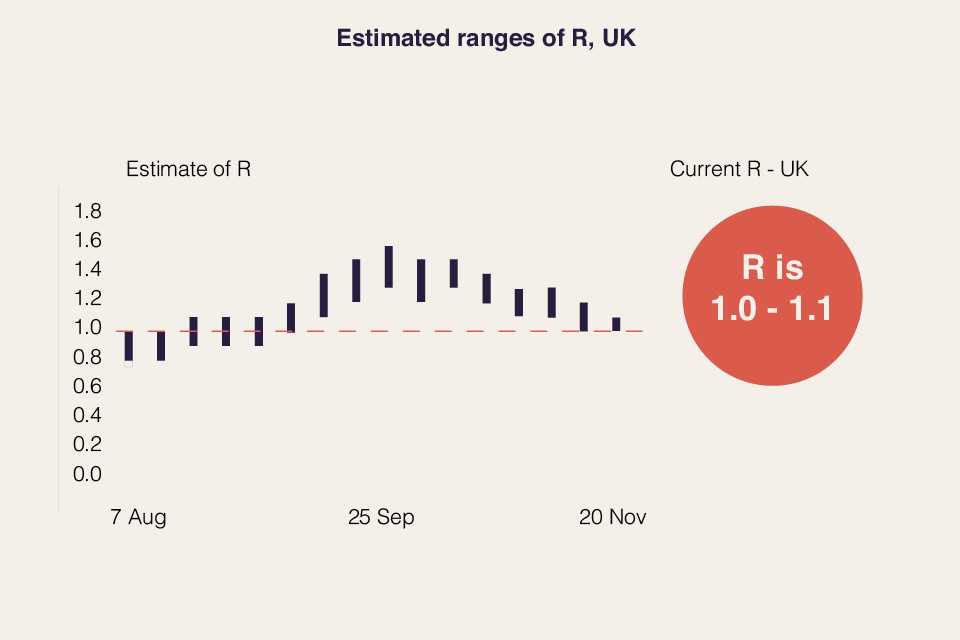
a. Bring R below 1 and keep it there on a sustained basis. R is the epidemiological term for the reproduction number. The R number combined with the growth rate describes how quickly the virus is moving through the population. An R of 3 would suggest that, on average, each infected person would infect three other people. This means that, assuming the infection occurs over a short period of time, the virus is spreading rapidly. Keeping R below 1 means that on average, each infected person will infect fewer than one other person, which will result in the number of new infections falling over time. If no action is taken to suppress the virus, exponential growth will, at some point, exceed regular and surge NHS capacity. As a result, there would be a greater number of direct COVID-19 deaths, and a higher number of indirect COVID-19 deaths due to the impact on healthcare provision.
b. Find new and more effective ways of managing the virus and enabling life to return closer to normal. This will be achieved through: developing and rapidly deploying vaccines; new, improved medical treatments to reduce mortality and morbidity; expanding the capacity of the existing test and trace programme; and using rapid testing to quickly identify and isolate cases.
c. Minimise damage to the economy and society, jobs and livelihoods. Education will be safeguarded in nurseries, schools, colleges and universities. This means ensuring the right support is available for jobs and that early years settings, schools, further education providers and universities continue their excellent work in ensuring a safe environment for students to learn.
2. Route back to normality
20. Over the coming months, the government will be able to rely less on economic and social restrictions and more on solutions provided by scientific progress. This shift will not happen overnight. But recent developments on testing make it possible to reduce cases in the highest prevalence areas alongside the tiers. Together with the prospect of effective vaccines, these advances provide confidence that as we approach spring, life can begin to return closer to normal.
2.1 Vaccines
21. Vaccines that provide durable and effective immunity to COVID-19 will substantially reduce the mortality rate of the virus and may limit its transmission. The deployment of vaccines therefore offers the opportunity to manage the epidemic while gradually lifting many of the restrictions which currently apply.
22. The government is supporting efforts to research and produce an effective, safe and widely available vaccine as early as possible. The government has announced agreements with seven separate vaccine developers. In total, the government has secured access to over 350 million doses between now and the end of 2021. The table below outlines the progress of the different vaccines for which the government has agreements. The government will make vaccines available for all of the UK, plus the Crown Dependencies and Overseas Territories.
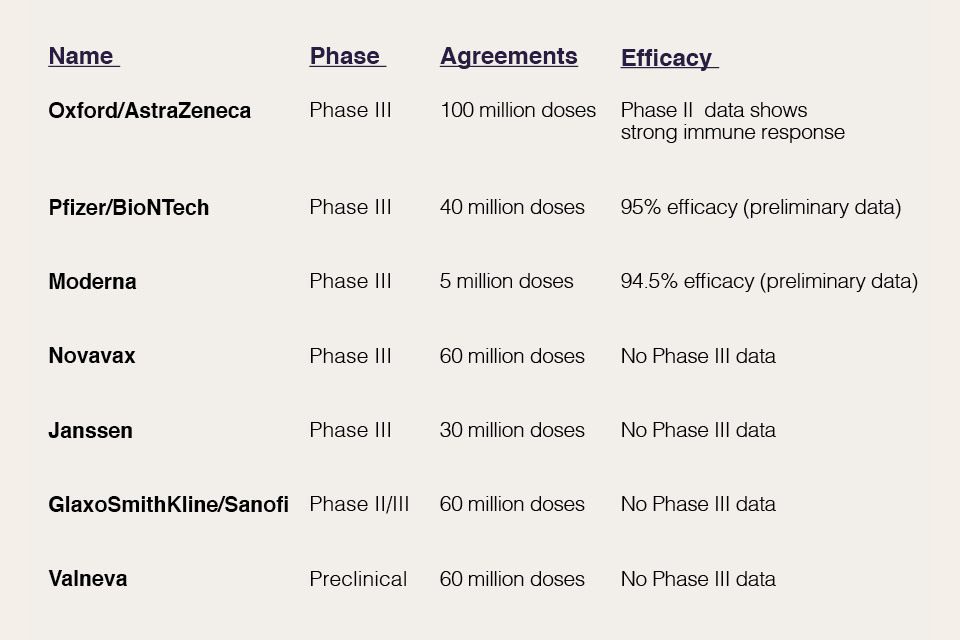
23. There have been positive recent announcements on vaccine development:
a. On 9 November, Pfizer/BioNTech announced interim conclusions of the phase II study of their COVID-19 vaccine candidate, reporting an efficacy of 90%.[footnote 7]
b. On 17 November, Moderna announced the conclusion of the phase III study of their COVID-19 vaccine candidate, with a 94.5% vaccine efficacy.[footnote 8]
c. On 18 November, Pfizer/BioNTech announced the conclusion of the phase III study of their COVID-19 vaccine candidate, with an efficacy of 95% after two doses.[footnote 9] They have formally applied for a license in the United States.
d. On 19 November, Oxford/AstraZeneca announced interim results from the ongoing Phase II/III trial in which strong immune responses were demonstrated across all age groups, and boosted after a second dose.
e. On 20 November, the Secretary of State for Health and Social Care announced that the government has formally asked the MHRA to assess the Pfizer vaccine for its suitability for authorisation.
24. The safety of the public will always come first. A COVID-19 vaccine will only be approved for use if it has met robust standards on safety, effectiveness and quality through clinical trials. The MHRA will apply the key criteria of safety, quality and efficacy before authorising the use of a vaccine. This means that, once the data is submitted, MHRA scientists and clinicians will carefully and scientifically review the safety, quality and effectiveness data, how it protects people from COVID-19 and the level of protection it provides. The data will include:
a. results from the lab and clinical trials in humans
b. manufacturing and quality controls
c. product sampling
d. testing of the final product
e. On 20 November, the Secretary of State for Health and Social Care announced that the government has formally asked the MHRA to assess the Pfizer vaccine for its suitability for authorisation.
25. The Joint Committee on Vaccination and Immunisation (JCVI) is the independent medical and scientific expert body that advises the government on prioritisation for all vaccines. The Committee has been considering COVID-19 vaccine prioritisation for several months and has already provided provisional advice. The purpose of this provisional advice is to support planning for the deployment of any safe and effective vaccines as soon as they are authorised by the MHRA for use across the UK. As with the influenza vaccine, the underlying principles of the advice are to concentrate first on reducing mortality, improving population health by reducing serious disease and protecting the NHS and social care system. It is by achieving these goals that the government can begin to lift the current restrictions safely.
26. It is also important to remember that the exact strength and duration of immunity provided via vaccination is not yet known. Protection by vaccination takes time to build, requires a full course, and it is unknown how well the first vaccines will stop the virus passing between individuals.
27. The JCVI has found that the risk of serious disease and death from COVID-19 increases sharply with age and is also increased in those with a number of underlying health conditions. They have advised that as long as an available vaccine is both safe and effective in older adults, they should be a high priority for vaccination. The Committee’s provisional advice, therefore, largely prioritises vaccination based on age. The provisional JCVI prioritisation has been published, but will continue to be updated.[footnote 10]
28. The JCVI will finalise advice on prioritisation of any vaccine based on consideration of the final phase 3 clinical trial data. The characteristics of the different vaccines are key considerations in the delivery methodology which may necessarily affect prioritisation. As understanding of the clinical characteristics of a vaccine is increased following rollout, the merits and prioritisation of vaccinating lower risk adults throughout the UK will be considered, and the UK’s system of pharmacovigilance will conduct ongoing monitoring of the safety and effectiveness of all vaccines.
29. The urgent work that the NHS is doing will ensure that it will be ready to deploy the vaccine as soon as it is ready and licensed by the MHRA for use in England, Scotland, Wales and Northern Ireland. This work includes having service locations and staff secured, delivery models operational and an active supply chain in place so that when a vaccine does become available, it is set to mobilise. Depending upon their final characteristics, some vaccines may be better suited to differing models of delivery. The NHS delivery programme may need to be adapted from the JCVI priority list to avoid unnecessary wastage.
30. The NHS is in the process of establishing mass vaccination centres across the country that can manage the logistical challenge of needing to store the Pfizer vaccine at minus 70 degrees Celsius. In addition, it is establishing vaccination hubs in hospitals for NHS staff. There will also be a community rollout, which will encompass those who find it difficult to travel.
2.2 Treatment
31. Effective treatments for COVID-19 will continue to be vital to manage the virus even as vaccines are rolled out in the UK and globally, including for those who cannot be vaccinated, for example because they are immunocompromised. Finding effective treatments will reduce risk to lives and serious illness for people who do contract the virus and support the return to normal life.
32. The government is delivering a world-leading programme of clinical trials, including RECOVERY (the world’s largest randomised controlled clinical trial for treatments in the hospitalised setting) and REMAP-CAP, which are testing potential treatments in primary, acute and intensive care respectively. Early indications from the global REMAP-CAP trial this month suggest that tocilizumab may play an important role in improving the outcome of patients in ICU.
33. More results are expected for immunomodulatory drugs, anti-virals, antibiotics, therapeutic antibodies and convalescent plasma for patients in different stages of the illness and various care settings, including hospitals and intensive care, primary care and care home patients.
34. Antibodies are an important component in managing COVID-19 in everyday lives. They can be used therapeutically for infected patients and prophylactically for immunocompromised patients who cannot receive vaccines. The government is supporting efforts to research and produce effective antibody therapies and phase III trials are ongoing.
35. The government will continue to recruit into clinical trials to further global understanding of which therapeutics are effective, and make proven interventions available to the NHS.
36. Patients who have received a positive COVID-19 test may be eligible to participate in a clinical trial: see https://bepartofresearch.nihr.ac.uk for details. The government also urges those who have recovered from COVID-19 to consider donating convalescent plasma to help others. Further details on convalescent plasma.
2.3 Testing
37. Testing capacity for those with COVID-19 symptoms has increased almost five-fold in six months, from 100,000 a day at the end of April to 500,000 a day by the end of October, with plans to go even further by the end of the year. This is available to citizens in every part of the UK. Altogether, over 37 million tests have been conducted, more than any other comparable European country. [footnote 11] The government has opened over 680 test sites, reducing the median distance travelled for a test to 2.6 miles.[footnote 12] Utilising new testing technologies and building new labs will significantly increase the scale of testing, enabling much more testing of key groups such as NHS staff, care homes and social care, as well as creating surge capacity to target cities and regions where needed.
38. The government is working to improve turnaround times for these tests despite the increase in scale and logistical complexity in the expanded network. The government is working with local Directors of Public Health to ensure that Local Authorities play a key role in helping deploy testing in ways that reach people most at risk of having the virus and those working in settings where there is the highest risk of transmission.
39. The increase in testing capacity has been supplemented by work to improve contact tracing. In the last week of reported figures (5 to 11 November) 156,853 people were transferred to the contact tracing system, 85% of those were reached and asked to provide information about their contacts and 78% of those contacts whose details were provided responded to notifications asking them to self-isolate.[footnote 13] Work to improve contact tracing continues, including the roll-out of tracing partnerships with Local Authorities to ensure a greater proportion of people who have tested positive are reached, help provide the support they and their families need to self-isolate successfully and more quickly, and identify and reach any contacts they have had outside their immediate household. In addition, the NHS COVID-19 app has been downloaded 20 million times, and this is supporting the contact tracing effort, including through use of the QR code check-in capability.
40. To date, testing has focused on symptomatic testing, testing in areas with outbreaks and protecting those most at risk, for example in care homes. Those efforts will continue but the use of testing is now being broadened to identify those showing no symptoms who can infect people unknowingly. The government plans to introduce frequent testing as an alternative to the need for self-isolation for people who have had close contact with someone who has COVID-19. Instead, contacts will be offered regular tests as an alternative to isolation and only have to self-isolate if they test positive. This will be trialled in Liverpool first, then some institutional settings (e.g. the NHS, care homes, education, employers) before the end of the year, ahead of rollout across the country from early next year.
41. The government has been working to validate new testing technologies, and there are now three main forms of test in addition to PCR which are available for deployment: lateral flow devices, LAMP (Loop Mediated Isothermal Amplification) and LamPORE. Lateral flow devices are already available at significant scale, and so are the focus of our near-term expansion of rapid testing.
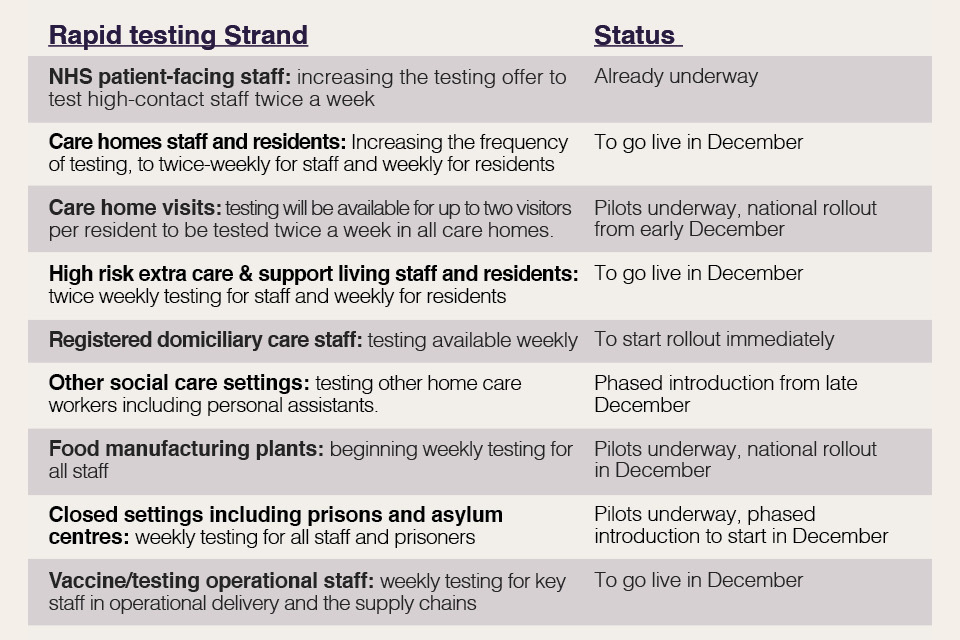
42. The immediate priorities for the expansion in asymptomatic testing are laid out in the table below. They are based on areas where the most vulnerable in society need to be protected and where more positive cases are expected to be found. The government is working to increase capacity further into 2021 and will consider additional strands in due course, as well as looking to enable further delivery of tests in the private sector and in partnership with universities. All of this capability will help the government to target measures to find cases quicker than before and break chains of transmission.
Figure 3, Expansion of testing - status of rapid testing workstreams
43. The government will continue piloting further rapid testing in schools, colleges and universities, and will deploy rapid testing for specific one-off events. This includes testing university students before they travel for Christmas, starting from 30 November, as well as supporting universities to establish sustained testing regimes. Regional testing pilots in Liverpool (over 100,000 people tested at asymptomatic test sites)[footnote 14] and Merthyr Tydfil have trialled offering rapid tests to a wider population and are making a contribution to a fall in positive cases alongside other measures.
44. These pilots have helped the government to develop an offer for a rapid community testing surge. The community testing programme will offer Local Authorities in tier 3 areas the opportunity to participate in a six week testing surge. This will enable Local Authorities to offer tests to the general population as well as targeting high-risk workplaces and industries, hard-to-reach communities and schools in a coordinated effort to drive prevalence down. It will be delivered in partnership with Local Authorities to ensure it is tailored to local circumstances and need. The government is also working with the devolved administrations to coordinate on testing plans and deliver additional testing capability in Scotland, Wales and Northern Ireland.
45. The government will continue, in all tiers, to use early-warning mechanisms like waste-water testing, providing rapid tests for deployment by Directors of Public Health, expanding partnerships on contact tracing and deploying flexible testing sites where outbreaks occur. This should help reduce prevalence further in areas of lower prevalence, enabling a greater range of normal activity to continue.
46. This winter strategy is backed by an additional £7 billion for NHS Test and Trace to support increased testing, including community testing and ongoing improvements to tracing, taking the overall funding provided for Test and Trace this financial year to £22 billion.
47. The government recognises the huge importance and health benefits of visits to people in care homes and their loved ones. The government wants to bring an end to the pain of separation and help care homes bring families and loved ones together in a way that recognises the risks, but enables these to be managed in the best way possible. The launch of visitor testing is a crucial step to making that happen and this approach is currently being piloted in 20 care homes. The government is committed, by Christmas, to providing twice weekly testing to enable all care home residents to have regular visits from up to two visitors. If a visitor has a negative test, is wearing appropriate PPE, and follows other infection control measures, then it will be possible for visitors to have physical contact with their loved one, such as providing personal care, holding hands and hugging. Detailed guidance will be published shortly.
48. It is also important to manage the number of cases seeded from abroad. The government has introduced public health measures at the border including a 14-day isolation period for international arrivals, and introduced the travel corridors system to limit these requirements to those countries with higher prevalence. The government wants to enable people to travel internationally, both for business and leisure, so following extensive work undertaken by the Global Travel Taskforce over the last month, the government will announce next steps shortly. The government will also set out the broader measures recommended by the Taskforce to support the safe recovery of international travel. The government will continue to work with international partners to deliver a shared global understanding of how to integrate a range of measures to support international travel.
3. Controlling the virus
3.1 A targeted approach in England
49. The scientific advances described above provide the route back to normality. But until these have been deployed, the government must continue to use other tools to suppress the virus.
50. As the country emerged from the first wave during the summer, the government sought to target regional growth in infections by taking the necessary measures to contain the virus where it was most prevalent while minimising disruption.
51. In the autumn, the number of cases began to rise. The government responded with a tiered system to simplify and streamline the previous local approach.
52. At the end of October, modelling from NHS England showed that the trajectory of the virus meant the NHS was at risk of exceeding regular and surge capacity in parts of the country within weeks. Under SPI-M’s combined projection, almost 30,000 people were projected to be in hospital across England in early December - close to double the 17,000 beds occupied during the first peak.[footnote 15] In England, the ONS survey indicated that 618,700 - or 1 in 90 - people had COVID-19, with over 50,000 new cases per day.[footnote 16] These numbers were not only high, they were rising. SAGE estimated that R remained above 1 and COVID-19 cases were rising across the country. National intervention was therefore necessary.
Figure 4: COVID 19 hospital inpatients in England. Graph showing the rising number of hospital patients with COVID-19, particularly through October and November. Includes all people in an NHS or independent sector inpatient bed with a positive test for COVID-19. Source

53. The latest results of the ONS infection survey published on 19 November suggest the infection rate has stabilised in recent weeks, and the number of new infections per day fell to 38,900 from 47,700 the week before. Given their enormous economic, social and public health impact, the government believes it is right to end national restrictions on 2 December now the virus is being brought under control. As a result, across the whole of England, the stay at home instruction will end, non-essential shops will reopen, personal care will open, the gym and leisure sector will no longer be closed, outdoor sporting activities will be able to take place once again, people will be able to meet friends and family in outdoor open spaces through the rule of 6, and weddings and collective worship can resume.
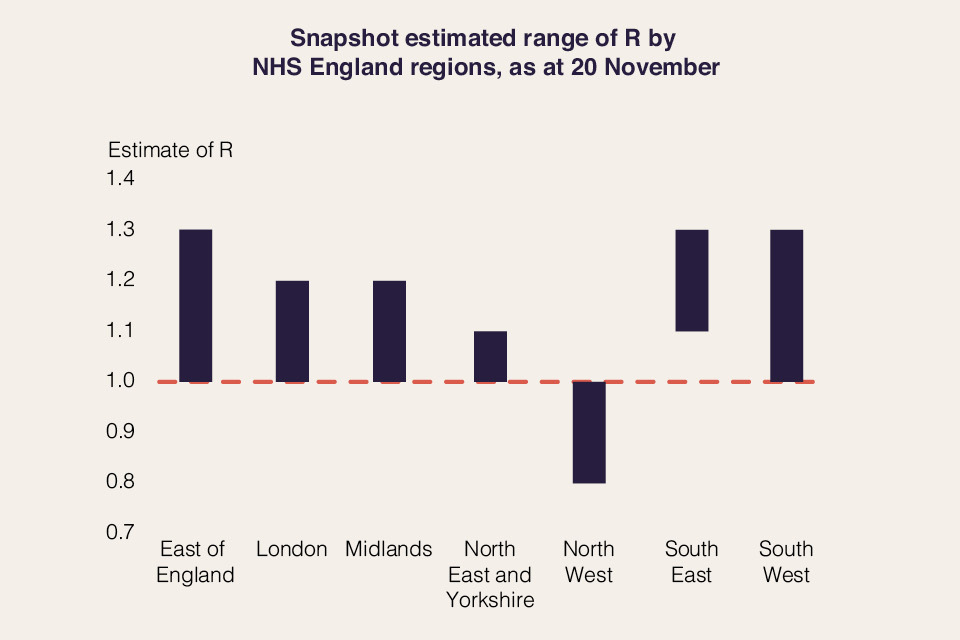
54. The prevalence of the virus will remain high across the country on 2 December, with regional differences. The government must therefore reimpose a tiered regional approach in England to keep suppressing the virus through the winter period. This approach will once again seek to target measures at the appropriate geography and will stop outbreaks at source.
55. The Scientific Pandemic Influenza Modelling group (SPI-M), a subgroup of SAGE, estimates that the initial tier 3 restrictions agreed by local areas may have been associated with a reduction in R between a quarter to a half relative to the impact of tier 1. However it is unclear whether baseline tier 3 restrictions alone would have been sufficient at a regional or national level to reduce R below 1, and some localities may have needed a stronger tier to prevent the epidemic from growing. SPI-M also estimates that moving from tier 1 to tier 2 was associated with a modest reduction in R. These impacts were sufficient to bring R below 1 in some areas, but importantly were not sufficient to stem the continued overall growth across the country.
56. It is vital to learn from the previous tiers and adapt them to ensure they are sufficient to keep R below 1 on a sustained basis – otherwise the virus would again begin to spread rapidly and the country would be faced with the choice of further devastating national restrictions or allowing the NHS to be under greater operational pressure. SAGE met on 12 November and concluded that, to meet the aim of keeping R below 1, “it will be important to consider a range of restrictions that are more stringent than those in the current baseline package of measures in tier 3 for potential use in some areas where tier 3 measures are not able to reduce prevalence.”
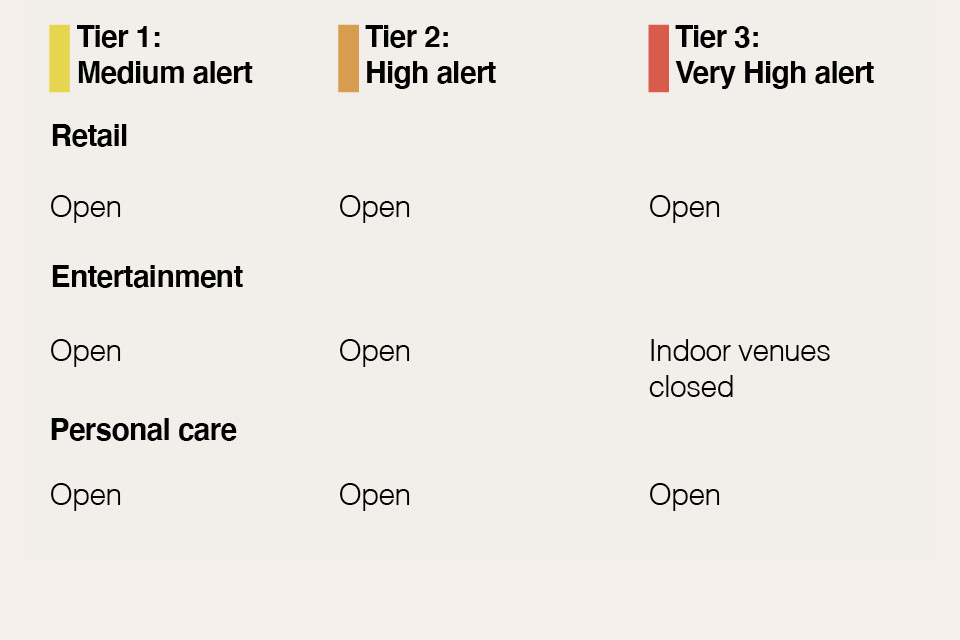
57. Therefore, the government will introduce a new, stronger and more sustainable tiers framework on 2 December. The following table summarises the restrictions that will apply in each tier.


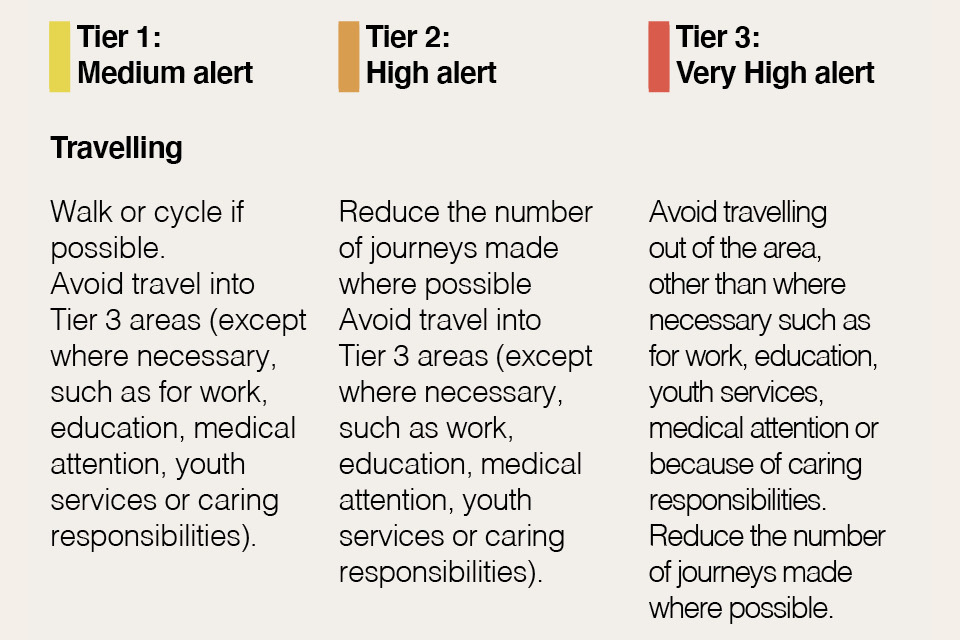


58. The government has learned from the evidence of the impact and implementation of the previous tiers to modify its approach. The government must be confident that the new measures will control transmission, while delivering the minimum possible disruption to society and the economy. These new tiers strike that balance:
a. In order to provide greater clarity and consistency, all tier restrictions will now be standardised rather than negotiated with local areas.
b. For hospitality in tiers 1 and 2, the previous 10pm closing time policy has been modified to 10pm last orders and 11pm closing time, ensuring customers can depart across that period, rather than all at the same time, in order to help with social distancing. In order to strengthen tier 2, venues that serve alcohol can only remain open where they operate as if they were a restaurant, which means serving substantial meals (and accompanying drinks). In tier 3, hospitality will be closed except for takeaway, delivery or drive-through.
c. The evidence suggests that indoor social contact is associated with a far higher degree of transmission risk than outdoor social contact[footnote 17] (with one systematic review finding most transmission clusters occurred indoors).[footnote 18] Therefore, in the very highest tier, indoor group exercise (including sports) will be restricted to people from the same household or bubble, spectators and audiences will not be permitted at sports events or live performances (unless these events are drive-in), business events should not take place, and indoor entertainment venues such as cinemas, theatres, bowling alleys and casinos must close. Elite sport itself will continue to be permitted in all tiers.
d. The government is expanding eligibility of ‘support bubbles’ to help limit transmission while also mitigating the worst impacts of the restrictions on parents of children aged under one (or under five, but with a disability that necessitates continuous care) and for those households where a single adult cares for someone with such a disability.
e. The government will also introduce spectator capacity limits for sports stadia, business events and live performances in tiers where these are permitted. These limits will vary depending on whether the event is held indoors or out. At tier 1 these will be 50% capacity or 4,000 outdoors and 1,000 indoors, whichever is lower and at tier 2 these will be 50% capacity or 2,000 outdoors and 1,000 indoors, whichever is lower.
59. The government recognises these tiers are, overall, more restrictive than those that applied in October. In order to control the virus effectively, it is also likely that more of the country is placed into tiers 2 and 3 at first, as part of the continued effort to suppress infections and protect NHS capacity. This is a necessary step in order to meet the government’s first objective of suppressing the virus and holding R below 1. This is critical because it means the epidemic will shrink rather than grow, allowing areas to move down the tiers as prevalence falls. No one wants these tough restrictions, which damage lives and businesses, in place for any longer than necessary. The government will review the tiering allocations every 14 days. However, as prevalence remains high it is likely that it will be longer before many places move down tiers. The tiering regulations will lapse at the end of March, at which point the government would need to return to Parliament with any proposals for further economic and social restrictions.
60. It is important that the latest data is used to inform decision making, including the impact of current measures, so the government will announce later this week which tier will apply in each area from 2 December, based on analysis of the most up-to-date information. Decisions will primarily be based on five key indicators:
a. Case detection rates in all age groups
b. Case detection rates in the over 60s
c. The rate at which cases are rising or falling
d. Positivity rate (the number of positive cases detected as a percentage of tests taken)
e. Pressure on the NHS, including current and projected occupancy
61. The government will need to maintain some flexibility to weight these indicators against each other as the context demands. For example, hospital capacity in a given area will need to be considered in the light of the capacity in neighbouring areas and the feasibility of moving patients. Case detection rates will need to be weighted against whether the spread of the virus appears to be localised to particular communities. Given these sensitivities, it is not possible to set rigid thresholds for these indicators, as doing so would result in poorer quality decisions. The government will, however, be transparent about the decisions that it takes and make available the evidence informing those decisions. The movement of areas up and down tiers will also be informed by broader economic and practical considerations, such as the anticipated movement of individuals between areas.
3.2 Behaviours and compliance
62. The government has asked the public to adopt a range of behaviours that limit the spread of the virus. These behaviours include wearing face coverings in enclosed environments, maintaining social distancing, and self-isolating when infection is suspected or confirmed. The normalisation of these behaviours has had an undoubted impact on reducing the spread of the virus, even where they may cause economic hardship and social sacrifice. Continued adherence to these behaviours will remain just as critical through the winter.
Figure 6, maintaining the right behaviours. The most important way to suppress the virus is if we all continue to follow the right behaviours.
63. Working from home can reduce transmission. Between 24 April and 3 May, 36% of employees were working exclusively from home.[footnote 19] These numbers declined as expected over the summer. However, since the government renewed its Work From Home guidance in late September and through the period of the November national restrictions, the numbers working from home have remained relatively low compared to earlier in the year.[footnote 20] SAGE advice is that typically over one third of contacts are made at work, that these are often of long duration and highly clustered and that homeworking can have a significant effect on reducing transmission if all those who can work from home do so.[footnote 21] The government encourages employers to enable a greater degree of home working, and will strengthen guidance to be very clear that anyone who can work from home should do so. The government recognises that there are specific reasons why attendance in the workplace may be needed, including mental health issues or concerns; and / or a need to work on-site physically. In industries and sectors where working from home is not possible, including, for example, in much of the construction and manufacturing sectors, and where people’s jobs necessitate working in other people’s homes, businesses have taken clear steps to protect the health and safety of staff and customers through following government guidance, making their workplaces COVID-secure, enabling staff to observe hands, face, space and adopting behaviours that will reduce transmission. In circumstances such as these, people should continue going to work.
64. The vast majority of businesses are operating within the rules and have gone to enormous lengths to ensure they are COVID-secure. However, a small number of businesses are not complying with the law and operating in an unsafe way. This puts progress in controlling the virus in jeopardy, and risks further restrictions being imposed on compliant businesses to make up for the reckless approach of a minority. Local Authorities have said to the government that current powers are inadequate and do not allow them to enforce the law.
65. The government will therefore legislate to enhance the tools available to Local Authorities. Local Authorities will be given streamlined powers to issue improvement and restriction notices to businesses that are breaching COVID-secure rules, with the ability to compel the immediate closure of a premise that is not complying with COVID-Secure regulations. These new powers will enable upper and lower tier Local Authorities to take swift and effective action against those premises that are posing a risk to public health. Businesses will also face financial penalties for not meeting the requirements of an improvement or restriction notice issued by a Local Authority. The government is clear that these powers should only be used where necessary and proportionate to do so, and by trained local authority enforcement officers. Local Authorities will continue the approach they have taken to date; engaging, educating and encouraging premises to comply, and only taking enforcement action to address the most pressing public health risks.
66. The Contain Outbreak Management Fund will be extended so that it can provide monthly payments to Local Authorities facing higher restrictions until the end of the financial year. For those authorities under the highest level of restrictions, this funding will amount to £4 per head of population per month. This funding will be made available from the end of national restrictions, and will be subject to review in January 2021. Further details will be provided to Local Authorities before the end of national restrictions on 2 December. This further funding, worth up to £900 million, recognises the ongoing public health and outbreak management costs to Local Authorities of tackling COVID-19. It will be in addition to the more than £780 million that has been committed to Local Authorities from the Contain Outbreak Management Fund to date.
67. Promoting the right behaviours will continue to be crucial as the government seeks to reopen the economy and use measures such as rapid testing and vaccines. The government will continue UK-wide campaigns across England, Scotland, Wales and Northern Ireland such as Hands, Face, Space to help people understand how to keep themselves and their communities safe. The government is also examining additional support options to increase adherence to behaviours that are particularly difficult for those in challenging circumstances, such as self-isolation for those who cannot work from home. Where there are flagrant breaches of the rules, the government will hold those responsible to account, enforcing through fines and other measures.
3.3 Christmas and beyond
68. COVID-19 continues to pose a very real threat to the UK. This means that it will not be possible to celebrate Christmas in the “normal way”.
69. However, the government recognises that Christmas is an important time of year for many people, all across the UK. Regardless of faith, the Christmas period is a time often spent with family and friends, with schools and offices closing and people travelling over the bank holidays. The fact that this has been a difficult year for everyone means that time with loved ones will be even more important. For this reason the government is considering carefully how to balance the increased risk of transmission while allowing some increased social contact for everyone, supported by guidance on how to celebrate safely, over the Christmas period.
70. The government and the devolved administrations are working together to design a time-limited change to social restrictions over the Christmas period. This will not be risk-free. Meeting up with other households will increase the risk of catching COVID-19 and passing it on to others. Even where it is within the rules, meeting with friends and family over Christmas will be a personal judgement for individuals to take, mindful of the risks to themselves and others, particularly those who are vulnerable.
71. Ministers have endorsed a shared objective of facilitating some limited additional household bubbling for a small number of days, but also emphasised that the public will be advised to remain cautious, and that wherever possible people should avoid travelling and minimise social contact. Work is continuing to finalise the arrangements, including relating to travel. The UK Government, Scottish Government, Welsh Government and Northern Ireland Executive hope to conclude this work this week, subject to agreement by each administration.
72. The government also recognises the significant sacrifices that people of all faiths have made this year; restrictions have been in place over a number of religious celebrations and observances, and it is thanks to these sacrifices that it has been possible to control the virus. Communal worship will be possible for all faiths in all three tiers and faith leaders continue to play a key role, consulting on how to make religious practice as safe as possible.
73. Nurseries, schools and colleges should not change their Christmas holidays or close early this term. Parents should continue to send their children to school during term time and students should continue to attend college right up until the end of term – our senior clinicians continue to advise that the best place for children and young people is in education. A time-limited change to social restrictions over Christmas does not require any children to be taken out of school prematurely. The leaders and staff of education settings have been doing an extraordinary job to remain open, keep settings safe and provide education.
74. It will be particularly important to be cautious early in the new year. Christmas will likely lead to an increase in transmission and, historically, the period after Christmas is when the NHS sees the greatest pressure on services such as Accident & Emergency and the highest rates of bed occupancy. During the busiest week of winter, hospital bed occupancy often goes above 95% in many Trusts. Hospitals take steps to manage this demand by opening surge capacity, and if necessary, postponing planned surgery. This year, the NHS is dealing with COVID-19 in addition to these usual winter pressures. The government urges caution before, during and after Christmas - particularly for those travelling.
4. Protecting the NHS and the vulnerable
4.1 Protecting the vulnerable
75. Under recent national measures, the clinically extremely vulnerable have been advised to take extra precautions and stay at home as much as possible. Local Authorities have been working to ensure the right support is available for those that need it.
76. As the national restrictions end, the guidance to the clinically extremely vulnerable not to go to work or school will also end. The government will reintroduce the specific advice for clinically extremely vulnerable people on how they can protect themselves at each tier. The government will constantly monitor the latest evidence and the evolving situation in local areas to keep the advice for clinically extremely vulnerable people up to date. Support will be available for those who need it, either through Local Authorities in tier 3 areas or NHS Volunteer Responders. Supermarket priority delivery slots will also continue for those who have already registered. The government has also made free influenza vaccinations available to the household contacts of those on the Shielded Patients List.
77. A better understanding of the factors contributing to clinical risk has informed the clinical advice from Medical Officers that most children can be removed from the Shielded Patient List, following a clinician-parent conversation. It has also led to the addition of those with Chronic Kidney Disease Stage 5 and of adults with Down’s Syndrome to the Shielded Patients List, ensuring that they are provided with the best advice on protecting themselves.
4.2 Social care
78. In September, the government published an Adult Social Care Winter Plan, which set out measures to prevent and contain the virus, including increasing the Infection Prevention Control funding. To date, £1.1 billion has been provided to implement infection prevention and control measures. This is in addition to the £4.6 billion that has been made available to Local Authorities in England to address pressures on local services caused by the pandemic, including adult social care.[footnote 22]
79. In the first wave, the movement between care homes of staff who were unwitting carriers was one cause of the virus being introduced to these settings. The government is therefore introducing legislation, by the end of the year, that requires care home providers to restrict all but essential movement of staff between settings in order to reduce transmission.
80. To further prevent the risk of infections entering care homes, the government is working with the Care Quality Commission (CQC) and the NHS to ensure everyone discharged to a care home has an up-to-date COVID-19 test result, and anyone testing positive will be discharged to a setting that has been assured by the CQC specifically for the purposes of providing safe care for COVID-19 positive residents.
81. In addition, the influenza vaccine is being made available, free of charge, to all care staff, personal assistants and unpaid carers to further protect staff over the winter period.
82. Care homes registered with the PPE Portal are able to access all of their COVID-19 PPE requirements this way and 83% of eligible care homes are now registered, with registrations still increasing weekly. Over 41,000 providers have registered for this portal across primary and social care. Personal assistants, supported living, shared lives and day care services can obtain free PPE from their Local Authority or Local Resilience Forum for COVID-19 needs. The government continues to review PPE usage in order to match supply to demand.
83. Repeat testing was introduced across care homes in July which helps care homes to identify and contain outbreaks. All care home staff are now offered weekly testing and this will be increased to twice weekly by the end of December. Resident testing started in April and all care home residents have been offered monthly testing since July. This will be increased to weekly testing in December.
84. The government recognises it is important to protect those receiving care in their own home, and while the risks are lower than for those in communal residences, many of those receiving care at home are vulnerable to COVID-19. The Government is therefore providing weekly testing to domiciliary carers working for CQC registered domiciliary care providers across England, using PCR tests initially from 23 November and moving to lateral flow testing once clinically validated for self testing.
85. The government has also launched the Adult Social Care COVID-19 Dashboard to help Local Authorities monitor outbreaks and infection prevention measures.
4.3 Disproportionately impacted groups
86. The government is determined to address the disproportionate direct and indirect impact of COVID-19 on individuals who may be most at risk from COVID-19 infection, hospitalisation and mortality. Individuals who are elderly, disabled and / or from ethnic minority backgrounds have been disproportionately impacted by COVID-19. The government is improving data to help build a clearer picture of how COVID-19 affects different groups of people with specific characteristics. Research to date has shown that a range of socioeconomic and geographical factors - such as occupational exposure, population density, household composition, and pre-existing health conditions - contribute to the higher infection and mortality rates for ethnic minority groups.
87. The government will continue to provide better data, clearer guidance, and a toolkit to help businesses protect individuals at higher risk, in part due to their occupation, when they are in the workplace. The government is continuously working to improve the data to help build a clearer picture of how COVID-19 affects people with specific characteristics. The government is spending up to £25 million to establish a network of Community Champions to help those most at risk and hard-to-reach communities access and adhere to the latest government COVID-19 guidance, and to give these people a greater voice in public health.[footnote 23] The scheme will also provide funding for voluntary and community groups who specialise in working with communities most at risk from COVID-19. The government is also considering what further action is needed to protect disabled people. It is especially important that the needs of people with characteristics that could put them at greater risk are fully considered and that the fullest efforts are made to engage them in the roll-out of rapid testing and vaccines.
4.4 NHS capacity
88. The response of the NHS in this crisis has shown the service at its best. Recognising the work of all the brave and resilient staff, the government has made clear its commitment to support the NHS as it responds to the virus. This support is not just to assist in efforts to treat those afflicted by COVID-19; it is to preserve the essential and necessary functions of the healthcare system for all those who need it.
89. In July, the government announced up to £3 billion of additional funding to support the NHS in preparation for the winter. This is in addition to the £450 million the government has already invested to make sure A&E departments are ready for winter. This included maintaining the Nightingale hospital sites and access to the independent sector capacity, together with expanding eligibility for free influenza vaccinations and the NHS’s enhanced discharge policy.
90. The NHS has increased staff numbers by 70,000 since last year and has plans in place to allow for local peaks in COVID-19 patients to be safely managed. This involves reallocating staff temporarily to areas of high demand, increasing productive clinical time and minimising absences (for example, through staff influenza vaccinations and a focus on wellbeing). The NHS is continuing to recruit, making use of the returning NHS staff who volunteered their services in the spring. Over 12,000 of these individuals remain in contact with the NHS and while the expectation is that the bulk of them will be deployed to support projects such as the rollout of a COVID-19 vaccine, thousands are already working in the NHS.
91. Initiatives have been put in place to make use of existing capacity across the NHS, such as NHS 111 to provide more effective triaging, and accelerated discharge to support patients to leave hospital safely and more quickly. The government is also increasing eligibility for free influenza vaccinations to all 50 to 64 year olds from December. Vaccinating this cohort, in addition to those groups who are already eligible to receive the influenza vaccine free of charge, will reduce pressure on the NHS during the winter months as well as provide additional protection to a group of people who are vulnerable to COVID-19. The expanded cohort will receive their free influenza vaccines from 1 December.
92. By December, it will be possible to meet 70% of the expected winter demand for PPE from UK manufacturing and, although gloves are not currently produced in the UK, the government is confident in supply. Almost 32 billion items of PPE have been ordered, of which over half are already in the UK. This month stockpiles will be in place for all COVID-critical PPE, sufficient to cover 120 days usage at COVID-19 levels.[footnote 24]
93. NHS staff have worked to maintain non-COVID-19 health provision throughout the pandemic, and even at the peak of the first wave, there were over twice as many people in NHS acute inpatient beds without COVID-19 as there were with COVID-19. Thanks to the efforts of staff across the country there are now over five times as many patients in NHS acute beds without COVID-19 as there are with COVID-19. The “Help Us, Help You - Accessing NHS services” campaign launched on 9 October, and urges the public to continue seeking care when they need it. In September, there were nearly 27 million GP appointments, an increase of 20% compared to the previous month, and 700,000 more than last year. Since the first wave receded, the NHS has worked to restore non-COVID-19 activity and even during the second wave, most trusts have continued to deliver electives, including non-urgent electives. The latest figures show that hospitals are carrying out more than a million routine appointments and operations per week.
94. The government is providing an additional £205 million of support for the NHS this winter. This includes an additional £80 million to bring forward the recruitment of staff. The government will also invest up to £125 million to secure additional hospice capacity. The government has also announced an additional £1 billion for the NHS next year to begin tackling the elective backlog, including continuing to prioritise the most urgent patients and enabling catch-up for long waiters, and around £500 million to address the mental health backlog, give more people the mental health support they need, and invest in the NHS workforce.
95. More broadly, the government is committed to supporting everyone’s wellbeing and mental health throughout the winter period to help people through this difficult time. The Wellbeing and Mental Health Support Plan for COVID-19, which will be published by the Department for Health and Social Care, will outline the government’s plan to strengthen the mental health and wellbeing support and services available to those who need them.
5. Keeping education and the economy going
5.1 Business support and minimising economic impact
96. The impact on the economy and individuals’ livelihoods has been severe, despite the government’s actions. Output fell around 25% between February and April, reversing 18 years of economic growth in just two months, before starting to pick back up from May as the economy reopened. While GDP grew by 15.5% in Q3 2020 as restrictions on movement eased, GDP in September remained 8.2% below the levels seen in February 2020.[footnote 25]
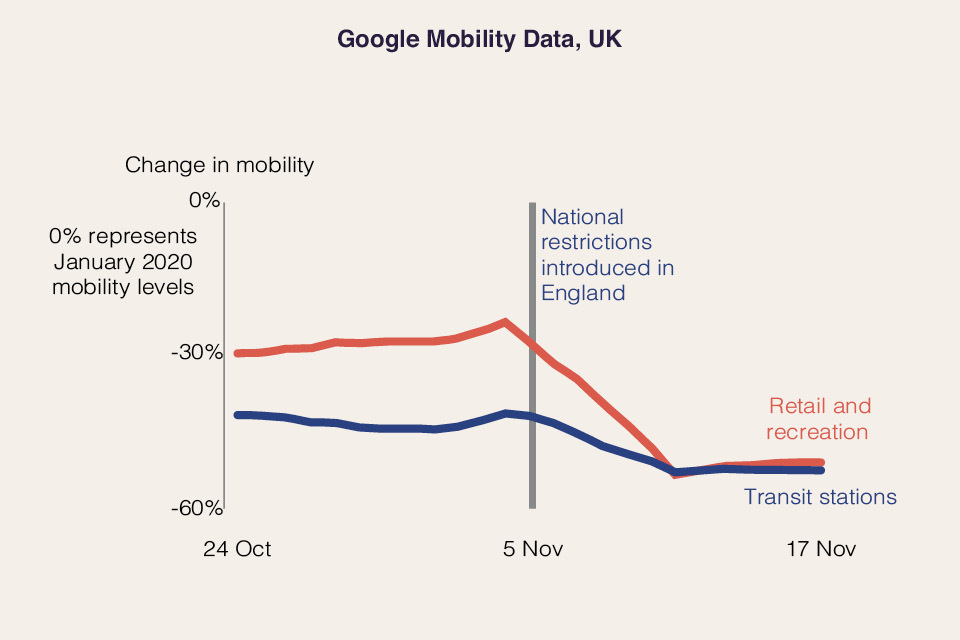
97. Since March 2020, the number of payroll employees has fallen by 782,000.[footnote 26] The impact will have been felt hardest by those who work in the hospitality, entertainment, retail sectors, and related industries. Timely measures of activity, such as mobility, have shown falls in England across November.[footnote 27] The latest consensus of independent forecasts published by HM Treasury in November also suggests that the economy will contract again in Q4.[footnote 28] The Office for Budget Responsibility (OBR) will publish their overall economic and fiscal forecast on 25 November.
98. The government has moved swiftly to support the economy and protect jobs across the four nations of the UK with the Coronavirus Job Retention Scheme, Self-Employment Income Support Scheme as well as a number of support schemes for businesses.[footnote 29] More than £65 billion has been provided in government-backed loans for businesses. Support schemes introduced include:
a. Coronavirus Job Retention Scheme (CJRS): CJRS has been extended until the end of March 2021 for all parts of the UK, with employees receiving 80% of their usual salary for hours not worked, up to a maximum of £2,500 per month. As of 18 October, 9.6 million jobs have been supported by the CJRS.[footnote 30]
b. Self-Employment Income Support Scheme (SEISS): SEISS is in place until April 2021. The scheme is currently in its third stage and will offer grants to the self-employed at 80% of average trading profits for November to January, capped at £7,500 in total.
c. Access to Finance schemes: Under the Coronavirus Business Interruption Loan Scheme (CBILS) and the Coronavirus Large Business Interruption Loan Scheme (CLBILS), the government provides lenders with an 80% guarantee to enable them to support viable small and medium sized enterprises (SMEs) and larger businesses respectively. Under the Bounce Back Loans Scheme (BBLS), the government provides lenders with a 100% guarantee to enable them to provide loans between £2,000 and £50,000 to small and medium-sized businesses with a simple, streamlined application process. All three government-backed loan schemes are open until the end of January 2021.
d. Local Restrictions Support Grants: Businesses in England that are forced to close will receive up to £3,000 for each 28 day period. Where businesses have not been required to close but have been severely affected by restrictions in tier 2 or tier 3 areas, Local Authorities will receive funding that will enable them to make grants worth up to £2,100 for each 28 day period.
e. Business Rates holiday: All eligible businesses in the retail, hospitality and leisure sectors will pay no business rates in England for 12 months from 1 April 2020, and nurseries in England will also receive a one-year holiday.
f. Increased funding for the welfare system through a £20 per week increase to the Universal Credit standard allowance and Working Tax Credit basic element for 2020-21, and an increase in the Local Housing Allowance rates for Universal Credit and Housing Benefit claimants. These changes are collectively worth over £7 billion this year.
g. Reduced VAT rate for hospitality and tourism: The government is extending the reduced VAT rate of 5% for eligible businesses in the hospitality and tourism sectors until 31 March 2021.
h. Devolved administration funding: The government is guaranteeing at least £16 billion in funding this year to the devolved administrations on top of their spring Budget 2020 funding: Scottish Government - £8.2 billion, Welsh Government - £5.0 billion and Northern Ireland Executive - £2.8 billion.
i. Funding for cultural organisations, charities and spectator sports via the £1.57 billion Culture Recovery Fund; a £750 million package of support for charities; and a £300 million Sport Winter Survival Package.
99. Overall, the government has acted with speed to protect lives and safeguard jobs with an unprecedented £200 billion. The impact on livelihoods cannot be underestimated, and these response measures have been necessary to help support individuals and businesses through this challenging period.
5.2 Protecting education
100. Since the summer, the government’s priority has been to ensure that education remains open. The policy in England is that education settings will remain open in all tiers. Children’s life chances, as well as the long-term health of the economy, depend upon students continuing to learn and develop vital skills, and adults being able to train and retrain to meet the changing needs of industry and the economy. Educational settings have remained open during the November national restrictions and the government has committed to delivering a full set of exams in England next summer. Thanks to the enormous effort by early years practitioners, teachers, lecturers and support staff who have worked so hard to implement protective measures, 99% of schools have been open throughout the term so far, with millions of children and young people benefitting from attending early years settings, school and college throughout the term.[footnote 31] The Department for Education will update its guidance in the coming days to reflect how settings should operate under the strengthened tier system, and an updated contingency framework in the exceptional circumstances in which further restrictions on education are required in any area. The government will do everything possible to avoid enacting those contingency measures at any stage.
101. The government has also ensured that schools and colleges have access to COVID-19 tests, with every school provided with an allocation of tests for those staff and students that are not able to access testing via other routes. The government will continue piloting further rapid testing in schools.
102. When it is necessary for children to isolate, schools have a duty to provide high quality remote education; a Direction which places an express legal duty on schools to provide remote education in these circumstances has been in effect since October. The Oak National Academy launched in April 2020 to provide online lessons and curriculum resources to schools and pupils. The pace and scale of the Department for Education’s Get Help with Technology programme is unprecedented. The department purchased over 340,000 laptops this term alone to support disadvantaged children.[footnote 32] By Christmas, this will amount to an increase of over half a million since the pandemic hit. This is part of over £195 million invested to support remote education and access to online social care, which includes 220,000 laptops and tablets and over 50,000 4G wireless routers already delivered to children over the summer term. At the peak, 27,000 laptops were delivered in a single day.
103. To support children and young people to catch up, the government has provided £1 billion of ‘catch up’ funding, including providing catch up premium funding direct to schools, as well as launching the National Tutoring Programme. This will ensure all schools have the support they need to help all pupils make up for lost teaching time. Catch up funding can be used to improve the language skills of reception age children who have missed out on early education at a crucial time for their development as a result of the pandemic. The Hungry Little Minds campaign has provided support and ideas about home learning to parents of preschool age children.
104. Registered early years childcare providers were one of the first sectors to have restrictions lifted in the summer, in recognition of the key role they play in society. Childminders and nursery staff across the country have worked hard to keep settings open through the pandemic so that children can be educated, and parents can work.
105. Further Education providers and training and assessment organisations have worked tirelessly to remain open for on-site face-to-face provision, and to successfully increase the effectiveness of remote provision, giving young people and adults the opportunity to master the practical and academic skills that are crucial to their careers and the UK’s economic recovery.
106. The government has funded all apprentices who have been made redundant and who are at least 75% of their way through to complete their apprenticeship. This has allowed apprentices that are close to the end of their apprenticeship to continue on their programme, putting them in a stronger position to secure new employment once they have completed their apprenticeship.
107. The government has supported providers to ensure that they can deliver effective remote provision through peer-to-peer advice and training through the EdTech Demonstrator programme, and the Department for Education has funded digital curriculum content and resources from organisations such as Jisc and World Skills UK. 108. The government has also provided £96 million to support small group tuition for students aged 16 to 19 in English, maths, and other courses where learning has been disrupted by COVID-19, including vocational courses where assessment has been deferred because of national restrictions.
108. The government has also provided £96 million to support small group tuition for students aged 16 to 19 in English, maths, and other courses where learning has been disrupted by COVID-19, including vocational courses where assessment has been deferred because of national restrictions.
5.3 Universities
109. Universities have worked hard to make campuses as safe as possible and provide blended learning to enable students to return to campuses and engage in face to face learning. All universities developed plans for managing and controlling outbreaks and there has been close working between public health experts and universities, who have successfully managed and controlled outbreaks to reduce risks for students, staff and the communities in which they live.
110. The government has established walk-through sites and deployed mobile units so that almost all universities are within 1.5 miles of a testing centre, allowing staff and students to get access to tests should they develop symptoms.[footnote 33] Every university in England has now been offered access to rapid asymptomatic testing. The government is supporting universities in rolling this out based on a range of factors including local prevalence rates, whether testing is available already, and the percentage of high-risk students in each institution.
111. The government has worked with the devolved administrations to ensure that all students, no matter where they live or study, are treated fairly and can travel home as safely as possible. From 3 December to 9 December, known as the ‘student travel window’, students will be allowed to travel home on staggered departure dates set by universities. Reduced social contact due to the period of national restrictions that students will have undergone will make this safer. Tests will be offered to as many students as possible before they travel home for Christmas, targeted using a range of factors including local prevalence rates, whether testing is available already, and the percentage of high-risk students in each institution. 108 higher education institutions have signed up for the government rapid testing programme, covering the majority of students expected to travel home for Christmas. This will provide further reassurance that where students test negative, and self-isolate if they test positive, they can return home safely and minimise the risk of passing COVID-19 on to their loved ones. Once at home, in terms of the social contact rules, they and the family members they live with, will be treated as being part of the same household.
112. Following the end of term break, the government is looking to make the return to higher education as safe as possible, and will provide further guidance in due course, considering future developments and the relevant scientific advice.
6. Annex: data and evidence







7. Annex sources
-
Source: Office for National Statistics - Coronavirus (COVID-19) Infection Survey *These estimates refer to infections reported in the community in private households. These estimates exclude infections reported in hospitals, care homes or other institutional settings.
-
Source: Office for National Statistics - Coronavirus (COVID-19) Infection Survey *These statistics refer to infections reported in the community, by which we mean private households. These figures exclude infections reported in hospitals, care homes or other institutional settings. After 11 November, estimates have more uncertainty as we are expecting further swab test results for these dates.
-
Source: Office for National Statistics - Coronavirus (COVID-19) Infection Survey *These statistics refer to infections reported in the community, by which we mean private households. These figures exclude infections reported in hospitals, care homes or other institutional settings. After 11 November, estimates have more uncertainty as we are expecting further swab test results for these dates.
-
*Data for Wales includes confirmed and suspected COVID-19 patients in acute hospitals only. Data for Scotland up to 16 November. Definitions vary across the devolved administrations. See statistical notes for more information.
Source: https://coronavirus.data.gov.uk/. Further details on data sources -
Data for Scotland and Wales up to 19 November. Data for Northern Ireland up to 18 November. See statistical notes for more information. Source: https://coronavirus.data.gov.uk/.
Further details on data sources -
Data for Northern Ireland, Scotland and Wales up to 19 November. See statistical notes for more information. Source: https://coronavirus.data.gov.uk/. Further details on data sources
-
Source: https://coronavirus.data.gov.uk/. Further details on data sources
-
Source: Office for National Statistics deaths registered weekly in England and Wales
Further details on data sources -
Source: Opinions and Lifestyle Survey, Office for National Statistics.
*Working from home includes those solely working from home, and those who both travel to work and work from home. Further details on data sources -
Source: Google LLC “Google COVID-19 Community Mobility Reports”. Accessed: 20/11/2020. Further details on data sources
-
Support Bubble: A support bubble is an exclusive close support network between two households. It means you can have close contact with that household as if they were members of your own. From 2 December, you can form a support bubble with another household, if at least one has: only one adult; (including a household where any children are under the age of 18); only one adult carer (i.e. living with any additional adult(s) in the household that have a disability and require continuous care); a child under 1 (regardless of how many other adults are in the household) ; or a child under 5 with a disability that requires continuous care (regardless of how many other adults are in the household) Childcare Bubble: A childcare bubble is where one household links exclusively with one other household to provide informal childcare to a child or children aged 13 or under. They can provide the childcare in either or both of the homes from the 2 households. ↩
-
https://www.data.gouv.fr/fr/datasets/donnees-hospitalieres-relatives-a-lepidemie-de-covid-19/ ↩
-
Royal Society DELVE Initiative (7-day rolling average, 21 Nov) ↩
-
Pfizer, Pfizer and BioNTech Announce Vaccine Candidate Against Covid-19 Achieved Success In First Interim Analysis From Phase 3 Study, November 2020 ↩
-
Moderna, Moderna’s COVID-19 Vaccine Candidate Meets its Primary Efficacy Endpoint in the First Interim Analysis of the Phase 3 COVE Study, November 2020 ↩
-
Pfizer, Pfizer And BioNTech Conclude Phase 3 Study Of Covid-19 Vaccine Candidate, Meeting All Primary Efficacy Endpoints, November 2020 ↩
-
As of 22 November, the list was: older adults’ resident in a care home and care home workers; all those 80 years of age and over and health and social care workers; all those 75 years of age and over; all those 70 years of age and over; all those 65 years of age and over; high-risk adults under 65 years of age; moderate-risk adults under 65 years of age; all those 60 years of age and over; all those 55 years of age and over; all those 50 years of age and over; and the rest of the population (priority to be determined) ↩
-
Public Health England & NHSX, Testing in United Kingdom, November 2020 ↩
-
Department of Health and Social Care, Test and trace weekly stats (5-11 November), November 2020 ↩
-
Department of Health and Social Care, NHS Test and Trace Weekly statistics, November 2020 ↩
-
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/932251/Slides_presented_by_Chief_Scientific_Advisor_to_accompany_coronavirus_press_conference_31_October_2020.pdf ↩
-
ONS Covid-19 Infection Survey, 6 November 2020 ↩
-
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/933225/S0824_SARS-CoV-2_Transmission_routes_and_environments.pdf ↩
-
ONS, Social Impacts of Coronavirus, 14 May. ↩
-
ONS, Social Impacts of Coronavirus, 20 November. ↩
-
Non-pharmaceutical interventions (NPIs) table, 21 September 2020 ↩
-
Ministry of Housing, Communities & Local Government, Coronavirus (COVID-19): emergency funding for local government, March 2020 (Updated October 2020) ↩
-
Minister for Equalities sets out government action to tackle Covid disparities ↩
-
Department of Health and Social Care, Personal protective equipment (PPE) strategy: stabilise and build resilience, September 2020 ↩
-
ONS, Earnings and Employment from PAYE Real Time Information, November 2020 ↩
-
HM Treasury, Forecasts for the UK Economy: a comparison of independent forecasts, November 2020 ↩
-
HM Treasury, Coronavirus (COVID-19) business loan scheme statistics, 19 November 2020 ↩
-
HMRC, Coronavirus (COVID-19) statistics, 22 October 2020. ↩
-
Department for Education, Attendance in education and early years settings during the coronavirus (COVID-19) ↩
-
Department for Education ↩