Guidance on the hepatitis B antenatal screening and selective neonatal immunisation pathway
Updated 11 August 2023

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/hepatitis-b-antenatal-screening-and-selective-neonatal-immunisation-pathway/guidance-on-the-hepatitis-b-antenatal-screening-and-selective-neonatal-immunisation-pathway--2
Foreword
The World Health Organization (WHO) has classified hepatitis as an international public health challenge comparable to malaria, HIV and tuberculosis.
We are committed to the WHO global goal of eliminating viral hepatitis, re-emphasised as a priority in the Public Health England (PHE) Infectious Disease Strategy 2020 to 2025.
The introduction of the hexavalent vaccine, as part of the universal childhood immunisation programme in 2017, provided an opportunity for collaborative working by the infectious diseases in pregnancy screening programme and national immunisation team.
The aim was to develop a quality improvement strategy to improve the care for women living with hepatitis B and their babies.
A review of the hepatitis B antenatal screening and neonatal immunisation pathways has clearly illustrated that an integrated approach is essential to the effective delivery of linked programmes, particularly at the point of handover of care from one service to another.
Women living with hepatitis B do not tend to have ‘loud voices’. We must be their advocates and support them throughout their pregnancy journey and beyond.
Even though we are classified as a low prevalence country we must continue to strive for optimum delivery of equitable care for all to address inequalities – a PHE and NHS England and Improvement priority.
These new national guidelines and resources, developed with extensive stakeholder input, will support professionals across the health care community in delivering effective care so that women, their babies and families receive the right care at the right time to make a positive difference to their lives.
We would like to thank everyone involved in producing these guidelines and resources and most of all those in the NHS who deliver screening and immunisation services every day.
The purpose of the guidelines
The purpose of this document is to provide a guide for providers and commissioners on the delivery of antenatal screening and selective neonatal immunisation services for pregnant women living with hepatitis B and their babies.
The aim is to support the provision of timely antenatal screening and entry into clinical care for women living with hepatitis B and optimise delivery of the infant hepatitis B selective immunisation programme for infants who are at a risk of vertical transmission of hepatitis B virus infection.
The document summarises the elements of the screening and immunisation pathways, including the current recommended immunisation schedule. The scope does not extend into clinical care. This is addressed in clinical guidelines from the British Association for the Study of the Liver (BASL) and British Viral Hepatitis Group (NHVG). However, it is important to acknowledge the need for seamless transition from screening and clinical care to immunisation services.
This document provides a chronological description of the hepatitis B antenatal screening and selective neonatal and infant immunisation pathways with required actions and signposting to patient information and resources to support safe and effective delivery of the services.
The pathway guidelines writing group
| Name | Title |
|---|---|
| Sharon Webb | Programme Manager, NHS Infectious Diseases in Pregnancy Screening (IDPS) Programme, PHE Screening |
| Dr Sema Mandal | Consultant Epidemiologist, Lead for Viral Hepatitis, Immunisation and Countermeasures Division and Section Head – Blood Safety, Hepatitis, STI and HIV Division, PHE |
| Dr Samreen Ijaz | Clinical Scientist, Deputy Head – BBV Unit, PHE |
| Patricia Schan | Clinical Project Advisor, IDPS Programme, PHE |
| David Green | Consultant Nurse, Immunisation and Countermeasures Division, PHE |
| Michelle Falconer | Immunisation Nurse Specialist, Immunisation and Countermeasures Division, PHE |
| Dr Miranda Mindlin | Consultant in communicable disease control, South London Health Protection Team, PHE |
Introduction
Hepatitis B is an infectious disease caused by the hepatitis B virus (HBV) that affects the liver. The virus causes both acute and chronic infections. An estimated 257 million people or 3.5% of the global population are living with chronic hepatitis B virus infection: WHO Global hepatitis report 2017.
Clinical picture
The incubation period of HBV infection ranges from 40 to 160 days, with an average of 60 to 90 days.
Acute infection
This can be asymptomatic. If symptoms occur they may include fever, malaise and abdominal pain. Jaundice occurs in approximately 10% of younger children and in 30 to 50% of adults. Most adults (90%) with acute HBV infection recover completely but only 10% of infants will clear the virus. Acute infection may occasionally lead to fulminant hepatic necrosis, which is often fatal.
Chronic infection
This develops in 5 to 10% of adults, 20 to 50% of children under the age of 6 years and over 90% of newborns following infection. Individuals with chronic HBV infection may carry the virus for the rest of their lives. They have an increased risk of developing liver cirrhosis (permanent scarring of the liver) over a period of years and sometimes cancer of the liver. Patients with chronic infection should be managed by a hepatologist or gastroenterologist. Antiviral treatment can help to reduce the progression of liver disease and complications.
Transmission
Globally, perinatal transmission vertically (from mother to baby) is the most common route of HBV acquisition and represents an important contribution to establishing chronic infections within populations. Hepatitis B is more infectious than other blood borne viruses like hepatitis C and HIV.
Hepatitis B virus can be passed from person to person through unprotected sexual intercourse, direct contact with the blood of an infected person, including within the household (horizontal transmission), sharing contaminated needles and through perinatal transmission.
Perinatal transmission rates, in the absence of immunisation of the newborn at birth, can be as high as 90% from higher infectivity mothers and approximately 10 to 40% from lower infectivity mothers. Of those babies who are infected at birth or during the first year of life, around 90% will go on to develop chronic infection. The disease will progress to liver cirrhosis and liver cancer in 15% to 40% of children with chronic infection. See PHE Green Book Hepatitis B: chapter 18.
The global elimination strategy
WHO has classified hepatitis as an international public health challenge comparable to malaria, HIV and tuberculosis. WHO has called for specific action to eliminate it as a public health threat by 2030 in the first ever global health sector strategy for viral hepatitis WHO, 2016.
In 2015, hepatitis B resulted in 887,000 deaths, mostly from complications including cirrhosis and hepatocellular carcinoma (primary liver cancer).
The strategy addresses all 5 hepatitis viruses (hepatitis A, B, C, D and E), with a focus on hepatitis B and C, owing to the relative public health burden they represent. It also provides a vision of a world:
- where viral hepatitis transmission is halted
- where everyone living with viral hepatitis has access to safe, affordable and effective care and treatment
- with a reduced incidence of chronic hepatitis infection from the current 6 to 10 million cases of chronic infection to 0.9 million infections
- with a reduction in annual deaths from chronic hepatitis from 1.4 million to less than 0.5 million
Five core intervention areas have been identified
1. Vaccines
- A, B, E available
- large scale hep B childhood programmes
2. Prevention of mother-to-child transmission of hepatitis B
- antenatal testing
- antivirals in pregnancy
- timely birth dose
3. Injection, blood and surgical safety
- universal precautions and safety measures
- safe blood
4. Harm reduction for people who inject drugs
- access to sterile equipment and drug dependence treatments
5. Treatment
- effective treatment and monitoring regimens
Prevention of perinatal transmission
The UK is a very low-prevalence country. HBV infection is unevenly distributed throughout England with some areas of the country having a higher prevalence of infection than others. Prevalence of HBV infection is higher in those born in high-endemicity countries, many of whom will have acquired infection at birth or in early childhood Boxall et al., 1994; Aweis et al., 2001.
This is reflected in the rates found in women presenting for antenatal screening. Coverage of antenatal screening remains high at over 99%. Overall 0.4% of pregnant women in England screen positive or are known to be HBV infected (Tables 1 and 2) PHE.
Table 1: Screen positive rates for hepatitis B in pregnant women, England, 2018 to 2019*
| Region (returns included/expected) | Women tested | Screen positive women | Newly diagnosed women | ||
|---|---|---|---|---|---|
| n | Rate/1000 women tested | n | Rate/1000 women tested | ||
| London (26/26) | 145,728 | 1,030 | 7.07 | 223 | 1.53 |
| Midlands and East (41/41) | 197,347 | 735 | 3.72 | 193 | 0.98 |
| North (41/43) | 177,929 | 490 | 2.75 | 111 | 0.62 |
| South (36/36) | 155,616 | 370 | 2.38 | 78 | 0.50 |
| England (141/146) | 676,620 | 2,630 | 3.89 | 605 | 0.89 |
Table 2: Screen positive rates for hepatitis B in pregnant women, all screen positive women, England, 2016 to 2019*
| 2015 to 2017 | 2017 to 2018 | 2018 to 2019 | ||||
|---|---|---|---|---|---|---|
| Returns included (included/expected) | Rate/1000 women tested | Returns included (included/expected) | Rate/1000 women tested | Returns included (included/expected) | Rate/1000 women tested | |
| England | 90/145 | 3.79 | 125/147 | 4.16 | 141/146 | 3.89^ |
| ^The rate for total screen positive women in year 2018 to 2019 is based on a count that has been rounded to the nearest multiple of 5 to prevent disclosure by comparison with other published data. |
*The screen positive rates are based upon 2 separate data collections relating to the number of women who were booked for antenatal care in the reporting period and subsequently tested (including women who were known positives and not retested), and the number of women with screen positive results/known positive status reported in the reporting period. The 2 cohorts of women may therefore differ slightly, and the screen positive rates should therefore be interpreted with caution.
In pregnant women who are positive for hepatitis B virus, the aim is to eliminate vertical transmission to the baby through timely immunisation with a hepatitis B vaccine (Table 3). Where the mother is deemed higher infectivity the addition of hepatitis B immunoglobulin (HBIG) is recommended within the first 24 hours of birth (Tables 4 and 5). If the schedule is carried out according to the Green Book recommendations it has a dramatic impact on reducing perinatal transmission, with significant reduction in infections in babies Wait S; Chen D. 2012.
Table 3: The proportion of babies born to hepatitis B positive women who has received timely neonatal hepatitis B vaccination within 24 hours of birth, 2018 to 2019
| Region (returns included expected) | Babies receiving vaccination within 24hrs of birth | Babies requiring vaccination | Performance (%) |
|---|---|---|---|
| London (26/26) | 831 | 833 | 99.8 |
| Midlands & East (41/41) | 570 | 584 | 97.6 |
| North (43/43) | 418 | 422 | 99.1 |
| South (36/36) | 293 | 296 | 99.0 |
| England (146/146) | 2,112 | 2,135 | 98.9 |
Table 4: The proportion of babies born to hepatitis B positive women who has received timely hepatitis B immunoglobulin within 24 hours of birth, 2018 to 2019
| Region (returns included expected) | Babies receiving immunoglobulin within 24hrs of birth | Babies requiring immunoglobulin | Performance (%) |
|---|---|---|---|
| London (26/26) | 73 | 75 | 97.5 |
| Midlands & East (41/41) | 61 | 61 | 100 |
| North (43/43) | 43 | 46 | 93.5 |
| South (36/36) | 22 | 24 | 91.7 |
| England (146/146) | 199 | 206 | 96.6 |
Table 5: The proportion of babies born to hepatitis B positive women who received timely neonatal vaccination +/- immunoglobulin, England, 2016 to 2019
| HBV vaccination | Hepatitis B immunoglobulin | |||||
|---|---|---|---|---|---|---|
| 2016 to 2017 | 2017 to 2018 | 2018 to 2019 | 2016 to 2017 | 2017 to 2018 | 2018-2019 | |
| England | 98.4% | 98.9% | 98.9% | 93.3% | 97.9% | 96.6% |
Source: PHE Screening
Antenatal screening and selective neonatal immunisation programmes
The provision of antenatal screening and a targeted neonatal immunisation programme has been supported by Department of Health (DH) policy since 1998 (DH, 1998). The UK National Screening Committee (UK NSC) recommends systematic population screening in pregnancy for HIV, hepatitis B and syphilis (PHE).
The NHS IDPS Programme, part of PHE, requires all pregnant women to be offered and recommended screening separately for all 3 infections early in every pregnancy, irrespective of previous results (PHE; NHS England). The aim is to significantly reduce the vertical transmission of HIV, hepatitis B and syphilis by early detection, intervention and treatment to safeguard the health of the baby and the woman’s own health.
The aim of the PHE selective hepatitis B immunisation programme is to prevent babies acquiring HBV following exposure to their mothers’ blood and body fluids especially around the time of birth. As this is a post-exposure vaccination programme, timely administration of all doses of vaccine (±HBIG at birth) is vital in preventing the baby becoming persistently infected with hepatitis B virus.
In 2014 the Joint Committee on Vaccination and Immunisation (JCVI), which advises government on national immunisation programmes, recommended that a universal infant immunisation programme be introduced in the UK, subject to a combination hepatitis B containing vaccine being procured at a cost-effective price.
In autumn 2017, following successful procurement, a hexavalent vaccine (DTaP/IPV/Hib/HepB) which includes protection against hepatitis B was added to the routine childhood vaccination in the UK schedule for babies born on or after 1 August 2017. As well as protecting against hepatitis B virus, this vaccine also protects against diphtheria, tetanus, pertussis (DTaP), polio (IPV) and Haemophilus influenzae type B (Hib).
As the hexavalent vaccine is given at 8, 12 and 16 weeks of age in the routine childhood schedule, babies born to hepatitis B infected mothers still need to have urgent post exposure vaccination with hepatitis B monovalent vaccine at birth and 4 weeks old, followed by 3 hexavalent vaccine doses as part of the routine programme and a final monovalent dose at one year old.
As chronic infection in an infant is asymptomatic, testing at one year old is strongly recommended, preferably with a dried blood spot (DBS) test provided free by PHE Colindale, Virus Reference Department.
The quality improvement initiative
The UK has a comprehensive package of measures designed to significantly reduce the risk of transmission of hepatitis B virus infection from the mother to her baby during the perinatal period but evidence suggests there is scope to improve the delivery of these.
The introduction of the hexavalent vaccine as part of the universal childhood immunisation programme in autumn 2017 provided an opportunity for collaborative working by the PHE screening and the immunisation programmes and clearly illustrated that an integrated approach is essential to the delivery of an effective screening programme and infant immunisation service.
Health professionals should be aware of the importance of ensuring that babies born to women with hepatitis B require an accelerated course of hepatitis B immunisation starting at birth. This vaccine course is urgent targeted treatment for babies that have been significantly exposed to HBV around the time of birth.
Post exposure vaccination is critical targeted treatment for babies that have been significantly exposed to HBV around the time of birth
Evidence driving quality improvements
The need for a collaborative quality improvement initiative was reinforced by:
- national audit findings
- immunisation surveillance findings
- evidence from screening quality assurance reviews
- data analyses of screening programme standards and key performance indicators
- immunisation data returns
- reports of safety incidents in both screening and immunisation programmes
National hepatitis B in pregnancy audit
In 2013, the IDPS Programme commissioned an epidemiology team at UCL Great Ormond Street Institute of Child Health to undertake a national clinical audit of the management of pregnant women with hepatitis B in England. This was modelled on the National Study of HIV in Pregnancy and Childhood (NSHPC). The aim was to measure current practice against IDPS standards to highlight aspects of service provision that required improvement and to optimise current strategies for prevention of vertically-acquired hepatitis B in the UK.
The audit included 2,538 pregnant women with hepatitis B who booked for antenatal care in England in 2014 with information on maternity care and, for high risk women, care in specialist services. The audit was later extended to work in partnership with PHE Immunisation Division to link audit data with information on whether infants born to women in the audit went on to receive the full hepatitis B vaccination schedule at 4 and 8 weeks and vaccination and serology test to ascertain infection status at one year.
Gaps in the delivery of the screening and immunisation pathways were noted, and disconnect between health care service providers, which can undermine actions to address inequalities – a PHE and NHS England priority.
Main findings
Sociodemographic
- a total of 2,542 pregnancies in 2,538 women with hepatitis B surface antigen (HBsAg) were reported to the audit, 45% from London
- a third of women were born in Africa, a third in Asia and a third in Europe (6% in the UK)
- 18% of women had basic and 21% < basic level of English
- antenatal care began at a median 11 weeks gestation, and at ≥ 20 weeks gestation in 10% of the women
- 70% of pregnancies were in women with a prior hepatitis B diagnosis
- women newly screened HBsAg positive were younger, more likely to lack basic level English and more likely to have booked for antenatal care at ≥ 20 weeks gestation than the previously diagnosed group
Screening and clinical pathways
- of 151 pregnancies without a documented scheduled specialist appointment at the reporting trust, reasons included:
- late booking
- receiving specialist care at, or being transferred to, another trust
- referral not made or specialist appointment not offered
- women declining or not responding to appointment invitations
- and lack of clarity around documentation
- defaults on specialist appointments were reported by maternity units in 18% of pregnancies and were more common among women with less than basic English and ≥ 2 previous live births
- antiviral treatment was received in 11% (180/1672) of pregnancies with treatment data available, and in 74% (37/50) of pregnancies with an HBV DNA level of >107 IU/ml reported at notification
Child vaccination and serology at 12 months
- of the total 2,204 liveborn infants:
- 85% of babies were given hepatitis B vaccine within 24 hours of delivery
- 1.4% at > 24 hours after delivery
- 11% were vaccinated but timing unknown
- there was a small number of deceased babies who were not given vaccine
- 2.5% of babies had missing information on vaccine administration
- data on HBIG administration to the baby was available for 238 (92%) of the 260 pregnancies with higher infectivity markers at notification
- of these, HBIG was administered to the baby in 87% (207/238)
- linked data on completion of the vaccination schedule at 1 and 2 months and 1 year, and infant serology at 1 year was available from PHE for a subgroup of 309 babies from 302 audit pregnancies, mostly those of higher infectivity. Of these:
- all of them received the second vaccine dose (scheduled for 1 month)
- 241 (78%) were reported to have received the fourth dose while for the remainder, this was unknown or missing
- only 167 (54%) of the 309 children in the linked data set had infection status available, none of these had evidence of hepatitis B infection
National infant hepatitis B immunisation surveillance data
The PHE national surveillance programme of infants born to women deemed to be of higher infectivity shows that since 2016, HBIG administration and birth dose vaccine uptake rates are consistently over 95% (Tables 3 to 5) but this percentage falls below 90% for the 4-week dose and 75 to 85% for the 12-month dose (Table 6).
In England up to 3 infants per year born to women deemed to be of higher infectivity acquire persistent infection despite receiving HBIG and vaccine. However, only half of the higher risk infants are reported as being tested at 12 months for evidence of HBV infection so this number may be more.
Investigations are undertaken in samples from infants who are found to be HBV infected when tested at 12 months of age. A recent review by PHE of possible factors associated with HBV infection in 69 infants found all to have received HBIG and vaccine in accordance to national recommendations May et al., 2018.
Approximately 40% of infants harboured a virus with amino acid changes in the HBV major antigenic region which may allow the virus to escape the vaccine.
Maternal viral load was also shown to be an important factor in those infants found to be HBV-infected. The review could not explore if babies had been infected during pregnancy (in utero infection).
Table 6: Neonatal hepatitis B vaccine coverage of 3 doses (HepB3) at 12 months, by PHE Centre, 2018 to 2019 in those at risk of vertical transmission
| PHE centre/region | 2018 to 2019 | ||
|---|---|---|---|
| Local authority returns included (included/expected) | Infant denominator | HepB3 coverage % | |
| London | 33 (33) | 816 | 83.3 |
| East of England | 12 (12) | 256 | 82.0 |
| West Midlands | 14 (14) | 248 | 94.8 |
| East Midlands | 9 (9) | 120 | 89.2 |
| North East | 12 (12) | 29 | 93.1 |
| North West | 16 (23) | 472 | 27.3 |
| Yorkshire and the Humber | 15 (15) | 156 | 90.4 |
| South West | 16 (16) | 102 | 86.3 |
| South East | 17 (18) | 226 | 91.6 |
| England | 144 (152) | 2,425 | 75.2 |
Source: PHE. Note experimental data: annual data is not routinely published in national immunisation statistics because of data quality issues (completeness and reporting)
Screening programme data
Data is collated both quarterly and annually against each of the screening standards for the IDPS programme in England. The standards data gives a high-level overview at key points on the screening pathway and contributes to the quality assurance of the screening programme.
Standard SO5b measures the percentage of women with confirmed screen positive results for hepatitis B, or known positive for hepatitis B, who attend a screening assessment appointment ≤ 10 working days with the maternity services screening team. The rationale for the standard is to provide assurance that all women are referred in a timely manner and receive timely intervention.
A screening assessment is a face-to-face appointment with a member of the screening team (screening coordinator, specialist midwife or clinical nurse specialist), to facilitate reporting of a new confirmed positive screening result and, or a comprehensive assessment of women with a known positive status.
Data collated by PHE demonstrated that no region is currently meeting the acceptable threshold for IDPS- S05b (Tables 7 and 8), supporting the need for providers to review their pathways for hepatitis B to achieve timely assessment by the screening team.
The principles of the assessment visit are to:
- form a proactive working relationship with the woman
- carry out a holistic, person-centred assessment
- provide a central, continuous point of contact for the woman
- act as the key advocate for the woman when required
- assist the woman in the successful navigation of complex health and social care systems
Table 7: Proportion of screen positive women attending specialist assessment within 10 working days, England, 2018 to 2019
| Region | Attended screening assessment within 10 working days | Screen positive women | Performance (%) |
|---|---|---|---|
| London (26/26) | 822 | 1,032 | 79.7 |
| Midlands and East (41/41) | 545 | 735 | 74.1 |
| North (43/43) | 434 | 502 | 86.5 |
| South (36/36) | 311 | 371 | 83.8 |
| England (146/146) | 2,112 | 2,640 | 80.0 |
Table 8: Proportion of women with screen positive results attending a screening assessment within 10 working days, England, 2016 to 2019
| 2016 to 2017 | 2017 to 2018 | 2018 to 2019 | ||||
|---|---|---|---|---|---|---|
| Returns included (included/expected) | % attending screening assessment within 10 working days | Returns included (included/expected) | % attending screening assessment within 10 working days | Returns included (included/expected) | % attending screening assessment within 10 working days | |
| England | 122/145 | 72.8 | 128/147 | 78.2 | 146/147 | 80.0 |
Source: PHE Screening
Screening and immunisation safety incidents
Screening and immunisation safety incidents have been reported and investigated across multiple points on the pathway, with recurrent themes. This further demonstrates the need for regular review of services and pathways to drive continuous quality improvement.
The incident themes included:
Referral issues:
- woman referred to hepatology, but no appointment was sent. This was not discovered until submitting Screening Key Performance Indicator quarterly data returns
- woman hepatitis B positive, referral sent to hepatology secretary by fax, not received, so no appointment or follow up care arranged
- woman disclosed a positive status at the booking visit with her community midwife but specialist midwife was not informed so no follow up care arranged
Vaccine and HBIG issues:
- missed and delayed vaccine doses
- missed HBIG and emergency issue requests for HBIG
- no request made for HBIG
- HBIG lost
- HBIG used on a different child
- multiple pregnancies did not order HBIG for every infant
Aim of the quality improvement initiative
The aim of the PHE collaborative quality improvement initiative was to enable and facilitate improvements in the current service provision to ensure there are effective antenatal screening and infant immunisation pathways for women with hepatitis B and their babies in England.
This was a joint project with the PHE IDPS programme and the National Infection Service (NIS) Blood-borne Virus Unit (BBVU) and Immunisation and Countermeasures Division.
Two project groups were convened to support the project:
-
internal project group – members from the PHE IDPS programme, NIS BBVU and Immunisation and Countermeasures Division teams led on the project work streams and deliverables and presented these to the strategic group for review and comment
-
strategic project group – multidisciplinary representation from the PHE IDPS, BBVU, Immunisation and Countermeasures teams, PHE local Health Protection Teams (HPTs), Screening and Immunisation Teams (SITs), NHS clinical specialists, antenatal screening coordinators and primary care teams and professional bodies.
The project objectives were to:
- facilitate a multi-disciplinary approach with clear roles and responsibilities
- improve surveillance services
- empower women and their families
- increase public awareness and knowledge
- improve professional knowledge
- increase multidisciplinary working
A comprehensive work plan was devised including:
Policy and guidelines
- to develop new guidance for professionals to replace existing 2011 Department of Health best practice guidelines
- to support the review of the British Association for the Study of the Liver BASL and British Viral Hepatitis Group (BVHG) 2008 clinical guidelines
- to update the NHS England and Improvement IDPS and hepatitis B infant immunisation programme service specifications to include a new generic IDPS screening pathway; the rationale for retesting all women in each pregnancy and a reference to these guidelines
Screening and immunisation pathway
- to design a detailed screening pathway for women with hepatitis B and their babies
- to update the current care pathway to offer testing to all pregnant women including those already known to be hepatitis B positive
- to develop new parent leaflets for screen positive women to focus on the importance of the immunisation schedule for their babies
- to clarify roles, responsibilities and timeframes for screening and primary care teams at all points in the care pathway
- to improve handover of infant’s care from maternity to primary care to ensure timely completion of immunisation schedule
- to develop a practical safety checklist for screening coordinators to utilise to aid the management of care for hepatitis B positive women and their babies
- to design a ‘PHE hepatitis B delivery suite box’ to aid the timely ordering, safe storage and administration of HBIG and follow up surveillance processes
- to develop notification letter templates for trusts to utilise to help standardise and manage the handover of care from one service to another for women and their babies
Surveillance services
- to embed the data fields from the national hepatitis B in pregnancy outcomes audit into the IDPS Integrated Screening Outcomes Service (ISOSS)
- to implement the enhanced requirements for the National Hepatitis B Infant Surveillance to improve monitoring of the impact of the immunisation programme
- to establish clear guidance on disease notification processes
Training and education
- to deliver a series of regional stakeholder workshops to inform the development of the pathways, resources and supporting guidance for providers
- to publish professional communications and blogs to raise awareness of the quality improvement initiative
- to produce resources to support the delivery of the programmes
Surveillance services and programmes
Monitoring of screening outcomes is a core deliverable for all national screening programmes. Within the IDPS Programme, the collation and analyses of screening outcome data is essential to:
- monitor the performance of the screening programme
- review all positive cases to inform screening programme pathways, policies and standards
- identify areas for further audit, research and service improvements
The hepatitis B infant immunisation programme informs on vaccine coverage, timeliness and outcome in eligible infants by monitoring vaccination at the recommended age, completion of the full course of vaccines, and testing for infection at one year of age.
This is to ensure optimal benefit from vaccination and early referral to specialist services if required. The programme also monitors for changes in the hepatitis B virus that may impact on the effectiveness of the immunisation programme.
Integrated screening outcomes surveillance service
The Integrated Screening Outcomes Surveillance Service (ISOSS) monitors and evaluates outcomes of the IDPS programme. Data analysed through the ISOSS allows PHE to assess the impact of the programme on:
- prevention of vertically acquired HIV, hepatitis B and syphilis
- protecting the health of women with HIV, hepatitis B and syphilis during and after pregnancy
- protecting the health of any children born to women with HIV, hepatitis B and syphilis
- protecting the health of infants and children diagnosed with HIV, hepatitis B, congenital syphilis and congenital rubella syndrome
By collecting data on a national level, ISOSS can assess vertical transmission rates on a larger scale. Audits can be completed, trends can be analysed and common complicating issues in care can be identified. This leads to recommendations being made locally and nationally, strengthening policy and practice, and improving care for mothers and their children.
Enhanced maternal and infant hepatitis B surveillance programme
A comprehensive programme of enhanced surveillance of HBV screen positive women and babies born to these women will be introduced from April 2021. This will build on the existing surveillance programme established in the 1990s. The purpose of surveillance is to evaluate the impact of the infant selective immunisation programme on transmission of infection to the baby.
The aim is to:
- confirm the mother’s infectivity risk
- determine if the mother is infected with a mutant HBV strain which might evade the vaccine (vaccine escape strain) and therefore potentially affect the management of this and future pregnancies
- monitor factors associated with HBV infection in babies born to screen positive women
- quantify the contribution of vaccine failure and in utero transmission in HBV infections in these infants
- inform future interventions such as earlier antiviral therapy to prevent in utero transmission during pregnancy
Surveillance data on the mother will be obtained by:
- HBV DNA levels at the first screening assessment in pregnancy from all screen positive women
- HBV DNA levels at time of delivery from higher infectivity women
Surveillance data on the baby will be obtained by:
- HBV DNA and HBsAg testing via heel-prick DBS at birth in babies born to higher infectivity women
- HBsAg and anti-HBc testing ideally via DBS at 12 months old. This is the definitive assessment of chronic persistent infection in the baby
In higher infectivity women, HBV DNA viral load will be determined in the early stages of pregnancy and at the time of delivery which will inform on how this marker has changed during the pregnancy, particularly in response to antiviral treatment. In the baby, the DBS samples taken at birth will be tested for HBV DNA (viral load) and HBV serological markers. This will indicate whether the baby had been infected with hepatitis B virus in utero. This may affect the management of the woman’s future pregnancies.
Samples collected for surveillance purposes will be tested and retained at PHE Virus Reference Department (VRD), Colindale, London. The purpose of the PHE surveillance samples should be discussed with the woman and informed verbal consent obtained to take the samples as per normal maternity care practice. The discussion and consent should be documented in the maternal notes and on the hepatitis B in pregnancy checklist.
Antenatal maternal surveillance sample
The first maternal surveillance venous sample should be taken at the screening assessment appointment with the antenatal and newborn screening team to discuss the woman’s positive HBV result:
- this should be arranged within 10 days of notification of the confirmed HBV screen positive test results from the laboratory to the screening team IDPS Standard 5
- this sample will be requested from all HBV screen positive mothers (higher and lower infectivity risk)
- the sample should be collected in provided ethylenediaminetetraacetic acid (EDTA) blood tubes and sent to the PHE laboratory in Colindale with a completed request form in pre-paid return packaging
This surveillance blood sample should not interfere with the collection of samples for HBV viral load and marker testing as per local practice as agreed with the virology laboratory and hepatology clinical team.
If the woman declines to have maternal serology and or neonatal DBS taken it should be recorded in her notes and on the completed request forms and returned to PHE Colindale.
Postnatal maternal surveillance sample
The second maternal venous surveillance sample should be taken on delivery suite from those women classified as being of higher infectivity after the woman has delivered her baby. EDTA blood tubes, request forms and pre-paid return envelopes will be available in the ‘hep B delivery suite box’ which, along with the HBIG, will be sent to maternity units approximately 7 weeks prior to the estimated delivery date.
Newborn DBS sample
A DBS test should be taken on delivery suite from babies born to mothers classified as being at higher infectivity before administration of the vaccine and HBIG.
The DBS cards, instructions on collection and pre-paid return envelopes will be provided in the hep B delivery suite box, which along with the HBIG, will be delivered to maternity units approximately 7 weeks prior to the estimated delivery date.
This surveillance blood sample is different to the newborn blood spot screening sample taken on day 5 after the baby’s birth. The mother should be informed that the baby will still need to have the newborn blood spot screen sample on day 5. This DBS is not subject to the standards or requirements of the newborn blood spot screening programme.
If the woman declines to have maternal serology and or neonatal DBS taken it should be recorded in her notes and on the completed request forms and returned to PHE Colindale.
12-month infant DBS sample
At 12 months old a diagnostic sample should be taken from the infant to check if they have become infected with HBV via vertical transmission.
This is the definitive test for determining the infant’s hepatitis B status and should not be confused with the newborn DBS test at birth which is collected for surveillance purposes and not to inform individual patient management at that time.
A DBS sample taken in primary care is the preferred method, as it is non-invasive, quick and simple and does not require a referral to hospital phlebotomy services.
It can be taken at the same appointment as the 12-month immunisations.
PHE offers the free national DBS testing service for infants.
If the national DBS service is not used, results of venous sample testing arranged locally should be reported to the Immunisation team at PHE Colindale using the request for information form which will be sent to the infant’s practice at 12 to 15 months.
Reporting of test results
Maternal
- the antenatal maternal blood test results will be sent back to the screening coordinator or team to report to the specialist team responsible for the woman’s hepatology care
- occasionally the results from PHE VRD will be different from the test results from the local laboratory. If this difference would change the infectivity status of the mother, or alter the planned care for mother or baby, specialist clinical teams from maternity should discuss with PHE VRD, using the telephone number provided on the laboratory test results report
- the postnatal maternal blood test results will not be reported as they will not change the management of the mother. This sample is part of the PHE surveillance process. These results are to monitor HBV DNA viral load changes during pregnancy to better understand the impact on transmission of HBV and inform intervention recommendations. The results will be available on request only
Neonatal
- the baby’s birth DBS result will not be reported at the time of testing as it will not influence the immediate management of the baby
- the baby should complete the hepatitis B immunisation course and the baby’s hepatitis B status should be checked at 12 months, ideally using the PHE infant DBS service
- if DBS is not used for the 12-month sample then the result of the test should be communicated to the VRD clinical team at Colindale to triangulate results. VRD can be contacted by phone: 0208 327 6554 or by email at phe.hepatitisbbabies@nhs.net (please send from an nhs.net email address only)
- the baby’s 12-month serology/DBS test results will be sent to the GP. If the 12-month DBS is done by PHE, the birth DBS result will be included if appropriate. The 12-month result gives a definitive result on the baby’s HBV infection status
- if in any doubt as to interpretation of results, a clinician can contact PHE VRD clinical team on the telephone number provided on the laboratory test results report
Screening and immunisation pathways
Delivery of the total pathway from maternal booking for antenatal care up to completion of the infant immunisation schedule at one year requires multidisciplinary team (MDT) working and excellent communication between primary and secondary care services (Appendix 3). Care must be handed over seamlessly from one provider to the next to ensure that women and their babies receive the appropriate optimum care and treatment, particularly as the pathways transcend different organisations. Every health care professional involved in the pathways plays a vital role in this process to ensure ‘every contact counts’.
The following teams are likely to be involved in the delivery, commissioning and monitoring of the pathways, subject to local arrangements and individualised care requirements:
Midwifery, nursing and medical teams
- antenatal and newborn screening coordinator or teams
- liver specialists (hepatologists, virologists, gastroenterologists, microbiologists)
- clinical nurse specialists and specialist midwives
- community midwives
- obstetricians
- delivery suite teams
- paediatric and neonatology teams
- screening and diagnostic laboratories
- pharmacists
NHS England and Improvement
- commissioners
- screening and immunisation teams
PHE
- IDPS programme
- Screening Quality Assurance Service (SQAS)
- health protection teams
- Immunisation and Countermeasures Division (in National Infection Service, NIS)
- BBVU of the VRD in NIS
Primary Care
- general practitioners
- practice nurses
- practice managers, reception and clerical teams
Others
- health visitors
- child health information services
- clinical commissioning groups
The antenatal screening pathway
All pregnant women with hepatitis B and their babies should be cared for by a defined MDT in line with national guidance:
- NHS IDPS programme PHE
- National Institute for Health and Care Excellence (NICE) hepatitis B (chronic): diagnosis and management: clinical guideline 165
- British Association for the Study of the Liver (BASL), British Viral Hepatitis Group (BVHG) Consensus Statement – UK guidelines for the management of babies born to women who are HBsAg positive
- Immunisation against Infectious Disease: Green Book, chapter 18
Personalised care is the key to the delivery of safe care and there is high-level evidence that midwifery-led continuity of carer across the antenatal, intrapartum and postnatal period improve health outcomes. Continuity of carer focuses on relational, woman- centred care and can build trust and significantly improve outcomes for mothers and babies, particularly in BAME and vulnerable populations.
As well as continuity of care, there is a need for providers to develop specialist services and enhanced referral pathways which are shaped by local need and protected as a core function.
The screening coordinator or team should coordinate the care in maternity services, working with hepatology and virology specialists to ensure the woman is fully supported and aware of the importance of completion of the neonatal vaccination schedule and blood test at 12 months for her infant. There must be an agreed local IDPS MDT and clinical hepatology protocol for the management of screen positive women and their babies.
The offer of screening
All pregnant women should be offered and recommended screening for hepatitis B in each pregnancy, irrespective of their previous results and care. This is to:
- ensure there is a current result on the providers laboratory and maternity IT systems
- reduce the risk of missed entry in to the care pathway
- ensure the woman receives updated information on her condition, current care and treatment options and support services and resources available
Screening providers should use information in the Screening tests for you and your baby resource to inform the woman about screening for hepatitis B in pregnancy in a language or format according to her needs to facilitate a personal informed choice.
Women who decline screening
Women may decline screening for several reasons such as a known positive status or needle phobia. Local policies should be in place to support women who decline in line with the national screening pathway and guidance. The IDPS programme commissioned the National Study of HIV in Pregnancy and Childhood (NSHPC) to conduct an audit to investigate the circumstances surrounding the transmission of perinatal HIV (PHIV) in children born in the UK between 2006 to 2013.
The audit identified 108 children with PHIV, of whom around 60% were born to mothers undiagnosed at delivery. Cases were often complex and multifactorial with high rates of adverse psycho-social issues affecting women during the pregnancies.
At least one key factor likely to have contributed directly to PHIV transmission was identified in most cases. The most common were decline of HIV screening in pregnancy (accounting for nearly half of undiagnosed women) and seroconversion (around a quarter).
A subsequent survey found wide variation in the management of women who decline antenatal screening. An expert review panel recommended that the screening programme should consider formalising a clinical pathway for women who decline HIV screening.
Since April 2016 all providers should have a local process in place to notify the screening coordinator or team directly if a woman declines any of the 3 infections offered to facilitate prompt follow up by the screening coordinator or team. The screening coordinator or team should be notified directly to support women who decline screening for any of the 3 infections. This notification should be acknowledged on receipt. The midwife who offered the initial screen should:
- inform the woman that she will be contacted by the screening coordinator or team as soon as possible to discuss her decision
- ensure a blood sample is taken for any of the test(s) the woman accepted and sent to the laboratory with a completed request form, paper and, or, electronic, that clearly identifies the screening tests she has declined
The screening coordinator or team should contact the woman as soon as possible after receipt of a decline notification to facilitate the formal re-offer of screening to the woman by 20 weeks’ gestation (or within 2 weeks if ≥ 24 weeks’ gestation).
The onus of the re-offer is to facilitate personalised choice and not to coerce women to accept screening. The purpose of the re-offer is to:
- enable the woman to have a discussion with a specialist health professional that facilitates an informed decision, not to coerce her to accept screening
- discuss her decision to decline and ensure that she is fully apprised of the benefits of screening for her, her baby, her partner and other children
- offer the screening test(s) and if accepted, arrange testing and follow-up of the result
If the woman declines the second formal re-offer of screening, the local MDT will be responsible for further review and management in line with local clinical protocols. The woman should also be informed her GP will be notified to inform any future health assessments.
Women who are living with hepatitis B
Women who are living with hepatitis B (known to be positive) should be offered screening in the current pregnancy to provide a failsafe mechanism to ensure a current result is available on the trusts reporting system. It should not be presumed that women who are living with hepatitis B fully understand their condition, the implications for their current pregnancy and the current treatment and care regimes available in the UK.
Women who are needle phobic
All providers should have a process in place for MDT management of women with a needle phobia including an anaesthetic team review.
Laboratory testing
The key serological marker of acute and chronic HBV infection is the detection of HBsAg in serum/plasma. Further laboratory investigations will include the assessment of infectivity with the following HBV markers:
- HBV e antigen (HBeAg) – HBV is replicating at high levels and the patient is highly infectious
- HBV e antibody (anti-HBe) – the body’s immune response to the HBeAg and usually indicates lower infectivity
- HBV DNA (viral load) – gives a direct assessment of infectivity. A high HBV DNA level indicates higher infectivity
Further details can be found in the IDPS Screening and Laboratory handbooks.
The screening assessment
Women who are known to be HBV positive or have a confirmed screen positive result, should be invited to attend for screening assessment within 10 working days of the positive report being received from the laboratory, or known positive status being reported to the screening coordinator IDPS Standard SO5.
The time between initial contact with the woman and the appointment should be as short as possible to minimise the duration of the anxiety she is likely to experience. Results should be discussed with her in a face-to-face appointment made with a member of the screening team (screening coordinator, specialist midwife, clinical nurse specialist) within agreed timescales.
A triage system should be adopted to complete any further tests and assessments within local multidisciplinary clinical protocols.
The purpose of the face-to-face appointment with a member of the screening team is:
- to facilitate reporting of a new HBV positive screening result
- support a comprehensive assessment of a known positive woman’s condition and care
- ensure a comprehensive assessment of all women’s needs, including social circumstances and status of possible co-infections, to ensure appropriate involvement of clinical expertise and other support agencies
Using the PHE hepatitis B leaflet the screening coordinator or team member should discuss with the woman, and her partner if present (see appendix 2).
- hepatitis B infection and what it means
- screening test result and what it means
- importance of the MDT in the planning of care for the woman and her baby in pregnancy and beyond
- PHE surveillance process
- requirement to notify all health professional and agencies involved in her and her baby’s care
- importance of completing the vaccination schedule
All women who has accepted and had the screening test performed should receive their result including women whose pregnancy has ended through termination or miscarriage. In the case of a positive result this must include referral into the clinical pathway. A template letter is available (see appendix 2).
Actions required
-
commence PHE hepatitis B maternal and neonatal checklist (see Appendix 2)
- take additional serology tests as per local protocols – HBV viral load, LFTs, hepatitis C
- take PHE maternal venous surveillance sample using supplied sampling kit and send to PHE VRD, Colindale in prepaid packaging
- check, document and manage all other antenatal screening results
Assessment of infectivity
Confirmed positive screening tests are followed with an assessment of hepatitis B infectivity using viral load and hepatitis B e markers. The laboratory team are responsible for the final interpretation, and providing a comment on the HBV results to assign infectivity status in line with the IDPS laboratory handbook screening and reporting algorithms.
If the mother is deemed to be of higher infectivity, the laboratory should advise the responsible team to request HBIG. It is acknowledged that laboratories and maternity services have different processes in place for management of infectivity marker testing. Some laboratories will test for infectivity markers on the initial screening sample, whereas others request a further blood sample. These processes must not delay timely referral to the IDPS MDT and subsequent clinical services.
Actions required
If the woman is deemed to be higher infectivity, then HBIG should be requested from PHE Colindale’s Hepatitis B Infant Coordinator using the current HBIG request form. Indications for HBIG in addition to hep B vaccine are detailed in the Green Book and summarised below.
Babies are considered ‘high risk’ of vertical transmission and should receive HBIG as well as vaccine if:
- mother is HBsAg positive and HBeAg positive
- mother is HBsAg positive and anti-HBe negative
- mother is HBsAg positive and e markers are not available
- mother has acute hepatitis B in pregnancy
- mother is HBsAg positive and infant is born weighing 1,500g or less
- mother is HBsAg positive and known to have an HBV DNA level equal to or above 1 x 106 iu/ml in any antenatal sample in this pregnancy
Babies receive hepatitis B vaccine but do not receive HBIG if:
- mother is anti-HBe positive and HBeAg negative (and no other indication listed above)
Newly diagnosed women should follow the higher or lower infectivity pathway according to their infectivity status.
Management of lower infectivity pregnancies
Following the screening assessment consultation, the screening team should refer the woman to the specialist team as per local arrangements (hepatology, gastroenterology) dependant on whether she is a new diagnosis or known HBV positive woman.
- lower infectivity, known positive – within 18 weeks as per NHS England referral to treatment target
- lower infectivity, new diagnosis – within 6 weeks regardless of infectivity status IDPS Standard SO6
Actions required
The screening team should:
- refer pregnant woman to the specialist team
- notify the GP, Health Visitor, Child Health Information Service (CHIS) and Health Protection Team of the positive result and plans for care (see Appendix 2)
- create a neonatal alert to ensure timely administration of neonatal vaccination on delivery suite within 24 hours of delivery
Antenatal review
A face-to-face appointment with the screening team or MDT in the third trimester of pregnancy, around 34 weeks gestation, provides an opportunity for a reinforcement of the advice that the infant(s) require an accelerated course of hepatitis B vaccination to protect them from the exposure to the virus at birth.
Actions required
An appointment should be arranged to facilitate a review of the woman’s care and utilise the PHE leaflet (see appendix 2) available in multiple languages, to discuss:
- prompt registration of baby with GP
- prompt registration of the baby’s birth
- the importance of completing vaccination programme
Delivery suite and postnatal management of women with lower infectivity
There should be agreed protocols in place to ensure an MDT approach to caring for women with HBV when they present in labour.
Actions required
These should include:
- informing the screening team of the woman’s admission
- arranging administration of monovalent hepatitis B vaccine within 24 hours of the baby’s birth
- completion of the PHCR red book hepatitis vaccination page
- notify screening team of birth and returning notes and checklist to the team
Screening team responsibilities after delivery
Actions required
Ensure the CHIS, Health Visitor and GP are notified of:
- vaccine administration at birth
- the requirement for the second dose of vaccine at 4 weeks and completion of the hepatitis B selective and routine immunisation schedules
Complete:
- PHE hepatitis B in pregnancy maternal and paediatric checklist (See Appendix 2: ‘Resources Template neonatal notification letter, Primary care aide memoire, PHE hepatitis B checklist’)
- PHE IDPS Integrated screening outcomes surveillance service (ISOSS) hepatitis B database (from April 2021)
An aide memoire for primary care staff on the vaccination schedule and testing of the infant is available to download and print or order. This can be enclosed with communications to primary care, for example when CHIS send reminders to GPs for scheduling vaccine appointments (see Appendix 2)
Management of higher infectivity pregnancies
Actions required
The screening team should:
- refer the woman for an appointment with the specialist team (hepatology, gastroenterology etc) within 6 weeks of the positive result being reported to the maternity service Standard S06 – KPI ID2 or by 24 weeks gestation. The screening team should track the progress of this appointment to ensure timely attendance and assessment and support tracking any women not attending
-
notify GP, Health Visitor, CHIS and Health Protection Team of positive result and plans for care (see Appendix 2)
- create a neonatal alert for postnatal neonatal vaccination plus HBIG
- request HBIG and the hepatitis B delivery suite box from the PHE Hepatitis B Infant Coordinator, Immunisation Division, Colindale – email: phe.hepatitisbbabies@nhs.net (from @nhs.net email addresses only as this is patient identifiable information)
Specialist clinical services
Actions required
The clinical team should ensure:
- women are seen within 6 weeks of result or by 24 weeks gestation to plan care and consideration of antiviral therapy as per national clinical guidelines – BVHG and NICE
- request HBIG and the hepatitis B delivery suite box from the PHE Hepatitis B Infant Coordinator, Immunisation Division, Colindale – email: phe.hepatitisbbabies@nhs.net (from @nhs.net email addresses only as identifiable information)
Antenatal review
A face-to-face appointment with the screening team or MDT in the third trimester of pregnancy, around 34 weeks gestation, provides an opportunity for a reinforcement of the advice that the infant(s) require an accelerated course of hepatitis B vaccination and HBIG to protect them from the exposure to the virus at birth.
Actions required
The screening team or MDT should:
- take additional serology and coordinate antiviral therapy as indicated in line with BVHG and local guidelines
- prepare the woman for birth using the PHE screening and immunisation leaflets, including discussing and seeking verbal consent from the mother for the PHE hepatitis B maternal and neonatal surveillance samples at birth
Leaflets are available in multiple languages and include information on:
- hepatitis B virus infection
- care during pregnancy and birth
- prompt registration of baby with GP
- prompt registration of the baby’s birth
- importance of completing vaccination programme
- PHE hepatitis B surveillance processes
Delivery suite and postnatal management of women with higher infectivity
Actions required
On admission to delivery suite:
- inform screening team of admission
- ensure the PHE ‘hepatitis B delivery suite box’ containing HBIG is transferred to delivery suite and stored appropriately according to the Medicines Act in a locked fridge at 2°C to 8°C
After delivery, following the ‘PHE hepatitis B delivery suite box’ instructions:
- take maternal serology sample (pack 1)
- take neonatal HBV DBS prior to vaccination (pack 2)
- administer HBIG (pack 3) plus monovalent hep B vaccine (from local stock)
- complete all paperwork and store with samples in the box
- notify screening team of birth and return notes, box and checklist to the team as soon as possible
- if weekend or bank holiday – store in fridge at 2°C to 8°C and ensure it is delivered to screening team next day
- complete PHCR red book hepatitis vaccination page
Screening team responsibilities following delivery
Actions required
- check maternal blood and newborn DBS samples have been taken
- check laboratory request forms for maternal blood and newborn DBS samples & PHE notification form is fully completed
- dispatch maternal samples and DBS to PHE BBVU in Virus Reference department, Colindale using prepaid supplied envelope7
- ensure the CHIS, Health Visitor and GP or Practice nurse are notified of:
- vaccine administration at birth
- the requirement for the second vaccine at 4 weeks and completion of selective immunisation schedule
- complete:
- PHE hepatitis B in pregnancy maternal and paediatric checklist
- PHE IDPS Integrated screening outcomes surveillance service (ISOSS) hepatitis B database (from April 2021)
Women presenting without screening results
There should be a process in place to inform the screening team of a woman presenting in labour or as an in-patient with no reliable laboratory evidence of screening results from a UKAS accredited screening laboratory. Where screening has not been done delivery suite or in-patient teams should:
- facilitate the offer and recommendation of screening as soon as possible to inform clinical care and prior to discharge from maternity services
- liaise directly with the laboratory to ensure they have the necessary clinical information to inform prompt analyses
- ensure all results are obtained, reported and managed appropriately
In the event of a woman presenting on delivery suite where the hepatitis B status of the mother is not known, every effort should be made to test the mother to ascertain her hepatitis B status. If the mother’s hepatitis B status is unknown, vaccine alone should be given as per the Green Book recommendations.
HBIG is only indicated for the infant (in addition to vaccine) in situations where the mother is known to be hepatitis B infected but viral load or HBV markers of infectivity for this pregnancy are absent or inconclusive. (See Green Book for details). In these circumstances, an emergency issue of HBIG can be requested.
HBIG
HBIG provides passive immunity and is used after exposure to give rapid, immediate, but temporary protection until hepatitis B vaccine becomes effective.
Ordering and delivery of HBIG and hepatitis B delivery suite box
- HBIG distribution is coordinated by the PHE Hepatitis B Infant Coordinator in the Immunisation Division at Colindale – email: phe.hepatitisbbabies@nhs.net (from @nhs.net email addresses only as identifiable information)
- where HBIG is indicated it should be requested by sending a completed Hepatitis B Immunoglobulin issue form to the Hepatitis B Infant Coordinator using the contact details on the form
- the HBIG request form should be signed by a GMC registered doctor responsible for their patient as per MHRA regulations
- HBIG is issued for individual infants and should only be used for the infant named on the paperwork
- on receipt of the HBIG request form, the PHE Infant Coordinator will send an acknowledgment of receipt to the sender
- if there are multiple pregnancies, the antenatal screening coordinator should complete a form to request HBIG and a hepatitis B delivery suite box for each expected baby
Delivery and receipt of HBIG and hepatitis B delivery suite box
The request for HBIG will prompt delivery to the screening coordinator of the PHE ‘hepatitis B delivery suite box’ containing instructions for HBIG or vaccination, maternal serology sample and neonatal HBV DBS.
HBIG will be delivered by a logistics company in cold chain to the hospital pharmacy department approximately 7 weeks prior to the EDD. The HBIG pack will consist of:
- the HBIG vial
- a delivery note which quotes ‘PHE Ref No: XXXX’
- an information leaflet for pharmacy which states the HBIG has been issued for a ‘named baby’
The screening coordinator is responsible for ‘matching up’ the named baby HBIG vial from pharmacy with the named baby hepatitis B delivery suite box and ensure these are stored securely according to local arrangements so that they are available for that named baby at all hours of the day to the delivery suite team. The storage location of the HBIG and delivery suite box should be documented in the maternal notes.
Storage of HBIG
- HBIG is an MHRA regulated blood product, requiring cold chain, and should be tracked and stored accordingly
- HBIG should be stored in a refrigerator between 2°C and 8°C
- lost or misplaced HBIG is a common cause of delays or failure to administer the recommended prophylaxis. To minimise the risk of loss of the product there should be an agreed local arrangement for a single, secure, specific location where HBIG will be stored in the receiving trust, with 24/7 hours access
- the location of the HBIG should be recorded in the mother’s notes and/or the birth plan. The screening team should be aware of and record the location of HBIG
- while cold chain should be maintained, the manufacturers’ product information states that HBIG is stable at ambient temperatures for up to one week, so check with your pharmacy and/or Colindale before disposing of any HBIG that has been out of the cold chain for a short period of time (for example, if transferred to another trust with the mother)
Emergency supply of HBIG
If HBIG has not been ordered for the baby, then this can be requested from PHE Immunisation Division, Colindale:
During working hours:
By contacting the Hepatitis B Infant Coordinator at Colindale on 0330 1281 020 and select option 2 and send an accompanying email with the completed Hepatitis B Immunoglobulin issue form to phe.hepatitisbbabies@nhs.net (from @nhs.net email addresses only as the request will contain patient identifiable information)
Out of hours:
HBIG may be requested via the PHE National Infection Service Colindale Duty Doctor on 020 8200 4400
- HBIG may be requested via the PHE National Infection Service Colindale Duty Doctor on 020 8200 4400
- HBIG orders in the evening will generally be deferred to the next morning
- HBIG orders on weekends and bank holidays will only be accepted between 8am and noon for delivery that day or the following afternoon, following a risk assessment by the Colindale Duty Doctor
- requests to issue immunoglobulin at other times will only be considered where there is an immediate threat to life which is unlikely for hepatitis B
- alternatively, HBIG may be collected from the nearest issuing centre after a completed request form has been received by the duty doctor can provide the contact details following risk assessment
- if PHE duty doctor issues HBIG, it will be dispatched from a logistics company which holds stock of immunoglobulin on behalf of PHE
- Colindale no longer holds stock of immunoglobulin so a courier collection is no longer possible
- if courier collection of HBIG is required from a local stockholder, it is the responsibility of the Trust or requester to organise courier collection using an NHS approved courier service
In all emergency issues:
- the HBIG only will be packaged and sent or collected. PHE will not send out a hep B delivery suite box with surveillance blood sample kits as there is no expectation for these surveillance blood samples to be taken in unplanned deliveries
In all emergency issues:
- the completed Hepatitis B Immunoglobulin issue form, with the birth notification section completed if the baby has already been born, should be sent to the PHE Hepatitis B Infant Coordinator
Vaccine administration should not be delayed while organising HBIG:
- vaccine should be obtained from hospital pharmacies, not PHE
Low birthweight babies
Response to hepatitis B vaccine is lower in pre-term, low-birth weight babies because of immaturity of their immune system. It is essential that premature infants receive the recommended doses of hepatitis B vaccine, and (if ≤1500g) HBIG at birth even if the mother is of low infectivity risk, in accordance with the immunisation schedule to ensure optimal protection for these infants.
See above: Emergency supply of HBIG.
There is no expectation that pre-term low-birth weight babies that require emergency HBIG issues would have the neonatal birth DBS sample and maternal taken, regardless of the mother’s infectivity risk.
Multiple pregnancies
HBIG will be required for each individual infant. For multiple pregnancies complete a request form for each infant to ensure that the correct amount of HBIG is available.
Pregnancy loss and transfer of care provider
- the antenatal screening coordinator should inform the PHE Hepatitis B Infant Coordinator at Colindale of all women who subsequently miscarry or end their pregnancy after HBIG has been requested
- if a woman transfers her care to another provider prior to HBIG receipt the screening coordinator should notify Colindale of transfer and new trust if known. The new receiving trust should ensure HBIG is ordered for the woman by contacting Colindale
- if a woman transfers her care to another provider after the trust has received and stored the HBIG, as a prescribed medicine for the individual baby, arrangements should be made by the trust to transfer the named HBIG (including all vials for a multiple pregnancy) to the receiving hospital prior to delivery if the trust is known. Failure to do so will delay the administration of the product and may require an emergency replacement of HBIG to be issued
- if transfer of HBIG does not occur, the receiving hospital will have to contact the Hepatitis B Infant Coordinator at PHE Colindale to arrange for a replacement to be issued. See above: Emergency supply of HBIG.
Unused HBIG
Unopened vials that are not going to be used for a named baby (for example, due to pregnancy loss) should be returned to PHE Colindale. The product should not be retained for use on another infant without permission and notification of PHE Colindale. Any opened and partially used HBIG vial should be discarded.
Handover of care
The success of the combined screening and immunisation pathways is dependent on efficient and timely communication and handover of care from antenatal and maternity service providers in secondary care to practice nurses, GPs, CHIS and health visitor services in primary care.
From a programme delivery and outcomes perspective, the handover is critical in ensuring that the 4-week vaccine dose is given on time to the infant. Routine childhood immunisations are administered from 8 weeks of age. As the dose of hepatitis B vaccine due at 4 weeks of age is not part of the routine schedule, the infant may miss a dose if an appointment is not made for the infant to attend primary care specifically for this dose.
It is essential that the infant receives the birth and 4-week doses at the recommended age to ensure optimal benefit from them. Any missed or delayed doses may impact on the effectiveness of immunisation in preventing the infant from becoming infected with HBV.
From a patient safety, equity and experience perspective, a smooth handover is essential to ensure that mothers and their infants complete the care pathway. This group are often from migrant populations with poorer access to care and possibly less able to advocate for themselves.
Clear roles and responsibilities are needed for handover. Staff whose role it is to handover should do so and must ensure cover is in place when they are not available. If staff are in any doubt whether handover has been done, and it is not clearly documented, it is better to check, rather than risk delay to the actions needed for the baby.
For a seamless transition of care, there needs to be a designated person(s) to ensure:
- a robust process is in place so that the infant is registered with a GP in time for the 4-week immunisation to be scheduled and the vaccine ordered
- a clear and reliable process of handover throughout the care pathway
- handover of care and subsequent vaccination has been completed
Pathway points, mechanisms and persons responsible for handover to primary care services identified in the pathway are:
- the screening coordinator or team antenatally and after the birth of the baby informing the GP, health visitor, community midwife and CHRD (Child Health Records Department) or CHIS
- the community midwife and health visitor to supporting the mother in registering the infant with a GP (especially if noted as vulnerable and if there are barriers to effective communication)
- the CHRD or CHIS sending reminders to GP to schedule vaccinations
- the mother when registering baby at GP for 4-week dose by showing the infant’s Red Book and patient leaflet on hepatitis B immunisation
- in line with PHE commissioning guidance, health visitors should use their mandated and any additional visits as an opportunity to check that immunisations have been given or are scheduled
- if doses are missed or delayed, the health visitor or other relevant health professional should discuss the reasons why with the parent(s) and liaise with the infant’s GP to ensure immunisation takes place as soon as possible. Guidance is available on GOV.UK for healthcare professionals
Health visitors at the new baby review at 10 to 14 days should check that the baby is registered with a GP and arrangements are in place for the 4-week dose.
In handover communications during pregnancy, key messages to be communicated are:
- the pregnant woman has been screened and found to be have HBV infection
- her newborn infant will require urgent post exposure vaccination starting at birth (+/-HBIG if mother is of higher risk of infectivity) to prevent chronic infection because of exposure to HBV at the time of birth (see Appendix 2)
In handover communications after delivery, the key messages to be communicated are:
- the baby was born to a HBV infected mother
- the infant has had a birth dose of vaccine (+/- HBIG)
- timely vaccination of the baby is critical; a dose of monovalent hepatitis B vaccine needs to be given at 4 weeks; any delay in vaccination will increase the chances of the baby developing HBV infection
- the mother has been advised to register her infant at the GP practice as soon as possible after discharge to ensure the 4-week dose is given on time
- subsequent doses of hepatitis B vaccine should be given via a combination vaccine in the routine childhood programme at 8, 12, 16 weeks and with a final 12-month monovalent dose
- the infant needs to be tested to exclude HBV infection at one year old, preferably by a dried blood spot sample (via a heel prick)
Maternal and neonatal notification letter templates are available for screening coordinators and delivery suite teams to send to the GPs following the discussion with mother of her hepatitis B status at the screen positive appointment and after the birth of the baby and administration of vaccine +/- HBIG.
Timely vaccination of the baby is critical, any delay will increase the chances of the baby developing HBV infection.
Birth and GP registration
Registering the birth
All births in England, Wales and Northern Ireland must be registered within 42 days of the infant being born:
- all maternity providers should have local arrangements in place to support the parents to register the baby’s birth promptly
- parents should be advised to register the birth as soon as possible at the local register office for the area where the baby was born
- contact details for local registry offices are found at: www.gov.uk/register-offices.
Registering the infant with a GP
Prompt registration of the infant after birth with a GP practice is important to ensure the infant receives the 4-week dose of hepatitis B vaccine and subsequent immunisations are received on time:
- advise the mother to register with a local GP, if she is not currently registered
- following the birth, advise mother to register her infant immediately with a GP
- if there are concerns about access to GP registration, this should be discussed within the MDT and this should include her health visitor
- the nearest GPs to the mother’s residence may be found here: www.nhs.uk/Service-Search/GP/LocationSearch/4
- resources are available to support the discussions with the woman and her family on GP registration
Parents or guardians can register a baby at a practice by completing and presenting form FP58 which is issued at the same time as a birth certificate. However, this is not required, and the Red Book and completed GMS1 form and babies NHS number (given by the maternity unit at birth) should be sufficient.
Some GP practices may ask for proof of identity for the parent. This may be used to check the patient details match with the information held on the NHS central patient registry and that their previous medical notes are passed on to the new practice.
A patient should not be refused registration because they do not have proof of address or personal identification at hand. This also applies if the patient is an asylum seeker, refugee, a homeless patient or an overseas visitor, whether lawfully in the UK or not. In an emergency, temporary registration can be done to avoid missed or delayed immunisations. Information on temporary registration is available.
Eligibility for NHS treatment
The diagnosis and treatment of viral hepatitis is included in the list of services exempt from charges irrespective of residency and status, including asylum seekers, refugees and their dependants. In addition, failed asylum seekers are exempt for charges for maternity care as well as diagnosis and treatment of communicable diseases.
These mothers and their infants should be treated according to the clinical guidelines and HBIG, and vaccination ordered and prescribed accordingly.
Further information on NHS entitlements and immunisation for migrants.
The selective neonatal hepatitis B immunisation pathway
The aim of the post-exposure hepatitis B immunisation programme is to prevent infants acquiring the hepatitis B virus from their mothers’ blood and body fluids to which they are exposed during birth. Timely completion of the vaccine course is required for full protection.
As commissioner of the Section 7a programmes, NHS England and Improvement (NHSE/I) and the Screening and Immunisation Teams (SITs) and the Screening and Immunisation Leads (SILs) embedded in NHSE/I, are responsible for ensuring arrangements are in place for the provision of the selective neonatal hepatitis B immunisation programme.
In most areas, the selective hepatitis B programme vaccinations given after the birth dose are administered in primary care, but a minority of areas have different arrangements, such as delivery of the vaccinations by acute or community paediatric services.
The NHSE SIT/SIL should ensure that:
- arrangements for scheduling and delivering the vaccine are fit for purpose and should regularly audit their processes and impact on uptake of vaccine
- arrangements for scheduling are set out in a local SOP which specifies the geographical area covered, the roles and responsibilities for contacts, and the actions to be taken when the vaccine has been delayed or missed, and serious incident escalation if transmission resulting in chronic infection in the infant occurs. This will require liaison with Primary Care and CCGs at regional and national level
Selective neonatal and routine infant hepatitis B immunisation schedule
Babies born to mothers who has screened positive for HBV in pregnancy, or whose mothers have acute hepatitis B infection in pregnancy, are offered an accelerated course of hepatitis B immunisation starting at birth and continuing as part of the routine childhood immunisation programme with hexavalent vaccine.
For this reason, timely administration of all doses of vaccine (+/-HBIG at birth if mother is assessed as higher infectivity), is vital in preventing the infant becoming infected with hepatitis B:
- the first dose of monovalent hepatitis B vaccine (+/-HBIG) should be given in hospital no later than 24 hours after birth
- the second dose of monovalent hepatitis B vaccine is given at 4-weeks of age
- the hexavalent vaccine (DTaP/IPV/Hib/HepB), (currently given as Infanrix hexa), including protection against hepatitis B is given at 8, 12 and 16 weeks of age as part of the routine childhood schedule
- a final dose of monovalent hepatitis B vaccine is offered at 12 months old along with a blood test (for HBsAg and anti-HBc) to ascertain if the baby has become infected with hepatitis B virus.
The schedule is detailed in the Green Book and summarised in Table 9 below.
The mother’s hepatitis B virus status and all doses of monovalent and combination hepatitis B vaccines that are administered to the infant must be recorded in the relevant pages of the Personal Child Health Record (PCHR) known as the ‘Red Book’, entered on the GP system, and reported to the local CHIS or CHRD.
This acts as a central record of an infant’s immunisation history and facilitates estimating vaccine uptake locally and nationally which are in turn used to evaluate effectiveness, impact and quality of the immunisation programme.
Table 9: Hepatitis B immunisation schedule for routine childhood and selective neonatal immunisation programmes following the introduction of hexavalent hepatitis B-containing vaccine (adapted from Green Book)
| Age | Routine childhoodprogramme | Babies born to hepatitis infected mothers |
|---|---|---|
| Birth | Monovalent HepB | |
| 4 weeks | Monovalent HepB | |
| 8 weeks | DTaP/IPV/Hib/HepB | DTaP/IPV/Hib/HepB |
| 12 weeks | DTaP/IPV/Hib/HepB | DTaP/IPV/Hib/HepB |
| 16 weeks | DTaP/IPV/Hib/HepB | DTaP/IPV/Hib/HepB |
| 12 Months | * | Monovalent HepB Test for HBsAg |
| *Give the recommended non-hepatitis B containing vaccines as per the routine schedule |
Payment for administration of hepatitis B vaccines
The baby’s GP is responsible for administering hepatitis B vaccines. There is provision in the General Medical Services Statement of Financial Entitlements (Amendment) Directions 2014 section 14B and amendment number 2 (2017), for general practices to administer the following:
- the first dose of monovalent vaccine (if not already given in hospital)
- the second dose (at 4 weeks)
- the dose at one year
The General Medical Services Statement of Financial Entitlements (Amendment) Directions 2018 Annexe I makes provision for general practices to administer DTaP/IPV/Hib/HepB vaccine at 8, 12 and 16 weeks of age.
Scheduling immunisation appointments
Scheduling vaccinations is known to improve uptake. The population eligible for the HBV neonatal selective programme is particularly likely to benefit from scheduling and reminders because of their sociodemographic characteristics, with frequent language barriers.
Having the child’s status as infant of a hepatitis B positive mother recorded on their CHIS record will ensure this status transfers with the infant if they move between areas. Different models of care provision exist for implementing immunisation programmes.
After the birth dose in maternity care, subsequent vaccine doses are generally administered in the primary care setting, and occasionally in local paediatric services.
CHRD and CHIS primarily schedule routine rather than selective immunisation appointments and provide local vaccine coverage data. Whilst CHRD or CHIS may schedule the 8, 12 and 16-week doses of hexavalent hepatitis B containing vaccines, CHRD or CHIS may also send prompts to remind the GP to schedule the appointments for monovalent doses of hepatitis B at 4 weeks and 12 months old with the patient rather than schedule the appointments themselves.
Those responsible for scheduling the vaccine (for example, CHIS) should communicate at an early stage with the practice to arrange the 4-week dose, and depending on local arrangements, either the CHIS or GP should contact the parent(s) to ensure they are aware of the appointment date and time. Process and systems in place should be set out in a locally developed protocol.
As the hepatitis B neonatal programme is post-exposure prophylaxis following birth, scheduling of the birth and 4-week dose should be counted from the date of birth, so the interval between the birth dose and 4-week dose may be reduced if the birth dose is given late. Maintaining a minimum interval of 4 weeks between doses is most important for the hexavalent vaccine doses to achieve optimal immune responses for the other antigens contained in the vaccine.
Actions for CHRD or CHIS
To support scheduling of the 4-week and 12-months dose and testing the CHRD or CHIS could (see Appendix 2)
- schedule a paper or email reminder to the practice when the baby is approaching 2 weeks old alerting them to arrange an appointment for the 4-week dose
- include in the text of the reminder that:
- the vaccination is post exposure treatment to prevent chronic infection, liver disease and cancer so it is important that vaccine is given on time;
- the practice can claim reimbursement for the dose from NHS Business Services Authority using form FP43
- enclose or attach to the reminder the aide memoire for primary care staff
- schedule a paper/email reminder to the practice when the infant is 11 months old that they need to arrange an appointment for the 12-months dose and blood test, preferably by DBS, to exclude infection
- include in the text of the reminder that:
- the priority with the blood test is to exclude hepatitis B virus infection (rather than check for immunity);
- DBS sample by a heel-prick is strongly recommended as the preferred means of getting a blood sample in the practice
- there is a webpage and video on taking a DBS sample and insert the link
- provide local arrangements for the practice to obtain/order the DBS kits, *testing to exclude infection is crucial, particularly if there have been missed or delayed vaccine doses
- hepatitis B vaccine should be given at the same appointment as the DBS blood alongside other routine immunisations.
- if the DBS kit is not sent out by the CHRD or CHIS with the reminder, alert the local coordinator responsible for distributing the DBS kits that the practice needs to receive one that week.
Note: PHE Colindale Immunisation Division normally sends DBS kits in bulk to local coordinators (not direct to GPs) who are responsible for dispatching kits to practices as required); except for babies on higher risk follow up where the GP can request a DBS kit, PHE Colindale will not routinely send a kit directly to the GP.
Immunisation appointments before 12 months old
Actions required
The practice nurse or immuniser should:
- review the immunisation schedule with the mother/parent explaining how the hepatitis B immunisations fit in with the routine immunisation schedule (see table 2)
- vaccinate the child according the selective neonatal immunisation schedule set out in the Green Book (summarised in table 9)
- record the vaccine dose given (type, batch number) in the GP system and PCHR (Red Book)
- advise the mother or parent of subsequent doses and the importance of completing the schedule on time
- advise the mother or parent that their infant should have a blood test to test for HBV infection at 12 months old and how this will be done (venous sample or, preferably, DBS sample, preferably before vaccine is given (see also section on PHE DBS service)
- give the mother or parent the hepatitis B infant immunisation leaflet and advise her to book appointment dates for subsequent doses and the 12-months blood test (see Appendix 2)
- ensure that CHIS are informed that the dose has been given and subsequent doses need to be scheduled
- if not already done, arrange for testing and vaccination of sexual partners (of mother), close family and household contacts and refer to specialist if infected
- provide advice to mother on preventing hepatitis B virus spread to the family
- for high risk infants only: complete and return PHE hepatitis B infant surveillance request form for information on vaccine doses given
- ensure a DBS test kit is available for the 12-months appointment
Immunisation appointment at 12 months old
When the child is 12 months old, they should receive a final dose of monovalent hepatitis B vaccine at the same time as the other vaccines routinely given at this age (MMR, PCV, MenB and Hib/MenC).
Although hepatitis B vaccine is highly effective at preventing infection if started at birth, a very small number of infants may still acquire infection despite vaccination and immunoglobulin.
Testing children at 12 months is important for early assessment of their HBV infection status. Finding out if a child is infected at this point and referral for specialist care can reduce risk of long term liver disease and complications in later life. As most children who are infected will not have any clinical features, testing is the only way to identify them.
At the appointment, a sample from the child should be taken to test for HBV infection before vaccine is given to reduce the risk of a false positive result due to the hepatitis B vaccine antigen.
Infants should ideally have blood taken before the vaccine is administered
Whilst a venous sample is acceptable, obtaining a venous sample from a child may require referral to hospital and non-attendance may result in the baby’s hepatitis B virus infection status not being ascertained. DBS testing, which can be performed in primary care settings, provides a simple and easy alternative to venous blood sampling.
Actions required
The practice nurse or immuniser should:
- review the immunisation schedule with the mother/parent (table 2)
- take a heel prick DBS sample from the infant – preferably before hepatitis B vaccine is given (to avoid vaccine HBsAg being detected in the sample)
- vaccinate the child with the 12-months dose according the selective neonatal immunisation schedule set out in the Green Book (summarised in table 2) (see Appendix 2)
- give other infant vaccines recommended in the routine immunisation schedule
- record the vaccine doses given (type, batch number) in the GP system and PCHR (Red Book)
- advise the mother or parent that her infant has now completed the immunisation schedule for hepatitis B
- ensure that CHIS or CHRD are informed that the dose has been given
- advise mother how and when the results will be communicated back to her
- complete and return PHE hepatitis B infant surveillance laboratory request form, including the information on vaccine doses given
PHE DBS testing service
The preferred sample at 12 months testing is a DBS sample (heel-prick) as this can be done in primary care and so reduces non-attendance and loss of follow up.
PHE data suggests that the proportion of infants tested at 12 months is sub-optimal due to difficulties in obtaining venous blood samples in primary care. This places these infants at an increased risk of long term complications if their infections are not recognised and managed early on.
The DBS kit for 12 months testing provided by PHE Colindale includes a single-use safety lancet, suitable for use with infants aged 6 to 24 months, to prick the heel of the infant which allows several drops of blood to be applied to a filter paper. The blood spots should fill the circles on the filter paper. The kit and lab request form look very different to those for the birth DBS test and will be distributed to primary care not hospital teams.
Simple standard infection control precautions prevent any risk of cross-infection. The blood should be allowed to air dry onto the filter paper so it does not smudge or make the sample inadequate and it is safe for posting to the laboratory.
DBS testing provides a simple, safe and easy way to test the baby at 12 months in primary care
The DBS sample will be tested for HBsAg and anti-HBc (core-antibody). The DBS assay currently cannot test for antibody response to vaccination (anti-HBs). However, testing for infection (HBsAg) is the priority over testing for immunity as the major risk of transmission is at the time of birth, and because the response rate is high in those who escape infection. Many children will also be boosted by the vaccine given at the same time as the test is taken. Information about accessing the PHE national DBS testing service, including training materials and a video on how to take the sample is available at the PHE webpage on hepatitis B DBS testing.
Management of 12-month HBV test results
PHE Colindale will return DBS test results to the GP (or other sender) with electronic or paper copy to the HPT and SIT (or other local DBS coordinator) within about 2 weeks of receipt of sample. The DBS results report will have a commentary on what actions are necessary. Venous sample results from local phlebotomy services may take longer.
If the infant is found to be hepatitis B surface antigen (HBsAg) positive at 12 months, this indicates that the infant has acquired hepatitis B virus infection despite immunisation.
Some laboratory reports, such as DBS from Colindale, may also report hepatitis B core antibody (anti-HBc) results. Presence of anti-HBc can indicate past exposure or maternal antibodies, depending on the levels, but it does not indicate current infection on its own. Hepatitis B surface antigen (HBsAg) must be present to indicate the baby is currently infected. Confirmatory venous sample testing should be done on referral to a specialist.
Actions required
- note that the 12-months DBS result is a definitive result on the infant’s HBV infection status (and should not be confused with the DBS testing at birth which is collected for surveillance purposes)
- inform mother of the infant’s 12-months test result
- if infant not infected: inform parents and advise no further actions for the infant
- if infant infected:
- counsel parents in person and provide a factsheet on hepatitis B
- refer infant to a paediatric liver specialist for confirmation and further management record infant’s 12-months test result (positive or negative) in the GP system and ensure CHIS or CHRD is informed
- complete and return the PHE hepatitis B infant surveillance request form for the 12-months test result and information on any missing vaccine doses
- if not already done, arrange for testing and vaccination of sexual partners (of mother), close family and household contacts, and refer to specialist care if infected.
- If testing was not done by DBS at PHE Colindale, report local laboratory results to PHE by returning the form that will be sent by PHE to the infant’s practice when the infant reaches 12 months old (see Appendix 2)
Any chronic hepatitis B infection identified in an infant born to a hepatitis B infected mother should be escalated to the SIT and HPT as an incident and prompt an investigation. PHE NIS Colindale (Immunisation and Countermeasures Division and BBVU) and IDPS programme should be informed and provide input into the investigation.
This investigation into why transmission to the infant occurred should aim to identify avoidable reasons, issues with the pathway and learning points so that improvements can be made to prevent future transmissions as far as possible.
Special situations and scenarios
Missed or delayed doses of vaccine
Screening and Immunisation Teams (SITs) should have arrangements in place to monitor and follow up late and missed vaccine doses and 12-months testing. These follow-up arrangements will usually be via the CHIS or CHRD to ensure the information follows the child if they move area. Missed or delayed doses of hepatitis B containing vaccines may be identified by primary care staff or CHIS or CHRD. Delayed or missed doses should be recorded, escalated and investigated according to local policy, and where appropriate, reported to the relevant SIT.
An investigation should be carried out to identify any possible issues with the pathway and avoidable causal factors to facilitate learning and prevent reoccurrence. The investigation should be an opportunity to improve service delivery and share learning.
CHRD and commissioners should have a protocol or SOP in place for managing missed or delayed doses, including a ‘watch list’ for infants whose doses were late or missed with enhanced follow up at 12 months to ensure testing for chronic infection occurs.
Actions for practice nurse or immuniser
Once a missed or delayed dose is identified:
- give the dose immediately and resume the immunisation schedule
- for the 4-week and 12-months doses, monovalent paediatric hepatitis B vaccine is preferred but alternative products can be used to avoid delay, with the following order of preference:
- hepatitis B paediatric monovalent vaccine (Engerix-B paediatric or HBvaxPRO Paediatric)
- hepatitis B adult monovalent vaccine (Engerix-B and HBvaxPRO).
- a combined hepatitis A and B vaccine (for example, Twinrix Paediatric)
- if a birth dose has been given but the 4-week dose is 2 or more weeks late, the 8-week dose of hexavalent vaccine can be brought forward and given instead of a late monovalent hepatitis B vaccine dose, as the hexavalent vaccine is licensed from 6 weeks of age.
- a 4-week interval should be maintained between the remaining hexavalent doses to ensure adequate immune response to the other vaccine components. This means that the subsequent infant immunisations may be given slightly earlier. Further information is available in the Hexavalent combination vaccine: selective programme guidance
- if at the 12-months or subsequent visits, it is noted that no blood or DBS test has been arranged, this should be arranged ASAP, preferably using DBS kit, and the results reported to PHE.
- any chronic hepatitis B infection diagnosed in an infant born to a hepatitis B infected mother should be escalated to the SIT and PHE HPT as a serious incident and prompt an investigation, with input from PHE Colindale.
Actions for CHIS or CHRD
If the birth dose is given more than 24 hours after birth, this is considered a late dose from a programme performance perspective. For subsequent doses, if given 2 or more weeks after the due date (based on time since birth (not since last dose), this should be considered late and prompt further action:
- late doses should prompt the CHIS or CHRD to follow up with the GP to satisfy themselves that:
- reasonable exceptions exist for no dose being given such as patient moved abroad, has not attended multiple appointments
- sufficient steps have been taken by the practice staff, including by health visitors, to contact and engage the parents
- any infants with delayed or missed doses are flagged on the GP system to ensure additional efforts are made to ensure subsequent doses are given and 12-months testing done
- alert and escalate missed or delayed doses to the NHSE/I SIT if:
- no exceptions reported by the practice
- no mitigating factors reported by the practice
- no feedback from the practice
- the parents/guardian decline vaccination for the baby (see also section on vaccine decline)
- flag infants to a watch list for additional reminders for subsequent doses and test at 12 months to exclude infection. Infants should go on this watch list even if there are mitigating factors for non-vaccination as it is still in the best interests of the child to be tested at a year and referred for management if infected
- if there is no record of the 12-months blood/DBS test and no result reported by 15 months, issue a reminder to the GP and arrange for a DBS kit to be re-sent to the practice.
Investigation of incidents
Where missed or delayed doses are escalated as incidents, investigation by the SIT or Screening Quality Assurance Service team, as appropriate, should examine root causes. It is good practice to audit incidents regularly looking for common underlying factors between incidents in the area such as training, availability of DBS kits, access to information etc and should include a strategic action plan to address these. This investigation and remediation should take place in response to errors – an adverse outcome should not be required to instigate the quality improvement work.
If chronic HBV infection occurs in an infant born to a hepatitis B infected mother, this should be considered a serious incident as it is an adverse outcome with significant potential harm for the infant.
An investigation led by the SIT with PHE HPT, Immunisation Division and BBVU at PHE Colindale and IDSP input should examine root causes to establish whether hepatitis B infection was avoidable, whether management, design (system, pathway), training, personnel and processes were contributing factors, and how these issues should be remedied and learning embedded to prevent future incidents.
Further guidance is available in NHS England’s Serious Incident Framework and PHE Managing safety incidents in the NHS screening programmes guidance
Management of close family contacts of a hepatitis B infected pregnant woman
Sexual partners of infected women are most at risk of HBV transmission, and they and close family and household contacts should be vaccinated and tested as per Green Book guidance.
Actions required
The screening team should inform the GP of the mother so that the family contacts can be tested and vaccinated appropriately:
- advice given to the mother and her partner(s) that protection such as condoms should be used until he is immunised or found to be infected
- all close family /household and sexual contacts should have blood taken at the time of the first dose of vaccine to determine if they have already been infected
- contacts shown to be HBsAg, anti-HBs or anti-HBc positive do not require further immunisation; otherwise a hepatitis B immunisation schedule should be followed
- post vaccination testing for immune response is not required in healthy contacts
- contacts shown to be HBsAg positive – that is, have evidence of current hepatitis B infection should be referred for specialist management
Management of a baby whose mother is hepatitis B negative but another household member is hepatitis B infected
Newborn infants born to a hepatitis B negative woman but known to be going home to a household with another hepatitis B infected person may be at immediate risk of exposure to hepatitis B virus. In these situations, a monovalent dose of hepatitis B vaccine can be offered before discharge from hospital to provide some protection before routine immunisations begin. Infants should then continue the routine childhood schedule commencing at 8 weeks.
If infants have received the routine schedule and there has not been any known significant exposure to the infected household member then they do not require testing at 12 months of age because they have not been exposed vertically.
Management of parental decline of vaccine +/- HBIG for the baby
If the parent or legal guardian declines immunisation of their baby with vaccine and/or HBIG, there should be a process in place to ensure this refusal is identified as early as possible in pregnancy, recorded and escalated promptly to the MDT.
The reasons why parents decline vaccination include:
- stigma and anxiety that family and friends will find out about their hepatitis B status
- general concerns about vaccine safety, including possible refusal of routine programme
- specific concerns about hepatitis B vaccination in a newborn
- denial of their hepatitis B infection status or risk of vertical transmission to their infant
It is critical that conversations about immunisation of their newborn begin early on in pregnancy as soon as the screen positive result is communicated. Fears, worries or misunderstandings of the parents should be addressed, and information leaflets provided at every opportunity during the antenatal pathway when there is more time to have these discussions so that parents are fully counselled to make an informed decision in good time.
Most parents will accept vaccination when recommended by trusted and familiar professionals, often their GP, health visitor or midwife. The recommendation should be supported by clear and sensitive communication about the safety and effectiveness of the vaccine and the health risks to their baby if not immunised.
Multiple attempts should be made to give vaccine doses; the birth dose of vaccine +/- HBIG should be offered at every opportunity as HBIG can be given up to 7 days after exposure, and there is no limit to when vaccine can be given. The parents should be informed, however, that the effectiveness of vaccine and HBIG decreases dramatically as time after birth increases. If the mother will accept vaccine only, this should be given without delay.
When a parent refuses immunisation at birth, a meeting should be convened with the parents, other trusted professionals and senior clinical leads to understand the rationale for the decline; ensure the parents are fully appraised of the risks for the baby’s health and explore a solution to ensure the best outcome for the infant.
Timeliness in arranging the meetings is important as there is an imperative to act in the first 24 hours of life with diminishing benefits from immunisation as the days become weeks.
Discussions with senior clinicians, parents and their trusted professionals, should occur in a calm, quiet and private space, with written information and translation services available if necessary, to:
- allow the parents to explain their reasons for withholding consent for their infant to be immunised
- allow the clinical team with senior support to respond, explaining the importance of immunising their baby in that it dramatically reduces the high risk of her infant developing chronic infection, liver damage, cirrhosis and potentially liver cancer in later life (see section on Transmission)
- advise the parents that hepatitis B vaccination schedule starting at birth is ‘post exposure’ urgent treatment and may be ineffective if it is delayed. Note that this is very different to the routine childhood immunisations starting at 8 weeks where a short delay is less important because the routine vaccines mainly protect their child against future risks (pre-exposure treatment). For babies born to a hepatitis B infected mother, the infant will already have been exposed to hepatitis B during birth.
- assure the parents that the vaccine is very safe and effective when given at birth and HBIG (if indicated) provides additional rapid protection while the vaccine starts to work
- assure the parents of the confidentiality of the mother’s and the child’s care
- provide the parents with PHE’s leaflets on the selective neonatal immunisation programme to read and consider.
All discussions with parents and the outcomes should be fully documented in medical records. As this is a health protection issue, if the parents still decline, the local Health Protection Team can be involved to provide advice to the team and the parents and discuss whether escalation is required. The local NHSE/I Screening and Immunisation Team should also be notified as they have oversight of the delivery of the immunisation and screening programmes.
In some instances, continued refusal by the parents may invoke an MDT decision to referral to specialist services or referral via child safeguarding protocols to child social services and the legal team, as parental refusal could be considered to be contrary to the child’s health and wellbeing, indeed putting the child at significant risk of harm.
When there are competing ethical principles, parental autonomy versus the best interests of the infant, the level of risk is an important aspect of deciding whether or not to seek legal intervention (Basu Roy R. et al, 2020). A high risk of a severe outcome probably justifies intervention but if the risk is very low, whether the parents’ autonomy should be overruled is less clear. The question of what level of risk justifies legal action is debatable.
In the case of hepatitis B vertical transmission, the risk of chronic infection in the infant with a higher infectivity risk mother is very high (70 to 90%) and can be reduced dramatically to under 5% with vaccine and HBIG; the additional benefit from enforced immunisation (with both vaccine and HBIG) would appear to outweigh the concerns around infringement of parental autonomy.
In lower infectivity risk mothers where the risk of transmission is 5 to 40% and there is more uncertainty in the absolute risk of chronic infection and severe complications and risk reduction to the infant, the threshold for legal intervention to overrule the parents may be less clear-cut Basu Roy R. et al, 2020.
However, given the long-standing safety and effectiveness data for hep B vaccination, and the high probability of chronicity and risk of death from HBV-related cirrhosis and liver cancer, the threshold for intervention can still be reached Isaacs D, Kilham HA.et al, 2011.
Figure 3 is a schematic of the key elements in the management of parental refusal of vaccination, including considerations for escalation to social services and courts.
In Australia there have been 2 published reports of the courts authorising medical staff to immunise a child born to a hepatitis B infected mother where the parents refused. One with an HBeAg negative mother refusing vaccination and a second HBeAg positive Jehovah’s Witness mother who declined HBIG but accepted vaccination Isaacs D, Kilham HA.et al, 2011.
In the UK, there is case law from 2019 where a court judge ruled against the parents’ refusal to vaccinate and in favour of the infant completing the hepatitis B vaccination schedule. There are also at least 2 court judgements in recent years where it was ruled that it was in a child’s best interests to receive routine vaccinations (no risk of hepatitis B perinatal transmission) where the child was subject to a care order and /or a parent objected to vaccination. Precedent for courts overruling parental decisions on mother to child transmission prophylaxis exists in the HIV arena, where court orders have enforced post-natal anti-retroviral treatment of infants born to HIV positive mothers Wolf L, Lo B.et al, 2001.
Although the possibility of social services involvement and legal action may persuade parents to accept vaccine, it is always preferable to maintain trust and bring the parents along with the clinical team.
Despite all efforts, if immunisation with vaccine +/- HBIG at birth is declined and not mandated by the courts, this should be documented in the mother’s and baby’s notes, the Red Book and flagged with the GP and community midwife and Health Visitor team.
Vaccine appointments for subsequent hepatitis B doses should still be arranged, and the parents supported to attend them and accept vaccination for their child. The child should also be referred to local paediatric or paediatric infectious diseases services for follow-up to see if they did indeed acquire HBV either vertically, or through horizontal transmission within the home.
Figure 3: Schematic of managing parental refusal of HBV immunisations
Figure 3 Schematic of managing parental refusal of HBV immunisations
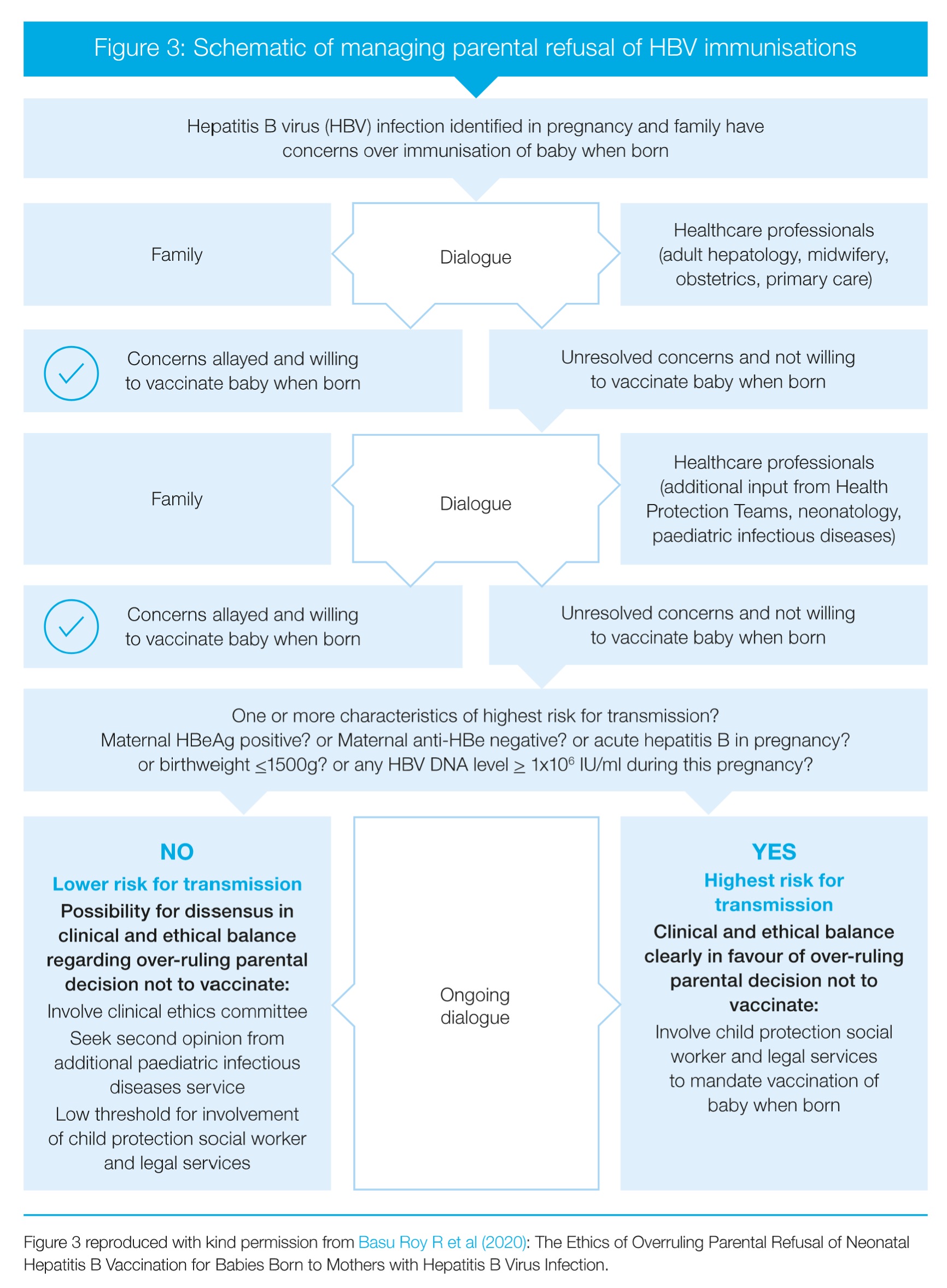{kind=link}
(Figure 3 reproduced with kind permission from Basu Roy R et al (2020) ‘The Ethics of Overruling Parental Refusal of Neonatal Hepatitis B Vaccination for Babies Born to Mothers with Hepatitis B Virus Infection’)
Appendix 1: Membership of project groups
PHE hepatitis B antenatal screening and neonatal immunisation pathway internal project group
| Chair | |
|---|---|
| Sharon Webb | Programme Manager, NHS Infectious Diseases in Pregnancy Screening |
| Dr Sema Mandal | Consultant Epidemiologist, Lead for Hepatitis, Immunisation and Countermeasures, PHE Colindale |
| Members | |
| Nigel Attah | Project Officer, IDPS/FASP, PHE Screening |
| Shirley Cole | Hepatitis B Babies Coordinator and Project Support, Immunisation and Countermeasures, PHE Colindale |
| Michelle Falconer | Immunisation Nurse Specialist, Immunisation and Countermeasures, PHE Colindale |
| David Green | Consultant Nurse, Immunisation and Countermeasures, PHE Colindale |
| Iain Hayden | Scientist (Epidemiology), Immunisation and Countermeasures, PHE Colindale |
| Dr Samreen Ijaz | Clinical Scientist, Head of BBV Unit, PHE Colindale |
| Peter Lamb | PH Specialist Registrar, PHE Colindale |
| Nadia Permalloo | Head of Screening Quality Assurance Development (Clinical)/Portfolio Lead ANNB Screening Programmes, PHE Screening |
| Patricia Schan | Clinical Project Advisor, IDPS Programme, PHE Screening |
| Tracey Smeulders | Hepatitis B 12 months DBS Coordinator, Immunisation and Countermeasures, PHE Colindale |
PHE Hepatitis B antenatal screening and neonatal immunisation pathway strategic group
| Chair | |
|---|---|
| Sharon Webb | Programme Manager, NHS Infectious Diseases in Pregnancy Screening |
| Dr Sema Mandal | Consultant Epidemiologist, Lead for Hepatitis, Immunisation and Countermeasures, PHE Colindale |
| Members | |
| Nigel Attah | Project Officer, IDPS/FASP, PHE Screening |
| Dr Heather Bailey | Epidemiologist ICH/Coordinator National Hepatitis B Audit, Institute of Child Health, GOSH, UCLH |
| Dr Ashley Brown | Consultant Hepatologist, Imperial College London |
| Joanne Caines | Clinical Nurse Specialist, Hepatology, University Hospitals of Birmingham |
| Shirley Cole | Hepatitis B Babies Coordinator and Project Support, Immunisation and Countermeasures, PHE Colindale |
| Margaret Costello | Specialist Midwife, London North West Healthcare NHS Trust |
| Helen Donovan | Professional Lead for Public Health, Royal College of Nursing |
| Michelle Falconer | Immunisation Nurse Specialist, Immunisation and Countermeasures, PHE Colindale |
| David Green | Consultant Nurse, Immunisation and Countermeasures, PHE Colindale |
| Catherine Heffernan | Principal Advisor Commissioning and Vaccinations Services, NHS London |
| Iain Hayden | Scientist (Epidemiology), Immunisation and Countermeasures, PHE Colindale |
| Dr Samreen Ijaz | Clinical Scientist, Head of BBV Unit, PHE Colindale |
| Dr Shamez Ladhani | Consultant in Paediatric Infectious Disease, St George’s Hospital NHST |
| Peter Lamb | Public Health Specialist Registrar, PHE Colindale |
| Chloe Leggat | Screening & Immunisation Coordinator, East Midlands South Health Protection Team |
| Clare Livingstone | Public Health Lead, Royal College of Midwives |
| Dr Alison Mackenzie | Consultant in Public Health Medicine – Screening and Immunisation Lead, PHE/NHS England South |
| Madeleine McMahon | National screening data and information manager, PHE Screening |
| Lorraine Martin | ANNB Projects & Implementation Officer, PHE Screening |
| Dr Miranda Mindlin | Consultant in communicable disease control, South London Health Protection Team, PHE |
| Dr Eleni Nastouli | Consultant Clinical Virologist, UCLH/Honorary Consultant in Paediatric Infectious Diseases at Great Ormond Street Hospital |
| Juliette Penney | Institute of Health Visiting |
| Nadia Permalloo | Head of Screening Quality Assurance Development (Clinical)/Portfolio Lead ANNB Screening Programmes/Chair, IDPS Laboratory Task Group, PHE |
| Pat Schan | Clinical Project Advisor, IDPS Programme, PHE Screening |
| Reisha Simmonds | Scientist (Epidemiology), Immunisation and Countermeasures, PHE Colindale |
| Tracey Smeulders | Hepatitis B 12 months DBS Coordinator, Immunisation and Countermeasures, PHE Colindale |
| Dr Judith Timms |
IDPS Laboratory Advisor/Deputy Director of Pathology Services, Coventry and Warwickshire |
Appendix 2: Supporting resources
Supporting guidance
World Health Organization Global hepatitis report, 2017
Hexavalent combination vaccine: selective programme guidance
Hepatitis B Immunoglobulin – when to use
NHS England Public health national service specifications
PHE Screening safety incident guidance
NHS England’s Serious Incident Framework
Inequalities PHE and NHS England priority
Immunisation against Infectious Disease: Green Book, chapter 18
PHE Hepatitis B immunisation pathway resources flyer
PHE Infectious Disease Strategy 2020 to 2025
Patient and professional resources
Template result letter after pregnancy loss
Migrant health and NHS entitlements
PHE hepatitis B in screening and immunisation maternal and paediatric checklist
PHE maternal and neonatal notification letter templates
PHE hepatitis B DBS testing service for infants
Hepatitis B immunoglobulin request form
Hepatitis B neonatal immunisation leaflet: protecting your baby against hepatitis B
Aide memoire on hepatitis B immunisation for primary care staff
Information webpages
IDPS Integrated Screening Outcomes Service
Immunisation of infants born to hepatitis B infected mothers
Hepatitis B infant DBS testing service
British Association for the Study of the Liver
British Viral Hepatitis Group (BVHG)
Appendix 3: Pathways
IDPS Programme
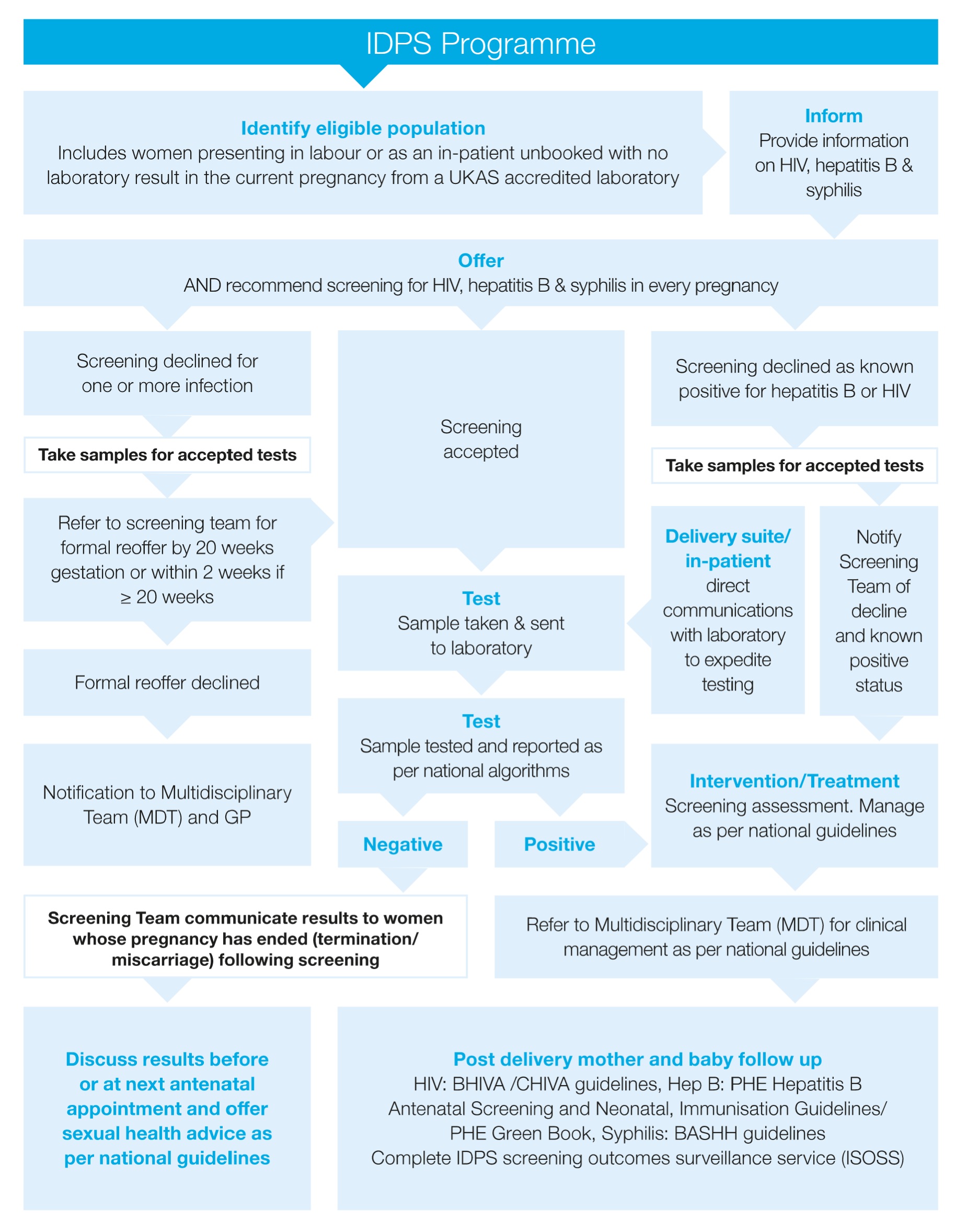{kind=link}
Flowcharts summarising the hepatitis B antenatal screening and selective neonatal immunisation pathways
Lower infectivity pregnancy pathway: Flowchart
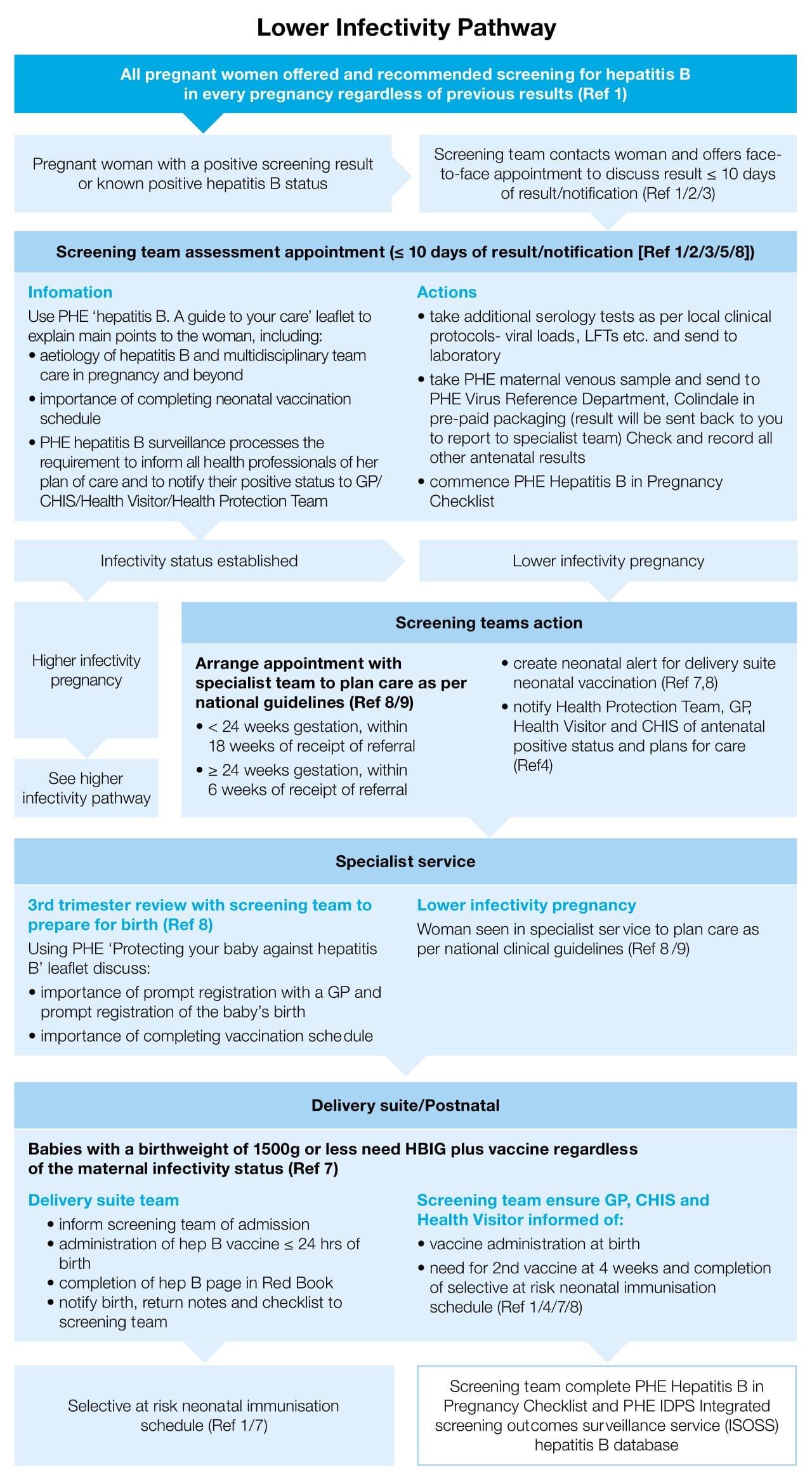{kind=link}
Higher infectivity pregnancy pathway: Flowchart
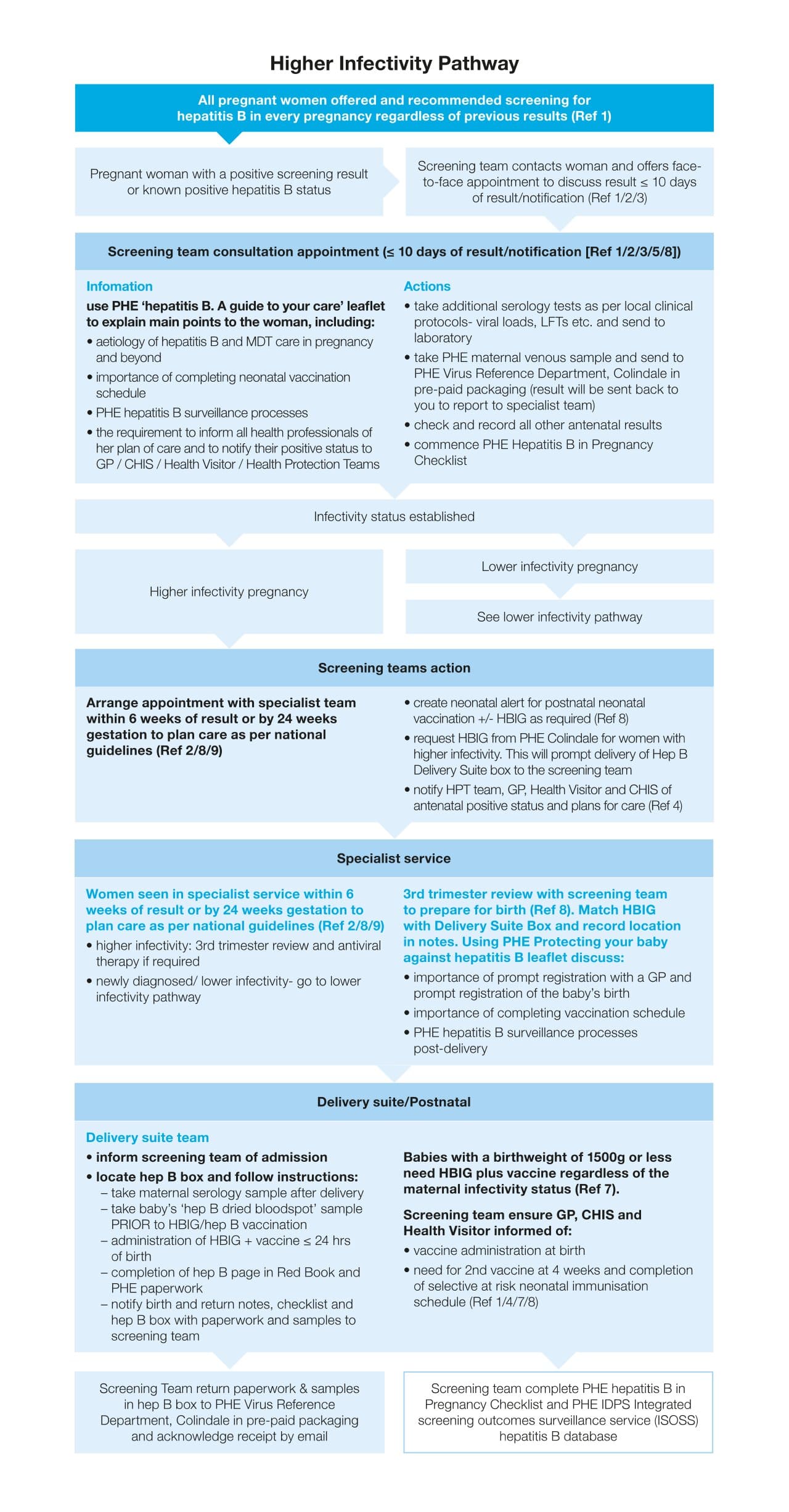{kind=link}
References
- NHS Service specifications No 1 and 15
- IDPS Programme Standards
- IDPS Screening Handbook
- Notification letter templates
- IDPS Laboratory Handbook
- IDPS Audit and Checks document
- PHE Green Book
- PHE Guidance on the hepatitis B antenatal screening and selective neonatal immunisation pathway
- Clinical Guidelines (BASL/BVHG)
- PHE Healthy Child Programme 0 to 19: Health Visitor service specifications
Flowchart summarising the neonatal post exposure immunisation schedule for infants born to women with hepatitis B
Live birth-baby born to a woman with hepatitis B: Flowchart
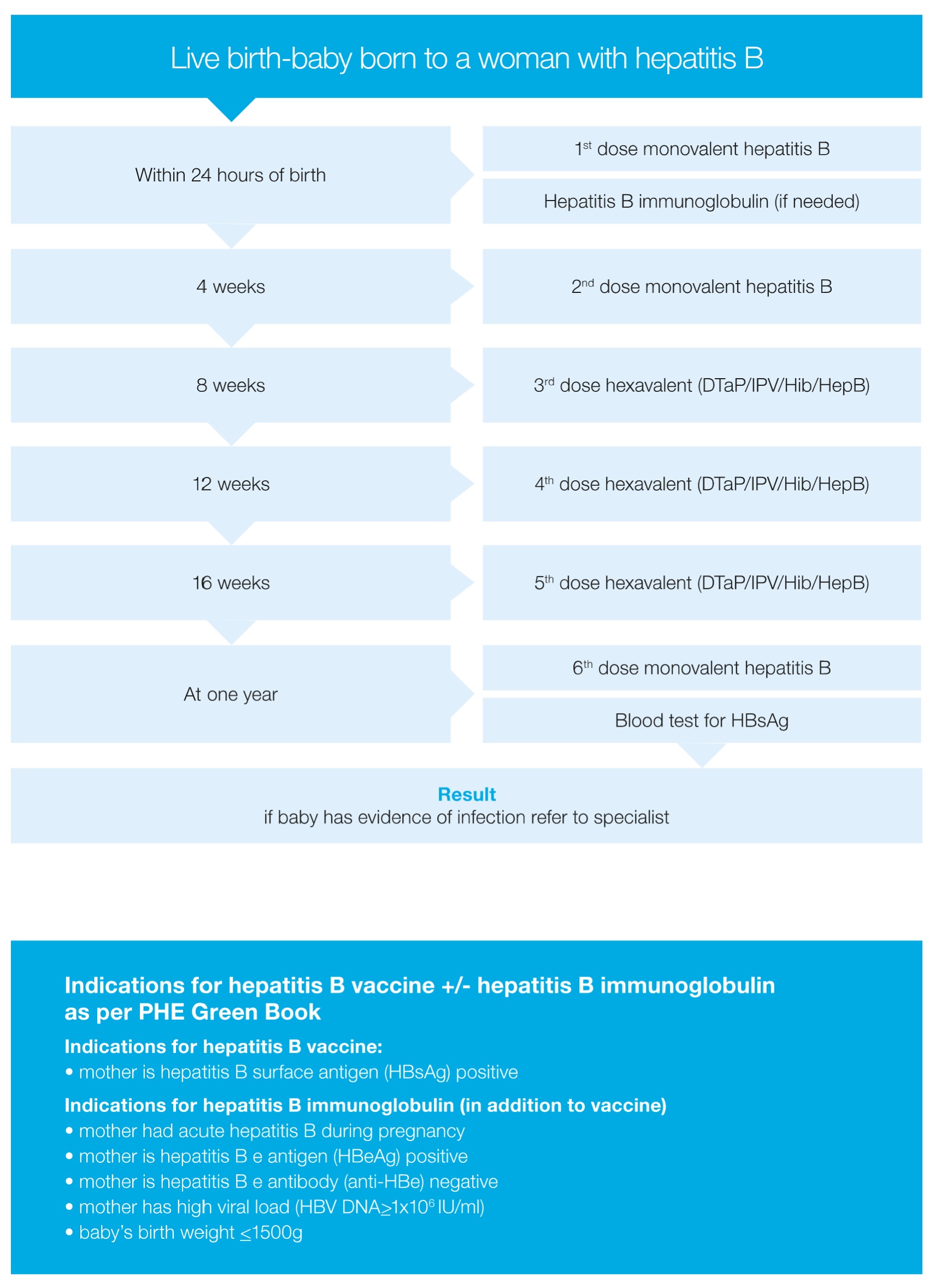{kind=link}
Indications for hepatitis B vaccine +/- hepatitis B immunoglobulin as per PHE Green Book
Indications for hepatitis B vaccine:
- mother is hepatitis B surface antigen (HBsAg) positive
Indications for hepatitis B immunoglobulin (in addition to vaccine):
- mother had acute hepatitis B during pregnancy
- mother is hepatitis B e antigen (HBeAg) positive
- mother is hepatitis B e antibody (anti-HBe) negative
- mother has high viral load (HBV DNA > 1 x 106 IU/ml)
- baby’s birth weight ≤ 1500g
Appendix 4: Legal permissions to collect personal information
PHE has been given responsibility by the Secretary of State for Health and Social Care to act to protect and improve the nation’s health and reduce health inequalities. To do this, the law on data protection allows us to use personal information. We are trained to use personal information and treat this in the strictest confidence, in compliance with the General Data Protection Regulation (GDPR) and the NHS Caldicott principles. Our staff have the same duty as other healthcare professionals to maintain confidentiality.
PHE IDPS programme and National Infection Service has legal permission to collect and process patient identifiable information without the need to seek consent from individual patients under Regulation 3 of the Health Service (Control of Patient Information) Regulations 2002.
The service also conforms to the requirements of the Data Protection Act (2018).
For queries or further information from healthcare professionals about information governance and data protection please contact:
The PHE Screening helpdesk at screening.helpdesk@nhs.net or the PHE immunisation clinical team at immunisation.lead@phe.gov.uk.