
Annual Report for 2020
Published 21 April 2021

© Crown copyright 2021
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/raib-annual-report-published-2021/annual-report-for-2020
Our Purpose: We independently investigate accidents to improve railway safety and inform the industry and the public.
1. Chief Inspector’s review of 2020
The coronavirus pandemic made 2020 a challenging and difficult year for all of us, and continues to do so. On the UK’s railways, reduced passenger traffic levels saw fewer trains running, but rail freight continued to play a vital part in sustaining the country’s economy. At RAIB, our job carried on, but we had to modify the way we worked as a consequence of the restrictions that have been a part of everyday life since March 2020.
At RAIB, we remember only too well the derailment of a Pendolino express train at Grayrigg in Cumbria in February 2007 that led to the death of one passenger and serious injuries to many others. Following that accident, the UK’s national railway network saw no other fatal train derailments or collisions for more than 13 years, a remarkable record. Sadly, the tragic accident at Carmont, Aberdeenshire, in which three people died, was a painful reminder that the risk of such accidents remains with us.
Unfortunately, 2020 saw three other fatal accidents on the operational railway, all of which are being investigated by RAIB (a fourth fatal accident at Eastleigh long welded rail depot on 30 November is outside RAIB’s scope). On 8 April 2020 a track worker died after being struck by a train at Roade, Northamptonshire, the third to die in this way in less than twelve months. The year also saw the launch of two RAIB investigations into the death of passengers on station platforms (Eden Park on 26 February and Waterloo Underground on 26 May). RAIB’s report into the first of these was published on 19 February 2021 (report 01/2021).
I am saddened to report that February 2021 saw the death of another track worker, this time at Surbiton in south-west London. This too will be the subject of a thorough RAIB investigation.
1.1 Safety of track workers
In the 2019 report I referred to RAIB’s investigation into the death of two track workers who were struck and killed by a train at Margam in July of that year. For their families, friends and those close to them this was a devastating loss.
Our report on the accident was published in November 2020 (report 11/2020). It identifies a number of underlying factors which I believe may also apply across the rail industry. These related to the following areas:
- implementation of safe work planning processes
- monitoring and supervision
- safety behaviours and leadership
- corporate culture
- change management
We made eleven recommendations to address these and the other factors that led to the accident.
The areas that need to be addressed to improve the safety of track workers have been repeatedly highlighted by 44 investigations carried out by RAIB over the last 14 years. The most obvious need is for smart and accurate planning to reduce the number of occasions that workers are on the track when trains are running, while also meeting the need for access to assets on an operational railway system. I believe it is essential that Network Rail addresses the fundamental requirements that have been highlighted by RAIB’s investigations over the years. These include developing leadership skills and involvement of the site team in the planning process, including the identification of site hazards and the local management of risk. There is also a need for better management of people who work on the track, including a higher standard of supervision and assurance, that will make sure correct working practices are in use, and identify areas for improvement. There is scope for greater use of technology to control access to the infrastructure, to provide warnings of approaching trains and to protect possession limits.
In recent years the industry has launched projects intended to make a real difference to track safety, but they have not always been successful. It is frustrating that the railway has been unable to carry people with it in its attempts to bring about real change. However, I am encouraged by the steps taken to address the issues so vividly highlighted by the dreadful events at Margam. I can see that the UK’s rail safety regulator, the Office of Rail and Road (ORR), and Network Rail, share a genuine determination to drive forward actions to make real and lasting improvements to the safety of the people who maintain our railway, as evidenced by the Improvement Notices served by ORR and the rapid establishment of an active and well-funded Safety Task Force.
However, commitment by those at the top is not enough, and engagement with those on the front line is vital. Track workers and their supervisors need to understand how the changes that are being made will benefit their own safety, while enabling them to do their important job effectively.
Our Safety Digests on near-miss incidents involving track workers at Kirtlebridge (safety digest 03/2020) and Leighton Buzzard (safety digest 05/2020), in which people only narrowly avoided being struck by trains travelling at more than one hundred miles an hour, illustrate that the railway has some considerable way to go. The lessons from the incidents are similar to those we identified in the Margam investigation, and reinforce the need for proper safety management, and in particular, assurance that good practice is actually being followed out on the track.
I continue to be hopeful that the industry will find a better way to maintain our railway safely and further reduce the risk to our colleagues who inspect, maintain and renew the infrastructure. We have come a long way since the days when fatal accidents involving track workers were a regular occurrence, yet they still happen. There is now a real sense that things must urgently change, and the railway needs clear thinking and decisive action. We can and must do better.
1.2 Depots and sidings
Sadly, the accident at Margam was not the only staff fatality that we reported on during 2020. A train driver died after being trapped when two trains were being coupled together at Tyseley depot in December 2019 (report 09/2020). This accident highlights how dangerous depots and sidings can be.
We found that the department within the train operating company responsible for managing traincrew and the department responsible for the servicing and maintenance of trains were not working well together. This meant that the company, as a whole, did not understand or sufficiently manage the risks posed to drivers who were working or walking in depots. The company was also not taking effective action to deal with unsafe behaviour in depots. Good safety management requires both an understanding of risk and spotting when things are not being done properly, and then doing something about it.
1.3 The safety of people getting on and off trains
We have continued to look closely at the safety of people getting on and off trains. At Eden Park, a visually impaired man fell from the edge of a station platform that had no tactile surface to indicate the closeness of the platform edge, just as a train pulled in, with fatal consequences. Our report, published on 19 February 2021 (report 01/2021), recommended that the rail industry introduces an improved process for considering when to install tactile surfaces at the edge of station platforms. It also recommended that Network Rail and the Department for Transport (in consultation with train operators) should develop and progress a time-bound programme to install tactile surfaces at those stations where they would give greatest safety benefit.
Quite rightly, the government and the rail industry have invested significant funds to improve the accessibility of the UK’s rail system. This report serves as a reminder of the importance of considering the safety of the visually impaired when doing so. It is good to see that tactile surfaces have now been installed at Eden Park as part of a wider installation programme in Kent and Sussex.
An investigation is still ongoing into the death of a passenger who fell under a tube train at Waterloo station in May 2020. Once again, this accident highlighted the risk to vulnerable passengers and the need to take them into account when assessing risk at the interface between trains and platforms. This is particularly important at those locations, such as Waterloo Underground station, where station infrastructure built more than 100 years ago features tightly curved tracks, which results in the gaps between train and platform being larger than is normally the case.
1.4 Freight wagon maintenance
The year 2020 also served as a reminder of the damage that can be caused by the derailment of a freight train carrying dangerous goods. At about 23:15 hrs on 26 August 2020 a train en-route from Robeston to Theale, conveying 25 tank wagons, each containing up to 75.5 tonnes of diesel or gas oil, derailed near Llangennech, in Carmarthenshire. The derailment and the subsequent damage to the wagons resulted in a significant spillage of fuel and a major fire. Local homes were evacuated and spilt fuel was observed to have reached the Afon Llwchwr/Loughor estuary, endangering local shell fisheries and sites of special scientific interest (SSSI). The area is within the Carmarthen Bay and Estuaries European marine site (EMS).
Subsequent examination of the site revealed that a total of 10 wagons, beginning with the third in the train, had derailed, and that around 330,000 litres of fuel had been spilt. Although RAIB’s investigation is ongoing, it is already clear that the derailment was caused by a malfunction of the braking system such that the wheels on the leading axle of the third wagon were no longer able to rotate.
In November, RAIB issued urgent safety advice (USA 02/2020) urging entities in charge of maintenance (ECMs) to review their system of inspection and maintenance for wagons that primarily carry dangerous goods, to ensure that they have appropriate arrangements in place to manage the safety risk associated with malfunction of the braking system.
RAIB has previously expressed concerns about the maintenance of freight wagons and their contribution to the risk of derailment. During 2020, RAIB’s investigations into the freight train derailments at Willesden High Level Junction (report 07/2020) and Wanstead Park (report 12/2020) both identified issues with the maintenance of freight wagons.
These and other recent RAIB investigations raise concerns about the extent to which the current regulations for freight wagon maintenance, as laid down in the Railways and Other Guided Transport Systems (Safety) Regulations, are being correctly applied. These regulations specify that the responsibility for any freight wagon’s maintenance falls to a certificated ECM. This entity is required to have a system of maintenance in place that allows vehicles to be safely maintained. Such a system must include instructions on the periodicity of certain examinations and renewals as well as arrangements for checking that others undertaking maintenance activities are correctly implementing the maintenance regime.
The role of ECM is vital to the safe conveyance of goods on the rails, particularly when dangerous goods are involved. Given the environmental and economic benefits of rail freight, it is important to get the basics right in yards, depots and workshops across the country. I am therefore encouraged that the National Freight Safety Group is already working to better understand the risk posed by defective freight wagons, and to identify any additional control measures that may be needed to protect people, property and the environment.
1.5 Managing the consequences of bad weather
The UK’s railway infrastructure has always been exposed to the weather. Over the last 15 years or so RAIB’s investigations have featured wind, rain, ice, snow and high temperatures as factors in the causation of accidents. Examples have included wind-felled trees, containers blown from the back of freight trains, earthwork and structural failures linked to heavy rain, flooding and scour, ice falls from tunnel ventilation shafts, snow-induced brake failures and buckled rails. To manage these risks, infrastructure managers have a range of options available to them. These include:
- adapting the infrastructure to make it more resilient to weather events (for example, by improving drainage and earthwork resilience, or heating the conductor rail)
- by regular examination of railway infrastructure, and risk assessment, to prioritise investment in improving its resilience to unusual weather events
- by forecasting unusual weather events and adopting additional risk control measures, such as monitoring high-risk locations and slowing down trains
- by establishing processes that enable the railway to become aware of unusual weather events as they occur (so-called ‘nowcasting’), or recent infrastructure failures, in real-time; and adapting train operations accordingly (for example, by asking drivers to examine the line)
- by adapting the infrastructure to mitigate the consequences of infrastructure failures and events in high-risk locations (for example by keeping derailed trains in line on the approach to tunnel portals)
Train operators also have a part to play by procuring rolling stock that can operate reliably and safely in all weather conditions. Those specifying and designing trains should also seek to mitigate the consequences should a train derail following a failure of the infrastructure, for example by considering ways to limit the lateral deviation of passenger trains during a derailment. Train operators should also ensure that measures are in place to ensure that their drivers are aware of emergency speed restrictions, that may have been introduced in response to forecast, or actual, severe weather. They need also to ensure that drivers are trained on how to adapt their driving style in hazardous weather conditions, such as by increasing the number of running brake tests in snowy conditions.
Earthwork failures can occur suddenly or over a longer period of time. The investigation into the derailment of a freight train at Willesden High Level Junction in 2019 (report 07/2020) identified how the gradual movement of an underlying earthwork can reveal itself as irregular track geometry. An earlier example of this was found in RAIB’s investigation into the derailment of a freight train at Barrow upon Soar (report 22/2013). This means that there is real value in regular communication between the different engineers who are responsible for the track and the earthworks.
At Corby, Northamptonshire in 2019 (report 04/2020), a train became trapped in debris washed out by flood water after a period of continuous rainfall. We found that the railway and other parties had not adequately managed the flood control systems in the local area. This investigation serves as a reminder that Network Rail needs to identify locations prone to flooding, and review how it manages the flood risk at each one, sometimes in conjunction with bodies outside the railway. It is also significant that the weather that led to the catastrophic infrastructure failure at Corby was not particularly unusual.
The weather over Aberdeenshire on 12 August 2020 was unusual: 75% of the normal monthly rainfall fell in four hours during the morning. There were multiple instances of obstructions on the railway as a result, and the 06:38 hrs train from Aberdeen, heading towards Dundee, had only just passed Carmont signal box, 21 miles (34 km) into its journey, when it was stopped by a radio message and forced to turn back because of a landslip obstructing the line. It began to return to Aberdeen, but 1.4 miles (2.25 km) north of Carmont, while travelling at just under the line’s speed limit of 75 mph (121 km/h), it ran into debris that had been washed out from a drainage trench.
The train derailed, striking a bridge parapet with catastrophic consequences. The train driver and conductor and a passenger were killed. Our investigation began immediately and is still in progress. We have published an interim report on our findings to date. The ongoing investigation is focusing on drainage issues, the operating procedures that were designed to manage the risk of extreme weather events and the behaviour of the train during and after the der ailment.
RAIB has been impressed by Network Rail’s determination to think through the long-term implications of climate change, which will almost certainly lead to more extreme weather events. With this in mind, Network Rail has launched two independent task forces, each led by a renowned expert, to help it better manage its massive earthworks assets, and improve its understanding of and response to severe weather events. RAIB will take the findings of these task forces into account as its own investigation continues.
1.6 Railway operations
In May 2020 we published our class investigation into the factors affecting safety-critical human performance in signalling operations (report 03/2020). The decisions made by signallers have an immediate, vital impact on the safety of people using the railway. Whether giving a level crossing user permission to cross the line or making sure that track workers are protected from the approach of trains, a good decision by the signaller is often the last line of defence against tragedy.
RAIB has been concerned for some time about the vulnerability of this decision-making process, and how the performance of signallers can be affected by multiple, systemic factors that are within the control of railway management. As the railway got busier (in the years prior to the COVID-19 emergency), so the demands on the signaller increased. Much of what signallers deal with, mostly successfully, is down to experience and implicit knowledge, but current processes don’t recognise this.
We are recommending that Network Rail looks closely at how it manages the day-to-day work of signallers. The experience and knowledge of signalling staff is a vital asset, and needs to be properly and consistently developed, supported and made use of, for the safety of everyone who interacts with the railway.
The possible effects of distraction on the performance of train drivers were highlighted in our investigation into the accident at Neville Hill, Leeds (report 13/2020). A poor understanding of how to use the train’s computer system, and a lack of familiarity with driving a modern train were both factors. While it is important that drivers remain focused on their task and aware of the situation of their train, it is also vital that the equipment which they use, both hardware and software, is suitably designed, and that drivers are trained to use it appropriately.
1.7 Management assurance
Every railway and tramway duty holder in the UK is required to record its arrangements for managing safety risks. This written record is known as the safety management system (SMS); typical components include a statement of policy, formally defined management responsibilities, procedures, competence management and reporting systems.
An important element of any SMS is ‘management assurance’. Management assurance is about an organisation’s leaders and managers being aware of any gaps between theory and practice, and then taking action to address these. Since it relies on good information about what is really happening in the field, processes such as audit and formal management reviews have a role to play. However, more important still is the free flow of accurate intelligence between the front line and leaders. This requires honesty, openness and a willingness to give and receive bad news.
Good safety management is all about making sure that the systems you have set up, and what you have said you will do, are really happening on the ground. An underlying theme in many of the investigations this year has been the divergence between what the management system said should be happening, and what was actually going on. By way of example, RAIB’s investigation into the accident at Margam identified that Network Rail’s management assurance system was not effective in identifying the full extent of procedural non-compliance and unsafe working practices, and so did not trigger the management actions needed to address them. Similar issues with management assurance were also identified in the investigations into the death of a train driver at Tyseley depot (report 09/2020) and a signal passed at danger near Loughborough (report 10/2020), and they have been a factor in the ongoing investigation into the fatal accident involving a track worker at Roade in April 2020.
Our investigation of the incident at Loughborough, in which a train delivering new rolling stock to a storage depot passed a signal at danger, found some significant deficiencies in the way that the train operator was managing safety. This led to a train being driven faster than was permitted on the route, and therefore being unable to stop before passing a red signal by a significant distance. There was a gap between documented safety processes, and what was actually happening. There also appeared to be no management awareness of how well, if at all, the company was following its own safety processes, including those related to competence management.
Certainly, good management assurance relies on formal systems. However, our investigations are revealing that a positive, open and honest culture is also needed if leaders are to be properly informed, and protected from wishful thinking. There also needs to be recognition that only very rarely are accidents caused by people who are reckless or irresponsible. What we often observe is people trying hard to get the job done, often in a very difficult working environment. It is that commendable eagerness to complete the task that can so easily cause people to overlook the risks that they are taking.
1.8 Safety culture
Safety culture has been defined as “the way we do things round here”. Good safety culture can make a huge difference, creating an environment in which people behave in a safe way without hesitation and without embarrassment.
At Balham (report 01/2020), we investigated an incident in which a poor standard of communications played a crucial part. In this case, the way in which the key individuals talked to each other resulted in a misunderstanding. The consequences of the misunderstanding were that a very large item of yellow plant, a tamping machine, came out of an area where it had been working, onto a line where a passenger train had passed in the opposite direction only a short time before.
Our investigation found a culture of poor communications among staff involved with engineering work. People were embarrassed to use the proper protocols when passing messages to colleagues. The aviation industry confronted this problem head-on many years ago, and now any pilot or air traffic controller who does not use the correct form of words and phrases would instantly stand out as less than competent. We found evidence that the standard of voice communications between train drivers and signallers has improved in recent years. However, the same cannot be said for engineering operations staff, even when talking to signallers. We are challenging the railway industry to come into line with aviation and embed the same standards among its people.
This theme continued at Rochford (report 08/2020), where two road-rail mobile lifting platforms collided in an engineering worksite. Although the consequences of this accident were minor, the people who were in the machine that was struck could easily have been killed if they had not been wearing their safety harnesses.
Our investigation found a catalogue of errors and omissions which could have had much more serious consequences. It was particularly disturbing to find underlying evidence that racial, language and cultural tensions were factors in the accident at Rochford. Safety relies on mutual respect within teams, for each other and for each person’s role. If this is lacking for any reason, then as well as creating a culture of disrespect, it creates an environment in which accidents are more likely to happen. I am pleased that Network Rail has already recognised this problem in one of its subsidiary companies and is taking action to improve the situation.
1.9 Other themes
Other important themes highlighted in the last year included:
-
The design and management of train braking systems. See our new ‘Summary of learning’ in this area
-
The management of emergency speed restrictions
- The last year saw examples of passenger trains grossly exceeding emergency speed restrictions: at Dauntsey, Wiltshire (on 12 August 2020); between Laurencekirk and Portlethen (on 4 December 2020); and near Beattock (on 20 December 2020). The first of these was the subject of a letter to Network Rail and RSSB, the second is being investigated by RAIB and our findings relating to the third have been published as a safety digest (safety digest 02/2021). These three incidents highlighted a theme explored by RAIB on a number of occasions in recent years (for example, the investigation into an overspeeding event at Sandy on the East Coast Main Line in October 2018 (report 10/2019)) and the continued need for the industry to think hard about how best to manage the risk of overspeeding at emergency speed restrictions.
1.10 International issues
The close of 2020 saw the end of the implementation period following the UK’s exit from the European Union. Following this, we have maintained strong professional relationships with our colleagues investigating accidents in Europe and elsewhere. These cross-border links are invaluable to RAIB, enabling us to learn from others while also facilitating co-operation on matters related to railway safety. We have also updated our memoranda of co-operation with our equivalent organisations in France (the Bureau d’Enquêtes sur les Accidents de Transport Terrestre) and Ireland (the Rail Accident Investigation Unit), so assuring continued co-operation in case of an accident near the UK’s international borders.
1.11 Concluding thoughts
RAIB’s primary function is to identify safety learning. Although our findings can sometimes be uncomfortable for the organisations involved, they often point the way to improve railway safety in the future. Our recommendations are not ‘instructions’ to industry but suggestions as to where safety can be improved. It is the job of the safety authority (usually the Office of Rail and Road) to determine if appropriate action has been taken, and to enforce change should it consider it to be necessary.
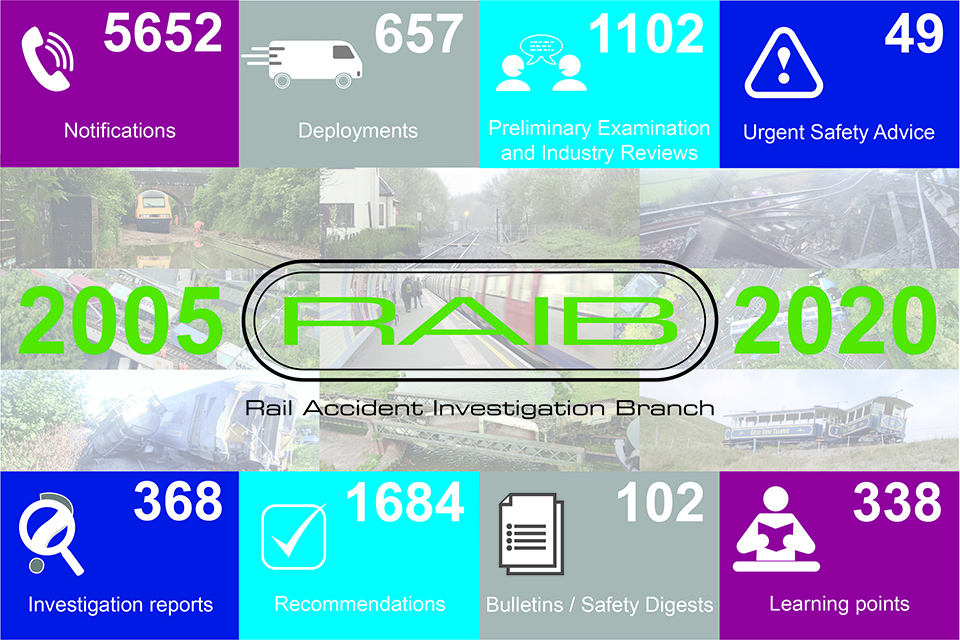
On 17 October 2020, we marked 15 years from RAIB’s start of operations. During that time, RAIB has published 368 investigation reports and 102 short-form safety digests/bulletins covering every sector of this huge and complex industry. One of RAIB’s core functions is to inform the industry, government and the wider public by conducting independent and open investigations of accidents and incidents, the results of which are always made public. This duty to report our findings means that the rail industry is one of the most open sectors of the UK economy on matters relating to safety. This openness also means that our work is available for public scrutiny, which we welcome. It also means that the entire industry benefits from learning from accidents, regardless of which companies were involved.
The process of learning from what has gone wrong has formed the basis of massive improvements in railway safety over nearly two centuries. In the early 1980s, when I joined the rail industry, the 10-year rolling average number of fatal train accidents on the main line network was close to three a year, and by 2005 this had fallen to one a year. In 2017, the 10-year rolling average number of fatal train accidents fell to zero, a remarkable achievement for the industry (sadly, it has now risen to 0.1 following the derailment at Carmont). Furthermore, the UK’s railway industry is now one of the safest in Europe.
Although it is impossible to quantify RAIB’s contribution to this trend of improvement, I am proud to be part of an organisation that has done so much to further rail safety, and that has built an international reputation for high quality independent investigation.
It is tragic that the year 2020, which was already proving so difficult for the industry due to the COVID-19 emergency, saw the Carmont derailment. RAIB inspectors and support staff were on site within hours of the accident and maintained a continuous presence until the train was recovered. Throughout this period, they worked hard, in co-ordination with other statutory agencies, to examine the site and collect the evidence that will be needed to investigate what has happened. Despite the traumatic effect of the pandemic and the disruption to their family lives, the team responded magnificently, travelling long distances, staying away from home in a local lockdown area, sometimes for weeks at a time, and working in difficult conditions.
Two weeks later, when we were still on site at Carmont, a team including people who had just returned from Carmont was called to attend the scene of a major derailment and fire involving an oil train at Morlais Junction in Carmarthenshire.
I am impressed by the professionalism and dedication of my colleagues who made all of this happen in August 2020. Once again RAIB has proved its resilience and its continued worth to the rail industry and the wider public, and for that I am deeply grateful.
This will be the sixth Annual Report that we have published since I was appointed as Chief Inspector. It is also my last, since I plan to retire from the role in the autumn of 2021, after 39 years as part of this exciting and dynamic industry. I will look back on my years at RAIB, from its very earliest days, with a huge sense of pride. I know that the Branch will march on and continue to provide the expertise and independence that has formed the bedrock of its success over its first 16 years of operations.
Simon French
Chief inspector of Rail Accidents
April 2021
2. 2020 marked RAIB’s fifteenth year of operations
17 October 2020 was the fifteenth anniversary of the day that RAIB’s full legal powers came into force and we started investigating accidents on the UK’s railway network. Very early the day after we became operational, a freight train derailed near Hatherley, just south of Cheltenham Spa station, and the RAIB’s work began. Since then we have become an integral part of the UK’s railway safety regime, an independent and expert body that stands in constant readiness to investigate when things go badly wrong.
RAIB marked fifteenth year of operation
The establishment of an independent rail accident investigation body was recommended by Lord Cullen following the terrible accident at Ladbroke Grove, London, in 1999, that led to the death of 31 people.
To put this into effect, legislation to set up RAIB was included in the Railways and Transport Safety Act 2003. The Act also empowered the Secretary of State for Transport to create the detailed regulations needed to ensure the effective operation of the new body: The Railways (Accident Investigation and Reporting) Regulations 2005.
The creation of the Branch required the recruiting of personnel from industries across the country, the establishment of two operational centres, one in Derby and the other in Woking, subsequently moving to Farnborough. Other activities included the procurement of equipment to support operations and extensive training.
3. Our Aims
We aim to be:
- world-class accident investigators, respected and trusted by the public and railway industry
- positive, sensitive and efficient in dealing with others, both inside and outside of the organisation
- adaptive to changes in industry, technology and society
We will:
- have a culture of integrity, honesty, objectivity and impartiality
- encourage and help our people to develop
- act in accordance with the highest professional standards
- publish safety learning as quickly as possible to help industry manage any risk

Aims
4. Operational Activity
The UK rail industry is required to notify us of accidents and incidents as defined in the Regulations. Of the 457 notifications we received between 1 January and 31 December 2020, we deployed to 23 events to carry out a preliminary examination of the evidence. We identified 15 other notified events that also deserved a preliminary examination, which in many cases was carried out remotely. A review of the findings of each of these examinations allowed us to decide on the most appropriate response.

Outcome of PERs undertaken by RAIB in 2020
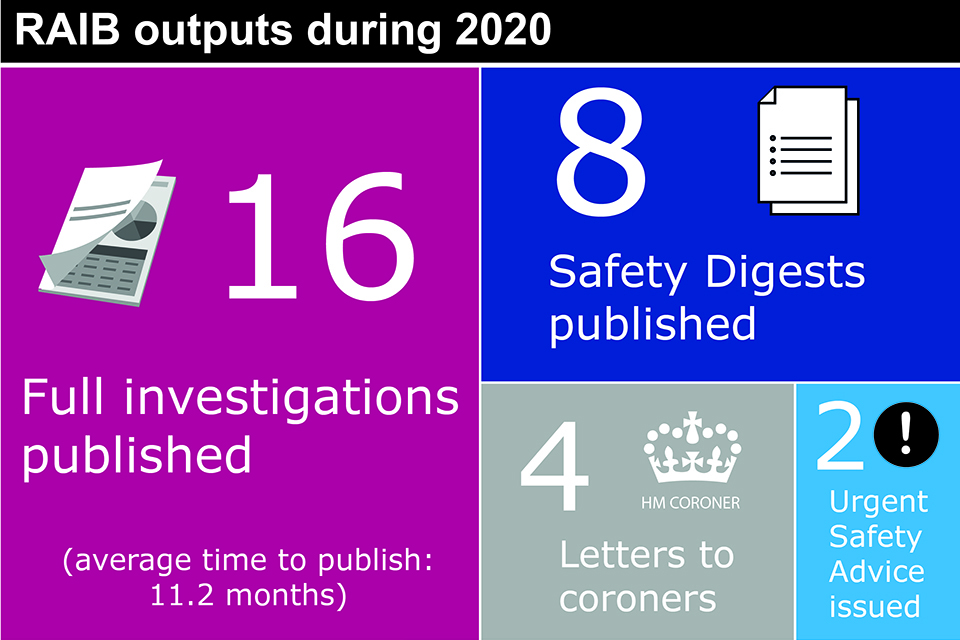
RAIB outputs during 2020
Having reviewed the evidence we have gathered, if we do not believe there is sufficient safety learning to be gained from further investigation, we may write a letter to the industry. We may decide to share the evidence we have collected with the industry parties involved, to assist them with their own investigations into the event. We may also review industry investigations to inform ourselves about the quality of the investigation or technical aspects of the event that it relates to.
Read more about the Regulations at bit.ly/3gka9q3
4.1 Northern Ireland and the Channel Tunnel
We continue to maintain good working relationships with our counterparts in the Republic of Ireland (the Railway Accident Investigation Unit; RAIU), and France (the Bureau d’enquetes sur les accidents de transport terreste; BEA-TT), and with the relevant infrastructure managers, railway undertakings, and safety authorities.
4.2 Accidents investigated by RAIB
The Railways (Accident Investigation and Reporting) Regulations 2005 (the Regulations) set out the types of accidents which are classified as ‘serious’. RAIB has a duty to investigate all serious accidents including derailments and collisions of rolling stock resulting in the death of one person, serious injuries to five or more people, or extensive damage to the rolling stock, infrastructure or environment.
We have a similar duty for incidents and accidents which, under slightly different circumstances, could have resulted in serious accidents, and which have an obvious impact on railway safety regulation or the management of safety.
The Regulations transposed the requirements of the EU Directive 2004/49/EC into UK law.
The European Agency for Railways (ERA) has published guidance to promote consistent categorisation of investigations in accordance with the Directive. During 2020, we used this to classify our investigations according to Articles 19(1) and 19(2) of the Directive.
- Article 19(1) - a ‘serious’ accident where the investigation is mandatory
- Article 19(2) - an accident or incident, which under slightly different conditions might have led to a serious accident, such as a narrowly avoided serious accident
We have investigated 88 serious accidents and incidents between 2016 and 2020. Of these, 18 were classified under article 19(1) and 70 under article 19(2). During 2020, 15 investigations were classified under these Articles.
| Basis for investigations by the European Railway Safety Directive category | 2016 | 2017 | 2018 | 2019 | 2020 | Total |
|---|---|---|---|---|---|---|
| Article 19(1) | 5 | 4 | 3 | 4 | 2 | 18 |
| Article 19(2) | 14 | 14 | 16 | 13 | 13 | 70 |
| Total | 19 | 18 | 19 | 17 | 15 | 88 |
The graphic below shows the total number of investigations and safety digests started, by type of accident, for the five-year period 2016 – 2020
| Categories | Full investigations | Safety digests |
|---|---|---|
| Events involving moving trains (passengers and members of the public) (20) | 18 | 2 |
| Level crossing accidents and near misses (19) | 9 | 10 |
| Events involving moving trains (staff) (17) | 8 | 9 |
| Collision with an obstacle (14) | 7 | 7 |
| SPAD or unauthorised train movements (13) | 9 | 4 |
| Near misses (12) | 2 | 10 |
| Passenger train derailments (12) | 5 | 7 |
| Freight train derailments (11) | 8 | 3 |
| Runaway incidents (10) | 7 | 3 |
| Collisions with other trains (9) | 8 | 1 |
| Infrastructure failures (6) | 6 | 0 |
| Train defects (6) | 4 | 2 |
| Class investigations (2) | 2 | 0 |
| Failure of signalling system (2) | 2 | 0 |
| Fires on rolling stock (1) | 0 | 1 |
During the five-year period 2016 to 2020, we started 154 full investigation reports and safety digests. Twenty involved passengers and moving trains (such as a passenger trapped in train doors) and 17 involved railway employees and moving trains (such as accidents to track maintenance workers). Another 19 involved harm, or the risk of harm, to people at level crossings. We also investigated 23 derailments (12 involved passenger trains and 11 freight trains), 14 collisions with obstacles, 13 unauthorised train movements, 10 runaways and 9 collisions between trains.
5. Recommendations
Our recommendations are made with the sole objective of improving railway safety. They aim to reduce the chance of a similar accident recurring, or to reduce the consequences if such an event were to happen again.
Recommendations clearly identify the organisation that we consider is best placed to implement the changes required. We refer to these organisations as the ‘end-implementers’. These organisations include railway, non-railway, and private and public sector bodies.
Most recommendations are also addressed to the appropriate safety authority. On Great Britain’s railways this is the Office of Rail and Road (ORR). The safety authority for railways in Northern Ireland is the NI Department for Infrastructure (who are advised by HSE). Up to 31 December 2020, the safety authority for the Channel Tunnel system was the Intergovernmental Commission (IGC).[footnote 1] If a recommendation relates to an organisation that is not regulated by the railway industry’s safety authority it can be addressed to any other public body such as the Health and Safety Executive.
Having received our recommendations, the safety authority is legally required to ensure that the ‘end-implementers’ consider the recommendations, and where appropriate, act on them, as required by the Regulations. The Regulations also give the safety authority the power to require end implementers to provide full details of the measures they intend to take, or have taken, to implement the recommendation.
The safety authority is required to ensure that proper consideration has been given to each recommendation and, where appropriate acted upon. It should also inform us of the measures taken in response to the recommendation, or the reasons why no implementation measures are being taken.
RAIB collates data on the actions in response to recommendations. In most cases, the data is based on reports received from the safety authority (usually ORR). Public bodies who are recipients of RAIB recommendations are required to respond directly to us.
The current status of RAIB recommendations
The responses to our recommendations, as reported to RAIB, are categorised as follows:
i. Implemented - all actions to deliver the recommendation have been completed
ii. Implementation ongoing - work to deliver the intent of the recommendation has been agreed and is in the process of being delivered
iii. Implemented by alternative means – the intent of the recommendation has been satisfied in a way we did not identify during the investigation
iv. Progressing – the relevant safety authority has yet to be satisfied that an appropriate plan, with timescales, is in place to implement the recommendation; and work is in progress to provide this
v. Awaiting response – the relevant safety authority has yet to receive a report from the end-implementer on the actions that have been taken, or are planned, in response to an RAIB recommendation
vi. Insufficient response – the relevant safety authority considers that the response received from an end-implementer is insufficient
vii. Non-implementation – recommendation considered, and no implementation action is to be taken
5.1 Recommendations made during 2020
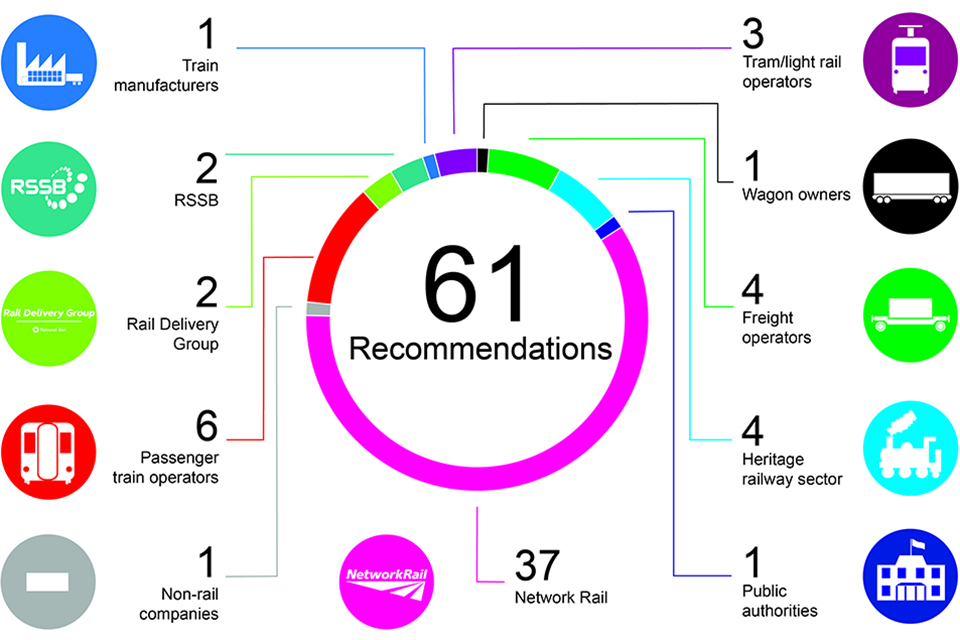
During 2020, we made 61 recommendations which were directed to 11 different organisations including operators, manufacturers and other authorities. In one case, a recommendation was made to more than one end implementer.
Recommendations made during 2020
The status of all recommendations made between 2016 and 2020 is as follows:
- 57% are either implemented, or their implementation is ongoing
- for 21% of recommendations the safety authority has yet to be satisfied that an appropriate plan, with timescales, is in place for implementation (that is, the response is still ‘progressing’)
- for 21% of recommendations a sufficient response has still to be reported to the safety authority (these are mainly recommendations made during 2020)
- less than 1% of recommendations have been reported as not being implemented
Of all the recommendations made between 2016 and 2019 (that is, all recommendations that were more than one year old on 31 December 2020), 69% have already been reported as implemented or are in the process of being implemented. The remaining 31% of recommendations made between 2016 and 2019 remain open. This is because ORR has yet to receive a sufficient response, or because ORR is still considering the duty holder’s response.
Implementation
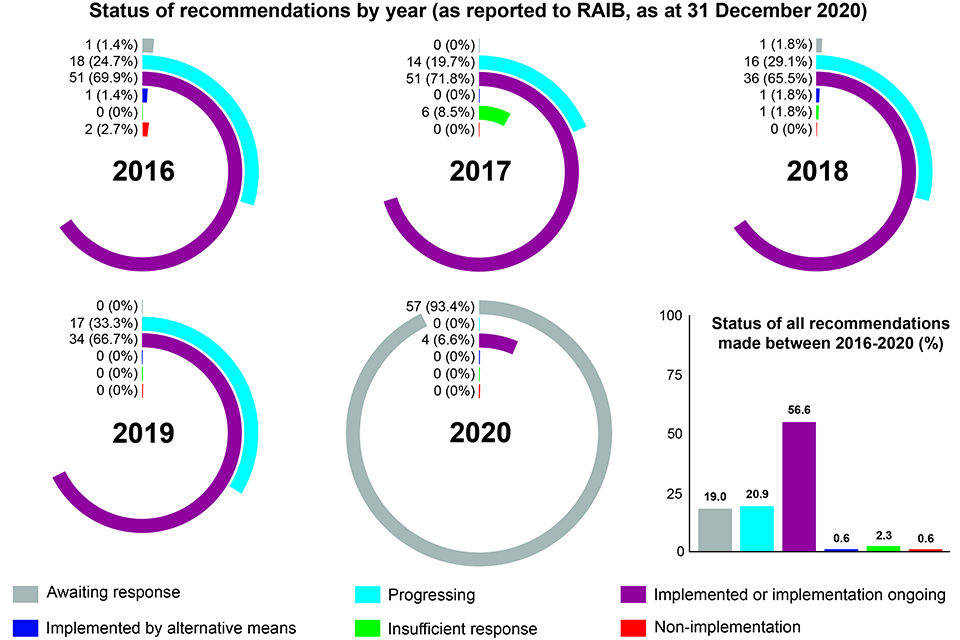
Status of recommendations by year 2016 - 2020
We recognise that there is an inevitable time lag between a duty holder reporting the actions taken or planned in response to a recommendation, and ORR reporting the outcome to RAIB. This period of time is required for ORR to consider the appropriateness of the actions and can sometimes be prolonged if ORR needs further information from the duty holder, or is concerned about the appropriateness of the actions.
The status of each recommendation is reported to RAIB by the safety authority, or other public body, to whom the recommendation was addressed. An up-to-date status of each recommendation is available in the Index of RAIB recommendations. The Index provides information as supplied by the relevant safety authority or public body. Each entry is linked to a recommendation status response that provides the full text of each recommendation.
Areas of concern
On occasions, the end-implementer may propose do less than is specified in a recommendation, or to address the risk in another way. In each such case the safety authority will consider whether the intent of the recommendation has been met and whether it is reasonably practicable for the end-implementer to do more.
Based on our own understanding of the risk, we may sometimes have concerns about the way an organisation has responded to a recommendation, or the information provided to us by the safety authority. When this happens, we will first discuss the issue with the relevant safety authority, or other public body, before recording any remaining concerns in the next Annual Report. Shown below are summaries of all such issues that were identified during 2020.
When RAIB records its concerns regarding the actions taken in response to recommendations, it marks them with coloured triangles according to the following categorisation:
Red - we have concerns that no actions have been taken in response to a recommendation
Blue - we are concerned that the actions taken are inappropriate or insufficient to address the risk identified during the investigation
White - we note that substantive actions have been reported but we still have concerns about the underlying risk.
Report 10/2012 – Fatal accident at Mexico footpath crossing (near Penzance)
Recommendation 3 - White
Intent of recommendation – for Network Rail to undertake a project to develop and implement a national approach to the location and marking of decision points and the measuring of sighting distances at footpath level crossings.
ORR status – Implemented
RAIB concern – Considerable work has been undertaken on the use of yellow decking to define danger zones, however, safe and consistent maintenance of such surfaces has not always been practical. As a result, provision of such marking has remained a local decision ‘where this is considered appropriate’. While Network Rail is still considering danger zone marking as part of a review of signage at user worked crossings, RAIB is concerned that ORR has defined the recommendation as implemented, when its overall aim, at present, is only partially met.
Report 05/2015 – Fatal accident at Frampton level crossing
Recommendation 6 - White
Intent of recommendation – to provide clear information about locations where public vehicular restrictions exist at level crossings that cross highways.
ORR status – Implemented
RAIB concern – Network Rail has informed ORR that it now is working with local highway authorities and other bodies to identify the need for additional measures at level crossings where safety management depends on the public being aware that they are not allowed to cross using vehicles such as cars, motorcycles and trail bikes. ORR does not think it reasonably practicable for Network Rail to install signs at all such locations.
RAIB notes the approach adopted by Network Rail but remains unclear how these new relationships will translate into action at locations where the use of crossings by prohibited vehicles is considered particularly dangerous.
Report 11/2018 – Near miss with a group of track workers at Egmanton level crossing, Nottinghamshire
Recommendation 1 - Blue
Intent of recommendation – to both strengthen safety leadership behaviour on site and reduce the occurrences of potentially dangerous rule breaking by those responsible for setting up and maintaining safe systems of work (COSS, SWL, PIC).
ORR status – Implemented
RAIB concern – Network Rail has reviewed its responses to this recommendation in view of the subsequent double-fatal, trackworker accident at Margam. This is considered the correct approach by ORR. RAIB agrees; however, as a result we consider the status ‘implemented’ as premature because the actions to address it are ongoing.
Report 11/2018 – Near miss with a group of track workers at Egmanton level crossing, Nottinghamshire
Recommendation 2 - Blue
Intent of recommendation – to mitigate the potentially adverse effect that client-contractor relationships can have on the integrity of the Worksafe procedure when contract workers are not willing to challenge unsafe systems of work set up by Network Rail staff in safety leadership roles, due to the fear of losing future employment.
ORR status – Implemented
RAIB concern – ORR’s view is that Network Rail has been clear in responses that the bulk of the detailed recommendation is not practical or is prevented by commercial considerations, but that Network Rail has tried to do what it can to meet the intent. RAIB’s concern is that what has been done to date (noting Network Rail’s ongoing work as a result of the Margam accident) is insufficient to have the desired effect of reinforcing the willingness of contractors to challenge site safety leaders.
5.2 Summaries of learning
Since we became operational in 2005, RAIB has gained insight into a wide range of different accidents and causal factors. As the years pass, it is possible to identify a number of recurrent themes and we felt it useful to document these in short summary reports. These reports, entitled ‘Summaries of learning’ were introduced for the following themes in the 2019 Annual Report:
1 - Design and operation of user worked level crossings
2 - Protection of track workers from moving trains
3 - Managing risk at the platform-train interface
4 - The safe management of abnormal train-operating events which put passengers and crews at risk
6 - Safe design, operation and maintenance of on-track plant and trolleys
These have been reviewed and updated as necessary to incorporate learning from 2020. We have also identified two other recurrent themes which are now the subject of a Summary of learning:
7 - The safe management of weather-related events which affect train operation
8 - The integrity of train braking systems
More information on each of these areas can be found at: gov.uk/government/collections/summaries-of-learning
6. Other activities
6.1 Rail accident investigators’ good practice seminar
With global events overtaking everyone’s plans in 2020, we had to postpone our fourth accident investigators’ good practice seminar.
The aims of these seminars have been to encourage sharing and discussion of issues and experiences among professionals responsible for rail accident investigation.
We are already making plans for 2021 in the hope that we’ll be able to host the event and bring together colleagues from across the rail industry.
6.2 Working with Academia
As part of our Branch development activities, RAIB has been nurturing informal relationships with a small number of universities for the last three years.
Aimed primarily at improving our investigation capabilities by keeping us at the forefront of scientific developments, the relationships are two-way and also offer universities a source of ideas and assistance for student projects, as well as occasional guest lectures on relevant programmes delivered by RAIB inspectors. The universities involved in this initiative were included for their breadth of expertise across a range of subjects relevant to RAIB’s work, such as mechanical engineering and human factors.
To date, several postgraduate projects involving RAIB have been successfully completed, while RAIB has benefitted from academic input on two of its recent investigations (the class investigation into human performance in signalling operations, report 03/2020, and the investigation into track workers struck by a train at Margam, report 11/2020).
Given the success of the initiative so far, RAIB has also recently instigated the formation of a similar academic working group across the three accident investigation branches (Air, Marine and Rail), with the aim of more effective collaboration on areas of mutual interest.
6.3 External events
While the COVID-19 emergency meant that RAIB participated in fewer external events during 2020 than is usual, we were still able to present at a number of web conferences, such as the event hosted by the Rail Division of the Institution of Occupational Safety and Health in November and the European Rail Agency (ERA) conference in December.
6.4 International relations
RAIB has been a longstanding member of the International Transportation Safety Association (ITSA). ITSA is an international network of heads of independent safety investigation bodies, covering all modes of transport, including aviation, marine, railways, road transport, pipelines and underground infrastructure. The membership includes major investigation bodies across five continents, such as the NTSB in the USA and the ATSB in Australia.
This year’s meeting of ITSA, planned to take place in Sydney, was cancelled due to the pandemic. However, the heads of the investigation bodies were able to meet by virtual means.
RAIB has maintained cordial professional links with the network of EU National Investigation Bodies and continues to work to promote the sharing of information, learning and good practice across international borders in Europe and beyond.
RAIB has signed protocols with its equivalent organisations in France (Bureau d’Enquêtes sur les Accidents de Transport Terrestre) and Ireland (Rail Accident Investigation Unit) which document the way that RAIB and its international partners will work together in the event of an accident on or near the UK’s frontiers. The protocol with BEA-TT covers accidents in the Channel Tunnel system and allows for joint investigation should both investigation bodies declare an interest. The Irish protocol allows for co-operation in the event of an accident involving the Enterprise service between Belfast and Dublin. Both protocols have recently been updated to take into account the departure of the UK from the EU.
6.5 Road accident investigation
We continue to provide support to the RAC Foundation as it progresses its Road Collision Investigation Project (RCIP).
The project seeks to establish whether there is a business case for putting more resource into the investigation of road crashes, based on a comparison with the approach to accident investigations used for other modes (rail, air and sea) and safety-critical industries (oil and gas). The project is well under way with investigations in a number of police force areas in order to develop and trial a different approach to identifying and understanding common themes and patterns that result in death and injury on the public highway.
RAIB is assisting the RAC Foundation by releasing an experienced investigator to work with the RCIP team.
This helps the team develop its investigation approach, review its investigation reports and provide input to various other strands of the project including:
- a review of road collision investigation approaches in other countries
- identifying the legal powers any future road collision investigation body would need to carry out independent investigations
- assessing the training requirements for future investigators
The project is due to be completed by Summer 2022.
Find out more about the project and the work of the RAC Foundation at: racfoundation.org/collaborations/road-collision-investigation-project.
6.6 The Accident Investigation Chiefs’ Council (AICC)
The Accident Investigation Chiefs’ Council (AICC) comprises a non-executive chair and the Chief Inspectors from Air, Marine and Rail Accident Investigation Branches.
The AICC aims to promote the AIBs’ effectiveness, efficiency and resilience through collaboration; establishing common positions on issues of mutual interest, including the development of joint Memoranda of Understanding and other collaborative working arrangements; maintaining an overview of quality, the timeliness of outputs and value for money; and actively promoting the AIBs as centres of excellence. This includes the sharing of technical skills and knowledge in areas such as analysis of electronic data, administration and, given the geographic separation between the branches, sharing equipment to allow rapid deployment throughout the UK.
The work of the AICC is facilitated by a joint resource, the Head of Joint Policy.
Read more about the role of the AICC, its terms of reference, and its Memorandum of Understanding (MoU) at gov.uk/government/publications/accident-investigation-chiefs-council/accident-investigation-chiefs-council.
6.7 RAIB’s own safety record
Responding to railway accidents and incidents can expose our team to a variety of significant health and safety hazards. We have developed, and continue to update, our own Safety Management System (SMS). This includes our health and safety policy and arrangements for how we manage risk. These include a dynamic risk assessment process for the real-time assessment of risk.
We monitor our own health and safety performance as an integral part of our management and governance process. We have an in-house Health, Safety and Welfare committee which meets regularly to consider how best to manage our risk.
We also work with our colleagues across the Accident Investigation Branches to identify and share good practice.
Two minor injuries to members of our team were reported during 2020. One member of the team also experienced a narrowly avoided accident. Each of these was recorded and investigated.
As with all organisations, the events of 2020 have meant that we have had to take account of the risk to health from Covid-19, and the consequences of restrictions on movement and activities, when responding to accidents and incidents. We have been continuously working to make sure the branch can operate safely, protecting both colleagues and people who we may come into contact with as part of our investigations.
6.8 Funding
Our operating budget for the 2020-21 financial year was £5 million.
7. Data tables
7.1 Investigations completed and commenced in 2020
Table 1 lists all RAIB investigations published during 2020. Details of all investigations started by RAIB during 2020 are provided in table 2.
During 2020 we classified our investigations according to Article 19 of guidance published by ERA. This guidance promotes consistent categorisation of investigations in accordance with the EU Rail Safety Directive. The classifications are:
- Article 19(1) - a serious accident where the investigation is mandatory
- Article 19(2) - an accident or incident, which under slightly different conditions might have led to a serious accident, that is, a narrowly avoided serious accident
You can read summaries of all of our current investigations.
Table 1 – Full investigations completed in 2020
| Report Number | Event date | Publication date | Title of the investigation (location) | Occurrence type | Basis for investigation |
|---|---|---|---|---|---|
| 01/2020 | 20/04/2019 | 03/02/2020 | Serious operational irregularity at Balham | SPAD or unauthorised train movement | 19(2) |
| 02/2020 | 16/04/2019 | 06/02/2020 | Runaway locomotive at Beddgelert, North Wales | Runaway incident | 19(2) |
| 03/2020 | n/a | 12/05/2020 | Class investigation into human performance in signalling operations | Class investigation prompted by various safety incidents involving signaller error | 19(2) |
| 04/2020 | 13/06/2019 | 26/05/2020 | Train collision with material washed out from a cutting slope at Corby, Northamptonshire | Collision with an obstacle | 19(2) |
| 05/2020 | 01/08/2019 | 28/05/2020 | Loss of brake control on a sleeper train approaching Edinburgh | SPAD or unauthorised train movement | 19(2) |
| 06/2020 | 17/05/2019 | 03/08/2020 | Signal passed at stop and near miss, Deansgate-Castlefield, Manchester | SPAD or unauthorised train movement | 19(2) |
| 07/2020 | 06/05/2019 | 25/08/2020 | Freight train derailment at Willesden High Level Junction, north-west London | Freight train derailment | 19(2) |
| 08/2020 | 25/01/2020 | 28/09/2020 | Collision between mobile elevating work platforms, Rochford, Essex | Collision with other train | 19(2) |
| 09/2020 | 14/12/2019 | 07/10/2020 | Fatal accident at Tyseley depot | Train Movement Event involving staff | 19(1) |
| 10/2020 | 26/03/2020 | 09/11/2020 | Signal passed at danger at Loughborough South Junction, Leicestershire | SPAD or unauthorised train movement | 19(2) |
| 11/2020 | 03/07/2019 | 12/11/2020 | Track workers struck by a train at Margam, Neath Port Talbot | Train Movement Event involving staff | 19(1) |
| 12/2020 | 23/01/2020 | 16/11/2020 | Derailment of a freight train at Wanstead Park | Freight train derailment | 19(2) |
| 13/2020 | 13/11/2019 | 18/11/2020 | Collision and derailment at Neville Hill | Collision with other train | 19(2) |
| 14/2020 | 23/03/2020 | 19/11/2020 | Passenger train collision with a derailed locomotive at Bromsgrove | Collision with other train | 19(2) |
| 15/2020 | 24/11/2019 | 14/12/2020 | Near miss at Norwich Road level crossing | Level crossing near miss | 19(2) |
| 16/2020 | 09/03/2020 | 23/12/2020 | Runaway and derailment of a wagon at Clitheroe | Runaway incident | 19(2) |
Table 2 – Full investigations commenced in 2020
| Event date | Title of the investigation (location) | Occurrence type | Basis for investigation |
|---|---|---|---|
| 23/01/2020 | Derailment of a freight train at Wanstead Park | Freight train derailment | 19(2) |
| 25/01/2020 | Collision between mobile elevating work platforms at Rochford | Collision with other train | 19(2) |
| 28/01/2020 | Freight train derailment at Eastleigh | Freight train derailment | 19(2) |
| 26/02/2020 | Person struck by a train at Eden Park station, south-east London | Train movement event involving pax/pedestrians | 19(1) |
| 09/03/2020 | Runaway and derailment of a wagon at Clitheroe | Runaway incident | 19(2) |
| 23/03/2020 | Passenger train collision with a derailed locomotive at Bromsgrove | Collision with other train | 19(2) |
| 26/03/2020 | Signal passed at danger at Loughborough South Junction, Leicestershire | SPAD or unauthorised train movement | 19(2) |
| 08/04/2020 | Fatal accident near Roade | Train Movement Event involving staff | 19(1) |
| 26/05/2020 | Fatal accident at Waterloo Underground station | Train movement event involving pax/pedestrian | 19(1) |
| 21/06/2020 | Signal passed at danger and subsequent near miss at Chalfont & Latimer station, Buckinghamshire | SPAD or unauthorised train movement | 19(2) |
| 12/08/2020 | Passenger train derailment near Carmont, Aberdeenshire | Fire on rolling stock / Passenger train derailment | 19(1) |
| 26/08/2020 | Derailment and fire involving a tanker train at Llangennech, Carmarthenshire | Fire on rolling stock / Freight train derailment | 19(1) |
| 11/11/2020 | Freight train derailment at Sheffield station | Freight train derailment | 19(2) |
| 04/12/2020 | Overspeeding trains between Laurencekirk and Portlethen | SPAD or unauthorised train movement | 19(2) |
| 19/12/2020 | Near miss with a member of staff at Rowlands Castle | Train Movement Event involving staff | 19(2) |
7.2 Safety digests commenced or completed in 2020
Table 3 – Safety digests commenced or completed in 2020
| Event date | Publication date | Digest number | Title of the investigation (location) |
|---|---|---|---|
| 26/09/2019 | 09/01/2020 | D01/2020 | Equipment explosion on an empty passenger train, Central Rivers |
| 17/10/2019 | 18/02/2020 | D02/2020 | Train collision with tree near Spittal, Pembrokeshire |
| 14/11/2019 | 14/04/2020 | D03/2020 | Near miss with track workers near Kirtlebridge, Dumfries and Galloway |
| 10/03/2020 | 23/07/2020 | D04/2020 | Person struck by tram at Gravel Hill tram stop, Croydon |
| 16/06/2020 | 06/08/2020 | D05/2020 | Near miss with a track worker near Leighton Buzzard, Bedfordshire |
| 07/05/2020 | 18/08/2020 | D06/2020 | Signals passed at danger due to reduced brake performance, near Crofton West Junction, West Yorkshire |
| 08/06/2020 | 27/08/2020 | D07/2020 | Near miss at Worlingham user worked crossing, Suffolk |
| 22/10/2020 | 17/12/2020 | D08/2020 | Passenger train derailment at Bognor Regis |
| 10/12/2020 | 16/03/2021 | D01/2021 | Runaway and near miss at Dereham Station |
| 20/12/2020 | 24/03/2021 | D02/2021 | Overspeed through emergency speed restriction near Beattock |
7.3 Urgent Safety Advice issued in 2020
We can issue urgent safety advice at any stage during an investigation when we believe there is a need to provide immediate information to the relevant industry bodies about the wider safety issues we have identified.
If the issue affects other European member states, we report the safety advice to ERA via their safety information system (SIS); this action alerts all member states to the advice.
During 2020 we issued two items of urgent safety advice.
| Event date | Event | Urgent safety advice | Date of USA |
|---|---|---|---|
| 14/12/2019 | Fatal accident at Tyseley depot | Passing between or close to the end of stationary rail vehicles in depots, yards and sidings | 03/03/2020 |
| 26/08/2020 | Derailment and fire involving a tanker train at Llangennech | Maintenance arrangements for wagons that primarily carry dangerous goods | 05/11/2020 |
-
From 1 January 2021 the IGC will remain the safety authority for the UK half of the Channel Tunnel until this role passes to ORR later in the year. The Établissement Public de Sécurité Ferroviaire (EPSF) became the safety authority for the French half of the Channel Tunnel on 1 January 2021. ↩