Young people's substance misuse treatment statistics 2018 to 2019: report
Published 28 November 2019

© Crown copyright 2019
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/statistics/substance-misuse-treatment-for-young-people-statistics-2018-to-2019/young-peoples-substance-misuse-treatment-statistics-2018-to-2019-report
1. Main findings
1.1 Trends in treatment numbers among young people
There were 14,485 young people in contact with alcohol and drug services between April 2018 and March 2019. This is a 7% reduction on the number the previous year (15,583) and a 40% reduction on the number in treatment in the year 2008 to 2009 (24,053).
1.2 Trends in substance use among young people
Cannabis remains the most common substance (88%) that young people come to treatment for, the same proportion as the last 3 years.
Around 4 in 10 young people (44%) said they had problems with alcohol (compared to 46% the previous year), 14% reported ecstasy and 10% reported powder cocaine problems.
There was a slight increase in the number of young people seeking help for opiates such as heroin (216 young people compared to 187 last year), which is less than 1% of those in treatment.
There was a 53% increase in young people reporting a problem with benzodiazepines from the previous year, and 3 times the number in 2016 to 2017.
1.3 Mental health treatment need
Almost a third of young people (32%) who started treatment this year said they had a mental health treatment need, which is higher than last year (27%). A higher proportion of girls reported a mental health treatment need than boys (42% compared to 28%).
Most young people (73%) who had a mental health treatment need received some form of treatment for it, usually from a community mental health team.
1.4 Vulnerabilities among young people in treatment
The most common vulnerability reported by young people in treatment was early onset of substance use (77%), which means the young person started misusing substances before the age of 15. This was followed by poly-drug use (56%).
Proportionally, girls tended to report more vulnerabilities than boys, particularly self-harming behaviour (29% compared with 10%) and sexual exploitation (11% compared with 1%).
1.5 Treatment exits
Of the young people who left treatment, most (80%) left because they successfully completed the programme, which is slightly below the proportion the previous year (81%). The next most common reason for leaving treatment (13%) was leaving early or dropping out, which was slightly higher than the previous year (11%).
2. Young people in treatment: substance, sex, age
2.1 Overview
This National Drug Treatment Monitoring System (NDTMS) statistics report presents information about young people under the age of 18 who received specialist substance misuse treatment in England between 1 April 2018 and 31 March 2019.
2.2 Age and sex of young people in treatment
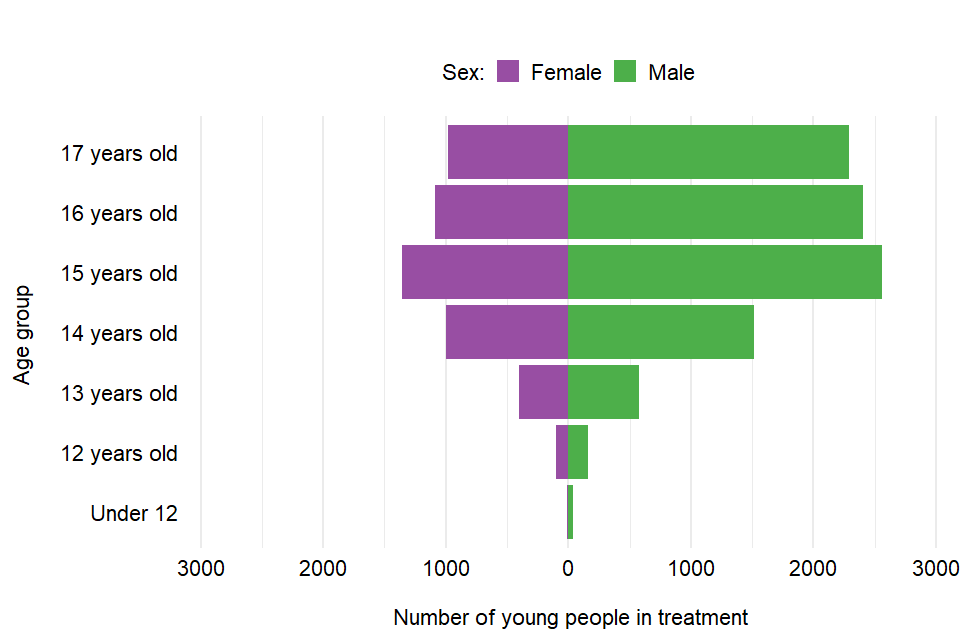
Bar chart showing the number of young people in treatment by sex and age group.
There were 14,485 young people in contact with drug and alcohol services in 2018 to 2019. Two-thirds were male (66%), which was the same proportion as the last 2 years. The median age for both male and female was 15 years old. The number of younger children (under 14) in treatment remained relatively low (9%).
3. Substance use by young people

Bar chart showing the number of young people in treatment and the substances they have problems with.
When young people enter treatment, they can record up to 3 substances that they have a problem with. The first substance is the ‘primary substance’ and the others are ‘adjunctive substances’.
There were 12,702 young people who said they had a problem with cannabis, either as a primary or adjunctive substance (88% of all in treatment), followed by 6,376 (44%) who said they had a problem with alcohol.
Fourteen per cent said they had a problem with ecstasy and 10% reported a problem with cocaine powder. There was a 53% increase in young people reporting a problem with benzodiazepines (483, up from 315 the previous year). The number is now 3 times what it was in 2016 to 2017 (161).
New psychoactive substances were reported by 137 young people, which is a 49% reduction from the previous year (270).
4. Referral routes into treatment

Bar chart showing the number of young people in treatment and the referral routes into specialist treatment services.
The most common route for young people to get into specialist treatment services was a referral from education services (such as mainstream education or alternative education). There were 4,940 (32%) young people who entered treatment this way.
Referrals from the youth justice system were the second largest source of referral (20%). Social care services accounted for 17% of referrals and health services referrals for 10%.
5. Vulnerabilities among young people in treatment

Bar chart showing the number of young people in treatment and the vulnerabilities they reported split by sex.
Young people often enter specialist substance misuse services with a range of problems or ‘vulnerabilities’ which are related to, or in addition to, their substance use. These include using multiple substances, having a mental health treatment need, being a looked after child or being not in education, employment or training (NEET). Other risk factors can affect their substance use, such as self-harming behaviour, sexual exploitation, offending or domestic abuse.
Vulnerabilities are reported here only for young people who entered alcohol and drug treatment services during 2018 to 2019.
The most common vulnerability was early onset of substance use (77%), which means the young person started misusing substances before the age of 15. This was followed by young people reporting poly-drug use (56%) and almost a third (32%) who had a mental health treatment need.
Proportionally, girls tended to report more vulnerabilities than boys, including self-harming behaviour (29% compared with 10%) and sexual exploitation (11% compared with 1%).
More than a third (37%) of young people report 4 or more vulnerabilities.
6. Sexual exploitation

Bar chart showing the number of young people reporting sexual exploitation by age group and sex.
The Department for Education has published guidance which defines child sexual exploitation (CSE):
Child sexual exploitation is a form of child sexual abuse. It occurs where an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child or young person under the age of 18 into sexual activity (a) in exchange for something the victim needs or wants, and/or (b) for the financial advantage or increased status of the perpetrator or facilitator. The victim may have been sexually exploited even if the sexual activity appears consensual. Child sexual exploitation does not always involve physical contact; it can also occur through the use of technology.
Overall, 4% of the young people who entered treatment reported CSE (compared with 5% the previous year). Of those who reported CSE, 10% of girls were under 14 years old compared with 13% of boys.
7. Mental health needs

Pie chart showing the percentage of young people in substance misuse treatment with a mental health treatment need and where they received this mental health treatment.
There were 3,364 young people who started treatment in 2018 to 2019 who said they had a mental health need, which was nearly a third (32%). This compares to 27% of young people who started treatment the previous year (2,954).
A higher proportion of girls reported a mental health treatment need than boys (42% compared to 28%). Most young people (73%) who had a mental health treatment need received some form of mental health treatment, usually from community mental health teams.
8. Treatment types

Bar chart showing the number of young people in treatment by the intervention type they received and the setting in which they received it.
Most young people who started a treatment intervention received psychosocial interventions (94%) during their time in treatment. These are ‘talking therapies’ to encourage behaviour change.
There were 8,805 young people (61%) who received structured harm reduction interventions. These include support to manage risky behaviour associated with substance misuse, such as overdose or accidental injury.
Only 49 young people (less than 1%) received a pharmacological intervention during treatment. These interventions involve medication prescribed by a clinician and include detoxification, stabilisation, relapse prevention and substitute prescribing for opiates.
Young people can receive more than one of the same treatment type in different settings.
9. Treatment exits

Pie chart showing the percentage of young people exiting the treatment system and the reasons for their exit.
Two-thirds (67%) of young people in treatment exited the treatment system. Of those who left, 80% successfully completed their treatment and 13% dropped out. A further 5% were referred to another provider for treatment and 2% declined the treatment offered.
10. Trends over time
10.1 Trends in age and numbers in treatment

Bar chart showing the trend over time of the number of young people in treatment split by age group.
The number of young people in specialist substance misuse services has fallen in each of the last 10 years, since a peak of 24,053 in the year 2008 to 2009. The number of young people attending services in 2018 to 2019 was 7% lower than the previous year and 40% lower than the peak.
10.2 Trends in primary substance misuse

Line graph showing the trends over time of the combined primary and adjunctive problem substances young people came to treatment for.
The number of young people in treatment who said that cannabis was their primary problem substance has been falling over the last 5 years, but the proportion has remained stable for 3 consecutive years at 77%.
The number who reported alcohol as their primary substance has fallen substantially since the year 2008 to 2009, when they made up 37% of those in treatment and was 14% in 2018 to 2019.
The number of young people who reported other drugs as their primary problem substance has remained relatively stable over the last 3 years.
Bar chart showing the trend over time of the number of young people in treatment split by age group.
The number of young people who said they had problems with cocaine declined substantially from a peak of 3,050 in 2008 to 2009 to around 1,500 in 2012 to 2013 but has remained relatively stable since then.
Young people reporting amphetamines increased rapidly from 2007 to 2008 until 2012 to 2013. It has since decreased each year and is now at a historic low (204).
The number of young people who reported ecstasy as a problem substance has been on an upward trend since 2011 to 2012 reaching a peak last year (2,112) and has fallen slightly in the last 12 months (1,967).
The number of young people who reported a problem with new psychoactive substances has fallen substantially from a peak of 1,056 in 2015 to 2016 and was at the lowest recorded level last year (137).
The number of young people reporting a problem with benzodiazepines has trebled since 2016 to 2017, rising from 161 to 483 this year.
11. Background and policy context
11.1 Background to the data
This report presents statistics on the availability and effectiveness of young people’s alcohol and drug treatment in England and the profile of those accessing this treatment.
The statistics in this publication come from analysis of the National Drug Treatment Monitoring System (NDTMS). The NDTMS collects data from sites providing structured substance misuse interventions to young people in every local authority in England.
The data collected includes information on the demographics and personal circumstances of young people receiving treatment, as well as details of the interventions delivered and their outcomes.
You can find more details on the methodology used in the report in the NDTMS annual statistics quality and methodology information paper.
11.2 Policy context
Specialist substance misuse services for young people are normally separate from adult treatment services because young people’s alcohol and drug problems tend to be different from adults’ and need a different response. This includes being child-centred, considering the age and maturity of young people, acting on safeguarding concerns and making sure the young people do not mix with adult drug users.
These services support young people, help them to reduce the harm their alcohol or drug use causes them and try to prevent it from becoming a bigger problem as they get older. Services should be part of a wider network of local prevention services, which support young people with a range of issues and help them to build their resilience.
Young people’s alcohol and drug treatment in England is commissioned by local authorities using the public health grant. They are responsible for assessing local need for treatment and commissioning a range of services and interventions to meet that need.
The public health grant conditions make it clear that:
A local authority must, in using the grant: have regard to the need to improve the take up of, and outcomes from, its drug and alcohol misuse treatment services.
Public Health England (PHE) works with local authorities and provides them with bespoke data, guidance, tools and other support to help them commission services more effectively.
PHE guidance for alcohol and drug treatment is available in the Alcohol and drug misuse prevention and treatment guidance collection.
A wide range of NDTMS data is available at the NDTMS website, including some data reports that are only available to local authority commissioners (via login).
The government’s strategy for drug treatment and prevention is set out in the ‘reducing demand’ and ‘building recovery’ sections in the Drug Strategy 2017.