
Annual Report for 2025
Published 23 June 2026

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/raib-annual-report-2025-published-2026/annual-report-for-2025
Our Purpose: We independently investigate accidents to improve railway safety and inform the industry and the public.
1. Chief Inspector’s review of 2025
2025 marked 20 years since RAIB became active on 17 October 2005. In that time, the railway has got safer by virtually all significant measures. When Lord Cullen recommended the setting up of RAIB, his report also recommended that the British rail industry have a separate standard‑setting body (now RSSB) and that safety regulation remain independent. The result was a tripartite safety structure: the regulator (ORR in Great Britain); RAIB, as accident investigator; and the industry, as duty holder – three independent parties, with a little bit of inbuilt conflict. That structure has delivered a huge safety benefit. While RAIB certainly cannot claim all the credit for a big improvement in safety over the last 20 years, we are an essential pillar of a structure that did, and continues, to deliver it. We can also see in many areas where an RAIB recommendation, made based on a detailed, impartial analysis of the evidence, has led to significant and lasting change. Over that time, we have achieved our mission to improve safety and inform.
However, 2025 has also been a year in which we have investigated a relatively high number of fatal accidents and some of those investigations remain ongoing. Every fatal accident has tragic and long-lasting consequences for those left behind and serves as a reminder that, even on our statistically ever-safer railways and tramways, there is always a need for vigilance and a need to learn.
All but one of those investigated accidents are referred to later in this foreword. The exception is the accident at Talerddig on 21 October 2024 (report 08/2026). This was a head-on collision of two passenger trains at around 30 mph, in which a passenger died after secondary impact with a table, and four people were seriously injured. The accident occurred on a single line stretch of railway, after a westbound train, which was supposed to stop in a passing loop, did not do so, and entered the single line on which an eastbound train was approaching. This was a result of the low levels of available wheel‑rail adhesion on an autumn evening, the westbound train’s sanding systems not operating and the westbound train’s approach speed to the passing loop. As with most accidents, behind this lay a number of significant underlying factors.

2025 has been a year of relatively low published output, primarily as a result of taking on fewer investigations in 2024. However, the number of investigations started, and which will result in reports published in 2026, is relatively high.
This report summarises the work of the Branch in 2025. Five main themes have run through our investigative activity and these are outlined below.
1.1 Track worker safety
Network Rail has moved away from track work being carried out on, or close to, open lines using unassisted lookouts for protection. This is positive and has made track work statistically safer. However, a level of near miss incidents persists, albeit lower than in the era of lookouts.
More maintenance tasks are now being undertaken by staff working on lines blocked to traffic. This should be inherently safer than lookout working and the statistics bear that out. In such systems, the understanding of which lines are blocked, the limits of the safe working area, when lines are blocked, how the blocked lines are to be safely accessed and the exact locations of work groups is critical. Near misses at Chiltern Green (report 06/2025), Morton Junction (safety digest 02/2025), Bookham Tunnel (report 07/2026), London Bridge (safety digest 06/2025) and Millbrook (safety digest 04/2026) graphically illustrate how close to being killed track workers can come as a result of not having that understanding. Safety theory tells us, as does past experience with track worker accidents, that a string of near misses will ultimately lead to an accident. This has recently been tragically illustrated by the death of a track worker, struck by a train at in Hertfordshire in March 2026, which is currently under RAIB investigation. For all the parameters of a line blockage to be fully understood, and correctly acted upon by track workers, requires consistently high levels of planning, supervision and management assurance.
Although not working on the track, a shunter, who had moved out of sidings to conduct shunting operations, was nearly struck by a passing train at Washwood Heath (under investigation).
1.2 Platform safety
In times past, the majority of accidents and incident that made up this Annual Report theme involved passengers becoming trapped in train doors and dragged and Chief Inspector Forewords have discussed the issue extensively. This year we have only investigated one such incident, at Ealing Broadway (report 01/2026). Issues included the platform layout which, being platform specific, illustrates, once again, that platform‑train interface risk has to be comprehensively managed on a platform-by-platform basis.

Sadly, we have investigated two accidents where people fell onto the track and were stuck by trains sometime later and were killed. At Stratford, on London Underground’s Jubilee Line (report 01/2025), the issue of attention levels in operators of automatic trains was raised. As more tasks become automated, we will need to get better at understanding the relationship between the human and the machine. Automation is naturally undertaken on a cost-benefit basis and that often means the parts of a task that are difficult to automate get left to a human. Yet it is known that humans are not suited to being under-stimulated while supervising an automated task and then having to quickly adapt to perform critical tasks. This will need careful consideration in many parts of the railway and London Underground has started to do this.
At Ickenham (report 02/2026), CCTV evidence suggests that the passenger, who had fallen onto the track, was aware that a train was approaching and was probably attempting to move towards the platform face and out of the path of the train. However, the under-platform recess was occupied by communication cables and this meant that there was insufficient space to accommodate the passenger and to allow a train to pass without contacting them. RAIB identified two underlying factors. The first, a probable underlying factor, was that London Underground’s standards relating to under-platform recesses were not being complied with and were not consistent with each other. The second, a possible underlying factor, was that London Underground had not completed platform-specific risk assessments for most platforms on its network or identified the safety benefit of some measures intended to mitigate the risk of people falling from platforms and subsequently being struck by trains.
At Crossacres Tram stop on Manchester Metrolink, an 11-year-old child became trapped between the platform and a departing tram. The child was then dragged along the platform, suffering life-changing injuries as a result. Our investigation into this accident is ongoing.
At Norwood Junction (report 09/2026), a train departed with a manual access ramp still attached to it. These ramps are used to facilitate boarding and alighting for mobility scooters and wheelchairs and should be removed before trains depart. The access ramp involved had been attached at a doorway by platform staff to assist a passenger in a mobility scooter, who was planning to board the train. The driver of the train was not aware that the access ramp was attached when they closed the doors, and the train departed with it still attached.
No one was on the ramp as the train started to move. The access ramp was dragged along the platform where two members of staff and a member of the public took action to avoid it. No one was injured. One cause was that the driver was using a mobile phone at the time of the incident. This is not the first time RAIB has investigated non‑compliant phone use by train drivers that resulted in an accident.
1.3 Asset integrity
The derailment of a passenger train travelling at 56 mph (90 km/h) at Grange‑over‑Sands (report 02/2025) was a result of the collapse of an embankment.
I said at the time that ‘Derailments of passenger trains are thankfully rare. The elements that came together and led to the derailment at Grange-over-Sands include some factors that have been seen in previous RAIB investigations. In this case Victorian infrastructure, increasing rainfall, a known flood water management problem which multiple parties had not fully resolved over years, ineffective communication and a short-term fix effectively becoming the permanent solution all played a part. As the railway’s infrastructure will continue to age, and given the challenges of climate change, the importance of avoiding the other factors is ever more vital if such derailments are to remain a rarity’.
That the railway has to react to mitigate the risk of climate change and ageing assets is self‑evident. But climate change and asset age also make the world in which the railway operates less forgiving of not getting day-to‑day things, such as effective communication and timely repair of faults, right.
At around 06:20 on 3 November, we received a first report that a passenger train had derailed at Shap having hit something at speed. There was no other detail then and my mind went back to the fatal accident at Grayrigg nearly 20 years ago because of the Cumbrian location. After a while, it thankfully became clear that any injuries were minor and that the train had struck a landslip that had occurred after heavy rainfall. My mind then moved to the multi-fatal derailment at Carmont 5 years previously.

At Carmont, a drain had not been constructed properly and heavy rain washed stone used as part of the drain onto the track. At Shap, drainage had been overwhelmed leading to water entering a cutting slope and causing the landslip. Network Rail has put a lot of thought and work into this area as a result of the accident at Carmont and the recommendations that stemmed from it. However, while the RAIB investigation into the Shap derailment continues, we issued urgent safety advice in December 2025 that lineside monitoring equipment used on Network Rail managed infrastructure may not be able to detect the failure of slopes in some circumstances. As a result, this equipment may not provide data as expected to support safety decision-making, particularly during extreme weather conditions.
1.4 Level crossings
Level crossings have not featured as a theme in the last two years’ Annual Reports. However, 2025 was marked by a significant number of level crossing accident investigations. A child was killed at Bourneview footpath crossing (report 08/2025) near Croydon; a young person was killed at Chestnut Grove footpath crossing near Nottingham (under investigation); a van driver was killed at Bax user worked level crossing in Kent (under investigation); and an older person was killed while crossing Pewsey footpath crossing in Wiltshire (report 05/2026). Additionally, in early 2026, a young person was killed on a level crossing at Bottesford, which is also subject to an RAIB investigation, and a number of similar accidents have occurred where RAIB decided to produce a note for the coroner, rather than a full investigation. The exact circumstances of each of these tragic events are different, but they illustrate the inherent risk associated with passive crossings. There still remain a large number on the railway network, despite efforts by the railway to reduce their numbers by closure or adding active protection.
At Redcar full barrier level crossing (report 05/2025), a car was struck by a train when both entered the crossing with the barriers open, at Nordan Farm user worked crossing near Hereford (report 06/2026), an agricultural trailer was struck by a passenger train, and at Helpston automatic half barrier crossing near Peterborough (safety digest 01/2026), barriers were raised in front of road users as a freight train entered the crossing. While the causes vary, in each case actions by the controlling signaller led to an unsafe situation, leading to questions around training, competence and management supervision.
Tramways are not immune from such accidents. At Staniforth Road in Sheffield (investigation ongoing), a young person was seriously injured by a tram as they were out jogging with a friend. The crossing has been the location of a number of previous accidents, including one that was investigated by RAIB (report 01/2006).
1.5 Overspeeding
In the 2024 Annual report, I referred to two overspeeding events at Spital Junction near Peterborough in the context of not learning lessons from incidents. The first in 2022 (report 06/2023) resulted in a train almost overturning at high speed. This was followed by an almost identical incident at the same place in 2023 (Urgent Safety Advice 02/2023 and report 10/2024). The immediate cause of the incidents was train drivers responding incorrectly to junction indicators when signals were approach released to green in front of them, and consequently accelerating high‑performing trains as if routed straight through the upcoming junction. When the trains reached the junction, they were exceeding the diverging route speed by two to three times.
A similar incident occurred at Manor Park, Essex, in September 2024 (safety digest 01/2025) and again at Grantham South Junction, Lincolnshire, in February 2025 and, given the similarities to the Spital incidents, and the two completed investigations with open recommendations, we wrote to the Safety Regulator (ORR) in response to this incident. We drew the Regulator’s attention to the fact that, ‘this incident again illustrates the issues associated with relying completely on train drivers reacting appropriately to a junction or route indicator to control the risks presented by trains taking diverging low-speed turnouts on high-speed through routes. This risk may be increased by the introduction of higher performing train fleets, and possibly by routing patterns on an ever-busier railway’.
In September 2025, a second similar incident occurred at Grantham South Junction (safety digest 05/2026) and another occurred at Cambridge Junction, Hertfordshire, in December 2025 (safety digest 02/2026).
The Safety Regulator has responded to our letter, is aware of the risk and is taking action to push the various parts of the railway industry to sufficiently control the risk. I refer to this issue again in my concluding thoughts.
Another type of overspeeding event that RAIB has investigated in recent years is drivers not obeying blanket temporary speed restrictions, usually placed in response to adverse weather, as a result of not being aware of them. Safety digest 03/2025 explains a series of overspeeding events in south Wales of this type.
1.6 Concluding thoughts
There are three related points I would like to make.
Firstly, it is noticeable that, over the past years, a number of themes of RAIB investigations recur. Track work, platform-train interface, level crossings and asset integrity are examples. This is perhaps to be expected. Level crossings and platforms are places where the public can be exposed to moving trains. Level crossings carry inherent levels of risk, even after mitigations, and closure can be difficult and replacement with bridges, expensive. The climate is changing and assets are getting older. These are genuine reasons why risks can be more difficult to manage in these areas, but this must not be allowed to lead to an acceptance of inevitability. In the area of track worker safety, Network Rail has shown that significant reductions in near misses can be achieved with radical change and as technology improves, levels of risk will drop further. Perhaps that also gives a clue as to how other, seemingly intractable, issues can stop becoming repeated RAIB themes. More radical thinking by the industry and other involved parties, and the application of technological advances will be important.
RAIB Annual Report themes give a snapshot of the accidents RAIB has dealt with over a given year. The presence, or not, of a theme, is not an accurate indicator of risk associated with a given part of railway or tramway operations. The re-emergence of level crossing investigations this year, after very few in the previous 2 years, echoes the re-emergence of track worker accidents in 2017, after a period with no fatal accidents involving track workers.
This leads to the second point. In areas where high-consequence accidents are relatively rare, but where there are many near misses, probably under-reported, the distribution of tragic accidents can appear random. But this reinforces the theory which correctly holds that an absence of high‑consequence accidents is not necessarily an indication of safety. This does not just apply to level crossings and track worker safety, it is a general principle. I hope the potential for this to apply now in relation to overspeed events is recognised by the industry. Universal fitment of automatic train protection in the UK is a very long way off. In the meantime, we cannot just hope that the current spate of overspeed events, with relatively benign outcomes, will always be benign.
Thirdly, the advent of Great British Railways will have the potential for different parts of the railway to work more co‑operatively and holistically together on shared risks, such as overspeeding. However, such an improvement is not a given; many large organisations work in silos. It will require active high-level managerial effort to reap the full potential safety benefits.
To conclude, I would like to thank all those who have assisted RAIB in our first 20 years. In that time, RAIB attended 777 accident sites, undertook 427 full investigations and 138 short investigations, made 1892 recommendations and generated 725 learning points. That would not have happened as successfully as it did without help and co‑operation from the railway and tramway industries, safety regulators, DfT and the emergency services. We have also been greatly assisted by the individuals involved in, or affected by, accidents, who often talk to us at a time of grief or stress in their lives. I would also like to recognise the dedication and expertise of my colleagues in the branch now, and those who preceded them over the previous two decades.
This is my fifth and final Chief Inspector’s review as I intend to retire in the autumn, after over 22 years with the Branch. This has not been an easy decision. I have been very lucky, both because of the nature of the work we do, and the people I have worked with and met. It has indeed been a privilege and to all those in the Branch now and since its inception, I will always be grateful.
Andrew Hall
Chief Inspector of Rail Accidents
June 2026
2. Operational activity
The Railways (Accident Investigation and Reporting) Regulations 2005 (the Regulations) govern how RAIB investigates accidents and incidents on the UK’s rail and tramway network. The regulations detail those accidents and incidents which the railway and tramway industries are required to report to us.
Between 1 January and 31 December 2025, we received 488 notifications. From these we conducted 54 preliminary examinations to determine the course of action required. This resulted in 16 becoming full investigations, with a further 8 becoming safety digests. A further 5 of these preliminary examinations lead to us starting industry reviews, with 7 more being closed by writing to the coroner. We concluded that 16 preliminary examinations required no further action. In addition, we wrote 2 letters to industry advising them of the preliminary examination, how it related to previous accidents and why we were not going to investigate. The writing of such letters and their broad content is published on our website.

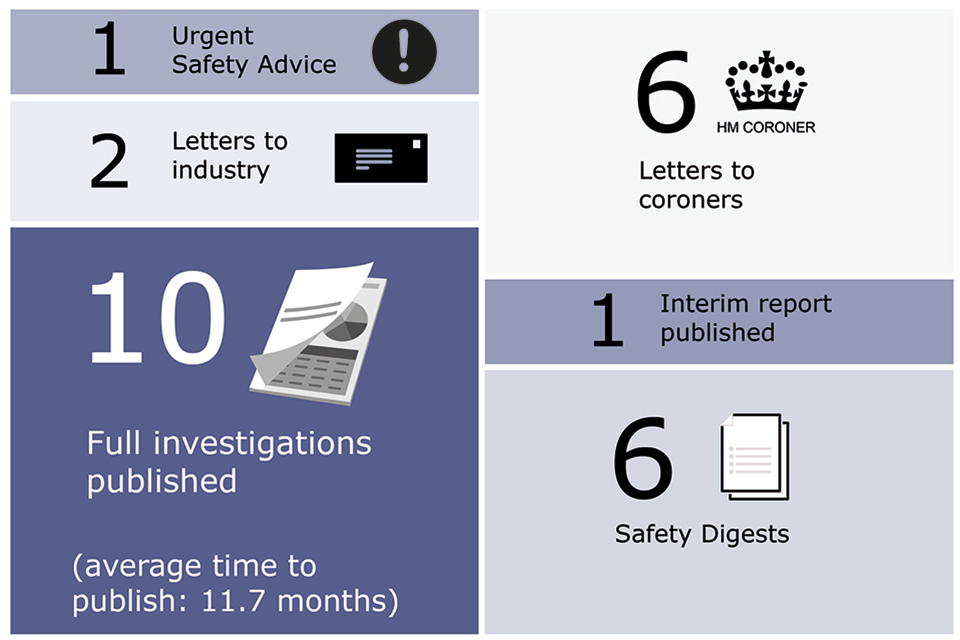
In 2025 we published 10 full investigation reports. The average time to publish these was 11.7 months. We also published 6 safety digests, issued an urgent safety advice to the industry, and published an interim report as an update to an ongoing investigation. In addition to these publications, we wrote 6 letters to coroners, as well as 2 letters to industry.
2.1 Accidents investigated by RAIB
RAIB has a duty to investigate all serious railway accidents as defined by the Regulations. These include derailments and collisions of rolling stock resulting in the death of one person, serious injuries to five or more people, or extensive damage to rolling stock, infrastructure or the environment.
We are also required to investigate incidents and accidents which, under slightly different circumstances, could have led to a serious accident, or which have an obvious impact on railway safety regulation or the management of safety.
We may investigate other notifiable railway accidents where an investigation will improve safety.
If we identify that the safety learning from an accident or incident is widely applicable, but we have previously investigated, or it is primarily about compliance, we may choose to produce a safety digest. This is shorter than a full investigation report which identifies safety learning but does not contain recommendations.
During the 5-year period 2021 to 2025, we undertook 104 full investigations and safety digests. Twenty-four of these involved railway employees and moving trains, including accidents involving track workers. Nineteen involved passengers and moving trains (such as a passenger trapped in train doors and dragged).
We also investigated thirteen unauthorised train movements, ten derailments (seven involved passenger trains and three involved freight trains), ten collisions with obstacles and seven collisions with other trains. A further ten involved harm, or the risk of harm, to people at level crossings, and five were runaway incidents. Three involved failures of infrastructure and two involved train defects.
| Categories | Full investigations | Safety digests |
|---|---|---|
| Events involving moving trains (staff) (24) | 10 | 14 |
| Events involving moving trains (passengers and members of public) (19) | 13 | 6 |
| SPADs or unauthorised train movements (13) | 6 | 7 |
| Level crossing accidents and near misses (10) | 7 | 3 |
| Collisions with an obstacle (10) | 5 | 5 |
| Collisions with other trains (7) | 6 | 1 |
| Passenger train derailments (7) | 6 | 1 |
| Runaway incidents (5) | 4 | 1 |
| Freight train derailments (3) | 3 | 0 |
| Infrastructure failures (3) | 3 | 0 |
| Out-of-gauge train collisions (2) | 1 | 1 |
| Train defects (2) | 2 | 0 |
2.2 Northern Ireland and the Channel Tunnel
While we did not deploy to Northern Ireland in 2025, nor publish any reports relating to accidents there, we continue to liaise with Northern Ireland Railways (NIR) and the safety regulator, Department for Infrastructure (NI), on matters relating to accident investigation and safety learning.
There were no RAIB deployments to the Channel Tunnel or investigation activity related to it in 2025.
We continue to maintain good working relationships with our adjoining counterparts in the Republic of Ireland (Railway Accident Investigation Unit; RAIU), and France (the Bureau d’Enquêtes sur les Accidents de Transport Terrestre; BEA-TT), and with the relevant infrastructure managers, railway undertakings, and safety authorities.
Memoranda of Co-operation (MoC) with RAIU and BEA-TT remain in place covering joint working in the event of a cross-border accident.
On 9 April 2025, the UK and French governments signed a treaty establishing a new regulatory framework for the Channel Tunnel. The new framework sets out updated governance arrangements and safety and interoperability requirements for railway operations and rail accident investigation in the Channel Tunnel.
The Government plans to bring forward legislation to give legal effect to the treaty in UK law, after which the provisions in the treaty and the new regulatory framework established by it will come into effect.
Currently, regulatory supervision of the Channel Tunnel is undertaken by the Intergovernmental Commission (IGC) (for the UK part) and the Établissement Public de Sécurité Ferroviaire (EPSF) (for the French part), with the latter having transferred from IGC to EPSF as a result of the UK’s departure from the EU.
Once the treaty takes effect, supervision and safety permissioning functions will transfer to the ORR which will assume the role of safety authority for railway safety matters in the UK half of the Channel Tunnel, while EPSF will be the safety authority in the French section.
Under the new framework, the RAIB will continue to be the accident investigation body in the UK section, whilst the Bureau d’Enquêtes sur les Accidents de Transport Terrestre (France’s land transport accident investigation body) will be responsible for accident investigation in the French section.
The treaty will require the Accident Investigation Bodies to investigate serious incidents and near misses in the Channel Tunnel in their respective sections, and to co‑operate in deciding whether investigations should be conducted jointly or separately, including by participating in and supporting each other’s investigations.
3. Recommendations
The purpose of our recommendations to industry and other bodies is to improve railway safety. Our recommendations aim to reduce the chance of a similar accident occurring, or to reduce the consequences if such an event were to happen again.
When making recommendations, we identify those organisations we consider best placed to implement changes or safety improvements. These organisations are known as ‘end implementers’. They include railway, non-railway, private, and public sector bodies.
The majority of our recommendations are addressed to the relevant safety authority. For railways in Great Britain this is ORR while in Northern Ireland it is the NI Department for Infrastructure (which is advised by the Health and Safety Executive NI). The safety authority for the UK part of the Channel Tunnel system is the Intergovernmental Commission until the new regulatory framework comes into effect.
If a recommendation relates to an organisation not regulated by the railway industry’s safety authority it can be addressed to any other public body as required.
The law requires that the safety authority ensures end implementers consider our recommendations and act on them where required. The Regulations require end implementers to provide full details to the safety authority of the measures they intend to take, or have taken, to implement the recommendation.
The safety authority is required to consider each recommendation and action as appropriate. It should also inform us of any measures taken in response to the recommendation, or the reasons why no measures have been taken.
We collect information on actions taken in response to our recommendations. This information is generally based on reports we receive from the safety authority (usually ORR). Any public bodies which are the recipients of our recommendations are required to respond directly to us.
3.1 Current status of RAIB recommendations
We provide updates on the status of each recommendation in our (index of RAIB recommendations). The index provides information as supplied to us by the relevant safety authority or public body. Each entry is linked to a recommendation status response that provides the full text of each recommendation.
Responses to recommendations are currently categorised as follows:
Open: Actions to address the recommendation are ongoing.
Closed: ORR considers the recommendation to have been taken into consideration by an end implementer and evidence provided to show action taken or justification for no action taken.
Insufficient response: The end implementer has not provided sufficient evidence that the recommendation has been taken into consideration, or if it has, the action proposed does not address the recommendation, or there is insufficient evidence to support no action being taken.
Superseded: The recommendation has been superseded either by a newer recommendation or actions have subsequently been taken by the end implementer that have superseded the recommendation.
Other recommendations not yet reported on are categorised as ‘Awaiting response’.
3.2 2025 Recommendation distribution
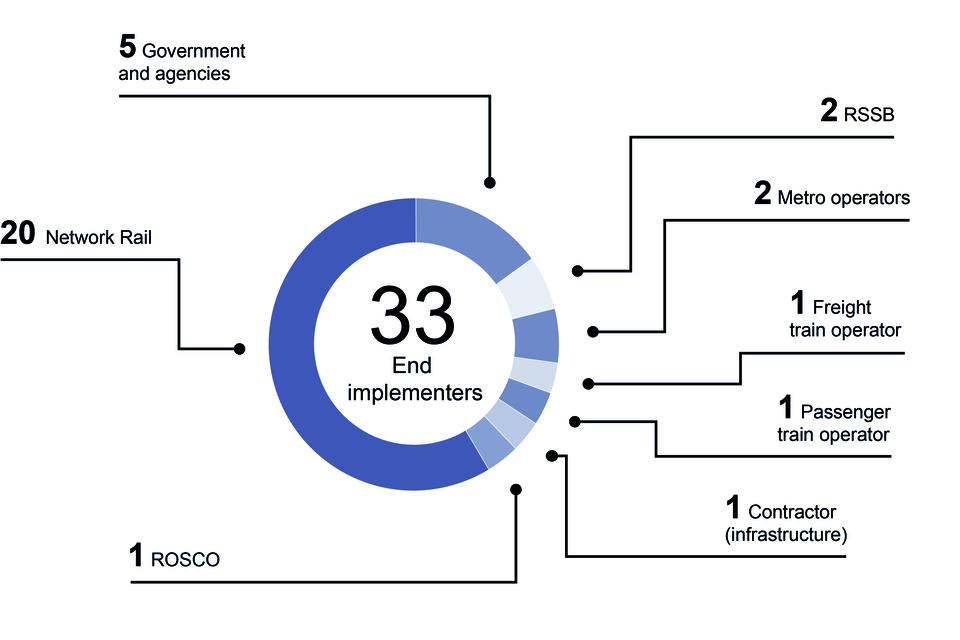
In 2025, we made 31 recommendations with 33 end implementers. These included Network Rail, London Underground, passenger operators, light rail operators, freight train operators, central government and local government.
3.3 Recommendations
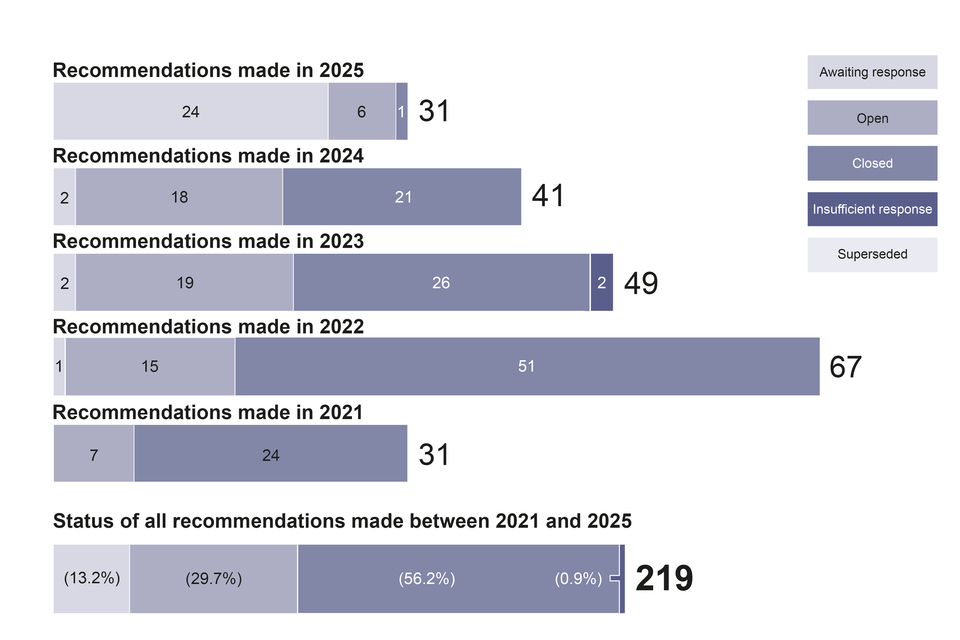
Between 2021 and 2025, we made 219 recommendations. The status of these recommendations as reported to us was:
- For 13.2% of recommendations, the safety authority is yet to receive a response from the end implementer (‘awaiting response’).
- For 29.7% of recommendations, the safety authority or public body considers that actions to address the recommendation are ongoing (‘open’).
- For 56.2% of recommendations, the safety authority or public body considers the recommendation to have been taken into consideration by an end implementer and evidence provided to show action taken or justification for no action taken (‘closed’).
- For 0.9% of recommendations, the safety authority or public body considers that the response received from an end implementer is insufficient (‘insufficient response’).
No recommendations have been reported as being superseded.
Status of recommendations by the year that they were made (as reported to RAIB by 31 December 2025):
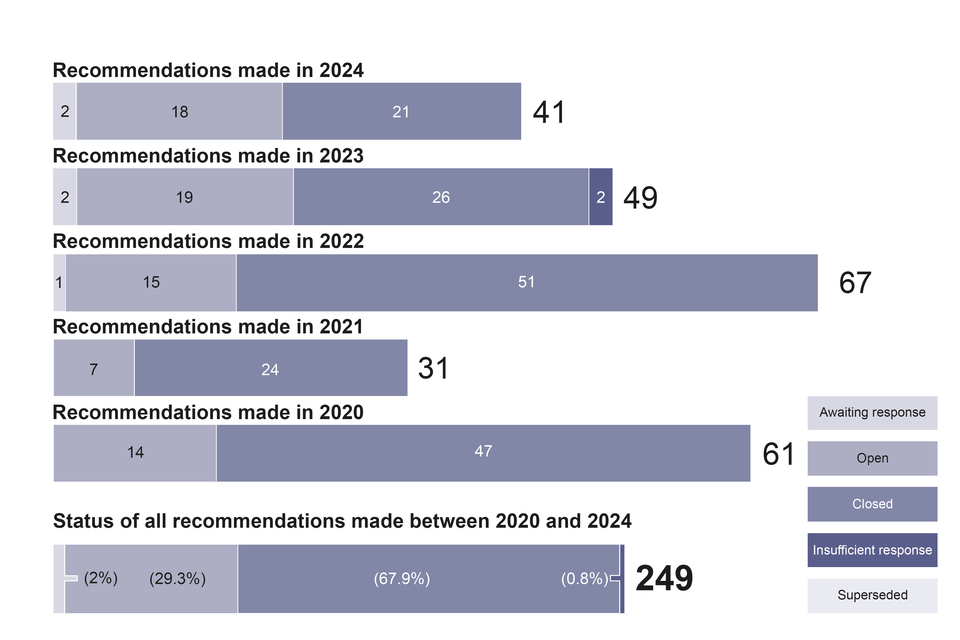
In the 5-year period from 2020 to 2024 (that is, those recommendations more than one year old on 31 December 2025) 67.9% of them have been reported as closed.
3.4 Areas of concern to RAIB
We receive updates on the status of each recommendation from the safety authority, or public body to whom our recommendations are addressed. On occasion, after receiving this response, we may have concerns either about how the organisation has responded to the recommendation, or because of the information we receive from the safety authority.
When this happens, we will discuss our concerns with the safety authority or public body before recording any remaining concerns in the following year’s annual report.
If we have concerns regarding any actions taken in response to our recommendations, we highlight them using the following categorisation:
Red – we have concerns that no actions have been taken in response to a recommendation.
Blue – we are concerned that the actions taken are inappropriate or insufficient to address the risk identified during the investigation.
White – we note that substantive actions have been reported but we still have concerns about the underlying risk.
Report 12/2023 - Collision between passenger trains at Salisbury Tunnel Junction
Recommendation 5 – White
Intent of recommendation – The intent of this recommendation is for Network Rail to improve wheel-rail adhesion conditions through the application of improved understanding of the effectiveness of railhead treatment regimes.
ORR status – Closed
RAIB concern – ORR reported that, in response to this recommendation, RSSB undertook knowledge search S381 ‘An overview on wheel/rail contamination and railhead treatments’.
This research found that the high-pressure water jets used on the rail head treatment train fleet is currently the most effective control. The research also found a lack of a consistent testing methodology for railhead treatment methods and products and that the impact of different treatments and methods when used together was not well understood. Network Rail plans to conduct laboratory tests of different treatment methods and products, with consideration given to the impact of using different treatments together.
ORR considers the research to be detailed and thorough and reported that Network Rail has circulated the research report to its routes and operations functions, with a request that it be considered as best practice. ORR are supportive of the work done so far and will continue to pursue the appropriate implementation of the findings, via their business-as-usual interactions with Network Rail. ORR considered that the requirements of the recommendation have therefore been achieved.
Substantive actions have been taken in response to this recommendation, with RSSB undertaking the research discussed above. However, part C of recommendation 5 concerned undertaking research to better understand the effectiveness and longevity of railhead treatment regimes. While RSSB’s research concluded that there is some useful data on the effectiveness of railhead treatment regimes, data on the longevity of such treatments was found to be more limited. Further trials were seen as necessary to compare the effectiveness of current and future products and materials. The response does not explain how research with conclusions of this nature can be used to support Network Rail seasons delivery specialists in decision-making relating to the necessary frequency of railhead treatment and understanding the impact of missed or delayed treatment.
For these reasons, RAIB remains concerned about the underlying risk which this recommendation sought to address.
Report 12/2023 - Collision between passenger trains at Salisbury Tunnel Junction
Recommendation 7 – White
Intent of recommendation – The intent of this recommendation is to reduce the risk of overrunning signals at danger where there is a line speed change on the approach after the preliminary caution signal.
ORR status – Closed
RAIB concern – To be considered in TPWS installation design, a speed change on approach to a signal must occur more than 450 metres on approach to it. Technical Instruction TI022 ‘Provision of TPWS at signals’ later extended this to 800 metres to improve TPWS effectiveness for trains approaching at higher speeds. Network Rail did not apply TI022 retrospectively to existing TPWS installations, including signal SY31, which was protecting Salisbury Tunnel Junction before the collision. This recommendation asked Network Rail to review this decision.
ORR has reported that Network Rail has closed the recommendation on the basis that a network-wide programme of retrospective application of TI022 would not be reasonably practicable. ORR obtained further evidence as to the cost-benefit analysis used to support this decision.
Network Rail stated that the retrospective application of TI022 is done where a reasonable opportunity arises, typically as part of wider renewal scheme. Network Rail reported that it has re-evaluated previous calculations for signal SY31 and concluded the TPWS in this instance was in the optimum position.
Although Network Rail has undertaken a substantive action in response to this recommendation RAIB is concerned that the underlying risk which this recommendation sought to address remains.
4. Summaries of learning
Our investigations have allowed us to gather detailed insights into a range of accidents and their associated causal factors. Using this information, we have identified recurring themes and have shared this information with the industry in the form of summaries of learning documents.
We regularly review these themes and will update them based on our latest investigations.
The current themes we have identified are:
1 - Design and operation of user worked level crossings
2 - Protection of track workers from moving trains
3 - Managing risk at the platform-train interface
4 - Safe management of abnormal train-operating events
6 - Safe design, operation and maintenance of on-track plant and trolleys
7 - The safe management of weather-related events which affect train operation
8 - The integrity of train braking systems
9 - Wrong side failures of signalling
10 - Management assurance
Where appropriate, these have been updated to incorporate learning from 2025.
For 2025, we have added a further topic:
11 - Overspeeding
You can read each of the summaries of learning at: https://www.gov.uk/government/collections/summaries-of-learning
5. Safety and funding
5.1 RAIB’s own safety record
We aim to have the highest standards for health, safety, and wellbeing in all aspects of our operations. We continually review our processes, and apply any lessons learned from attending site to improve our safety management. We regularly review our office practice and update our health and safety governance arrangements, incorporating learning from accidents and incidents. No accidents were recorded in 2025.
We work closely with external partners, particularly the Air and Marine Accident Investigation Branches. Sharing common lessons learnt and best practice across work areas such as health, safety and wellbeing helps keep both our own team, as well as those we work with, as safe as possible.
5.2 Funding
Our operating budget for the 2024 to 2025 financial year was approximately £6.1 million.
6. Other activities
6.1 External events
Throughout 2025, we have participated in a number of different events. Engaging with organisations and different bodies in this way allows us to fulfil our aim of informing the industry and public.
These include lecturing at the Police College, the Railway Engineering Institution (RailEI) formerly known as Permanent Way Institution, Cranfield University, Heritage Rail Association, and the British Transport Police among others,
Topics covered included: how we investigate, track engineering, earthworks and drainage, and family liaison.
2025 also marked the 200th anniversary of Britain’s railways. We were pleased to be invited to the Greatest Gathering celebrations in Derby as well as providing guest speakers.
Find our more about our previous presentations
6.2 Rail accident investigators’ good practice seminar
In November 2025, we held our annual Railway Accident Investigators’ Seminar which broadly coincided with the 20th anniversary of RAIB’s formation. This marked the seventh such event.
Along with welcoming colleagues from across the rail industry, we heard guest speakers from Network Rail, Eurostar, RSSB and Transport for London, as well as presentations from our own inspectors. Subjects included investigating failure, just and fair investigations, safety-critical communications, human performance factors, and family liaison strategies. You can read these presentations on our website.
6.3 Working with academia
University collaboration continues to play an important role within the RAIB, deepening our understanding of the latest specialist findings relevant to accident investigation and delivering industry-focused teaching at various institutions.
This year has seen an ongoing relationship with the University of Sheffield in training of inspectors in the understanding and quantification of low adhesion. We have delivered teaching seminars at the University of Derby around the forensic aspects of accident investigation, and academics have presented their latest finding in the area to the three accident investigation branches. We have continued to support specialist courses in accident investigation at Cranfield University and have played a part in guiding the future of university courses with industrial advisory roles at Loughborough University, Cranfield University and the University of Derby.
6.4 International relations
RAIB has been a longstanding member of the International Transportation Safety Association (ITSA). ITSA is an international network of heads of independent safety investigation bodies, covering all modes of transport, including aviation, marine, railways, road transport, pipelines, and underground infrastructure. It has established a Railway Accident Investigators International Forum of which we are also a member. ITSA membership includes major investigation bodies across five continents, such as the NTSB in the USA and the ATSB in Australia.
Separately, RAIB continues to maintain mutually beneficial relationships with the EU National Investigation Bodies (NIB) and the European Rail Agency. We attend NIB plenary meetings three times per year and sit on three subject specific task groups in an advisory capacity, including one on peer review of other NIBs. In 2025, for the first time, RAIB was peer reviewed by other European NIBs. This resulted in a positive review with no suggested actions.
As in previous years, RAIB received a number of requests for advice or assistance from investigation bodies around the world and, if resource allowed, provided it.
6.5 The Accident Investigation Chiefs’ Council
The Accident Investigation Chiefs’ Council (AICC) comprises a non-executive chair and the Chief Inspectors from the Air, Marine and Rail Accident Investigation Branches.
AICC aims to enhance co-operation between the Air, Marine and Rail Accident Investigation Branches. It seeks to achieve this through encouraging collaborative working practices and promoting effective working arrangements with external bodies to improve RAIB’s effectiveness and efficiency.
Find out more about the role of AICC and its terms of reference at: GOV.UK and search AICC.
7. Table of investigations started, ongoing and published 2025
(Items prefixed with the letter ‘SD’ are safety digests, the remainder are full investigations)
| Event (National Network unless stated otherwise) | Event date | Published | Occurrence type |
|---|---|---|---|
| SD – Overspeeding at Cambridge Junction | 11/12/2025 | 14/04/2026 | SPAD or unauthorised train movement |
| Fatal accident at Chestnut Grove footpath crossing | 26/11/2025 | n/a | Train movement event involving passengers / pedestrians |
| Derailment of a passenger train at Shap | 03/11/2025 | n/a | Passenger train derailment |
| SD – Near miss at Helpston level crossing | 21/10/2025 | 09/03/2026 | Level crossing event |
| Serious injury to a child at Crossacres tram stop | 07/10/2025 | n/a | Train movement event involving passengers / pedestrians |
| SD – Overspeeding at Grantham South Junction | 26/09/2025 | 06/05/2026 | SPAD or unauthorised train movement |
| SD – Near miss between a passenger train and a van near Millbrook | 25/09/2025 | 16/04/2026 | Train Movement Event involving staff |
| Near miss with ground staff at Washwood Heath | 18/09/2025 | n/a | Train Movement Event involving staff |
| SD – Collision with footbridge on the Dean Forest Railway | 14/08/2025 | 26/11/2025 | Out of gauge train collision |
| Near miss involving a member of staff on the Bluebell Railway | 09/08/2025 | n/a | Train Movement Event involving staff |
| SD – Near miss with staff at London Bridge | 30/07/2025 | 23/12/2025 | Train Movement Event involving staff |
| Collision between a train and a van at Bax user worked level crossing | 13/07/2025 | n/a | Level crossing event |
| Near miss with an access ramp at Norwood Junction station | 01/07/2025 | 22/06/2026 | Out of gauge train collision |
| Derailment at Denbigh Hall South Junction | 26/06/2025 | 13/04/2026 | Passenger train derailment |
| Pedestrians struck by a tram at Staniforth Road | 22/06/2025 | n/a | Train movement event involving passengers / pedestrians |
| Collision between a train and an agricultural trailer at Nordan Farm user worked level crossing | 22/05/2025 | 21/05/2026 | Level crossing event |
| Near miss with track workers at Bookham Tunnel | 29/04/2025 | 15/10/2026 | Train Movement Event involving staff |
| SD – Person struck by train on Gartell Light Railway | 17/04/2025 | 22/07/2025 | Train Movement Event involving staff |
| Fatal accident at Ickenham station | 28/03/2025 | 05/03/2026 | Train movement event involving passengers / pedestrians |
| Two track workers struck by a wagon at Port Glasgow | 15/03/2025 | 24/03/2026 | Train Movement Event involving staff |
| Fatal accident at Pewsey footpath crossing | 26/02/2025 | 07/05/2026 | Train movement event involving passengers / pedestrians |
| SD – Trains overspeeding in south Wales | 27/01/2025 | 10/06/2025 | SPAD or unauthorised train movement |
| Fatal accident at Bourneview footpath crossing, Kenley | 23/01/2025 | 04/11/2025 | Train movement event involving passengers / pedestrians |
| Buffer stop collision at London Bridge station | 13/12/2024 | 17/12/2025 | Collision with an obstacle |
| SD – Near miss with track workers at Morton Junction | 27/11/2024 | 01/04/2025 | Train Movement Event involving staff |
| Trap and drag accident at Ealing Broadway | 24/11/2024 | 04/03/2026 | Train movement event involving passengers / pedestrians |
| Collision between passenger trains near Talerddig | 21/10/2024 | 18/06/2026 | Collision between trains |
| SD – Overspeeding incident near Manor Park | 24/09/2024 | 27/01/2025 | SPAD or unauthorised train movement |
| Derailment of a freight train at Audenshaw | 06/09/2024 | 24/12/2025 | Freight train derailment |
| Runaway of a trolley and subsequent collision at North Rode | 26/05/2024 | 01/05/2025 | Runaway incident |
| Passenger train collision with a road vehicle at Redcar level crossing | 01/05/2024 | 03/04/2025 | Level crossing event |
| Track worker near miss at Chiltern Green | 23/04/2024 | 17/04/2025 | Train Movement Event involving staff |
| Derailment of a passenger train at Grange-over-Sands | 22/03/2024 | 28/01/2025 | Passenger train derailment |
| Derailment of a passenger train near Walton-on-Thames | 04/03/2024 | 17/02/2025 | Passenger train derailment |
| Derailment of a passenger train at Roudham Heath | 06/02/2024 | 03/02/2025 | Passenger train derailment |
| Fatal accident at Stratford London Underground station | 26/12/2023 | 16/01/2025 | Train movement event involving passengers / pedestrians |