Laboratory confirmed cases of pertussis in England: annual report for 2021
Updated 6 July 2022
Applies to England

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/pertussis-laboratory-confirmed-cases-reported-in-england-2021/laboratory-confirmed-cases-of-pertussis-in-england-annual-report-for-2021
In England, there were 49 new laboratory confirmed cases of pertussis (culture, PCR, serology or oral fluid) reported to the UK Health Security Agency (UKHSA) pertussis enhanced surveillance programme in 2021. The 49 confirmed cases in England in 2021 were 95% lower than the 994 reported in 2020 (figure 1). The total number of samples submitted to UKHSA for testing were nearly 3-fold higher in 2021 (19,254) compared to 2020 (6,841) with a positivity rate of 0.3% (62/19,176) and 16% (1,059/6,825) in 2020.
Figure 1. Total number of laboratory confirmed pertussis cases per quarter in England, 2011 to 2021

The coronavirus (COVID-19) pandemic and the implementation of social distancing measures and lockdown across the UK from 23 March 2020 had a significant impact on the spread and detection of other infections including pertussis. From July 2021, COVID-19 containment measures were withdrawn in England. Vaccination against pertussis and other infectious diseases continues to be important as increasing levels of these diseases are expected following the easing of control measures; higher levels of activity are already being seen in some cases, such as measles and chickenpox.
Pertussis is a cyclical disease, with increases occurring every 3 to 4 years, with pertussis activity usually peaking each year in quarter 3 (July to September). In 2021, the highest proportion of cases was observed in the fourth quarter (October to December), when 20 cases (41%) were reported followed by 11 cases (22%) between January and March. Nine cases were reported in both April to June and in July to September (table 1). In 2020 the majority of cases (81%; 806 of 994 cases) were reported between January and March, before the first lockdown, and the number of reported cases decreased each subsequent quarter with the lowest reported between October and December 2020 (20 cases).
The national incidence for all age groups, based on laboratory confirmed cases of pertussis in England and 2020 population estimates (1) was 0.1 per 100,000 in 2021 compared to 1.8 per 100,000 in 2020 and 6.5 per 100,000 in 2019; it reached 17.5 per 100,000 in 2012 (epidemic peak year). Prior to the major peak in 2012, incidence ranged between 0.4 per 100,000 and 2.0 per 100,000 (figure 2).
Laboratory confirmed pertussis cases in infants aged under 1 year, were 96% lower in 2021 (2 cases), than in 2020 (50 cases). This compares with 508 confirmed cases reported in 2012.
There has been a decline in pertussis incidence in infants under 3 months of age since the introduction of the maternal vaccination programme, from 234 per 100,000 in 2012 to 93 per 100,000 in 2016, 20 per 100,000 in 2020 and 0.7 per 100,000 in 2021 (figure 2). The number of confirmed cases in infants under 3 months in 2021 was 97% lower (1 case) than in 2020 when 30 cases were reported. The number of confirmed cases in infants under 3 months and overall for infants under 1 year of age in 2021 were the lowest reported since the introduction of enhanced surveillance in 1994. Incidence in infants under 3 months of age in 2021 equalled the incidence in infants aged between 3 to 5 months for the first time since the introduction of enhanced surveillance. Cases in infants aged 3 to 5 months has also remained low since the 2012 epidemic peak, when there were 74 cases (43 per 100,000) – there was 1 case (0.7 per 100,000) in this age group in 2021 compared to 15 (10 per 100,000) in 2020.
In the 2016 cyclical peak, confirmed cases aged between 6 and 11 months were higher (34 cases, 10 per 100,000) than in any year since the introduction of enhanced surveillance. In 2019, incidence in this age group was 7 per 100,000 (21 cases) – in 2020 it was 2 per 100,000 (5 cases). There were no reported cases in infants aged between 6 and 11 months in 2021. These low numbers are consistent with protection from primary vaccination offered at 2, 3 and 4 months of age in conjunction with measures introduced to control the SARS-CoV-2 pandemic.
In all children aged 1 year and older, numbers of confirmed cases were markedly lower in 2021 than in 2020 – 94% lower in those aged 1 to 4 years, 96% lower in 5 to 9 year olds and 98% lower in 10 to 14 year olds. Ascertainment in those aged 5 to less than 17 years has improved with availability of oral fluid testing since 2013. From 1 May 2018, the availability of oral fluid testing was extended to all children aged from 2 up to and including 16 year olds, which may underpin earlier increases observed in the 1 to 4 year age group. In 2021 oral fluid alone accounted for half (4 of 8) of cases in children aged between 1 and 14 years.
Most (80%; 39 of 49 cases) (table 2) laboratory confirmed cases in England in 2021 occurred in individuals aged 15 years and older – total numbers in this age group in 2021 were 94% lower than in 2020 (693 cases).
Deaths
In England, 14 deaths were reported in infants with confirmed pertussis in the 2012 epidemic peak year. Following the introduction of pertussis vaccination in pregnancy there have been 20 further deaths in babies with confirmed pertussis. There were no reported deaths in infants with confirmed pertussis in 2021. The last pertussis-related death of an infant was reported in the second quarter (April to June) of 2019.
All the deaths in 2012, and those that have occurred following the introduction of the maternal programme, were too young to be fully protected by infant vaccination. Only 2 of the infants born after the introduction of the maternal programme had a mother who had been vaccinated during pregnancy. In both cases, the vaccination was too close to delivery to confer optimal passive protection in the infant.
Childhood vaccination uptake
The national vaccination schedule recommends pertussis vaccination at 8, 12 and 16 weeks of age and a pre-school booster at 3 years and 4 months.
The latest vaccine coverage estimates for 2021, evaluated between October to December for DTaP/IPV/Hib/HepB immunisation across England, was 92.0% for 3 doses at 12 months of age and 84.2% for the booster dose by 5 years of age (2). Coverage estimates at 12 months of age were slightly higher than the coverage estimates for October to December 2020 when the proportion of children vaccinated at 12 months was 91.5% and coverage estimates for the booster dose were lower than the 85.4% reported (3).
The introduction of social distancing in response to the COVID-19 pandemic from late March 2020, when some of this cohort would have been scheduled for vaccination, may have contributed to the modest decrease seen in the booster dose coverage.
Maternal vaccination programme
The maternal pertussis immunisation programme (4) introduced in response to the 2012 outbreak (5), became permanent from June 2019 (6) based on evidence of disease impact, high effectiveness and safety (7-10). The recommended gestational age for vaccination is between 20 and 32 weeks, ideally after the 20-week scan, but the vaccine can be given as early as 16 weeks (6) for pragmatic reasons to ensure vaccination.
The most recent UKHSA figures report that the proportion of mothers due to give birth in 2021 who had been immunised with a pertussis containing vaccine in pregnancy in England ranged from a monthly average of 63.1% (May) to 67.8% (January) compared to 2020 where monthly averages ranged from 66.4% (August) to 72.5% (January) (11). The impact of the pandemic on healthcare services has possibly resulted in vaccine coverage being lower than any May to December coverage estimates since April 2016. This could be due in part to a potential increase in the delivery of the vaccines through maternity units, during the pandemic, which may not have been captured completely in the survey and therefore resulted in an under-estimation of coverage.
The annual vaccine coverage for maternal pertussis vaccine in the financial year 2020 to 2021 was 67.8%, which was 2.7 percentage points lower compared to 2019 to 2020 financial year (12).
Surveillance data in young infants following the introduction of the pertussis immunisation in pregnancy programme demonstrated that a low incidence had been maintained in this age group, with expected seasonal increases. COVID-19 control measures appear to have had an additional impact on these observed effects. With the withdrawal of COVID-19 containment measures and increased social mixing it is expected that the number of cases will increase and therefore it is even more important that women are offered pertussis vaccination in pregnancy (ideally between 20 and 32), to optimise protection for their babies from birth, and for infants to complete the vaccination schedule on time.
Supplementary data tables from 1994 to 2021 are available.
Figure 2. Incidence of laboratory confirmed pertussis cases by age group in England: 1998 to 2021
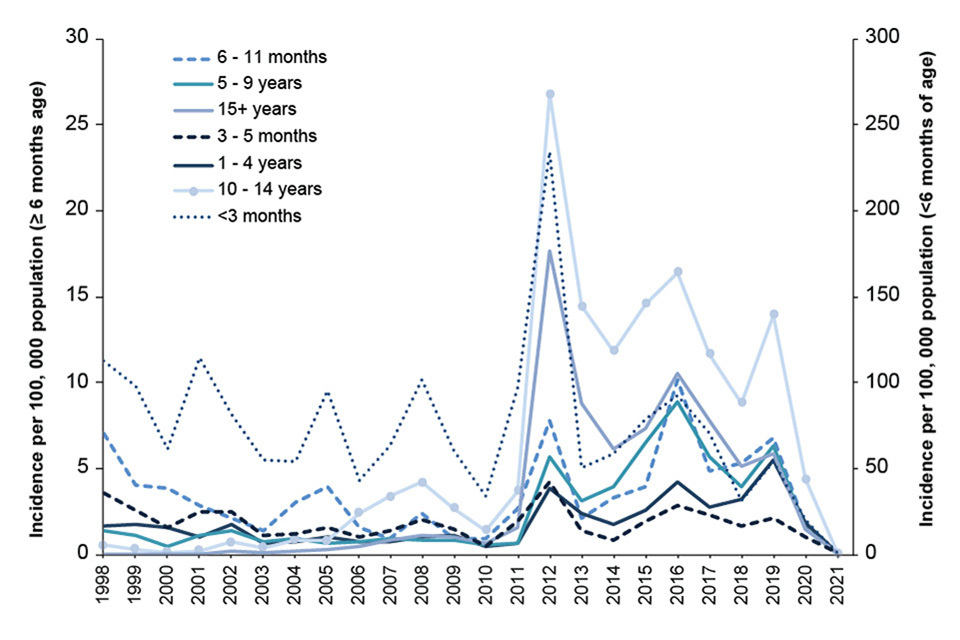
Table 1. Laboratory confirmed cases of pertussis by quarter and test method* in England: 2021
| Age group | Culture | PCR | Serology | Oral fluid only | Total |
|---|---|---|---|---|---|
| January - March | 0 | 1 | 10 | 0 | 11 |
| April - June | 0 | 2 | 7 | 0 | 9 |
| July - September | 0 | 0 | 8 | 1 | 9 |
| October - December | 0 | 2 | 15 | 3 | 20 |
| Total | 0 | 0 | 40 | 4 | 49 |
*Culture-confirmed cases may additionally have tested positive by any other method; PCR-confirmed cases may have additionally tested positive by serology or OF; and serology-confirmed cases may also have been confirmed by OF. Cases are only represented once in the table. Submission of all presumptive B. pertussis isolates is encouraged for confirmation of identity and to allow further characterisation for epidemiological purposes.
Table 2. Age distribution of laboratory confirmed cases of pertussis by test method* in England: 2021
| Age group | Culture | PCR | Serology | Oral fluid only | Total |
|---|---|---|---|---|---|
| Less than 3 months | 0 | 1 | 0 | 0 | 1 |
| 3 to 5 months | 0 | 1 | 0 | 0 | 1 |
| 6 to 11 months | 0 | 0 | 0 | 0 | 0 |
| 1 to 4 years | 0 | 1 | 2 | 0 | 3 |
| 5 to 9 years | 0 | 0 | 0 | 2 | 2 |
| 10 to 14 years | 0 | 0 | 1 | 2 | 3 |
| 15 years and over | 0 | 2 | 37 | 0 | 39 |
| Total | 0 | 5 | 40 | 4 | 49 |
*Culture-confirmed cases may additionally have tested positive by any other method; PCR-confirmed cases may have additionally tested positive by serology or OF; and serology-confirmed cases may also have been confirmed by OF. Cases are only represented once in the table. Submission of all presumptive B. pertussis isolates is encouraged for confirmation of identity and to allow further characterisation for epidemiological purposes.
References
1. Office for National Statistics, 2020 population estimates
2. Quarterly vaccination coverage statistics for children aged up to 5 years in the UK (COVER programme): October to December 2021. Health Protection Report volume 16 number 4, 29 March 2022
3. Quarterly vaccination coverage statistics for children aged up to 5 years in the UK (COVER programme): October to December 2020. Health Protection Report volume 15 number 7, 30 March 2021
4. Confirmed pertussis in England and Wales continues to increase (2012). Health Protection Report volume 6 number 15
5. Department of Health (2012) Pregnant women to be offered whooping cough vaccine (website news story, 28 September)
6. Joint Committee on Vaccination and Immunisation (2014). Minute of the meeting on 4 June 2014
7. Amirthalingam G and others (2014). Effectiveness of maternal pertussis vaccination in England: an observational study. The Lancet
8. Dabrera G, and others (2014). A case-control study to estimate the effectiveness of maternal pertussis vaccination in protecting newborn infants in England and Wales, 2012 to 2013. Clinical Infectious Diseases
9. Donegan K, and others (2016). Safety of pertussis vaccination in pregnant women in UK: observational study. British Medical Journal
10. Amirthalingam G and others (2016) ‘Sustained effectiveness of the maternal pertussis immunization program in England 3 years following introduction’, Clinical Infectious Diseases
11. Pertussis vaccination programme for pregnant women update: vaccine coverage in England, October to December 2021. Health Protection Report volume 16 number 4, 22 March 2022
12. Pertussis vaccination programme for pregnant women update: vaccine coverage in England, January to March 2021 and 2020 to 2021 annual coverage. Health Protection Report volume 15 number 9