Incentivising SME uptake of health and wellbeing support schemes
Published 15 March 2023

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/incentivising-sme-uptake-of-health-and-wellbeing-support-schemes/incentivising-sme-uptake-of-health-and-wellbeing-support-schemes
DWP research report no. 1024
A report of research carried out by RAND Europe on behalf of the joint Work and Health Unit (Department for Work and Pensions and Department for Health and Social Care).
Crown copyright 2022.
You may re-use this information (not including logos) free of charge in any format or medium, under the terms of the Open Government Licence. To view this licence, visit http://www.nationalarchives.gov.uk/doc/open-government-licence/ or write to:
Information Policy Team
The National Archives
Kew
London TW9 4DU,
Email: psi@nationalarchives.gov.uk
This document/publication is also available on the Research at DWP page on the GOV.UK website
If you would like to know more about DWP research, email: socialresearch@dwp.gov.uk
First published March 2023.
ISBN 978-1-78659-506-5
Views expressed in this report are not necessarily those of the Department for Work and Pensions or any other government department.
Statement of Compliance
This research complies with the three pillars of the Code of Practice for Statistics: trustworthiness, quality and value.
The following explains how we have applied the pillars of the Code in a proportionate way.
Trustworthiness
This research was conducted, delivered and analysed by RAND Europe, a not-for-profit, nonpartisan policy research organisation with a long and proven commitment to high-quality research, underpinned by rigorous analysis.
RAND Europe worked closely with the joint Work and Health Unit (Department for Work and Pensions and Department for Health and Social Care) to understand the aims of the research, but led on the design, delivery and analysis of the research approach.
The work was undertaken in line with the Government Social Research code of practice, and the large scale survey of small and medium-sized enterprises (SMEs) was undertaken by Accent, a market research agency who sub-contracted to RAND Europe, and are members of the Market Research Society and work to their code of conduct
The authors of this report were all within the employment of RAND Europe at the time of their contributions to the research.
Quality
The mixed-methods approach to this research was carried out using well-established quantitative and qualitative research methods.
The research has been quality assured using RAND Europe’s internal quality checking processes, which have been shared with the Work and Health Unit. The report has been checked thoroughly by Work and Health Unit analysts to ensure it meets the highest standards of analysis and drafting.
Value
This research provides fresh insights into SMEs current activity, their desire to do more, and the current barriers to this. In addition, it provides a quantification of the relative influence that policy leavers could have on what employers say they would do. Findings from this report have informed the ongoing development of policy decisions relating to health and wellbeing support among SMEs.
Executive summary
This research aimed to provide new insight into how incentives might be used to encourage and support SME employers to invest in more health and wellbeing schemes for employees.
The report considers:
- What support are SMEs already providing in this space?
- What do SMEs say prevents them from doing more?
- What kind of interventions would SMEs like to invest in, should greater support to do so be available?
- What impact could a government intervention have in improving uptake?
The mixed-methods approach centred around a discrete choice experiment (DCE) undertaken within a survey of 500 SMEs (with at least 10 employees) in Great Britain. This was supplemented with a series of 30 qualitative interviews to provide more detailed insight into some of the issues identified through the survey.
The research finds that 70% of SMEs surveyed reported they currently provide at least one type of proactive health promotion scheme for all employees, but smaller SMEs generally provide lower levels of support. Provision is often employee led and comes about as a result of requests from staff.
SMEs have an appetite to do more but lack of resources – both money and/or time – are the top barriers to implementation, along with a lack of knowledge about what support to invest in. Support to address issues surrounding musculoskeletal conditions, common mental health problems and the way work is organised or managed were the top three areas in which employers wanted to do more.
The discrete choice experiment, supported by qualitative evidence, suggests that both financial support and the provision of advice and support have a role to play in improving SME uptake of health and wellbeing schemes. With regards to financial support, a greater impact could be achieved by funding a larger group of SMEs at 50% reimbursement than half as many SMEs at 100%.
Navigating the market for these services can be challenging for SMEs and many stated they would not know what health and wellbeing programmes to invest in even if there was financial support. Access to supplementary advice, in the form of a needs assessment and signposting to appropriate health and wellbeing schemes, was observed to have a significant impact on stated uptake in the experiment. Such assistance could help SMEs to deliver on their often-stated desire to help improve the health and wellbeing of their staff.
The risk of “deadweight loss” from SMEs using any financial support to simply subsidise actions that they are currently taking appears low. Both the survey and interviews identified that employers had a desire to do more and intended to use any funding provided to either extend their current provision or move into new areas.
The report concludes with some suggestions for further research to better inform future policy design.
Acknowledgements
The authors at RAND Europe would like to thank the team at the Work and Health Unit (Lisa Schulze, Michael Oldridge, Paige Portal and Karen Taylor) for their guidance and support throughout this project.
Thanks are also due to colleagues at Accent who helped with survey recruitment and fieldwork. We would also like to acknowledge the important contributions of Rob Prideaux who helped lead aspects of the study whilst on secondment to RAND Europe, and Dr Chris van Stolk and Bhanu Patruni who acted as quality assurance reviewers throughout the study.
Last, but by no means least, the authors would also like thank all the employers who took part in the research.
The Authors
This report was authored by researchers at RAND Europe:
- Peter Burge (Operations Director)
- Hui Lu (Senior Analyst)
- Pamina Smith (Analyst)
- Nadja Koch (Research Assistant)
Glossary and abbreviations
| Term | Definition |
|---|---|
| Deadweight loss | A measure of lost economic efficiency when the socially optimal quantity of a good or a service is not produced. In the case of this study this would include the use of public funding to pay for activities that are already being paid for in other ways |
| Discrete Choice Experiment (DCE) | A quantitative research method for valuing different factors that influence the choices that individuals or organisations may make. DCEs enable choice alternatives to be broken down into a range of component parts, which are taken into account through the inclusion of a range of different attributes |
| Employee Assistance Programme (EAP) | Helpline and/or other services offered to all employees to provide confidential expert advice when needed; may cover wider health and wider wellbeing issues, such as financial |
| Incentivised action plan | A health and wellbeing financial incentive scheme entailing an action plan aimed at improving the health and wellbeing of employees. An incentive would be paid to the participating company, based on the number of employees involved, in return for an ongoing time commitment from the company over a one-year period |
| Long-term health conditions and/or disabilities (LTCD) | A condition that cannot at present be cured but can be controlled by medication and therapies |
| Musculoskeletal conditions | Conditions that affect the joints, bones and muscles |
| Occupational Health (OH) | Advisory and support services which help to maintain and promote employee health and wellbeing. OH services support organisations to achieve these goals by providing direct support and advice to employees and managers, as well as support at the organisational level e.g. to improve work environments and cultures |
| Reimbursement rate | The proportion of costs of services that might be reimbursed to employers providing health and wellbeing interventions within the scope of a given scheme |
| Small and medium-sized enterprise (SME) | Employers with up to 249 employees. For the purpose of this study we excluded micro employers with less than 10 employees |
Summary
Background
The Health is Everyone’s Business consultation outlined the crucial role employers play in supporting the health of employees. Improved employee health and wellbeing can benefit employees, employers, and the wider economy by reducing ill-health related job loss, sickness absence, presenteeism, and improving productivity.
However, previous research shows that whilst most employers recognise their role, many face multiple barriers to investing in health and wellbeing support, such as lack of expertise, time constraints and cost. There is also wide variation in the support provided by employer size, with small and medium-sized employers significantly less likely to invest in formal health and wellbeing initiatives than large employers.[footnote 1]
The joint Work and Health Unit (Department for Work and Pensions and Department for Health and Social Care) commissioned RAND to research what incentives could be used to encourage and support small and medium-sized enterprise (SME) employers to invest in more health and wellbeing schemes for employees.
Methodology
The research included a quantitative telephone survey with 500 SME employers (with at least 10 employees) in Great Britain, 30 in-depth qualitative interviews, and a discrete choice modelling experiment embedded within the survey.
The survey and interviews explored the main health concerns of SME employers, their current provision of health and wellbeing support, and the barriers to providing it. The survey uses a sampling frame but is not weighted to be representative nationally.
The discrete choice experiment explored the potential uptake amongst SMEs of government-provided financial incentives and signposting advice for health and wellbeing schemes, including the importance of attributes relating to how that support is delivered. Each SME was given a range of hypothetical ‘choice scenarios’. Within each scenario, SMEs were asked to choose between three options; two involving participation in a new health and wellbeing scheme and one ‘continue as now’ option. The health and wellbeing schemes offered were varied in carefully controlled ways by five groups of attributes:
| Attribute | Levels |
|---|---|
| Types of health and wellbeing services in scope for purchase | - Proactive health-promotion schemes open to all employees, i.e. schemes to encourage healthy eating, or stress management - Schemes targeted for employees with health conditions, i.e. occupational health assessments - Both in scope |
| Needs assessment and advice on interventions | - No support available – baseline - Online resources available - Personal advisor available |
| Financial support (% of cost is reimbursed) | - No financial support – baseline - 25% of cost is reimbursed - 50% of cost is reimbursed - 75% of cost is reimbursed - 100% of cost is reimbursed |
| When support payment is made | - All paid at the end – baseline - 30% paid up front and 70% paid at the end |
| Administrative requirements | - Only proof of purchase required – baseline - Proof of purchase plus funding request submitted beforehand - Proof of purchase plus requirement to provide data on impacts of scheme - Proof of purchase plus both |
An example of a choice scenario put forward to respondents is below:
Responses were used to model the relative contribution of each attribute level to the likelihood that SMEs would choose a scheme. These were used to illustrate potential SME uptake for schemes with different configurations of attributes. However, it is advised that specific uptake estimates should be interpreted with extreme caution for the following reasons:
- They assume 100% of SME employers are aware of any scheme. In reality, raising awareness of such provision amongst SMEs can be challenging.
- Hypothetical scenarios can only include a limited amount of detail and so may exclude details that in reality might affect the employer’s decision. For instance, two potentially important details not included in these scenarios include:
- Gross costs of health and wellbeing schemes – in reality, cost is likely to influence employer decisions, and it may also influence the relative importance of other factors, such as financial reimbursement rate.
- Time required to fulfil administrative requirements – whilst the DCE explored the impact of different forms of administrative requirement, it did not specifically test the sensitivity of uptake to different time commitments.
- Responses may be subject to social desirability bias, meaning respondents may choose the more socially acceptable answer (i.e. they would provide support) even if it’s not the choice they would make in reality.
- The sample of respondents excluded micro employers (with fewer than 10 employees), who may be less likely to uptake formal health and wellbeing support.
This research was carried out in 2018, prior to the COVID-19 pandemic.
Survey and qualitative interview findings
Key health concerns for employers
When asked about the most important health and wellbeing concerns affecting their organisation, over 80% of respondents reported each of musculoskeletal conditions or mental health problems. This supports previous research which found these to be the two most common health concerns of employers.[footnote 2] They are also the two single most common reasons for sickness absence in the UK after minor illnesses.[footnote 3]
The qualitative research highlighted that concerns about musculoskeletal conditions clustered into two different groups: those that were concerned about low levels of activity at desk-based work along with repetitive movements, and those that were concerned about heavy lifting and physical strain.
Concerns regarding mental health could also be clustered into two groups: those that were aware of the stresses and strains of the workplace, and those that recognised that their staff could have complications outside of work that could also impact on their working life.
Current provision of health and wellbeing support
Employers were asked about two categories of health and wellbeing scheme:
- proactive health promotion for all employees in the workplace, for example schemes to encourage healthy eating, physical activity, or stress management
- support targeted for employees with health conditions, beyond legal obligations, for example Occupational Health assessments, or access to psychological therapy
70% of SMEs reported they currently provide at least one type of proactive health promotion scheme for all employees. This varied significantly by employer size, with only 58% of employers with 10-19 employees providing at least one type of proactive support, compared to 82% of employers with 50-249 employees. The most common types provided were mental health support or training (39%) and help with managing stress (39%).
Similarly, when asked about provision targeted for employees with health conditions, medium employers reported much higher levels of current provision. However, this is to be expected since smaller employers are less likely to have employees with health conditions. For example, previous research found that the most common reason small employers do not provide Occupational Health services for their employees was a lack of employee need.[footnote 4]
Therefore, to explore willingness to provide support, employers were asked both whether they currently provide support specifically for employees with health conditions, and whether they would provide it if an employee need arose. Taking into account this stated willingness to provide support should it be required, the difference by employer size reduces significantly, but a difference does remain.
Qualitative interviews highlighted that smaller employers did appear to have a strong interest in the health and wellbeing of their staff, but they tended to have more of a ‘family’ culture than larger employers and therefore tended to use more informal approaches to handling health problems in the workplace.
Barriers to investing in health and wellbeing
The most common reported barriers to providing health and wellbeing support were lack of expertise to know what support to invest in (49% of respondents), lack of time or resources to implement policies (49%), and lack of capital (52%). This supports previous research which found that lack of time and capital are the main barriers for SMEs in supporting employees to return to work after a spell of sickness absence.[footnote 5]
A theme highlighted in the interviews was that knowing what to invest in is complicated and navigating the market can be difficult and requires a time investment. Some SMEs explained that whilst cost was a key barrier to SMEs, many would not know what health and wellbeing programmes to invest in even if there was financial support.
Discrete Choice Experiment findings
Importance of type of health and wellbeing scheme on SME uptake of support
SMEs were equally as likely to choose a preventative health and wellbeing scheme as they were to choose a scheme targeted for employees with health conditions, but they were more likely to choose a scheme including both types of support than just one.
SMEs with experience of employees with long-term health conditions or disabilities were more likely to choose either type of scheme than SMEs without that experience but they were particularly more likely to choose preventative schemes.
Importance of financial incentives on SME uptake of support, including payment timing
The experiment found that as the rate of financial reimbursement increases, the likelihood of choosing an option increases. However, there are diminishing marginal returns as reimbursement rates increase.
Taking the example of an option that covered both categories of health and wellbeing schemes, where 30% of any financial reimbursement is paid up front and 70% is paid at the end, which includes an online needs assessment and signposting to appropriate schemes, and for which there are no administrative requirements for participating, the experiment estimated that 53% of SMEs who know of the scheme would participate even if there was no reimbursement. If the government offered a 25% financial reimbursement, uptake would increase by 13 percentage-points to 66%, but for each additional 25% reimbursement, the amount by which take up would increase gets smaller. Increasing the subsidy to 50%, then to 75%, then to 100%, would increase uptake by a further 11 percentage-points (to 77%), 5 percentage-points (to 82%), and then 4 percentage-points (to 86%), respectively.
In practice, this means that for a given pool of funding, greater impact could be achieved by funding a larger group of SMEs at 50% reimbursement than half as many SMEs at 100% reimbursement.
To test whether capital, or more specifically cash-flow constraints, were the barrier for SMEs, the experiment varied the timing of the reimbursement payment between having a payment made on delivery, or having 30% paid up front and the remaining 70% on delivery. This had no statistically significant impact on uptake. This finding was generally supported through qualitative interviews, though some SMEs reported that a quick reimbursement following delivery was important.
It is worth noting, however, that information which was not provided in the hypothetical scenarios, such as gross scheme cost to providers, could change the relative importance of the financial reimbursement rate or timing of payment in reality.
This is particularly important given a common theme in the qualitative interviews was that many SMEs appeared to have limited understanding of the costs of health and wellbeing schemes, and many had not seriously considered how much they might be willing to spend. This means that many SMEs made decisions in the experiment without a clear and consistent understanding of the costs to the business.
Importance of supplementary advice and guidance on SME uptake of support
The choice experiment tested whether supplementary advice and guidance would increase uptake of the support package. This was described as an upfront needs assessment to help SMEs better understand staff health needs or on how to source or implement best-practice schemes to address those needs. The experiment varied whether this advice was delivered through access to online resources or access to a personal advisor.
The provision of supplementary advice had a statistically significant positive impact on uptake of the support package. However, on average there was no statistically significant difference between whether this support was delivered online or by a personal advisor. Model forecasts show that by taking the same option as expressed in the previous section but holding the rate of financial reimbursement fixed at 50%, the availability of online resources or a personal adviser would increase SME uptake by 7 to 8 percentage-points compared to if no advice was available.
The qualitative interviews showed a mix of preferences, with some employers strongly preferring online advice and others preferring a personal adviser.
Importance of administrative requirements on SME uptake of support
Including additional administrative requirements for employers to participate in a scheme had no statistically significant impact on the likelihood of employers choosing that scheme. However, in the qualitative interviews, many SMEs emphasised that any administrative requirements needed to be proportionate to the funding and support being provided. This indicates that whilst the experiment did not detect an impact, excessive and disproportionate administrative requirements could still have an impact on uptake.
Conclusions
Findings from the survey and qualitative interviews were consistent with other research. Medium-sized employers are more likely than small employers to invest in formal health and wellbeing initiatives for their employees. For support specifically to manage existing health conditions in the workplace, this difference by employer size reduces significantly when taking into account whether SMEs would be willing to provide the support should an employee need arise, yet a difference does remain. The most common barriers to SMEs providing health and wellbeing support were lack of expertise to identify initiatives, lack of time to implement, and lack of capital to invest in them.
The experiment, supported by qualitative evidence, suggests that the following could be effective at improving SME uptake of health and wellbeing schemes:
- Financial support. However, a greater impact could be achieved by funding a larger group of SMEs at 50% reimbursement than half as many SMEs at 100%.
- Supplementary advice, in the form of a needs assessment and signposting to appropriate health and wellbeing schemes.
1. Introduction
1.1. Policy background
Improved employee health and wellbeing is in everyone’s interests. It can benefit employees, employers, and the wider economy by reducing ill-health related job loss, sickness absence, presenteeism, and improving productivity. In 2017, ‘Improving Lives: The Future of Work, Health, and Disability’[footnote 6] set out an ambitious agenda to transform employment outcomes among people with long-term health conditions or disabilities. The 2019 ‘Health is Everyone’s Business’ consultation[footnote 7] built on this with proposals to minimise the risk of ill-health related job loss, outlining the crucial role employers play in supporting the health of employees.
Existing evidence points towards best practice employer-led interventions that can prevent ill-health, maintain wellbeing, and support the recruitment, retention and reintegration of disabled people or people with health conditions. There is a growing market for workplace health and wellbeing initiatives, from Occupational Health (OH) services, Employee Assistance Programmes (EAPs), access to psychological or physiological therapy, through to workplace cycling schemes and suppliers providing of health and wellbeing training. Workplace health and wellbeing initiatives have the potential to improve both business and health outcomes[footnote 8], hence can contribute to overall public health, productivity and work retention.
However, there is limited empirical evidence on what would encourage employers to implement these interventions or invest in health and wellbeing programmes. The current system to support people with health problems and the responsibilities of different actors (e.g. sick pay) creates a unique system of incentives and disincentives for them to act. Developing the evidence-base on levers that could encourage employer action, particularly for small and medium-sized enterprises (SMEs), is critical in developing policy that will deliver on the overall agenda.
1.2. Wider context
Evidence suggests employers generally recognise their role in supporting employee health and wellbeing, but investment in health and wellbeing is often not considered a priority.[footnote 9] There is also wide variation in the support provided by employer size, with small and medium-sized employers less likely than large employers to state they proactively seek to address these areas and are less likely to provide health and wellbeing services like OH and EAPs[footnote 10]. Many report facing multiple barriers, such as lack of expertise, time constraints and cost[footnote 11]. In addition, they may not consider the positive externalities of improved health and wellbeing support on employees, their businesses, and the wider economy when choosing whether or not to invest in it.
The provision of financial incentives to employers or improved advice about what to invest in have been suggested as possible solutions to improve provision of support for employees. However, internationally, very few studies have looked specifically at the impact of offering financial support for employers to invest in employee health and wellbeing.[footnote 12] Moreover, whilst economic theory suggests that financial incentives or improved advice about what works could help increase health and wellbeing provision, there is still large uncertainty around the optimal level and structure of such policies to encourage action.
1.3. Research aims
This research contributes to the overall understanding of employer decision-making in the work and health space, with a focus on workplace and employer-led prevention of ill-health and health-related job loss, and how and what policy levers should be utilised for encouraging action.
In particular, this research aims to answer the following research questions:
- What support are SMEs already providing in this space?
- What do SMEs say prevents them from doing more?
- What kind of interventions would SMEs like to invest in, should greater support to do so be available?
- What impact could financial reimbursement or signposting advice have on uptake of health and wellbeing schemes, and what is the optimal structure of this intervention?
1.4. Method
The mixed-method approach developed for this research centred around a discrete choice experiment (DCE) undertaken within a survey of SMEs. This was supplemented with a series of qualitative interviews to provide more detailed insight into some of the issues identified through the survey. For more detail on the research design mentioned below, please refer to the appendix. This research was carried out in 2018, prior to the COVID-19 pandemic.
1.4.1. Use of a discrete choice experiment
Fundamentally the core policy questions regarding the possible structure of a policy intervention relate to how SMEs would make choices if faced with different options, and how these choices would vary depending on the alternatives available. Discrete choice experiments provide a research approach that is well suited to such situations. They provide an approach to unpick how different factors influence the choices made by decision-makers. Respondents in a survey are asked to consider a range of different hypothetical choice situations, which differ in carefully controlled ways. The experimental design behind these scenarios means that it is possible to understand the influence of different factors on the choices that they state they would make.
This approach to understanding, and quantifying, how different factors can influence decisions is strongly grounded in economic theory. Prof Daniel McFadden was awarded the Nobel Prize for Economics in 2000 for his work in developing the theoretical basis that underpins the modelling of discrete choice data.
In the context of this study, a choice experiment was developed to give insight into the decision making of SMEs, and how uptake of health and wellbeing schemes might be improved through a government support package including financial reimbursement and/or signposting advice for the SME, with careful consideration of how different configurations of this scheme are designed and the support that might be provided to SMEs to help them access these. The experiment specifically tested how different levels of support might affect uptake of the whole package of government support for SMEs to purchase health and wellbeing schemes. However, it is assumed that anything which increases SME uptake of the government support package would increase SME uptake of the health and wellbeing scheme in scope for that package.
By observing the choices made between different SME support packages, including the option not to take up any support package, the research could measure the strength of preference and trade-offs of SMEs towards different characteristics that can influence their decision to take up the support, including but not exclusive to the level of the financial incentive.
This approach provides an indirect way to establish the importance of different factors and is less prone to bias and gaming by respondents than asking directly about what is important. It provides a mechanism under which it is not possible to say that everything is important and forces respondents to consider the sorts of trade-offs that they have to make in real life. It therefore provides a better measure of how much weight is placed upon different factors when choosing between alternatives.
This choice experiment was embedded in a wider telephone survey which allowed us to ask additional questions to ascertain both current levels of provision and the extent of aspirations to do more, alongside questions to assist in profiling the nature of the SME responding so that differences between sub groups could be explored.
1.4.2. Development of survey and discrete choice experiment
The design of the survey was informed by some initial qualitative interviews with SMEs to understand how they conceptually understood the issues of interest and to explore the language used by SMEs when discussing these. A workshop was also held with key stakeholders to identify the policy dimensions to explore within the choice experiments and how to translate these to attributes and their associated levels. The draft survey and choice experiment was then iterated within the wider project team before being formally piloted with a group of 45 SMEs, and then refined.
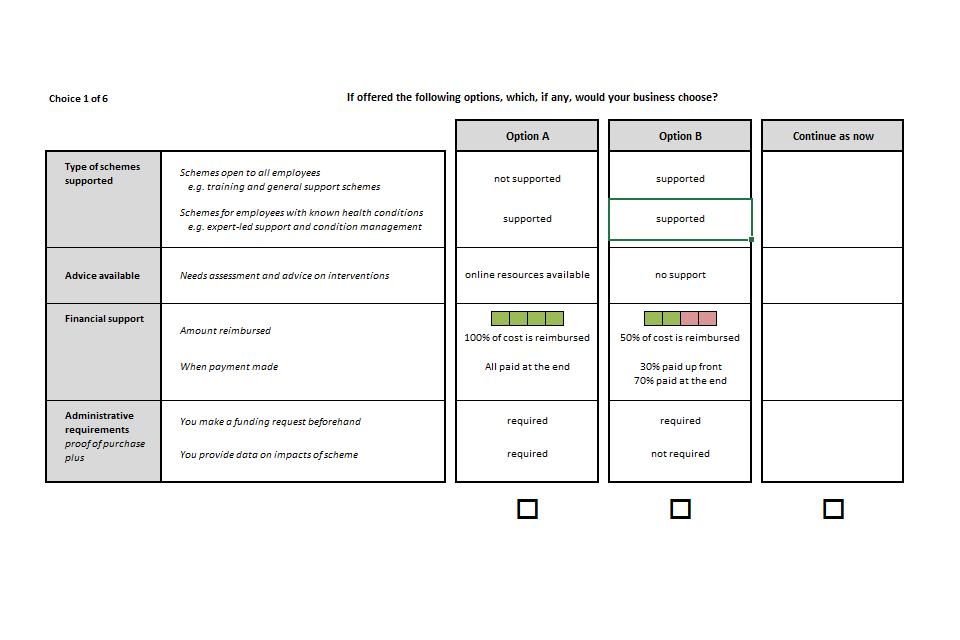
The final choice experiment asked SMEs to consider choices with three alternatives: they could choose one of two available support packages, or indicate that they would continue as they were. Each support package was described by four groups of attributes:
- the type of scheme supported,
- the advice available to SMEs
- the financial support offered, including payment terms
- and the administrative requirements if participating.
An example choice is shown in Figure 1.1.
Figure 1.1 Example of the choice scenario
The dimensions and different options for each attribute are described in Chapter 4, along with the findings from the experiment.
Each SME was asked to consider six different scenarios, with the levels presented on each attribute describing the offer being varied according to a statistical experimental design. In total 90 different sets of scenarios were considered across the sample, providing the data required to model the influence that each attribute has on the likelihood that a support package is chosen.
1.4.3. Telephone survey
The survey containing the DCE was rolled out to 500 SMEs across Great Britain, providing a rich dataset for the analysis of SMEs current practices and interest in engaging in future schemes to support employees.
The survey comprised 500 telephone interviews with SME employers in Great Britain (GB) with at least 10 employees. The sampling frame for the survey was sourced from DBS Data Solutions. A decision was taken to deliberately stratify the sample by SME size, as shown in Table 1.1, to obtain sufficient data from larger SMEs and support meaningful comparisons between groups. Survey fieldwork took place between November 2018 and January 2019. The descriptive statistics presented in this report relate to the survey sample and are unweighted. However, the forecasts from the model are weighted to provide insight into the potential uptake of support packages across the SME population.
Table 1.1 Distribution of SMEs (between 10-249 employees) by size
| SME Size | Survey sample | UK population (2018) |
|---|---|---|
| 10-19 employees | 36% | 55% |
| 20-49 employees | 37% | 29% |
| 50-99 employees | 15% | 10% |
| 100-199 employees | 10% | 5% |
| 200-249 employees | 2% | 1% |
Note: The survey sample was drawn from GB, but the BEIS Business Population Estimates are based on all UK
Further details regarding the design of the discrete choice experiment and data collection and the survey questionnaire are provided in the appendix.
1.4.4. In-depth interviews
To supplement the information collected through the online survey, a set of 30 follow-up telephone interviews with a subset of the SMEs that had participated in the survey were undertaken to gain richer insight into some of the issues emerging in the survey analysis.
Organisations were selected to provide coverage of SMEs that differed in size, differed in their experience of employing staff with long term health conditions or disabilities, and differed in their indicated interest in engaging with new initiatives to support the health and wellbeing of their staff. Responses provided in the main survey were used to identify potential participants on these criteria. The sampling frame for these interviews is shown in Table 1.2. The criteria for whether the respondent had previously stated that they would be likely to opt into an incentivised action plan provided insights from those with differing interest in engaging with an intervention. Whether the SME employed disabled staff was emerging as a distinguishing factor in the analysis of the value that SMEs placed on some dimensions of the interventions on offer so there was interest in further exploring the factors behind this.
Table 1.2 Sampling frame for qualitative interviews
| SME Size (number of employees) | Stated likelihood to opt for incentivised action plan | Employ staff with disabilities or long term conditions | Sample requirements | Interviews completed |
|---|---|---|---|---|
| 10-19 | Likely | Yes | minimum 7 respondents | 4 |
| 10-19 | Likely | No | minimum 7 respondents | 5 |
| 10-19 | Unlikely or don’t know | Yes | minimum 7 respondents | 3 |
| 10-19 | Unlikely or don’t know | No | minimum 7 respondents | 4 |
| 20-249 | Likely | Yes | minimum 7 respondents | 6 |
| 20-249 | Likely | No | minimum 7 respondents | 1 |
| 20-249 | Unlikely or don’t know | Yes | minimum 7 respondents | 3 |
| 20-249 | Unlikely or don’t know | No | minimum 7 respondents | 4 |
The purpose of these interviews was to help provide a better understanding of SMEs’ underlying rationales when choosing between support packages and survey responses, as well as to explore research questions not suitable to be covered within a survey. The timing of the interviews post-survey allowed emerging findings to be further explored.
The full protocol used for these follow-up interviews is included in the appendix.
Information on the sector within which the business operates was also collected when undertaking these interviews. This is provided alongside company size to provide some context to the quotes that are used to illustrate the attitudes and behaviours identified.
2. What SMEs currently provide
This chapter includes findings from the quantitative survey and qualitative interviews. It explores:
- what health and wellbeing services small and medium-sized enterprises (SMEs) already invest in, or are willing to invest in should they identify a need (section 2.1)
- barriers to providing health and wellbeing schemes (section 2.2)
2.1. Current provision of health and wellbeing support
The survey explored two broad categories of health and wellbeing schemes for employees:
- Interventions aimed at proactively promoting health and wellbeing for all employees, ranging from programmes to encourage individual behaviour change, (e.g. cycling schemes) to programmes reducing (the impact of) stressors in and outside the workplace (e.g. stress management schemes or Employee Assistance Programmes (EAPs)).
- Interventions specifically supporting employees with existing health conditions, ranging from independent expert advice on how to manage a condition in the workplace (e.g. Occupational Health services), to employer-funded therapeutic interventions (e.g. physiotherapy).
Within the survey, SMEs were asked about their current provision of schemes across both of these categories. For both, the interest was to identify what, if anything, they were providing above and beyond legal obligations like Health and Safety regulations or the provision of accommodations for disabled people under the Equalities Act (2010).
When discussing the support available to all staff, respondents were asked to report their current provision across eight possible sub-categories, with examples provided to help illustrate the types of support that might be considered within each category. The breakdown by category is shown in Table 2.1.
The survey found that the three most common programmes offered in the past 12 months were mental health support or training (39%), help with managing stress (39%), and employee assistance programmes (34%).
Whilst the data in Table 2.1 shows the provision of different forms of health and wellbeing scheme, it is also informative to look at how many of these different types of scheme are provided by any individual employer. The counts are therefore presented along with the cumulative totals that reveal the proportion of SMEs with different levels of provision.
Table 2.1 Health and wellbeing schemes currently provided to all employees
| Type of health and wellbeing scheme | Examples | Provided in the last 12 months |
|---|---|---|
| Mental health support or training | Mental health awareness training; training for line managers on how to recognise and address mental health issues; confidential helpline for employees with mental health concerns. | 39% |
| Help with managing stress | Workshops or training to raise awareness about work-related stress; briefings about stress at work; employee stress survey; staff training to prevent bullying or harassment; line manager training on dealing with stress. | 39% |
| Employee assistance programme | Helpline and/or other services offered to all employees to provide confidential expert advice when needed; may cover wider health and wider wellbeing issues, such as financial. | 34% |
| Schemes to encourage physical activity | Loans/discounts on bicycle purchases; free or subsidised gym membership; fitness classes at work; any measures to encourage running, cycling and walking. | 33% |
| Free or subsidised health services offered to all employees | Health screening, health checks, or free vaccination; health insurance | 32% |
| Other activities, such as campaigns to raise awareness about healthy lifestyles | General advice, bulletins or posters on how to live healthily; workshops or seminars on healthy lifestyles; training for line managers on improving employee health and wellbeing | 27% |
| Schemes to encourage healthy eating | Healthy food offered in the workplace /canteen; training or advice on how to eat well; weight loss advice or programmes. | 25% |
| Advice or support for employees to give up smoking | Promotional advice or material in the workplace; smoking cessation classes; help with accessing external smoking cessation programmes | 19% |
| Base | 500 |
Base: All respondents (unweighted)
Employers could select more than one response, therefore column percentages do not add to 100%.
As can be seen from Table 2.2, in total, 70% of SMEs surveyed provided at least one form of support to all staff, with 43% providing three or more forms of support. 30% do not provide anything.
Table 2.2 Number of different types of health and wellbeing scheme currently provided by SMEs to all employees
| Types of scheme provided | Count |
|---|---|
| 8 | 7% |
| 7 | 3% |
| 6 | 4% |
| 5 | 5% |
| 4 | 11% |
| 3 | 14% |
| 2 | 13% |
| 1 | 13% |
| None | 30% |
| Base | 500 |
Base: All respondents (unweighted)
| Types of scheme provided | Cumulative |
|---|---|
| 8 | 7% |
| 7 or more | 10% |
| 6 or more | 14% |
| 5 or more | 19% |
| 4 or more | 29% |
| 3 or more | 43% |
| 2 or more | 56% |
| 1 or more | 70% |
The survey also asked about provision of schemes specifically for people with existing conditions, either to help them get better or to manage their condition more effectively. Ill-health and the need to manage long-term health conditions in the workplace can be infrequent occurrences for small employers. Hence, the survey asked what employers were currently providing, and also what they would provide if faced with an employee need. This allowed us to identify the proportion of SMEs that were open to providing such schemes, and those that would not provide it should a need materialise. The descriptions of the different types of schemes that employers were asked to consider are shown in Table 2.3 along with summary data on the proportions of SMEs that would be willing to provide these to their staff.
For those that have experienced a need to which they have responded, the provision of independent expert advice such as occupational health is the most common response, stated by 36% of employers. Only 22% of employers stated that they would not provide this should the need arise. Employers stated that they were less likely to provide other forms of (potentially more costly) support should the need arise.
However, it is important to note that the data on “what employers would provide should the need arise” is self-reported, so it may be subject to social desirability bias. In addition, ‘employee need’ is subjective, and therefore could be impacted not only by incidence of the relevant health issues, but also by the employer’s awareness of employee health issues and the bar they set for employee need. Despite this, the high proportions indicating a willingness to do so suggests that any low provision of health-related support services for staff with health conditions could be at least partly due to lack of perceived need and not low willingness to pay.
Examining the responses across all categories of targeted scheme reveals that whilst 53% of the sample do not currently provide any of these types of scheme, only 17% say they would not provide any of these if the need arose.
Table 2.3 Targeted health and wellbeing programmes currently provided or would be provided by SMEs to employees
| Type of scheme | Examples | We currently provide this or have in the last 12 months | We would certainly provide this if the need arose | Would not provide this |
|---|---|---|---|---|
| Independent expert advice for employees and line managers on how to manage a condition in the workplace | Such as by occupational therapists or via an Occupational Health service | 36% | 42% | 22% |
| Free or subsidised access to psychological therapy | Cognitive behavioural therapy, counselling | 19% | 41% | 40% |
| Free or subsidised access to rehabilitative services for physical health conditions | Physiotherapy | 16% | 37% | 46% |
| Access to programs to address specific problems | Programmes or services to tackle: mental health issues; eating disorders, weight management; addiction issues | 14% | 46% | 40% |
| Other forms of non-medical advice | Mentoring programmes; independent expert advice on health and wellbeing issues | 18% | 41% | 41% |
Base: All respondents (unweighted), row total = all respondents (500)
2.1.1. Smaller SMEs are observed to provide fewer health and wellbeing schemes
The analysis examined whether there were significant differences in level of provision between different groupings of SMEs.
Larger SMEs (with 50 or more staff) showed a higher percentage of current provision than smaller SMEs. The differences are relatively consistent between types of support, and show a progression in provision from the smallest SMEs through to the mid and large SMEs.
With regards to proactive preventative support for all staff, Figure 2.1 shows a marked difference in the provision of mental health and wellbeing provision between different size SMEs – with approximately 30% of SMEs with 10-19 employees providing mental health support or training or help with managing stress, compared to over 50% for SMEs with more than 50 employees. There is also a large difference by employer size on services that require an ongoing financial commitment, such as subsidised health services and EAPs, although for EAPs this may in part be due to the wider insurance products targeted at the larger SME market that sometimes include EAP provision.
Figure 2.1 Proportion of SMEs currently providing general health and wellbeing programmes to all employees, by company size (multiple choice)
| Company size | 10-19 (179) | 20-49 (186) | 50+ (135) |
|---|---|---|---|
| Mental health support or training | 30% | 37% | 55% |
| Help with managing stress | 31% | 39% | 49% |
| Schemes to encourage physical activity | 27% | 33% | 40% |
| Schemes to encourage healthy eating | 21% | 22% | 35% |
| Advice or support for employees to give up smoking | 17% | 19% | 20% |
| Free or subsidised health services offered to all employees | 23% | 31% | 47% |
| Employee assistance programme | 22% | 34% | 49% |
| Other activities, such as campaigns to raise awareness about healthy lifestyles | 20% | 25% | 39% |
| None of these | 42% | 28% | 18% |
Base (unweighted): All respondents (500)
More than 40% of employers with less than 10 employees have not provided any of the listed forms of general health support to their staff in the past 12 months.
Differences can also be observed in the current provision of, and intent to provide, targeted health and wellbeing support for those that have known long term conditions.
Figure 2.2 Proportion of SMEs currently providing targeted health and wellbeing schemes, or would provide, to employees with health conditions, by employer size (multiple choice)
Independent expert advice for employees and line managers on how to manage a condition in the workplace:
| Employer size | Current/last 12 months | Would provide | Would not provide | Total |
|---|---|---|---|---|
| 10-19 (179) | 21.23% | 50.28% | 28.49% | 100% |
| 20-49 (186) | 27.96% | 48.39% | 23.66% | 100% |
| 50+ (135) | 65.19% | 22.96% | 11.85% | 100% |
Free or subsidised access to psychological therapy:
| Employer size | Current/last 12 months | Would provide | Would not provide | Total |
|---|---|---|---|---|
| 10-19 (179) | 8.38% | 46.93% | 44.69% | 100% |
| 20-49 (186) | 13.98% | 41.40% | 44.62% | 100% |
| 50+ (135) | 40.00% | 31.85% | 28.15% | 100% |
Free or subsidised access to rehabilitative services for physical health conditions:
| Employer size | Current/last 12 months | Would provide | Would not provide | Total |
|---|---|---|---|---|
| 10-19 (179) | 11.17% | 43.02% | 45.81% | 100% |
| 20-49 (186) | 11.83% | 34.95% | 53.23% | 100% |
| 50+ (135) | 29.63% | 33.33% | 37.04% | 100% |
Access to programs to address specific problems:
| Employer size | Current/last 12 months | Would provide | Would not provide | Total |
|---|---|---|---|---|
| 10-19 (179) | 9.50% | 51.96% | 38.55% | 100% |
| 20-49 (186) | 10.22% | 43.55% | 46.24% | 100% |
| 50+ (135) | 25.19% | 42.22% | 32.59% | 100% |
Other forms of non-medical advice:
| Employer size | Current/last 12 months | Would provide | Would not provide | Total |
|---|---|---|---|---|
| 10-19 (179) | 13.41% | 42.46% | 44.13% | 100% |
| 20-49 (186) | 15.05% | 37.63% | 47.31% | 100% |
| 50+ (135) | 28.15% | 42.22% | 29.63% | 100% |
Base (unweighted): All respondents (500)
Larger SMEs (with 50 or more staff) showed a much higher level of current provision, as would be expected given the higher likelihood of employing staff requiring support. Once the stated intent to provide support should it be required is taken into account, there is only a small gap in overall willingness to pay for support for employees with health conditions between larger and smaller SMEs.
2.1.2. Provision is often employee led, and comes about as a result of requests
The follow-up qualitative interviews were used to get more insight into how SMEs approach providing health and wellbeing schemes for their staff. SMEs were asked the types of scheme they provided and how they identified the need for this support. This revealed a tendency amongst SMEs to use informal approaches to identify where their staff may benefit from support, and typically in a reactive manner once they see indications that something may not be right. This can be characterised as “detect and talk”; they will see that something does not seem right and then try to ascertain what is wrong and how the business might help. In the words of one interviewee:
It is reliant upon people reporting it to us or other colleagues or managers reporting it to us, we don’t have a monitoring system.
(Arts, entertainment, and recreation, 20-49 employees)
Within smaller companies there is often an ethos of operating as an extension of the family:
Basically I look after long-standing employees, we’re a family business. I keep an eye on my staff. If I can see something is wrong, I’ll ask them and basically I will see if I can help.
(Information and communication, 10-19 employees)
It’s really a case of understanding the team itself. There’s only twelve of us, rather than having a formal situation whereby, you know, you fill in some tick boxes or meet on a Monday and, you know, discuss your issues, it’s very much a case of managing bottom up and top down so that if people have any issues it’s discussed and then brought to the attention of myself as MD as necessary. I think a lot of help and support comes out of the culture of the organisation as much as from pre-arranged schemes.
(Other service activities, 10-19 employees)
And those that do not currently provide a framework for support often feel that the size of their business does not justify it and they would deal with issues should they arise:
It’s not that we don’t see a need, it’s the extent to which we need to formalise stuff, in a much larger organisation, things need to be more formalised because there may be an absence of communication on a subject. We have management group meetings once a week and any issues of this would be discussed there and communicated to make sure line managers are aware of any concerns that we might have.
(Professional, scientific and technical activities, 50-99 employees)
We know our employees quite well, a lot of our employees are older people. They have been here for a long time. We like to think that we know something about them, we know them personally. We know their moods, we know when they’re down and we talk to them. If somebody has a specific need, we would absolutely find them some help if we could. So, we are not anti it, it’s just we haven’t had to do it.
(Manufacturing, 50-99 employees)
There are however some SMEs that do not see providing support to their staff in this area as necessary, or something that they could easily accommodate:
I don’t really have a need for it, because generally the staff are young and fit at the end of the day
(Accommodation and food service activities, 20-49 employees)
We don’t have that sort of budget to do a lot of in-worktime activities
(Human health and social work activities, 20-49 employees)
I think now we have fourteen members of staff. So it would be quite difficult to see us setting up a very elaborate sort of… although I guess there’s stuff that you could buy off the shelf. Another thing is that, because we’re small, because we work as well as we can in a consensual way, you hope that those sort of issues can in some sense, be dealt with internally.
(Information and communication, 10-19 employees)
Without exception, all of the SMEs interviewed spoke in a way that suggested that they took an interest in their staff and would support them in times of difficulty. What was clear, however, was that whilst some had taken steps to raise issues of mental health in the workplace or put in place schemes to help encourage physical activity, very few had thought in any structured way about how they might take this further. Most would wait until a member of staff brought forward an idea or issue before taking any additional steps.
This research therefore suggests that SMEs are often more reactive than proactive in their approach to health and wellbeing, and are frequently led by their staff and their emerging needs.
2.1.3. More SMEs provide preventative general support than targeted support for employees with existing conditions
Across the sample, 40% of SMEs employ staff with long-term health conditions and/or disabilities; ranging from 29% of SMEs with 10-19 employees to 51% of SMEs with more than 50 employees. The survey showed that these SMEs were more likely to have preventative support in place for all of their workers than those that do not employ such staff.
These SMEs also provided more health promotion schemes for all staff than schemes targeted for employees with health conditions. This might suggest that employers that experience health issues in the workplace (or are more open to employing such staff) are more likely to invest in health promotion schemes for the benefit of all staff. As such, there could be a level of latent willingness within the wider SME population to do more if they better understood the potential benefits.
Figure 2.3 Proportion of SMEs currently providing preventative health and wellbeing programmes to all employees, by whether staff have LTCD (multiple choice)
| Types of health and wellbeing programmes | Do not have staff with disabilities or long term conditions (301) | Have staff with disabilities or long term conditions (199) |
|---|---|---|
| Mental health support or training | 36% | 44% |
| Help with managing stress | 35% | 44% |
| Schemes to encourage physical activity | 28% | 40% |
| Schemes to encourage healthy eating | 22% | 29% |
| Advice or support for employees to give up smoking | 16% | 23% |
| Free or subsidised health services offered to all employees | 27% | 41% |
| Employee assistance programme | 28% | 43% |
| Other activities, such as campaigns to raise awareness about healthy lifestyles | 22% | 35% |
| None of these | 37% | 21% |
Base (unweighted): All respondents (500)
Nearly 30% of SME employers who reported they did not employ staff with long-term health conditions and/or disabilities have invested in advice on how to manage a condition in the workplace. These could have been provided to manage injuries, sicknesses, and conditions considered to be short-term, or to support staff that have since left the business.
Figure 2.4 Proportion of SMEs currently providing targeted health and wellbeing programmes, or would provide, to employees with LTCD, by whether staff have LTCD (multiple choice)
Independent expert advice for employees and line managers on how to manage a condition in the workplace:
| Employer size | Current/last 12 months | Would provide | Would not provide | Total |
|---|---|---|---|---|
| No (301) | 29.24% | 44.85% | 25.91% | 100% |
| Yes (199) | 45.23% | 38.19% | 16.58% | 100% |
Free or subsidised access to psychological therapy:
| Employer size | Current/last 12 months | Would provide | Would not provide | Total |
|---|---|---|---|---|
| No (301) | 16.61% | 38.87% | 44.52% | 100% |
| Yes (199) | 22.61% | 43.72% | 33.67% | 100% |
Free or subsidised access to rehabilitative services for physical health conditions:
| Employer size | Current/last 12 months | Would provide | Would not provide | Total |
|---|---|---|---|---|
| No (301) | 13.29% | 38.21% | 48.50% | 100% |
| Yes (199) | 21.11% | 36.18% | 42.71% | 100% |
Access to programs to address specific problems:
| Employer size | Current/last 12 months | Would provide | Would not provide | Total |
|---|---|---|---|---|
| No (301) | 10.30% | 45.85% | 43.85% | 100% |
| Yes (199) | 19.60% | 46.73% | 33.67% | 100% |
Other forms of non-medical advice:
| Employer size | Current/last 12 months | Would provide | Would not provide | Total |
|---|---|---|---|---|
| No (301) | 15.95% | 42.19% | 41.86% | 100% |
| Yes (199) | 21.11% | 38.19% | 40.70% | 100% |
Base (unweighted): All respondents (500)
2.2. Barriers to providing health and wellbeing support
Respondents were asked what barriers they experience to providing health and wellbeing in the workplace. The top three barriers selected were lack of capital (52%), not having the time or resources (49%), and lack of knowledge about which areas to invest in (49%). Added to which, nearly a third of SMEs stated that not knowing where to purchase high quality health and wellbeing support was a barrier to investing. This suggests that, in addition to financial support, SMEs may benefit from advice services to understand what they need and how to procure it.[footnote 13]
Table 2.4 Barriers to supporting health and wellbeing intervention
| Barrier | % of SMEs |
|---|---|
| We don’t have the capital to invest in health and wellbeing initiatives | 52% |
| We don’t have the time or resources to develop and implement health and wellbeing policies | 49% |
| We don’t have the expertise or specialist support to know what health and wellbeing measures to invest in | 49% |
| We wouldn’t know where to purchase high quality health and wellbeing support | 31% |
| The way in which our work is organised does not allow flexibility to accommodate extra activities such as health and wellbeing training | 27% |
| Our employees would not be interested in health and wellbeing initiatives | 19% |
| It doesn’t fit with the priorities of our senior managers | 11% |
| The benefits of investing in health and wellbeing interventions don’t warrant the investment | 7% |
| None of these | 12% |
| Base | 500 |
Base (unweighted): All respondents (500)
Employers could select more than one response, therefore column percentages do not add to 100%
Given that there are observable differences in the propensity to offer support by size of the SME, barriers were also compared by SME size.
Figure 2.5 shows that the relative importance of each listed barrier is similar across companies of different sizes. In general, fewer larger companies report barriers, and they appear to have a better understanding of where to purchase support than smaller SMEs. However, the issues of capital and time to invest in these activities are consistently an issue across all sizes of SMEs, as is the issue of identifying what to invest in.
Figure 2.5 Proportion of SMEs identifying different barriers in supporting workplace health and wellbeing programmes, by company size (n = 500) (multiple choice)
| Company size | 10-19 (179) | 20-49 (186) | 50+ (135) |
|---|---|---|---|
| We don`t have the expertise or specialist support to know what health and wellbeing support to invest in | 50% | 52% | 42% |
| We wouldn`t know where to purchase high quality health and wellbeing support | 33% | 37% | 22% |
| We don`t have the time or resources to develop and implement health and wellbeing policies and interventions | 53% | 49% | 44% |
| The way in which our work is organised does not allow flexibility to accommodate extra activities such as health and wellbeing training | 27% | 24% | 30% |
| Our employees would not be interested in health and wellbeing initiatives | 25% | 16% | 16% |
| We don`t have the capital to invest in health and wellbeing support | 51% | 56% | 47% |
| It doesn`t fit with the priorities of our senior managers or organisational priorities | 8% | 11% | 16% |
| The benefits of investing in health and wellbeing interventions don`t warrant the investment | 7% | 8% | 7% |
| None of these | 11% | 8% | 18% |
Base (unweighted): All respondents (500)
Other evidence suggests that lack of funding is one of the biggest barriers to implementing schemes[footnote 14]. However, the interviews undertaken suggest there are also opportunities to assist SMEs with identifying what type of support is effective to invest in, and with helping them to identify support providers.
The follow-up qualitative interviews were also used to explore the obstacles that SMEs believed they might encounter in implementing health and wellbeing programmes. Again, cost and time came through as key factors:
Obviously there is potentially the cost. Also I guess the other obstacle is the potential amount of time that it takes to do. Those would be them and, I am talking about resources both in financial terms and peoples’ time.
(Information and communication, 10-19 employees)
It would have to be financial and the opinions of the directors, whether they would want to go ahead with something like that, I am not sure.
(Construction, 20-49 employees)
However, when it was suggested that there could be financial support made available, there was also some concern that funding doesn’t come without expectations and administrative burdens:
The problem I’ve always found with any funding that’s available is you end up spending so much time jumping through hoops that at the end you think, wonder whether it was worth it.
(Other service activities, 10-19 employees)
The need for advice and support also came through strongly:
I need the money but with all due respect, most HR people don’t. You need advice and guidance before the money I think.
(Education, 200-249 employees)
If you just get offered money up front you’re thinking ‘now I don’t quite know what to do with it, what am I supposed to do with it?’
(Construction, 20-49 employees)
There are a lot of brokers out there trying to sell you something that’s not always appropriate and they’ll often tell you what you want to hear and then find that it’s probably no good. So it pays to do a lot of research, probably get a referral from other people that are using an effective service.
(Accommodation and food service activities, 10-19 employees)
However, the issue of staff buy-in also came up in these conversations:
So it is more of a generation thing. They are proud, older and male - would not want to talk about mental health – it is already difficult to engage them in staff health questionnaire every year which is just ticking boxes. I think I would have stumbling blocks that I would walk into an empty room, the provider would be there and none of my employees would turn up.
(Manufacturing, 50-99 employees)
We can’t force people to take up the service. The obstacles would be reticence on the part of staff to take it up, they might see it as a weakness.
(Arts, entertainment, and recreation, 10-19 employees)
This research therefore confirms that lack of advice, lack of funding, and administrative requirements all play a role in SMEs offering health and wellbeing interventions to staff. These factors are explored further in the discrete choice experiment which provides insight into how these factors combine to influence that choices that SMEs may make. These findings are reported in Chapter 4.
On the whole, SMEs showed good levels of engagement with the issues of staff health and wellbeing, but current levels of provision are mixed. Currently, some SMEs appear to be doing a lot, whereas others are doing relatively little. Whilst intentions often appear to be good, companies of this size seem to largely be reactive to staff requests and needs rather than proactively promoting health and wellbeing for all staff. As such, there be may an opportunity to enhance provision by bringing information on the types of provision that is available, along with information on its benefits and where to buy it, to the attention of employers. However, financial constraints, as well as time, can be a barrier to adoption. This suggests that both advice and funding may help in supporting employers to take a more proactive approach to investing in employee health and wellbeing.
3. Employers have an appetite to do more
This chapter includes findings from the quantitative survey and qualitative interviews. It explores:
- key areas of health concern for SME employers (section 3.1)
- what outcomes would SME employers aim to improve if given support to provide health and wellbeing schemes? (section 3.2)
- what health and wellbeing schemes would SME employers use additional funding for? (section 3.3)
- would SME employers use funding to purchase new health and wellbeing support or to fund support they already provide? (section 3.4)
3.1. Key areas of concern for employers
When asked in the survey “which of the following do you regard as important health and wellbeing concerns that affect your business/organisation?”, musculoskeletal conditions, common mental health problems and the way work is organised or managed were the top three main concerns raised (all above 70%).
This supports previous research which found these to be the two most common health concerns of employers[footnote 15]. They are the two single most common reasons for sickness absence in the UK after minor illnesses[footnote 16] and the most common health conditions for disabled employees[footnote 17]. The gap between these three areas of concern and the others identified is significant, and suggests that any programme looking to engage SMEs would do well to focus in on these areas.
Figure 3.1 Proportion of SMEs reporting different health and wellbeing concerns (n= 500) (multiple choice)
| Musculoskeletal conditions | 83% |
| Common mental health problem | 81% |
| The way work is organised or managed | 70% |
| Addiction | 29% |
| Low levels of physical activity | 12% |
| Weight | 7% |
| Other | 3% |
Base (unweighted): All respondents (500)
Follow-up interviews found that the concerns around musculoskeletal conditions were driven by two quite different clusters: those that were concerned about low levels of activity doing desk based work along with repetitive movements, and those that were concerned about heavy lifting and physical strain.
One respondent gave an example of where they had provided additional support in the form of physiotherapy:
One of our chefs had a little bit of, we thought it was sciatica, so we knew the doctor would be fairly useless when he made an appointment to go to the doctor’s. They’re not specialists in musculoskeletal, so we use a physio chiro and wellbeing. So we sent him along to the physio for a session and they recommended a few tweaks and exercises and he’s feeling a lot better.
(Accommodation and food service activities, 10-19 employees)
Concerns regarding mental health could be clustered into two groups: those that were aware of the stresses and strains of the workplace, and those that recognised that their staff could have complications outside of work that could also impact on their working life.
The structure, and areas of specialisation, of SMEs can create environments that are stressful and the interview revealed examples of employers that are aware that mental health issues can occur within the workplaces.
Mental health issues, because we operate flexible work shift patterns, the staff can be working on a nightshift one day and they can be on a back shift the next day. They could be working early mornings all week; they could be away from home. That puts a lot of pressure on, or can put a lot of pressure on, people. But then their health needs to be regarded.
(Mining and quarrying, utilities, 10-19 employees)
You would think, looking at the type of work we do, I mean a lot of it is around stress control because of the nature of the work we do. So, I think trying to sort of manage your workloads and keep colleagues’ stress levels down is probably one of the main major key things for us as an organisation to look after their wellbeing.
(Other service activities, 10-19 employees)
Well, I think, realistically, stress is probably the most of concern because of the way our business is run, we do ad-hoc work, so it’s either not enough work and then you’re stressed because you’ve got to try and bring work in, or there’s far too much work and you’re stressed because you’ve got to deliver it all
(Information and communication, 10-19 employees)
Employers recognised that poor mental health can also be exacerbated by issues outside of the workplace, although there are a range of attitudes, with some seeing it as something that work can contribute to, whereas others see it as something that they just need to deal with as an employer:
… and the mental health issues we bring in with us as well to work, you know, we don’t work in a vacuum.
(Professional, scientific and technical activities, 10-19 employees)
The key issue on the health side would be stress and that can be work-based stress or non-work-based stress.
(Arts, entertainment, and recreation, 20-49 employees)
I think that the people have things happening in their lives, sometimes to do with work but also outside of work that cause them to have difficulties. To be anxious or depressed, so I think that that is an issue that most employers have to deal with.
(Information and communication. 10-19 employees)
With regard to emotional care, I think it’s very important that as an employer you holistically understand your team in order to help the company because by empathising and understanding and looking after your team you’re going to get the best from your people in the work environment.
(Other service activities, 10-19 employees)
Anxiety, depression? Yes, there are some examples that I am aware of. I would like to think that those are not caused by work, necessarily. I think some people are just predisposed to that, aren’t they? Again it is something that we are aware of that we try to be supportive of.
(Professional, scientific and technical activities, 100-199 employees)
Some employers felt that some aspects of staff health or wellbeing had impacts on their businesses, but did not seem to see it as their place to do anything about these:
Physical health, as a company, we don’t have much policy in this area. Again, I know you can do quite a bit in this area, but traditionally, my view, and the other directors’ view is, this is starting to cross a privacy boundary.
(Arts, entertainment, and recreation, 20-49 employees)
We lose staff who have issues with alcohol or drugs occasionally and because we employ lots of part-time staff who have to constantly juggle work/life issues.
(Accommodation and food service activities, 20-49 employees)
One SME felt that the way for them to address the issues that they had identified was through how they went about recruitment in the future, rather than an intervention to support those staff already working for them:
Structure of work, yes. I mean there are definitely some managers who perhaps need to work on work/life balance. Again, it is something we’re trying to deal with in ongoing recruitment, among all things we’re striving for.
(Professional, scientific and technical activities, 100-199 employees)
SMEs generally recognise the biggest challenges facing their business regarding health and wellbeing and can articulate why these are a challenge. In most cases they seem to accept the challenges as the nature of their business, and this suggests that there is an opportunity to better support and guide them in identifying proactive steps they could take to address these.
3.2. What outcomes would employers aim to improve with additional support
The follow-up qualitative interviews also explored what kind of outcomes employers would aim to improve by the provision of additional health and wellbeing services. Overall, proactive health and wellbeing promotion was more prominent in employers’ thinking when prompted to think about desirable outcomes.
It was generally appreciated that any intervention would be intended to achieve a change:
The point of running these courses is that the person participating improves whether it be financial, or health, or wellbeing, or, you know, whatever it is. I mean the course would dictate as to what you would expect the outcome to be.
(Other service activities, 10-19 employees)
If we put people in counselling, it keeps them at work. We have paid for things like Weight Watchers for other people in the past
(Education, 200-249 employees)
Key outcomes that SMEs identified that would be both desirable and measurable within their business were reductions in sickness absence and staff turnover:
If it was translated into less sickness days, that would certainly be a positive. And also increased happiness is very important to us. But I don’t quite know how to measure
(Construction, 20-49 employees)
There would certainly need to be a benefit to the practice. But, again, retention is a benefit, and so is them attending work on a regular basis.
(Manufacturing. 10-19 employees)
We would like to limit our staff turnover
(Arts, entertainment, and recreation, 10-19 employees)
That they feel happier and healthier and hopefully I suppose also leading on from that, you would hope that people were encouraged to want to stay longer I think it would be an incentive like ‘I enjoy working here’”.
(Construction, 20-49 employees)
I would hope the staff were happier, more relaxed, felt we were taking their wellbeing seriously and I suppose gluing them a bit more to the business, thinking we are a business worth working for.
(Information and communication, 10-19 employees)
We do monitor attendance and sickness and there are a lot of different factors that could influence that, but how we would monitor it is because it’s on an individual basis, we would be looking to see whether or not we are improving the health and welfare of that individual, just by talking to them, just by consultation.
(Arts, entertainment, and recreation, 20-49 employees)
However, there was also a significant cohort of SMEs within the group interviewed that did not really think about outcomes and measurement, especially employee subjective wellbeing; largely as a result of the size of their workforce and the ability (and desire, as mentioned earlier) to manage things at an individual level.
We don’t have any [outcome measures], it may sound stupid, but because we are so flexible, people like working here, we never really have a problem with that
(Administrative and support service activities, 10-19 employees)
No, I don’t measure specifically, as I say, we’re a small team of twelve so I am able to make judgement calls on a daily basis of how people interact, inter-relate, of if you like happiness within the workplace. I think they’re very difficult to measure, I think you really need your management to be sort of trained and understanding. You probably do need to have some sort of measurement tool if you have a relatively high turnover but then that’s probably going to be part of the problem if we have a high turnover of your managers and your staff. We I don’t think have lost anybody for years, probably ten years or so.
(Other service activities, 10-19 employees)
A theme that ran through many of these interviews was the notion of ensuring that their staff were happy and engaged, and that in itself was seen as a positive outcome that had value to the business. In considering how possible government supported schemes might be framed it would be important to recognise this and articulate both the benefits to the individual employee as well as the business as a whole.
3.3. What health and wellbeing support would employers invest additional funding in?
Within the survey respondents were asked “If additional money were to be offered by government as part of a scheme, which areas would you invest it in?”. The survey presented respondents with the same list of preventative and targeted forms of support that they were asked about in the current provision section, and asked them to indicate which three they would prioritise.
The three most common areas selected for further investment were mental health support or training, help with managing stress, and providing a free or subsidised health service. Services to support employees with existing conditions were less frequently chosen compared to preventative services
As can be seen from Figure 3.2, the differences by company size were small.
Figure 3.2 What would you use the funding for, by company size (choice of top three)
| What would you use the funding for | 10-19 (179) | 20-49 (186) | 50+ (135) |
|---|---|---|---|
| Mental health support or training | 55% | 53% | 61% |
| Help with managing stress | 50% | 55% | 54% |
| Schemes to encourage physical activity | 25% | 25% | 19% |
| Schemes to encourage healthy eating | 13% | 11% | 7% |
| Advice or support for employees to give up smoking | 12% | 9% | 10% |
| Free or subsidised health services offered to all employees | 39% | 32% | 36% |
| Employee assistance programme | 23% | 26% | 27% |
| Other activities, such as campaigns to raise awareness about healthy lifestyles | 10% | 11% | 12% |
| Independent expert advice for employees and line managers on how to manage a condition in the workplace | 16% | 22% | 22% |
| Free or subsidised access to psychological therapy | 9% | 10% | 11% |
| Free or subsidised access to rehabilitative services for physical health conditions | 16% | 14% | 12% |
| Access to programs to address specific problems | 21% | 20% | 18% |
| Other forms of non-medical advice | 7% | 6% | 8% |
Base (unweighted): All respondents (500)
It should however be noted that employers were asked this hypothetical question without further details on the amount of government funding provided, how it would be provided, or how much employers would need to invest themselves. With these additional details employers may give different answers. Therefore, this can only be used to show the areas in which employers are generally interested in investing more, but it cannot be used to estimate uptake of financial support. Uptake, taking into account these additional details, is explored further in the discrete choice experiment in Chapter 4.
3.4. Would employers increase provision or replace existing support?
Figure 3.3 and Figure 3.4 show the proportion of respondents who chose each area within their top three priorities for investment should additional funding be provided (as shown in Figure 3.2) and splits it by whether they already provide support in that area. Figure 3.3, which focuses on preventative support for all staff, shows many SMEs would invest in types of preventative support that they do not already provide (the orange bars). The priorities appear broadly similar between those that would invest the additional funding in entirely new types of support and those that would invest it in support they already provide (either as deadweight or to enhance existing support).
Figure 3.3 Intention to invest in preventative support for all staff compared to current provision (choice of top three)
| Types of health and wellbeing programmes | Currently provide | Do not provide | Total |
|---|---|---|---|
| Mental health support or training | 22% | 33% | 55% |
| Help with managing stress | 20% | 33% | 53% |
| Schemes to encourage physical activity | 9% | 15% | 24% |
| Schemes to encourage healthy eating | 2% | 8% | 10% |
| Advice or support for employees to give up smoking | 2% | 8% | 10% |
| Free or subsidised health services offered to all employees | 10% | 25% | 35% |
| Employee assistance programme | 8% | 18% | 26% |
| Other activities, such as campaigns to raise awareness about healthy lifestyles | 4% | 7% | 11% |
Base (unweighted): All respondents (500)
The intended uptake for support targeted for individuals with known health conditions is lower. However, as can be seen in Figure 3.4 , funding would mostly be used to fund types of targeted support that SMEs previously stated they either already provide or would do if the need arose. It is however also interesting to observe that this funding could also incentivise SMEs to invest in some areas where they had previously stated they would not provide support.
Figure 3.4 Intention to invest in targeted support for individuals compared to current provision (choice of top three)
| Types of health and wellbeing programmes | Currently provide | Would provide | Would not provide | Total |
|---|---|---|---|---|
| Independent expert advice for employees and line managers on how to manage a condition in the workplace | 8% | 9% | 3% | 20% |
| Free or subsidised access to psychological therapy | 3% | 3% | 3% | 9% |
| Free or subsidised access to rehabilitative services for physical health conditions | 2% | 6% | 7% | 15% |
| Access to programs to address specific problems | 3% | 10% | 7% | 20% |
| Other forms of non-medical advice | 1% | 3% | 3% | 7% |
Base (unweighted): All respondents (500)
Where employers stated they would use additional funding to invest in types of support they already provide, this could reflect either ‘deadweight’ (ie. the funding would just subsidise what the employer already provides) or an intention to enhance or expand existing provision of that support type. Therefore, employers were also asked “If your business/organisation received health and wellbeing funding from government, what would you be most likely to use it for?”. As can be seen from Figure 3.5 , over half stated they would use this funding to provide services they hadn’t previously been able to afford, and just over a third would use it to enhance their provision in areas that they were already targeting.
Only 9% of companies stated that they would use the funding to cover the costs of their existing provision. This suggests that in the vast majority of cases the intention would be to increase their provision, rather than use any additional funding to subsidise existing activity.
In the follow-up interviews, one respondent without prompting articulated the benefit of using any government funding to enhance what they are currently providing:
We try to supply lots and lots of support as it is but actually if it was matched by the government I think you’d probably get a lot more.
(Financial and insurance activities, 100-199 employees)
Figure 3.5 What employers would use government health and wellbeing funding for
| To provide health and wellbeing activities in areas that we haven`t been able to afford so far | 52% |
| To buy more of the services that we know are most relevant to our organisation/business | 35% |
| To pay for the health and wellbeing activities that we already provide | 9% |
| Don`t know | 4% |
Base (unweighted): All respondents (500)
These findings provide some reassurance that there is likely to be relatively low levels of deadweight loss whereby employers might take up financial support but spend it on existing activities. Only 9% stated that they would use funding to pay for health and wellbeing activities that they currently provide, and the charts above show internal consistency in the survey responses to validate the stated desire to expand provision beyond activities current undertaken.
In the follow-up interviews respondents were asked “Imagine there were a scheme through which the amount of money you invest in health and wellbeing services for your staff is matched by the government. For example, if you spent £500 on these services, the government would grant you the same amount, £500. Would this make you more likely to provide additional support to your staff? And if so, what would you put this money towards?”
A range of aspirations were articulated, with some employers identifying that this would allow them to do things that they were not currently considering:
It might make me more tempted to do something proactive
(Accommodation and food service activities, 20-49 employees)
The bit that we’re not doing is any preventative, so again, we would then say, ‘Okay, if there was an actual budget, how much would we then do towards preventative?’
(Arts, entertainment, and recreation, 20-49 employees)
Some saw this funding as being an enabler for providing better or different training to their staff:
I would go outside, I would get a provider such as Mind and I would bring them in and do sessions with probably not only for the management team but probably everybody in the business as well.
(Financial and insurance activities, 100-199 employees)
I would have thought the best thing for our type of organisation would be looking at training courses that addressed any preventative issues that could arise
(Other service activities, 10-19 employees)
A distance learning course would probably be easiest. You could have vouchers towards it or whatever and then nobody’s ripping anybody off, it’s all transparent.
(Arts, entertainment and recreation, 10-19 employees)
However, others found it harder to articulate what they would spend the money on. This included both SMEs that simply did not know where to start, and others that were clear they needed more information but would look externally for this:
I think it would be perhaps something that was suggested to us, perhaps schemes that companies that are financially well-off have found successful. So, something that had been backed already.
(Construction, 20-49 employees)
I would maybe do some research and find several initiatives that would match that funding and then go out to the staff and ask, you know, which they think would have the best impact on them.
(Manufacturing, 10-19 employees)
For these employers, providing support and advice alongside financial support could significantly influence their uptake and broadening of the support that they provide to their staff.
There were, however, a small proportion of companies that simply would not engage with increasing their provision in this area, even with the provision of financial incentives. These are discussed later in section 4.6.
4. What impact could a government intervention have?
This chapter presents findings from the discrete choice experiment, and supplements it with findings from the survey and qualitative interviews where appropriate. This chapter covers:
- Structure of the discrete choice experiment (section 4.1)
- The influence of financial support on uptake of support (section 4.2)
- The influence of different forms of advice and guidance on uptake (section 4.3)
- The influence of the type of health and wellbeing scheme in scope on uptake (section 4.4)
- The influence of administrative requirements on uptake (section 4.5)
- Characteristics of employers that would not be interested in using any government advice or funding to access health and wellbeing schemes (section 4.6)
- Forecasts of uptake under different scheme configurations (section 4.7)
4.1. Structure of the discrete choices experiment
The core of this research was the discrete choice experiment in which SMEs were asked to consider a range of different configurations of a financial incentive scheme.
An example of a choice scenario as presented to an employer is shown in Figure 4.1. For an overview of the attributes which described different schemes, please see Figure 4.2.
Figure 4.1 Example of a choice scenario
To understand how different rates of financial reimbursement might affect uptake, schemes varied with respect to the rate of financial reimbursement provided. The availability of complementary advice to support employers in their purchasing decisions was varied to test the importance of advice either alongside a financial reimbursement or as a stand-alone support offer. Other attributes and their levels were included to capture relevant design dimensions for any financial incentive scheme, i.e. what types of interventions would be in scope for purchase, the associated administrative requirements, and how different forms of delivery may influence take up.
Figure 4.2 Summary of DCE attributes and levels
| Attribute | Levels |
|---|---|
| Types of health and wellbeing services in scope for purchase | - Schemes open to all employees, i.e. training and general support schemes - Schemes for employees with known health conditions, i.e. expert-led support and condition management - Both in scope |
| Needs assessment and advice on interventions | No support available – baseline - Online resources available - Personal advisor available |
| Financial support (% of cost is reimbursed) | - No financial support – baseline - 25% of cost is reimbursed - 50% of cost is reimbursed - 75% of cost is reimbursed - 100% of cost is reimbursed |
| When support payment is made | - All paid at the end – baseline - 30% paid up front and 70% paid at the end |
| Administrative requirements | - Only proof of purchase required – baseline - Proof of purchase plus funding request submitted beforehand - Proof of purchase plus requirement to provide data on impacts of scheme - Proof of purchase plus both |
Each respondent was asked to consider six pairs of hypothetical schemes, and for each pair, choose which one they would prefer, or whether they would not be interested in taking up any scheme and instead “continue as now”.
Analysis of responses allowed SME preferences for each attribute to be modelled, including both the direction and strength of their preferences. Employers’ preferences are expressed in units of “utilities”, whereby a positive value means that employers have a positive preference for a specific level of an attribute over the baseline level of the attribute. A positive “utility” value also implies that, all other things being equal, the choice of this level of attribute will increase the likelihood of employers taking up the scheme. Tests were also undertaken to identify whether there were statistically significant differences in the sensitivity of different subgroups of SMEs to the level of attribute on offer (described in more detail in section 6.3.2). See the appendix for further methodological information.
Whilst specific values of “utilities” do not have specific meaning, higher magnitudes correspond to stronger preferences, which translates into higher uptake of the support. Therefore, after discussing the main effects observed in the models this chapter goes on to present illustrative forecasts to show how these models translate preferences into possible uptake (section 4.7).
Both preferences and uptake estimates should be interpreted with caution for the following reasons:
- Hypothetical scenarios can only include a limited amount of detail and so may exclude details that in reality might affect the employer’s decision. For instance, two potentially important details not included in these scenarios include:
- Gross costs of health and wellbeing schemes – in reality, cost is likely to influence employer decisions, and it may also influence the relative importance of other factors, such as financial reimbursement rate.
- Time required to fulfil administrative requirements – whilst the DCE explored the impact of different forms of administrative requirement, it did not specifically test the sensitivity of uptake to different time commitments.
- Responses may be subject to social desirability bias, meaning respondents may choose the more socially acceptable answer (i.e. they would provide support) even if it’s not the choice they would make in reality.
- The sample of respondents excluded micro employers (with fewer than 10 employees), who may be less likely to uptake formal health and wellbeing support.
4.2. The influence of financial support on uptake of support
4.2.1. The importance of the rate of the financial incentive
There were two aspects of financial support that were varied within the scenarios employers were asked to consider (Figure 4.3): the rate that would be reimbursed and when that payment would be made.
Figure 4.3 Financial support attributes
| Attribute | Levels |
|---|---|
| Financial support (% of cost is reimbursed) | - No financial support – baseline - 25% of cost is reimbursed - 50% of cost is reimbursed - 75% of cost is reimbursed - 100% of cost is reimbursed |
| When support payment is made | - All paid at the end – baseline - 30% paid up front and 70% paid at the end |
Five different reimbursement levels were considered: None, 25%, 50%, 75% and 100% (i.e. full reimbursement).
As expected, as the rate of reimbursement increases, the likelihood of choosing an option increases, all other things equal. However, results showed diminishing returns on employers’ likelihood to choose an option from higher rates of reimbursement.
This is demonstrated in Figure 4.4. A steep slope is found for the reimbursement ranging from 0 to 50%, which implies that within this interval, SMEs show a high preference for higher reimbursement rates. The slope then flattens slightly after the 50% reimbursement level, indicating that whilst respondents still respond positively to higher levels of reimbursement, the impact of these increments is reduced. In practice, this means that for a given pool of funding, greater impact can be achieved by funding a larger group of SMEs at 50% reimbursement than half as many SMEs at 100% reimbursement.
Figure 4.4 Relative preferences for reimbursement of cost (percentage of incentive amount being reimbursed)

There were no statistically significant differences in preferences for financial reimbursement between different subgroups of SMEs.
4.2.2. The influence of when costs are reimbursed
In the survey, 52% of SMEs reported “lack of capital to invest in health and wellbeing initiatives” as a barrier to investment. Therefore, to test whether cash-flow constraints might pose an issue for SMEs to take up a support offer, the experiment varied the timing of the payment of any incentive between: payment was made on delivery, or payment was structured so that 30% was paid up front and the remaining 70% on delivery.
The choice data reveals that this had no statistically significant impact on the choices that SMEs indicated they would make, and there were no differences by subgroup either.
Further probing with respondents in the follow-up interviews confirmed that for many SMEs the issue of payment structure was less important in this context. For some this was due to their financial good health:
Once again, that’s the beauty of being a long-standing business, you’ve built up reserves over a period of time.
(Administrative and support service activities, 10-19 employees)
No, it wouldn’t make any difference to me. (Interviewer: okay, so for you that doesn’t matter at all?) No, we don’t struggle with cash flow.
(Real estate activities, 10-19 employees)
Others were used to the concept of significant time elapsing before receiving payments in other areas:
I don’t think it would make a massive difference as long as it was … even if you got paid at the end. I don’t think that would be a barrier.
(Professional, scientific and technical activities, 100-199 employees)
How we get the money or when doesn’t really make any difference. In our culture, in education, even if you’re promised funding next year, we’re still happy.
(Education, 200-249 employees)
For one interviewee, the issue was more about how any scheme should be structured to ensure that it was not abused:
I can’t see how a percentage paid upfront would work, I don’t think the auditors would say, ‘Well yes, where’s that money going to and how is it being spent?’ How can you prove that taxpayer’s money isn’t being corruptly spent? I can’t see that one working.
(Arts, entertainment, and recreation, 20-49 employees)
However, this was not the case for all SMEs. Some explained that they have cash flow issues and they could benefit if an element of up-front payment was in place:
It’s obviously very beneficial to get money up front because small companies, most companies generally, have cash flow issues and so you know, spending out and not getting money until later would stop you doing something.
(Other service activities, 10-19 employees)
I think probably upfront would be most likely to be acceptable at the moment, because they would have something going forward. I don’t think it would necessarily be a deal-breaker though, to think that we paid initially, or only got some upfront and some after.
(Construction, 20-49 employees)
For a number of the SMEs interviewed the issue was less about receiving payment in advance, and more about timely repayment following delivery:
The longer you starve a small company of income it’s the bigger threat you place on the company. So, I would say the shorter term would be preferable.
(Mining and quarrying, utilities, 10-19 employees)
For cashflow, obviously, we would always prefer a speedier reimbursement, because it puts pressure on us in the bank really. It depends if it’s a good year or we’re on hard times.
(Construction, 20-49 employees)
Two respondents raised the idea that the reimbursement could be provided through the tax system:
The government could also do with taking over a tax bill, that’s another way the government could do it. So therefore, it would have to be within the year.
(Manufacturing, 50-99 employees)
If they were considering setting up a scheme, particularly on matched fund schemes, then I wouldn’t expect the money upfront and any claim back system means that it has a huge administrative burden. If there was a discount on tax, for instance, then if that went into an allocated account very similar to the tax-free childcare accounts that are run nowadays. So, you pay in, they top up and then you allocate the spend against people who are approved.
(Arts, entertainment, and recreation, 20-49 employees)
From the responses received in both the survey, interviews, and discrete choice experiment, it was clear that for the majority of SMEs the payment structure was unlikely to significantly influence their decision as to whether or not to participate.
4.2.3. How much employers are willing to spend in total
The choice experiment tested reimbursement in the form of a proportion of the cost of the health and wellbeing programme, and as discussed earlier, the DCE provides insight into the positive impact that these have on uptake.
Whilst this provides useful insight, it does not provide information on the absolute value that SMEs might be willing to consider spending, or the sensitivity to different absolute levels of any incentive. The follow-up interviews further explored SMEs understanding of the cost of providing support and whether they had a sense of how much they would be willing to spend in this area.
Most SMEs stated that they had a limited idea of the costs involved in providing workplace health and wellbeing programmes. Those that were able to make an estimate had quite different expectations:
(Interviewer: Coming back to health and wellbeing interventions, are you aware of how much health and wellbeing interventions usually cost?) No, actually. I imagine it could be very expensive to get the right things in place.
(Accommodation and food service activities, 10-19 employees)
Those private education, upskilling … you know … you want to keep moving up that scale doing something more and more. For a first aid course it’ll cost you 100 quid plus VAT. I imagine you’re looking at 500 quid per person for, you know – I haven’t looked into the more intense courses. I did the mental health care one and that was £100. … We’d probably put anywhere up to £500 to £1,000 in. Those courses, I know they vary in price, some are very good and you get what you pay for.
(Arts, entertainment and recreation, 10-19 employees)
We’re not a big company so we can’t afford just to throw money at stuff for no reason. But I think things like the Fit for Work, the Pilates, they weren’t expensive, in fact I think we got it subsided initially, but it just started people thinking about things that they could do together as a team. So, we did the yoga, we did Pilates and then we started walking and we’ve done various events and different people in the company have done different events because everybody can go and walk to some level.
(Other service activities, 10-19 employees)
We’re assuming that there would be not an extortionate but a reasonable cost to it, so yes, it’s not something that we’ve ever got to the point of considering really.
(Construction, 20-49 employees)
This in itself highlights one of the major challenges in this area: SMEs often have little sense of what sorts of interventions they could put into place, or the likely cost of these.
Turning to how much they would be willing to spend in this area, most SMEs struggled to answer this; in part because they had little idea of the costs involved, but also because these were conversations that they had not had within the business to date.
I have no idea. That’s like how long is a piece of string. I have really no idea.
(Professional, scientific and technical activities, 100-199 employees)
I think if they (the partners) thought it would have an obvious and definite outcome of making staff happier, increasing productivity and increasing retention, then the more they would be willing to pay. Whereas, if they think it’s not something that they’re not sure is going to work or not and people just sort of dip in and out of, then obviously they’ll probably think ‘no, we’re not willing to pay for that’. So something properly set up, they’d be willing to pay, but I don’t know what to quantify really in terms of amount.
(Construction, 20-49 employees)
Many of the smaller SMES stated that they approached things on an “as needed” basis and did not explicitly plan for spend in these areas, and those that did expressed concerns around budget constraints:
I’m always aware that I have to cut things off, if the budget won’t allow it, I will have to terminate whatever those extra luxuries are, and I’m afraid this would have to come in the form of ‘luxuries’, because salary is the one thing the staff really need.
(Construction, 20-49 employees)
Cost is important but it’s not the be all and end all. If someone said you can have a tailor made plan for, let’s say £25 a week or £300 a week, I’d have to say no to £300 a week and I’d have to say yes to £25 a week, that sort of thing. So it’s all what comes within affordability for us.
(Accommodation and food service activities, 10-19 employees)
The larger SMEs were more likely to have budgets in place that they could imagine utilising for these sorts of activities:
We normally have a training budget of close to about £100,000 which in our size of business is quite a lot of money. And I would say we would probably be prepared to spend probably 20 to 25 percent of that on those types of courses.
(Financial and insurance activities, 100-199 employees)
Other interviews highlighted both challenges as well as opportunities from getting value for money by purchasing services in the private market. One interviewee also expressed concerns about whether they would get value for money out of what they purchased in the private market:
One of the concerns I have would be that you got into a programme where the main purpose of it was to make money for the people providing it, rather than resolving the problem. In that sense, I would favour a more publicly structured, publicly funded intervention rather than people coming along saying, ‘We’ll set up a stress help line for you.’
(Information and communication, 10-19 employees)
Another SME highlighted potential economies of scale benefits that could be obtained from purchasing in services from external providers, but they did not identify what they described as an employee assistance programme or have any sense that such services were available within the market:
If you can provide a number for your staff to call, let’s say, for health and wellbeing, or for you to call in the initial instance and then hand over to your staff to say I’ve got a staff member who’s got problems at home that needs some counselling, they’re stressed, and you can then hand that phone to that member of staff and go, ‘Here’s a counsellor’ and you know that that’s costing you £12 a month, say, then that’s fine. And if that satisfies a need, that’s great. I think if you have something more complex that costs £300 a month, so many business have thought that out and would rather wing it, and handle it if the need arises, so it’s got to be cost-effectiveness to the organisation but deliver the right result as well. That’s why a big organiser could step and say, ‘We’ve got a health and wellbeing module’ which they can show us. It’s 25 quid more in your policy, because they’re paying a game of averages. They know if 20,000 companies sign up to it, 20,000 people aren’t going to phone them every day with health and wellbeing issues. But they can cover having 12 full-time counsellors sitting on a desk ready for a phone call.
(Accommodation and food service activities, 10-19 employees)
Overall, the follow-up interviews highlighted that few employers had already engaged with considering how much they might be willing to spend and the actual cost of purchase.
4.3. The influence of different forms of advice and guidance on uptake
In the survey, 49% of employers responded that a lack of “expertise or specialist support to know what health and wellbeing measures to invest in” was a barrier to them. The choice experiment therefore tested whether the provision of an upfront needs assessment, to help them better understand staff health needs or on how to source or implement best-practice schemes to address those needs, would increase uptake of the government support package. In addition, the experiment also varied whether this advice would be delivered through online resources or through a personal advisor. This provided insight into the possible impact of advice, as well as employers’ preferences in terms of format of that advice.
4.3.1. The importance of access to advice and guidance
The modelling of the responses to the DCE revealed that providing support and advice has a statistically significant positive impact on the likelihood of choosing a scheme.
Moreover, respondents that indicated that they had lack of ‘expertise to know what health and wellbeing support to invest in’ were more likely to take up schemes that included advice about what to invest in. This cluster of SMEs were also less likely to choose the “continue as now” option irrespective of the specifics of the schemes on offer.
In the follow-up interviews, respondents stressed the difficulty of navigating this area and the difference that well collated sources of information or pre-packaged schemes could make:
I think it takes a lot of time to research it and investigate it. It is something that gets suggested every so often as a nice to have and then there’s the limit in terms of anyone having the luxury of time to research it. I think there’s not a pressing need because if there was, it would be higher on the priority list. As it is, it doesn’t seem to be an urgent requirement which is why we just haven’t got round to it yet.
(Professional, scientific and technical activities, 100-199 employees)
I’d like a resource where you could refer to a … I don’t know, a directory maybe, or a provision resource where they would say this is what you … these are the options open to you because I don’t think there is anything like that.
(Mining and quarrying, utilities, 10-19 employees)
It’s a bit like the cycle scheme or something, as soon as there’s a scheme set up, you can think ‘I could ask about that, we could find out about how it works and how much it costs and what kind of levels of things you can partake in’. So yes, it would really help.
(Construction, 20-49 employees)
In the follow-up interviews, respondents articulated the sorts of advice they would be seeking:
I think we’ve identified the need, it would be finding people that can offer solutions. I think having done a needs assessment across the employee range, we would focus on those that obviously need a tailored approach.” (Financial and insurance activities, 10-19 employees)
In the past, we’ve had outside advice for people with, you know, specific physical needs, and we’ve taken their advice and taken advantage where there are grants for putting pieces of equipment in to users as well.” (Financial and insurance activities, 10-19 employees)
I think it would be good to have some guidance around engagement, so how you engage employees with the programme, what the best way is to communicate it and make sure that the message is delivered in the right way and that it’s something for them rather than the company saying, we’re doing this and you kind of just have to go along with it.” (Manufacturing, 10-19 employees)
In some of the choices, respondents chose options that had advice and guidance but no financial reimbursement, over a support package that would have some financial reimbursement. This confirms that just providing a point of access to schemes can, in itself, have benefits and lead to engagement and uptake. This is explored further in section 4.7.
In the follow-up interviews some respondents suggested advice could either take precedence over, or be a prerequisite to, the level of funding provided:
(Interviewer: So, would it be more important for you to actually have access to advice or to receive finding to assist with rolling out those programmes?) Well both would be good, but I think advice is more important. Because advice you’ve got choices, haven’t you? You’ve got options. It’s just having money that is available. It probably isn’t going to get used because people probably won’t understand how to use it, but it would be a good back-up to have there if you’ve made choices that were going to cost you something.
(Mining and quarrying, utilities, 10-19 employees)
(Interviewer: Would it be more important for you to actually have access to some advice or receive some funding to assist with rolling out new health and wellbeing programmes?) Well, I suppose a bit of both, because I think, initially, the advice would be the most important, what is it we could do, and then if there’s funding available following on from that, you would go, ‘Yes, I would like to do that and good, there’s some funding that comes with it that would help get it over the line.’ So initially, I think advice as to what would be good, because I think if you just get offered money upfront, you’re thinking ‘now I don’t quite know what to do with it, what am I supposed to do it?’
(Construction, 20-49 employees)
Taken alongside the discrete choice responses, these qualitative findings reinforce the idea that SMEs face difficulties in navigating this area, and the potential importance of providing support resources alongside funding. Just signposting schemes and making them accessible to SMEs appears to have an important impact.
4.3.2. Delivery of advice and guidance: Online versus personal advisor
Within the choices, two different forms of advice were offered: access to online resources or access to a personal advisor. Overall, this distinction had very limited impact on SME’s choices. However, the analysis identified two specific subgroups who do put particular value on one mode over the other.
There was a higher likelihood of choosing options involving online advice amongst SMEs that indicated that they have a lack of knowledge about where to purchase this support. This group of respondents valued having these online resources 76% higher than those that did not express difficulty with knowing where to purchase support.
Preferences for online support resources were also expressed in some of the follow-up interviews:
Yes, I’m quite happy to receive guidance, it needs to be easily understandable and succinct, obviously, because of the time constraints. So yes, something very useable, not a great big weighty document because I haven’t got time to read it, sorry. (Interviewer: Would that better be provided online or in person?) I’m quite happy to do online things.
(Construction, 20-49 employees)
I think we’re a digital age so online is fine.
(Manufacturing, 10-19 employees)
Probably online because then I could do it like a webinar rather than having to make specific appointments, so I could fit it in and complete the webinars rather than have, you know, have set times, same place.
(Professional, scientific and technical activities, 10-19 employees)
However, other SMEs felt that whilst online support would make most sense in the first instance, they would also value the opportunity to follow up with access to someone that they could ask questions of:
I think it’s probably easier to access online, but it’s probably easier to understand if it’s in person because in person you’ve got the opportunity to ask questions. And there’s only a limited flexibility of online services that provide that.
(Mining and quarrying, utilities, 10-19 employees)
I think online initially would be probably something that would be fine, but if there was then an option where you wanted to investigate something specific and someone coming in could get down to the nitty-gritty of what it involved, then we would be open to that. But I think, initially, online, to be able to read about it and investigate it that way would be the first thing.
(Construction, 20-49 employees)
In the choice experiment, SMEs that stated that they currently employed staff with long term conditions or disabilities had a greater likelihood of choosing options involving advice via a personal advisor. This group of respondents valued having access to a personal advisor 95% higher than the SMEs that did not employ staff with long term conditions or disabilities.
4.4. The influence of the type of health and wellbeing scheme in scope on uptake
Within the choices, employers were offered the same two types of health and wellbeing scheme that they were asked about in the survey when considering current provision. These include:
- Schemes aimed at proactively promoting health and wellbeing for all employees (e.g. cycling schemes, stress management schemes or EAPs).
- Schemes specifically supporting employees with existing health conditions, (e.g. Occupational Health services or physiotherapy).
As well as the ‘continue as now option’, the other two options within each of the choices included support accessing either one or both of these types of scheme. The responses were used to estimate how the type of scheme offered would affect uptake of that support.
Most SMEs placed a similar value on both types of scheme. Employers were more likely to invest in schemes including both types of support than just one type of support; meaning SMEs prefer schemes which are broader in their scope, as would be expected.
SMEs that currently employed staff with long term conditions or disabilities were more likely to take up support for either or both type of health and wellbeing scheme than other SMEs, but the premium they placed on support for health promotion schemes was higher than that on support for targeted schemes.
One of the respondents in the follow-up interviews articulated the influence of their previous experience and how this was leading to them thinking differently:
(Interviewer: Would you say that your interest in providing health and wellbeing arrangements changed in light of that one employee with his long-term health conditions?) Yeah, definitely. We’re more aware of it, we’re more able to react, you know, we’re aware of what options we can employ, what choices we can make. Going forward we’re planning on expanding, as I mentioned earlier, and we’re making sure when people come in that they’re aware that the flexibility is there to accommodate sort of any pressures that might cause them a problem.
(Mining and quarrying, utilities, 10-19 employees)
As has been noted previously, one of the challenges for SMEs is to know what support is available. However, many of the employers in this group, or their employees, may already have support contacts in place. They may also be more aware of the value of actively retaining staff in the workforce and hence place more value on preventative interventions.
SMEs with a high proportion of technicians and skilled tradespeople (over 50% of employees) showed a weaker preference towards targeted programmes being supported than other SMEs, although they would still prefer having these within scope than not.
In the follow-up interviews, a range of opinions were offered about the types of scheme that employers would value most. There was a cluster that expressed the importance of preventative actions:
Preventative is better because once the issue’s there it’s sometimes harder to get rid of. So, if there are preventative courses in place to try and tackle before you get to the worst-case scenario then that’s better.
(Other service activities, 10-19 employees)
However, there was a second cluster that recognised that whilst preventative actions were desirable, often in practice they find themselves being more reactive, and that this is when funding and support could really make a difference:
When you are facing those issues on a day-to-day basis you are going to be more responsive to them.
(Human health and social work activities, 50-99 employees)
Therefore, both types of schemes are considered important and whilst some SMEs might prefer to utilise the support for health promotion schemes for all employees, many would also use it for targeted schemes when specific needs arise.
4.5. The influence of administrative requirements on uptake
The choice experiment included information on the administrative requirements that would be expected of employers as a condition of receiving the financial reimbursement. The baseline for this under any circumstance where funding was accessed was that proof of purchase would have to be provided. However, the DCE also explored whether a requirement to make a funding request before purchasing the support, and/or a requirement to provide data on the impacts of the scheme (such as data on sickness absence or staff uptake) impacted on the likelihood of choosing a given scheme.
Requiring the SME to provide a funding request beforehand had no statistically significant impact on the likelihood of choosing the option. However, the hypothetical scenarios did not include details on the actual time requirement of participants, meaning that respondents based their responses on their own assumptions about the actual time commitment of these administrative requirements. Therefore, despite these findings, it is possible that SMEs’ decisions are sensitive to time commitment required.
This possibility is reinforced by the follow-up interviews which suggested that administrative requirements would not be a problem as long as they are proportionate and accessible. For example, some SMEs felt very comfortable with the idea of schemes having administrative requirements:
We have people that are looking at quite detailed applications on a regular basis, so it’s not a problem.
(Financial and insurance activities, 10-19 employees)
However, there were a number that emphasised that these requirements needed to be proportionate to the funding and support being provided:
You can apply for a funding pot of money for 20 grand and it’s one sheet of A4, or you can apply for the same 20 grand and it’s 20 sheets of A4. You could apply for a quarter of a million quid and it’s not as complicated as the £20,000 bid. So, I think sometimes it’s … you know, the people who are giving out any money need to be realistic in terms of the level of funding they are giving out as to what sort of level of information they require from an organisation.
(Other service activities, 10-19 employees)
Well, we’re very used to reporting, we spend our whole life reporting, I think it needs to be in proportion, to be honest. With our grants programmes, if someone is getting a grant of £10,000 or £100,000 or £10, we would expect the reporting to be in proportion with the amount of money.
(Human health and social work activities, 20-49 employees)
We don’t have a large amount of administrative time left over, but I think, saying that, if it wasn’t like constant, if you just did it once a year or once every six months or something, and it wasn’t a really long, difficult process to fill in, the form was like ticking boxes and stuff like that, then I can’t see that that would be an issue.
(Construction, 20-49 employees)
If it was too onerous, we would have to weigh up the benefits to how difficult it was to get the support, so yes, that would have a bearing. We can’t just hire more staff just to administer a health and wellbeing scheme, that’s not going to happen.
(Construction, 20-49 employees)
If it takes an awful long time to actually fill all the forms in and go through the hoops, then that’s going to be less interesting to us because, obviously, time is money, but otherwise, I think it will be fine. Obviously, there will be an element of having to say what you’re going to spend the money on, what you think the outcomes are going to be, how you’re going to measure them and all of that stuff.
(Financial and insurance activities, 10-19 employees)
Some SMEs also had concerns about the complexity that can be involved in applications and the need to make them accessible:
I think there’s not a problem with requiring a lot of detail as long as the people who are expected to provide it understand what’s expected. So, there would need to be an education step introduced prior to the level of detail for the report process.
(Mining and quarrying, utilities, 10-19 employees)
I know it’s not quite the same, but it would be good to use the example of the apprenticeship levy. There is just a wide feeling that no one understands it. So we haven’t taken advantage of it because no one understands it. The amount of times we’ve tried to access it and it just seems overwhelmingly complicated, so that’s a barrier.
(Professional, scientific and technical activities, 100-199 employees)
Including a requirement to provide data on the impacts of the scheme had no significant impact on the choices that SMEs made. This therefore did not appear to be a barrier to participation.
In the follow-up interviews a number of SMEs articulated that this was not a concern, and they would expect this to be a requirement within these forms of support.
(Interviewer: And if you had to provide data on the outcomes of the scheme would that affect your level of interest?) No. We’re used to that.
(Other service activities, 10-19 employees)
(Interviewer: And if you had to provide data on the outcome of the schemes would that affect your level of interest?) No. I mean as long as I knew what was expected, or the companies know what is expected, I don’t see any reason why they shouldn’t be able to provide it.
(Mining and quarrying, utilities, 10-19 employees)
Outputs have to be recorded. We’ve done that for the last five years on the last bit of spending we got, and that’s not a problem at all.
(Accommodation and food service activities, 10-19 employees)
4.6. Characteristics of employers that would not be interested in using any government advice or funding to access health and wellbeing schemes
Within the DCE, 16% of respondents always chose to “continue as now” in the six choices that they were offered, meaning they did not wish to use any of the variations of the advice or funding support that they were presented, which by design would have included some scenarios with 100% reimbursement.
One explanation could be that this group of SMEs already provide or intend to provide this type of health and wellbeing scheme for their staff and would just prefer not to use government advice or funding (the DCE specifically tested whether employers would choose to use the government advice or funding to support buying health and wellbeing schemes for their staff, rather than testing specifically whether they would provide the health and wellbeing scheme). For instance, SMEs that currently have good levels of provision in place and already provide higher levels of proactive preventative health and wellbeing support (in four or more areas) are less likely to choose to use government support. The same applies to those that state that they feel they already have the expertise to know what health and wellbeing support to invest in. The survey data also shows lower levels of stated uptake amongst charities and quasi-public sector firms compared to private companies.
The fact some SMEs would prefer not to use government support was also supported by the interviews. There are SME employers that feel that this is not something that public money should be funding. One respondent in the follow-up interviews stated:
No, because I’m not really a big fan of that. You should stand on your own two feet, it’s not the place of the government to do that, in my opinion. I think it’s community, it’s your communities, whether they be the work community, a church community or your local community. We’ve put too much emphasis on the government doing things rather than us, we have a personal responsibility to help each other, not the government.
(Administrative and support service activities, 10-19 employees)
Another possible explanation for SMEs who would not choose to use any government support is that they are simply not interesting in providing any health and wellbeing schemes for their staff. It is therefore encouraging that this is a relatively small group of SMEs as it suggests most SMEs have at least some interest in providing health and wellbeing schemes for their staff.
Willingness to engage with the schemes is lower amongst the smallest SMEs with 10-19 employees, and those where the owner or senior team makes any decision around investment in health and wellbeing, rather than an identified HR team (which may also be a reflection of size). This corresponds with comments in the follow-up interviews suggesting that they often consider requirements on a case-by-case basis and see supporting their staff as part of running a small business.
As noted earlier, there is also a small cohort of employers that do not currently provide any support for their staff in this area, and believe that they would struggle to engage their staff with participating in anything that they might put into place. When asked explicitly about the impact that financial support in this area could have, one interviewee stated:
No, I don’t think that would influence us doing it. (Interviewer: so it’s just basically there is currently not really the interest of the employees for things like that.) Exactly, no.
(Manufacturing. 20-49 employees)
The way that the support options are explained and framed could also have an impact on uptake and engagement. In the survey responses the uptake of government support was lower for those SMEs that stated “low levels of physical activity” as one of the more important health and wellbeing concerns for their company, whereas it was higher for those that identified addiction as an important concern. The wording used to articulate the scope of the support available did not intentionally differentiate which areas might be supported. However, these differences suggest that when developing a scheme there would be merit in careful review and testing of any wording in the supporting materials to ensure that they accurately convey the scope of what could be supported and do not inadvertently lead to lower engagement for certain target activities.
4.7. Forecasts of uptake under different scheme configurations
The discussion in the preceding sections of this chapter covers the relative preferences that respondents indicated through the choice experiments for changes in each individual attribute when all other things are held equal. In this section, the choice modelling approach is used to forecast the uptake of government support packages and to show the relative impact on uptake of changes in how the support package is configured.
However, it is advised that specific uptake estimates should be interpreted with extreme caution for the following reasons:
- They assume 100% of SME employers are aware of any scheme. In reality, raising awareness of such provision amongst SMEs can be challenging.
- Hypothetical scenarios can only include a limited amount of detail and so may exclude details that in reality might affect the employer’s decision. For instance, two potentially important details not included in these scenarios include:
- Gross costs of health and wellbeing schemes – in reality, cost is likely to influence employer decisions, and it may also influence the relative importance of other factors, such as financial reimbursement rate.
- Time required to fulfil administrative requirements – whilst the DCE explored the impact of different forms of administrative requirement, it did not specifically test the sensitivity of uptake to different time commitments.
- Responses may be subject to social desirability bias, meaning respondents may choose the more socially acceptable answer (i.e. they would provide support) even if it’s not the choice they would make in reality.
- The sample of respondents excluded micro employers (with fewer than 10 employees), who may be less likely to uptake formal health and wellbeing support.
- The survey collecting the attitudes and choice making behaviours on which these models are based was undertaken prior to the Covid pandemic, and it is possible that attitudes towards issues of employee wellbeing may have changed in the intervening period.
The sample was intentionally stratified to give coverage of a wide range of SME types. The analysis has therefore applied weights to the sample in order to produce forecasts that more closely represent the outcomes expected from the true distribution of SMEs. Detailed information on generating the weights is discussed in section 6.3.5 of the appendix.
Figure 4.6 shows an example of a policy scenario test. This reference case option considers a policy where:
- Health promotion schemes open to all employees are supported
- Targeted schemes for employees with known health conditions are not supported
- There is no advice available
- 50% of the cost will be reimbursed
- Payment would be received 30% up front and 70% at the end
- A funding request beforehand would not be required
- Data on impacts of the scheme would not need to be provided
Figure 4.6 Example of a policy scenario test
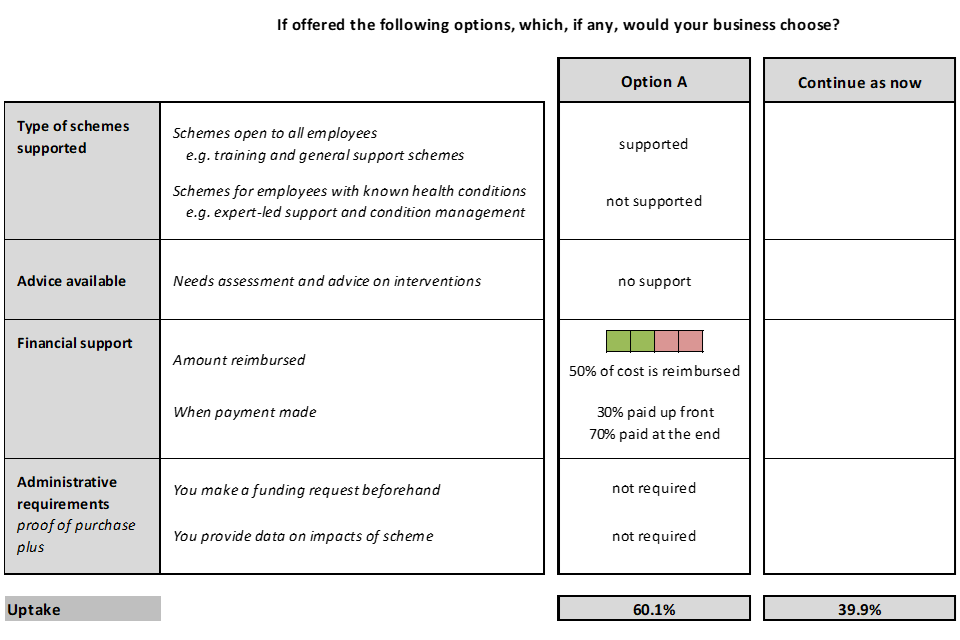
Under this scenario the forecasting model predicts (based on the results of the DCE) that 60% of SMEs who are aware of the government support would choose to use it.
If the policy scenario is then changed such that funding supports targeted schemes for those with known health conditions, but not health promotion schemes open to all employees, the forecast uptake drops to 58%. If the support package was changed to support both types of health and wellbeing programme, the forecasted uptake increases to 70%. This reinforces the earlier finding that uptake can be maximised by including both types of scheme within the scope of the support package.
Changes can then be made to the level of support and advice provided and their impact on each of these scenarios (holding the financial support at 50% reimbursement). The scenarios tested and their predicted outcomes are shown in Table 4.1.
As can be seen from these scenarios, providing advice, in addition to matched funding, can improve the level of uptake by between seven and nine percentage points.
Table 4.1 Forecasts of uptake of different supported schemes, holding level of reimbursement constant at 50%
| Supported schemes | No advice available | Online resources available | Personal advisor available |
|---|---|---|---|
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are not supported |
60% | 68% | 69% |
| - Schemes open to all employees are not supported - Schemes for employees with known health conditions are supported |
58% | 66% | 67% |
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are supported |
70% | 77% | 78% |
Base (weighted): All SMEs employing 10 or more staff
It is also possible to forecast how varying the level of reimbursement impacts on the predicted uptake. These scenarios are based around the reference scenario previously discussed, where there is no advice provided. The sensitivity of uptake to the level of reimbursement is shown in Table 4.2.
Table 4.2 Forecasts of uptake under different levels of reimbursement, assuming no advice available
| Level of reimbursement provided | 0% | 25% | 50% | 75% | 100% |
|---|---|---|---|---|---|
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are not supported |
34% | 47% | 60% | 67% | 73% |
| - Schemes open to all employees are not supported - Schemes for employees with known health conditions are supported |
32% | 45% | 58% | 65% | 71% |
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are supported |
45% | 58% | 70% | 76% | 81% |
Base (weighted): All SMEs employing 10 or more staff
These forecasts illustrate some of the findings discussed earlier:
- There is a willingness to engage without any funding, and just making schemes accessible appears to lead to significant uptake; the model forecasts on the basis of the choices made by respondents in the survey that 45% of SMEs would participate in an identified programme if it supported both preventative and targeted schemes.
- Moving to matched funding can increase the uptake by 25 percentage points, taking the level of uptake to 70% of SMEs.
- The impact of doubling that funding to fully cover all costs has a smaller impact, with a forecasted increase in the uptake of 11 percentage points, taking the level of uptake to 81% of SMEs. This reinforces the finding that under constrained resources greater impact can be achieved (in terms of uptake) by providing matched funding to a given number of SMEs than full funding to half that number.
A difficulty with these forecasts is that it is unclear how much of the uptake without funding is due to activities that would already have occurred, and how much is prompted by the act of offering access to these schemes. The assessment presented in section 3.4 suggests that the deadweight loss from employers investing in areas where they are already undertaking activity is likely to be low. However, for the purposes of interpreting these forecasts it would be prudent to take the forecasted uptake at zero reimbursement shown in Table 4.2 as a baseline and then pivot the incremental scheme impacts from this. As discussed at the start of this section, there are a number of caveats which add merit to the use of a conservative approach.
It is interesting to then change the level of advice provided from no advice to “online resources available”. Table 4.3 shows the sensitivity of uptake to the level of reimbursement with the level of advice held constant at online resources available.
Comparing table 4.3 to table 4.2 illustrates that the impact of providing additional access to advice differs according to the level of reimbursement (and hence the reference point on the demand curve). Advice has greater impact at lower levels of reimbursement and can be observed to increase forecast uptake by eight percentage points at the 0 to 50% levels of reimbursement, but this drops to a five percentage points difference when both types of schemes are in scope at full reimbursement.
Table 4.3 Forecasts of uptake under different levels of reimbursement with online support resources
| Level of reimbursement provided | 0% | 25% | 50% | 75% | 100% |
|---|---|---|---|---|---|
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are not supported |
42% | 55% | 68% | 74% | 79% |
| - Schemes open to all employees are not supported -Schemes for employees with known health conditions are supported |
40% | 53% | 66% | 72% | 78% |
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are supported |
53% | 66% | 77% | 82% | 86% |
Base (weighted): All SMEs employing 10 or more staff
As discussed previously, the payment timing has relatively little impact on uptake. For example, for the policy with 25 percent reimbursement, both types of schemes being supported and online advice being available, changing from 30% payment in advance to all paid at the end reduces uptake from 66% to 64%. Even in the most attractive scenario of full reimbursement, both types of schemes being supported and online advice being provided, moving to all payment at the end only reduces uptake from 86% to 84% . The impacts are therefore relatively marginal for a change which could add significant complexity to the operation of a programme.
The absolute cost of any scheme was not explicitly covered in this research and was out of scope for the choice experiment, so it is not possible to make statements about how this might impact on the importance placed on timing of reimbursement. However, it would be reasonable to expect that the reimbursement timing could become more important as the values under consideration increase.
4.7.1. Differences in uptake by whether currently employ staff with long-term health conditions or disabilities
About a third of the SMEs in the sample had employees with long-term health conditions or disabilities, and this was found to be a factor that influenced how attractive different SMEs found the schemes being offered. Table 4.4 and Table 4.5 take the scenario in Table 4.3 and segment the results by whether the respondent had an employee with a long-term health condition or disability or not.
This illustrates the scale of the difference in engagement between these two groups. Under the matched funding scenario, the model forecasts 72% of SMEs that do not currently employ staff with long term conditions would use government support if it covered both types of scheme. In contrast, the same programme is forecast to be adopted by 85% of SMEs that currently employ staff with long term conditions.
Table 4.4 Forecasts of uptake under different levels of reimbursement, assuming online resources available, for SMEs with no staff with LTCD
| Level of reimbursement provided | 0% | 25% | 50% | 75% | 100% |
|---|---|---|---|---|---|
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are not supported |
38% | 51% | 65% | 71% | 77% |
| - Schemes open to all employees are not supported - Schemes for employees with known health conditions are supported |
37% | 50% | 63% | 69% | 75% |
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are supported |
47% | 60% | 72% | 78% | 82% |
Base (weighted): All SMEs employing 10 or more staff
Table 4.5 Forecasts of uptake under different levels of reimbursement, assuming online resources available, for SMEs that employ staff with LTCD
| Level of reimbursement provided | 0% | 25% | 50% | 75% | 100% |
|---|---|---|---|---|---|
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are not supported |
49% | 62% | 74% | 79% | 84% |
| - Schemes open to all employees are not supported - Schemes for employees with known health conditions are supported |
46% | 59% | 71% | 77% | 82% |
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are supported |
65% | 76% | 85% | 88% | 91% |
Base (weighted): All SMEs employing 10 or more staff
4.7.2. Differences in uptake by company size
Smaller SMEs in the sample were more likely to choose “continue as now” and less likely to choose to use government support. According to Business Population Estimates (see appendix) at the time of the survey approximately 55% of SMEs fell into the 10 to 19 employee grouping. Table 4.6 and Table 4.7 take the scenario in Table 4.3 and segment the results by whether the SME had 10 to 19 employees or 20 to 250 employees.
Table 4.6 Forecasts of uptake under different levels of reimbursement, assuming online resources available, for SMEs with 10 to 19 employees
| Level of reimbursement provided | 0% | 25% | 50% | 75% | 100% |
|---|---|---|---|---|---|
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are not supported |
34% | 48% | 61% | 67% | 74% |
| - Schemes open to all employees are not supported - Schemes for employees with known health conditions are supported |
32% | 45% | 59% | 65% | 72% |
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are supported |
45% | 58% | 70% | 76% | 81% |
Base (weighted): All SMEs employing 10 or more staff
Table 4.7 Forecasts of uptake under different levels of reimbursement, assuming online resources available, for SMEs with 20 to 250 employees
| Level of reimbursement provided | 0% | 25% | 50% | 75% | 100% |
|---|---|---|---|---|---|
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are not supported |
52% | 65% | 77% | 82% | 86% |
| - Schemes for employees with known health conditions are not supported - Schemes for employees with known health conditions are supported |
49% | 63% | 75% | 80% | 85% |
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are supported |
64% | 76% | 85% | 88% | 91% |
Base (weighted): All SMEs employing 10 or more staff
This suggests that SMEs with 10 to 19 employees are harder to reach. Therefore, to improve uptake amongst this group, consideration must be taken to how the smaller SMEs might be specifically targeted to improve their awareness of the impacts health and wellbeing schemes can have for their business.
4.7.3. Differences in uptake by whether currently provide support to staff
One area of particular interest is how the likely uptake differs between those SMEs that currently provide some forms of health and wellbeing support to their staff and those that state that they currently do not. After weighting, these reflect 64% and 36% of the population of SMEs respectively. Table 4.8 and Table 4.9 take the scenario in Table 4.3 and segments the results by these two sub-groups.
Table 4.8 Forecasts of uptake under different levels of reimbursement, assuming online resources available, for SMEs that do not currently provide any health and wellbeing support
| Level of reimbursement provided | 0% | 25% | 50% | 75% | 100% |
|---|---|---|---|---|---|
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are not supported |
32% | 45% | 58% | 65% | 71% |
| - Schemes open to all employees are not supported - Schemes for employees with known health conditions are supported |
31% | 43% | 56% | 63% | 70% |
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are supported |
43% | 56% | 68% | 74% | 79% |
Base (weighted): All SMEs employing 10 or more staff
Table 4.9 Forecasts of uptake under different levels of reimbursement, assuming online resources available, for SMEs that currently provide some health and wellbeing support
| Level of reimbursement provided | 0% | 25% | 50% | 75% | 100% |
|---|---|---|---|---|---|
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are not supported |
48% | 61% | 73% | 79% | 84% |
| - Schemes for employees with known health conditions are not supported - Schemes for employees with known health conditions are supported |
45% | 59% | 71% | 77% | 82% |
| - Schemes open to all employees are supported - Schemes for employees with known health conditions are supported |
59% | 72% | 82% | 86% | 89% |
Base (weighted): All SMEs employing 10 or more staff
As expected from the earlier findings, it can be seen that uptake is significantly higher amongst those SMEs that currently provide health and wellbeing schemes to their staff; although the findings in section 3.4 suggest that this is intended to increase or broaden provision rather than using provided funding to cover existing activities.
However, it is encouraging to see the levels of uptake that might be achieved for those SMEs that do not currently provide support to their staff in this area. This reinforces the idea that there is a sizeable proportion of SMEs that could be influenced to take action through the provision of funding and/or advice signposting to appropriate schemes. These findings would suggest a large proportion of the benefit of any scheme would come from awareness raising of the forms of support available and clarity on how to access them. The financial incentives through reimbursement would then further increase uptake, but significant gains might be achieved through just bringing the issue to the attention of SMEs and helping them better navigate what is a complex space.
5. Conclusions
5.1. This research suggests there could be a role to play for government intervention
This research found that small and medium-sized enterprises (SMEs) generally appreciate the importance of staff health and wellbeing. However, there is currently mixed provision of health and wellbeing support amongst SMEs, and relatively few provide it in a structured way. A lot of current support appears to be reactive in nature and frequently only comes about in response to staff requests and needs.
Cost appears to be a one key barrier to adoption, and the experiment found that financial reimbursement of health and wellbeing scheme costs could increase uptake amongst SMEs.
Whilst cost appeared to be a key barrier, the research found SMEs tended to have relatively limited knowledge of actual costs, as well as little knowledge of what health and wellbeing schemes exist or where to purchase them. The experiment found that uptake of health and wellbeing schemes could be increased amongst SMEs with the provision of advice, in the form of a needs assessment to help them better understand staff health needs and advice on how to source or implement best-practice schemes to address those needs. There is also an opportunity to increase provision by bringing information on the possible benefits of health and wellbeing schemes to the attention of SME employers.
The risk of “deadweight loss” from SMEs using any financial support to simply subsidise actions that they are currently taking appears low. Both the survey and interviews identified that employers had a desire to do more and intended to use any funding provided to either extend their current provision or move into new areas.
The results suggest that there is an opportunity to influence levels of provision. However, in order to fully optimise the design of any policy it will be necessary to balance the benefits, as measured through levels of uptake of different policy configurations, against the cost of delivering those.
It may be that there are some profiles that the forecasts here suggest could lead to high levels of uptake, but in practice the cost of providing them would be disproportionate to the returns. However, by the same token there may be adjustments that these forecasts suggest could lead to relatively small differences in uptake but nonetheless are worth considering if the marginal cost of achieving them is also small.
5.2. Further research to inform future policy design
It is clear from this research that there is interest within many SME employers to provide greater health and wellbeing support for their staff. However, the barriers to this were lack of expertise to identify initiatives, lack of time to implement, and lack of capital to invest in them.
The experiment, supported by qualitative evidence, suggests that the provision of financial support and supplementary advice could be important enablers for increasing uptake. However, further research would be valuable to understand the steps that might be taken to increase employer awareness of the art of the possible, and improve their understanding of how to navigate this space better.
6. Appendix
6.1. Design of the discrete choice experiment
6.1.1. What is a Discrete Choice Experiment?
Research on the influence of factors on influencing choices is often approached from the perspective of qualitative surveys which might identify a long list of factors that influence decisions to follow a given course of action. These factors often take the form of a “laundry list” format – for example, ranking the importance of funding, information, other requirements etc. – a format that does not readily support policy makers, as it is hard to conclude how to then prioritise these factors in considering how to structure a policy intervention. Just knowing that “funding”, as an abstract concept, is stated to be important (or even most important) is not that helpful. It is more useful to consider different levels of funding that might be provided. Doing so both anchors the concept in a meaningful way, and allows clearer insights to be gained into the relative importance ascribed to smaller and larger changes, and how these may compare with the importance placed on changes in other factors.
Discrete Choice Experiments (DCE)[footnote 18], [footnote 19] are a quantitative research method for valuing different factors that influence the choices that individuals or organisations may make. DCEs enable choice alternatives to be broken down into a range of component parts, which are taken into account through the inclusion of a range of different attributes.
This research method has emerged as a very attractive method for researchers and policy makers alike, because it provides quantitative information on the relative importance of various characteristics as well as the trade-offs between these factors and the probability of uptake of different combinations of these.
This method goes beyond the traditional qualitative assessments and provides quantifiable data that can better guide the selection of the most appropriate strategies for optimising policy design. It also goes beyond the traditional ranking and rating exercises that do not provide information on strength of preference, trade-offs, or probability of uptake.
6.1.2. Attributes were selected to help address some of the key research questions
The set of the attributes included in the choice experiment were developed through a design workshop with the joint Work and Health Unit and other stakeholders. The design workshop assisted in bringing all parties together and identified the common grounds to meet the competing and complementary needs and expectations of different stakeholders.
These attributes and levels were then tested and refined through an initial set of qualitative interviews with small and medium-sized enterprises (SMEs) and then further tested through a more formal pilot survey. The following sections set out attributes selected for inclusion within the choice experiments.
Financial incentives
There are many ways that an incentive may technically be structured with fixed and variable elements, along with possible caps. Initially the intent was to test a range of financial incentive structures through this experiment by varying the packages tested both within and between groups of employers. However, the view was reached that from the perspective of any individual employer the details underpinning the payment structure was likely to be less important, and what they would ultimately be interested in is the amount that they may receive for participation (irrespective of how that was reached).
An alternative considered was presenting an incentive structure that was based on varying levels of contribution per employee and then presenting the survey respondent with the total contribution that they would be given for setting up the scheme for their workforce. However, there were concerns that this might make the choices more complicated and as the design process progressed the decision was taken to not discuss the absolute value of contribution received, but rather to frame this in terms of the proportion of spend that would be reimbursed, with the intention to collect supplementary information on the impacts that the absolute level of funding may have through the follow-up interviews.
A broad range of incentive attribute levels were tested, from zero reimbursement through to 100% reimbursement. This allowed us to test the sensitivity of employers to different levels of reimbursement and examine the impact that different levels could have on the uptake of different types of scheme. It also allowed us to investigate scenarios where advice was provided but without any financial support.
To test whether capital constraints could be an issue for SMEs the impact of varying the timing of the payment of any incentive was considered. Two levels were included: all reimbursement paid at the end and another level where a small percentage is paid up front (30%).
Types of intervention within scope of support
There are a range of types of interventions that could be supported in this space, ranging from preventative actions to actively promote good health or prevent ill-health through to targeted support for people with existing conditions to help them get better or to manage their condition more effectively. The choices were therefore constructed to vary whether each of these two types of intervention were within scope of being supported. In all choices at least one was included, but in some both were.
This allowed us to explore the extent that the uptake is contingent on both the incentive offered and the programme that it would contribute towards.
These attributes were presented in the choice experiment as a set of separate binary (supported/not supported) attributes for each package component.
Other non-financial support
A working assumption was that the level of support available to SMEs to navigate this space and the assistance in identifying the wellbeing interventions that they could put in place could have an important role to play in incentivising uptake of schemes. This was therefore included as an attribute within the experiment to test the extent to which this influences choices and uptake, and to understand how this may be traded off against other aspects such as the level of incentive on offer. Three levels of support were tested: no support, online resources being available, or a personal advisor being available. These were framed as resources to provide advice on needs assessment and/or advice on interventions to address identified needs.
Administrative burden of participation
Respondents were informed that the minimum amount of information that they would need to provide in all cases was proof of purchase. In addition to this, two attributes were included to explore how the administrative burden entailed in participating in the programme might impact on uptake. The first was whether a funding request was required before purchasing schemes, and the second was whether it was necessary to provide back information on outcomes.
This would allow us to understand whether these acted as a barrier to participation, and how significant that barrier was when compared to other factors.
The final specification of the attributes and their levels are detailed in Table 6.1.
Table 6.1 Selected attributes and levels for the choice experiment
| Attribute | Levels |
|---|---|
| Aware - 0 - 1 |
Schemes open to all employees, i.e. training and general support schemes - Not supported - Supported |
| Target - 0 - 1 |
Schemes for employees with known health conditions, i.e. expert-led support and condition management - Not supported - Supported |
| Support - 0 - 1 - 2 |
Needs assessment and advice on interventions - No support - Online resources available - Personal advisor available |
| Incentive - 0 - 1 - 2 - 3 - 4 |
Financial support (% of cost is reimbursed) - No financial support - 25% of cost is reimbursed - 50% of cost is reimbursed - 75% of cost is reimbursed - 100% of cost is reimbursed |
| Payment - 0 - 1 |
When a payment made - All paid at the end 30% paid up front - 70% paid at the end |
| Request - 0 - 1 |
Administrative requirements: you make a funding request beforehand - Required - Not required |
| Feedback - 0 - 1 |
Administrative requirements: you provide data on impacts of scheme - Required - Not required |
The choice also included a continue as now option
Choice scenarios were developed presenting two packages of possible health and wellbeing schemes on offer using combinations of attribute levels specified through the experiment design. However, it was also anticipated that there may be some scenarios that were not attractive to SMEs or some subgroups of employers that are reluctant to engage, independent of the structure of the package on offer. As a result, a “continue as now” alternative was included in each choice scenario, to allow employers to indicate that neither of the offered schemes were of interest. An example of a choice scenario is shown in Figure 6.1.
Figure 6.1 Example of the choice scenario
6.1.3 Experimental design
Experimental designs were developed to determine the combinations of attribute levels for each option presented to survey respondents. The choice experiment design was specified to ensure that the choices presented to the respondents were realistic whilst having the necessary statistical properties to support the subsequent model analysis. The experimental design was developed using Ngene 1.1.2.[footnote 20]
A d-efficient design algorithm was used, with zero priors on the coefficients. Within the main effects design, constraints were imposed to ensure realism and avoid combinations that would seem counter-intuitive. These constraints avoided combinations where:
- the package did not provide support without either of the two types of scheme
- the package did not provide cases where there was no advice and no financial support
- both packages provided no financial support
- the payment structure (timing attribute) was shown were no financial support was offered,
- a funding request was required but no financial support was provided
- the package for Option A dominated that for Option B or vice versa (i.e. was better in all respects).
A design was generated with 90 rows that were blocked into 15 blocks of 6 rows each. The blocking algorithm within Ngene was utilised, using a search which minimised the total correlation values between the blocking column and all of the attributes. In practice this ensured that no single respondent saw similar combinations of attribute levels across the different choices offered to them. This provided a design where each respondent could be asked 6 choice scenarios, with 15 different versions of these used across the sample.
6.1.4. Additional information collected through the questionnaire
Within the wider survey questionnaire questions were included to collect information to both contextualise the existing situation with regard to SME provision of health and wellbeing support, along with information on SME’s characteristics that could prove to be important explanatory variables. Table 6.2 summarises the information collected through the wider survey questionnaire.
Table 6.2 Background information included in the main survey questionnaire
| SME’s characteristics | Current health and wellbeing schemes provision |
|---|---|
| Country and company size | Current health and wellbeing schemes provided to employees |
| Industry group (sectors), and company type (public/private) | Current health and wellbeing schemes provided to the targeted employees |
| Composition of the employees | The current top health and wellbeing concerns |
| Employees main working location (working in office or not) | Barriers for implementing health and well-being schemes |
| Respondents’ role in business | |
| Who made decisions in the company | |
| Whether employees have disabilities or long term conditions | |
| Current benefits provided to employees |
After the choice experiment a question was included to ask respondents the likelihood of the uptake of health and wellbeing schemes, with an incentive scheme of either £100 or £200 per employee which was randomly assigned across the sample. This question was initially designed to help inform the design of a West Midlands health and wellbeing scheme trial. This question was conceptually different from the earlier stated choice experiment. The choice experiment was designed to understand SMEs’ preference response to different levels of reimbursement for different schemes, whereas this latter question was designed to provide some insight into the willingness to commit to rolling out of programme under two different levels of funding (in absolute terms rather than proportion reimbursed).
The survey further asked respondents some attitudinal questions regarding the barriers that the SMEs have experienced in supporting health and wellbeing schemes.
The full questionnaire is provided in section 6.2.
6.2. Piloting the survey
The questionnaire was then tested and refined through a pilot survey with a small group of SMEs in September 2018. The pilot survey was undertaken by Accent and responses were collected from 45 SMEs across Great Britain.
Through the pilot survey the team concluded that the survey design and questionnaire generally worked as intended, but the survey needed to be shortened.
As a result of the pilot survey, a few changes were made to the main survey:
- Reduced the length of the survey by removing some questions to bring the survey down to the intended 15 minute duration
- Removed some visual symbols (√ or ×) from the attributes in the choice experiment to avoid any potential confusion or misleading of respondents
- Changed the wording for the ‘when payment made’ levels from “on delivery” to “at the end”
- Decided to send the choice experiments to the respondents in advance of the interviews along with any other show material to help them familiarise themselves with the choices and reduce the survey duration
The finalised questionnaire used in the main survey is included in section 6.2.
6.2. Survey questionnaire
The survey questionnaire is available at Incentivising SME uptake of health and wellbeing support schemes - GOV.UK
6.3. Development of the discrete choice models
In this section, some additional information is provided for the more technical reader to explain the discrete choice model theories and analysis.
6.3.1. Theory underpinning the discrete choice models
The basic tenet of discrete choice modelling is utility maximisation, that is, given a set of alternatives, each individual chooses the alternative which brings them the most utility. It is assumed that utility is derived from the underlying characteristics or attributes[footnote 21] and typically on the Random Utility Model developed by McFadden (1973)[footnote 22] and by Manski (1977) [footnote 23], under which utility has a systematic and a random component. The random component may result from unobserved or unobservable attributes, unobserved taste variations, measurement errors or specification errors[footnote 24] .
The model estimation can therefore be conducted within the framework of random utility theory, thus accounting for the fact that the analyst has only imperfect insight into the utility functions of the respondents. Mathematically, the utility function for an alternative, i (iota), being chosen (from of a set of J alternatives) is decomposed into the systematic component, labelled Vi, and a random component εi:
The observable part of the utility function (Vi) for each alternative contains the characteristics of the alternatives (the attributes and levels from the choice experiment) and the individual, and can be written as:
where βik are coefficients multiplying attributes in the choice experiment and background variables, i.e. Xik. The attributes included in the experiment are detailed in Table 6.1. The values of these vary across alternatives (k - kappa) and individuals (i - iota). The probability of choosing alternative i (iota) can be written as:
The model includes a nested tree structure which allows us to represent different substitution patterns between alternatives such that:
- for any two alternatives that are in the same nest, the ratio of the probabilities is independent of the attributes or existence of all other alternatives; and
- for any two alternatives in different nests, the ratio of the probabilities can depend on the attributes of the other alternatives in the two nests.
This structure allows us to recognise that the two health and wellbeing packages on offer (Options A and B) may be more similar as alternatives to each other than these two packages and the “continue as now” option, as shown in Figure 6.2. This would allow for the representation of the substitution patterns discussed above.
Figure 6.2 Nested model structure
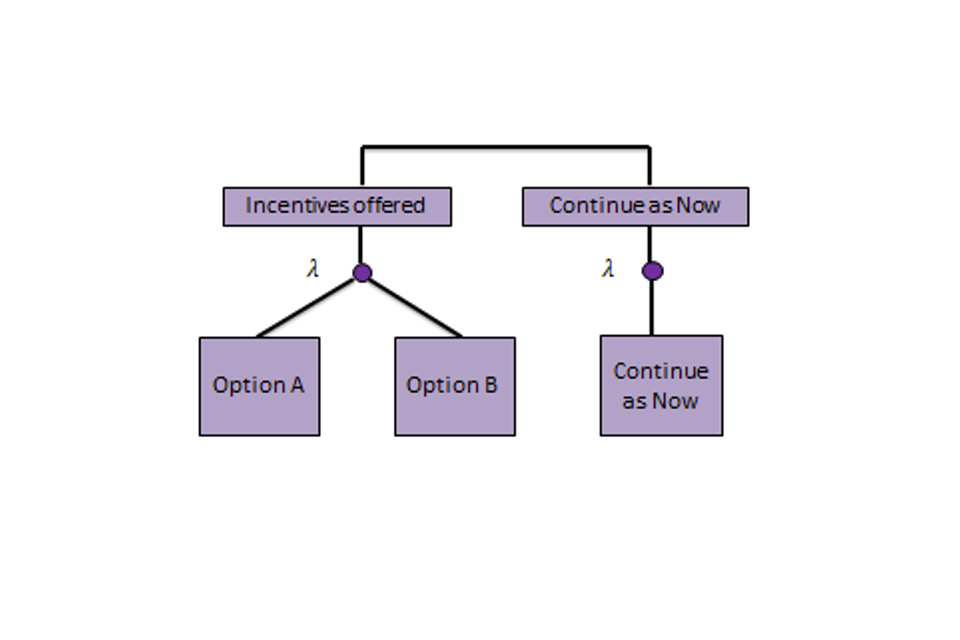
In order for this model to be consistent with utility maximising behaviour for all possible values of the explanatory variables, the structural parameter l (lambda) for the nest must take a value between zero and one. l (lambda) represents the degree of independence in unobserved utility among the alternatives in the nest. If l (lambda) takes a value of 1 there is complete independence within a nest, and the model collapses to the multinomial logit model. As it approaches 0 the degree of independence within a nest reduces, leading to increasing substitution within each nest.
This nested model can be decomposed into two logits:
where:
represents the conditional probability of choosing alt i (iota) given that an alternative in nest Bk is chosen
and:
is the marginal probability of choosing an alternative in nest Bk
with:
the “logsum” term, which brings information from the lower model to the upper model
From this it is possible to form the likelihood function that allows the estimation of the coefficients with the utilities (the b’s - betas) and the structural parameter (the l - lambda).
Table 6.3 describes the interpretation of the resulting model fit statistics and model coefficients.
Table 6.3 Interpretation of the model fit statistics and coefficient estimates
Model fit statistics:
| Observations | The number of choice observations included in the model estimation (reflecting the number of respondents and number of choice scenarios). |
| Final log (L) | This indicates the value of the log-likelihood at convergence. The log-likelihood is defined as the sum of the log of the probabilities of the chosen alternatives, and is the function that is maximised in model estimation. The value of log-likelihood for a single model has no obvious meaning; however, comparing the log-likelihood of two (nested) models estimated on the same data allows the statistical significance of new model coefficients to be assessed properly through the Likelihood Ratio test. |
| DOF | Degrees of freedom, i.e. the number of coefficients estimated in this model. Note that if a coefficient is fixed to zero then it is not a degree of freedom. |
| Rho2(c) | Comparing the log-likelihood (LL(final)) value with the log-likelihood of a model with only constants (LL(c)) gives: Rho2(c) = 1 – LL(final)/LL(c) A higher value indicates a better-fitting model. |
Interpreting the coefficient estimates:
| Sign | The sign of the coefficient indicates the preference for that attribute. A positive sign indicates that the attribute has a positive impact on respondents’ choices, and therefore the attribute is preferred by respondents and vice versa. In the case of attributes with different levels that have been coded as categorical variables in the choice models it indicates the preference for an attribute level relative to its base level. The base level is a fixed attribute level relative to which the effects of other attribute levels are measured. A positive sign indicates that the attribute level is preferred relative to the base level by respondents and vice versa. |
| Magnitude | The magnitude of the coefficient indicates the degree of preference. The larger the coefficient the stronger the preference for the attribute. |
| Base level | In the case of categorical variables it is necessary to fix a coefficient related to one of the levels to zero in order to estimate the model. The coefficients estimated for all other levels in that variable are then estimated with reference to the base level. |
| t-ratio | This indicates the significance of the coefficient. A ‘t-ratio’ numerically greater than (+/-) 1.96 indicates that the corresponding coefficient is significant at a 95% level and in practice is a commonly accepted level at which the effect implied by the coefficient is called significant. A 95% significance level indicates that the corresponding effect identified has only a 5% chance of being purely random. |
6.3.2. Testing for differences between the subgroups of the SMEs
The utility functions were then developed, testing for and taking into account any differences in preferences that could be observed between groups of SMEs. The current model at each stage was used to forecast the predicted choices of the respondents in the sample, and these were compared with the observed choices across a wide range of background characteristics to identify whether certain subgroups appeared to be responding in ways that the model was not capturing. Additional covariates were introduced to the model to address the potential under-specification, and the statistical significance of these (through individual coefficient t-ratios) and their impact on the model fit (through likelihood ratio tests) was examined and used to inform whether the additional terms provided a better fit to the data.
In developing the models these characteristics could be found to interact with the observed decision making in two possible ways. There may be some subgroups of employers that have differing sensitivity to different attributes within the package on offer (e.g. greater sensitivity to the reimbursement rate, differing engagement dependent upon the administrative requirements placed on them, etc). These would be picked up through covariates on the attributes in the models.
There may be some subgroups of employers that are just more reluctant to engage, independent of the structure of the package on offer. These would be picked up through the use of dummy terms in the utility function of the ‘continue as now’ alternative, which would allow differing levels of inertia by employee types.
The background characteristics that were systematically examined included:
-
SME’s characteristics
- Country
- Company size
- Respondents’ role in business
- Industry group (sectors)
- Company type (public/private)
- Composition of the employees (proportions of managers, technicians and low or unskilled occupations)
- Employees’ main working location (working in office or not)
- Whether employees have disabilities or long term conditions
- Current benefits provided to employees
- Decision makers in the company
- Current health and wellbeing schemes provision
- Aspects of preventative schemes provided to all employees
- Aspects of provision to disabled people or people with long-term conditions
- The current top health and wellbeing concerns
- Barriers for implementing health and well-being schemes
This comprehensive set of tests undertaken over 105 model runs have led to a final model specification that simultaneously takes into account any differences between the SMEs and reveals how preferences for different aspects of the health and wellbeing schemes influence the preferences of the packages offered.
6.3.3. Correcting for the repeated measures nature of the choice data
In discrete choice experiments there are multiple observations from the same individuals, and in the case of this study each respondent completed six choices in the survey. As such the individual observations on which the model is based are not independent and therefore the naïve model does not provide true likelihood estimates.
The bootstrap technique is applied to provide an improved estimate of the standard errors over those provided by the naïve estimation that assumes independence between observations. The bootstrap procedure[footnote 25] is a very general resampling procedure for estimating the standard errors in cases where the theory does not provide an exact estimate of the error. This resampling technique also identifies and corrects for other aspects of model misspecification.
This procedure is used in the present study. The model results presented in this report contain standard errors and parameter t-ratios from models that have been bootstrapped.
6.3.4. Final model specification
Table 6.4 presents the final model results post the treatment of the multiple measures issue of the choice observations. Table 6.3 should be considered when interpreting the coefficient values.
Table 6.4 Final model results (post bootstrap)
Schemes open to all employees, i.e. training and general support schemes
| Attribute | Description | Estimate | t ratio |
|---|---|---|---|
| Aware | not supported (base) | 0.0000 | n/a |
| Aware | supported | 0.5245 | 5.7 |
| Aware | - with disability (additional) | 0.4066 | 3.1 |
Schemes for employees with known health conditions, i.e. expert-led support and condition management
| Attribute | Description | Estimate | t ratio |
|---|---|---|---|
| Target | not supported (base) | 0.0000 | n/a |
| Target | supported | 0.5201 | 4.8 |
| Target | - with disability (additional) | 0.3259 | 2.0 |
| Target | - over 50% of the staff are technicians or skilled trades (additional) | -0.2993 | -1.6 |
Needs assessment and advice on interventions
| Attribute | Description | Estimate | t ratio |
|---|---|---|---|
| Support | no support (base) | 0.0000 | n/a |
| Support | online resources available | 0.3353 | 3.0 |
| Support | - We wouldn’t know where to purchase high quality health and wellbeing support (additional) | 0.2541 | 1.8 |
| Support | personal advisor available | 0.3768 | 3.6 |
| Support | - with disability (additional) | 0.3580 | 2.3 |
Financial support
| Attribute | Description | Estimate | t ratio |
|---|---|---|---|
| Incentive | Percent reimbursed (linear term - lower than 50%) | 2.6020 | 12.2 |
| Incentive | Percent reimbursed (linear term - 50% and above) | 1.4072 | 8.2 |
When a payment made
| Attribute | Description | Estimate | t ratio |
|---|---|---|---|
| Payment | All paid on delivery (base) | 0.0000 | n/a |
| Payment | - 30% paid up front - 70% paid on delivery |
0.1074 | 1.5 |
Administrative requirements: you make a funding request beforehand
| Attribute | Description | Estimate | t ratio |
|---|---|---|---|
| Requirements | required | -0.1130 | -1.8 |
| Requirements | not required (base) | 0.0000 | n/a |
Administrative requirements: you provide data on impacts of scheme
| Attribute | Description | Estimate | t ratio |
|---|---|---|---|
| Feedback | required | -0.0026 | 0.0 |
| Feedback | not required (base) | 0.0000 | n/a |
Constant terms – on utility function for prefer to stay as now
| Attribute | Description | Estimate | t ratio |
|---|---|---|---|
| Continue as Now | Constant term for as Now (base) | 2.7289 | 7.9 |
| Continue as Now | - Company size 10 - 19 | 0.6765 | 2.3 |
| Continue as Now | - Industry group - manufacturing | 0.9424 | 2.9 |
| Continue as Now | - Non private sector | 0.8985 | 2.4 |
| Continue as Now | - Currently provide 3 or more benefits in the list | -0.6212 | -2.0 |
| Continue as Now | - Currently provide 3 or less health and wellbeing schemes | -0.7021 | -2.7 |
| Continue as Now | - Select low levels of physical activity, e.g. fitness, exercise | 0.7300 | 1.6 |
| Continue as Now | - Selected addiction (e.g. smoking, alcohol, drugs) | -0.6929 | -2.2 |
| Continue as Now | - HR takes decision or ad hoc decisions are made whenever the business case is strong enough | -0.8648 | -2.4 |
| Continue as Now | - We don’t have the expertise or specialist support to know what health and wellbeing support | -1.0738 | -3.9 |
Model structure parameters
| Attribute | Description | Estimate | t ratio |
|---|---|---|---|
| Theta1 | Nesting on “health and wellbeing schemes” offered (Options A and B) and “Continue as Now” | 0.6293 | 7.8 |
Summary statistics
| Attribute | Description | Estimate | t ratio |
|---|---|---|---|
| Observations | 3000 | ||
| Final Log Likelihood | -2864.6 | ||
| D.O.F | 25 | ||
| Rho²(0) | 0.131 | ||
| Rho²(c) | 0.129 |
6.3.5. Forecasting
It is important to note that the probabilistic nature of the model is carried through in the application; it would be wrong to assume that the respondent chooses the alternative with the highest probability, rather the model suggests that on some occasions they will choose one alternative and on others another, in proportion to the predicted probabilities.
Therefore if the choice model is to be used for forecasting uptake of a specified health scheme package, the total shares, or referendum-style voting intentions, are calculated using a sample enumeration approach. This entails calculating the probabilities that each of the respondents in the sample will choose the package offered. The probabilities are then summed over the sample to provide the aggregate demand for the package offered for the complete sample.
In the sampling process for a survey it is possible that some groups may be over or under-represented compared to the proportions that are expected in the population from which they have been drawn. In the forecasting process it is possible to apply weights to individuals in the sample as part of the sample enumeration in order to produce forecasts that more closely represent those that would be expected from the population.
Below Table 6.5 and Table 6.6 show the sample composition and national statistics on the number of SMEs by size and business sectors.
Table 6.5 Sample composition from this study
| Employees | Private* | Non-profit Organisations | Central or Local government | Total |
|---|---|---|---|---|
| 10-19 | 163 | 10 | 6 | 179 |
| 20-49 | 162 | 7 | 17 | 186 |
| 50-99 | 61 | 5 | 7 | 73 |
| 100-199 | 48 | 2 | 2 | 52 |
| 200-249 | 7 | 3 | 0 | 10 |
| Total | 441 | 27 | 32 | 500 |
Note: private category includes private sector, other and PPP. Categories
Base (unweighted): All respondents (500)
Table 6.6 SME statistics
| Employees | Private sector | Non-profit Organisations | Central or Local Government | |
|---|---|---|---|---|
| Total | ||||
| 10-19 | 137,420 | 9,115 | 405 | 146,940 |
| 20-49 | 72,230 | 5,095 | 1,105 | 78,430 |
| 50-99 | 22,995 | 1,950 | 1,260 | 26,205 |
| 100-199 | 9,825 | 1,155 | 1,275 | 12,255 |
| 200-249 | 2,015 | 275 | 265 | 2,555 |
| Total | 244,485 | 17,590 | 4,310 | 266,385 |
Base: All SMEs employing 10 or more staff
Source: National Statistics: Business population estimates 2018[footnote 26]
Table 6.7 Weights used in the forecast
| Employees | Private | Non-profit Organisations | Central or Local government |
|---|---|---|---|
| 10-19 | 1.582423 | 1.71087 | 0.126696 |
| 20-49 | 0.836879 | 1.366175 | 0.122004 |
| 50-99 | 0.707561 | 0.732023 | 0.337857 |
| 100-199 | 0.384195 | 1.083957 | 1.196576 |
| 200-249 | 0.540303 | 0.172057 | 0 |
Weights are calculated as shown in Table 6.7 by sites and business sector type. The team were not able to find statistics by whether or not SMEs have employees with long term conditions or disabilities, and therefore did not include this when calculating the weights. However, there is no reason to believe that the survey systematically over- or under-sampled according to this characteristic.
6.4. Follow-up interview protocol
Introduction
1. Could you briefly describe your professional background, current role, and how long you have worked in the business?
2. Could you elaborate on the nature of your business?
2.1. Do your employees need to have highly specialised skills?
Prompt: Would it be difficult to find others with a similar skillset should someone leave?
2.2. Do you train employees within your organisation?
3. When you were previously interviewed, you said that X, Y, Z were your top 3 areas of concern for staff health and wellbeing. Could you explain why this is the case? Which of these is the most important? Why?
Conditional:
Organisation employs staff with long-term health conditions and/or disabilities
You indicated that you currently employ staff with long-term health conditions and/or disabilities.
4. Has your organisation put in place health and wellbeing changes or support based on the needs of these employees? What sort of provisions?
Prompt: Changes in physical work environment, provision of equipment, changes in work organisation, external support or training
5. What sort of provisions did you have in place before these staff members arrived/staff developed a condition?
6. Has your interest in providing (or: your perception of the need to provide) health and wellbeing services changed in light of employing individuals with disabilities or long-term health conditions?
6.1. If so…how?
6.2. If not…
6.2.1. Are there things that you feel would make this particularly difficult for your organisation?
6.2.2. Is there support that could be offered that could make this easier?
Alternative 1:
Organisation implements health and wellbeing interventions
According to the survey, you already provide health and wellbeing support to employees.
7. What kind of support do you currently provide?
8. How did you identify these needs within your organisation?
Prompt: Many employers did not currently provide targeted support for at risk employees but said they would should the need arise. Is that the case for you? Why?
9. How did you locate the providers?
9.1. Who are the providers
Prompt: Small or large providers; long-term contracts or one-off contracts;
Prompt: If in-house – who provides and what is their experience?
9.2. Did you experience any obstacles or did anything greatly help you when locating and purchasing health and wellbeing services?
10. What outcomes are you hoping to achieve through the programmes?
Prompt: Financial performance improvement/increase in efficiency through reduced sickness absence/faster returns after long-term sickness absence etc., indirect benefits through retention and attracting potential employees, happiness/general welfare, probe with some employers how important that there is a net positive financial return
11. Do you think that the programs you currently have available are achieving this? How do you measure or assess this?
12. Does it matter to you whether there is strong evidence behind a certain intervention? Why?
13. Is there more that you would like to be able to do?
13.1. If so…
13.1.1. How much do you expect this to cost?
13.1.2. Are there any obstacles (other than cost) preventing you from implementing them?
13.1.3. What guidance would you like to receive to help you deliver new health and wellbeing interventions/improve your current programs?
13.1.4. What is the biggest challenge for you: Identifying staff needs, determining solutions, finding a provider, or implementing the program?
13.1.5. Would this be better provided online or in person? Why?
13.2. If not… why?
14. Do you feel more inclined to offer general wellbeing interventions to everyone in the organisation or to a more targeted audience? Why?
Prompt: If targeted: skill level of employee, length of employment, type of contract etc. (differentiates based on value of employee?)
14.1. Do you have a preference for services that are preventative (re-emphasising healthy behaviours/ addressing wellbeing without actual problems in the organisation) or reactive (addressing issues when they arise)? Why?
Alternative 2:
Organisation does NOT yet implement health and wellbeing interventions
According to the survey, you current do not provide health and wellbeing support to employees.
15. To what extent is this because you do not currently see a need for it, or because of a lack of assistance?
16. If some assistance was provided to you, would you consider implementing such programmes?
Prompt: Assistance could be either through funding or advice/guidance.
16.1. If so… (if not, go to 17)
16.1.1. Under which circumstances would it be most helpful for you? What kind of support would you consider providing?
16.1.2. How much would you expect the programmes to cost?
16.1.3. How would you go about finding the providers?
16.1.4. Do you anticipate any obstacles to setting this support up?
17. If you were to implement such a programme, what outcomes would you hope to achieve?
Prompt: Financial performance improvement/increase in efficiency through reduced sickness absence/faster returns after long-term sickness absence etc., indirect benefits through retention and attracting potential employees, happiness/general welfare, probe with some employers how important that there is a net positive financial return
18. Would you seek to measure or assess whether the programme was achieving these outcomes? If so, how?
19. Does it matter to you whether there is strong evidence behind a certain intervention? Why?
20. What guidance would you like to receive to help you deliver new health and wellbeing interventions or improve your current programs?
21. Would this be better provided online or in person? Why?
22. What is the biggest challenge for you: identifying staff needs, determining solutions, finding a provider, or implementing the program?
23. Do you feel more inclined to offer general wellbeing interventions to everyone in the organisation or to a more targeted audience? Why?
Prompt: If targeted: skill level of employee, length of employment, type of contract etc. (differentiates based on value of employee?)
24. Do you have a preference for services that are preventative (re-emphasising healthy behaviours/ addressing wellbeing without actual problems in the organisation) or reactive (addressing issues when they arise)? Why?
Advice and funding
25. Would it be more important to you to have access to some advice, or receive some funding to assist with rolling out new health and wellbeing programmes in your organisation? Why?
Costs and willingness-to-pay
26. How do the costs of health and wellbeing interventions influence your decision to consider them for your staff?
27. How much would your organisation be willing to spend on health and wellbeing programmes (given current constraints)?
28. Imagine there were a scheme through which the amount of money you invest in health and wellbeing services for your staff is matched by the government. For example, if you spent £500 on these services, the government would grant you the same amount, £500. Would this make you more likely to provide additional support to your staff?
28.1. If so…
28.1.1. What would you put this money towards? Why?
28.1.2. Would you prefer a programme offering support available to all staff or one more focused on at-risk employees?
28.1.3. How much would you invest in the programmes?
28.1.4. If you were to see benefits to your business, do you think you would continue providing this support long-term? What sort of benefits would you need to see?
28.2. If not…
28.2.1. What would encourage you to invest in these services?
28.2.2. What amount of money would you require?
28.3. How much do the total cost of the purchase, i.e. whether it is a large or small investment for the organisation overall, influence your decision to take-up a (matched-funding) scheme?
Prompt: Do investments with high total cost require higher levels of % reimbursement? (Is it just about the % reimbursement that matters?)
29. How difficult is it for your organisation to acquire the necessary upfront capital to pay for a scheme?
30. When we previously asked organisations about the importance of how the payment is structured, it was found not to be significant whether a percentage is paid up front or whether it was all paid after the services were purchased. Would this be the case for your organisation? Why?
Prompt: time between purchase and reimbursement (tax takes at least 12 months), level of upfront capital matters?
31. Any support would come with administrative requirements attached.
31.1. Assume you had to provide a funding request, how would the level of detail you would have to provide affect your level of interest in a programme?
Prompt: E.g. high level of detail in funding request;
31.2. If you had to provide data on the outcomes of the scheme, would it affect your interest?
Next steps
32. Is there anything else that RAND should be aware of or that should factor into the discussions with organisations?
33. Do you have any questions for us?
-
DWP/DHSC, Sickness absence and health in the workplace: understanding employer behaviour and practice, 2021 ↩
-
DWP/DHSC, Sickness absence and health in the workplace: understanding employer behaviour and practice, 2021 ↩
-
ONS, Sickness absence in the UK labour market: 2018, 2019. ↩
-
Tu T, Maguire K and Shanmugarasa T. ‘Sickness absence and health in the workplace: understanding employer behaviour and practice’ DWP/DHSC report number 981 July 2021. Available at: https://www.gov.uk/government/publications/sickness-absence-and-health-in-the-workplace-understanding-employer-behaviour-and-practice ↩
-
Tu T, Maguire K and Shanmugarasa T. ‘Sickness absence and health in the workplace: understanding employer behaviour and practice’ DWP/DHSC report number 981 July 2021. Available at: https://www.gov.uk/government/publications/sickness-absence-and-health-in-the-workplace-understanding-employer-behaviour-and-practice ↩
-
DWP/DHSC, 2016. Improving Lives: The Future of Work, Health, and Disability Green Paper. Available at: https://www.gov.uk/government/consultations/work-health-and-disability-improving-lives ↩
-
DWP/DHSC, 2021. Health is Everyone’s Business Consultation. Available at: https://www.gov.uk/government/consultations/health-is-everyones-business-proposals-to-reduce-ill-health-related-job-loss ↩
-
EPPI, ‘Developing evidence-informed, employer-led workplace health: Final Report’, 2016, As of 18 February 2019: https://eppi.ioe.ac.uk/CMS/Portals/0/PDF%20reviews%20and%20summaries/Employer-led%20workplace%20health%202016%20Brunton.pdf ↩
-
Tu T, Maguire K and Shanmugarasa T. ‘Sickness absence and health in the workplace: understanding employer behaviour and practice’ DWP/DHSC report number 981 July 2021. Available at: https://www.gov.uk/government/publications/sickness-absence-and-health-in-the-workplace-understanding-employer-behaviour-and-practice ↩
-
Ibid ↩
-
Ibid ↩
-
To our knowledge there are no examples in the UK of implemented schemes that sought to stimulate health and wellbeing activity. There have been a number of US states that have offered employer tax incentives to set up wellness programmes but none of them have been formally evaluated in terms of uptake. Moreover, incentives are different as a result of employer-paid medical insurance. ↩
-
No need for health and wellbeing interventions’ wasn’t listed as a barrier to supporting health and wellbeing interventions, although this would likely be captured through other barriers listed or the ‘none of these’ option. ↩
-
Bajorek, Zofia, Victoria Shreeve, Stephen Bevan, Tyna Taskila. (2014) ‘The Way Forward: Policy options for improving workforce health in the UK.’ The Work Foundation. As of 18 February 2019: http://www.theworkfoundation.com/wp-content/uploads/2016/11/372_The-Way-Forward-FINAL.pdf ↩
-
DWP/DHSC, 2021. Sickness absence and health in the workplace: understanding employer behaviour and practice. ↩
-
ONS, 2019. Sickness absence in the UK labour market: 2018. ↩
-
DWP, 2020. The employment of disabled people 2019. ↩
-
Ben-Akiva, M. and Lerman S. R. (1985) Discrete Choice Analysis: Theory and Application to Travel Demand. The MIT Press, Cambridge, Massachusetts. ↩
-
Train, E. (2003) Discrete Choice Methods with Simulation. Cambridge University Press ↩
-
ChoiceMetrics. (2018) Ngene 1.1.2 ↩
-
Lancaster, K.J. (1966) A New Approach to Consumer Theory. Journal of Political Economy, 74, 132-157. ↩
-
McFadden, D. (1973) Conditional Logit Analysis of Qualitative Choice Be. In: Zarembka, P., Ed., Frontiers in Econometrics, Academic Press, New York, 105-142. ↩
-
Manski, C. F. (1977) The structure of random utility models. Theory and Decision, 8(3), 229-254. ↩
-
Ben-Akiva, M. and Lerman S. R. (1985) Discrete Choice Analysis: Theory and Application to Travel Demand. The MIT Press, Cambridge, Massachusetts. ↩
-
Efron, B. (1979) Bootstrap methods: another look at the Jackknife. Ann. Statist. 7 1-26 ↩
-
Available at: https://www.gov.uk/government/statistics/business-population-estimates-2018 ↩