Impact on school absence from COVID-19 vaccination of healthy 12 to 15 year old children
Published 13 September 2021

© Crown copyright 2021
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/impact-on-school-absence-from-covid-19-vaccination-of-healthy-12-to-15-year-old-children/impact-on-school-absence-from-covid-19-vaccination-of-healthy-12-to-15-year-old-children
Background
On 3 September 2021, the Joint Committee on Vaccination and Immunisation (JCVI) issued advice that the health benefits from vaccination of 12 to 15 year olds are marginally greater than the potential known harms. However, it considered the margin of benefit too small to support universal vaccination of healthy 12 to 15 year olds at this time. It is not within the JCVI’s remit to consider the wider societal impacts of vaccination beyond health, hence they suggest:
the government may wish to seek further views on the wider societal and educational impacts from the chief medical officers of the UK 4 nations.
JCVI have already recommended 2 doses of vaccine for an estimated 350,000 12 to 15 year olds in England who are at risk or who live in households of immunosuppressed individuals.[footnote 1] This makes up 13% of all 12 to 15 year olds in England. The analysis here considers the remaining ‘healthy’ population, an estimated 2.24 million children in England.
This note presents a range of initial, scenario-based estimates of school absences due to COVID-19 infections in 12 to 15 year olds in England with and without vaccinating healthy 12 to 15 year olds. Reducing school absences is one of several wider impacts of vaccination. Other impacts include the knock-on impact of school absence on children’s wellbeing and the economic impact of workforce absences due to parents having to care for children. These considerations are not within the scope of this paper.
The analysis provided here is scenario-based because of the significant uncertainty in the epidemiological progression of COVID-19. Some of the modelling is highly simplified but this is proportionate given so much uncertainty in the background epidemiology. We do not think any further refinement will be of significant value while the epidemiological picture is so uncertain but it could be revisited when there is a stronger consensus on the epidemiological picture following data on the impact of schools returning from the summer break.
Epidemiological scenarios
The trajectory of the pandemic over the next 6 months remains extremely uncertain. We therefore use a number of scenarios providing a range of estimates for the number of future infections in this analysis. The most up-to-date modelling available from SPI-M that covers this period is the step 4 roadmap modelling from 7 July 2021.[footnote 2] Modelling from LSHTM, Imperial and Warwick University is available, all providing different scenarios for infections (available for all ages combined) over this period.
Looking at all these models, we have taken 3 scenarios for the main analysis:
- one each for the highest and lowest scenarios that encompass range of all other scenarios
- one scenario that closely follows the actual infections in the intervening period
These 3 scenarios are all from the Warwick University model (though they encompass the scenarios of LSHTM and Imperial) and are detailed in table 1 below.
However, the step 4 roadmap modelling do not cover the full range of potential trajectories and the modelling is currently under review by SPI-M. A significant future wave could occur in this period as a result of waning of vaccine effectiveness, as well as if there is a vaccine-escape dominant variant. To demonstrate this risk, we have therefore created an alternative scenario by shifting the highest peak in the Warwick scenarios to 2 months later, hence a peak of about 170,000 infections per day falls into the period where a vaccine would have most impact. It is important to note that there are plausible scenarios even worse than the contingency scenario presented here.
Figure 1: daily infections – Warwick scenarios and contingency scenario, all ages, England, July 2021 to March 2022
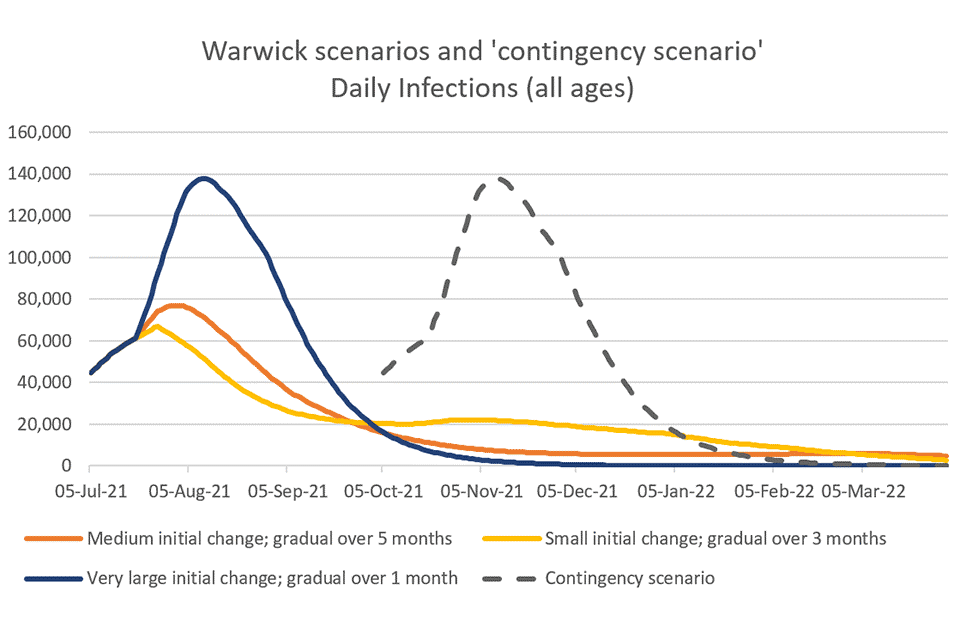
Table 1: summary of scenarios
| Corresponding Warwick step 4 roadmap modelling (SPI-M, 7 July 2021) | Total infections in all age groups (18 October 2021 to 31 March 2022) | |
|---|---|---|
| Main scenarios – no waning of immunity, no new dominant variant | Medium initial change: gradual over 5 months | 1.0 million |
| Main scenarios – no waning of immunity, no new dominant variant | Small initial change: gradual over 3 months | 2.2 million |
| Main scenarios – no waning of immunity, no new dominant variant | Very large initial change, gradual over 1 month | 150,000 |
| Contingency scenario – potentially caused by waning of vaccine effectiveness and/or a new dominant vaccine-escape variant | Very large initial change: gradual over 1 month, shifted later by 2 months | 6.9 million |
COVID-19 related school absences
The Department for Education (DfE) provides data on COVID-19 related school absences according to the following 5 categories:
-
pupils with a confirmed case of COVID-19
-
pupils with a suspected case of COVID-19
-
pupils self-isolating due to contact inside school
-
pupils self-isolating due to contact outside school
-
pupils unable to attend due to school closure related to COVID-19
Table 2 below shows COVID-19 related school absences in state secondary schools between 14 June 2021 and 17 July 2021.
Table 2: COVID-19-related school absences in state secondary schools between 14 June 2021 and 17 July 2021
| Category | Secondary school absences |
|---|---|
| Proportion of pupils with a suspected case of COVID-19 | 0.31% |
| Proportion of pupils with a confirmed case of COVID-19 | 0.50% |
| Proportion of pupils self-isolating due to contact inside school | 7.18% |
| Proportion of pupils self-isolating due to contact outside school | 1.24% |
| Proportion of pupils unable to attend due to school closure | 0.30% |
This shows the vast majority of COVID-19 related absences in that period were due to pupils self-isolating due to contact inside or outside school.
Non-pharmaceutical interventions (NPIs) in the education setting to reduce spread of COVID-19
Education NPIs have changed significantly since summer term 2021.
Education NPIs as in summer term 2021
-
A requirement for close contacts inside or outside school to self-isolate. Contacts in school were often defined as a whole year group or even wider
-
Bubbling, mask wearing, restrictions on sharing equipment, and many other changes within schools to reduce transmission between pupils and pupils to staff
-
Contingency measures to deal with any outbreaks, including closure of schools where absolutely necessary
Education NPIs as at 1 September 2021
-
No requirement to self-isolate due to contact inside or outside school for pupils or vaccinated adults
-
No bubbling, no mask wearing and reduced restrictions on sharing equipment, and so on
-
Contingency measures to deal with outbreaks, which include reintroducing mask wearing and other measures, minimising absences where at all possible, but including closure of schools where absolutely necessary
In the main scenarios presented here, we assume that the current education NPIs can continue to be in place. In the contingency scenario, we assume that the education NPIs from summer term 2021 would be reintroduced as a means to manage overall infections.
Pupils with a confirmed case of COVID-19
Table 3 shows the estimated school absences with and without vaccination of healthy 12 to 15 year olds for confirmed COVID-19 cases. These absences are for COVID-19 PCR test-confirmed cases, each of which is assumed to self-isolate for an average of 11 calendar days (we adjust for some of these falling on weekends or in school holidays). Absences relating to suspected COVID-19 that have negative PCR tests have not been estimated.
This analysis assumes the vaccine programme would provide a single dose of Pfizer/BioNTech vaccine, with an uptake rate of 60%. This is based on the uptake in school-age children of the flu vaccination programme. The actual uptake is extremely uncertain. The ONS School Infection Survey (SIS) regularly reviews parental hesitancy to COVID-19 vaccination of children. The latest round (round 6) of SIS found only 14% of parents of secondary-age school children to be hesitant, with 86% sharing that they definitely would or probably would consent for their children to be vaccinated.[footnote 3] Therefore, the 60% assumption used in this analysis may be an underestimate.
A single dose is assumed, based on the latest JCVI advice for 16 to 17 year olds on 4 August 2021. The range of estimates represent different epidemiology scenarios and a range of vaccine effectiveness against all infections from a single dose (mid-estimate 55%, range: 40% to 70%).[footnote 4] With 60% uptake, this means we estimate that, at 60% uptake, vaccinating healthy 12 to 15 year olds will reduce confirmed case of COVID-19 by 33% (range: 24% to 42%) in this group.
We assume the programme will be rolled out in September so vaccine effectiveness will be achieved from 18 October 2021 onwards.
Table 3: results for 12 to 15 year olds between 18 October 2021 and 31 March 2022
| No vaccine scenario | With vaccine scenario | Difference | |
|---|---|---|---|
| Total infections in 12 to 15 years | 89,000 (13,000 to 190,000) | 59,000 (10,000 to 110,000) | 30,000 (3,000 to 80,000) |
| Total school days absent – confirmed case of COVID-19 | 320,000 (50,000 to 700,000) | 220,000 (40,000 to 400,000) | 110,000[footnote 5] (10,000 to 290,000) |
| …per 1,000 students (total over period) | 125 (18 to 269) | 84 (14 to 156) | 41 (4 to 113) |
| Average % students absent at any one time – PCR-confirmed cases | 0.13% (0.02% to 0.27%) | 0.09% (0.01% to 0.14%) | 0.04% (0.004% to 0.11%) |
The analysis suggests, for the epidemiological scenarios considered, in the period up to 31 March 2022, vaccinating healthy 12 to 15 year olds will prevent 30,000 (3,000 to 80,000) infections in 12 to 15 year olds, or 110,000 (10,000 to 290,000) school days absent in this age group due to confirmed COVID-19 cases. In terms of average daily absence, this is equivalent to a decrease from 0.13% (0.02% to 0.27%) without vaccination to 0.09% (0.01% to 0.14%) with vaccination.
In the ‘contingency scenario’, which has 7 times the number of infections as the central scenario in the main analysis, 12 to 15 year olds will have 2.2 million school days absent that are confirmed COVID-19 cases without vaccination over this period. Vaccination would prevent 720,000 of these absences in the time period in question.
Pupils with a suspected case of COVID-19
This category of absence is for pupils that have a COVID-19 symptom. They are required to self-isolate while awaiting a PCR test result. DfE statistics include both pupils who go on to have a positive or a negative test result in this category. In this report, we include the absences before a positive test result is received within our estimates for category ‘pupils with a confirmed case of COVID-19’. Of the remaining absences, for those who go on to have a negative COVID-19 PCR test result, it is unclear how they would be impacted by a COVID-19 vaccine.
The main driver for these absences will be the rates of other viruses which will increase as we move into colder months. With a vaccine, there may be behavioural change in the vaccinated population who may be less likely to respond to COVID-19 like symptoms with self-isolation. However, this is very hard to predict as it would be going against government advice (which is to self-isolate with COVID-19 symptoms regardless of vaccine status). The challenges of modelling these complex factors mean we have not been able to estimate future rates of these absences, with or without vaccination, in this paper.
Pupils self-isolating due to contact inside school
In the 3 main scenarios, we assume that the current education NPIs remain in place, and hence there will only be absences due to contact inside school as a last resort to manage an outbreak. We do not have a reasonable way to estimate these absences, but therefore assume them to be close to zero.
In the contingency scenario we assume that self-isolation of close contacts in schools will return, and we base our analysis on the historic ratio of these absences to PCR-confirmed cases. Even if this does not return as an official policy, given the level of infections is so high in this scenario, it is likely to result in a large number of outbreaks which would in turn result in such measures likely to be taken at a local level.
In the contingency scenario, we estimate an additional 18 million (15 million to 20 million) school days absent due to contact inside school. See the technical annex (below) for methodology.
Pupils self-isolating due to contact outside school
Current government policy does not require children to self-isolate if they are a close contact outside of school. In the 3 main scenarios, overall infection levels are low and so it is reasonable to assume that this policy continues. We would assume these absences would therefore be close to zero.
In the contingency scenario we assume that self-isolation of close contacts will return, and we base our analysis on the historic ratio of these absences to PCR-confirmed cases. Based on this we estimate an additional 3.1 million (2.7 million to 3.5 million) school days absent due to contact outside school. See the technical annex (below) for methodology.
Pupils unable to attend due to school closure related to COVID-19
Over 2020 and 2021 there were several periods where the government required all schools to close apart from to children of key workers and vulnerable children. Outside of these periods, the national policy has been to keep schools open wherever possible, and school closure is very much a last resort measure for schools.
Despite best efforts, some schools did have to close in the summer term, and 0.06% of children were absent because of a school closure in the last 6 weeks of summer term 2021. Though no data is available on the precise reasons, anecdotally we know on many occasions this was because of lack of staff as so many staff members were instructed to self-isolate.
In our 3 main scenarios we assume there will be very small numbers of school closures, given overall infections are expected to be low, and assume this to be zero. In the contingency scenario we assume that there are school closures and estimate the absences due to school closures and base our analysis on the historic ratio of these absences to PCR-confirmed cases. Based on this we estimate an additional 2 million school days absent due to contact inside school, reducing to 1.3 million days absent with vaccination (hence averting 650,000 days absent). See the technical annex (below) for methodology.
Summary of results
Table 4: scenario results for COVID-19 related absences for 12 to 15 year olds between 18 October 2021 and 31 March 2022 (total absences)
| Main scenario: no vaccine | Main scenario: with vaccine | Main scenario: difference | Contingency scenario: no vaccine | Contingency scenario: with vaccine | Contingency scenario: difference | |
|---|---|---|---|---|---|---|
| Pupils with a confirmed case of COVID-19 | 320,000 (50,000 to 700,000) | 220,000 (40,000 to 400,000) | 110,000 (10,000 to 290,000) | 2.2 million | 1.3 million (1.1 million to 1.6 million) | 0.8 million[footnote 6] |
| Pupils with a suspected case of COVID-19 | Not estimated | Not estimated | Not estimated | Not estimated | Not estimated | Not estimated |
| Pupils self-isolating due to contact inside school | Not estimated – assumed to be zero | Not estimated – assumed to be zero | Not estimated – assumed to be zero | 27 million | 18 million (15 million to 20 million) | 9 million (6 million to 11 million) |
| Pupils self-isolating due to contact outside school | Not estimated – assumed to be zero | Not estimated – assumed to be zero | Not estimated – assumed to be zero | 4.6 million | 3.1 million (2.7 million to 3.5 million) | 1.5 million (1.1 million to 1.9 million) |
| Pupils unable to attend due to school closure related to COVID-19 | Not estimated – assumed to be zero | Not estimated – assumed to be zero | Not estimated – assumed to be zero | 2.0 million | 1.3 million (1.1 million to 1.5 million) | 0.7 million (0.5 million to 0.8 million) |
Discussion
The impact of vaccination on school absences in the main scenarios is estimated to reduce school absences from 320,000 (50,000 to 700,000) to 220,000 (40,000 to 400,000), a decrease of 110,000 (range: 10,000 to 290,000) school days between 18 October 2021 and 31 March 2022.
In contrast, in the ‘contingency scenario’ modelled, the impact of vaccinating this cohort could be very significant. The estimates provided here are that, for all COVID-19 related absences combined, with vaccination in the contingency scenario the number of school days absent would reduce from 36 million to 24 million (20 million to 27 million) – a difference of 12 million (9 million to 16 million).
Caveats
This analysis is based on epidemiology scenarios for which there is significant uncertainty. Even including the contingency scenario, the 4 scenarios do not necessarily capture the full range of uncertainty in the epidemiology of COVID-19 in the coming months.
In addition, the modelling has not accounted for how infection rates in school-age children (as a proportion to the rest of the population) could be different going forward. The modelling for this group is based on schools staying open but children’s close contact patterns changing in line with the rest of the population. This potentially underestimates the impact of returning to school with fewer school NPIs than were in place earlier in the year.
In addition, the modelling itself has a number of simplifications which makes the estimates further uncertain. One key limitation in the analysis is that it does not factor in the reduction in onward transmission within this age group due to vaccination. In this sense it is an underestimate of the expected impact.
There may also be some educational costs of vaccination: a small amount of school time is likely to be lost as a result of children attending vaccination sessions and some may have side effects of the vaccine that may lead to school absences which are not factored in here.
DfE data on pupil absence in the autumn term 2020 showed that pupils eligible for free school meals missed 30% more school days than other pupils. This suggests that children from disadvantaged areas may have more to gain from vaccination. However, if vaccination rates among this group are lower among the most deprived areas, as they have been for adults overall, then vaccination could increase disparities in health between high and low socio-economic group. Hence, the overall direction of impact is hard to predict.
Technical annex
Background
Vaccinating children has impacts on them wider than health impacts alone. The pandemic has caused significant disruption to education. Infection, self-isolation and lockdowns have resulted in children across England missing days of school throughout the pandemic. Statistics from DfE show that COVID-related pupil absences in schools reached a peak rate in July since schools reopened in March 2021. 14.3% of school pupils were absent from school due to COVID-related absence on 15 July 2021. In secondary schools specifically (ages 11 to 16), the proportion was 17.9% on the same date. Note the majority of these absences were due to pupils self-isolating after being traced as a close contact. The policy of self-isolation for close contacts has since been removed for all children.[footnote 7]
This note provides estimates of the number of days of school absence that may be avoided in the 12 to 15 year old age group due to vaccination of this age group. This analysis considers universal vaccination of 12 to 15 year old children. It is currently based on just one dose of the Pfizer/BioNTech vaccine, in order to match the JCVI dosing advice given for the 16 to 17 year old age group published on 4 August 2021.[footnote 8] Note that JCVI has recently advised that at-risk 12 to 15 year olds should be offered 2 doses of a vaccine, hence we consider the remaining 12 to 15 year olds in this analysis.
The trajectory of the pandemic over the next 6 months remains extremely uncertain. We therefore use a number of scenarios providing a range of estimates for the number of future infections in this analysis. The most up-to-date modelling that covers this period is the step 4 roadmap modelling from 7 July 2021. Modelling from LSHTM, Imperial and Warwick University is available, all providing different scenarios for infections (available for all ages combined) over this period. Looking at all these models, we have taken 3 scenarios:
- one each for the highest and lowest scenarios
- one scenario that most closely follows the actual infections in the intervening period
These 3 scenarios are all from the Warwick University model:
Medium initial change; gradual over 5 months
This scenario models a medium drop in precautionary behaviour from 19 July 2021 followed by a gradual reduction to pre-pandemic levels over 5 months. This most closely matches the data available on actual infections to date.
Small initial change; gradual over 3 months
This scenario models a small drop in precautionary behaviour from 19 July 2021 followed by a gradual reduction to pre-pandemic levels over 3 months. This provides a maximum scenario for the period in question.
Very large initial change; gradual over 1 month
This scenario models a large drop in precautionary behaviour from 19 July 2021 followed by a gradual reduction to pre-pandemic levels over 1 month. This provides a minimum scenario for the period in question.
However, the step 4 roadmap modelling do not cover the full range of potential trajectories and the modelling is currently under review by SPI-M. A significant future wave could occur in this period as a result of waning of vaccine effectiveness, as well as if there is a vaccine-escape dominant variant.
To demonstrate this risk, we have therefore created an alternative scenario by shifting the Warwick scenarios’ ‘very large initial change – gradual over 1 month’ to 2 months later, hence the peak of about 170,000 infections per day falls into the period where a vaccine would have most impact.
It is important to note that it is plausible infections could be even worse than the contingency scenario presented here.
Adjusting scenarios for 12 to 15 year olds
These models are at the level of the whole population, so it has been necessary to adjust for expected infections in 12 to 15 year olds. We use separate modelling from Warwick University that modelled vaccination of children 12 to 17 years and estimate from this the share of all infections that would fall into the 12 to 15 years age group, which we keep constant over the duration of the no vaccine scenarios.
Note that the Warwick modelling does not account for the changes in children’s infections that might occur as a result of the changing policies such as school NPIs, isolation of contacts, and so on. Instead it takes a simple approach of assuming schools stay open and non-household contacts for all age groups change in line with each other. Therefore, there is a possibility that the relaxation of school NPIs result in proportionately more infections in this group than the rest of the population. In this regard this modelling may be an underestimate of infections in this age group.
We provide estimates for the number of infections and days of school absence averted between 18 October 2021 and 31 March 2022.
Due to uncertainty in the parameter, we also use a range of different vaccine efficacies against infection: 40%, 55% and 70%. The one-dose Pfizer/BioNTech efficacy is based on studies exploring efficacy against the dominant B.1.617.2 Delta variant undertaken in the UK[footnote 9] and Qatar.[footnote 10]
Note: vaccination will cause a decrease not only in an individual’s ability to become infected, but it also causes a decrease in an infected individual’s ability to transmit the disease further. This analysis does not consider effects of the vaccine on further transmission, and so the benefits quantified in terms of decrease in averted days of school absence may be an underestimate in this way.
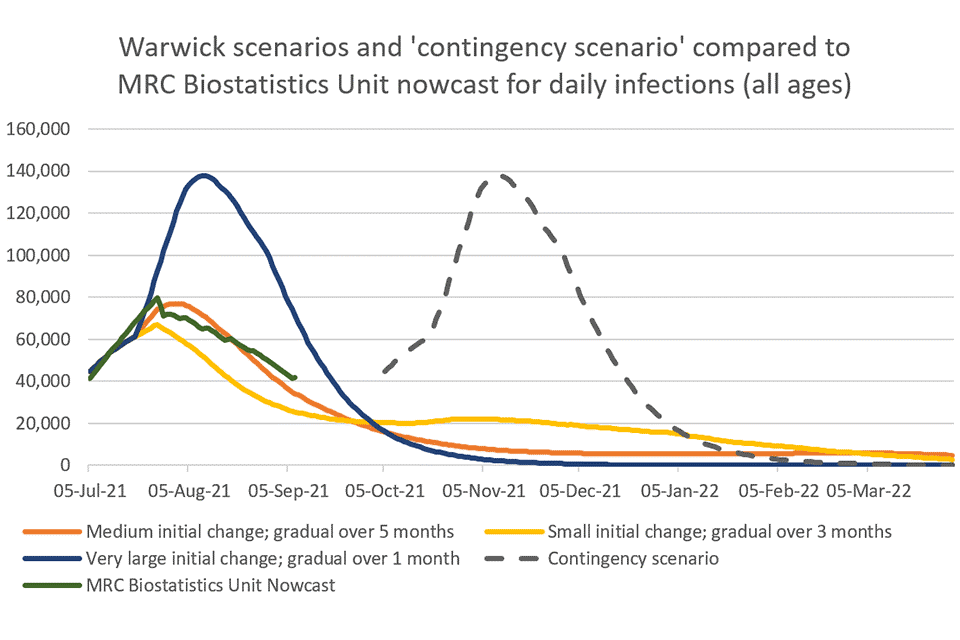
Figure 2: Warwick scenarios and contingency scenario compared to MRC daily infections – all ages, England, July 2021 to March 2022
School absence due to confirmed infection
Figure 2 shows the estimated number of infections in the 12 to 15 year old population in the 7 Warwick University scenarios. The dotted line represents nowcast estimates undertaken by the University of Cambridge MRC Biostatistics Unit and Public Health England. This is included to provide a comparison of the number of infections estimated by each of the Warwick scenarios to the reality of the trajectory of the pandemic.
Table 5 shows estimates for the number of averted infections in 12 to 15 year olds in England in a circumstance where 12 to 15 year old individuals are invited to have one dose of a vaccine. We assume a 60% uptake in this age cohort which aligns with the uptake of the seasonal influenza vaccine in school age children.[footnote 11]
Some recent surveys have suggested quite optimistic levels of support in parental views on vaccinating children with a COVID-19 vaccine. The ONS School Infection Survey (SIS) regularly reviews parental hesitancy to COVID-19 vaccination of children. The latest round (round 6) of SIS found only 14% of parents of secondary-age school children to be hesitant, with 86% sharing that they definitely would or probably would consent for their children to be vaccinated.[footnote 3] Therefore, the 60% assumption used in this analysis may be an underestimate.
We assume that a vaccination programme is completed in September 2021 and vaccine effectiveness is achieved from week commencing 18 October 2021 onwards (allowing for approximately 3 weeks for protection to start).
Table 5: number of averted infections in 12 to 15 year olds occurring post-vaccination of 12 to 15 year olds with 60% uptake in England – 18 October 2021 to 31 March 2022
| Scenario | Number of averted infections: 40% VE, 60% uptake | Number of averted infections: 55% VE*, 60% uptake | Number of averted infections: 70% VE, 60% uptake |
|---|---|---|---|
| Medium initial change, gradual over 5 months | 20,000 | 30,000 | 40,000 |
| Small initial change, gradual over 3 months | 50,000 | 60,000 | 80,000 |
| Very large initial change, gradual over 1 month | 3,000 | 4,000 | 5,000 |
- VE is vaccine efficacy.
The effects of vaccination will not be apparent from day 1 of the vaccine programme. It takes time for the effects of vaccination to become apparent, and so we assumed that infection rates up to 18 October 2021 is still comparable to those of an unvaccinated population.
Averted infections in 12 to 15 year old infections translate to a decrease in days missed from school due to sickness and self-isolation. We assume an average number of isolation days per PCR-confirmed infection of 11 days. A proportion of infections and isolation days will occur outside of school periods – we adjust for this in our estimates. We also adjust for the fact that not all infections will translate to positive cases – some will go untested and undetected.
The MRC true infection estimates were compared to PHE COVID-19 case surveillance data for the 12 to 15 year old cohort.[footnote 12] This calculation suggests that around 64% of infections will translate to a positive test. Table 6 shows the estimated number of saved school days per scenario.
Table 6: number of averted COVID-related missed school days for 12 to 15 year olds due to vaccination in this group, assuming a 60% uptake – October 2021 to March 2022
| Scenario | Number of averted COVID-related missed school days: 40% VE | Number of averted COVID-related missed school days: 55% VE | Number of averted COVID-related missed school days: 70% VE |
|---|---|---|---|
| Medium initial change, gradual over 5 months | 90,000 | 110,000 | 140,000 |
| Small initial change, gradual over 3 months | 180,000 | 230,000 | 290,000 |
| Very large initial change, gradual over 1 month | 10,000 | 20,000 | 20,000 |
In total the range in the number of averted miss school days up to 31 March 2022 occurring given the 3 various scenarios and 3 assumed vaccine efficacies is between 10,000 and 290,000. The 290,000 occurs in the ‘small initial change, gradual over 3 months’ scenario with the 70% vaccine efficacy against symptomatic infection from Delta. The minimum estimate of 10,000 averted missed school days occurs in the ‘very large initial change, gradual over 1 month’ scenario with a 40% vaccine efficacy.
Pupils absent due to contact inside and outside of school
In the 3 main scenarios we assume that infections are at such a level that current NPIs remain in place, and therefore we assume no absences due to self-isolation due to contract tracing of 12 to 15 year old students.
In the contingency scenarios, we assume that self-isolation of close contacts – both contacts within the school setting and outside – will return. We estimate the number of days of absence caused by the number of pupils self-isolating due to close contact using ratios of absence to infection in 12 to 15 year olds in the historic data. The ratio is calculated using DfE data on days of self-isolation of close contacts during the summer term 2021 (week 24 to week 28) and data on the number of infections in 12 to 15 year olds during this period. This estimated ratio is then applied to the estimates of infections occurring between October 2021 and March 2022 in 12 to 15 year olds in the contingency scenario in order to estimate the number of days lost due to self-isolation of contacts.
Table 7: number of averted absences from self-isolation due to close contacts in and out of school with and without vaccination of 12 to 15 year olds – contingency scenario, 18 October 2021 to 31 March 2022
| No vaccination | Vaccinated, 60% uptake, 40% VE | Vaccinated, 60% uptake, 55% VE | Vaccinated, 60% uptake, 70% VE | |
|---|---|---|---|---|
| Days of absence to self-isolation due to contact in school | 27,000,000 | 20,000,000 | 18,000,000 | 15,000,000 |
| Days of absence to self-isolation due to contact outside of school | 4,600,000 | 3,500,000 | 3,100,000 | 2,700,000 |
| Averted days of absence to self-isolation due to close contact in and out of school | N/A | 8,000,000 | 10,000,000 | 13,000,000 |
Pupils absent due to closure of schools
Over the course of the pandemic there were periods where school closure became a mandatory NPI. Outside of these periods, it has been a priority to keep schools open when possible, and schools are only closed as a last resort measure. In the 3 main scenarios we assume infections are at such a level that school closures do not occur. DfE data shows that, over the 6 school weeks from 14 June to 18 July, the percentage of children absent due to school closure increased from 0.06% to 0.86% as compared to the average for the period of 0.38%.
We use historic data from June 2021 to estimate the ratio of absence days due COVID-19-related school closure and infections in the 12 to 15 year old population. We apply this to the contingency scenario, where we assume that levels of infection are high enough for school closures to again occur.
Table 8: number of absences due to school closure post-vaccination of 12 to 15 year olds in the contigency scenario – 18 October 2021 to 31 March 2022
| No vaccination | Vaccinated, 60% uptake, 40% VE | Vaccinated, 60% uptake, 55% VE | Vaccinated, 60% uptake, 70% VE | |
|---|---|---|---|---|
| Days of absence due to COVID-19-related closure of schools | 2,000,000 | 1,500,000 | 1,300,000 | 1,100,000 |
| Averted days of absence due to COVID-19-related closure of schools | N/A | 500,000 | 700,000 | 800,000 |
Socio-economic impact
Evidence suggests that children experiencing higher levels of disadvantage have experienced greater days of lost schooling. Analysis undertaken by the Education Policy Institute suggests that there is a relationship between missed classroom learning days and deprivation.[footnote 13] DfE data on pupil absence in the autumn term 2020 showed that pupils eligible for free school meals missed 30% more school days than other pupils.[footnote 14]
Uptake of the COVID-19 vaccine among the eligible cohorts to date has been lower in more deprived areas. Statistics published by NHS England show that as of 31 July 2021 81.9% of adults living in the least deprived areas of England according to the Index of Multiple Deprivation (IMD) deciles have received 2 doses of a COVID-19 vaccine, whereas only 61.4% of adults living in the most deprived areas have received 2 doses of a vaccine. Table 5 shows the difference in uptake by IMD decile in England for the period 8 December 2020 to 31 July 2021.[footnote 15]
Table 9: uptake of COVID-19 vaccine, ages 18 and above, by IMD decile in England
| IMD decile | % who have had at least one dose | % who have had both doses |
|---|---|---|
| 1 (most deprived) | 78.9% | 61.4% |
| 2 | 80.8% | 63.1% |
| 3 | 81.9% | 64.5% |
| 4 | 84.3% | 67.5% |
| 5 | 86.7% | 70.7% |
| 6 | 88.7% | 73.3% |
| 7 | 90.6% | 75.9% |
| 8 | 92.6% | 77.8% |
| 9 | 93.7% | 79.5% |
| 10 (least deprived) | 95.7% | 81.9% |
If there was to be a large discrepancy in uptake between children in the most and least deprived areas, it could possibly widen the discrepancies in missed school days that already exists between those in the most and least deprived regions.
-
JCVI advice on 15 July 2021 is estimated to apply to 150,000 12 to 15 year olds, and further advice on 3 September is estimated to add an additional 200,000 to the definition of at-risk 12 to 15 year olds. ↩
-
For further details on these models, see University of Warwick: Roadmap scenarios and sensitivity – step 4, 6 July 2021. ↩
-
ONS, COVID-19 Schools Infection Survey, England: round 6, June 2021. ↩ ↩2
-
This one-dose Pfizer/BioNTech efficacy is based on studies exploring efficacy against the dominant B.1.617.2 Delta variant undertaken in the UK and Qatar. ↩
-
Figures presented here are rounded to 1 to 2 significant places. As a result, subsequent calculations on these values, such as adding and subtracting columns, will not give accurate results. ↩
-
The range on contingency scenario difference is based on vaccine effectiveness only. This ranges from 40% to 70% with a mid-estimate of 55%. ↩
-
‘Tracing and self-isolation’ in What parents and carers need to know about early years providers, schools and colleges. ↩
-
JCVI issues updated advice on COVID-19 vaccination of young people aged 16 to 17 ↩
-
BNT162b2 and mRNA-1273 COVID-19 vaccine effectiveness against the Delta (B.1.617.2) variant in Qatar, medRxiv. ↩
-
Seasonal flu vaccine uptake in children of school age: winter 2020 to 2021 ↩
-
Education Policy Institute, School attendance and lost schooling across England since full reopening. ↩
-
NHS, COVID-19 vaccinations (monthly statistics, 12 August 2021). ↩