[Withdrawn] Data saves lives: reshaping health and social care with data (draft)
Updated 10 February 2022

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/data-saves-lives-reshaping-health-and-social-care-with-data-draft/data-saves-lives-reshaping-health-and-social-care-with-data-draft
Ministerial foreword
When facing the greatest public health emergency that this country has tackled for generations, one of the most impactful tools at our disposal was the power of data. With the facts, data, and science at our disposal, we can provide the meaningful and measurable results that the public deserves.
Data identified those who are most vulnerable to coronavirus. It helped us to help them shield, which protected both themselves and their families.
Data was essential to our day-to-day response.
And it powered vital research that helped us discover new treatments that saved lives in communities across the world.
Data made all the difference.
Across the health and care system people are using data more efficiently and effectively than ever before in a myriad of different and essential applications.
The urgency of this pandemic has driven unprecedented digital transformation throughout health and care. It has transformed people’s relationship with the NHS - for the better. People who might have only used the NHS once a year have been using the NHS COVID-19 app and NHS Test and Trace as part of their daily routines. Comfort and familiarity are already paying dividends for public health and will for decades to come.
Now is not the time to slow down or pause for breath, when the opportunities are so vast, and the momentum is so great. To the contrary, now is the time to grow our gains. It is our solemn responsibility to continue to improve the quality of life of every person in every community.
Our strategy delivers a strong set of commitments showing how we can build on this engagement, and this passion, and promote this transformative work even further.
It sets out our mission to unleash the unlimited potential of data in health and care, while maintaining the highest standards of privacy, ethics, and accountability.
Putting this strategy into action will deliver better treatment for patients, better health results for people who need care and support, and better decision making, research, and support for our colleagues on the front line. It also sets out how we will support the developers and researchers who we’ve all seen have so much potential to transform health and care. They save and improve lives, every day. They deserve our tireless support, just as they have worked tirelessly for our citizens.
Within this strategy you’ll find bold commitments like separating data from the underlying application to provide greater flexibility, boosting the platforms that can drive more effective clinical trials, and giving people the right to see their own data.
Just as we’ve done all throughout this pandemic, we want to bring to bear expertise from both inside and outside the government. So, we want to hear from you about our plans, and about what more we can do to improve them. We want you to be in control.
Our plan of action contains big ambitions, but there’s no better time to act. Our shared experience of this pandemic has shown us the prize that’s on offer. Now we must bottle the spirit we’ve seen and use the full power of data to deliver real solutions to the new challenges ahead.
Rt Hon Matt Hancock MP
Secretary of State for Health and Social Care
Executive summary
In England and in every community around the world, digital developments have been essential to the pandemic response. People have accessed advice and care remotely in unprecedented numbers, helping keep them and their families safe. World class genomics helped identify and track new variants. Daily analysis allowed problems to be understood rapidly, and resources redeployed. Staff worked remotely. And the COVID-19 vaccination service was mobilised in record time.
Such an efficient and effective response was only possible because of investment in digital systems, innovation and skills over the last few years, and the partnerships forged between digital, clinical and operational colleagues.
The opportunity now is for the health and care sector to apply such approaches with increased urgency and consistency to both our long-term challenges and to the immediate tasks of rebuilding from the pandemic. We have a responsibility to do both.
The Digital Transformation Plan sets out the overarching vision for how we will digitise, connect and transform the health and care sector. This data strategy explains in more detail the role that data will play in that transformation and how it can inspire effective collaboration across the NHS, adult social care, and public health, help us care for people in the best possible way, and ensuring that our citizens have the best experience possible when using the system.
There are 3 key priorities which underpin this strategy:
-
first to build understanding on how data is used and the potential for data-driven innovation, improving transparency so the public has control over how we are using their data
-
second to make appropriate data sharing the norm and not the exception across health, adult social care and public health, to provide the best care possible to the citizens we serve, and to support staff throughout the health and care system
-
third to build the right foundations – technical, legal, regulatory – to make that possible
We know that this will be a long and complex task. The health and care system is vast – with every facet important – and parts of it are at different stages of their data transformation journey. The COVID-19 pandemic has had a huge impact in accelerating this process, but legacy systems and less efficient ways of working will be a barrier to change. Patients, service users, clinicians, carers, analysts, researchers and innovators from across health and care have individualised and personalised needs and priorities.
But we cannot ignore that these are challenges worth taking on and we are not beginning with a blank page. A meaningful collaboration has already been initiated to promote our data and digital capabilities across the system.
Each chapter of this strategy describes our vision for the future of health and adult social care data - for citizens, for staff, for decision makers, researchers, developers and innovators - and the commitments required to achieve that vision.
Chapter 1: Bringing people closer to their data
Our vision: our most important responsibility is to deliver truly patient-centred care, which puts people before systems, so people will have better access to their personal health and care data and understand exactly how it is used.
We will achieve this by:
- bringing people closer to their data
- harnessing data to improve patient and service user safety
- giving people confidence
Chapter 2: Giving health and care professionals the data they need to provide the best possible care
Our vision: staff can only do their best when they have the right information, so staff will have easy access to the right information to provide the best possible care.
We will achieve this by:
- simplifying information governance
- creating a new duty to share
- delivering shared records
- reducing the data collection burden
- harnessing safe and effective innovation
Chapter 3: Supporting local and national decision makers with data
Our vision: leaders and policymakers have a responsibility to continually improve how the people we serve receive care, so leaders in every community will have up-to-date sophisticated data to make decisions and help the health and care system run at its best.
We will achieve this by:
- integrating local care systems with a culture of interoperable by default
- building analytical and data science capability
- working transparently in the open
- sharing data for wider purposes
- collaborating with wider partners
Chapter 4: Improving data for adult social care
Our vision: service users and their carers will have high quality, timely and transparent data to improve outcomes, and can easily access to help them make choices about their care.
We will achieve this by:
- improving access to information for adult social care providers
- integration of health and social care data
- expanding the use of care technologies
Chapter 5: Empowering researchers with the data they need to develop life-saving treatments, models of care and insights
Our vision: our researchers can only deliver results based on the information available to them, so they will be able to safely and easily access data to provide innovative solutions to health and care issues for the benefit of every citizen in every community.
We will achieve this by:
- providing safe and secure data for analysis and research
- sharing data for research
- encouraging clinical research
Chapter 6: Helping colleagues develop the right technical infrastructure
Our vision: to maximise the efficiency and effectiveness of our infrastructure, we will ensure the data architecture underpinning the health and care system can easily work together to make better use of data, no matter where it is kept.
We will achieve this by:
- modernising our data architecture
- promoting and developing data and technical standards
- staying ahead of evolving cyber risk
- separating the data layer
Chapter 7: Helping developers and innovators to improve health and care
Our vision: time and safety are both essential, so innovators will be supported to develop and deliver new solutions safely and sensibly for the benefit of all citizens, staff and the system.
We will achieve this by:
- driving interoperability for innovation
- encouraging AI innovation
- clear and understandable AI regulation
- supporting innovators to work with health and care organisations
- creating fair returns in data partnerships
This strategy aligns with the government’s National Data Strategy, and the forthcoming NHSX Digital Transformation Plan.
1. Bringing people closer to their data
Our vision
Our most important responsibility is to deliver truly patient-centred care, which puts people before systems, so people will have better access to their personal health and care data and understand exactly how it is used.
As someone using health and adult social care services, I will have:
-
digital access to my health and care information, such as test results, medications, procedures and care plans from across all parts of the system so I can better understand and plan my care
-
systems to easily manage appointments, refill medications, and speak with health and care staff
-
the ability, if I want, to share additional data I have collected to improve my wellbeing, such as sleep, food, exercise, and genome
-
confidence that health and care staff have my up-to-date information, regardless of the care setting so I won’t have to repeat details unnecessarily
-
increased transparency about how the health and care system protects and uses my data
Why this matters
Data helps the whole health and care system deliver the best care to the citizens we serve.
We need to make sure that patients and service users have the peace of mind that health and care staff have all the relevant information about them at their fingertips so they can provide the best quality of care possible. We want to make sure that patients should not have to unnecessarily repeat information on their medical history or have duplicate diagnostic tests when one is enough. We need to make sure that any preferences or requests for reasonable adjustments are all kept on record so that staff can easily find the information.
Patients and service users have often been far removed from the information that the system has on them, and so they are not partners in their care. This needs to change. They need to know what information the health and care system has about them, such as inoculations or previous medicines, as long as it does not impact their safety. We need to bring our citizens closer to their data, so they can be properly involved in their own care.
The NHS is one of the most trusted organisations in the UK, and responses to the government’s National Data Strategy consultation further showed widespread support for harnessing data for public benefit, so we know that everyone wants to make sure that we provide the public with the best possible services and care.
For example, the recent report from the National Data Guardian for Health and Care (NDG), Putting good into practice, highlighted that the public did not feel that data had to be used only for its original purpose if it was bringing wider public benefit. Their main priority was that the data is used in a relevant way, such as for research or to benefit even a small number of people.
We want to ensure that this data is made available for use to help effectively deliver care and support our health and care system. However, it is critical that we do this in a way where patient confidentiality and trust is prioritised and never compromised. Our priority is that a system exists to maintain the highest standards around data transparency and accountability. There are strict legal, privacy and security controls on how people’s health and care data can be used, such as GDPR, the Common Law Duty of Confidentiality, and the Health Research Authority’s Confidentiality Advisory Group.
The public’s data belongs to them so it’s important it is safely and securely only used in ways that benefit everyone using the health system. We do not sell health and care data for the benefit of private companies. Where access to data is granted, having met these high thresholds, it must always have the explicit aim to improve the health and care of our citizens, or to support the improvements to the broader system. This includes sharing data with researchers to develop COVID-19 vaccinations, for improved cancer treatments to be developed, and help health and social care organisations to more effectively support their patients and service users.
We must make sure that we build on our approach and use data to provide every single person that uses the health and care system with the best possible care and experience.
Progress so far
People are engaging with their health and care data more and more:
-
almost 2 million people are now using the NHS App, a simple and secure way to access a range of NHS services. In February 2021 there were more than 3 million logins to the App, compared with 570,000 in February 2020
-
the GOV.UK coronavirus dashboard was created to provide people with up-to-date local and national data. The site has over 19 million weekly views and during the third lockdown, there were a record 76.5 million hits in 24 hours
Taking this further
Harnessing data to improve patient and service user safety
Keeping our citizens safe is the guiding principle of all staff across heath and adult social care. Patients and service users need to be confident that staff have the right information about them, their diagnoses, medications, and preferences.
They need to be confident that the people caring for them have up-to-date information about them, such as the medications they are taking or are allergic to; the previous care they have been given; and any important things they should know about. If health and care staff can easily access the right information about people in their care, citizens can be confident that they are being given the best care possible.
The information we collect from care can also help us improve everyone’s safety, outcomes and experience. It helps us continually improve the health and care system; develop new treatments, advice and guidance; and introduce new ways of working. All with the aim of improving care and patient safety.
Collecting data on Patient Reported Outcome Measures (PROMs) which assess the quality of care delivered to NHS patients from the patient’s perspective also supports this. Data from the National Diabetes Audit, for example, has been used to identify areas of the country where action is needed to ensure more targeted treatment to reduce unnecessary leg and foot amputations. Data on PROMs also helps us enhance benchmarking for care, and, where appropriate, helps patients choose their clinicians.
Case study: Mothers and Babies: Reducing Risk through Audit and Confidential Enquiries (MBRRACE-UK)
Sharing data and information on maternal and child population health is vital if we are to continuously improve the services we provide to keep mothers and children safe.
While it is uncommon for women to die during or after pregnancy in the UK, we must examine the care received by all women who have sadly died. Because these deaths are rare, in order to identify problems, see patterns, and make change, we must have timely and accurate data from every organisation about every death. Only then can we see the full national picture of what needs to change, where and how.
In 2016 to 2018, 217 women died during or up to 6 weeks after pregnancy, from causes associated with their pregnancy, among a total of 2,235,159 women giving birth in the UK. Analysis of this data shows us that women who have pre-existing medical conditions are at higher risk of dying in pregnancy. However, the data also helps inform us about what actions can be taken to reduce these risks.
Each maternal death is investigated by MBRRACE-UK. Their most recent report into maternal deaths (2020) highlighted that 13% of women who died during 2016 to 18 was due to epilepsy or strokes.
Of particular concern, the report identified an increase in deaths amongst women with epilepsy from a condition known as ‘Sudden Unexpected Death in Epilepsy’ or SUDEP. The number of deaths from SUDEP almost doubled compared with the previous 3 years, from 8 in 2013 to 2015 to 18 in 2016 to 2018.
Most women who died had clear risk factors for SUDEP, such as fits that were not well controlled or that happened at night. However, they did not have prevention measures discussed with them, or a review of their anti-epileptic medication to make sure they were the best prescription for them.
By using the data collected about the circumstances of these tragic deaths, we have been able to make sure that pregnant women with epilepsy are better supported. This includes discussing their risk of SUDEP, reviewing their medication, and being given advice such as to not bathe or sleep alone while they are pregnant or new mothers.
Harnessing data from the health and care system helps us keep pregnant women and their children safe and prevents pregnant women from dying from epilepsy in the future.
We must also make sure that patients and service users are kept safe, regardless of their care setting (hospital, care home, in their own home). People often feel more comfortable being treated at home but may be concerned about their safety if they are not close to their clinicians or carers.
Tools such as remote monitoring help keep people safe at home, and allow health and care staff to see the data that is being captured and respond quickly and effectively if someone becomes unwell at home.
Case study: COVID-19 remote monitoring
Large numbers of COVID-19 patients have been supported through Oximetry@home and COVID-19 virtual ward pathways. Patients with COVID-19 are given a device to measure their blood oxygen levels (a pulse oximeter) teamed with an app on a smartphone or accessible via the web.
This enables them to track their symptoms and share their results with the clinical team supervising them quickly and easily. It allows their progress to be reviewed and for any deterioration to be picked up rapidly and reduces the time it takes clinical teams to safely monitor their patients.
In May 2020, a COVID-19 patient with severe asthma and phobia of hospitals was selected by clinicians for remote monitoring. On day 7 of her infection, the clinical team were alerted to worsening oxygen saturation levels and quick action was taken to triage her into an acute setting for proactive management of her symptoms. Had she not been monitored it is expected the patient would have presented late through emergency and required more intensive and costly critical care.
Patient feedback:
I just want to say a huge thank you for the fantastic level of care I received when I was unwell. Your dedication, the daily phone calls, access to the app and delivering all my medications to me were greatly appreciated.
Clinician feedback:
We’ve been able to recognise changes and prompt a medical review or treatment that could prevent a hospital admission or even a near-death experience. This technology is good and works well.
Patients and service users from every community and background also need to feel confident that they will be looked after to the best of their ability, no matter their ethnicity, gender, or where they live. For example, in the first wave of the pandemic people from ethnic minority backgrounds had higher age-adjusted COVID-19 mortality rates. That is why in June 2020, the Prime Minister and the Secretary of State for Health and Social Care asked the Minister for Equalities to lead cross-government work to address this disparity. We must use all the data at our disposal to keep each one of our citizens safe.
Our commitments:
-
we will improve information governance guidance so staff are confident in sharing people’s data for their individual care, including publishing the Information Governance Framework for Integrated Health and Care (July 2021)
-
we will undertake further work on harnessing data to improve health outcomes and reduce inequalities, including the AI Ethics Initiative which will report in 2022/23 on its research call exploring how to use those technologies to improve health outcomes for minority ethnic populations in the UK (ongoing)
-
we will digitalise personal child health records to ensure families and professionals have the information they need, when they need it. This work is supported by the Early Years Healthy Development Review published in March 2021 which sets out how better data-sharing could improve the experiences of parents, carers and staff (2023)
Bringing people closer to their data
We know from research that the public is supportive of their data being shared, both for their own care and for the wider benefit of others.
The Putting good into practice programme showed that the public is keen that the health and care system be transparent about its use of data, so people can easily find and understand information on how decisions are made and with broad engagement across different sections of society. The programme found that, as long as the legal and ethical safeguards are in place, people are ready to put their trust in the system to use their data for the wider public benefit, not just for their own care.
Data also forms the basis for published statistics which helps us understand the overall picture of the health and care system at a national, regional and local level. Statistics are not just for decision makers across the system. The pandemic has also shown us how important it is for our citizens to understand what is happening across the country, and there has been huge public interest in the aggregate picture of issues through the engagement with GOV.UK coronavirus in the UK dashboard. We will work to make sure that statistical data is accessible to continue to inform the general public on health and care issues.
However, not everyone is familiar with how their data is being used, which can create unease about sharing data and adopting digital technologies. We have a responsibility to help everyone understand how their health and care data is being used, and how they can make the most of it.
The NHS App and other patient-facing apps are driving forward better access to data. However, if specific data that patients and service users need isn’t available through those methods, they must make a subject access request (SAR) to each care provider. We need to help them easily access appropriate levels of their information so that they can safely become partners in their care. We will set out further rights for people to access their record, to update their contact details in their NHS record via a digital mechanism, and to decide how they want the system to interact with them. We will also make them aware how the data they’ve shared has been used for cutting edge research: saving lives, improving treatments, and helping the health and adult social care system to plan for the future.
Our commitments:
- we will make sure that the technology is in place to enable everyone across England to have easy access to their own health and care data (2022)
This example below compares the experiences of an individual with asthma under the current system, compared with how it could potentially look in the future.
Context
Aisha is diagnosed with mild asthma at age 5, and assigned an Asthma Action Plan. Her asthma continues over the next 20 years in a mild form with few complications.
Current situation
Aisha has an asthma attack away from home and has to go to the nearest Emergency Dept (ED). They can only access basic information about her current medication.
Aisha is referred for a follow-up with her GP. The GP can only access basic information about Aisha’s visit to ED and current medication. The GP makes an appointment with the asthma nurse.
Aisha receives a phone call from the GP practice with the appointment details.
Before the appointment, Aisha’s asthma worsens and she attends her local ED. They do not have access to information about her other hospital admission.
Aisha is given some additional medication at ED.
Aisha attends the appointment with the asthma nurse, and has to update him on the medication she was prescribed at ED.
In the future
ED staff pull Aisha’s medical history and can see her childhood asthma diagnosis and treatment history. They treat her accordingly, run tests, and add this information to her record.
Aisha’s GP accesses the information relating to her visit to ED, reviewing this and any changes to medication. Using this information, the GP makes a referral to a respiratory clinic.
After receiving a notification, Aisha can see from the online access she has to her records the referral appointment details.
The respiratory clinic recommends additional quantities of long-term preventative medication, which is updated on her record.
Aisha can access this information via her NHS Account, and request a repeat prescription for her new medication.
Aisha is booked in for a follow-up with the respiratory clinic, and adds this appointment, and a reminder, directly to her mobile calendar.
Case study: personal data stores
Personal data stores are a technology that allows a person’s data from multiple sources to be brought together into their own data store. It takes the concept of separating data from the systems that hold it to create a network of decentralized personal data stores. This includes information from systems in hospitals or general practice, data from wearable devices and home monitoring technology, or data entered directly by the citizen and/or an authorised representative.
People can update information about their preferred method of contact in their data store which helps avoid them informing multiple organisations if they wish to change their address or phone number. Overall, these data stores allow the health and care system to use patient data more effectively and efficiently to deliver better care for patients.
Social Linked Data (SOLID) is an example of this technology. Developed by World Wide Web founder Sir Tim Berners-Lee, it uses international open standards to let people control their data and choose the applications and services to use with it.
We are supporting a SOLID pilot project with an NHS team based in Salford. This will build on their experience to develop a series of use cases and prototypes, working alongside academics from the University of Edinburgh to better understand any related sociological, professional, commercial and economic consequences to ensure the best possible outcomes for the health system.
Giving people confidence
Anyone receiving care will only share their information with confidence if they feel like there are proper safeguards in place, and that those entrusted with their data will keep it safe. That is why we have, for example, the National Data Guardian, an independent champion for the public to ensure that people’s personal information is safely shared to improve health and care outcomes.
Most of all, every organisation, every clinician and carer, every scientist accessing the data needs to be able to show that they handle it with great care. For example, appropriate data sharing is often critical for providing holistic care to patients with mental health issues, however this must be handled with huge sensitivity and care. Clinicians should only seek to access information that is relevant to their patients and are accountable to their regulatory bodies if they do not follow appropriate information governance and confidentiality guidelines.
We need to trust that information about our health is always used responsibly and with strict safeguards to help us make our own decisions about our health, for our own care, to help the NHS, our care system, and to drive research.
We are committed to making sure that our citizens’ data is handled safely, lawfully and transparently in line with the UK’s data protection legislation. The work we do is always for the overall benefit of everyone using the health and care system.
We must also look to the development of new advances in how data is collected, stored and analysed, and we already work with de-identified, anonymised and pseudonymised data which helps us maintain people’s privacy.
We must continue this work including with new privacy enhancing technologies (PETs) that support keeping personal information safe. As noted by the Centre for Data Ethics and Innovation, PETs include:
-
synthetic data: generating data that is statistically consistent with a real dataset and can replace or augment sensitive data
-
federated analytics: applying data science techniques by moving code to the data, rather than the traditional approach of collecting data centrally
-
homomorphic encryption: allowing computations to be performed on encrypted data
-
differentially private algorithms: enabling useful population-level insights about a dataset to be gained, while limiting what can be learned about any individual in the dataset
Part of this includes secure data processing and trustworthy data sharing which ensure that data is used safely and in an ethical way. Test and Trace’s data platform EDGE is a secure environment for the Joint Biosecurity Centre (JBC) to undertake data analysis and modelling, linking safely to the Office for National Statistics’ Secure Research Service. The interactive map for COVID-19 in the UK also publishes data so people can see cases in their area but with people’s privacy still protected.
Additional techniques such as creating synthetic data based on anonymised health and adult social care data help us produce data that is statistically aligned with real data but doesn’t contain any information about ‘real’ people. This can either replace or augment sensitive data use in research or data-driven systems.
Our commitments:
-
publish the first transparency statement setting out how health and care data has been used across the sector (2022)
-
give citizens the ability to see what research their data has informed, and who has had access to their data, as soon as the technology allows (ongoing)
-
embed an open-working approach across health and social care, consistent with protecting privacy, so the public can easily find and understand the data delivery work (ongoing)
-
lead the Health and Care Information Governance Panel to develop guidance, frameworks and standards such as data sharing and transparency so the public can be confident in our handling of their data (December 2021)
Case study: keeping patient data safe with synthetic datasets
Synthetic datasets are a way to protect people’s privacy because they don’t include data on real patients. Instead, they mirror the symptoms, diagnoses and treatments of genuine patients. This means that researchers and innovators can validate their data-driven technology and medical devices without real people’s data ever being seen by them. This enables a more open relationship between health and social care providers and industries, as no personal data is flowing between them.
Using synthetic data means that innovative research and products can be developed more quickly than if real patient data was used. This means that new advances can be brought to market sooner for patients to benefit from them.
We already have fantastic synthetic datasets across the health system which help us keep people’s data safe. For example, NHS England’s SynAE project created synthetic datasets based on over 70 million A&E records in England. The data can be used to develop predictive models on who is most likely to attend A&E or who is most likely to be admitted, which helps the health and care system work on prevention.
The Simulacrum is another dataset that contains artificial patient-like cancer data to help researchers gain insights. It imitates some of the data held securely by the Public Health England’s National Cancer Registration and Analysis Service. It allows anyone who wants to use record-level cancer data to do so, safe in the knowledge that while the data feels like the real thing, there is no danger of breaching patient confidentiality. The MHRA is also creating 2 innovative synthetic datasets to support the development of cutting-edge medical technologies to fight coronavirus (COVID-19) and cardiovascular disease so that these can be brought to patients as safely and quickly as possible.
Collaboration is vital if we are to drive the use of privacy enhancing technologies and to embed their use across health and social care. For example, MHRA’s datasets were produced by Clinical Practice Research Datalink (CPRD), MHRA Medical Devices Division and researchers at Brunel University. The COVID-19 synthetic dataset was funded by the NHS AI Lab, and the cardiovascular dataset was funded by the Regulators’ Pioneer Fund and managed by Innovate UK.
2. Giving health and care professionals the data they need to provide the best possible care
Our vision
Staff can only do their best when they have the right information, so staff will have easy access to the right information to provide the best possible care.
As health and adult social care staff, I will have:
-
systems that provide quick and easy access to information about the people in my care, no matter where they have been treated before, so I can:
- have the data to make the right decisions and recommendations about their care
- reduce the time looking for information to spend more time with the people I am caring for
-
all relevant information about people in my care, such as data about their sleep or physical activity, so I can have information-driven conversations about their care
-
confidence about when I can share data and how, so that I can share for the benefits of people in my care and for the running of the system
Why this matters
Health and social care are built on the scientific foundations of what can be done to improve people’s health and wellbeing, and data is the lifeblood of this scientific approach. We need to give staff up to date information about the person in front of them so they can provide the best possible care by making more accurate diagnoses, understanding patient and service user preference to offer more personalised care, and keeping people safe.
There is a large burden on staff to spend large amounts of time collecting data on the frontline, often because data isn’t shared with them and they need to collect it again. When information is not at their fingertips, they must find workarounds or look through paper-based documents. We want to make sure that the data is immediately available on the systems they use to do their jobs.
We also have an unprecedented number of data analysis tools, helping us find patterns and trends, identify diagnoses and treatment possibilities at previously unimaginable speed.
If we get this right, we will not only deliver huge benefits to our citizens, but we can also free up staff time to focus on what they do best - giving the best possible care to patients and service users.
Progress so far
To support the COVID-19 pandemic response:
-
NHSX issued one page of simple information governance guidance to help staff share data with confidence, with the support of the Information Commissioner and the National Data Guardian (NDG)
-
government used the Control of Patient Information (COPI) (2002) Regulations to issue notices requiring public sector organisations to share patient information to support the COVID-19 response
-
NHSX, with NHS England and NHS Improvement, established a Single Front Door for anyone requesting data for COVID-19 response purposes
Tripled the use of NHS mail in the social care sector, with over 10,000 care homes and nearly 4,000 domiciliary care sites enabled so staff can securely share data across email. We also expanded secure sharing across other secure email systems.
Made good progress with some form of operational shared care record solution in place in 60 areas across England.
Developed the Information Governance Framework for Integrated Health and Care to provide a structured approach when processing data for individual care, and other uses such as population health management, commissioning, and needs assessments.
Created the Information Governance Portal to act as a single point of access for information governance guidance for health and care staff, the public and information governance professionals.
Established the Data Alliance Partnership and the Data Alliance Partnership Board which has assumed system-wide leadership of data collections across the health and care system.
Invested in new technologies, such as Robotic Process Automation to automate appointment bookings or situational reporting, to free staff up to spend more time with patients and service users.
Taking this further
Simplifying information governance
We know that information governance policies are complicated and can differ from trust to trust, which means that health and care data is often not shared, even when it should be. Confusion around the legal framework, and a multitude of organisations giving guidance, further complicates the situation. For staff at the frontline, the risk of ‘getting it wrong’ can feel so great that it feels safest not to share.
Case study: Carl Starbuck, Leeds and York Partnership NHS Foundation Trust
Speaking as an Information Governance professional, an NHS employee and senior manager, and perhaps most importantly as a UK citizen, I have both welcomed and valued the timely, focused and concise Information Governance advice provided by NHSX throughout the COVID-19 emergency.
The simplified Information Governance guidance enabled Carl to:
- maintain support to his community of mental health patients via video conferencing when face-to-face contact was unsafe under lockdown
- select the right solutions with information security assurance at pace so that patient care was not impacted by delays
- feel empowered, as an Information Governance professional, to select solutions in the best interests of service users
- ensure staff could feel confident that the NHS Information Governance leadership ‘had their back’
In short, at a time of great turmoil across the health and social care system, NHSX empowered Information Governance professionals to clear the path for our clinical colleagues to do the day job without fear of Information Governance or Data Protection come-back.
Awareness of information governance is not just important for experts. All health and care staff need the confidence to appropriately share data to support and deliver people’s care. Just as we are encouraging digital skills across health and care organisations, we must encourage information governance awareness across the whole workforce.
We need to give our staff clear, unified, simple guidance on what they can share, who they can share it with, and for what purpose. We need to change the culture in which the rules are seen as an insurmountable barrier to data sharing, in which the safest option is not to share data even when this is to the detriment of care.
Our commitments:
- embed the Information Governance Portal as the one-stop shop for help and assistance, guidance and advice (December 2021)
- complete the key priority areas in our work to align national information governance guidance (April 2022)
- with the Health and Care Information Governance Panel, create fit-for-purpose rules around different types of data (such as pseudonymised), so that staff can clearly understand rules around the use of data (April 2022)
- we will develop a national Information Governance Strategy to address training for frontline staff (April 2022)
- we will review tool kits and language to bring into line with simplification work (July 2022)
- with the National Data Guardian (NDG), develop new e-learning packages on the use of data for frontline staff, information governance professionals, and Caldicott Guardians (2021)
Case study: Kelly Brow, speech and language therapist, Bradford District Care NHS Foundation Trust
Returning from maternity leave at the start of a major pandemic, I did expect to see fundamental changes. My first week back started with a session to fit my personal protective equipment (PPE). I was also told I’d take a video-first approach to my patients… We needed to get to grips with video calling tools.
The simplified guidance video conferencing with colleagues gave Kelly confidence to:
- provide videocare and assessments to service users ranging in age and level of disability
- spend time with patients instead of issuing and chasing individual video call consent forms
- undertake in-depth video and telephone triage of swallowing difficulties to give instant advice over the phone where appropriate and make follow up calls more quickly
- easily share tools and exercises with patients for use during the video session or to refer to between appointments
NHSX guidance has helped staff and trusts to quickly recognise that we are covered appropriately to use video calling tools.
Creating a new duty to share
Although a duty to share data for individual care already exists (Section 251B of the Health and Social Care Act 2012), staff still find it difficult to share information about patients between primary and secondary care, or for administrative tasks.
There is also no equivalent duty to share data between health and adult social care services, so staff often do not have enough information about the people they are caring for.
We want to drive an emphatic change in the culture toward data sharing across health and care. For health and care staff to be able to access the right information at the right time and in the right place, we need to remove the internal barriers to sharing data safely and appropriately. We want to give them the right information to do their jobs and keep people safe.
We will create a new duty on health and care organisations to share anonymous data (both data that was never identifiable, for example bed capacity, and de-identified data) so it will be more effectively and seamlessly shared across the system. It will send a clear signal that sharing to help staff do their jobs is a key duty and responsibility of all organisations across health and adult social care.
Our commitments:
- we will introduce legislation in due course to create a statutory duty for organisations within the health and care system to share anonymous data for the benefit of the system as a whole (ongoing)
Delivering shared records
We want to move towards a world where every doctor, surgeon, district nurse, pharmacist, allied health professional, and social care worker could draw information from, or put information into, what feels like the same shared care record, in a safe and straightforward way.
To make this vision a reality, we are building on our Shared Care Records (ShCRs) programme. These make it possible for staff that use different data systems, or record their data in different ways, to see a person’s information in one shared record. This will not only help us to break down the barriers that exist between health and care, but it will also improve patient safety and care.
It will focus first on linking general practice and hospital trusts, working towards comprehensive record sharing by 2024, in line with the NHS Long Term Plan and allowing people to make their own contributions into that shared care record.
Our commitments:
-
ensure that each Integrated Care System has a basic shared care record in place to enable sharing of key information between GP practices and NHS trusts (by end of September 2021)
-
deliver comprehensive shared records in line with the commitments in the NHS Long Term Plan so that authorised staff for other care partners can easily and appropriately access data regardless of where care is delivered (by 2024)
Reducing the data collection burden
Requests for data can often be burdensome on the front lines of the NHS and in social care. In November 2020, the Department of Health and Social Care published report on excessive bureaucracy in the health and social care system. The results were striking, showing how collecting data can pull staff away from their critical tasks of providing health and care.
Clinicians can be asked to record every instance of a particular procedure, or managers to pull together counts of bed or care home occupancy. This is important to make sure the right information is collected, but we need to do so in a smarter, more efficient way.
Reducing data burden on staff has huge benefits for being able to give them time back. By moving away from manual data collection to automated systems, staff can spend more time using data to do their jobs than collecting it. Freeing up staff time and understanding where we have the right levels of data collection means we can prioritise the areas where we urgently need more data, for example across adult social care.
This will help free up staff time to spend with patients, service users, or for the effective running of the system. It will help eliminate duplication, save unnecessary costs and make sure that we have the right data we need for the health and care system to work at its best.
The new Data Alliance Partnership, made up of organisations from across health and social care, will have a resolute focus on placing a minimal burden on the frontline. Its remit includes:
- accountability: working on behalf of the whole system when collecting and sharing data, and reporting on progress to the Secretary of State for Health and Social Care
- streamlining data collection: setting sharp, measurable targets for reducing the burden on frontline staff
- preventing ‘collection creep’: new collections may not be mandated if the Alliance’s Board does not agree to put them on the list
- encouraging data sharing: sharing data across the Alliance, using existing powers and in accordance with agreed criteria for different categories of data
- building for the long-term: agreeing an architecture which reduces the burden over time
- advocacy: communicating the work that’s being done, so colleagues can see the work being done and the value of the collections that remain
Our commitments:
- have in place a system-wide target for the rationalisation of data collections to reduce the time spent by health and care staff inputting and processing data for national use (by 2021 to 2022 and reviewed annually)
Harnessing safe and effective innovation
Remote monitoring gives health and care staff access to robust, real-time data to help inform their decisions to prevent illness and support recovery. Access to this data allows staff to monitor and provide high quality and safe care to people at home, freeing up time for them to focus on people who need the most urgent and complex care in a clinical setting.
This includes reviewing, where appropriate, when patients and service users would like to share data or validated insights they generate from technology, such as wearables and trackers, to safely share with clinicians.
Case study: digital cardiac pathway
The Barts Health NHS Trust Heart Centre is the largest cardiac centre in the UK, with 3,500 outpatient appointments and diagnostics weekly. Timely follow-up of patients enables identification of symptomatic recurrences or late complications. However, St Bart’s Hospital was experiencing delays in patient follow-up and low rates of medication dosage increases following a heart attack.
Bart’s deployed a digital system which helps patients and their clinicians to connect through virtual appointments using a computer or mobile phone, rather than face-to-face. The system captures biometric data including blood pressure, heart rate and Patient Reported Outcome Measures (PROMs) to intervene if needed by communicating directly with patients through the service.
Patients also have access to data, such as medical documentation and clinical notes, that supports the management of their long-term conditions at home.
The data involved helped to increase appropriate medication dosage levels from 11% to 88% of patients, follow up times were reduced, and data collected from continuous monitoring reduced appointment times. This all supported the experience, outcomes, and safety of the patients.
Our commitments:
- scale up our digital home care projects to support many more people with care at home, including those resident in care homes, improving their health outcomes (March 2022)
Automation at Kettering Hospital
The NHS AI Lab Skunkworks commissioned Foundry4 to undertake a discovery to determine the suitability of intelligent automation (IA) within NHS hospitals and trusts across England.
To support the COVID-19 pandemic response, Kettering General Hospital decided to automate some of their processes to free up staff time to focus more on patient care. Each hospital must provide a daily COVID-19 situational report with information provided by multiple departments. The team was able to build the automation in just 9 weeks, and it is estimated that over 4,400 hours of staff time will be saved every year to focus more on patient care.
Following this successful project, Kettering identified 2 further processes ideally suited for automation. The first was automating appointment bookings for GP referrals, speeding up the process so people are contacted sooner and saving nearly 1,500 hours of staff time.
The second is the ‘Unappointed Patients’ process where outpatient referrals that are no longer relevant (for legitimate health reasons) are removed from the system. This created a lot of ‘noise’ in internal systems and took up valuable appointment spaces from people who needed to book as quickly as possible, having been referred from primary care such as their GP. This process had a negative impact on staff motivation with the existence of the year-long backlog due to COVID-19. The automation helped Kettering gain an estimated staff time saving of 550 hours per year.
We will be taking learnings from these projects to help other NHS trusts use technology to free up staff time so it can be spent on higher value tasks.
3. Supporting local and national decision makers with data
Our vision
Leaders and policymakers have a responsibility to continually improve how the people we serve receive care, so leaders in every community will have up-to-date sophisticated data to make decisions and help the health and care system run at its best.
As a local decision maker, I will have data about our current service delivery and our local population to:
- plan or commission services to suit local needs, including areas that need support or improvement
- evaluate services and care, including safety risks and good practice
- manage vital management functions such as workforce planning
As a national decision maker, I will have:
-
information about the operation of health and adult social care organisations to:
-
support the needs of health and social care organisations through planning national programmes, and targeting areas that need support and to take action, intervening where there are serious failings
-
spot emerging risks and issues, and respond to national emergencies such as COVID-19
-
manage population health by understanding current health and care needs and predicting future ones
-
commission specialised services
-
-
data to develop policy and produce guidance and standards, improvement, and regulation
Why this matters
The insights and analysis that can be drawn from data are vital for local leaders to plan, commission and improve their services to best suit the needs of the populations they serve. If decision makers are using inaccurate information, for example an underestimate in those at risk of developing diabetes in their area, they will not be able to provide enough resources to support those individuals.
Similarly for national leaders, insights and evidence drawn from data gives them an accurate understanding of the health and care system to develop better policy and guidance and provide better oversight and national assurance. The shared experience of the coronavirus pandemic has only highlighted the critical role data has to play for these leaders to make decisions.
We have a huge amount of talented data analysts and data professionals on hand throughout the health and care system and local and national government. We must harness their skills to seize this opportunity and expand our use of data to drive continuous improvement.
Progress so far
-
NHSX has worked with NHS England and NHS Improvement to set up the NHS COVID-19 Data Store, to ensure the health and care system had the data it needed to manage extraordinary demand during the pandemic and to ensure that the system could make effective use of data for the benefit of patients and service users
-
NHSX created AnalystX on the FutureNHS platform to begin collaborating, sharing tools, methodologies and best practice – this is one of the largest online communities of practice in the world for data and analytical professionals working in health, with 14,000 members to date
-
Public Health England created the Fingertips Service to provide data across a range of health and wellbeing themes that supports commissioning to improve health and wellbeing, and reduce inequalities
-
NHS Digital has developed the GP Data for Planning and Research (GPDPR) collection. Its implementation will mean that data is collected once in a secure manner and used many times, resulting in a reduction in burden for the GP workforce. Once fully operational, the service will provide an efficient data feed ensuring that planners and commissioners can make informed decisions. Access to this data will only be granted for specific health and care planning and research purposes, to those who have a legal basis and legitimate need to use the data, with independent oversight of any data access requests. Its implementation later in 2021 will mean that data is collected once in a secure manner
Case study: NHS COVID-19 Data Store
To effectively respond to the COVID-19 pandemic, decision makers need access to accurate, real-time information. To achieve this NHSX and NHS England and NHS Improvement established the NHS COVID-19 Data Store, which brings together multiple data sources from across the health and care system in England into a single, secure location.
In a matter of months, the NHS achieved what would have taken years under normal circumstances. Using cutting-edge technology, data from the NHS COVID-19 Data Store is integrated into a single data platform where it is cleaned, harmonised and analysed to develop the single version of the truth that is needed to support decision-making and improve outcomes for patients at a time of immense pressure.
Various dashboards and tools have been developed within this data platform. These include the Strategic Decision Makers Dashboard which aids senior national figures to make strategic policy decisions, and the NHS Operational Dashboard which provides local and regional NHS leaders and local government officials with the information they need to make informed decisions. Analytical tools and products have also been developed, which play a key role in supporting ministers and system leaders to make effective, data-led decisions through effective use of data collection, analysis and insight generation.
NHS teams have been given access to cutting-edge predictive technology to help them save lives by forecasting COVID-19 hospitalisations. Using these forecasts, NHS trusts are able to plan how to use their available capacity for both COVID-19 patients and routine care and operations, with the benefit of advance knowledge of how the need to care for more or fewer patients with the virus might change over the coming one to three weeks.
Overall, the NHS COVID-19 Data Store has helped us to:
- understand how the virus is spreading and identify risks to particularly vulnerable populations
- proactively increase health and care resources in emerging hot spots
- ensure critical equipment is supplied to the facilities with the greatest need
- divert patients and service users to the facilities that are best able to care for them based on demand, resources, and staffing capacity
- support clinical research to understand more about the virus and the impact it is having
Taking this further
Integrating local care systems with a culture of interoperable by default
NHS England and NHS Improvement published a consultation on Integrated Care Systems (ICSs) in November 2020, which made clear that being an effective local system means being driven by quality data.
Traditional divisions between hospitals and GPs, between physical and mental health, between the NHS and council services, and between statutory and voluntary sector bodies created divisions of data across these organisations. This not only meant that people’s care has been disjointed, but that it has been very difficult for local and national leaders across health and care to effectively plan, commission, and develop policy.
As part of our long-term plans for the future of the health and care system, we are creating a more coordinated local approach, with ICSs at the heart of our plans. ICSs are new partnerships that meet health and care needs across an area, coordinating services across local organisations and planning in a way that improves population health and reduces inequalities between different groups. ICSs will lead on deciding how the data they hold benefits their populations. For example, Our Dorset has introduced the Dorset Care Record.This enables community pharmacists to access relevant information about patients, which can help pharmacists support their management of long-term conditions, preventing future hospital admissions.
ICSs will help the NHS join up data and delivery more seamlessly, working side-by-side with local government, third sector partners, and the wider health and care system to address long-term challenges. Each ICS will be expected to use digital and data to drive systems working, connect health and care providers, improve outcomes and put the citizen at the heart of their own care.
Our commitments:
- we will ensure the inclusion of adult social care providers (where they have digitised records) to integrate with basic shared record solutions across health (September 2022)
Building analytical and data science capability
During COVID-19, the analytical community mobilised to provide quick and robust analysis to inform decision-making including tracking the virus, predicting outbreaks, and managing bed capacity. The pandemic has been a case study in the importance of expertise in data and analytics, and the necessity of encouraging this talent in the future.
There are around 10,000 analysts in the NHS, as well as a government analyst profession across the DHSC, Public Health England (PHE) and Care Quality Commission (CQC), and analysts across primary care and adult social care. NHSX, NHS England and NHS Improvement have been working together to build on existing approaches to data and analytics, and by replacing traditional, high-effort, low-value processes. Through using machine learning and natural language processing, we can drive better predictive and insightful analytics to improve decision and policymaking.
We will also build the profile of the analyst profession more broadly across national policymakers and central government. This will include accreditation, training, career opportunities, status and pay to match.
It is important that analysts use data to harness insights that can be used directly for people’s care or to support front line staff. Clear data visualisations are an efficient way of enabling time-pressured staff to see the benefits of changes made based on the data they have provided.
The GOV.UK coronavirus dashboard has been a clear example where analysts are able to share their insights at scale across the system and the wider public.
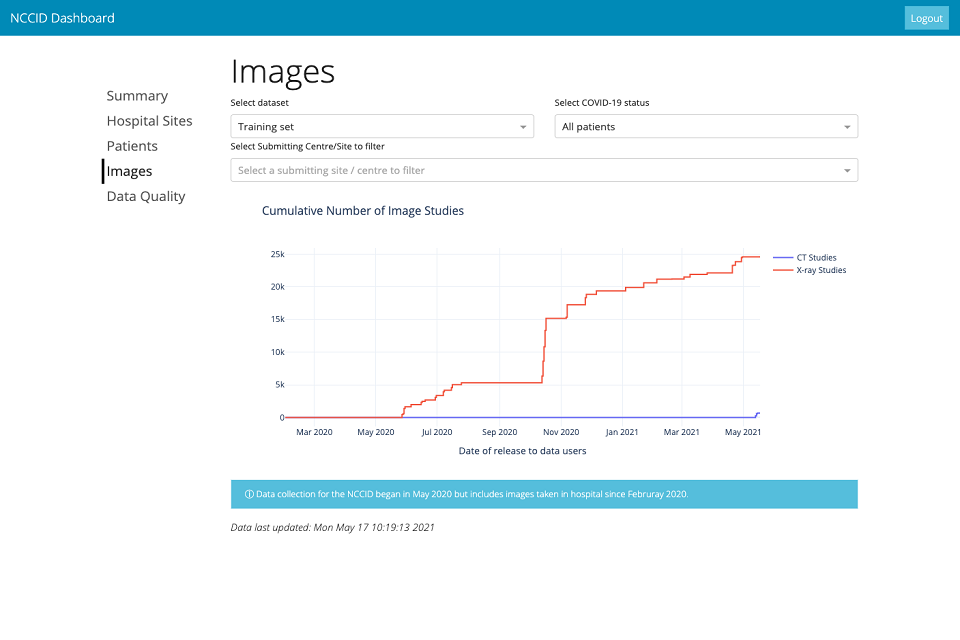
Additionally, the National COVID Chest Imaging Database (NCCID) dashboard provides an overview of the makeup of the data held within the database. This helps to improve the demographic representation of data used to train AI-driven technologies and provides greater assurance that they are tested on data representative of the UK population, whilst also potentially highlighting any gaps in the collection of data from different demographic groups. Additionally, the dashboard can compare demographic variables between the data available to train AI-driven technologies and the unseen data used to test them, allowing for a more robust evaluation of performance. The image below shows an example of the NCCID dashboard.
By providing high quality tools and training to analysts on visualising data, both health and care staff and the public are provided with information presented in a clear and accessible way.
By doing all of this, we are creating an analytical community that is a powerhouse for data science and modern analytical techniques, and that works openly and transparently. This community will forge new productive partnerships with academia to expand its innovative analytics and build capability on a massive scale.
Case study: AnalystX: connecting and empowering the data and analytics community
The COVID-19 pandemic was a galvanising moment for the analytical community. The NHS faced a surge in demand for sophisticated analysis and game-changing insights. The analytical community worked in unprecedented ways, collaborating across organisations and using tools and approaches that were previously confined to academia or other industries.
Building on this, NHSX and NHS England and NHS Improvement established AnalystX, a social movement of data professionals and analysts to provide support to help health and care teams in England to battle the pandemic. This network now has 14,000 members, committed to common principles of adaptability, innovation at pace and working in new ways.
To enable collaborative working at scale, we leveraged the already flourishing FutureNHS platform and created a workspace that is a mixture of 4 components:
-
community-curated and indexed data and analytical resources such as dashboards, web applications, evidence syntheses and insight reports
-
vibrant discussion forums to regularly exchange ideas, form virtual cross-organisational teams and come together to solve a common challenge
-
an analytics market exchange to match requests for support with surge analysts and relevant partners within our ecosystem
-
an analytics champions programme with a focus on developing the analytical leaders of the future
Data skills are not just important for analysts. These skills are valued in all roles and at all levels, and so we need to promote these skills across our health and care system. Just as we’re encouraging digital skills across organisations, we need to encourage data skills across the whole workforce, and make sure analytics expertise is represented at board level.
The pandemic response has created a lot of momentum, and we need to build on it.
Our commitments:
- we will develop an analyst workforce observatory, including an annual census to inform how to better harness the professional skills of analysts and data scientists, and support their professional learning and development (March 2022)
- we will develop an online Analytics Hub, working with AnalystX, to share, promote and endorse training, events and other resources (2021)
- we will grow the AnalystX community and build the team of future analytical leaders through a champions programme (March 2022)
- we will pilot a data and analytics accelerator (March 2022)
- we will develop and roll out a unified set of competency frameworks aligned to the government Analysis Function skills (2022)
-
through the ‘Developing Data and Analysis as a Profession Board’, we will:
- agree frameworks, guidelines and policies to operate in
- build the ecosystem of the profession through communities of practice (local, regional, national and virtual)
- signpost and provide development opportunities for analysts (Ongoing)
Working in the open
Public services are built with public money, and so the code they are based on should be made available for digital pioneers across the health and care system, and those working with it, to reuse and build on.
Analysts should be encouraged to think from the outset of a project about how work can be shared, or consider ‘coding in the open’ for example, through use of open notebook science. This will include sharing of technical skills and domain knowledge through sites like Cross Validated and StackOverFlow, and sharing code and methodology through platforms like GitHub, will build high quality analytics throughout the system
Our commitments:
- we will begin to make all new source code that we produce or commission open and reusable and publish it under appropriate licences to encourage further innovation (such as MIT and OGLv3, alongside suitable open datasets or dummy data) (end of 2021)
Sharing data for wider purposes
The ability to see the current position and trends in health and social care data and use analysis to understand the drivers of those trends is critical. This allows us to analyse the effectiveness of previous actions that have been taken, or what challenges and opportunities the system faces.
Currently, there is a lack of clarity about when personal information can be shared to support the health and care system. This can create a barrier to the effective sharing of information for work vital to the operation and improvement of the health and care service such as such as commissioning and planning services for local communities, analysing data to develop policies to help children with chronic illnesses, and having the right information for risk management.
Not having data for these essential functions has an impact on us being able to continually improve services so that our citizens are being given the best care possible. Additionally, this lack of information acts as a barrier to effectively identify, prepare for, and respond to future diseases. This must change.
Our commitments:
-
we will use secondary legislation in due course to enable the proportionate sharing of data including, where appropriate, personal information for the purposes of supporting the health and care system without breaching the common law duty of confidentiality (ongoing)
-
we will work closely with stakeholders and the public to make sure that these changes are implemented transparently and that appropriate safeguards are in place (ongoing)
Collaborating with wider partners
Government has long understood the importance of data to provide effective services for everyone in the UK. The government’s National Data Strategy sets out how best to unlock the power of data for the UK. It highlights the importance of using data for the benefit of delivering complex public sector services that support millions of people across the UK every year. It notes that public services are increasingly interconnected and so need to work better together to deliver for our citizens.
If we are to shift the health system much more into a service focused on wellbeing as well as illness or to effectively respond to emergencies, we need to appropriately use all the data we have to deliver the best services and outcomes possible.
For example, a person might experience an acute mental health issue and be hospitalised for it. If they do not have housing available after their treatment, it is not safe for them to leave the hospital. This may keep them in hospital for longer than is necessary, impacting their health, employment and access to community support. It can also entrench existing inequalities for individuals of specific communities or backgrounds. As local authorities and Jobcentre Plus manage housing and welfare support, it is imperative in these situations that all these public service organisations can share data to keep the person safe.
These wider factors that impact people’s health and wellbeing are imperative to get right so that we support all our citizens. Supporting disabled people and people with health conditions to enter or to stay in work when they are able to is an important part of this, and why we created the joint Work and Health Unit between DHSC and the Department of Work and Pensions (DWP). By safely and securely sharing appropriate levels of data between these departments, we can support individuals and work to improve their wellbeing and health outcomes.
The Shielded Patients List, part of the COVID response, is a good example of how organisations such as NHS, NHS Digital, local government, adult social care, and the Ministry for Housing, Communities and Local Government (MHCLG) can work together to share data to keep people safe.
Children and young people’s social care is led by the Department for Education (DfE) and so it is important for us to work together to provide them with the best possible outcomes. For example, children and young people only make up 25% of our population, but the number of children with complex health and special educational needs that require social care involvement is increasing. We need to make sure that they are kept safe and supported through their childhood across health and care, and when they transition into adult social care.
Case study: sharing information for children and young people’s care
Providing appropriate and safe access to data across health and social care is imperative to deliver the best care to the populations we serve. This is no different for ensuring coordination and safety of care for individual children. For example, providing certain information about a child (such as education and social care records) can help health staff make the best decisions possible about their care.
However, children and young people’s healthcare is provided by the health service and led by the Department of Health and Social Care (DHSC). Children’s social care is led by the Department for Education (DfE) and delivered by local authorities across England. This means that we must appropriately share data across organisational boundaries to make sure that they are kept safe. It also helps us to integrate health and education outcomes, for example, for children with Special Educational Needs and Disabilities and for those with long term conditions such as epilepsy or diabetes.
Eight Local Authorities in North West London developed the Whole Systems Integrated Care (WSIC) dataset, which provides data on patients to support their individual care in primary, community and hospital settings. Out of over 2.3 million people included in the programme, there was information on appropriately 400,000 children and young people. The data was used to study Adverse Childhood Experiences (ACEs) through a ‘Rising Risk’ data dashboard. This information will be used on a pilot project from summer 2021 to link children’s educational and social care data held by Westminster and Kensington and Chelsea local authorities.
As a Consultant Paediatrician working closely with local GPs, WSIC has already improved the coordination and quality of care I can deliver – for example by flagging those infants who are high users of hospital emergency care; these infants are offered a paediatric review which usually identifies and addresses underlying concerns and stops the unplanned use of A&E. Additional linkage to education and social care records will transform our ability to safeguard vulnerable children, by ensuring that clinicians have the information they need to make the right decision for each child.
Dr Mando Watson, Consultant Paediatrician, Imperial College Healthcare NHS Trust
In addition to clinical care, WSIC provides a unique research resource as the largest integrated dataset of its kind in Europe. Researchers at Imperial College London are using the data to study a wide range of questions. This includes refining Connecting Care for Children which is a pioneering new model of integrated care for children and young people, and improving care and outcomes of children and young people with asthma.
We must also recognise that not everyone receives care within traditional health and care settings. For example, those in custody or detention still require care so health and care data must be safely and appropriately shared with the Ministry of Justice to ensure that the right healthcare services are commissioned to meet the needs of people in prison.
It is also important that we have a UK-wide data focus and response, making sure that people have confidence that the health and care system will support them, regardless of where they live or work in the UK.
This means making sure that health and care data can be shared safely and effectively across the UK to support individual care and to improve outcomes for people across the UK. This will include working with officials across the devolved administrations, noting the devolved nature of health and care policy, and building on the work of units such as the Joint Biosecurity Centre and the newly established UK Health Security Agency. This will also help us collaborate to solve public health issues, improve disease surveillance, and to overcome any behavioural or structural obstacles to appropriate data sharing across our respective health and social care systems.
Our commitments:
-
we will work across central government, including with colleagues in MHCLG, DfE, the Cabinet Office, MoJ, DWP and across the devolved administrations to improve appropriate data linkage to support people’s health and wellbeing (ongoing)
-
our public health agencies will draw on multiple data sources to gain new insights into the public’s health, with quicker access to high quality health intelligence to inform improved decision-making and responses to crises (ongoing)
4. Improving data for adult social care
Our vision
Service users and their carers will have high quality, timely and transparent data to improve outcomes, and can easily access to help them make choices about their care.
As an adult social care service user, I will:
-
have access to my own data and be able to share information with everyone supporting me, including friends and family, so they have the full picture about my needs and preferences
-
have access to data on the nature and quality of local care services so I can make better informed choices about my care and preferences
As an adult social care professional, I will:
-
have access to information about the needs of those I care for and the care they have received across the system, so I can provide seamless person-centred support
-
have operational and service-user-level data to support smoother transitions between NHS services and social care, and to plan future services
-
understand what technology is available to collect better data to improve care, understand people’s needs, and plan and commission services
-
be able to easily and securely record, access and share information about those in my care, making the best use of new technology
Why this matters
By harnessing adult social care data, we can provide care that maintains people’s dignity and helps them live independently for longer. It also helps children and young people transfer from the children’s social care system led by the Department for Education (DfE), to the adult social care system led by the Department for Health and Social Care (DHSC).
Adult social care staff need to be able to safely and confidently access the information they need, whenever and wherever they need it. Staff and service users need to be relieved of the burden of chasing health updates, discharge summaries, and accessing locally held paper records. Instead they need to be enabled to use data to make better decisions, such as engaging the most appropriate physiotherapy option for an individual service user, delivering more personalised care that focus on their preferences and needs.
Good and timely data is needed about the care being provided. This includes information on quality, costs and workforce requirements which can then be used to plan people’s care services, provide information to help people and their carers access information, and for planning and commissioning services. This is essential to make sure that the social care system is working for the people that use it, helping them lead more fulfilling lives with better outcomes.
Service users and their families should not have to repeatedly provide information in either health or social care settings. They should only have to give their details once, including when moving between care and health settings, so that it can be safely seen by everyone who is caring for them.
We want to work with local authorities and care providers to make sure we all have the technology and systems that help us share data and improve the experiences of people who need care and support. Technical and data standards will be a key underpinning factor in enabling a more seamless flow of information, as well as making it easier for national and local leaders to use the data to improve services.
Progress so far
- we published, in the health and care white paper, our plan to improve data collection, with an enhanced assurance framework, and improve accountability within the social care sector
- we have created an initial use-case blueprint through the Yorkshire and the Humber Local Health and Care Record Exemplar programme of what the future model of care could look like for cancer services, with a single integrated care record bringing together data from across health and social care
- we have been enabling GP-Connect to support appropriate staff (registered nurses) in care provider settings to have access to information held within GP systems. Authorised staff are able to view appropriate levels of information from GP records within their own local care management system
- for regional and national level data requirements, we are refreshing the Adult Social Care Outcomes Framework. The Association of Directors of Adult Social Services (ADASS) has contributed to the initial work. This will help us to understand what data we need to support high quality services for everyone.
- we have collected data from providers via the Capacity Tracker tool and developed an adult social care COVID-19 dashboard, allowing this and other critical data to be viewed, in real time, at national, regional and local levels by national and local government
- we have begun to collect client-level data from local authorities through a voluntary collection process. This will give us more detailed adult social care data, which we can then link to health datasets to better understand outcomes for people in our care
Taking this further
Improving access to information for adult social care providers
At present, very few adult social care providers have online access to information about the people in their care. Research by NHS Digital suggests 71% of the sector has no digital access to people’s medications information. Approximately 30% of social care providers are partially digitised with a further 30% still using entirely paper-based systems, which means approximately 15,000 CQC registered care providers have limited or no access to basic digital infrastructure, for example internet connections and devices. Care providers who are not fully digitised cannot access digital services; we will work with the sector to help providers to improve their internet connections and access to devices.
The COVID-19 pandemic has reinforced the need for access to regularly updated and detailed data to improve the development of policy at a local, regional and national level and to identify emerging issues. It exposed large gaps in social care data and inconsistencies in the quality of this information, such as workforce absences, PPE levels and overall risks. The Office for Statistics Regulation’s 2020 report, adult social care statistics in England, further highlighted that the social care system would be assisted by more comprehensive and better data.
Local authorities only collect data about services that they fund, leaving a gap in information about people that pay for their care themselves. Further, many existing data collections are annual, meaning that information is often not up to date which stops us from identifying problems and responding in real-time.
The project underway to collect client-level data from local authorities will deliver positive changes to the way local authorities and central government can understand the pathways and interactions of clients within social care. This project will also link client-level data from local authorities to health data meaning pathways between health and care can be understood – and improved in many ways – significantly contributing to the aim of having fully integrated health and care data. Work underway to develop an enhanced assurance framework and improved data collection will improve accountability within the social care sector.
Case study: data support planning for adult social care
As the sector adopts digital technologies, the collection and sharing of data will become increasingly automated, helping make it more accurate and less resource-intensive for staff to collect. It will equip everyone involved in the care sector with the information needed to plan, evaluate and improve care services.
The adult social care Capacity Tracker is an intervention which proved essential during the COVID-19 pandemic in responding to a fast-moving public health emergency. It is an example of how giving people involved in planning services the right data leads to better decision making and improves the quality of our health and care system.
It allows care homes to share their vacancies in real-time, meaning hospital discharge teams and other health professionals can rapidly search availability throughout England, reducing the need to make multiple calls to identify locations with vacancies.
It was updated to accommodate the latest demands of the pandemic, for example to identify PPE levels, COVID-19 positive residents, and then later on to cover vaccination data.
Care colleagues welcomed the support it provided at a difficult time:
The new Business Continuity features of the Capacity Tracker enabled the local authority and clinical commissioning groups to identify those providers who were in need of the most support. Those providers who had identified themselves as Red or Amber are contacted first by the contracts team in order to identify and understand the challenges being faced by these providers.
Kirklees Care Homes
We must ensure that adult social care-related data development and technology work at a national level is aligned to the delivery of shared objectives, has good collaboration; and that there is a shared understanding in support of system reform.
Our commitments:
-
collect client-level data rather than aggregate data from local authorities to ensure that we have regular and comprehensive data to enable person-centred, sustainable innovation for adult social care (2023)
-
DHSC will develop a plan for sharing data with local authorities that looks beyond the pandemic, building on the learning from the COVID-19 response (ongoing)
-
provide digital skills frameworks to identify what good digital working looks like in practice, supported by the delivery of training opportunities to improve the data and digital literacy of the adult social care workforce (by March 2022)
Integration of health and social care data
Information about people’s health is usually received by social care providers through hospital discharge summaries, which are often missing, incomplete, or need a further conversation with the GP. To ensure better integration of health and social care, we want to make sure that data is only collected once and flows better across health and social care so that services can meet the needs of users without multiple conversations.
The Digitising Social Care Records programme will support social care providers to capture real-time information, view relevant information from the NHS record and enable more effective quality management. It has the potential to transform care outcomes and provides greater personalisation of care planning that focuses on the individual. Digital Social Care Records that can interoperate with Shared Care Records means care workers are equipped with the information they need to deliver integrated care.
Our commitments:
- work with care providers to accelerate the adoption of digital social care records through the NHSX Digitising Social Care Record programme for better access and interoperability with Shared Care Records (2024)
- we will introduce legislation in due course to require information from all adult social care providers (both public and private), so that we can build a better picture of the delivery of adult social care services across England (ongoing)
- establish a data framework for adult social care setting out what data we intend to collect and the standards used to collect it so we know we are getting the data we need (March 2022)
- work with NHS Digital and NHS England and NHS Improvement to continue to build the foundations needed to support care providers in accessing the information they need to deliver high quality care for people (March 2022)
- we will continue to promote NHSmail (or other appropriate services that meet the government’s secure email policy requirements) to all care providers to enable secure information sharing with colleagues and with the NHS (2021 to 2022)
Case study: developing a minimum research dataset for care homes
A 4-year National Institute of Health Research (NIHR) funded research study is aiming to enhance how researchers and health and social care services can use existing data to improve the care and quality of life for care home residents, families and staff.
The £2.2 million DACHA study (Developing research resources and minimum data set for care homes’ adoption and use) is led by the University of Hertfordshire. Researchers are aiming to address the need to develop robust systems that support how all the different services and individuals – such as care staff, NHS professionals, family, regulators, and social services – work together for residents’ benefit.
The study team is reviewing how current health and social care systems work and exploring the evidence on how to integrate data and test what a minimum dataset would need to be the key resource for all those working in and for care homes. The findings have the potential to deliver a step-change in how we understand the needs of people living in care homes, and this could be a resource that supports the provision of high-quality care across the country.
Expanding the use of care technologies
We want individuals to be able to use their own health and care data to help them manage their needs. This will support them to live at home independently for longer and more easily in their communities.
There are some compelling examples of the data from assistive technologies (such as room sensors, activity monitors and alarm systems) providing 24-hour background support while enabling the individual to live independently and giving carers and family members reassurance about their wellbeing and safety.
The Local Government Association has worked in collaboration with NHS Digital to grant-fund innovative projects using technology to collect and share information. These have included work on apps in Southwark Council to prevent and manage falls by older people in community settings and in North Somerset Council to improve hydration for care home residents, while work in Kirklees Council has focused on developing a self-service care account to give more control to their clients through access to their data and information 24 hours a day.
Our commitments:
-
we will engage and collaborate with a range of partners, including Local Authorities, care providers (tech-enabled or otherwise), innovators, and the wider health and care system, to build strong relationships and:
- improve their confidence in the commissioning and purchasing of care technologies that support integrated working
- support the creation of a vibrant CareTech marketplace
- spread the use and adoption of these technologies and evaluate how the data they generate can be used to improve the quality of care
This will ensure that we continue to focus on the challenges and opportunities that will have the greatest impact in driving digital transformation in social care. (2021 to 2022)
5. Empowering researchers with the data they need to develop life-changing treatments, models of care and insights
Our vision
Our researchers can only deliver results based on the information available to them, so they will be able to safely and easily access data to provide innovative solutions to health and care issues for the benefit of every citizen in every community.
As a researcher or analyst, I will have:
- easy ways to find people to join research studies on areas such as developing new treatments, vaccines or diagnostic tools to support patients and service users
- safe environments to analyse people’s data so that I can explore hypotheses or identify new areas for research, through access to wide-ranging study or clinical data including:
- data from the NHS and social care such as clinical data from diagnoses and outcomes for treatments
- rich genetic and genomic data through Genomics England, UK Biobank, and Our Future Health, alongside one of the world’s most comprehensive collections of disease registries
- individual-generated data from monitors, wearables and trackers
- data that allows targeting research at those who are most at risk for poorer health, that is to investigate health inequality
Why this matters
The UK is a world-leader in clinical and healthcare research, and we have committed to further strengthening our role and our contribution in the coming years. We have an exceptional health and care research ecosystem including the NHS, world class universities and research institutes, the National Institute for Health Research (NIHR), a strong life sciences sector, and medical research charities.
We also have the unparalleled health dataset held by the NHS, offering the potential for a unique view of a large and diverse population. We have to close the gap between the lab and the delivery of people’s care and encourage research participation and innovation across the system. By increasing the scale of the datasets available to researchers and enabling more assets to be linked, while maintaining the necessary safeguards, we can create even richer data insights. This provides us with huge potential for new clinical options and improved care pathways, as shown using dexamethasone in treating COVID-19.
Research can also inform new care delivery approaches and techniques. Staff will be able to personalise the care they offer, informed by data-driven models that help identify the optimal treatment for an individual, learning from the experience of others. We will need to use data-driven models to monitor and study early signs of disease and drive our prevention strategies.
Collaboration is also imperative to ensuring we reach our research goals. UK Research and Investment (UKRI) and its Medical Research Council (MRC) have provided funding for some of our most successful programmes, including UK Biobank, NHS Digitrials, Global Alliance for Genomics and Health (GA4GH), and Our Future Health. Health Data Research UK (HDR UK), the national institute for health data science, has already undertaken a significant amount of work to unite the health data ecosystem, which helps us capture a clear picture of the current and future research landscape.
Our mission is for patients to benefit from new therapies, technologies and better more personalised care, and a world-class life sciences sector working closely with the NHS.
Progress so far
During the COVID-19 response, we have seen much closer cooperation and joint working between national and local organisations.
There has also been unprecedented collaboration across academic and public health services which has transformed the use of data at national level. COVID-19 has shown us what can be achieved when the right access frameworks, like the COPI Notices, are in place and when we work together across boundaries.
-
NIHR BioResource (£37.5 million) draws together over 130,000 genotyped and phenotyped volunteers, with and without health conditions, who have agreed to be approached to participate in research investigating the links between genes, the environment, health and disease
-
we have enabled rapid recruitment into COVID-19 vaccine studies through the NHS Vaccines Permission to Contact Tool with more than 450,000 individuals signed up to the registry
-
we have provided funding (£1 milllion) to the Global Alliance for Genomics and Health to develop standards and policies for sharing genomic and health-related data
Case study: UK Biobank
UK Biobank is a large-scale biomedical database and research resource, containing in-depth genetic and health information from half a million UK participants. It has led to several scientific breakthroughs to improve human health including:
-
a University College London (UCL) study into factors increasing risk of dementia. Researchers were able to study participant blood samples to elucidate how genetic makeup affects risk. The diverse participant pool has enabled the research team to explore ethnic differences in dementia risk
-
research into the hypothesis that ‘good’ cholesterol may help in the fight against sepsis which causes 11 million deaths worldwide each year. Researchers were able to access genetic data from Biobank to provide critical information for the study
This data has proved especially valuable during the COVID-19 pandemic. The integration of data across a wide range of medical records has enabled researchers to identify individuals diagnosed with COVID-19 across the full spectrum of disease severity.
Coupled with the genetic and lifestyle data already available, this rich dataset helps researchers to understand the extent to which genetics, lifestyle and underlying health conditions affect disease severity, and recovery.
Case study: National COVID-19 Chest Imaging Database
The NCCID is a centralised UK database containing x-ray, computed tomography (CT) and magnetic resonance images (MRI) from hospital patients across the country to support a clearer understanding of the COVID-19 virus long term and develop technology which will enable the best care for patients hospitalised with a severe infection.
It is a unique resource for researchers to analyse the impact of COVID-19 on patients and a way for new artificial intelligence (AI) tools to be trained on a powerful real-world dataset. With over 40,000 images from over 20,000 patients in England, Scotland and Wales, researchers will be able to apply machine learning models in a way not previously possible in the UK.
Going forward, the NCCID will continue to provide a valuable data resource for the development and training of AI technologies. The NHS AI Lab will work with more NHS hospitals and trusts to share data and expand the database. This will provide access for other researchers and AI companies to safely train their algorithms.
The NCCID has also demonstrated that, despite the present fragmentation of data collection across different institutions and initiatives, the technology and research communities are ready to work towards a stronger data integration coordinated by NHSX. The NHS AI Lab is now using learnings from NCCID to inform a programme of work supporting the innovation to deployment pathways of AI technologies as part of the development of a new AI medical imaging initiative.
Taking this further
Providing safe and secure data for analysis and research
To provide reassurance to the public that those entrusted with their data are keeping it safe, we are also looking to the development of new technological advances in how data is collected, stored and analysed. Multiple datasets can be linked within a secure environment in a way that enables appropriate access to a vast array of data whilst still protecting the privacy of individuals.
The system will look increasingly to trusted research environments (TREs) which are secure spaces where researchers can access sensitive data without breaching privacy. In-depth analysis can be undertaken on rich datasets without identifiable information ever being seen by researchers and analysts.
Case study: OpenSAFELY
OpenSAFELY is a new secure analytics platform for electronic health records in the NHS which was established at the beginning of the emergency to deliver urgent results. Working on behalf of NHS England and NHSX, it is a collaboration between the DataLab at the University of Oxford, the Electronic Health Records group at London School of Hygiene and Tropical Medicine, The Phoenix Partnership (TPP), EMIS and other electronic health record software companies, who already manage NHS patient records.
The platform uses a new model for enhanced security and timely access to data: data stays in the secure environment in which it is stored for individual care. It does not involve the transfer of large volumes of pseudonymised patient data outside of the secure environments managed by a GP IT systems supplier. It allows the creation and application of models to patient-identifiable data without moving the data.
Trusted analysts run large scale computation across near real-time pseudonymised patient records, enabling a range of major breakthroughs in COVID-19 research. For example, it identified key factors related to COVID-19 death included being male, older age, having uncontrolled diabetes and severe asthma.
A particular characteristic of the OpenSAFELY operation is the use of modern open working methods. This involves sharing all analytic code and development insights, which supports the accelerated development of analyses and other tools by groups with other datasets. This approach of sharing code has many benefits including increasing reproducibility, providing an opportunity for quality review, and good practice in terms of transparency and working in the open. By making this code available, the opportunity exists for review and this can help to engender greater public trust in the research findings and analysis derived from the data.
NHS Digital’s TRE for COVID-19 links appropriately with regulatory and research systems. It aims to give researchers across health and care the ability to review data at speed, streamlining research processes for quicker results whilst maintaining confidentiality.
HDR UK has been working with NHSX to develop standard operational and governance approaches to trusted research environment (TRE) through the TRE Green Paper. However, there is also a proliferation of TREs. To ensure we are making the most out of these environments, we must continue to examine how they operate and are governed to ensure they are fit for the future.
Our commitments:
-
create partnerships between academic researchers and frontline analytical teams to enhance the exchange of skills and knowledge (ongoing)
-
produce a consistent and clear glossary of terminology and legal definitions working with the research community to alleviate confusion and improve the quality of research access requests (October 2021)
Sharing data for research
Research is critically important in developing the medicines, treatments, technologies and scientific insights of the future, so we will need to make sure researchers can access the data they need for their work, while also adhering to clear and robust legal safeguards, and preserving privacy.
We have seen the positive impact this can have during the COVID-19 pandemic, with COPI notices giving the health and care system the ability to easily share and access data to help with the response. We have also seen the benefits of the research community developing vaccines and treatments for, and enhancing our understanding of, COVID-19. However, the research community is still often hampered in its efforts to maximise the opportunities of health and care data.
Even though legislation already provides ways to access identifiable data for research subject to approval, researchers are often seen as operating ‘outside’ of the system. This makes it more difficult for researchers to access the information they need. A misunderstanding of information governance can lead to a researcher with justified purposes being denied access to the data they need; an issue that may be compounded by the complexity of the number of organisations providing access to data, each with slightly different access requirements and approvals processes and interpretations of the law and guidance. This is something we need to change.
To help us address these current challenges and barriers, the Secretary of State for Health and Social Care has asked Dr Ben Goldacre to conduct a rapid review into the more efficient and safe use of health data for research and analysis for the benefit of patients and the healthcare sector, including how access to data can be better facilitated.
The review aims to gather real-world stories of the impact of data and how it can be shared and used, and conversely the impact when not shared, as well as common blockers to using health data for research and analytics. The process has included interviews, open sessions and deep dives, and the review will report its findings and recommendations in the next few months.
Alongside this review, we will invest in improving the quality and accessibility of at-scale data assets that make the most of the UK’s health and care data. These will support clinical research and data-driven innovation, benefiting patients and the NHS, as well as generating economic growth. In particular, we will deliver more efficient and effective clinical trials by ensuring data is used to support the design, recruitment, and follow-up of trials. This will reduce unnecessary burdens on the front-line workforce and ensure as many people as possible have access to cutting edge trials that might benefit them.
Our commitments:
-
consider and, where appropriate, act on the findings and recommendations of the Goldacre Review into the use of data for research and analysis (end of 2021)
-
progress towards creating at-scale data assets that bring together the different types of health data to develop new tools for prevention, diagnostics and clinical decision-support (2023)
-
progress towards bringing together genomics data assets, and work with NHS England and NHS Improvement to ensure genomic data generated through clinical care is fed back into patients’ records (2023)
Encouraging clinical research
As set out in the UK vision for clinical research delivery, clinical research is the backbone of healthcare innovation: it is the way we improve the prevention, detection, diagnosis and treatment of disease. Health data is critical to deliver faster, more effective, and innovative clinical research.
Our ambition is to ensure the UK has the most advanced and data-enabled clinical research environment in the world, capitalising on our unique data assets to improve the health and care of patients across the UK. Building on digital platforms such as NHS DigiTrials and other key infrastructure, we will be able to:
-
rapidly assess the feasibility for specific clinical studies, utilising intelligence on patient populations, disease prevalence and site capacity and capability, and speeding up key research processes
-
improve our ability to identify and approach patients who may be eligible for specific studies, increasing access to research for a greater diversity of patients, and ensuring that health research and innovation delivers for everyone
-
monitor the progress of patients that agree to take part, reducing the administrative burden of research on frontline, clinical and research teams
-
deliver new and innovative research designs to answer questions in new ways and enable studies in cutting edge fields, such as genomics, cell-based therapies and digital therapeutics
Using such digital platforms, we also have new opportunities to connect with and involve the public, patients and service users in shaping research. Success at recruitment and retention has declined over recent decades, and now is the time to reverse that trend.
Case study: NHS DigiTrials RECOVERY Trial
This trial was aimed to find treatments for those hospitalised with severe COVID-19. As an Urgent Public Health Research study core funded by NIHR, RECOVERY was set up through the University of Oxford in a matter of days. Within weeks, over 10,000 patients from 176 NHS hospital organisations were enrolled, with data being tracked and analysed. Since then, over 39,000 participants have been involved.
By providing centrally collected and curated data on a weekly basis to track progress and outcomes of participants, NHS DigiTrials made the scale of this trial possible. The data was drawn from extracts from routine electronic health record data and NHS DigiTrials supported rapid access to new COVID-19 specific data. This removed the burden on the NHS ‘front line’ to field additional data requests and enabled the trial team to make rapid decisions.
Within 100 days, the trial identified the world’s first coronavirus treatment proven to save lives: dexamethasone. The results were announced on 16 June 2020, adopted into UK practice later the same day and included in new US guidelines within 2 weeks. This treatment has since saved 22,000 lives in the UK and an estimated one million worldwide.
‘Platform’ and data-enabled trials like this have the potential to be used outside of a pandemic, making it faster and more efficient to find safe and effective treatments for widespread and common illnesses like cardiovascular disease. They also open up the opportunity for trials of different treatments to run simultaneously, all within a common trial framework and using routinely collected NHS data.
Through the NHS DigiTrials programme we can reduce the cost of bringing new drugs to the NHS and collaborate with clinical trialists to find and recruit the participants they need to make them successful.
We will work closely with the research community to embed these principles further, so we can make research as accessible, streamlined and safe as possible. While doing this, we must continue to explain to the public how their data is being used to support research through increasing their engagement and involvement.
Our commitments:
-
build on platforms such as NHS DigiTrials to enable and support best use of data and digital tools in study feasibility, identification and monitoring of research participants to enable faster, more efficient and effective clinical trials (March 2022)
-
publish the first implementation plan to progress UK priorities for clinical research as set out in the UK Vision for Clinical Research Delivery, including a key theme on research enabled by data and digital tools (2021)
-
working with other countries and G7 members to facilitate the rapid generation of compelling evidence through randomised clinical trials of treatments and to enable timely and decisive action on the findings in this pandemic and for future clinical trials (2021)
-
working with other countries and G7 members to develop a framework to share testing methods and materials would ensure that the data generated could more readily be compared in vaccine development (2021)
6. Helping colleagues develop the right technical infrastructure
Our vision
To maximise the efficiency and effectiveness of our infrastructure, we will ensure the data architecture underpinning the health and care system can easily work together to make better use of data, no matter where it is kept.
As a Chief Technology Officer, technical architect, commissioner, provider or standards lead, I will:
-
have quick access to the information I need to plan and run my systems effectively
- drive interoperability across the health and care system by:
- having clear and open standards making it easier to share data safely and efficiently
- understanding the wider data architecture so I can build and buy the right systems
- have clear cybersecurity guidance to make sure that my systems and the data held within them is as safe as possible
Why this matters
Data-driven technologies have so much potential for our health and care system, but we can only unlock this potential if we have the right technical infrastructure in place. Data is a shared asset, and as we break down the organisational silos that hold data, we must rebuild them based on the foundations of a unified architecture, open standards and better interoperability. And we must give those leaders in health, adult social care, and other related public services such as housing and education, who understand cyber risks the clear cyber standards they need to keep that data as safe as possible as those risks change over time.
We want to reshape our legacy systems and platforms into smaller discrete services by creating national platforms that can talk to each other and work together, and so can easily be used to access and share data. This will avoid delays in diagnosis, prevent tests from being repeated unnecessarily, and get people the treatment and care that they need.
Progress so far
-
requiring use of the NHS Number for transfers of information, which has allowed us to link information to people in a consistent national way. We have developed a number of services to support access to the NHS Number across health and care
-
creating the CareConnect profiles, a set of Fast Healthcare Interoperability Resources (FHIR)-based models and Application Programming Interface (API) specifications which facilitate the exchange of patient, allergies, procedures, problems, observations, encounters, medications and immunisations data
We already have a number of widely-used national components and services which provide us with learning to build on. Some broad examples include:
-
Summary Care Record application: a national portal enabling access to a view of core information from the GP record like medications and allergies
-
2 information services give clinicians a way of notifying and identifying children and young people at risk, for Child Protection (CP-IS) and Female Genital Mutilation (FGM-IS)
-
Personal Demographics Service: a national master demographics service used across the NHS to access information such as the NHS Number
-
Electronic Prescription Service: a national service to support efficient and secure sending of prescription data from general practice to pharmacies
Progress on data standards work across government, with learning shared across health and social care, includes:
-
the Data Standards Authority (DSA), which establishes standards to make it easier and more effective to share and use data across government
-
the Government Data Quality Framework, which provides a consistent approach to managing data quality across government
Taking this further
Modernising our data architecture
Currently, there are many legacy systems and platforms used by health and care staff. The Topol Review found that between 15% and 70% of a clinician’s working time can be spent on administrative tasks. As well as this, 27% of doctors who responded to a survey by the British Medical Association (BMA) in its Vision for NHS IT report said they lost more than 4 hours a week because of inefficient hardware or systems. We must use the best data-driven technologies to support our staff with their life-saving work.
By moving towards smaller discrete services built to work with national systems, we can improve interoperability, reuse, and agility across health and adult social care to access and share data. This requires us to think of the health and care system as a platform.
Our goal is a modern architecture in which data can be accessed real-time through APIs via a national gateway. This goal cannot be achieved when the data is held in silos within individual electronic patient record (EPR) systems. Modernising the data architecture represents a significant task and we will work with trusts and ICSs to understand any impact this may have on current plans.
Set out below are our new data architecture principles that set out the rules and guidelines that must be followed when we create or adopt new services that work with health and care data. Our principles answer the key questions:
- how will we use data?
- what data do we have and what data do we need?
- where do we store data?
- how do we manage data?
- how do we integrate data across the system?
Data architecture principles
1. All data will be validated at the point of entry to improve data quality
Poor quality data leads to many downstream problems. It can have serious impacts on the quality of care a person receives and create extra work for our colleagues in health and care. All of our national platforms will automatically validate data at the point of entry to improve data quality and prevent poor quality data being used within our health and care system. Where necessary, we will provide validation services, like address lookup, using APIs to allow systems to improve the quality of data at point of entry.
2. All data will be made discoverable
Right from inception, data needs to be seen as a shared asset. Using well-defined APIs and metadata to create a catalogue of the data will help it be easily discovered and reused across all appropriate settings, where information governance allows. Every team that creates new data assets must adhere to this principle.
3. Data will not be duplicated
We will not allow programmes or teams to simply copy data from one application or system to another. This approach has led to duplicate datasets which mean more silos and more time for maintenance and development. When data is stored in disparate repositories, people may unintentionally duplicate it which can cause confusion about which dataset is correct.
The best datasets work according to one single version of the truth, and provide the opportunity for challenging or correcting false data with an associated audit mechanism. In the future, data will be accessible using APIs with both read and write access, where permissions allow. We will also make sure there is a contract between the data asset or service owner to make sure availability and performance is guaranteed for users across the system. We will also make the origin of data more transparent and highlight where data is not held authoritatively.
4. All clinical data stored will be made accessible using APIs published on the API gateway
Patients, their carers and clinicians should be able to access the data relevant to them using a standard suite of APIs, reducing the complexity of using multiple systems. The NHS England and NHS Improvement COVID-19 Vaccinations programme have started on this journey with how they present flu and COVID vaccination data. Patients and carers will be able to access all appropriate clinical records, transactional data and events (like booking an appointment) relating to them, where clinically safe to do so, using APIs.
5. People will be able to self manage any data relating to their contact details and personal preferences
They will have the ability to manage their own data to make sure it is up to date and reflects their circumstances and preferences.
6. Organisations should be able to self-manage any data relating to them, for example locations and types of services offered
Organisations working with and on behalf of the NHS and adult social care will have the power to manage the data relating to them in one place.
7. Data should be digitally signed to an appropriate level
Data about certain activities should have unique digital identifiers attached to them to show who made a decision. Prescription services already are ‘digitally signed’ in this way, but there are other activities that also require assurance to manage issues such as fraud.
We have already been working hard to put these principles into action through our COVID-19 programme. There are a number of simple steps we can follow as shown in the image below:
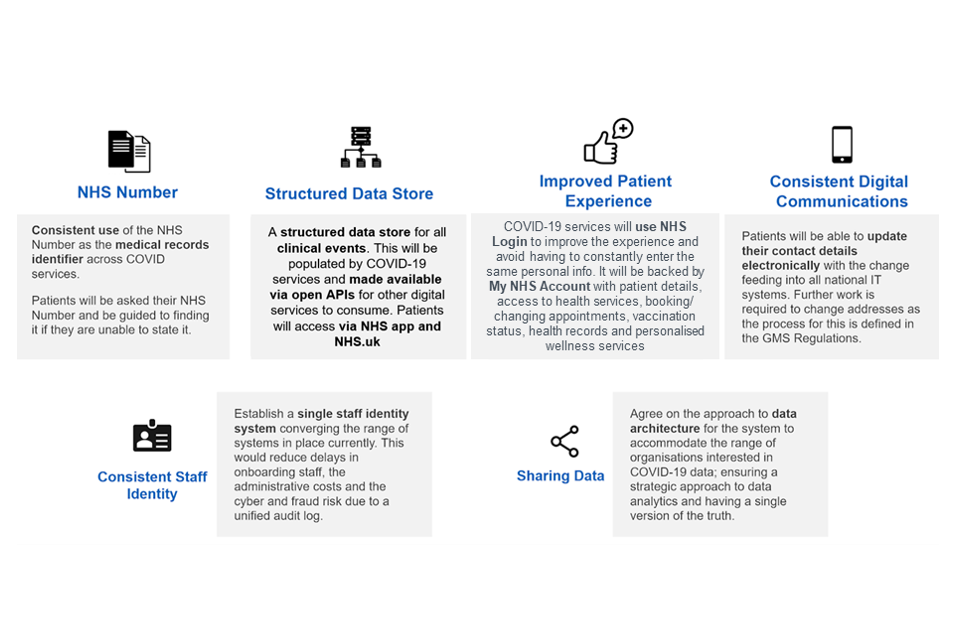
-
Consistent use of the NHS Number across COVID-19 services: this is the primary identifier for anyone who uses our NHS. We want it to be used consistently across all our digital services. By accurately identifying individuals at the start of their journey, we can make sure all data generated about them is associated with their NHS Number, and that we have a more complete record of their data.
-
Structured data store for clinical events: national NHS services aggregate a variety of clinical data for different purposes. We will bring these different datasets together into a structured data store which is accessible to both clinicians and patients, where appropriate. We will use standard data formats to enable data-driven outcomes and more responsive, real time analytical capabilities.
-
NHS Login: we need to make sure all our digital services provide the option for citizens to register and login using their NHS Login, which provides trusted verification of their identity when using NHS services.
-
NHS Account: we will also develop an NHS Account that will bring patient details from different services across the system into a collective individual account, including information found in appointment bookings, vaccination status, health records and personalised wellness services. An account API will be made available nationally for strategic partners to integrate with.
-
Update patient details electronically: we need to make sure that we have up to date and accurate contact information for people, including their contact preferences.
-
Consistent staff identity: we need to be able to confirm staff identity consistently across all services through a single staff identity system, instead of the multiple systems in use now. This will make it easier for them to be able to verify themselves at a workplace and allow them to move more freely across areas that need them.
-
Agreed approach on data architecture: the COVID-19 pandemic has highlighted the need for a change in how data is structured and shared throughout the health and social care sector. Changes to the data architecture had to be made at pace to help clinicians make decisions. Those changes must now be secured and scaled across the wider system, using the goals outlined above as early priority areas.
This will support us to fix any technical debt (legacy technical issues or systems) that no longer work for what the health and care system currently needs. This debt is often in the form of a narrow solution that was selected because it could be implemented quickly but can no longer meet the changing needs of the system, with staff having to find workarounds.
By developing our data architecture with this vision, underpinned by the principles outlined, we can deliver the best structure for innovation to thrive, with the resulting benefits for staff and service users.
Our commitments:
-
agree a target data architecture for health and social care outlining how and where data will be stored, shared and sent (winter 2021)
-
map the technical debt for national systems, and prioritise what must be addressed and completed through relevant programmes of work (March 2022)
-
provide services to find and retrieve records from wherever they are located across health and social care (spring 2022)
-
develop APIs that can be accessed over the internet to access multiple channels including clinical systems, web pages and apps, and for both patients and clinicians to access patient data, underpinning the creation of the NHS Account (March 2022)
-
improve the process of onboarding to national systems to increase uptake of national services and products such as the NHS Number (November 2021)
-
develop the roadmap for core services within the NHS using cloud technology (October 2021)
-
increase the number of APIs available on the national healthcare gateway (August 2021)
-
develop data infrastructure services to enable the flow of data across the system to support interoperability (October 2021)
-
build Centres of Excellence (CoEs) in the area of data architecture that focus on promoting best practices, support and training (August 2022)
Promoting and developing data and technical standards
Instead of data flowing seamlessly between digital systems in different health and social care organisations, too often staff face ‘information jams’. Their time is wasted logging into disparate systems or searching for information in outdated formats. Staff may have to rely on people to repeat their information, forcing them to remember difficult histories and running the risk that care is provided on partial or inaccurate information. This can impact the relationship between the patients and service users receiving and the staff providing care.
Standards and interoperability help to overcome this by providing benefits to the system and citizens such as:
-
improving patient safety by reducing errors from re-keying information across systems and care settings and by ensuring clinicians and carers have the data they need on patients in transfers, discharges and referrals
-
enabling better care by making relevant data available when clinicians need it, providing context and saving time for staff, patients and people who need care and support
-
avoiding lock-in and supporting innovation by enabling providers to choose from a diverse set of supplier products and systems, knowing they won’t lose access to information and the technology will work with other parts of the health and care. This allows them to be driven by quality and value, not fear of things breaking and losing data
-
enabling better policy and decision making through frictionless reporting and analysis based on accurate, real time and granular data; and audit trails
-
supporting people to access and own their health and care data to enable them to access and understand information, and personalised guidance and support benefiting from innovation
In order to make sure that our standards are fit for the health and care system and for suppliers working with it, we must promote ready to use standards that are:
-
Open, maintained, usable and accessible: standards are powerful when everyone can use and find them. This means they’re free and openly licensed, maintained and well documented.
-
Tested in reality and based on actual behaviours and needs: we understand that staff may not have the time and skills to correctly code up all their observations, diagnoses and procedures, and will develop our standards accordingly.
-
Designed to meet people’s needs: standards must benefit people, not just make it easier for products to interoperate. Standards development should be purpose and person-centric, considering the context and needs of patients and people who need care and support as well as care and health professionals, from clinicians to carers to administrative staff.
-
Developed collaboratively with vendors, suppliers, digital technologists, app developers and the open source community: we will be looking to digital health, innovator and vendor communities to ensure standards are realistic and help health technologies interoperate consistently. Part of this means balancing a variety of different perspectives and preferences, making sure standards don’t favour specific suppliers and we don’t overburden small suppliers.
Our commitments:
-
we will develop and publish the standards and interoperability strategy to get fit-for-purpose standards widely adopted across health and adult social care (March 2022)
-
we will introduce legislation in due course to create a power for the Secretary of State for Health and Social Care to mandate standards for how data is collected and stored, so that data flows through the system in a usable way. This will make sure that when it is accessed or provided (for whatever purpose), it is in a standard form, both readable by and consistently meaningful to the user or recipient (ongoing)
-
publish and maintain a standards roadmap, working with vendors and procurement frameworks to ensure effective implementation (April 2022)
-
develop a core of UK-wide Fast Healthcare Interoperability Resources profiles to be the foundation for new standards (November 2021)
-
begin tracking the adoption of standards and develop a standards catalogue/registry to improve visibility and accessibility of what exists to support and monitor adoption and make compliance easier (March 2022)
Staying ahead of the evolving cyber risk
As the digital transformation of the health and social care system accelerates, so does the volume of data collected and the devices used to collect it. We must maintain public trust in the cyber security of the health and adult social care sector, helping people to share data with confidence and enabling innovative data-driven technologies that can improve the quality and outcomes of people’s care.
Cyber security incidents can impact services and the delivery of people’s care. Incidents can have a large financial impact, both for costs incurred by recovering systems, or financial penalties if any of the incidents ended in a regulatory breach. Further, if public confidence in the health and care system as a safe haven is reduced, it can have a negative impact on how we can innovatively use data for the benefit of patients and service users.
Case study: the Data Security and Protection Toolkit (DSPT)
The DSPT is an online self-assessment tool that helps NHS and social care organisations measure their performance against the National Data Guardian’s 10 data security standards. It is mandatory for all arms length bodies, NHS trusts, commissioning support units, clinical commissioning groups and GP practices to complete the DSPT each year. The content is updated every year and is tailored to different types and sizes of organisations to understand their specific cyber security risks.
Analysis of DSPT data provides us an overall picture of progress made by NHS organisations and adult social care, and importantly highlights areas where challenges remain. It also provides an in-depth picture of cyber resilience and maturity at individual trust level, so we can provide a more tailored approach to helping them improve.
Good cyber hygiene and compliance with basic cyber standards goes a long way to mitigating cyber threats to system data, for example, making sure that security patches are implemented quickly, and systems do not become unsupported.
However, our biggest weapon in staying ahead of the cyber threat is ensuring that we have security baked into the design of everything we do. Since WannaCry in 2017, our centralised defences have been radically upscaled. NHS Digital’s Cyber Security Operations Centre (CSOC) now provides local and national network monitoring, incident response and threat intelligence. It blocks around 21 million items of malicious activity every month and has, since 2018, prevented at least 5 WannaCry-style attacks.
Government’s cyber security lead, the National Cyber Security Centre (NCSC), also provides regular threat assessments to help the health and social care system stay up to date in our understanding of cyber risks so that we can plan our defences accordingly.
Case study: cyber incident exercising
In February 2021, our latest cyber incident exercise ‘Exercise Cashmere’ expanded the reach of our exercising programme to primary care and gave South Central and West Commissioning Support Unit an opportunity to take us step-by-step through its incident management plans in the event of an IT incident affecting its client organisations. The event was tailored to the remote working environment and represents the first time NHSX has delivered a remote exercise of this type.
NHSX worked with an independent-sector Cyber Incident Exercising Provider alongside partner organisations including National Cyber Security Centre, NHS Digital, and the NHS England and NHS Improvement Emergency Preparedness, Resilience, and Response (EPRR) team to develop and deliver the event.
Due to the exercise’s success, we will integrate the materials and exercise constructs developed for Exercise Cashmere with other cyber-exercising resources and materials for the sector. This supports wider knowledge sharing across the sector which can be reused by other health organisations to develop their own cyber resilience in future.
Skills are also important for any cyber security defence. Training and guidance are available for everyone working in health and social care on the importance of cyber security and basic cyber hygiene.
NHSD is promoting the upskilling of the cyber workforce through professional training, which will extend to the general health and care workforce, offering cyber basics and an annual training scheme. Board and Senior Information Risk Owner-level training is also being developed, to ensure that all levels of the workforce develop strong cyber skills.
Our commitments:
-
provide leaders with the data they need to understand their organisation’s cyber risk status (March 2022)
-
work with the Medicines and Healthcare products Regulatory Authority, NHSD and NCSC through the Connected Medical Device Security Steering Group to better understand the risks around connected medical devices across the health and care system (March 2022)
-
complete 100% of backup reviews for target organisations (in 2021)
-
develop a long-term plan for cyber aiming for a cross-government approach in the NHS and adult social care (end of 2021)
-
invest funds to increase DSPT compliance and deliver direct support across the entire adult social care sector (2022)
-
set clear cyber standards for health and care organisations and suppliers, annually reviewing and publishing standards in the mandatory DSPT (annually)
-
continue to support the system to drill and regularly rehearse national incident response plans (at least annually)
-
work with NCSC to set higher standards for parts of the system most at risk of cyber attack (ongoing)
As we move towards Integrated Care Systems, we will continue to work more broadly to embed effective cyber security across the health and care system, including adult social care.
Separating the data layer
To better access people’s data on EPR systems held by third party suppliers, we will make sure a person’s data is separated from the applications that are used by health and care professionals to deliver and manage healthcare.
The data layer will consist of a set of structured data records stored in the cloud, separate from the EPR systems themselves. The data can then be easily accessed and updated by both third party and NHS systems, rather than just third party suppliers. Data will be controlled in a way that ensures secure and safe access, in line with information governance principles.
This will allow:
-
a standardised version of the data
-
a cleansed dataset that removes duplicated or obsolete records
-
data that can be more easily accessed and analysed
-
data held in the cloud, with all the proven benefits in terms of scalability, availability and security
-
a more modular approach to EPRs, avoiding vendor lock-in and creating a more dynamic and responsive market
-
innovation to take place securely and openly on top of the data, with applications able to access the data directly rather than wait for the EPR vendors to provide access
We will begin this approach for diagnostic test results, both in pathology and radiology. The procurement of the new laboratory information management systems (LIMS) and radiological information systems (RIS) that provide the underpinning digital infrastructure for the diagnostic system will give us an opportunity to design a separate data layer from the start and demonstrate its value.
We will work with both vendors and tech leaders in health and care to gather views, so we might construct the most effective route map to get to our intended goal.
Our commitments:
-
separate the data layer from the application layer (ongoing)
-
develop a data layer to manage nationally held patient data that meets the criteria set out above with a set of APIs to enable access for patients and clinicians (by 2023)
-
populate the national patient data layer with diagnostics and medicines data derived from COVID-19 initiatives (by 2023)
-
build upon the work done in shared care records to standardise API data access to shared care records (end of 2022)
7. Helping developers and innovators to improve health and care
Our vision
Innovators will be supported to develop and deliver new solutions quickly and safely for the benefit of all citizens, staff and the system.
As an innovator creating or deploying new data-driven technology for health and social care, I will have:
-
a clear understanding of how to work with the health and care system through:
-
clear guidance on data partnerships which maximise benefits to citizens and the system
-
open standards, code, APIs and systems architecture so that my innovations will easily and effectively work across the system
-
adequate documentation of the data and the APIs, and appropriate visibility on prior work that uses them
-
clear understanding of any regulatory, data protection, data handling and cyber security obligations, so that I know how to build these in at the beginning of my project
-
a speedy and simple approvals process for my application to interact with health and care data, so that I can get it out to users quickly
-
clear route maps to deploy technology at scale across the system, so that my solution has the best chance to seamlessly integrate into care pathways and frontline ways of working
-
Why this matters
The UK has a large and vibrant health and care tech sector. It gives us huge potential both to improve care and to power the UK economy. The Department of Digital, Culture, Media and Sport (DCMS) has estimated that the digital sector accounted for 7.7% of the UK economy as a whole and contributed £149 billion to it in 2018. Growth in the sector is nearly 6 times larger than growth across the rest of the economy.
As data is the cornerstone of the health and care tech sector, we must make sure innovators are given clarity over what, how, and where it can be accessed and used.
Clear frameworks, standards and guidance on data use ensuring the highest levels of data protection, will allow us to bring all the benefits of innovation back into the system.
Data partnerships are central to accelerating opportunities for innovation. Over recent years, the UK has seen the growth of multidisciplinary innovation, with collaboration between health and care partners, academia and industry, occurring at increasing scale and pace. In addition to running our own analysis and buying data-driven tools, local health and care organisations also have opportunities to work with innovators directly to create new algorithms and digital services.
So that we can continue to provide the best care for the citizens we serve, we must safely grasp the opportunities for data-driven innovation to enhance the care provided, supporting staff and colleagues to do their jobs, and to continually improve how our health and care system works.
Progress so far
We have:
-
created the Centre for Improving Data Collaboration (CIDC) to guide NHS trusts in their discussions with potential industry partners to improve returns and to renegotiate improved terms in their partnerships
-
created the NHS AI Lab to promote the effective, ethical and safe use of AI technologies within health and adult social care
-
established the AI in Health and Care Award (NHS AI Lab) and already supporting 42 promising AI products that align with the aims of the NHS Long Term Plan
-
made the case for international cooperation, producing an original policy white paper and recommendations, AI for healthcare: creating an international approach together, on behalf of the Global Digital Health Partnership
-
published code for the NHS COVID-19 App, the National COVID-19 Chest Imaging Database and our analysis in OpenSafely through the NHSX GitHub
Taking this further
Driving interoperability for innovation
Open and reusable code also helps data-driven innovators build systems that can easily work with the health and care system.
Our new standards registry will be open source and documented on the NHSX GitHub page to enable and encourage feedback, suggestions and collaboration. We will explore ways in which we can signpost or host reference implementations, guidance and best practice around interoperability interfaces (in particular FHIR APIs, guides and profiles) to share learnings amongst digital health communities and accelerate standards adoption.
NHSX, NHS Digital and NHS England and NHS Improvement will lead by example, as well as pushing the case across the system to modernise and strengthen the use of data and analytics.
Case study: Shielded Patients List
Early on in the COVID-19 pandemic, the Chief Medical Officer requested that leading scientists, academics and clinicians work together to create a model to predict which factors would place patients at higher risk if they caught coronavirus.
This research consortium, led by Oxford University, used linked anonymous GP records to develop a model, QCovid, that used various factors to work out a patient’s risk of hospitalisation and death if they caught coronavirus. This information became invaluable when prioritisation was being assessed for vaccinations. As a result of this model, in February 2021, 1.5 million people were added to the Shielded Patient List, ensuring the most vulnerable were prioritised for the vaccine.
In addition to the publication of the Oxford University research that created the QCovid algorithm in the BMJ, Oxford University Innovation provided a reference implementation to demonstrate how the algorithm works, and have since made the QCovid® Calculation Engine source code available at GitHub in the interests of transparency, flexibility and accountability, and in line with HMG guidance on the use of open-source code. This will enable the model to be used by interested researchers for academic purposes, enabling further potential societal benefits.
This data driven, population risk stratification to identify and protect those at high risk from COVID demonstrates the power of data driven population health management, for which the technology now exists within the NHS.
Our commitments:
-
publish a digital playbook on how to open source your code for health and care organisations with guidance on where to put the code, how to license and what licences to use, how to maintain and case studies of teams who have done this (2021)
-
collaborate with the MRC, NIHR, and UK Research and Innovation to ensure that grants for research involving health and care data follow open and reusable code principles (ongoing)
Encouraging AI innovation
AI technologies, in particular, have real potential to improve the delivery of health and care services by analysing large quantities of complex information.
The AI in Health and Care Award run by the NHS AI Lab and the Accelerated Access Collaborative makes £140 million available over 3 years to support both homegrown and international innovators and technologies across the full spectrum of development, from initial feasibility to NHS adoption and testing within clinical pathways.
The first round of the AI in Health and Care Award concluded in September 2020, taking forward 42 promising AI technologies that align with the aims of the NHS Long Term Plan. Round 2 of the competition concludes in May 2021, with a third round opening to applicants in July 2021. Details of some previous winners can be found in the case study below.
Case study: Al in Health and Care Award winners
The 42 winners in the first round include:
Brainomix for E-Stroke, a set of tools that uses AI methods to interpret acute stroke brain scans, and helps doctors make the right choices about treatment and the need for specialist transfer of patients with confidence. It also provides a platform for doctors to share real-time information between hospitals, avoiding the delays.
Kheiron Medical Technologies for Mia Mammography Intelligent Assessment, deep learning software. It has been developed to solve critical challenges in the NHS Breast Screening Programme, including reducing missed cancers, helping manage staffing pressures and tackling delays that put women’s lives at risk.
Mirada Medical Ltd for DLCExpert, which uses AI software to automate the time-consuming and skill-intensive task of contouring organs on medical images for radiotherapy planning so that the healthy tissue is spared from irradiation.
Ibex Medical Analytics to study the effectiveness of their AI system for detecting cancer and other clinically important histological features in biopsy slides. The study uses data from 600 men across 6 NHS hospitals, and compares the results of their system with conclusions from trained pathologists.
Ultromics Ltd for the EchoGo Pro, a fully automated application for quantification and interpretation of stress echocardiograms, that autonomously processes echocardiographic images to predict cardiac disease.
For innovations to be successfully deployed, staff and patients must have confidence that they are safe. NHSX is developing an approach to technical validation of algorithms for screening pre-deployment to provide buyers and clinicians with the assurance that a product’s technical performance is appropriate for clinical use.
The NHS AI Lab has been working with PHE to test a validation approach for AI models for future screening programmes. We have focused on mammography initially and are working towards publishing a paper with our methodology in 2022.
We work with regulators to enable the independent validation of algorithms for screening into the regulatory pathway. This will provide NHS commissioners and healthcare regulators with the necessary standards to judge the safety, efficacy, and external validity of AI models for screening before their deployment in clinical practice.
A robust evaluation methodology for algorithms when deployed into practice is also required. The NHS AI Lab, in partnership with the Accelerated Access Collaborative and academics, has developed an evaluation methodology for the phase 4 products in the AI in Health and Care Award, which we will iterate and improve as we test it in practice. The evaluation of the AI Awardees is being undertaken throughout the lifespan of the NHS AI Lab.
The NHS AI Lab has also launched the AI Ethics Initiative to ensure that we have a rigorous approach to using AI products in health and care settings, including:
- working with the Ada Lovelace Institute to design and trial algorithmic impact assessments
- empowering healthcare professionals to make the most of AI
Our commitments:
- support up to 100 AI companies through the AI in Health and Care Awards to achieve market authorisation and/or the real world evidence required to support long-term NHS commissioning of their technology (March 2026)
Clear and understandable AI regulation
Following our departure from the EU, we also have an opportunity to make the UK the leader in proportionate, innovation-friendly regulation of AI technologies.
The NHS AI Lab is working to create a clear and robust regulatory framework for AI, that supports innovation and gives patients and clinicians confidence that AI products are safe and effective.
The NHS AI Lab is doing this in partnership with the UK’s regulatory bodies and other key health organisations including the MHRA, NICE, CQC, Health Research Authority (HRA), and NHS Resolution.
Our commitments:
- develop unified standards for the efficacy and safety testing of AI solutions, working with MHRA and NICE (2023)
- develop a National Health and Adult Social Care AI Strategy (2024 to 2030) to consolidate the system transformation achieved through the NHS AI Lab (2022)
We will support UK regulators to:
-
ensure AI regulation is fit for purpose as part of amending the Medical Devices Regulations 2002 following our departure from the EU
-
streamline the regulation pathway for AI technologies to enable innovators to get their product to market in a seamless, efficient manner
-
develop a multi agency service for innovators seeking advice on their regulatory journey in getting their product to market will be piloted in 2021, following the identification of gaps in the regulatory landscape, and rolled out by 2023
-
develop a regulatory position on the acceptability of using synthetic data as training data for AI as a medical device and explore the use of synthetic data for the validation and benchmarking of AI as a medical device
-
enhance and extend Medicines and Healthcare products Agency’s (MHRA’s) Yellow Card technology to deliver data-driven, smart reporting on adverse incidents (July 2023)
Supporting innovators to work with health and care organisations
Some of the most exciting areas of tech innovation in health and social care come from artificial intelligence, algorithms and data-driven technologies.
We know that this cutting-edge work isn’t always easy to sell into the NHS, and we are taking steps to help local NHS organisations become stronger buyers and more informed consumers of data-driven tools and services. Similar work has already been undertaken for the government guidelines on AI procurement.
Additionally, the size and structure of the health and care system means that to scale data applications or software, you have to work with multiple organisations. To help make this as simple as possible, our work across information governance and standards (as mentioned in previous sections) includes:
-
issuing clear guidance through our Information Governance Portal for data protection rules for data-driven technologies that access people’s data
-
providing open standards for interoperability so that developers know how to build for the health and social care system
-
working with vendors, suppliers, developers and the open source community to ensure that standards are realistic, don’t favour specific suppliers, and don’t overburden small suppliers
Case study: University Hospitals Birmingham
University Hospitals Birmingham (UHB) has partnered with a number of technology companies to deliver improvements in 3 key areas: smart access, smart diagnostics and smart support. This has led to the adoption of cutting edge digital technologies which have transformed models of care for the population of Birmingham and Solihull, as well as supporting the restoration and recovery of services impacted by the COVID-19 pandemic.
Projects include:
-
an artificial intelligence powered skin cancer pathway, which has helped 40% of patients avoid the need for a hospital appointment
-
an ophthalmology pathway where scans and diagnostics are carried out in the community without the need for a hospital appointment, with all information being reviewed by UHB consultant ophthalmologists remotely. This care model and technology is now being applied to a broad range of specialties across the trust
-
a 5G connection between community intermediate care and acute hospital teams, including digital stethoscopes, ECG and high resolution video, to allow comprehensive assessments to be carried out without the need to convey patients to hospital
-
ask A&E symptom checker, where 64% of 19,000 users were appropriately sign-posted to non-hospital settings to receive care
UHB has established contractual relationships that recognise the expertise and intellectual property that UHB brings through their clinical staff and pathway mapping as well as through their data.
Our commitments:
-
make £140 million of funding available through the AI in Health and Care Award to accelerate the testing and evaluation of AI technologies (2024)
-
helping regulators develop an approach for independently validating AI technologies for screening (June 2022)
Creating fair returns in data partnerships
The government’s National Data Strategy’s mission two reiterates that we want to make sure the UK data protection regime maintains standards, but that we are able to benefit from innovative new ways to work and deliver care by reducing unnecessary burdens to responsible data use. This helps us create a safe and accessible environment for researchers and innovators, while streamlining the process.
Through the CIDC, we will give health and care bodies guidance and tailored support to help them navigate data partnerships, so they can make decisions properly informed by legal advice and commercial best practice. This includes support to:
-
raise awareness of the potential benefits to patients, service users and the NHS and wider society of using data to drive research and innovation, together with the assurance that partnerships can be done well
-
clarify what is expected as a minimum standard, and where there is room for local flexibility
-
provide common approaches to establishing the most appropriate partnership model, as well as consistent financial valuation models, treatment of Intellectual Property, accounting methods, and legal and contractual drafting
-
ease access to the UK’s healthcare data assets, to stimulate a new wave of digital and data-driven innovation to benefit patients and the wider system
The 5 principles for data partnerships will further support innovators to thrive and to provide fair returns to the system and the people it serves.
The 5 principles to help the NHS realise benefits for patients and the public in data partnerships
In 2018, the Second Life Sciences Sector Deal set out 5 draft principles to realise benefits for patients and the NHS where data underpins innovation.
The 5 principles were tested and refined following an extensive period of engagement with the NHS, medical research charities, public and patient engagement advocates, healthcare professionals, researchers, regulators and industry experts, and a revised version was published in July 2019.
-
Any use of NHS data, including operational data, not available in the public domain must have an explicit aim to improve the health, welfare and/or care of patients in the NHS, or the operation of the NHS. This may include the discovery of new treatments, diagnostics, and other scientific breakthroughs, as well as additional wider benefits. Where possible, the terms of any arrangements should include quantifiable and explicit benefits for patients which will be realised as part of the arrangement.
-
NHS data is an important resource and NHS organisations entering into arrangements involving their data, individually or as a consortium, should ensure they agree fair terms for their organisation and for the NHS as a whole. In particular, the boards of NHS organisations should consider themselves ultimately responsible for ensuring that any arrangements entered into by their organisation are fair, including recognising and safeguarding the value of the data that is shared and the resources which are generated as a result of the arrangement.
-
Any arrangements agreed by NHS organisations should not undermine, inhibit or impact the ability of the NHS, at national level, to maximise the value or use of NHS data. NHS organisations should not enter into exclusive arrangements for data held by the NHS, nor include conditions limiting any benefits from being applied at a national level, nor undermine the wider NHS digital architecture, including the free flow of data within health and care, open standards and interoperability.
-
Any arrangements agreed by NHS organisations should be transparent and clearly communicated in order to support public trust and confidence in the NHS and wider government data policies.
-
Any arrangements agreed by NHS organisations should fully adhere to all applicable national level legal, regulatory, privacy and security obligations, including in respect of the National Data Guardian’s (NDG’s) Data Security Standards, the UK General Data Protection Regulation (GDPR) and the Common Law Duty of Confidentiality.
Our commitments:
-
publish the Value Sharing Framework and Guidance (July 2021)
-
translate the 5 principles in the context of the adult social care sector (March 2023)
-
develop a resource hub for healthcare leaders on data partnerships (September 2021)
-
review and update NHS Digital’s data sharing contracts to reflect the Value Sharing Framework Guidance (2022)
Next steps
The coronavirus pandemic has been a tough year for us all. However, one thing we have learnt from this difficult time is the importance of data and the potential it has to make a difference if we use it appropriately and effectively.
COVID-19 has led to vaccine development, new medical treatments, and testing, all driven by the safe and secure use of data. We saw in 2020 the power of data to save lives.
For too long, health and care data has been kept in silos, which means people have been cared for in silos. We need to do more to unlock the potential of our health and care data, so we can make its benefits felt for everyone.
We must not stand still. We must keep this momentum going, and make sure everyone involved in health and care can benefit.
Data can feel like an abstract subject, but data underpins so many of our interactions with our health and care system. This means that if we can transform the way we use data, then every single person can benefit.
Through changing how we use data, there are vast opportunities to deliver real opportunities for everyone involved in health and care: patients, service users, researchers, and colleagues on the front line.
This draft strategy shows how we will make data the foundation of our health and care system, changing laws and regulations where they are no longer fit for purpose, so everyone has the confidence to share and use data.
What makes the opportunities so exciting, the fact that we all interact with our health and care system, also presents challenges too. People rightly want their data to remain private, and so as we move forward, we will put in place strong frameworks for security and data ethics.
The shared experience of this pandemic has shown how data saves lives. The work in this strategy is vital if we are to create a health and care system that is fit for the future, and well equipped to meet the challenges ahead.
Before we publish the final version of the strategy later this year, including a more detailed implementation plan, we want to hear your views on:
-
whether the commitments and timetable in this strategy are achievable
-
whether there are any barriers we should consider when planning implementation
-
how we best increase transparency and communicate progress on how data is being used and shared
Increasing transparency and communicating progress
Successful initiatives, such as the OneLondon Citizens’ Summit public engagement programme and the Yorkshire and Humber Care Record citizen engagement work, show how people can be brought together to discuss how their data is being used and support decision-making in the future. These exercises showed support for a joined-up approach to data and proved to be extremely useful for gathering feedback.
This year NHSX, alongside the National Data Guardian (NDG) and University of Manchester, commissioned 3 Citizens Juries to discuss data sharing in a range of contexts, from Summary Care Record with Additional Information to the NHS COVID-19 Data Store. The conclusions of those juries will be published later this year. We would welcome other suggestions, for example the final version of this strategy could commit to:
-
hold regional public engagement events to find out how people would like to use and access their data
-
work with partners including Understanding Patient Data, Sciencewise, and research charities, to establish good practice with regard to transparency and meaningful public involvement in data use
Annex A: list of all commitments
1. Bringing people closer to their data
Harnessing data to improve people’s safety
-
we will improve information governance guidance so staff are confident in sharing people’s data for their individual care, including publishing the Information Governance Framework for Integrated Health and Care (July 2021)
-
we will undertake further work on harnessing data to improve health outcomes and reduce inequalities, including the AI Ethics Initiative which will report in 2022 to 23 on its research call exploring how to use those technologies to improve health outcomes for minority ethnic populations in the UK (ongoing)
-
we will digitalise personal child health records to ensure families and professionals have the information they need, when they need it. This work is supported by the Early Years Healthy Development Review published in March 2021 which sets out how better data-sharing could improve the experiences of parents, carers and staff (2023)
Bringing people closer to their data
- we will make sure that the technology is in place to enable everyone across England to have easy access to their own health and care data (2022)
Giving people confidence
-
publish the first transparency statement setting out how health and care data has been used across the sector (2022)
-
give citizens the ability to see what research their data has informed, and who has had access to their data, as soon as the technology allows (ongoing)
-
embed an open-working approach across health and social care, consistent with protecting privacy, so the public can easily find and understand the data delivery work (ongoing)
-
lead the Health and Care Information Governance Panel to develop guidance, frameworks and standards such as data sharing and transparency so the public can be confident in our handling of their data (December 2021)
2. Giving health and care professionals the data they need to provide the best possible care
Simplifying information governance
-
embed the Information Governance Portal as the one-stop shop for help and assistance, guidance and advice (December 2021)
-
complete the key priority areas in our work to align national information governance guidance (April 2022)
-
with the Health and Care Information Governance Panel, create fit-for-purpose rules around different types of data (such as pseudonymised), so that staff can clearly understand rules around the use of data (April 2022)
-
we will develop a national Information Governance Strategy to address training for frontline staff (April 2022)
-
we will review tool kits and language to bring into line with simplification work (July 2022)
-
with the NDG, develop new e-learning packages on the use of data for frontline staff, information governance professionals, and Caldicott Guardians (2021)
Creating a new duty to share
- we will introduce legislation in due course to create a statutory duty for organisations within the health and care system to share anonymous data for the benefit of the system as a whole (ongoing)
Delivering shared records
-
ensure that each Integrated Care System has a basic shared care record in place to enable sharing of key information between GP practices and NHS trusts (2021)
-
deliver comprehensive shared records in line with the commitments in the NHS Long Term Plan so that authorised staff for other care partners can easily and appropriately access data regardless of where care is delivered (2024)
Reducing the data collection burden
- have in place a system-wide target for the rationalisation of data collections to reduce the time spent by health and care staff inputting and processing data for national use (by 2021 to 2022 and reviewed annually)
Harnessing safe and effective innovation
- scale up our digital home care projects to support many more people with care at home, including those resident in care homes, improving their health outcomes (March 2022)
3. Supporting local and national decision makers with data
Integrating local care systems with a culture of interoperable by default
- we will ensure the inclusion of adult social care providers (where they have digitised records) to integrate with basic shared record solutions across health (September 2022)
Building analytical and data science capability
-
we will develop an analyst workforce observatory, including an annual census to inform how to better harness the professional skills of analysts and data scientists, and support their professional learning and development (March 2022)
-
we will develop an online Analytics Hub, working with AnalystX, to share, promote and endorse training, events and other resources (2021)
-
we will grow the Analyst X community and build the team of future analytical leaders through a champions programme (March 2022)
-
we will pilot a data and analytics accelerator (March 2022)
-
we will develop and roll out a unified set of competency frameworks aligned to the government Analysis Function skills (2022)
-
through the ‘Developing Data and Analysis as a Profession Board’, we will:
- agree frameworks, guidelines and policies to operate in
- build the ecosystem of the profession through communities of practice (local, regional, national and virtual)
- signpost and provide development opportunities for analysts (ongoing)
Working in the open
- we will begin to make all new source code that we produce or commission open and reusable and publish it under appropriate licences to encourage further innovation (such as MIT and OGLv3, alongside suitable open datasets or dummy data) (end of 2021)
Sharing data for wider purposes
-
we will use secondary legislation in due course to enable the proportionate sharing of data including, where appropriate, personal information for the purposes of supporting the health and care system without breaching the common law duty of confidentiality (ongoing)
-
we will work closely with stakeholders and the public to make sure that these changes are implemented transparently and that appropriate safeguards are in place (ongoing)
Collaborating with wider partners
-
we will work across central government, including with colleagues in MHCLG, DfE, the Cabinet Office, MOJ, DWP and across the devolved administrations to improve appropriate data linkage to support people’s health and wellbeing (ongoing)
-
our public health agencies will draw on multiple data sources to gain new insights into the public’s health, with quicker access to high quality health intelligence to inform improved decision-making and responses to crises (ongoing)
4. Improving data for adult social care
Improving access to information for adult social care providers
-
collect client-level data rather than aggregate data from local authorities to ensure that we have regular and comprehensive data to enable person-centred, sustainable innovation for adult social care (2023)
-
DHSC will develop a plan for sharing data with local authorities that looks beyond the pandemic, building on the learning from the COVID-19 response (ongoing)
-
provide digital skills frameworks to identify what good digital working looks like in practice, supported by the delivery of training opportunities to improve the data and digital literacy of the adult social care workforce (by March 2022)
Integration of health and social care data
-
work with care providers to accelerate the adoption of digital social care records through the NHSX Digitising Social Care Record programme for better access and interoperability with Shared Care Records (2024)
-
we will introduce legislation in due course to require information from all adult social care providers (both public and private), so that we can build a better picture of the delivery of adult social care services across England (ongoing)
-
establish a data framework for adult social care setting out what data we intend to collect and the standards used to collect it so we know we are getting the data we need (March 2022)
-
work with NHS Digital and NHS England and NHS Improvement to continue to build the foundations needed to support care providers in accessing the information they need to deliver high quality care for people (March 2022)
-
we will continue to promote NHSmail (or other appropriate services that meet the government’s secure email policy requirements) to all care providers to enable secure information sharing with colleagues and with the NHS (2021 to 2022)
Expanding the use of care technologies
We will engage and collaborate with a range of partners, including local authorities, care providers (tech-enabled or otherwise), innovators, and the wider health and care system, to build strong relationships and:
- improve their confidence in the commissioning and purchasing of care technologies that support integrated working
- support the creation of a vibrant CareTech marketplace
- spread the use and adoption of these technologies and evaluate how the data they generate can be used to improve the quality of care
This will ensure that we continue to focus on the challenges and opportunities that will have the greatest impact in driving digital transformation in social care. (2021 to 2022)
5. Empowering researchers with the data they need to develop life changing treatments, models of care and insights
Providing safe and secure data for analysis and research
-
create partnerships between academic researchers and frontline analytical teams to enhance the exchange of skills and knowledge (ongoing)
-
produce a consistent and clear glossary of terminology and legal definitions working with the research community to alleviate confusion and improve the quality of research access requests (October 2021)
Sharing data for research
-
consider and, where appropriate, act on the findings and recommendations of the Goldacre Review into the use of data for research and analysis (end of 2021)
-
progress towards creating at-scale data assets that bring together the different types of health data to develop new tools for prevention, diagnostics and clinical decision-support (2023)
-
progress towards bringing together genomics data assets, and work with NHS England and NHS Improvement to ensure genomic data generated through clinical care is fed back into patients’ records (2023)
Encouraging clinical research
-
build on platforms such as NHS DigiTrials to enable and support best use of data and digital tools in study feasibility, identification and monitoring of research participants to enable faster, more efficient and effective clinical trials (March 2022)
-
publish the first implementation plan to progress UK priorities for clinical research as set out in the UK vision for clinical research delivery, including a key theme on research enabled by data and digital tools (2021)
-
working with other countries and G7 members to facilitate the rapid generation of compelling evidence through randomised clinical trials of treatments and to enable timely and decisive action on the findings in this pandemic and for future clinical trials (2021)
-
working with other countries and G7 members to develop a framework to share testing methods and materials would ensure that the data generated could more readily be compared in vaccine development (2021)
6. Helping colleagues develop the right technical infrastructure
Modernising our data architecture
-
agree a target data architecture for health and social care outlining how and where data will be stored, shared and sent (winter 2021)
-
map the technical debt for national systems, and prioritise what must be addressed and completed through relevant programmes of work (March 2022)
-
provide services to find and retrieve records from wherever they are located across health and social care (spring 2022)
-
develop APIs that can be accessed over the internet to access multiple channels including clinical systems, web pages and apps, and for both patients and clinicians to access patient data, underpinning the creation of the NHS Account (March 2022)
-
improve the process of onboarding to national systems to increase uptake of national services and products such as the NHS Number (November 2021)
-
develop the roadmap for core services within the NHS using cloud technology (October 2021)
-
increase the number of APIs available on the national healthcare gateway (August 2021)
-
develop data infrastructure services to enable the flow of data across the system to support interoperability (October 2021)
-
build Centres of Excellence (CoEs) in the area of data architecture that focus on promoting best practices, support and training (August 2022)
Promoting and developing data and technical standards
-
we will develop and publish the standards and interoperability strategy to get fit-for-purpose standards widely adopted across health and adult social care (March 2022)
-
we will introduce legislation in due course to create a power for the Secretary of State for Health and Social Care to mandate standards for how data is collected and stored, so that data flows through the system in a usable way. This will make sure that when it is accessed or provided (for whatever purpose), it is in a standard form, both readable by and consistently meaningful to the user or recipient (ongoing)
-
publish and maintain a standards roadmap, working with vendors and procurement frameworks to ensure effective implementation (April 2022)
-
develop a core of UK-wide Fast Healthcare Interoperability Resources profiles to be the foundation for new standards (November 2021)
-
begin tracking the adoption of standards and develop a standards catalogue/registry to improve visibility and accessibility of what exists to support and monitor adoption and make compliance easier (March 2022)
Staying ahead of the evolving cyber risk
-
provide leaders with the data they need to understand their organisation’s cyber risk status (March 2022)
-
work with the Medicines and Healthcare products Regulatory Authority, NHSD and NCSC through the Connected Medical Device Security Steering Group to better understand the risks around connected medical devices across the health and care system (March 2022)
-
complete 100% of backup reviews for target organisations (in 2021)
-
develop a long-term plan for cyber aiming for a cross-government approach in the NHS and adult social care (end of 2021)
-
invest funds to increase DSPT compliance and deliver direct support across the entire adult social care sector (2022)
-
set clear cyber standards for health and care organisations and suppliers, annually reviewing and publishing standards in the mandatory DSPT (annually)
-
continue to support the system to drill and regularly rehearse national incident response plans (at least annually)
-
work with NCSC to set higher standards for parts of the system most at risk of cyber attack (ongoing)
Separating the data layer
-
separate the data layer from the application layer (ongoing)
-
develop a data layer to manage nationally held patient data that meets the criteria set out above with a set of APIs to enable access for patients and clinicians (by 2023)
-
populate the national patient data layer with diagnostics and medicines data derived from COVID-19 initiatives (by 2023)
-
build upon the work done in shared care records to standardise API data access to shared care records (end of 2022)
7. Helping developers and innovators to improve health and care
Driving interoperability for innovation
-
publish a digital playbook on how to open source your code for health and care organisations with guidance on where to put the code, how to license and what licences to use, how to maintain and case studies of teams who have done this (2021)
-
collaborate with the MRC, NIHR, and UK Research and Innovation to ensure that grants for research involving health and care data follow open and reusable code principles (ongoing)
Encouraging AI innovation
Support up to 100 AI companies through the AI in Health and Care Awards to achieve market authorisation and/or the real world evidence required to support long-term NHS commissioning of their technology (March 2026)
Clear and understandable AI regulation
-
develop unified standards for the efficacy and safety testing of AI solutions, working with MHRA and NICE (2023)
-
develop a National Health and Adult Social Care AI Strategy (2024 to 2030) to consolidate the system transformation achieved through the NHS AI Lab (2022)
-
we will support UK regulators to:
-
ensure AI regulation is fit for purpose as part of amending the Medical Devices Regulations 2002 following our departure from the EU
-
streamline the regulation pathway for AI technologies to enable innovators to get their product to market in a seamless, efficient manner
-
develop a multi agency service for innovators seeking advice on their regulatory journey in getting their product to market will be piloted in 2021, following the identification of gaps in the regulatory landscape, and rolled out by 2023
-
develop a regulatory position on the acceptability of using synthetic data as training data for AI as a medical device and explore the use of synthetic data for the validation and benchmarking of AI as a medical device
-
enhance and extend Medicines and Healthcare products Agency’s (MHRA’s) Yellow Card technology to deliver data-driven, smart reporting on adverse incidents (July 2023)
-
Supporting innovators to work with health and care organisations
-
make £140 million of funding available through the AI in Health and Care Award to accelerate the testing and evaluation of AI technologies (2024)
-
helping regulators develop an approach for independently validating AI technologies for screening (June 2022)
Creating fair returns in data partnerships
-
publish the Value Sharing Framework and Guidance (July 2021)
-
translate the 5 principles in the context of the adult social care sector (March 2023)
-
develop a Resource Hub for healthcare leaders on data partnerships (September 2021)
-
review and update NHS Digital’s data sharing contracts to reflect the Value Sharing Framework Guidance (2022)
Annex B: legislative changes
The imperative for change
We acted quickly, using existing legislation, to enable the safe and effective use of data to support the response to the pandemic and the country has benefited from it. Government has ensured that health and care professionals, those managing the national response, and researchers have had access to the right information – quickly, easily and when they need it.
From the rapid establishment of the shielded patient list to the development of a new research platform such as the NHS COVID-19 Data Store, the changes we made were key both to our immediate response to the pandemic and our longer-term understanding of the disease and its impacts.
We want to ensure that these benefits can be felt by patients and service users across the health and care system and we are working to identify and tackle existing barriers including changes to legislation which will enable more effective use of data.
This will improve the delivery of care by supporting the health and care system to develop effective policies, plan and commission services, target care where it is most needed, and identify poor performance.
None of the changes we are making will remove the duties of organisations to meet the requirements of data legislation. This means that all uses of an individual’s data will need to be necessary, proportionate, transparent and subject to that individual’s rights to access, correction and information on use.
Primary legislation
We are looking to introduce new legislation as part of the Health and Care Bill to allow the following:
-
place a duty on organisations within the health and social care system to share anonymous information (both data that is not identifiable, for example, bed capacity, and de-identified data) that they hold where such sharing would benefit the health and social care system
-
introduce powers for the Secretary of State for Health and Social Care to require data from all registered adult social care providers about services they provide whether funded by local authorities or privately by individuals
- make changes to NHS Digital’s legal framework to:
- introduce a duty on NHS Digital to have regard to the benefit to the health and social care system of sharing data that it holds when exercising its functions
- clarify the purposes for which it can share data
- allow it to require data from private providers of healthcare (where directed to do so by Secretary of State)
- introduce a power for the Secretary of State for Health and Social Care to mandate standards for how data is collected and stored, so that data flows through the system in a usable way, and that when it is accessed/provided (for whatever purpose), it is in a standard form, both readable by, and consistently meaningful to, the user or recipient
Secondary legislation
We will use secondary legislation in due course to enable the proportionate sharing of data, including, where appropriate, personal information, for purposes of supporting the health and care sector (for example, for invoicing, commissioning, planning, analysis, policy development, audit and risk stratification) without breaching the common law duty of confidentiality.
We will work closely with stakeholders and the public to make sure that these changes are implemented transparently and that appropriate safeguards are in place.
Annex C: terms of reference for the Goldacre Review
How does the centre facilitate access to NHS data by researchers, commissioners, and innovators, while preserving patient privacy?
What types of technical platforms, trusted research environments, and data flows are the most efficient, and safe, for which common analytic tasks?
How does the system support researchers to overcome the technical, regulatory, and cultural barriers to achieving this goal, and how can they be rapidly overcome?
Where have current approaches been successful, and where have they struggled?
How does the system avoid unhelpful monopolies being asserted over data access for analysis?
What are the right responsibilities and expectations on open and transparent sharing of data and code for ALBs, clinicians, researchers, research funders, electronic health records and other software vendors, providers of medical services, and innovators? And how do we ensure these are met?
How can useful data science by the public and private sectors be best incentivised and resourced practically? What roles must the state perform, and which are best delivered through a mixed economy? How can the system ensure true delivery is rewarded?
How significant do the issues of data quality, completeness, and harmonisation across the system affect the range of research uses of the data available from health and social care?
If data is made available for secondary research, for example to a company developing new treatments, then how can those using data prove to patients that privacy is preserved, beyond simple reassurance?
How can data curation best be delivered, cost effectively, to meet these researchers’ needs?
What are the key successes and best practice in data science, commercial, and open source software development communities?
How can the NHS be supported to analyse and use data routinely to improve quality, safety and efficiency?