Enteric fever (typhoid and paratyphoid) England, Wales and Northern Ireland: 2021
Updated 22 August 2024
Applies to England, Northern Ireland and Wales

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/typhoid-and-paratyphoid-laboratory-confirmed-cases-in-england-wales-and-northern-ireland/enteric-fever-typhoid-and-paratyphoid-england-wales-and-northern-ireland-2021
Enteric fever (also known as typhoid and paratyphoid) is an illness caused by the bacteria Salmonella enterica subspecies enterica serovar Typhi (typhoid) or serovars Paratyphi A, B or C (paratyphoid). Typhoid fever is a serious disease and can be life-threatening unless treated promptly with antibiotics. The disease may last several weeks and convalescence takes some time. In the literature, paratyphoid is considered to be typically milder than typhoid and of shorter duration (1, 2).
The bacteria that cause typhoid and paratyphoid only occur in humans. Humans acquire infection through eating food or drinking water that has been contaminated with infected faeces or through direct faecal-oral transmission. Transmission occurs following the ingestion of food or water that has been heavily contaminated (10 or more organisms may be required to cause illness) by the bacterium S. Typhi or S. Paratyphi. In the UK, most cases of typhoid and paratyphoid are acquired abroad in countries and regions of the world where hygiene or sanitation is poor.
This report summarises the epidemiology of laboratory-confirmed cases of S. Typhi and S. Paratyphi reported in England, Wales and Northern Ireland (EWNI) in 2021. It includes both reference laboratory and enhanced enteric fever surveillance data.
Data sources
Confirmed symptomatic cases of S. Typhi and S. Paratyphi in England, Wales and Northern Ireland are diagnosed by the UK Health Security Agency (UKHSA) Salmonella Reference Service (SRS), within the Gastrointestinal Bacteria Reference Unit (GBRU) [footnote 1]. Data for laboratory-confirmed cases from 2007 onwards was extracted from the reference laboratory database using ‘date received by the laboratory’.
All S. Typhi and S. Paratyphi isolates referred to the SRS undergo identification using whole genome sequencing (WGS) and single nucleotide polymorphism (SNP) typing (3, 4). Epidemiological information was obtained from enhanced enteric fever surveillance (5).
Cases are occasionally tested multiple times for confirmation and to check the infection has cleared, therefore data has been deduplicated so that only one laboratory report for each case is counted.
Confirmed asymptomatic, probable and possible cases are analysed separately at the end of this report.
All data was analysed using Excel for Office 365 (Version 2002, Microsoft).
General trend
Since the beginning of the coronavirus (COVID-19) pandemic in early 2020 there has been a significant decrease in international travel worldwide as many countries, including the UK, imposed restrictions on both arriving and departing travellers (6). Data on travel to and from the UK was obtained from the Office of National Statistics (ONS) International Passenger Survey (7).
In 2021, UK residents made 19.1 million visits abroad, which was a 20% decrease from 2020 (23.8 million visits) and an 80% decrease from 2019 (93.1 million visits). There were 6.4 million visits made by overseas residents to the UK in 2021, a 43% decrease compared to 2020 (11.1 million visits) and an 84% decrease compared to 2019 (40.9 million visits) (8). In line with falling numbers of travellers arriving in the UK, in 2021 there was a decrease in cases of enteric fever (typhoid and paratyphoid) diagnosed in the UK compared to 2020 and previous years.
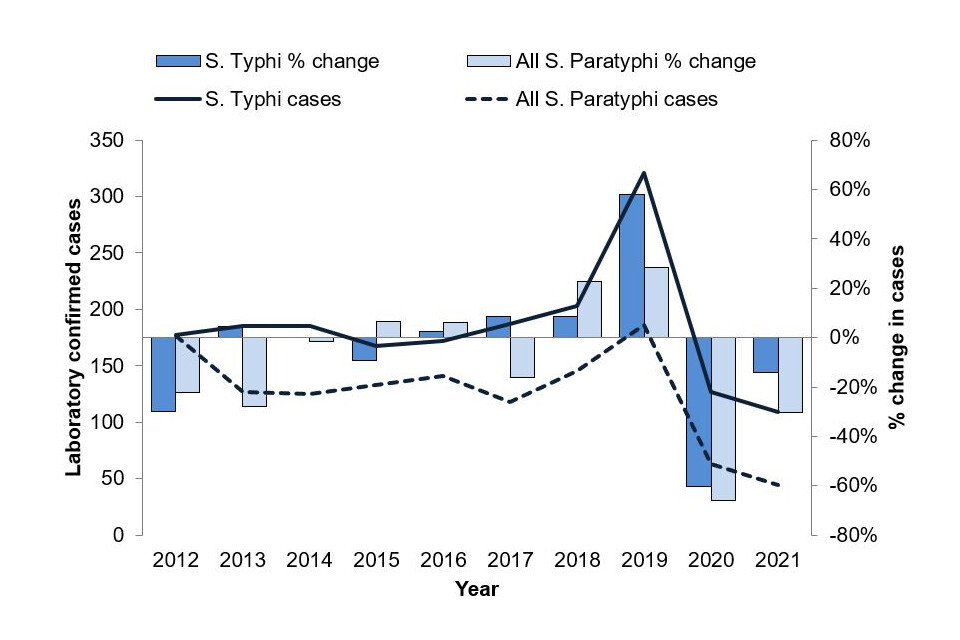
In 2021, 153 laboratory-confirmed symptomatic cases of S. Typhi and S. Paratyphi infection were reported by the UKHSA SRS in EWNI, which is a decrease of 19% when compared to the 190 cases reported in 2020 (see table 1 and figure 1). Cases of S. Typhi and S. Paratyphi increased by an average of 19% a year between 2017 and 2019 (range -3% to +46%), the largest increase occurring between 2018 and 2019. Following the beginning of the COVID-19 pandemic, however, cases have decreased in both 2020 (-63%) and 2021 (-19%) when compared to the previous year. In 2021, 71% of cases were caused by S. Typhi and 29% by S. Paratyphi A and B (see table 1). There were no cases of S. Paratyphi C reported in 2021.
From 2018 to 2020, the proportion of cases of enteric fever caused by S. Paratyphi B diagnosed in EWNI decreased from 5% to 3%. In 2021, despite an overall reduction in cases of enteric fever diagnosed in EWNI from 2020, the number of confirmed symptomatic cases of S. Paratyphi B more than doubled (13 cases) representing 9% of enteric fever cases, the highest proportion since 2015.
This increase has mainly been driven by a cluster of S. Paratyphi B in EWNI in returning travellers from Iraq, as detected by UKHSA (9). There were 14 confirmed cases (symptomatic and asymptomatic) S. Paratyphi B cases identified in 2021 and 11 of these were returning travellers from Iraq. Of these 11 cases, 5 were confirmed to be a part of the same 5-SNP cluster identified as outbreak strains by the GBRU. Analysis of enhanced surveillance questionnaires indicates that all of the cases who were part of this outbreak had visited the Kurdistan region of Iraq to visit friends and relatives, with the earliest travel date of 1 June to the latest return date of 6 October 2021. This time period coincides with the Islamic holiday Ashura where mass gatherings of thousands of people are known to occur, although none of the 11 cases who travelled to Kurdistan, Iraq reported attending a mass gathering event (9).
Table 1. Laboratory confirmed symptomatic cases of enteric fever, England, Wales and Northern Ireland by organism: 2012 to 2021
| Year | S. Typhi | S. Paratyphi A | S. Paratyphi B | S. Paratyphi C | Mixed infection | Total | % S. Typhi |
|---|---|---|---|---|---|---|---|
| 2012 | 177 | 162 | 12 | 2 | 1 | 354 | 50% |
| 2013 | 185 | 121 | 6 | - | - | 312 | 59% |
| 2014 | 185 | 114 | 10 | 1 | 1 | 311 | 59% |
| 2015 | 168 | 107 | 26 | - | - | 301 | 56% |
| 2016 | 172 | 133 | 8 | - | - | 313 | 55% |
| 2017 | 187 | 103 | 15 | - | - | 305 | 61% |
| 2018 | 203 | 126 | 19 | - | - | 348 | 58% |
| 2019 | 321 | 166 | 19 | 1 | - | 507 | 63% |
| 2020 | 127 | 57 | 6 | - | - | 190 | 67% |
| 2021 | 109 | 31 | 13 | - | - | 153 | 71% |
Figure 1. Laboratory confirmed cases of S. Typhi and S. Paratyphi, with % change year to year, England, Wales and Northern Ireland: 2012 to 2021
Age and sex
In 2021, sex was known for 149 out of 153 of the confirmed symptomatic cases and age was known for all of the confirmed symptomatic cases. 51% of the 153 cases were adults aged between 20 and 39 years (see figure 2) and the median age was 22 years (range 1 to 81 years). Those under 15 years accounted for 40% of cases, with 2% (3 cases) of the total in children under 2 years (and thus not routinely eligible for vaccination). Of the 149 cases where sex was known, there were slightly more male (55%) than female cases.
Figure 2. Laboratory confirmed cases of enteric fever, England, Wales and Northern Ireland by age and sex where sex is known: 2021 (total 149 cases)

Geographical distribution
Geographical areas were assigned based on patient postcode; in a small number of cases patient postcode was missing and the sending laboratory postcode was used. The largest proportion of English cases of S. Typhi and S. Paratyphi in 2021 were reported in London (36%), an increase on the previous year (29% in 2020) (see table 2). The largest relative decrease in cases reported in 2021 compared to 2020 was seen in the South West region (88%). London and Wales were the only regions that saw an increase in cases compared to the previous year.
Table 2. Laboratory confirmed cases of S. Typhi and S. Paratyphi, England, Wales and Northern Ireland by geographical distribution: 2020 and 2021
| Geographical area (UKHSA) | 2021 | 2020 | % change |
|---|---|---|---|
| London | 55 | 55 | 0% |
| North West | 24 | 35 | -31% |
| West Midlands | 18 | 30 | -40% |
| South East | 17 | 20 | -15% |
| Yorkshire and the Humber | 17 | 14 | 21% |
| East of England | 11 | 15 | -27% |
| East Midlands | 7 | 9 | -22% |
| North East | 1 | 2 | -50% |
| South West | 1 | 8 | -88% |
| England total | 151 | 188 | -20% |
| Wales | 2 | 1 | 100% |
| Northern Ireland | 0 | 1 | -100% |
| EWNI Total | 153 | 190 | -19% |
Disease presentation and outcomes
In 2021, symptom information was known for all cases. The most common symptom for all cases combined was fever (86%); followed by diarrhoea (67%); vomiting (48%); abdominal pain (45%); and headaches (43%). A higher proportion of S. Typhi cases reported having fever (89%) than S. Paratyphi cases (80%), as well as diarrhoea (70% S. Typhi compared to 61% S. Paratyphi), but cases of S. Paratyphi reported abdominal pain (55%) more often than S. Typhi (41%).
Where the data was available (115 out of 153 cases), more S. Typhi cases reported absence from work (70%) as a result of their illness than S. Paratyphi cases (66%). When figures for S. Paratyphi A and B are separated however, a similar proportion of S. Paratyphi B cases reported absence from work as S. Typhi cases (70%). Where data was available for length of absence (38 out of 115 cases), on average cases of S. Typhi reported missing at least 11 days of work as a consequence of their illness, while S. Paratyphi cases reported on average missing at least 14 days.
Where the data was available (150 out of 153 cases), more S. Typhi cases were admitted to hospital as a result of their illness (92%) than S. Paratyphi cases (88%). However, all 13 (100%) of S. Paratyphi B cases were admitted compared to 82% of S. Paratyphi A. Where the data was available for hospital length stay (107 out of 150 cases), on average S. Typhi and S. Paratyphi A cases had reported hospital length stay (LOS) of at least 4 days, compared to an average LOS of at least 6 days in S. Paratyphi B cases. This brings the average LOS for S. Paratyphi A and B cases to at least 5 days greater than the average for S. Typhi cases in 2021.
Travel history
In 2021, 99% (151/153) of symptomatic laboratory-confirmed cases of S. Typhi and S. Paratyphi had travel history information recorded (that is, whether they had travelled abroad or not) (see figure 3). In 2021, 87% (132 out of 151) of confirmed symptomatic cases with recorded travel history reported onset of illness within 28-days of travel to an endemic region of the world (and therefore were presumed to have acquired the infection abroad). This represents a decrease from 93% in 2020. Of cases in 2021, 118 out of 132 (89%) were UK residents and had travelled abroad from EWNI , while the remainder were new entrants to EWNI (11 cases) or foreign visitors to EWNI (3 cases). For 19 cases no foreign travel in the 28 days prior to becoming symptomatic was reported (an increase from 16 cases in 2020).
Figure 3. Laboratory confirmed cases of enteric fever, England, Wales and Northern Ireland by travel history: 2012 to 2021

Figure 4. Reason for travel for laboratory confirmed cases of enteric fever that travelled abroad from England, Wales and Northern Ireland: 2021 (total 118 cases)
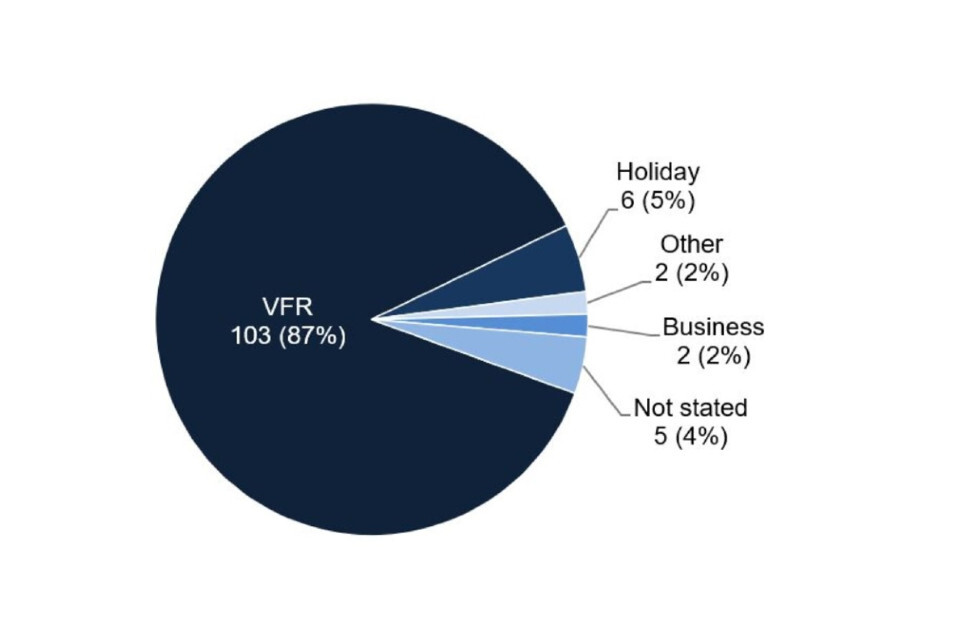
Where reason for travel was documented (113 cases), 91% of cases travelled abroad from EWNI to visit friends and relatives (VFR) (103 out of 113) (see figure 4). The majority travelled to countries in Southern Asia (see table 3) and acquired the infection while visiting friends or relatives abroad in Pakistan, India and Bangladesh.
Ethnicity was not known for 9 cases that travelled abroad to visit friends and relatives, these individuals travelled to Pakistan (4), India (4), and Iraq (1).
For those UK resident cases who did not visit friends and relatives (10 cases), where reason for travel was known the reasons provided included holidays (6), business (2), and other (2). Cases that did not travel to visit friends and relatives travelled to a number of countries, including Pakistan (3), India (1), Bangladesh (1), and countries in Africa (2), Europe (3) and the Americas (one), with some cases travelling to more than one country. For the 5 cases where reason for travel was not stated, 4 travelled to Pakistan and 1 to the USA.
Table 3. Countries of travel and ethnicity for laboratory confirmed cases of enteric fever that travelled abroad from England, Wales and Northern Ireland to visit friends and relatives: 2021 (total 103 cases)
| Presumed country of infection | Pakistani ethnicity | Indian ethnicity | Bangladeshi ethnicity | Asian other ethnicity | Black African ethnicity | White British ethnicity | Other or mixed ethnicity | Ethnicity not stated | Total |
|---|---|---|---|---|---|---|---|---|---|
| Pakistan | 55 | - | - | 1 | - | - | - | 4 | 60 |
| India | - | 22 | - | - | - | - | - | 4 | 26 |
| Bangladesh | - | - | 3 | - | - | - | - | - | 3 |
| Iraq | - | - | - | 7 | - | 1 | 1 | 1 | 10 |
| Africa | - | - | - | - | 3 | 1 | - | - | 4 |
| Total | 55 | 22 | 3 | 8 | 3 | 2 | 1 | 9 | 103 |
Since November 2016, Pakistan has had an ongoing outbreak of extensively drug-resistant (XDR) strain of S. Typhi in the Sindh province, with resistance seen to most antibiotics used to treat enteric fever, including ampicillin, chloramphenicol, co-trimoxazole (which confers multidrug-resistant (MDR) S. Typhi), fluoroquinolones and third generation cephalosporins (bla CTX-M-15 extended spectrum beta-lactamase (ESBL) producers) (10, 11).
Since 2019, the XDR strain has been found circulating in other areas of Pakistan and is no longer restricted to the Sindh province (11, 12).
Prior to the COVID-19 pandemic there had been an increasing trend of imported XDR S. typhi cases from Pakistan, with one case reported in 2017, 6 cases from 2018 and 34 in 2019 (10, 13).
In 2021, 21 cases of XDR S. Typhi were diagnosed in the UK that part of a 5-SNP cluster of cases imported from Pakistan, a slight decrease to 2020 when 27 cases were reported in the cluster. History of travel was known for 19 of these cases, of which 16 cases travelled abroad from the UK to Pakistan, representing 24% of all cases who travelled abroad from the UK to Pakistan. Of the remaining cases, one was a contact of a known enteric fever case, one had reported travel to Pakistan outside the 28-day period before symptom onset and the source for the third case was unknown. See clinical guidance for the management of these extensively drug-resistant cases.
Non-travel-associated cases
In 2021, there were 19 cases classified as non-travel-associated cases, these were confirmed cases of symptomatic enteric fever where the case reported that they did not travel in the 28 days prior to becoming symptomatic:
- 13 were caused by S. Typhi
- 5 were caused by S. Paratyphi A
- 1 was caused by S. Paratyphi B
Of the 19 non-travel-associated cases, 2 had contact with a family member or friend who had travelled to an endemic country. For 2 further non-travel-associated cases, potential sources of infection were identified as a possible non-household contact and a household contact who was a suspected chronic carrier (a chronic carrier is defined as a person who continues to excrete S. Typhi and S. Paratyphi for 12 months or more) (13). No potential source of infection was identified for the remaining 15, although 5 of these cases had returned from an endemic region more than 28 days before becoming symptomatic. In one of these cases, infection was discovered during treatment for another condition and may have represented chronic carriage. Two non-travel cases, one of whom was asymptomatic, were part of a 5-SNP cluster with 3 cases who reported travel to Pakistan.
Confirmed asymptomatic cases
In 2021, there were 6 confirmed cases of asymptomatic enteric fever caused by S. Typhi (5 cases) and S. Paratyphi B (1 case). Of these cases, 3 were non-travel-associated cases, one travelled to Iraq and one to Pakistan. Travel history was not known for the remaining case. Of the non-travel-associated cases, 2 were identified as chronic carriers having previous history of travel to Afghanistan in one instance, and to Zambia and the Democratic Republic of the Congo in the other. The additional case who did not travel is presumed to have acquired the infection from a family member with a history of travel. Of the asymptomatic cases who had not recently travelled, 2 were within the same 10-SNP cluster.
Probable and possible cases
In 2021, there were 15 probable cases of enteric fever as defined in the Public Health Operational Guidelines for Enteric Fever (14). Of these, all 15 travelled abroad from the UK. Travel history information for the probable and possible cases is detailed in table 4. Caution should be used when interpreting this data as it has not been confirmed by the UKHSA reference laboratory. There were no possible cases of enteric fever reported in 2021.
Table 4. Country of travel and reason for travel for probable and possible cases of enteric fever that travelled abroad from England, Wales and Northern Ireland: 2021 (total 15 cases)
| World region of travel | VFR | Holiday | Business | Total |
|---|---|---|---|---|
| Pakistan | 5 | - | - | 5 |
| India | 1 | 1 | 1 | 3 |
| Nigeria | 1 | 1 | - | 2 |
| Afghanistan | 1 | - | - | 1 |
| Cameroon | - | - | 1 | 1 |
| Ghana | 1 | - | - | 1 |
| Israel | - | 1 | - | 1 |
| Morocco | - | 1 | - | 1 |
| Total | 9 | 4 | 2 | 15 |
Information resources
NaTHNaC typhoid and paratyphoid fact sheet
NaTHNaC food and water hygiene advice
UKHSA typhoid and paratyphoid page
Typhoid: health advice for travellers (Asian languages)
Travelling overseas to visit friends and relatives – health advice
Gastrointestinal bacteria reference unit – reference and diagnostic services
References
- Cook GC and Zumla A. ‘Manson’s tropical diseases’ Elsevier Health Sciences 2009.
- Heymann DL. ‘Control of communicable diseases manual’ American Public Health Association 2008.
- Chattaway MA and others. ‘The transformation of reference microbiology methods and surveillance for Salmonella with the use of whole genome sequencing in England and Wales’ Frontiers in Public Health 2019, volume 7, page 317.
- Dallman, TJ and others. ‘SnapperDB: a database solution for routine sequencing analysis of bacterial isolates’ bioRxiv 189118 (viewed 7 February 2023).
- UK Health Security Agency. ‘Typhoid and paratyphoid: guidance, data and analysis’ - health protection collection (online) (viewed 7 February 2023).
- Office for National Statistics. ‘Coronavirus and the impact on the UK travel and tourism industry’ (online) (viewed 9 February 2023).
- Office for National Statistics. ‘International Passenger Survey’ (online) (viewed 9 February 2023).
- Office for National Statistics. ‘Overseas travel and tourism: 2020’ (online) (viewed 9 February 2023).
- Chattaway MA and others. ‘Genomic sentinel surveillance: Salmonella Paratyphi B outbreak in travellers coinciding with a mass gathering in Iraq’ Microbial Genomics 2023, volume 9.
- Nair S and others. ‘ESBL-producing strains isolated from imported cases of enteric fever in England and Wales reveal multiple chromosomal integrations of blaCTX-M-15 in XDR Salmonella Typhi’. Journal of Antimicrobial Chemotherapy 2021, volume 76, issue 6, pages 1459 to 1466.
- World Health Organization disease outbreak news item. ‘Typhoid fever - Islamic Republic of Pakistan’ (viewed 21 February 2023).
- Rasheed F and others. ‘Emergence of resistance to fluoroquinolones and third-generation cephalosporins in Salmonella Typhi in Lahore, Pakistan’ Microorganisms 2020, volume 8, page 1336 (viewed 21 February 2023).
- Chattaway MA and others. ‘Phylogenomics and antimicrobial resistance of Salmonella Typhi and Paratyphi A, B and C in England, 2016 to 2019’ Microbial Genomics 2021, volume 7, issue 8, 000633.
- Public Health England and the Chartered Institute of Environmental Health. ‘Public health operational guidelines for typhoid and paratyphoid (enteric fever)’ (viewed 7 February 2023).
-
As we only collect data from the UKHSA Salmonella Reference Service, local reports of cases of enteric fever may differ for Wales and Northern Ireland. ↩