HPR volume 11 issue 22: news (23 June)
Updated 15 December 2017

© Crown copyright 2017
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/health-protection-report-volume-11-2017/hpr-volume-11-issue-22-news-23-june
1. Fall in new HIV diagnoses among MSM at selected London sexual health clinics
Gay, bisexual and other men who have sex with men (MSM) account for half of all people living with HIV in England and are the group most at risk of acquiring HIV. The number of HIV diagnoses among MSM continued to rise from 2,413 in 2006 to a peak of 2,855 in 2014, with a further 2,648 diagnoses in 2015 [1]. However, in late 2016 and early 2017, media reports indicated that specific London sexual health clinics had observed a fall in HIV diagnoses in 2016 among MSM [2]. Public Health England undertook a rapid analysis of surveillance and monitoring data to confirm and explain this fall.
Between October 2014–September 2015 and October 2015–September 2016, new HIV diagnoses among MSM attending specialised sexual health clinics in England fell by 17% (from 2,060 to 1,707) and by 25% (from 1,227 to 915) in London. A 32% decline was observed among five major London clinics (from 880 to 595) compared with 8% at 30 other London clinics and 5% (from 833 to 792), in 191 clinics in the rest of England [3].
Since 2012, national guidelines have recommended up to three-monthly HIV testing for MSM at high risk of acquiring HIV [4]. Among the five clinics that observed a large-fall in HIV diagnoses, the number of HIV tests rose by 50% from 8,820 in January–March 2013 to 14,820 in July–September 2016. While the number of new testers (ie those not tested in the previous two years) was stable at around 5,000 per quarter, the number of repeat testers (ie those who had an HIV test within the previous two years) increased by 60%, from 4,800 to 9,760 (see figure). The three year rise in testing in the large-fall clinics coincided with an initial increase in HIV diagnoses during 2014, but in early 2015 the decline occurred predominantly in new testers. The median CD4 count at HIV diagnosis of men diagnosed at large-fall clinics increased substantially (from 469 in 2013 to 548 in 2015), indicating men were being diagnosed soon after infection. (In other London clinics, the number of new and repeat testers remained stable, and outside London, new and repeat testers increased equally, although there was no discernible effect on HIV diagnoses in either setting.)
Treatment guidelines now indicate ART regardless of CD4 count to prevent onward transmission (‘treatment as prevention’) [5]. Consequently, the number of men starting ART rose from 2,700 in 2013 to 3,600 in 2015. There has been a general reduction in the time to starting ART in those with a CD4 count >350, with the median time from diagnosed to ART substantially shorter at the five clinics that observed the decline in HIV diagnoses (120 days) compared with other London clinics (190 days) and clinics outside London (260 days). Consequently, the number of MSM with transmissible levels of virus (men who are undiagnosed, diagnosed but untreated or treated and not virally suppressed) reduced by 50% from 15,461 in 2013 to 10,184 in 2015..
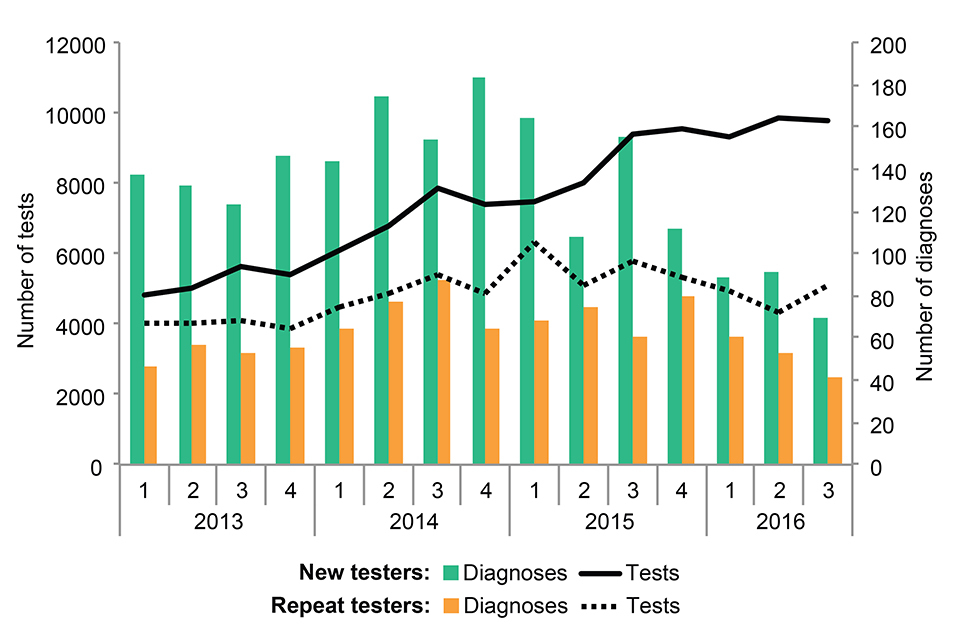
Number of HIV tests and diagnoses in MSM at London “large-fall” sexual health clinics, by new and repeat tests, 2013-2016
Available data suggest the number of MSM who began pre-exposure prophylaxis (PrEP) in England either as trial participants or via online purchase has been limited to date. Beginning in 2013, PrEP has been available to some MSM as part of the ‘Pre-exposure prophylaxis to prevent the acquisition of HIV-1 infection (PROUD)’ trial [6]. Although, all five clinics that observed a decline participated in the PROUD trial, three other clinics in London and five clinics outside London did so as well. If the large-fall in HIV diagnoses was predominantly due to PrEP, we would expect the decline to be most apparent in repeat HIV testers, whereas the fall mainly occurred in new testers (see figure).
The fall in HIV diagnoses in MSM at selected London sexual health clinics is a clear indication of the success of combination prevention. The volume of HIV tests across London combined with rapid treatment following diagnosis at the five London clinics is now likely to have reached a level that decreases the number of men with transmissible levels of virus thereby reducing transmission. The authors of the report on the London study [3] advocate replicating – nationally – the policy of intensive testing, especially repeat testing, adopted in the five London clinics studied (in addition to immediate ART) so as to achieve further substanital reduction in HIV transmission across the country.
1.1 References
- PHE (2016). HIV in the UK: 2016 report.
- NAM-aidsmap (2016). The UK’s largest sexual health clinic saw a 40% drop in new HIV infections this year.
- Brown AE, Mohammed H, Ogaza D, Kirwan PD, Yung M, Nask SG, et al (2017). “Fall in new HIV diagnoses among men who have sex with men (MSM) at selected Lonodn sexual health clinics since early 2015: Testing or treatment or pre-exposure prophylaxis(PrEP)?.” Euro Surveill 22(25), 22 June.
- BASHH and BHIVA (2012). UK National Guidelines on safer sex advice. The Clinical Effectiveness Group of the British Association for Sexual Health and HIV (BASHH) and the British HIV Association (BHIVA).
- Williams I, Churchill D, Anderson J, Boffito M, Bower M, Cairns G, et al (2014). BHIVA guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy 2012. HIV Medicine 15: 1–85.
- McCormack S, Dunn DT, Desai M, Dolling DI, Gafos M, Gilson R, et al (2016). Pre-exposure prophylaxis to prevent the acquisition of HIV-1 infection (PROUD): effectiveness results from the pilot phase of a pragmatic open-label randomised trial. Lancet 387: 53-60.
2. Measles outbreaks across Europe and the start of the summer festival season
There are currently several large measles outbreaks across Europe, with Romania and Italy being the worst affected countries. The World Health Organization (WHO) Regional Office for Europe has warned that this threatens progress towards elimination and urged national authorities to maximize efforts to achieve and/or sustain at least 95% coverage with two doses of measles, mumps, rubella (MMR) vaccine to prevent circulation in the event of an importation [1]. In response, the National Travel Health Network and Centre issued a reminder to travellers to ensure they are up to date with their MMR vaccination [2]. All WHO Regions have set targets for measles elimination by 2020 and although much progress has been made globally measles remains endemic in many countries [3].
Between 1 July 2016 and 31 May 2017 in England there were 27 confirmed measles importations, with limited onward transmission mainly among unimmunised or under-immunised household contacts (at least eight cases). Fourteen of the England importations were linked to travel within Europe, with Romania contributing the largest number of cases (eight of the 14 cases). Further importations to England are expected over the summer period with increasing travel to and from Europe and the rest of the world.
Also, PHE has previously reported 52 confirmed measles cases linked to music and arts festivals in England and Wales in 2016 [4]. Nearly half of these cases were among 15-19 year-olds. Several individuals who acquired measles at one festival that year subsequently attended another festival while infectious, resulting in multiple, interlinked outbreaks. Transmission within festivals resulted in a geographical spread of cases nationally as well as internationally.
PHE has reminded its Health Protection Teams to note the above when undertaking risk assessments of suspected cases this summer; also that, in order to monitor importations and chains of transmission, it is essential that every suspected case, including those confirmed locally, is tested with an oral fluid test, as per the National Measles Guidelines [5]. In addition HPTs are reminded to follow the measles guidance on international travel and travel by air [6].
2.1 References
- WHO Regional Office for Europe (2017). Measles outbreaks across Europe threaten progress towards elimination (press release, 27 March).
- NaTHNaC website (2017). Measles in Europe: a reminder for travellers to be up to date with measles vaccine (news story, 26 April).
- World Health Organization (2012). Global measles and rubella strategic plan: 2012-2020.
- le Polain de Waroux O, Saliba V, Cottrell S, Young N, Perry M, Bukasa A, Ramsay M, et al (2016). Summer music and arts festivals as hot spots for measles transmission: experience from England and Wales, June to October 2016. Euro Surveill 21(44).
- PHE website. National measles guidelines.
- PHE website. Measles: public health response to cases who have travelled by air whilst infectious.