Health Assessment Channels Research
Published 7 October 2024

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/health-assessment-channels-research/health-assessment-channels-research
DWP research report no. 1072
A report of research carried out by Ipsos on behalf of the Department for Work and Pensions. Crown copyright 2023.
You may re-use this information (not including logos) free of charge in any format or medium, under the terms of the Open Government Licence.
To view this licence, visit the National Archives
Or write to:
Information Policy Team
The National Archives
Kew
London
TW9 4DU
Email: psi@nationalarchives.gov.uk
This document/publication is also available on our website at: Research at DWP
If you would like to know more about DWP research, email: socialresearch@dwp.gov.uk
First published October 2024.
ISBN 978-1-78659-724-3
Views expressed in this report are not necessarily those of the Department for Work and Pensions or any other government department.
1. Executive summary
DWP conducted a Health Assessment Channels Trial to evaluate how well telephone and video assessments are working compared to face-to-face assessments. This report presents findings from mixed-method research conducted by Ipsos to understand the impact of the introduction of remote channels on claimant experiences.
1.1. Research design
This research comprises a multi-mode (online and CATI) survey conducted between the 3rd of March and 1st of May 2023. In total 7,262 responses were received from Personal Independence Payment (PIP), Employment and Support Allowance (ESA) or Universal Credit (UC) claimants who had an initial health assessment for their benefit between June 2022 and January 2023.
Key Drivers Analysis was run using the quantitative data. This identified which areas of the assessment were most important in determining participant agreement that that the assessor had understood their condition and how it affected their everyday life (for PIP claimants) or ability to work (for UC or ESA claimants). Sixty follow-up qualitative telephone interviews were also conducted to understand the assessment experience in more depth.
1.2. Findings
Findings from the quantitative survey, Key Drivers Analysis and qualitative interviews did not identify clear patterns in claimant beliefs that the assessor understood their health condition or disability, or that they had been able to explain this properly, by assessment channel (Section 6.6).
Rather, Key Drivers Analysis identified that perceptions of whether the assessor had understood their health condition or how it affected them were driven by agreement that:
- the questions which were asked allowed them to explain how their condition affected them
- the assessor had understood their application form and other evidence
- the assessor had listened to them during the assessment
The qualitative research found that positive interactions with an assessor were characterised by the assessor explaining the assessment process, having a high degree of confidence in the assessor’s ability to assess their condition and the assessment feeling tailored to their condition (or understanding the purpose of questions which felt less relevant).
This suggests that assessors should prioritise these behaviours. The evidence suggests that assessors can demonstrate these behaviours across all three assessment channels (face-to-face, telephone or video).
PIP claimants were more likely to express uncertainty about all the channels. This suggests that PIP claimants may need additional support or reassurance through the assessment process.
Claimants were more likely to agree a channel was suitable after experiencing it. Future preferences for assessment channel were strongly correlated to the channel claimants had experienced most recently. Participants who had a positive interaction with the assessor also had high confidence in their assessment channel (Section 7.2).
In the survey, awareness of the ability to change channel amongst trial participants was low. A minority of participants had changed from the assessment channel initially allocated for their assessment. The qualitative interviews identified that participants only changed their assessment channel when they could not attend the channel they had originally been allocated. They did this regardless of whether they recalled that they had been told they could change their assessment channel (Section 4.2).
When asked in the survey if they would like a choice of which channel their assessment is conducted by in the future, nearly nine in ten said that they would. In the qualitative research, offering a choice of assessment was seen as giving participants control over part of the process, empowering them. Participants felt they could choose the channel which they felt was appropriate for their condition and needs (Section 8.2).
Acknowledgements
This research was commissioned by the Department for Work and Pensions.
The authors would like to thank all of the people who gave their time to participate in this research.
We would also like to thank Deborah Grayson, Gursharan Gill, Abigail Holland and Bella Barton for their valuable input throughout the study.
2. Summary
2.1. Introduction
DWP commissioned Ipsos to conduct quantitative and qualitative research into the experience of respondents who had an initial health assessment as part of their benefit claim during the Health Assessment Channels Trial. DWP conducted the Health Assessment Channels Trial to evaluate how well telephone and video assessments are working compared to face-to-face assessments. The trial compares award outcomes across channels for people who have attended an initial Personal Independence Payment (PIP) assessment or Work Capability Assessment (WCA), who were eligible to attend all three channels, and whose assessment was automatically allocated to one of those channels. To understand the impact of the introduction of remote channels on claimants, DWP commissioned Ipsos to conduct a mixed-method study exploring claimant experiences. The trial and research will develop the evidence base on the use of different channels, inform wider implementation, assess value for money and determine next steps.
2.2. Study methodology
This research comprises a multi-mode (online and CATI) survey conducted between the 3rd of March and 1st of May 2023. In total 7,262 interviews were conducted with PIP, Employment and Support Allowance (ESA) or Universal Credit (UC) claimants who had an initial health assessment for their benefit between June 2022 and January 2023. The quantitative data was used to run a Key Drivers Analysis, to identify which areas of the assessment were most important in determining agreement that the assessor had understood their condition and how it affected them. As well as identifying the areas which were important to determining this, it identified how well the assessment experience was performing against these metrics.
Sixty follow-up qualitative telephone interviews were conducted to understand claimants’ assessment experience, and the role of assessment channel, in more depth.
2.3. Key findings
Information about the assessment
Over nine in ten (93%) recalled receiving information about their assessment before it took place. DWP was the most commonly recalled source of information and those who had a face-to-face assessment were most likely to recall receiving information from DWP. Participants recalled that the information related to the practicalities of attending the assessment, such as location, appointment length and the overall process.
Over eight in ten (81%) of claimants found the information provided by DWP or the assessment provider clear. There were no differences in the perceived clarity of information by assessment channel. However, ESA and UC claimants were more likely to have found the information clear than PIP claimants (Section 4.1).
A quarter of participants knew that they could ask for their allocated assessment channel to be changed. Overall, 12% had their assessment using a different channel to the one originally allocated, including those whose assessment channel was changed by the provider and participants who changed their assessment channel themselves. The qualitative interviews found that people requested to change assessment channel out of necessity, such as being unable to travel to a face-to-face appointment or take part in a video call, rather than preference (Section 4.2).
Perceptions before the assessment
Before receiving the invitation to the assessment, participants were more likely to be aware that they might need to have an assessment than why or what would happen. Awareness of the need to have an assessment was higher among PIP claimants (89%) than UC (82%) or ESA (81%) claimants (Section 5.1).
For most (at least six in ten) participants, knowing that the assessment could be carried out using telephone, video or face-to-face made no difference to their intention to make a benefit claim. Participants were most likely to say that knowing the assessment could be carried out face-to-face would make them less likely to apply whilst knowing that it could be carried out over the telephone would make them more likely to apply (Section 5.2.1).
Before the assessment, over half of participants felt that the assessor would be able to assess their condition very or fairly well using their assessment channel. Participants were most likely to express doubts about telephone or video assessments (38% each) and less so about face-to-face (28%). Across all channels, PIP claimants were least confident that an assessor would be able to accurately assess their condition (Section 5.2.2).
The qualitative interviews found that participants’ attitudes to claiming benefits shaped their attitudes towards the assessment. We identified three broad groups. The first group were reluctant to claim, and felt a stigma attached to doing so. They did not expect to receive a benefit award and expected the assessor to be hostile towards them (reflecting the stigma they attached to claiming). The second group included those who were uncomfortable about discussing their health condition. This group were at risk of leaving out important information or downplaying the severity of their condition. The third group had high confidence in being awarded their benefit claim and felt that this would validate the extent to which their condition affected them (Section 5.2.3).
Assessment experience
Nine in ten participants agreed that the appointment time they were offered was convenient and they were informed of this with time to prepare.
Despite this, six in ten said they were concerned about the assessment on the day. This was most likely amongst those who had a face-to-face assessment. PIP or UC claimants were more likely to be concerned than ESA claimants. The qualitative interviews found that the assessment was a significant event for participants which they found preparing for, and attending, stressful. Participants felt that more information about what would be covered in the assessment could help them to prepare and mitigate their anxiety about attending (Section 6.2).
The quantitative and qualitative strands identified that the interaction with the assessor was key to determining perceptions that the assessor had understood their condition. The qualitative interviews identified that feeling the assessor understood their condition helped ensure the legitimacy of the assessment, including for participants who were not given a financial award.
Overall, participants were most likely to agree that the assessor had treated them well. They were less likely to agree that they felt they had been able to explain how their condition affects them. Nine in ten agreed that the assessor treated them with respect and dignity through the assessment and the same proportion agreed that the assessor explained their role. Participants were less likely to agree that the questions asked were relevant and appropriate (74%) or that they allowed them to fully explain the impact of their condition (70%). Fewer were likely to agree that they had been able to explain how their health condition affects their daily life and / or ability to work (68%) or that the assessor understood this (61%). Experiences were consistent across assessment channels. PIP claimants were consistently less positive across all measures than ESA or UC claimants (Section 6.5).
The Key Drivers Analysis (KDA) identified that feeling listened to, feeling that the assessor had read and understood their application form, and being asked relevant questions, determined agreement that the assessor had understood their condition. Assessment channel did not play a role in this. In the analysis, DWP was performing strongly across these measures.
The qualitative interviews identified several characteristics of a positive assessment experience:
- the assessor introducing themselves and explaining their professional background
- the assessor explaining the purpose of the assessment and that not all questions would be relevant
- the assessor demonstrating that they had read the application form in advance
- participants understanding the questions and feeling able to answer them accurately, with support and further explanation from the assessor if needed
- the assessment feeling tailored to the individual’s needs and condition
Participants who had these experiences were more likely to feel positively about the assessment overall.
Together, the KDA and qualitative findings show the importance of the participant’s interaction with the assessor in determining agreement that their health condition, and how it affects them, had been understood. This identifies behaviours and actions for assessors to prioritise (Section 6.6).
Around two thirds of participants felt that their assessment channel was suitable. This was consistent across channels. PIP claimants were least likely to see their assessment channel as being suitable, across all assessment channels. This suggests that perceived suitability is related to the needs of PIP claimants rather than the channel (Section 6.9).
Having an assessment using a particular channel influenced perceptions of suitability. Claimants were more likely to see a channel as suitable after they had had an assessment using it, than before the assessment (Section 6.9).
Assessment outcomes and satisfaction
PIP claimants were most likely to know their assessment outcome at the point of the survey (91% compared to 82% of ESA claimants or 83% of UC claimants). They were also least likely to be satisfied with their outcome (44% compared to 69% of ESA and 71% of UC claimants).
There were no significant differences in satisfaction with outcomes between the different assessment channels (just over half for each channel). However, claimants who had a video assessment were more likely to be dissatisfied with the outcome of their assessment (43%) than those who had a face-to-face assessment (37%). There were no significant differences in dissatisfaction between either of these channels and those who had a telephone assessment (39%).
Those who were satisfied with their assessment outcome were more likely to agree that the assessor had understood their condition and how it affects their daily life or ability to work (Section 7.1).
Qualitative findings showed that claimant perceptions of the suitability of their assessment channel depended on how well they felt the assessor had understood their health condition. There was a relationship between claimants’ satisfaction (or dissatisfaction) with the interaction with assessor and their satisfaction (or dissatisfaction) with their award outcome.
Claimants who felt their assessment channel was more suitable than expected after receiving their award outcome were more likely to have had an assessment using remote channels. This group were likely to have been uncertain about having an assessment through a remote channel prior but felt positively about their interaction with the assessor following the assessment.
Claimants who felt that their assessment channel was less suitable than expected after receiving their award outcome were more likely to have had an assessment using remote channels and be dissatisfied with both their interaction with the assessor and award outcome. These claimants felt that the remote assessment channel had not enabled them to fully demonstrate how their condition affected them (Section 7.2).
Channel choice
When asked in the survey, 86% of participants said they wanted a choice of how their future assessments were carried out. Future preference for channel was closely correlated with the channel which participants had experienced for their most recent assessment.
In the qualitative interviews, participants felt that being offered a choice of assessment would enable them to choose the channel which they felt was appropriate for their condition and which would help them to best manage the emotional impact of the assessment. Participants felt that this would give them a sense of control and empowerment over the process (Section 8.2).
2.4. Conclusions
Findings from the quantitative survey, Key Drivers Analysis and qualitative interviews did not identify clear patterns in claimant beliefs that the assessor understood their health condition or disability, or that they had been able to explain this properly, by assessment channel.
Rather, Key Drivers Analysis identified that perceptions of whether the assessor had understood their health condition or how the participant’s disability affected them were driven by:
- being asked questions which allowed them to explain how their condition affected them
- feeling that the assessor had understood their application form and other evidence
- feeling listened to during the assessment
The qualitative research found that positive interactions with an assessor were characterised by the assessor explaining the assessment process, having a high degree of confidence in the assessor’s ability to assess their condition and the assessment feeling tailored to their condition (or understanding the purpose of questions which felt less relevant).
This suggests that assessors should prioritise these behaviours. The evidence suggests that assessors can demonstrate these behaviours across all three assessment channels (face-to-face, telephone or video). PIP claimants were more likely to express uncertainty about all the channels. This suggests that PIP claimants may need additional support or reassurance through the assessment process.
Claimants were more likely to agree a channel was suitable after experiencing it. Future preferences for channel were strongly correlated to the channel claimants experienced most recently. Participants who had a positive interaction with the assessor also had high confidence in their assessment channel.
Overall awareness of the ability to change assessment channel was low, and a minority of participants had changed the channel for their assessment. The qualitative interviews identified that participants only changed their assessment channel when they could not attend the channel they had originally been allocated. They did this regardless of whether they recalled that they had been told they could change channel.
When participants were asked about future choice, nearly nine in ten said they would like a choice of which channel their assessment is conducted using in the future. In the qualitative research, offering a choice of assessment was seen as giving participants control over part of the process, empowering them. Participants felt they could choose the channel which they felt was appropriate for their condition and needs.
3. Background and Methodology
3.1. Research background
Government financial support is available for people who are ill or have a health condition or disability which affects their ability to work or who have extra living costs because of their disability or health condition. People with limited capability for work and work-related activity (LCWRA) can claim an additional amount of Universal Credit (UC). New Style Employment and Support Allowance (ESA) is available to people who are ill or have a health condition or disability which affects their ability to work and who have been working within the last 2 to 3 years and have made (or been credited with) Class 1 or Class 2 National Insurance Contributions (NICs) before the year they are claiming in.
Personal Independence Payment (PIP) can help people with extra living costs if they have a long-term physical or mental health condition or disability and experience difficulty doing certain everyday tasks or getting around because of their condition. PIP is not income-related or means tested and people can claim PIP whilst they are in work.
As part of the claim process for UC LCWRA, ESA or PIP, claimants complete an application, provide evidence of how their health condition affects them and commonly have a health assessment.
DWP conducts around 1.9 million health assessments each year. Before the COVID-19 pandemic, 80% of assessments were conducted face-to-face and 20% were based on a review of application forms and supporting evidence. During the COVID-19 pandemic face-to-face assessments were stopped and remote health assessments by telephone and video were introduced, reflecting the social distancing regulations in place and the health vulnerabilities of these claimants. This represented a significant change to practice for DWP and claimants.
DWP conducted the Health Assessment Channels Trial to evaluate how well telephone and video assessments are working compared to face-to-face assessments. The trial has compared award outcomes across channels for people who have attended an initial PIP assessment or Work Capability Assessment (WCA), who were eligible to attend all three channels, and whose assessment was automatically allocated to one of those channels. To understand the impact of the introduction of remote channels on claimants, DWP commissioned Ipsos to conduct a mixed-method study exploring claimant experiences.
3.2. Research aims
The aim of this research was to understand what impact assessment channel had on claimant experience. It aimed to provide evidence on how claimant experience differed according to assessment channel and claimant characteristics, allowing DWP to consider the merits of each channel.
The quantitative survey explored:
- whether and how channel affected the claimant experience of the assessment
- the extent to which claimants felt able to convey what they needed to the assessor during their assessment and whether this was influenced by channel
- the extent to which there is claimant appetite for channel choice or change and whether this varies by claimant group or characteristics
- what the barriers are to having an assessment using the different channels
The qualitative strand explored the experience of participants in greater depth, specifically:
- claimant experiences of the assessment
- experiences of having an assessment using each of the channels in detail
- why customers perceived their assessment as being easier or more difficult than expected
- how the assessment experience influenced perceptions of channel suitability
- how the assessment influenced future channel preferences
- channel perceptions and preferences
- whether claimants saw the different assessment channels as fulfilling different roles
- what role the claimant’s personal context and benefit claim had in determining channel preferences
- what role changes to how other types of appointment are delivered had on attitudes towards choice of channel for these assessments
- how claimants balance speed of assessment or choice of assessment channel
- channel choice
- why some customers requested to change assessment channel
- why customers want a choice of assessment channel and how this may shape attitudes towards the assessment
- how being offered a choice of assessment channel could affect customers
3.3. Research design
A mixed methodology was used for this research, comprised of a quantitative survey and follow up in-depth qualitative interviews.
3.3.1. Quantitative survey
A stratified random sample of claimants who attended an initial health assessment between June 2022 and January 2023 was chosen for the survey. The sample was stratified by assessment type and channel to ensure inferences could be made about these subgroups in the wider population. Those for whom DWP held an email address were sent an email inviting them to take part in the survey online. Those for whom DWP held only a postal address were sent a letter inviting them to take part in the survey online. Both communications set out the different ways in which participants could take part in the survey if an online survey was not suitable or accessible for them. Participants who did not reply to the invitations to take part in the survey and did not ask to be removed from the research were contacted over the telephone to complete the survey.
A stratified sampling approach was used to ensure that there were sufficient sample sizes amongst each of the different benefit types for sub-group analysis and to allow for analysis at the total population level. Weighting was used to achieve a sample profile representative of the different benefit types at the total level and the age and gender profile for each benefit.
The quantitative survey achieved 7,262 responses completed either online or over the telephone between 3 March and 1 May 2023. The following numbers of responses were achieved with each benefit type:
- 4,370 Personal Independence Payment claimants
- 2,153 Universal Credit claimants
- 739 Employment and Support Allowance claimants
Full details of the sampling and weighting approach are in Appendix A.
3.3.2. Qualitative interviews
Ipsos conducted follow-up in-depth interviews with 60 purposively selected survey participants who had completed the quantitative survey. This comprised:
- 30 Personal Independence Payment claimants
- 15 Universal Credit claimants
- 15 Employment and Support Allowance claimants
Interviews were held either online (using MS Teams) or over the telephone. All interviews took place between 13th July – 17th August 2023 and lasted up to 45 minutes.
Full details of the achieved sample are in Appendix B.
3.3.3. Analysis and interpretation of the data
The survey data was weighted by gender, age and benefit type based on DWP data on the trial population. Only findings from the survey which are statistically significant at the 95% confidence level have been reported in the commentary (although charts and tables may include non-statistically significant differences). All tables and charts report weighted data but include the unweighted base.
The final data from the survey is based on a weighted subset of the Health Assessment Channels Trial population, rather than the entire population. Percentage results are therefore subject to margins of error which vary with the size of the sample and the percentage figure concerned. Where figures do not add to 100 per cent, this is due to rounding or because the question allows for more than one response. Where base sizes are less than 100, percentages have not been reported and findings should be treated with caution. All quantitative findings are aggregated, and no individual participant can be identified.
Qualitative research is detailed and exploratory. It offers insights into people’s opinions, feelings and behaviours. All participant data presented should be treated as the opinions and views of the individuals interviewed. Quotations from the qualitative research have been included to provide rich, detailed accounts, as given by participants. The qualitative interviews were follow up interviews with those who had completed the quantitative survey and given consent for Ipsos to contact them again for this purpose.
Qualitative research is not intended to provide quantifiable conclusions from a statistically representative sample. Owing to the sample size and the purposive nature with which it was drawn, qualitative findings cannot be considered representative of the views of the trial population as a whole. Instead, this research was designed to explore the breadth of views and experiences to develop a deeper understanding of the experiences of having a health assessment during the trial period.
3.3.4. Reporting notes
In this report, ‘participant’ is used to refer to DWP customers who had an initial health assessment as part of their PIP, ESA or UC claim during the trial period and completed the survey and / or took part in a qualitative interview. In some cases, an appointee responded to the survey or qualitative interview on behalf of the claimant.
4. Information about the assessment and channel change
This chapter presents findings about where participants recalled receiving information about their assessment from, what they recalled about these communications and how easy or difficult they were to understand. It goes on to cover participant understanding of their ability to change their assessment channel and motivations and behaviours in relation to doing so.
4.1. Information about assessment
4.1.1. Overall source of information
Over nine in ten (93%) recalled receiving information about their assessment prior to it taking place. DWP was the most commonly recalled source of information (37%) and a quarter had received information from friends and family (26%). As shown in Figure 4.1.1, one in ten recalled receiving information from their work coach (12%), the assessment provider (11%), or a charity (10%). Social media (8%), the UC journal (8%), and local authorities (5%) were less commonly used sources of information. A small percent of participants (4%) did not recall receiving any information about the assessment.
Participants who had a face-to-face assessment were more likely to recall receiving information from DWP (43%) than those whose assessments took place over a video (41%) or telephone call (39%). Participants who had a telephone or video assessment were more likely to remember receiving information from friends and family (27% and 26% respectively) than those who had face-to-face (23%) assessments.
Younger participants (aged 18 to 24) were more likely than the total population to turn to friends and family for information (39%, compared to 26% overall).
Figure 4.1.1 Sources of information participants recalled receiving information about the assessment from
| Source | Percentage |
|---|---|
| DWP | 37% |
| Friends and family | 26% |
| Other | 20% |
| Work Coach | 12% |
| Assessment provider | 11% |
| Charity | 10% |
| Social media | 8% |
| UC Journal | 8% |
| Local authority | 5% |
| Didn’t get information about the assessment | 4% |
| Don’t know | 3% |
B3. Before your assessment where did you/they get information about it from?
Base: All respondents (7,262). Percentages do not sum to 100% as claimants may have received information from multiple sources.
4.1.2. Information provided
Participants who received information or advice from DWP or the assessment provider commonly said that the advice they received related to the logistics of attending the assessment. Around two thirds said they had received information about how the assessment would be held (65%), how long the assessment would last (64%), how long the process takes from start to finish (62%) and what the overall assessment process involved (62%). This is shown in figure 4.1.2.
Figure 4.1.2 Information provided by the DWP / assessment provider
| Information | Percentage |
|---|---|
| How the assessment would be held | 65% |
| How long the assessment will last | 64% |
| How long assessment process takes from application to receiving decision | 62% |
| What the overall assessment process involves | 62% |
| How you would be informed about the decision after assessment | 61% |
B4. What type of information or advice did you/they get from DWP or the assessment provider?
Base: All those who received information from DWP/the assessment provider (2,984)
As shown in Figure 4.1.3, eight in ten (81%) participants who received information or advice from DWP or the assessment provider reported that they found this information clear. However, around a sixth said the information or advice provided was unclear (17%).
Over eight in ten participants found the information provided by DWP or the assessment provider very (38%) or fairly (43%) clear. Fewer than two in ten participants found the information not very (13%) or not at all (4%) clear. There were no differences in perceived clarity of information by assessment channel. There were differences by benefit type. ESA and UC claimants were more likely than PIP claimants to have found the information clear (84% and 82% respectively, compared to 79%, see Figure 4.1.4).
Figure 4.1.3 Clarity of information provided by the DWP / assessment provider about the assessment process
| Clarity | Percentage |
|---|---|
| Not at all clear | 4% |
| Not very clear | 13% |
| Fairly clear | 43% |
| Very clear | 38% |
B5. How clear or not was the information you/ they got from DWP/ the assessment provider about the assessment process? Base: All those who received information from DWP/the assessment provider (2,984)
Figure 4.1.4 Clarity of information provided by the DWP / assessment provider about the assessment process by benefit claimed
| Benefit | Not at all clear % | Not very clear % | Fairly clear % | Very clear % |
|---|---|---|---|---|
| PIP | 4% | 15% | 44% | 35% |
| ESA | 3% | 11% | 43% | 41% |
| UC | 5% | 10% | 40% | 42% |
B5. How clear or not was the information you/ they got from DWP/ the assessment provider about the assessment process? Base: All those who received information from DWP/the assessment provider (2,984)
In the qualitative interviews participants felt that the advance information they received gave them the practical and logistical details they needed to attend the assessment. Those who had an in-person assessment recalled information about the time and date of the appointment, and address of the assessment centre. Those who had a video call assessment recalled being sent the link to join the assessment appointment and how to check that they could log on to the online session. Those who had a telephone call had received information that someone would call and when. In addition to this practical information, participants would have welcomed more information about the types of questions which would be asked. Participants felt that this would have helped them prepare for the content of the assessment and help to mitigate any worry they felt before attending. Participants acting as an appointee for a claimant were also likely to feel that the claimant would have benefitted from being able to prepare for the content of the assessment.
Female, 45 to 54, PIP, In-person assessment, said:
The leaflet was useful - instructions around the time, the location and that the meeting was to understand how my illness affected me, directions and that you could claim for travel expenses.
Participants in the qualitative interviews, across all assessment channels, who had received a text message reminder of their appointment time identified that this had been particularly useful.
Male, 18 to 24, ESA, Telephone assessment, said:
And two days before, I got a text reminder. I think that’s really good, I’d give the system 9/10. That definitely made me feel more comfortable, it allows for the fact you might have forgotten about it.
Female, 35 to 44, UC, Video call assessment, said:
I also got confirmation in the post and reminders by text. That was brilliant, very useful.
Participants who discussed their assessment with someone before having it spoke about the practicalities of attending, the assessment channel (for video assessments only) and the emotional impact of the assessment. Participants were particularly likely to have discussed the practicalities of attending if they needed support to attend their assessment channel. For example, those attending a face-to-face assessment discussed travel arrangements, such as getting a lift or arranging a taxi. Those having a video assessment who needed support with logging on had discussed this. Participants who did not have someone who supported them and wanted additional information before the assessment went to GOV.UK.
Female, 55-64. ESA, In-person assessment, said:
Did discuss with my family, as I needed someone to take me and just be around after…. [I] didn’t need anyone in the room with me though, as I would feel judged.
Male, 45-54, UC, Video call assessment, said:
Spoke to dad about it, and he helped out, we logged in [to the assessment link] about 20 mins before to ensure it was all working.
For video assessments specifically, participants whose family or friends had recently attended a health assessment discussed having their assessment using this new channel, which they had not been aware of before.
Beyond the practicalities of attending, participants discussed the emotional impact of the assessment. The health assessment was a significant event for participants which could lead to feelings of anxiety. Those who were claiming because of a mental health condition were particularly likely to feel anxious about attending the assessment. As identified above, more information on the content of the assessment, such as the questions which would be asked was seen to be helpful in mitigating this anxiety.
Female, 45-54, PIP, In-person assessment, said:
I discussed it with my fiancé because I’m not very good at expressing myself in words, I’m very emotional and have severe anxiety, so [I] was worried about leaving the house and very anxious about the upcoming assessment.
4.2. Channel change
Claimants having a health assessment can request to change their assessment channel. In the quantitative survey, three quarters of assessments were conducted over the telephone (76%), 13% face-to-face and 10% over a video call. Two per cent of participants said they didn’t know which assessment channel was used.
4.2.1. Awareness of channel change
A quarter (25%) of participants were aware that they could change their assessment channel. Overall, 12% had their assessment using a different channel from the one they were originally offered, including those whose assessment channel was changed by the assessment provider.
Excluding those who said their assessment was changed by DWP or the assessment provider, around half who changed their assessment had originally been offered an in-person assessment (48%), a similar proportion had been offered a video call (45%) and 7% a telephone assessment. Nearly all (90%) of those who changed assessment channel changed to a telephone assessment.
UC claimants (15%) were most likely to have had a different assessment type from that originally offered, followed by ESA (12%) and PIP claimants (11%).
Awareness of the ability to change channel was highest among older participants, with 30% of those aged 65 or over saying they knew this was the case. Just over two in five (22%) of 25 to 34 year olds were aware they could request an alternative assessment channel.
In the qualitative interviews, awareness of the ability to change channel varied widely. No clear patterns in awareness of this were identified.
4.2.2. Process of changing assessment channel
Overall, seven in ten (71%) participants who changed their assessment channel reported the process of doing so was easy (this excludes those who said that DWP or the assessor changed their assessment channel). As shown in Figure 4.2.1, over four in ten (45%) said the process of changing the assessment channel was very easy and around a quarter (26%) fairly easy.
Figure 4.2.1 Ease of changing assessment channel
| Ease | Percentage |
|---|---|
| Very difficult | 6% |
| Fairly difficult | 6% |
| Fairly easy | 26% |
| Very easy | 45% |
C5. How easy or difficult was it for you/them to change the type of assessment you/they had? Base: All who changed assessment channel (829)
As shown in Figure 4.2.2, participants who had a telephone assessment were most likely to have found changing assessment channel easy. Three quarters (73%) found it very or fairly easy. Around six in ten of those who had a video assessment (62%) or in-person assessment (59%) found it easy to change assessment channel.
Figure 4.2.2 Ease of changing assessment channel by channel attended
| Channel | Very difficult % | Fairly difficult % | Fairly easy % | Very easy % | Very/Fairly easy % |
|---|---|---|---|---|---|
| In person | 12% | 16% | 28% | 31% | 59% |
| Telephone | 6% | 5% | 26% | 47% | 73% |
| Video call | 9% | 9% | 30% | 32% | 62% |
C5. How easy or difficult was it for you/them to change the type of assessment you/they had? Base: All who changed the type of assessment (829)
ESA claimants found the process of changing their assessment channel easier than other benefit claimant types. Fifty-six percent of ESA claimants said they found the process ‘very easy’, compared to 46% of UC claimants and 42% of PIP claimants. See Figure 4.2.3. Older participants were more likely to find the process of changing their assessment channel easier, with 48% of those aged 55 and over saying they found the process ‘very easy’.
Figure 4.2.3 Ease of changing assessment type by benefit claimed
| Benefit | Very difficult % | Fairly difficult % | Fairly easy % | Very easy % | Very/Fairly easy % |
|---|---|---|---|---|---|
| PIP | 7% | 6% | 28% | 42% | 70% |
| ESA | 4% | 5% | 23% | 56% | 79% |
| UC | 5% | 6% | 24% | 46% | 70% |
C5. How easy or difficult was it for you/them to change the type of assessment you/they had? Base: All who changed the type of assessment (829)
4.2.3. Reason for changing assessment channel
The two most common reasons why participants had an assessment using a different channel than originally offered were a) the channel was changed by the assessment provider (23%),or b) the participant did not feel able to attend using the original channel because of their health condition (22%). Other reasons included being anxious about completing the assessment in that way (15%), technical issues (14%) or being unable to travel to the assessment centre (11%).
ESA claimants (32%) were most likely to change their assessment type because of their health condition. This applied to around a quarter (23%) of PIP and just under one in five (18%) of UC claimants. Findings from the qualitative interviews reinforced the survey findings. Participants who changed their assessment channel did so for reasons related to their ability to attend that channel rather than simply preference.
Participants said they requested a change of assessment channel if they could not attend the original channel they were allocated, for example, they were unable to travel to the appointment or join an online video assessment. In the qualitative sample, no participants who were allocated a telephone assessment requested to change their assessment channel. As such, participants in this position requested to change channel, regardless of whether they knew or recalled being told that they could. Participants who were aware of the possibility of changing their assessment channel did so out of necessity rather that preference. If they were able to attend using their originally allocated channel, they did so.
Male, 55-64, PIP, Video call assessment, said:
I didn’t know how to use the technology to do a video call and didn’t have any technology, [computer or iPad or smart phone] so wouldn’t know where to start to have an online call. So [I] phoned the number on the letter and changed it to a phone call which was not difficult.
Qualitative research participants who had a poor preconception of DWP, and recalled information about being able to change assessment channel, did not always think that this offer was genuine. They believed that the offer of being able to change assessment channel was to identify ‘troublemakers’.
Male, 25-34, Universal Credit, Video call assessment, said:
I think it probably makes them [assessor] more hostile if you ask to change [assessment channel].
5. Participant perceptions before the assessment
This chapter discusses participants’ initial awareness of the assessment process, awareness of the different assessment channels available and expectations and attitudes towards the assessment.
5.1. Awareness of the assessment process
5.1.1. Awareness of the need to have an assessment
Before receiving the invitation to the assessment, participants were more likely to be aware that they might need to have an assessment than why or what would happen. Nearly nine in ten participants were aware that they might need to have an assessment (86%), compared to eight in ten (80%) who knew why they might need to have one, and nearly seven in ten (67%) who knew what might happen.
As shown in Figure 5.1.1, awareness of the need to have an assessment was higher among PIP claimants (89%) than ESA (81%) or UC (82%) claimants. PIP claimants were also more aware of the purpose of the assessment (81%) than ESA (76%) and UC (79%) claimants.
Participants were less likely to feel well informed about what would happen at their assessment. Two in three (67%) reported being aware of what happens; this was again higher for PIP claimants (69%) than ESA (61%) or UC (64%) claimants, and higher for female participants (70% compared to 63% of males).
Figure 5.1.1 Awareness of needing an assessment, why they need an assessment, and what happens at the assessment by benefit claimed
| Benefit | That you/the person you are claiming for might need to have an assessment % |
|---|---|
| PIP | 89% |
| ESA | 81% |
| UC | 82% |
| Benefit | Why you/the person you are claiming for might need to have an assessment % |
|---|---|
| PIP | 81% |
| ESA | 76% |
| UC | 79% |
| Benefit | What happens at an assessment % |
|---|---|
| PIP | 69% |
| ESA | 61% |
| UC | 64% |
B1A. Before you/they received an invitation to the assessment were you/they aware… %Yes Base: All respondents (7,262)
5.1.2. Awareness of the assessment channels
The majority of trial participants (83%) were aware that the assessment could be conducted over the telephone, and three quarters (75%) were aware that it could be held in-person. Fewer (56%) were aware that assessments could be held over a video call.
PIP claimants were more likely than ESA and UC claimants to know that the assessment could be conducted over the telephone. 85% of PIP claimants were aware that the assessment could be held over the telephone, compared to 79% of ESA and 78% of UC claimants. This is shown in Figure 5.1.2
Figure 5.1.2 Awareness of the channels available to conduct the assessment by benefit claimed
| Benefit | That the assessment may be held in person % |
|---|---|
| PIP | 76% |
| ESA | 71% |
| UC | 74% |
| Benefit | That the assessment may be held on the telephone % |
|---|---|
| PIP | 85% |
| ESA | 79% |
| UC | 78% |
| Benefit | That the assessment may be held on a video call % |
|---|---|
| PIP | 85% |
| ESA | 79% |
| UC | 78% |
B1A. Before you/they received an invitation to the assessment were you/they aware… %Yes
Base: All respondents (7,262)
5.2. Perceptions of assessment channels
5.2.1. Impact of channel on claim behaviour
Participants who were aware that the assessment could be carried out using each of the assessment channels were asked what impact, if any, this channel had on their likelihood of making a claim. Figure 5.2.1 shows that for around six in ten, knowledge of the different assessment channels available to them had no impact on their likelihood of applying.
Overall, knowing the assessment may be held in-person had the biggest impact on the likelihood of applying for a benefit. Whilst 61% said it would make no difference, 19% of participants said it would make them more likely to apply for the benefit and 16% said this made them less likely to apply.
Figure 5.2.1 Impact of awareness of assessment channels on likelihood of making a benefit claim
| Channel | Much less likely % | Little less likely % | Makes no difference % | Little more likely % | Much more likely % |
|---|---|---|---|---|---|
| Knowing assessment may be on a video call | 5% | 7% | 62% | 7% | 16% |
| Knowing assessment may be on the telephone | 4% | 4% | 60% | 9% | 20% |
| Knowing assessment may be in person | 7% | 9% | 61% | 6% | 14% |
B2. What impact did the following have on your/ their likelihood to apply for [Benefit]? Base: All respondents who were aware of each assessment channel (video: 4,127, telephone: 5,877, in-person: 5,493)
A greater proportion of people claiming PIP (17%) said that the assessment being conducted in-person made them less likely to apply than those claiming ESA (10%) or UC (14%).
Younger participants were most likely to say that having a face-to-face assessment would make them less likely to apply. About three in ten (31%) of those aged 18 to 24 and 25% of those in the 25 to 34 age group said that a face-to-face assessment would mean they were less likely to apply, compared to 4% of participants aged 65 or more. Similarly, people with psychiatric disorders (26%), anxiety and/or depression (21%) or any sensory disability or health condition (also 20%) were less likely to apply if this required attending an in-person assessment. In the qualitative research, these groups were more likely to find an in-person assessment difficult to attend.
Telephone assessments were considered the most accessible channel. Nearly three in ten (29%) said this made them more likely to apply for the benefit (60% no difference, 8% less likely). This was particularly the case for the groups who with psychiatric disorders (35%), anxiety/depression (32%), and younger participants (37% of 18 to 24s and 35% of 25 to 34s).
Around a quarter (23%) said that knowing they could have a video assessment made them more likely to apply. To 62% it made no difference. 12% said it made them less likely to apply. Differences by condition, disability, or age were less marked for this channel.
5.2.2. Expectations of the assessment channel
Participants were asked about their expectations of having an assessment using the channel using which their assessment was conducted. Prior to the assessment, over half of participants felt that the assessor would be able to assess their condition very or fairly well using the assessment channel their assessment was conducted using. However, a substantial minority expressed doubts about this. This was particularly the case for telephone and video calls (38% in each case). Fewer participants (28%) expressed concern about the accuracy of face-to-face assessments (Figure 5.2.2).
Figure 5.2.2 Confidence in the assessor’s abilities to assess their condition or disability accurately
| Channel | Don’t know % | Not at all well % | Not very well % | Fairly well % | Very well % | Very/Fairly easy |
|---|---|---|---|---|---|---|
| In person | 8% | 16% | 22% | 32% | 22% | 54% |
| Telephone | 13% | 11% | 17% | 31% | 27% | 58% |
| Video call | 8% | 17% | 21% | 34% | 20% | 54% |
C8. Before you/they had the assessment, how accurately did you/they think the assessor would be able to assess your/their health condition or disability?. Base: Respondents whose assessment was conducted via each channel (Telephone 4,904; In-person 1,163; Video call 1,105).
Across all channels, PIP claimants were least confident that the assessor would be able to accurately assess their condition. Overall, half of PIP claimants (50%) thought the assessor would be able to assess their condition very or fairly well using their assessment channel, whilst 43% believed they would not. Comparatively, ESA and UC claimants were more confident that the assessor would be able to assess their condition very or fairly well (64% and 61% respectively), and fewer thought this would be not very well or at all well (28% and 27% respectively).
5.2.3. Attitudes towards the assessment
In the qualitative interviews, participants described how the assessment was a significant experience for them. Participants’ attitudes towards the assessment before having it related to how they felt about their condition and making a benefit claim. In our sample, there were three broad attitudes to the benefit claim and the assessment:
- reluctance to claim benefits
- discomfort discussing their health condition
- high confidence in being awarded benefits
These attitudes fed into anxiety about the assessment either because of the uncertainty it caused, discomfort discussing their condition and/or importance of receiving an award.
Participants who were reluctant to claim described feeling like a failure or guilty for needing to claim benefits. These claimants usually had an extensive work history and described feeling that others were in greater need than them and should be prioritised above them. Seeing themselves as less deserving of a benefit award, this group demonstrated uncertainty about whether they would receive one. There were examples of participants in this group who said others had recommended they claim benefits, rather than claiming proactively. Some in this group demonstrated attitudes which suggested they saw claiming benefits as being stigmatised. Participants who were unwilling to claim or embarrassed about doing so worried about feeling judged by the assessor.
Female, 35 to 44, UC, In-person assessment, said:
I thought they [assessor] were there to punish me, because I’m not working, and to have a go at me because I’m not working.
Participants who felt uncomfortable discussing their health condition were either uncomfortable acknowledging the impact of their health condition(s) or found it difficult to talk about their condition and their need to claim. For example, one male claimant who was claiming PIP because of the effects of Multiple Sclerosis felt uncomfortable talking about this.
Male, 45 to 54, PIP, Video call assessment, said:
Maybe it’s a male pride thing…and the [assessor] was female and younger…When asked questions like how far I can walk without crutches. I double the length that I could actually walk… Speaking to a young girl…I was embarrassed to reveal that I can’t walk far…MS can also lead to bladder control issues. Now it’s really hard to say that to a stranger when you can see their face.
A claimant whose health conditions had been caused by being physically attacked also experienced Post Traumatic Stress Disorder (PTSD). He found it very difficult to discuss how his health conditions affected him because this brought back traumatic memories of when he had been attacked. This group also included those whose parents were acting as their appointee. In these cases, the appointee described the difficulty the claimant had in attending appointments and assessments. For example, one parent who was an appointee for her son reported that he become distracted and agitated during the assessment so had to leave.
Those who were confident that they would receive a benefit award were more likely to know someone else who was claiming PIP, ESA or in the UC LCW or LCWRA conditionality group. This led them to feel confident about their likelihood of receiving an award, as they compared their experiences to those of their friend or family member. There were also people in this group who had done research online into what the criteria for receiving a PIP award are, and felt they met them. As a result, they strongly believed they would receive an award. These participants felt that receiving an award would validate the extent to which their health condition affected them.
Attitudes towards, and anxiety about, the assessment intersected with assessment channel for some types of claimants. For example, those with some mental health conditions, such as anxiety, were more likely to prefer a telephone assessment to an in-person or video assessment. These participants felt that attending an in-person assessment, which would mean travelling and being around people they didn’t know, could exacerbate their condition. Some participants with these types of conditions also found taking part in a video assessment difficult for similar reasons. Participants with physical health conditions were also likely to find attending an in-person assessment difficult. They expressed concern about the practicalities of attending and the potential impact on their health. Participants who lacked digital confidence wanted support with attending the assessment and were more likely to prepare for this in advance, or get support, than more digitally confident participants. Attitudes towards the assessment channel intersected with previous experiences with DWP and subsequent expectations of what the interaction would be like. Participants who had neutral attitudes tended to have had little experience of the benefits system and no or few preconceptions. In contrast, those who had negative attitudes had heard negative stories about engaging with DWP, either through word of mouth or in the press. They believed that the assessor would be biased against giving them an award. There was no relationship between the assessment channel the participant attended and pre-existing attitudes towards DWP.
6. The assessment experience
This chapter covers participant’s overall experience of having a health assessment including the practical elements of preparing for the assessment and their thoughts and feelings during the assessment. This chapter also outlines the findings from Key Drivers Analysis to identify the factors which underpin agreement that the assessor understood their health condition or disability.
6.1. Preparation on the day of the assessment
When participants recalled how they felt on the day of their assessment, the majority felt satisfied that they had the information they needed to attend their assessment. Nine in ten (90%) agreed the appointment time was convenient and 92% that they were informed of this time early enough to give them time to prepare. Participants were less likely (75%) to agree that they knew who to contact if they had questions or needed to rearrange the appointment.
As shown in Figure 6.1, of those who attended an in-person assessment, two thirds (67%) agreed this was in a location they could get to easily; three in ten (31%) disagreed.
Figure 6.1 Perceptions before the assessment
| Perception | Strongly disagree % | Tend to disagree % | Tend to agree % | Strongly agree % | Don’t know % |
|---|---|---|---|---|---|
| The apppointment time I was offered was convenient for me/them | 3% | 4% | 34% | 57% | 3% |
| Informed of the assessment time in enough time to make preparations | 3% | 3% | 29% | 62% | 3% |
| I/they knew who to contact to ask questions or rearrange appointments | 9% | 9% | 22% | 53% | 7% |
| DWP made it clear that it is allowed to bring someone to the assessment | 9% | 9% | 22% | 53% | 7% |
| The face-to-face assessment was in a location that I/they could get to easily | 17% | 15% | 26% | 42% | 1% |
C9. To what extent do you agree or disagree with each of the following statements…? Base: Statements _1 to _4 all respondents (7,262); statement 5 all who were invited to an in-person assessment (1,163)
In the qualitative interviews, participants discussed making both general and channel specific preparations for their assessments. Across all channel and benefit types it was clear that the assessment was a significant event for participants. They placed great importance on arriving at or joining the assessment on time. This meant planning how they would attend and, for those joining remote sessions, making sure they were undisturbed. Participants wanted to be able to answer the assessor’s questions in detail. Reflecting this, almost all discussed ensuring that they had their medication and/or medical documents with them for the assessment. Participants who had an in-person assessment discussed organising transport and looking into travel routes and timings to the assessment centre. This included booking taxis, checking public transport routes or arranging a lift.
Those with lower digital confidence were likely to prepare in advance for a video call. This group discussed setting up their laptop or tablet before the assessment and testing joining the call. In some cases, this included getting support from a friend or family member to give the participant confidence that they would be able to join on time and reduce the risk of technical difficulties. Those with high digital confidence did not feel the need to prepare as they knew how to use the video call application and were confident they could join the call successfully.
Those who had a telephone assessment were least likely to describe making specific preparations, although one participant described changing their shift at work to ensure they were in a quiet area to receive the call.
6.2. Concerns on the day of the assessment
Across all benefit types and assessment channels, 6 in ten (60%) participants said they had been either very or fairly concerned about attending the assessment on the day.
Participants who attended an in-person assessment were most likely to have been concerned about it in advance (68%). Those who had a video (60%) or telephone (59%) assessment were equally likely to have been concerned about this.
People claiming ESA were less likely to feel concerned on the day than those claiming PIP or UC. Half (50%) reported feeling concerned, compared to around 6 in ten PIP (61%) or UC (62%) claimants.
Concern was higher among younger participants. Two thirds (66%) of those aged 18-24 reported feeling concerned about attending the assessment on the day compared to 44% of those aged 65 or over. Levels of concern were higher than average among participants with a psychiatric disorder (76%), anxiety/depression (68%) or a sensory disability or condition (67%).
Two fifths (41%) of participants with a psychiatric disorder thought the assessor would not be able to assess their health condition accurately, followed by 39% of those with a sensory disability or 38% of participants with anxiety and depression.
6.3. Participants who had a companion for the assessment
Participants were allowed to bring someone else to the assessment with them if they wanted to. Three quarters (75%) were aware of this, although 18% disagreed that DWP had made it clear that they could do this and 7% were not sure.
Overall, nearly three in ten (27%) participants took someone with them to their assessment. Those who had a face-to-face assessment were most likely to take a companion with them to the assessment (45%), compared to 31% for video and 24% for telephone assessments.
PIP claimants (29%) were more likely to have taken someone with them to the assessment than UC claimants (26%), who were in turn more likely to have done so than ESA claimants (20%).
Taking a companion was most common among those with sensory disabilities or conditions (34%) or psychiatric disorders (33%), and participants under the age of 25 (48%).
Figure 6.3 shows the proportion of participants who took someone with them into the assessment, by benefit type and channel.
Figure 6.3 Proportion of participants who had a companion for the assessment
| Assessment | Percentage |
|---|---|
| PIP – Telephone | 26% |
| PIP – In person | 50% |
| PIP – Video call | 32% |
| ESA – Telephone | 17% |
| ESA – In person | 35% |
| ESA – Video call* | 21% |
| UC – Telephone | 22% |
| UC – In person | 42% |
| UC – Video call | 28% |
C13. Did you/they take anyone into the assessment room/ask someone to join the telephone assessment/ask someone to join the video call with you/them? %Yes Base: All respondents (7,262) *Caution small base (90)
The most common reasons participants took a companion with them to their assessment were to support them with needs associated with their disability (69%), to provide moral support and company (58%), or help with the information needed to answer questions (52%). A third (34%) said their companion was there to answer questions on their behalf, around a quarter were there to take notes (27%) or to ask questions (24%). The qualitative interviews supported this, with participants sharing that the main reasons for taking someone with them to a face-to-face or video assessment was for either emotional or practical support.
In the qualitative interviews, experiences in the assessment depended on whether the companion was a formal appointee or not. Formal appointees reported that the way the assessor conducted the assessment reflected their formal role and that they were able to speak on behalf of the claimant. For example, one mother who was her son’s appointee reported that her son found the video assessment experience very challenging. Reflecting this, the assessor allowed the claimant to leave the assessment and for his mother, the appointee, to conclude the assessment without him present.
Participants took informal companions either to help better explain aspects of their condition to the assessor or to help them (the participant) better understand the assessor’s questions. In these cases, participants reported that informal companions were not able to respond on their behalf or that assessors could become frustrated if the companion tried to help the participant understand the questions. This came as a surprise to participants, as they had expected their companion would be able to fulfil this role. This suggests there is a need for greater clarity about the role informal companions can play during an assessment.
Female, 45 to 54, PIP, In-person assessment, said:
She [the assessor] was very abrupt and asked a lot of questions that I didn’t understand, so I kept looking at my fiancé and asking him to put them in a language that I could understand and sometimes he answered for me. I think she was getting a bit frustrated because I kept doing that.
6.4. Challenges attending the assessment
Around a third (35%) of participants reported experiencing some form of challenge attending the assessment on the day. Those who had a face-to-face assessment were most likely to report difficulties attending – over half (55%) reported at least one challenge. These were most commonly challenges related to accessing the assessment centre. Nearly a quarter (24%) of those who attended in-person reported difficulties accessing the assessment centre due to their health condition and a similar proportion (22%) had transport difficulties. In the qualitative interviews, the difficulties attending the assessment centre included having to park far away from the entrance to the assessment centre which was difficult for people with mobility difficulties; difficulty finding the assessment centre when driving; or not being able to access the assessment centre using public transport. The latter experience created a challenge to attending for those without a car.
Of those who had a video call, over four in ten (43%) reported at least one difficulty attending. The most common difficulty for this group was the assessor running late (17%). A similar proportion (15%) had difficulties using the video call technology or difficulties with their internal connection (15%). Around one in eight (12%) reported that the call was of poor quality.
Just over 3 in ten (31%) of those who had a telephone appointment reported at least one challenge attending, the lowest proportion of all channels. The most common challenge was delays to their appointment time (12%). Less than one in ten (9%) reported the call was of a poor quality, and 4% that the assessor called unexpectedly.
In total, 13% of participants reported delays to their appointment time as a challenge they experienced on the day. This was most common for face-to-face assessments (18%) or video calls (17%) and less common for telephone appointments (12%). In the qualitative interviews, participants who spoke about experiencing delays to their appointment described that this added to the anxiety they already felt about having the assessment. Those who had an in-person assessment reported having to wait in uncomfortable waiting rooms. If it was too hot or too cold this exacerbated their health condition, making the assessment harder for them.
Male, 35 to 54, PIP, said:
The waiting room was uncomfortable, and this was stressful. The assessment did not go well.
Participants who had video appointments reported waiting for up to 40 minutes for an assessor to join the video call without any communication about the delay or when their appointment would be held.
Male, 25 to 34, UC, said:
There was [sic] no tech issues, you were given a timeframe of when the appointment is but there was an additional 30-minute delay in starting…But you weren’t told why you were delayed or how long, you just sat there staring at a blank screen for the host to come on. This caused internal frustration…It is not the individual’s [assessor’s] fault and I tried not to feel antagonistic about it.
Some participants who had telephone appointments reported having to wait for up to two hours for the assessor to call.
Female, 55 to 64, UC, said:
The nurse rang me to say she was running late by one and a half hours…The hanging about then made me even more nervous, my stomach was in knots…I hate waiting, it just worked me up even more.
In all cases, delays to the assessment caused nervousness and anxiety for the participants. This seems to have been more pronounced for those having remote assessments, as they had no communication about why their appointment was delayed, when it would take place, or how to contact the assessor to find out when it would be. For nearly seven in ten (68%) participants who experienced a challenge attending their assessment, the appointment went ahead on the same day, using the original assessment channel. Less common consequences of challenges attending the assessment included the assessment being carried out through a different channel (9%) or being given a new date or time for the appointment (8%).
6.5. Interactions with assessor
Findings from both the quantitative and qualitative strands found that a participant’s interaction with their assessor determined how well they felt the assessor had understood their condition. This was the case across all assessment channels.
The quantitative survey found that participant’s ratings of the way the assessor communicated with them during the assessment were generally positive, as shown in Figure 6.5. In total, nearly nine in ten (89%) participants agreed the assessor treated them with respect and dignity throughout, and the same proportion that the assessor had explained what their role was in the assessment. The majority (86%) agreed the assessor had explained the assessment purpose and structure before starting.
Most participants were positive about their understanding of what they were being asked to do (82%). Of those who had a face-to-face or video assessment, fewer (54%) agreed that the measurements and functional tests that were carried out were relevant and appropriate. This question was not asked of those who had a telephone assessment as these activities are not included in telephone assessments.
Eight in ten (80%) said their communication and language needs were considered. Just over three quarters (76%) agreed they felt listened to during the assessment, and a similar proportion (75%) that they had enough time to explain how their condition affects them.
Three quarters (74%) agreed that the questions asked by the assessor were relevant and appropriate and a similar proportion (71%) agree they allowed the participant to fully explain the impact of their condition on their ability to work or their day-to-day life. Seven in ten (70%) said the assessor had understood their application form and supporting evidence.
Figure 6.5 Perceptions of the assessment experience
| Perception | Strongly agree % | Tend to agree % |
|---|---|---|
| The assessor treated me/them with respect and dignity during the assessment | 66% | 23% |
| The assessor explained what his/her role was | 59% | 30% |
| The assessor explained the purpose and structure of the assessment before starting | 57% | 29% |
| I/they understood what I/they were being asked about being asked to do | 50% | 32% |
| My/their communication and language needs were considered | 52% | 28% |
| I/they felt listened to during the assessment | 52% | 24% |
| I/they had enough time during the assessment to explain how my/their condition affects me/them | 50% | 25% |
| Questions were relevant and appropriate to my/their condition | 46% | 25% |
| Assessor had understood application form and supporting evidence | 47% | 23% |
| Relevant and appropriate measurements and functional tests were carried out | 35% | 19% |
C15. Please tell me to what extent you agree or disagree with each of the following statements about the assessment? Base: All respondents (7262) except “Relevant and appropriate measurements” statement: Respondents who had received an in-person or video call assessment (924)
Experiences were consistent across telephone, in-person and video call assessments.
Differences in attitudes were present amongst claimants of different benefit types. PIP claimants were less positive and were less likely to agree that:
- the assessor explained their role (88%, compared to 91% of ESA claimants and 90% UC)
- the assessor treated them with dignity and respect (87% compared to 93% of ESA claimants and 92% UC)
- they felt listened to during the assessment (71% compared to 85% of ESA claimants and 83% UC)
- their communication and language needs were taken into consideration (77%, compared to 85% of ESA claimants and 84% UC)
- the assessor understood their application form and other evidence (65%, compared to 79% of both ESA and UC claimants)
- they were asked relevant and appropriate questions (69%, compared to 82% of both ESA and UC claimants)
- the questions asked allowed them to explain the impact of their condition (66%, compared to 80% of ESA claimants and 79% UC)
- they had enough time to explain how their condition affects them (70%, compared to 84% of ESA claimants and 83% UC)
- they understood what was being asked of them (80%, compared to 90% of ESA claimants and 85% UC).
6.6. Assessors’ understanding of how the participants’ condition affected their daily life or ability to work
Participants were asked the extent to which they agreed that they were able to explain how their condition affects their daily life or ability to work, depending on the benefit they had an assessment for, and that the assessor understood this. PIP claimants were asked in relation to how their condition affected their day-to-day life and ESA and UC claimants in relation to their ability to work, reflecting the purpose of the different benefit types. This perception underpins the perceived efficacy, and therefore legitimacy, of the assessment.
Overall, around two-thirds of participants (68%) agreed they had been able to explain how their health condition affects their daily life or ability to work, and around six in ten (61%) agreed their assessor understood this. Assessment channel had no impact on the extent to which participants agreed with these statements.
Reflecting their lower positivity about the assessment experience overall, PIP claimants were less likely to agree with either statement. Around six in ten (62%) agreed they had been able to explain how their health condition affected them compared to around eight in ten ESA (80%) and UC (77%) claimants. PIP claimants were also less likely to agree that the assessor had understood the impact of their condition. Around half agreed with this (52%) compared to around three quarters of ESA (75%) claimants and UC (76%) claimants.
Figure 6.6 Agreement that the assessor understood their condition and how much it affected them
| Statement | PIP – Telephone | PIP – In person | PIP – Video call | ESA – Telephone | ESA – In person | ESA – Video call* | UC – Telephone | UC – In person | UC – Video call |
|---|---|---|---|---|---|---|---|---|---|
| Assessor understood condition and how it affects daily life/ability to work % | 53% | 49% | 52% | 75% | 78% | 74% | 77% | 77% | 82% |
| How much do you agree or disagree with the following statements – I/they was able to explain how healthy condition affects daily life/ability to work % | 62% | 58% | 61% | 80% | 81% | 83% | 79% | 78% | 85% |
C25_A. How much do you agree or disagree with the following statements… Base: All respondents (7262) *Caution small base (90)
6.6.1. Factors which underpin agreement that the assessor understood the impact of their condition
Key Drivers Analysis
Key Drivers Analysis (KDA) is a statistical technique used to identify the most significant factors which influence a particular outcome. In this study, KDA was used to understand which experiences during the assessment had the most impact on participants’ agreement that the assessor understood their condition. The analysis found that being asked questions which allowed the participant to explain the impact of their condition was the single most important factor driving agreement, followed by the assessor having understood the application form or other evidence. The third most important factor was feeling listened to during the assessment. In the analysis, DWP was performing strongly on all of these variables, as shown in the top right green box in Figure 6.6.1 below. The KDA diagram below also shows further measures on which DWP was performing strongly but had less impact on agreement that the assessor understood their condition: the assessor explaining his / her role, the assessor explaining the purpose and structure of the interview, the assessor treating the claimant with respect and dignity, and understanding what they were being asked to do during the assessment.
Figure 6.6.1 Key Drivers Analysis to understand what drives participant agreement that the assessor understood their condition
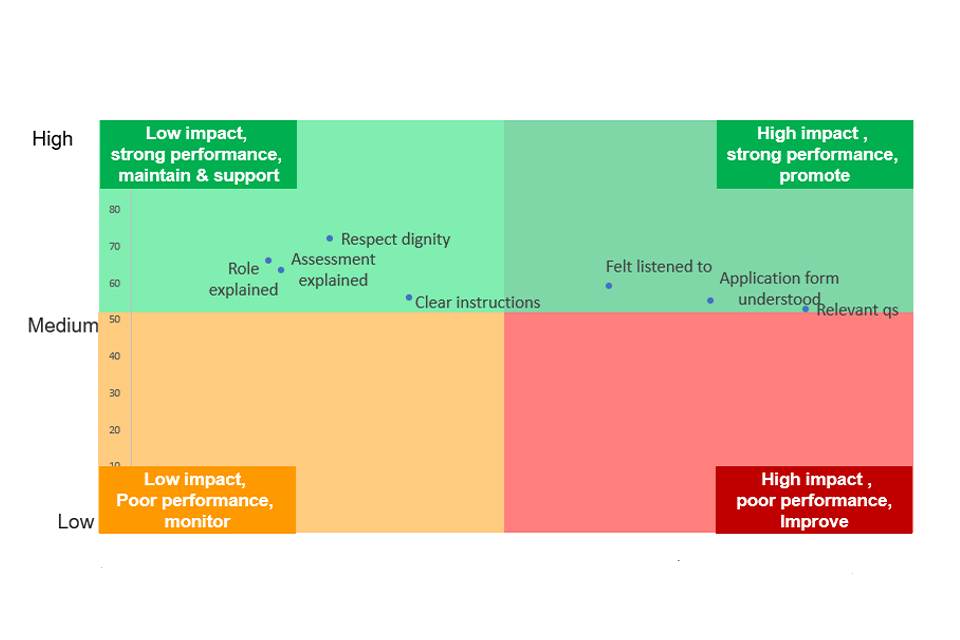
Assessment channel was used in the analysis for the KDA but was not found to have any impact on determining that the assessor understood their condition.
Qualitative findings
The qualitative findings showed that if participants felt that the assessor understood their condition and how it affected them, they were more likely to report that their assessment was a positive experience. This was the case for all assessment channels. This research found that where participants had a positive assessment experience, they were more likely to accept the outcome of their assessment.
The qualitative interviews identified several determinants of a positive assessment experience, defined as one in which the participant felt the assessor had understood their condition.
Firstly, when assessors introduced themselves and explained their professional background, this gave legitimacy to the assessor’s ability to understand the participant’s condition. Establishing this at the outset meant the assessment got off to a positive start for participants. In contrast, when assessors did not provide this background, the assessment lacked legitimacy from the outset.
When assessors explained the purpose of the assessment, and that not all of the questions asked would be relevant to their condition or circumstances, this helped participants to understand why particular questions were being asked. Understanding this meant participants were less likely to feel frustrated about being asked questions which were not relevant to their condition. They were less likely to perceive the assessment as a bureaucratic requirement and more likely to see it as adding value to DWP’s understanding of their condition. Without this explanation, participants who were asked irrelevant questions felt that the assessor had not read their application form or did not understand their condition.
Participants felt positively towards assessors who demonstrated that they had read their application in advance by referring to this during the assessment. This helped participants feel that the assessment was building on, rather than duplicating, the information they had provided in the application form.
When participants understood the questions being asked and were able to answer them accurately, they had a more positive perception of the assessment than if they did not understand the questions or found providing accurate answers difficult. For example, participants with conditions which fluctuated reported finding it difficult to know how to answer questions during the assessment. When an assessor explained to these participants that they should answer about their worst day, they found the questions easier to answer and were satisfied they had answered to the best of their ability. Participants who did not get this support found it harder to give an answer they were happy with. This demonstrates the role the assessor can play in helping participants give answers to the questions which they feel fully explain their condition and how it affects them.
When the assessor tailored the assessment to the participant’s needs this contributed to the belief that the assessor understood their condition. For example, when an assessor did not ask participants in face-to- face or video assessments to complete certain functional assessments if it was clear they were unable to do so. During telephone assessments, some assessors did not ask certain questions if they felt the participant had already covered this area sufficiently.
Female, 35 to 44, UC, In-person assessment, said:
[The assessor] said I can see you’re in pain, so I’m not going to make you stand up and walk around, you’ve got to walk back out yet so I’m not even going to attempt to get you to do anything. I did say to her I will try and she said ‘no, I’m not going to make you’.
If, at the end of the assessment, the participant felt that they had been listened to and that the assessor understood their condition and how it affected them they were more likely to feel positively about the assessment overall.
Together, the KDA and qualitative findings show the importance of the participant’s interaction with the assessor in driving agreement that the assessor understood their condition. The qualitative findings showed that this was essential to ensuring the assessment was seen as legitimate and helping participants accept the outcome of their assessment, regardless of whether they received an award.
6.7. Comfort sharing information about their health condition or disability
Overall, around two-thirds (65%) said they felt either “fairly” or “very” comfortable sharing the details of their health condition or disability. This was not affected by the assessment channel (66% for telephone assessments and 65% for both in-person and video call assessments). There were differences depending on the benefit being claimed, their age and the type of condition. ESA claimants were most likely to say they felt comfortable (76%), followed by UC claimants (69%). PIP claimants were considerably less likely to say they felt comfortable sharing details of their health condition or disability with the assessor (62%). PIP claimants were also least likely to feel that the assessor would be able to assess their condition accurately, across all channels and most likely to have taken someone with them to the assessment. Differences in comfort sharing information about their health condition or disability were evident across all channels (see Figure 6.7.1).
Figure 6.7.1 Comfort sharing details of health condition/disability
| Assessment | Fairly comfortable % | Very comfortable % |
|---|---|---|
| Total – total | 35% | 30% |
| PIP – Telephone | 35% | 28% |
| PIP – In person | 31% | 27% |
| PIP – Video call | 34% | 27% |
| ESA – Telephone | 32% | 44% |
| ESA – In person | 34% | 47% |
| ESA – Video call* | 39% | 39% |
| UC – Telephone | 39% | 31% |
| UC – In person | 35% | 35% |
| UC – Video call | 41% | 34% |
C18. During the assessment, how comfortable or uncomfortable did you/they feel about sharing the details of your/their health condition / disability? Base: All respondents (7,262) *CAUTION small base (90).
Just over half (52%) said that there had not been anything in the assessment which they wanted to explain but weren’t able to, suggesting that they had been able to explain everything they wanted to during the assessment. Four in ten said there had been things they had wanted to explain during the assessment which they weren’t able to (39%). This was consistent across all channels (video call 41%, telephone 39%, in-person 38%). PIP claimants were more likely to report having had things they weren’t able to explain during the assessment (46%, compared to 28% of UC claimants and 25% of ESA claimants.), as shown in Figure 6.7.2.
Figure 6.7.2 Agreement they/claimant were unable to explain things in the assessment
| Assessment | Percentage |
|---|---|
| PIP – Telephone | 46% |
| PIP – In person | 50% |
| PIP – Video call | 47% |
| ESA – Telephone | 25% |
| ESA – In person | 26% |
| ESA – Video call* | 31% |
| UC – Telephone | 29% |
| UC – In person | 27% |
| UC – Video call | 23% |
C19. Were there things you/the person wanted to explain at the assessment which you/they weren’t able to?
Base: All respondents (7,262) *Caution small base (90)
Half of all participants living with a psychiatric disorder said there were things they wanted to explain at the assessment but were not able to (49%), significantly higher than the average and all other condition types. This suggests that more could be done to ensure the assessment is appropriate for this group, that they are supported to explain their condition and that people with this type of condition fully understand the support they can receive.
Participants aged 25 to 34 years old were more likely to report that they had things they wanted to explain but were not able to (45%, higher than participants both younger and older than this).
People who said that there were things they had wanted to explain and had not been able to were more likely to feel it was not clear that they could bring someone to the assessment with them. Nearly six in ten (58%) of those who felt there were things they had wanted to explain but had not been able to also disagreed that DWP had made it clear that they could bring someone to the assessment and around a third (34%) agreed.
The most common reason given for not being able to explain all they wanted to during the assessment was that they had not been asked the right questions (47%). A quarter (25%) said they forgot to mention it, and 22% said they ran out of time. One in nine put it down to not having someone in the assessment with them (12%) and one in ten (10%) reported that the assessor was intimidating.
6.8. Participant perceptions of the ease or difficulty of the assessment
Participants were asked whether their experience of the assessment was easier, more difficult or as they expected. Participants were most likely to say their overall experience of the assessment was as expected (46%). Around three in ten participants (29%) thought it was more difficult, compared to two in ten who thought it was easier (19%). There were no differences by assessment channel. This is shown in Figure 6.8.1.
PIP claimants were more likely to find the overall assessment experience more difficult than expected (36%, compared to 19% of ESA claimants and 18% claiming UC). As shown in Figure 6.8.1, this was the case irrespective of the channel used for the assessment.
Figure 6.8.1 Perceptions of whether assessment was easier or more difficult than expected, by assessment channel and benefit claimed
| Assessment | Easier than expected % | More difficult than expected % |
|---|---|---|
| PIP – Telephone | 15% | 36% |
| PIP – In person | 14% | 35% |
| PIP – Video call | 17% | 34% |
| ESA – Telephone | 23% | 18% |
| ESA – In person | 19% | 20% |
| ESA – Video call* | 34% | 23% |
| UC – Telephone | 26% | 18% |
| UC – In person | 27% | 18% |
| UC – Video call | 33% | 13% |
C21. Thinking about the assessment itself, was your/their overall experience of the assessment…
Base: All respondents (7,262) *Caution small base (90)
The top two reasons for finding the assessment easier than expected included having a friendly (70%) and/or helpful (64%) assessor. Over half (54%) selected that they found it “less stressful than expected”. Around half (48%) said it had been good to speak to someone about the effects of their condition. Nearly a third (32%) found the assessment less intrusive than they had expected and three in ten (28%) had found the assessments and tests easier than expected. A quarter (25%) found it less tiring, 20% found it shorter than expected, and 19% found it less medical than they had expected. One in nine (11%) said it was easier than expected due to support from the person they had brought with them.
Participants with psychiatric disorders were more likely than average to find the experience more difficult than expected (36%).
The most common reason for finding the assessment more difficult than expected was that it was stressful (65%). Just over four in ten (43%) said they had been unable to present information or evidence; this was particularly the case for PIP claimants (47%). A similar proportion (41%) reported finding it more tiring than expected, whilst a quarter (24%) found it intrusive. Around a quarter (24%) reported the assessor had been “unhelpful” whilst 14% rated them as “unfriendly”. Around one in five (19%) reported they found the assessment more difficult than expected because they didn’t have anyone with them to help; 17% said the assessments and tests were difficult, and 11% said it had been more medical than they expected.
6.9. Perceived suitability of assessment channel
The majority of participants found the channel which their assessment was conducted using suitable for assessing their condition or disability. Two-thirds (66%) said it was either very or fairly suitable. Three in ten (29%) said they found the assessment channel either fairly or very unsuitable.
Participants rated all three channels similarly on suitability, indicating that there were no distinct differences between the channels. Around two-thirds rated each channel as being very or fairly suitable (telephone 66%, in-person 68% and video call 69%).
Overall, claimants for ESA or UC were more likely to say that they felt the channel used was suitable for assessing their condition or disability (77% for both groups). PIP were least likely to feel that the channel used was suitable (61%). This was the case across all assessment channels, as shown in Figure 6.9.1
Figure 6.9.1 Suitability of assessment channel in assessing condition
| Assessment | Fairly suitable % | Very suitable % | Very/Fairly suitable % |
|---|---|---|---|
| PIP – Telephone | 34% | 27% | 61% |
| PIP – In person | 34% | 24% | 59% |
| PIP – Video call | 35% | 29% | 64% |
| ESA – Telephone | 36% | 40% | 76% |
| ESA – In person | 30% | 52% | 82% |
| ESA – Video call* | 35% | 40% | 75% |
| UC – Telephone | 37% | 39% | 75% |
| UC – In person | 33% | 44% | 76% |
| UC – Video call | 34% | 51% | 85% |
C24. After you/they had your/their assessment, how suitable or unsuitable did you/they think was for assessing your/their condition / disability? Base: All respondents (7,262) *Caution small base (90)
Having an assessment using a particular channel changed participants opinions about it. This was the case across all channels. Over half (54%) of participants who had a telephone assessment felt the assessor would be able to accurately assess their health condition or disability before the assessment. After the assessment two thirds (66%) agreed it was a suitable assessment channel, a difference of 12 percentage points. For face-to-face assessments, the proportion changed from 58% before the assessment to 68% after. For video assessments, 54% agreed it was an accurate channel before the assessment and 69% felt it was suitable after the assessment, a difference of 15 percentage points. This is shown in Figure 6.9.2.
Figure 6.9.2 Perceived accuracy of assessment channel before assessment and perceived suitability after assessment
| Assessment | Net %Very/Fairly well before assessment | Net %Very/Fairly suitable after assessment |
|---|---|---|
| PIP – Telephone | 50% | 61% |
| PIP – In person | 53% | 59% |
| PIP – Video call | 50% | 64% |
| ESA – Telephone | 64% | 76% |
| ESA – In person | 62% | 82% |
| ESA – Video call* | 59% | 75% |
| UC – Telephone | 60% | 75% |
| UC – In person | 62% | 76% |
| UC – Video call | 66% | 85% |
C8. Before you/they had the assessment, how accurately did you/they think the assessor would be able to assess your/their health condition or disability? C24. After you/they had your/their assessment, how suitable or unsuitable did you/they think was for assessing your/their condition / disability? Base: All respondents who answered C8 (7172) and C24 (7262) *Caution small base (90)
There were some differences by type of condition or disability. Participants living with psychiatric disorders were less likely to deem the channel used as being suitable (63%) as were those with sensory disabilities (also 63%).
7. Assessment outcomes and satisfaction
This chapter describes the interaction between awareness of the award outcome and attitudes towards assessment channel.
7.1. Awareness of and satisfaction with assessment outcome
At the beginning of the survey, claimants were asked if they knew the outcome of their assessment. Just over nine in ten (91%) PIP claimants knew their assessment outcome, significantly higher than ESA (82%) or UC (83%) claimants.
Claimants who knew their assessment outcome were asked how satisfied or dissatisfied they were with it. PIP claimants were least likely to be satisfied with their assessment outcome (44%). Satisfaction was significantly higher amongst both ESA (69%) and UC claimants (71%). This aligns with patterns seen in other attitudes towards the assessment, such as PIP claimants being least likely to agree that the assessor understood their condition or that they were able to explain how their condition affects them (see Chapter 6).
In the quantitative survey, claimants who had a video assessment were more likely to be dissatisfied with the outcome of their assessment (43%) than those who had an in person assessment (37%). There were no significant differences in dissatisfaction between either of these channels and those who had a telephone assessment (39%). There were also no significant differences in satisfaction amongst the different assessment channels. Just over half of those who had an assessment using each channel were satisfied: 53% of those who had a telephone assessment, 56% of those who had an in person assessment, and 52% who had a video assessment.
Those who were satisfied with their assessment outcome were more likely to agree that the assessor had understood their condition and how it affects their daily life or ability to work. Eight in ten (80%) of those who were satisfied with their award outcome agreed that the assessor had understood their condition, compared to 13% of those who were dissatisfied. In contrast, 82% of those who were dissatisfied with their outcome disagreed with this statement, compared to 11% who were satisfied. A similar pattern was observed in agreement that claimants had been able to explain how their condition affects their daily life or ability to work. Over seven in ten (72%) who were satisfied with their outcome agreed that they had been able to explain their condition. Around two in ten (21%) who were dissatisfied with their assessment outcome agreed with this statement.
7.2. Influence of outcomes on attitudes towards assessment channel
The qualitative findings showed that claimant attitudes towards their assessment channel were due to both award outcome and their interaction with the assessor. Perceptions of suitability of assessment channel were determined by the extent to which claimants felt the assessor had understood their health condition.
Claimants who were dissatisfied with their interaction with the assessor were more likely to be dissatisfied with their award outcome. The opposite was also true. The qualitative interviews suggested that a positive interaction with the assessor could, in some but not all cases, help claimants accept their award outcome, even if this was a nil award. However, those who strongly believed they would receive an award at the outset and did not were likely to be dissatisfied with the assessment experience regardless.
Claimants who felt that their assessment channel was more suitable than expected after receiving their award outcome were more likely to have had an assessment using remote channels. This group were also likely to have been unsure about how the assessor would understand their condition and had been reassured by the interaction with the assessor. This improved their perception of the suitability of the remote assessment channel. This change in attitudes was not observed with in person assessments, as these were the default mode which people expected to receive. Nonetheless, some of those who had an in person assessment felt it had not been worth travelling to the assessment centre for, which had aggravated their health condition, because they did not get an award.
Claimants who felt that their assessment channel was less suitable than expected after receiving their award outcome were also more likely to have had an assessment using remote channels and were dissatisfied with both their interaction with the assessor and award outcome. These claimants felt that the remote assessment channel had not enabled them to fully demonstrate how their condition affected them.
Female, 18 to 24, PIP, Telephone assessment, said:
It [assessment outcome] was really disappointing, ‘cos I read the letter and there is a check list with different struggles and I scored zero for all of them. That is not accurate of my struggles…. at the time, I thought telephone was easier on my legs…but now I am thinking, it may have been better to go in (in person), at least then they can physically see me struggling.
However, not all claimants who were dissatisfied with their outcome and had a remote assessment believed that the assessment channel was inappropriate. As set out above, claimants who had a positive interaction with the assessor were likely to feel more positively about a remote assessment channel. This suggests that the interaction with the assessor was more important to influencing perceptions of the suitability of an assessment channel than the channel itself. More detail on the importance of interactions with the assessor is given in Chapter 6.
7.3. Appeals
Amongst participants who had appealed their award decision, motivations for appealing were a sense of personal or wider unfairness. Participants appealed if:
- they felt that the assessment report was inaccurate as it did not reflect their recollection of the assessment
- they felt that they deserved an award or a higher award based on their perceptions of the assessment of their condition
- they felt that the assessor had not accurately graded the severity of their condition
- they felt that their award was not fair to them or in one case because they felt their condition was widely misunderstood.
Female, 35 to 44, ESA, video call assessment, said:
I used to volunteer for an endometriosis charity, where I supported others with the condition…so really, I appealed on principle, as wanted to make a point, that the assessment was not fairly done to assess this condition.
Participants who had these experiences and did not appeal felt that appealing would not make any difference to the outcome.
There were no patterns observed between assessment channel and the decision to appeal in the research.
8. Channel choice and preferences
This chapter covers participants’ opinions on having medical appointments using remote channels, their overall preference for channel when having a DWP heath assessment, what is most important when having this assessment, and if they were given a choice of assessment channel, what information they would need to make decisions about this.
8.1. Participant perceptions of remote channels
To give context to their attitudes towards remote health assessments, participants in the qualitative interviews were asked about their experiences of, and attitudes towards, having remote assessments for medical appointments. Participants demonstrated pragmatism when it came to perceived suitability of assessment channels. Their priority was to get the best outcome and they chose the channel which they felt most effectively enabled this, depending on their personal context.
Telephone appointments for GP consultations and/or hospital appointments were more common than online appointments. From their experience, participants felt that telephone and video were most suitable for routine, follow up appointments or test results with a Healthcare Professional they were familiar with. Participants also felt that remote channels (telephone and video) were beneficial in enabling them to access care more quickly than attending in-person. Those who found it difficult to attend in-person due to mobility difficulties, health condition, or transport limitations discussed how remote channels were more accessible.
Female, 35 to 44, ESA, Video call assessment, said:
We only have one endometriosis nurse in the whole of [area], so the only option if I want to have her expertise is to do it by video call, I would rather have an appointment with her using this method, than not have an appointment at all.
Face-to-face appointments were seen as being most appropriate for a new diagnosis or health condition or for assessing the physical aspects of a condition. In these circumstances, participants would prefer a Doctor or Healthcare Professional to see them in-person.
Male, 45 to 54, PIP, Video call assessment, said:
I have telephone appointments with my pharmacist to review my medication, that was fine by phone as only asking questions…. I also have telephone appointments with my GP, who I have known for 10 years. I trust he is familiar with my condition…A lot of the time MS requires a physical examination, like with Orthopaedics, which is not served well by telephone.
8.2. Channel choice and preference
In the survey, participants were asked whether they would like a choice of how any future health assessments for benefits were carried out. Nearly nine in ten (86%) said they would like a choice of how future assessments are carried out. PIP claimants were most likely to want a choice of assessment channel (87%). ESA and UC claimants were equally likely to want this (both 83%). This contrasts with the actions participants reported in the survey, in which around one in eight had changed their assessment channel.
When asked about their channel preference for future assessments, channel preference was closely correlated to the channel through which their most recent assessment had been conducted. Those who had a telephone assessment were most likely to say they would choose telephone next time (49%), those who had a face-to-face appointment were most likely to choose this (39%), and those who had a video call were most likely to choose video call (37%) (see Figure 7.2.1). Overall, 15% of participants expressed no preference for assessment channel.
Figure 8.2.1 Channel preference for future assessments – total and by channel
| Channel | Total % | Video call % | In person % | Telephone % |
|---|---|---|---|---|
| Telephone | 43% | 16% | 30% | 49% |
| In person | 28% | 28% | 39% | 27% |
| Video call | 11% | 37% | 11% | 7% |
| No preference | 15% | 17% | 17% | 14% |
Base: All respondents (7262)
In the qualitative interviews, participants were asked whether having the next available appointment, a choice of channel or a specialist assessor was most important to them when having a future health assessment for a benefit claim. The most important elements selected reflected the participant’s personal priorities and prior experiences.
Those who selected the next available appointment as the most important were motivated by time. They wanted to have their assessment quickly, to enable them to access the benefits they believed they were entitled to. This attitude was most common amongst UC claimants.
Male, 25 to 34, UC, Video call assessment, said:
The most important to me is being quickly assessed and being able to access the funds your entitled to… [as long as] you’re reassured that you get the same respect and treatment…same standard of professionalism.
Participants who felt that that seeing an assessor who specialised in their condition was most important believed that they would better understand their condition. This was seen as meaning they would conduct a more accurate assessment. A specialist assessor was less important amongst those who had a positive assessment experience, as they had high confidence receiving an accurate assessment in the future. Those with low overall confidence in the ability of Healthcare Professionals to assess their condition were also less likely to prioritise this.
Being able to choose which channel the assessment was conducted using was important for those who felt a particular channel would enable them to better explain or demonstrate their condition. Those who believed they would get an equal treatment across all channels thought the channel choice was less important. This belief was related to having had a positive experience of their most recent assessment.
Male, 45 to 54, PIP, video call assessment, said:
I use a cane to walk, and I use furniture to hold for stability. If you see me walking into a room, you’ve got that interaction prior to the interview so the assessor would see the way you walk and will make a visual assessment of you, not just using the information on the screen. So I would have preferred face-to-face.
Overall, the qualitative findings found that providing health benefit claimants with a choice of channel had a series of intersecting benefits. A choice of channel was seen as enabling participants to choose the channel which they felt was appropriate for their condition and which would help them to best manage the emotional impact of the assessment. Participants felt that this would give them a sense of control and empowerment over the process, which would further help them to manage the emotional impact of the assessment. This is shown below in Figure 7.2.2.
Figure 8.2.2 Impact of being offered a choice of channel for future assessments
Choose the appropriate channel for their needs.
Feel a sense of control and empowerment over the process.
Choose the channel which will help them best manage the emotional impact of the assessment.
Participants were asked about what information they would need to make a choice about which channel to have an assessment using. Their information needs were both practical and emotional. Participants wanted to know the waiting times for each assessment channel. This was seen as enabling them to make an informed decision about how long they would have to wait for an assessment using each channel. The location of in-person assessments was important to allow participants to plan travel or determine if attending is feasible.
Male, 25 to 34, UC, Video call assessment, said:
A wait list for each of these channels, because it gives people that information…then they can select based on how long they want to wait. Also, the venue/ address of the proposed assessment centre to decide if the route is accessible by public transport and how much it will cost to travel to appointment.
On the emotional level, participants wanted reassurance from DWP that an assessment conducted using each channel would be equal. They wanted to know that how they were treated, and the award outcome, would be the same regardless of the assessment channel.
Male, 35 to 44, PIP, Video call assessment, said:
I think I would want to know from them [DWP] that all the methods have the same outcome…so if you choose video over telephone or face to face…then you’ll have the same results.
Related to this, some participants expressed a preference for being able to book their own health assessment appointments using an online booking system tool, similar to that for some NHS hospital appointments. They felt that this would give them more control and empowerment over the process.
9. Conclusions
Findings from the quantitative survey, Key Drivers Analysis and qualitative interviews did not identify clear patterns in claimant beliefs that the assessor understood their health condition or disability, or that they had been able to explain this properly, by assessment channel.
Rather, Key Drivers Analysis identified that perceptions of whether the assessor had understood their health condition or how the participant’s disability affected them were driven by:
- being asked questions which allowed them to explain how their condition affected them
- feeling that the assessor had understood their application form and other evidence
- feeling listened to during the assessment.
The qualitative research found that positive interactions with an assessor were characterised by the assessor explaining the assessment process, having a high degree of confidence in the assessor’s ability to assess their condition and the assessment feeling tailored to their condition (or understanding the purpose of questions which felt less relevant). This suggests that assessors should prioritise these behaviours. The evidence suggests that assessors can demonstrate these behaviours across all three assessment channels (face-to-face, telephone or video).
PIP claimants were more likely to express uncertainty about all the channels. This suggests that PIP claimants may need additional support or reassurance through the assessment process. Claimants were more likely to agree a channel was suitable after experiencing it. Future preferences for channel were strongly correlated to the channel claimants experienced most recently. Participants who had a positive interaction with the assessor also had high confidence in their assessment channel.
Overall awareness of the ability to change assessment channel was low, and a minority of participants changed the channel for their assessment. The qualitative interviews identified that participants only changed their assessment channel when they could not attend the channel they had originally been allocated. They did this regardless of whether they recalled that they had been told they could change channel.
When participants were asked about future choice, nearly nine in ten claimants said that they would like a choice of which channel their assessment is conducted using in the future. This choice was personal and dependent on individual preferences. Whilst there were intersections with health condition and digital confidence, neither of these could predict the assessment channel which claimants would prefer. Preferences for future assessments were shaped by past experiences. A positive assessment using any channel was more likely to give claimants confidence in this channel in the future.
In the qualitative research, participants felt that being offered a choice of assessment would enable them to choose the channel which they felt was appropriate for their condition and which would help them to best manage the emotional impact of the assessment. Participants felt that this would give them a sense of control and empowerment over the process.
Appendix A: Quantitative achieved sample
1. Quantitative sample achieved by assessment channel and benefit claimed
| Assessment Channel | Personal Independence Payment (PIP) | Universal Credit (UC) | Employment and Support Allowance (ESA) | Total |
|---|---|---|---|---|
| In person | 499 | 506 | 158 | 1,163 |
| Video call | 526 | 489 | 90 | 1,105 |
| Telephone | 3,309 | 1,113 | 482 | 4,904 |
| Don’t know | 30 | 38 | 9 | 77 |
| Prefer not to say | 6 | 7 | 0 | 13 |
| Total | 4,370 | 2,153 | 739 | 7,262 |
2. Quantitative sample achieved by interview mode
| Method | Number of completes |
|---|---|
| CATI | 4,884 |
| Web/Online | 2,378 |
| Total | 7,262 |
Appendix B: Qualitative achieved sample
1. Qualitative sample achieved by benefit type, age and gender
| Benefit type and channel | Interviews achieved |
|---|---|
| Personal Independence Payment (PIP) claimants | 30 |
| Telephone | 10 |
| Video call | 10 |
| Face-to-face | 10 |
| Employment and Support Allowance (ESA) claimants | 15 |
| Telephone | 5 |
| Video call | 5 |
| Face-to-face | 5 |
| Universal Credit (UC) claimants | 15 |
| Telephone | 5 |
| Video call | 5 |
| Face-to-face | 5 |
| Age | Interviews achieved |
|---|---|
| 18 to 24 | 5 |
| 25 to 34 | 11 |
| 35 to 44 | 10 |
| 45 to 54 | 16 |
| 55 to 64 | 12 |
| 65+ | 6 |
| Gender | Interviews achieved |
|---|---|
| Female | 35 |
| Male | 25 |
Appendix C: Quantitative questionnaire
Main questionnaire
Section A: Personal context
Ask if multiple_trial_assessments = Y:
A1. We understand that since July 2022 [S = 1 you] [S1 = 2 they] have had a health assessment for Personal Independence Payment (PIP) and a Work Capability Assessment. Is this correct?
1. Yes
2. No
3. Don’t know / can’t remember
Ask all who A1 = 1
A2. Our records show that [S = 1 your] [S1 = 2 their] most recent assessment was [benefit]. Is this correct?
1. Yes
2. No
3. Don’t know / can’t remember
Scripting: If 1 or 3 – code to most recent assessment type from sample. If no – soft check and if give same answer again, code to that assessment type.
Show screen to those who have multiple assessments in trial period
For the questions which follow, please answer about [S = 1 your] [S1 = 2 their] [benefit] assessment.
Asl all
A3. Have you / they been told about the outcome of [S = 1 your] [S1 = 2 their] [A1 = 1 most recent else = benefit] health assessment?
Single code
1. Yes
2. No
98. Don’t know
99. Prefer not to say
Ask all who code 1 [Yes] at A3.
A5. To what extent are you/they satisfied with the outcome of [S = 1 your] [S1 = 2 their] [A1 = 1 = most recent] health assessment?
Single code
1. Very satisfied
2. Fairly satisfied
3. Neither satisfied nor dissatisfied
4. Fairly dissatisfied
5. Very dissatisfied
6. Don’t know
Section B: Before the assessment
Show screen: The questions which follow are about the information [S = 1 you] [S1 = 2 they] received from DWP before the assessment. [A1 = 1 – Please think about [S1=1your] [S2=2 their] [benefit] assessment.]
Ask all
B1A. Before [S = 1 you] [S1 = 2 they] received an invitation to the assessment were [S = 1 you] [S1 = 2 they] aware:
Read out. Single code only.
A. That you/the person you are claiming for might need to have an assessment
B. Why you/the person you are claiming for might need to have an assessment
C. What happens at an assessment
D. That the assessment may be held in person
E. That the assessment may be held on the telephone
F. That the assessment may be held on a video call
1. Yes
2. No
3. Don’t know [Do not read out]
Ask all who B1A_D, E or F = 1
B2. What impact did this have on [S = 1 your] [S1 = 2 their] likelihood to apply for [Benefit]? Did it make [S = 1 you] [S1 = 2 them] …
Read out. Single code only. Show ciodes selected at B1A only.
A. Knowing the assessment may be held in person
B. Knowing the assessment may be held on the telephone
C. Knowing the assessment may be held on a video call
1. Much more likely to apply
2. A little more likely to apply
3. Made no difference
4. A little less likely to apply
4. Much less likely to apply
3. Don’t know [Do not read out]
Ask all
B3. Before your assessment, where did [S = 1 you] [S1 = 2 they] get information about it from?
Read out. Multicode
1. DWP
2. The Assessment provider
3. Friends and family
4. Social media, online forums, Facebook groups
5. My local authority
6. Charity e.g., Turn2Us, Citizen’s Advice Bureau, EntitledTo
7. [UC only] Through my Universal Credit Journal
8. [UC OR ESA only] From my work coach / at the Jobcentre Plus
9. Other (Please specify)
10. Didn’t get any information about the assessment [Exclusive]
11. Don’t know
Ask if obtained advice or information from DWP (B3=1) or assessment provider (B3 = 2).
B4. What type of information or advice did [S = 1 you] [S1 = 2 they] get from [B3 = 1 DWP] [B3 = 2 the assessment provider] [B3 = 1 and 2 = DWP or the assessment provider]?
Multicode. Read out.
1. How long the overall assessment process takes from filling in the application to receiving a decision
2. What the overall assessment process involves
3. How to reschedule appointments
4. How long the assessment will last
5. How the assessment would be held
6. Where the assessment would take place
7. How to prepare for an assessment
8. How to act during an assessment
9. Who would conduct the assessment
10. What supporting evidence is required at the assessment
11. Whether you/they could take somebody with you/ them
12. Whether you/they could bring supporting evidence that was not originally submitted with your/ their application
13. How you/they would be informed about the decision after the assessment
14. Other information or advice (Please specify)
15. Don’t know
16. Can’t remember
Ask if obtained advice or information from DWP (B3=1) or assessment provider (B3 = 2).
B5. How clear or not was the information [S = 1 you] [S1 = 2 they] got from [B3 = 1 DWP] [B3 = 2 the assessment provider] about the assessment process [B3 = 1 and 2 = DWP or the assessment provider]? Single code. Read out.
1. Very clear
2. Fairly clear
3. Not very clear
4. Not at all clear
5. Don’t know
Section C: Assessment Experience
Show screen
The questions which follow are about [S = 1 your] [S1 = 2 their] experience of your / their [benefit] assessment.
Ask all
C1. How was [S = 1 your] [S1 = 2 their] assessment conducted?
Single code
1. On the telephone
2. In person
3. On a video call
98. Don’t know
99. Prefer not to say
Scripting dummy variable: Attended DWP Sample channel:
If attended_channel = C1 – Yes
If attended_Channel IS not c1 – No
Ask all
C2. Was this the type of assessment [S = 1 you] [S1 = 2 they] were originally offered?
Single code
1. Yes
2. No
98. Don’t know
Ask all who code no at C2 [C2 = 2]
C3. What type of assessment were [S = 1 you] [S1 = 2 they] were originally offered?
Single code. Do not show code selected at C1.
1. On the telephone
2. In person
3. On a video call
Ask all who code no at C2 [C2 = 2]
C4. Why didn’t [S = 1 you] [S1 = 2 they] attend the type of assessment [S = 1 you] [S1 = 2 they] were originally offered?
Multicode.
1. [S = 1 I] [S1 = 2 They] didn’t think this would enable the assessor to fully understand [S = 1 my] [S1 = 2 their] condition / disability
2. [C3 = 3 video] [S = 1 I] [S1 = 2 They] don’t have access to the right equipment to have a video assessment
3. [C3 = 3 video] [S = 1 I] [S1 = 2 They] didn’t feel confident using the technology to have a video assessment
4. [C3 = 3 video] [S = 1 I] [S1 = 2 They] didn’t have suitable internet access to have a video assessment
5. [S = 1 I] [S1 = 2 They] didn’t feel able to attend [C3 = 2= in person c3 = 1 over the phone c3 – 3 online] because of my health condition / disability
6. [c3=2 in person] [S = 1 wasn’t] [S1 = 2 They weren’t] able to travel to the assessment centre
7. [C3 = 1 telephone] [S = 1 I was] [S1 = 2 They were] worried about / had poor reception
8. [S = 1 I was] [S1 = 2 They were] was anxious about completing the assessment in this way
9. Another reason (please specify)
10. Don’t know
Ask all who code no at [C2 = 2]
C5. How easy or difficult was it for [S = 1 you] [S1 = 2 them] to change the type of assessment [S = 1 you] [S1 = 2 they]had?
1. Very easy
2. Fairly easy
3. Fairly difficult
4. Very difficult
5. Don’t know
Ask all who C2=1
C2A. Were [S = 1 you] [S1 = 2 they] aware that [S = 1 you] [S1 = 2 they]could change [S = 1 your] [S1 = 2 their] assessment type?
Single code
1. Yes
2. No
98. Don’t know
Ask all
C7. Did [S1 = 1 you S1 = 2 the person you are answering for] attend the assessment time and date [S = 1 you] [S1 = 2 they] were initially offered?
Single code. Do not read out.
1. Yes, attended the assessment initially offered
2. No, did not attend the assessment initially offered
3. Don’t know
Ask all
C8. Before [S = 1 you had your] [S1 = 2 they had their] [A1 = 1 = most recent] assessment, how accurately did you/ they think the assessor would be able to assess your / their health condition or disability using [c1=1 over the telephone c1=2 in person c1=3 on a video call]?
1. Very well
2. Fairly well
3. Not very well
4. Not at all well
98. Don’t know
99. Prefer not to say
Ask all
C9. Please tell me to what extent you agree or disagree with each of the following statements?
Read out. Single code only for each statement.
A. The appointment time [S1 = 1 I was S1=2 they were] offered was convenient for me/them.
B. [S1 = 1 I was S1=2 They were] informed of the assessment time [Face-to-face only = and place] in enough time to make preparations
C. [S1 = 1 I S1=2 They] knew who to contact if [S1 = 1 I S1=2 they] needed to ask questions or rearrange appointments
D. DWP made it clear to me/them that I/they could bring someone to the assessment if [S1 = 1 I S1=2 They] wanted to
E. [Face-to-face only] The face-to-face assessment offered was in a location that [S1 = 1 I S1=2 They] could get to easily
1. Strongly agree
2. Tend to agree
3. Tend to disagree
4. Strongly disagree
5. Don’t know (Do not read out)
Ask all
C10. On the day of the assessment, to what extent, if at all, were [S = 1 you] [S1 = 2 they] concerned about attending it?
Single code
1. Very concerned
2. Fairly concerned
3. Not very concerned
4. Not at all concerned
98. Don’t know
99. Prefer not to say
Ask all S
C11. On the day of [S = 1 your] [S1 = 2 their] assessment, which, if any of the following challenges did [S = 1 you] [S1 = 2 they] experience?
Multicode
1. Assessor was running late / delays in appointment time
2. I was / they were running late
3. [Face-to-face only] Difficulty accessing the assessment centre due to my / their health condition / disability
4. [Face-to-face only] Difficulty accessing the assessment centre due to transport
5. [Telephone only] Missed the assessor’s telephone call / had trouble contacting the assessor
6. [Online only] Difficulties using the video call technology
7. [Online only] Difficulties connecting / difficulties with internet connection
8. [Online or telephone only] Poor quality [Online =video] [Telephone = phone] call
9. [Online or telephone only] The assessor called unexpectedly
10. Something else (please write in)
11. None of these
12. Prefer not to say
Ask all who experienced challenges [C11 = 1 – 9]
C12. You mentioned that [S = 1 you] [S1 = 2 they] experienced challenges on the day of the assessment. What happened because of these?
Multicode
2. The assessment went ahead on that date cannot combine 2 and 3]
3. [S = 1 I] [S1 = 2 they] received a new appointment for [S = 1 my] [S1 = 2 their] assessment [Cannot combine 2 and 3]
4. How the assessment was held changed (e.g. on telephone rather than in person)
5. Something else (please write in)
6. None of these
7. Prefer not to say
Ask all
C13. Did [S = 1 you] [S1 = 2 they] [Face-to-face = take anyone into the assessment room] [Telephone = ask someone to join the telephone assessment] [Video = ask someone to join the video call] with [S = 1 you] [S1 = 2 they]?
Single code. Do not read out
1. Yes, someone attended with me/them
2. No, no one attended with me/them
3. Don’t know/can’t remember
Ask if C13=1 (Attend with someone)
C14. Why did [S1 = 1 you] [S1= 2 the person you are claiming for] [Face-to-face = take someone with you/them into the assessment room] Telephone = ask someone to join the call video = ask someone to join the video call]?
Multicode
1. To support me/them with needs associated with my/ their disability/illness
2. Provided moral support or company
3. Answered the questions in the assessment on my/their behalf
4. Helped me/them with the information [S1 = 1 I] [S1= 2 they] needed to answer questions
5. Took notes for me/them so [S1 = 1 I] [S1= 2 they would remember what happened
6. Asked the assessor questions
7. [S1 = 1 I] [S1= 2 They care for them(they did not help during the assessment)
8. [Video only] To support me with the video call
9. Other
10. Don’t know
Ask all
C15. Please tell me to what extent you agree or disagree with each of the following statements about the assessment?
[S1 = 2 Please answer this question to the best of your knowledge even if you did not attend the assessment. If you do not know the answers, please select, don’t’ know.
Interviewer: If the respondent is claiming on behalf of someone else they can answer this question even if they did not attend the interview. If they don’t know the answers, use don’t know. Read out. Single code for each statement.
A. The assessor explained what his/her role was
B. The assessor explained the purpose and structure of the [face-to-face/ video / telephone] assessment before starting
C. The assessor treated [S1 = 1 me S1 = 2 them] with respect and dignity during the [face-to-face/ video / telephone] assessment
D. [S1 = 1 I] [S1= 2 They felt listened to during the [face-to-face/ video / telephone] assessment
E. [S1 = 1 My] [S1= 2 Their communication and language needs were considered in how the [face-to-face/ video / telephone] assessment was carried out
F. The assessor had understood [S1 = 1 my] [S1= 2 their application form and supporting evidence sent in advance correctly
G. [S1 = 1 I was] [S1= 2 They were asked questions which were relevant and appropriate to my/their condition
H. S1 = 1 I was] [S1= 2 They were asked questions which allowed me/them to fully explain the impact of my/their condition on my/their [PIP = day-to-day life] [WCA = ability to work]
I. [Face-to-face only] The measurements and functional tests that were carried out during the face-to-face assessment were relevant and appropriate
J. S1 = 1 I] [S1= 2 They had enough time during the assessment to explain how my/their condition affects me/them
K. S1 = 1 I] [S1= 2 They understood what S1 = 1 I was] [S1= 2 they were being asked about being asked to do
1. Strongly agree
2. Tend to agree
4. Tend to disagree
5. Strongly disagree
6. Don’t know
7. Not applicable
Ask all
C18. During the assessment, how comfortable or uncomfortable did [S = 1 you] [S1 = 2 they] feel about sharing the details of [S = 1 your] [S1 = 2 their] health condition / disability with the assessor?
Single code
1. Very comfortable
2. Fairly comfortable
3. Fairly uncomfortable
4. Very uncomfortable
98. Don’t know
99. Prefer not to say
Ask all
C19. Were there things [S1 = 1 you S1=2 the person you are claiming for] wanted to explain at the [face-to-face/ video / telephone] assessment which you/they weren’t able to?
Single code. Do not read out
1. Yes, there were other things [S1 =1 I S1=2 they] wanted to explain
2. No, there were no other things [S1 =1 I S1=2 they] wanted to explain
3. Don’t know
Ask if yes (C19=1)
C20. Why weren’t [S1 = 1 you S1 = 2 they] able to explain them?
Multicode.
1. [S1 =1 I was S1=2 they were] not asked the right questions
2. [S1 =1 I S1=2 they] forgot to mention them
3. There was no time
4. [S1 =1 I S1=2 they] had been advised not to say them
5. The assessor was ‘scary’ or intimidating
6. [IF C13 = 2 or 3] [S1 = 1 I S1 = 2 They]did not have someone in the assessment with [S1 = 1 me S1 = 2 them]
7. Other (Please specify)
8. Don’t know
Ask all
C21. Thinking about the assessment itself, was [S1 = 1 your S1 = 2 their] overall experience of the assessment ….
Single code. Reverse code.
1. Easier than expected
2. As expected
3. More difficult than expected
4. Don’t know/no opinion (Do not read out)
Ask if C21= more difficult (code 3)
C22. In what ways was the assessment more difficult than [S1 = 1 you] [S1 = 2 they] expected?
Multicode.
1. Longer
2. More tiring than expected
3. More medical than expected
4. Assessments/tests were difficult
5. The assessor was unfriendly
6. The assessor was unhelpful
7. [If took chaperone = ] The person I/ they brought to the face-to-face assessment was not able to help or allowed to help as much as I/ they thought they would be able to
8. [If did not take a chaperone = ] I didn’t have anyone to help me
9. It was intrusive
10. It was stressful
11. [S1 = 1 I was S1 = 2They were] not able to present the information or evidence I/they wanted to
12. [Video only] The video technology was difficult to use
13. Other
14. Don’t know/can’t remember
Ask if C21 = easier (code 1)
C23. In what ways was the assessment easier than [S1 = 1 you] [S1 = 2 they] expected?
Multicode. Probe fully.
1. Shorter
2. Less tiring than expected
3. Less medical than expected
4. Assessments/tests were easy or easier than expected
5. The assessor was friendly
6. The assessor was helpful
7. [If took a chaperone = ] The person I/ they brought to the assessment was able to or allowed to help more than I/ they thought they would be able to
8. It was less intrusive than expected
9. It was good to speak to someone about how my/their condition affects [S1 = 1 me S1 = 2 them]
10. It was less stressful than expected
11. [Video only] The video technology was easy to use
12. Other
13. Don’t know/can’t remember
Ask all
C24. After [S1 = 1 you had your] [S1 = 2 they had their] [If multiple = most recent] assessment, how suitable or unsuitable did you/ they think c1=1 the telephone c1=2 in person c1=3 a video call] was for assessing [S1 = 1 your S1 = 2 their] condition / disability?
1. Very suitable
2. Fairly suitable
3. Fairly unsuitable
4. Very unsuitable
98. Don’t know
99. Prefer not to say
Ask all
C25. How much do you agree or disagree with the following statements
A. Using the [face to face / video / telephone] assessment the assessor was able to understand [S1 = 1 my S1 = 2 their] health condition / disability and how it affects [S1 = 1 my S1 = 2 their] [PIP = day to day life WCA = ability to work]
B. Using the [face to face / video / telephone] assessment I was / they were able to explain to the assessor how [S1 = 1 my S1 = 2 their] health condition / disability and how it affects [S1 = 1 my S1 = 2 their] [PIP = day to day life WCA = ability to work]
1. Strongly agree
2. Tend to agree
3. Tend to disagree
4. Strongly disagree
98. Don’t know
99. Prefer not to say
Section D: Assessment Experience 2 (Multiple Assessment Claimants Only)
Ask all A1 = 1
D1. Our records show that you have also had an assessment for [prior_attend1_benefit or prior_attend2_benefit – PIP = Personal Independence Payment / UC = Universal Credit / ESA = Employment and Support Allowance].
Scripting: If records have prior_attend1_benefit and prior_attend2_benefit use prior_attend2_benefit.
How was [S1 = 1 your S1=2 their] [IF prior_attend1_benefit OR prior_attend2_benefit = PIP – health assessment IF = UC OR ESA = Work Capability Assessment]] conducted?
Single code
1. On the telephone
2. In person
3. On a video call
98. Don’t know
99. Prefer not to say
Ask all A1 = 1
D2. Before [S1 = 1 you had your S1 = 2 they had their] [Benefit shown D1] assessment, how suitable or unsuitable did you/ they think D1=1 telephone D1=2 in person D1=3 a video call] would be for assessing your / their condition / disability?
1. Very suitable
2. Fairly suitable
3. Fairly unsuitable
4. Very unsuitable
98. Don’t know
99. Prefer not to say
Ask all A1 = 1
D3. Please tell me to what extent you agree or disagree with each of the following statements?
Read out. Single code only for each statement.
A. The appointment time [S1 = I was S1 = 2 they were] offered was convenient for me/them.
B. [S1 = I was S1 = 2 They were] informed of the assessment time [Face-to-face only = and place] in enough time to make preparations
F. [D1 = 2] The face-to-face assessment offered was in a venue or building that was accessible to [S1 = 1 me S1=2 them] (e.g. with suitable ramps, handrails, light, sound proofing, toilets etc.)
G. [D1 = 2] The face-to-face assessment offered was in a location that [S1 = 1 I S1 = 2 they] could get to easily
1. Strongly agree
2. Tend to agree
3. Tend to disagree
4. Strongly disagree
5. Don’t know (Do not read out)
Ask all A1 = 1
D4. On the day of the assessment, to what extent, if at all, were [S1 = 1 you S1 = 2 they] concerned about it?
Single code
1. Very concerned
2. Fairly concerned
3. Not very concerned
4. Not at all concerned
98. Don’t know
99. Prefer not to say
Ask all A1 = 1
D5. On the day of your assessment, which, if any of the following challenges did [S1 = 1 you S1 = 2 they] experience?
Multicode
1. Assessor was running late / delays in appointment time
2. I was / they were running late
3. [Face-to-face only] Difficulty accessing the assessment centre due to my / their health condition / disability
4. [Face-to-face only] Difficulty accessing the assessment centre due to transport
5. [Telephone only] Missed the assessor’s telephone call / had trouble contacting the assessor
6. [Online only] Difficulties using the video call technology
7. [Online only] Difficulties connecting / difficulties with internet connection
8. [Online or telephone only] Poor quality [Online =video] [Telephone = phone call]
9. [Online or telephone only] The assessor called unexpectedly
10. Something else (please write in)
11. None of these
99. Prefer not to say
Ask all A1 = 1
D6. Did [S1 = 1 you S1 = 2 they] [Face-to-face = take anyone into the assessment room] [TelephoneE = ask someone to join the telephone assessment] [Video = ask someone to join the video call] with you / them?
Single code. Do not read out
1. Yes, someone attended with me/them
2. No, no one attended with me/them
3. Don’t know/can’t remember
Ask all A1 = 1
D7. Please tell me to what extent you agree or disagree with each of the following statements about the assessment?
Interviewer: If the respondent is claiming on behalf of someone else they can answer this question even if they did not attend the interview. If they don’t know the answers, use don’t know. Read out. Single code only for each statement.
A. The assessor explained what his/her role was
B. The assessor explained the purpose and structure of the [face-to-face/ video / telephone] assessment before starting
C. The assessor treated me/them with respect and dignity during the [face-to-face/ video / telephone] assessment
D. I/They felt listened to during the [face-to-face/ video / telephone] assessment
E. My/Their communication and language needs were considered in how the [face-to-face/ video / telephone] assessment was carried out
F. The assessor had understood my/their application form and supporting evidence sent in advance correctly
G. I was/They were asked questions which were relevant and appropriate to my/their condition
H. I was/They were asked questions which allowed me/them to fully explain the impact of my/their condition on my/their [PIP = day-to-day life] [WCA = ability to work]
I. The measurements and functional tests that were carried out during the face-to-face assessment were relevant and appropriate
J. I/They had enough time during the assessment to explain how my/their condition affects me/them
K. I/They understood what I was/they were being asked about and what I was/they were being asked to do
1. Strongly agree
2. Tend to agree
4. Tend to disagree
5. Strongly disagree
6. Don’t know
7. Not applicable
Ask all A1 = 1
D10. During the assessment, how comfortable or uncomfortable did [S1 = 1 you S1 = 2 they] feel about sharing the details of [S1 = 1 your S1 = 2 their] health condition / disability with the assessor?
Single code
1. Very comfortable
2. Fairly comfortable
3. Fairly uncomfortable
4. Very uncomfortable
98. Don’t know
99. Prefer not to say
Ask all A1 = 1
D11. Were there things [S1 = 1 you/ S1 = 2 the person you are claiming for] wanted to explain at the [face-to-face/ video / telephone] assessment which [S1 = 1 you S1 = 2 they] weren’t able to?
Single code. Do not read out.
1. Yes, there were other things [S1 = 1 I S1 = 2 they] wanted to explain
2. No, there were no other things [S1 = 1 I S1 = 2 they] wanted to explain
3. Don’t know
Ask all A1 = 1
D12. Thinking about the assessment itself, was [S1 = 1 your S1 = 2 their] overall experience of the assessment …
Single code.
1. Easier than expected
2. The experience was as expected
3. More difficult than expected
4. Don’t know/no opinion (Do not read out)
Ask all A1 = 1
D13. After [s1 = 1 you had your s1 = 2 they had their] [prior_attend1_benefit OR prior_attend2_benefit] assessment, how suitable or unsuitable did you/ they think D1=1 telephone D1=2 in person D1=3 a video call] was for assessing [S1 = 1 your S1=2 their] condition / disability?
Scripting: If records have prior_attend1_benefit and prior_attend2_benefit use prior_attend2_benefit.
1. Very suitable
2. Fairly suitable
3. Fairly unsuitable
4. Very unsuitable
98. Don’t know
99. Prefer not to say
Ask all A1 = 1
D14. How much do you agree or disagree with the following statements
C. Using the [face to face / video / telephone] assessment the assessor was able to understand [s1 = 1 my S1=2 their] health condition / disability and how it affects my / their [prior_attend1_benefit OR prior_attend2_benefit =PIP = day to day life prior_attend1_benefit OR prior_attend2_benefit = WCA = ability to work]
D. Using the [face to face / video / telephone] assessment [S1 = 1 I was S1 = 2 they were] able to explain to the assessor how my / their health condition / disability and how it affects [s1 = 1 my S1=2 their] [prior_attend1_benefit OR prior_attend2_benefit =PIP = day to day life prior_attend1_benefit OR prior_attend2_benefit = WCA = ability to work]
1. Strongly agree
2. Tend to agree
3. Tend to disagree
4. Strongly disagree
98. Don’t know
99. Prefer not to say
Section E: Preferences
Ask all
E1. Which of the following ways would [S1 = 1 you S1 = 2 they] like any future health assessments [S1 = 1 you S1 = 2 they] may have for [benefit] to be carried out?
Multicode
1. On the telephone
2. In person
3. On a video call
4. No preference [Exclusive]
- Don’t know [Exclusive]
Ask all who code more than one at E1
E1A. And which of these would be [S1 = 1 your S1 = 2 their] preference?
Single code. Show codes selected at E1.
1. On the telephone
2. In person
3. On a video call
4. No preference
98. Don’t know
Ask all
E3. Would [S1 = 1 you S1 = 2 they] like to be given a choice of how any future health assessments [S1 = 1 you S1 = 2 they] may have for [benefit] are carried out?
Single code
1. Yes
2. No
98. Don’t know
Section F: Demographics
This is the final section of the survey and [CATI: I’d just / ONLINE: we would] like to ask you a few details about yourself including your health, background and ethnic origin]. This information will be used to monitor the experiences that different groups have when they are dealing with DWP. You do not have to answer if you do not want to.
All of your answers will be treated in the strictest confidence and DWP will not be able to identify you from the anonymised responses that Ipsos supply.
Ask all
F1. Which of the following best describes the type of health condition(s) or disability/ disabilities [S1 = 1 you S1 = 2 they] have?
Multicode Ok
1. Anxiety and / or depression
2. Other Psychiatric disorder(s) not including anxiety and depression
3. A musculoskeletal condition or disability
4. A physical disability or health condition, not musculoskeletal
5. A sensory disability or health condition
6. Something else
Ask all, single code apart from 13 which should be set as MC
F2. Please could you confirm [S1 = 1 your S1 = 2 their] current employment status? If you [S1 = 1 you S1 = 2 they] doing more than one job please select [S1 = 1 your S1 = 2 their] main job, that is the one where [S1 = 1 you S1 = 2 they] earn the most money.
Single code. Do not read out but prompt to code and probe fully
1. Not looking for work/ not fit to work now, though could do in the future
2. Not employed because of long term illness or disability and unlikely to do so in the future
3. In paid employment – working full time (30+ hours per week)
4. In paid employment – working part-time (8-29 hours per week
5. In paid employment – working part-time (under 8 hours per week)
6. Self-employed - working full time (30+ hours per week)
7. Self-employed - working full time (8-29 hours per week)
8. Self-employed – working part-time (under 8 hours per week)
9. Unemployed and seeking work
10. Not employed – stay at home parent
11. Not employed for another reason
12. Full-time student
13. Retired
99. Prefer not to say
Ask all.
F3. Can I just check, are [S1 = 1 you S1 = 2 they] currently receiving any other benefits or state allowances in addition to [benefit (PIP / ESA / UC]]?
Multicode ok
1. Housing benefit
2. Income support
3. Jobseeker’s Allowance
4. [Autocode if UC sample] Universal Credit
5. State Pension
6. Incapacity Benefit or Severe Disablement Allowance
7. [Autocode if ESA sample] Employment and Support Allowance
8. Some other benefit for people with disabilities (e.g. Industrial Injuries Benefit)
9. Working Tax Credit
10. Child Tax Credit
11. Council Tax Benefit
12. Pension Credit
13. [Autocode if PIP sample] Personal Independence Payments
14. Carer’s allowance
15. Attendance Allowance
16. Some other state benefit (Specify)
17. No, none of these
18. Refused (Do not read out)
19. Don’t know (Do not read out)
F4. How would [S1 = 1 you S1 = 2 they] describe [S1 = 1 you S1 = 2 their] ethnic background? One answer, do not read out, prompt to code and probe fully
1. White [Expandable Header] * English / Welsh / Scottish / Northern Irish / British * Irish * Gypsy or Irish Traveller * Any other White background
2. Mixed / multiple ethnic groups [Expandable Header] * White and Black Caribbean * White and Black African * White and Asian * Any other Mixed / multiple ethnic background
3. Asian / Asian British [Expandable Header] * Indian * Pakistani * Bangladeshi * Chinese * Any other Asian background
4. Black / African / Caribbean / Black British [Expandable Header] * African * Caribbean * Any other Black / African / Caribbean background
5. Other ethnic group [Expandable Header] * Arab * Any other ethnic group, please write in: * Prefer not to answer
99. Prefer not to say
Ask all, multicode
F5. Which of these best describes [S1 = 1 you S1 = 2 their] living situation?
Please answer for the accommodation [S1 = 1 you S1 = 2 they] spend most time in.
Please select all that apply
Multicode, read out
1. Living alone
2. Living with partner [Mutually exclusive with option 3]
3. Living with spouse/civil partner [Mutually exclusive with option 2]
4. Living with parents
5. Living with friends/other adults / other family (i.e. not parents)
6. Living with dependent children (under the age of 16, or under the age of 20 and still in full-time education or training, below university or equivalent level)
99. Prefer not to say
Ask all, single code
F6. Which of these best describe the accommodation [S1 = 1 you S1 = 2 they] are living in at the moment?
Please answer for the accommodation [S1 = 1 you S1 = 2 they] spend most time in.
Single code
1. Private rented
2. Rented from a council or local authority
3. Rented from a Housing Association
4. Being bought on a mortgage/bank loan
5. Shared ownership where you pay part rent and part mortgage
6. Owned outright
7. Living with friends/relatives and paying some rent
8. Living with friends/ relatives and not paying any rent
9. Living in temporary or sheltered accommodation or rough sleeping
10. Something else (specify)
98. Don’t know
99. Prefer not to say
Ask all, multicode except 1 and 99
F7. Do [S1 = 1 you S1 = 2 they] have any of the following caring responsibilities? By caring responsibilities, we mean caring for anyone who needs help with everyday life due to illness, disability or old age. This could include help with grocery shopping, bathing, dressing, laundry, etc.
CATI read out. Select all that apply
1. No [Exclusive]
2. Yes – for Spouse / Civil Partner/ Partner
3. Yes – for Parent(s)
4. Yes – for another family member
5. Yes – for a friend
99. Prefer not to say [Exclusive]
Ask all, single code
F8. Is English [S1 = 1 your S1 = 2 their] first language? One answer, do not read out, prompt to code
1. Yes
2. No
3. Don’t know
4. Prefer not to say
Ask all, single code
F9. Would [S1 = 1 you S1 = 2 they] feel able to use the internet to access government services if they were available online?
Single code
1. Yes, able to
2. Yes, able to with help
3. No, not able
4. Don’t know
5. Prefer not to say
Section G: Thank you
On behalf of Ipsos UK and the Department of Work and Pensions we would like to thank you very much for your time.
Appendix D: Qualitative Discussion Guide
Overview of discussion
| Item | Timings |
|---|---|
| Intro and warm-up | 5 to 7 minutes |
| Claimant experience of the assessment and channel change | 20 minutes |
| Channel perceptions and preferences | 15 to 18 minutes |
| Channel choice | 10 minutes |
| Wrap up | 5 minutes |
When using the guide, the researcher will ask questions and use the prompts to guide where necessary. Not all questions or prompts will necessarily be used during the interview
Key Questions
Timings: 5 to 7 minutes
Introduction:
- thank participant for taking part
- Introduce yourself and Ipsos. We are an independent research organisation i.e., independent of the government. We adhere to the MRS Code of Conduct which ensures our research is carried out in an ethical and professional manner, based on voluntary informed consent, and that individuals’ rights, wellbeing and confidentiality is respected at all times
- the interview: informal conversation on their experiences, no right or wrong answers, should last around 45 to 60 minutes.
- the research: this research follows on from the survey you recently took part in with us. The objective of this interview is to explore your experiences in more depth to help DWP better understand your health assessment experience
- confidentiality: all responses are anonymous, and no identifiable data will be passed onto anyone, including to DWP or any other government department. The only exception to this, would be if you told us something that made us concerned you/someone else was at serious risk of harm, in which case we might need to pass this on
- reassure them that participation will have no impact on their benefit claim, now or in the future.
- consent: check that they are happy to take part in the interview and understand their participation is voluntary (they can withdraw at any time).
- recording: get permission to digitally record.
- any questions before we begin?
GDPR added consent (once recorder is on, if permission is given)
Ipsos’ legal basis for processing your data is your consent to take part in this research. Your participation in this research is voluntary. You can withdraw your consent for your data to be used at any point before, during, or after the interview. Can I check you are happy to proceed?
Warm up
To start off with, I’m going to ask a few questions about yourself…
Cover briefly:
Can you tell me a bit about yourself? Probe:
- family and home life – who you live with (partner, children), any other caring responsibilities, how long they have lived there.
- typical day Can you tell me briefly about a typical day in your life at the moment? Talk me through a typical day. What are your habits and routines? How does your health affect your day-to-day life?
Claimant experience of the assessment and channel change
Timings: 20 minutes
This section explores their most recent health assessment experience and their thoughts on suitability of the channel(s) offered and used.
In this section, I’d like to discuss your recent health assessment experience, which was conducted [channel] …
When were you told that you would need to have an assessment as part of your claims?
How did you first hear about your assessment?
- what information did you receive? How was this communicated to you? Who by?
- what specifically did you learn about your assessment? [Probe on: channel, ability to change channel, ability to change appointment time, ability to take someone with them]
- how useful did you find the information provided?
- how did you feel about your assessment at this point?
What did you think about having your assessment [channel type]? [If concerns are expressed, probe on whether these relate to the specifics of their health condition or the channel, or something else]
Did you discuss your assessment and how it would be held (i.e. channel type) with anyone? (e.g. family, friends etc.)
- [If yes] What type of things did you talk about?
- how easy or difficult did you find changing how your assessment was held?
- what difference did changing the channel have for you? [Probe on whether they believe this was a beneficial or unbeneficial change]
- [If no] would you have changed your channel type if you had known? [Probe fully on reasons why?/why not?]
- [If yes] [Probe fully on reasons for not changing]
Please can you talk me through your experience of the assessment step by step? Probe on:
- getting ready – how did you prepare (e.g. plan travel, test technology etc)
- getting to the assessment centre/ joining the call
- introductions to the assessor
- understanding the purpose of the assessment and what would happen
- what the assessor told them about the assessment process before starting
- how well they understood what the assessor was asking them
- how easy / difficult they found it to answer the questions asked / activities
- how they felt at the end – that they had been able to fully explain
[Throughout probe on extent to which channel influenced this experience / role of channel and what other factors influenced]
To what extent did you feel that the assessor was listening to you?
- how did this affect your experience of the assessment?
What more could the assessor do to build your confidence in their ability to understand the impacts of your condition(s)?
Probe on:
- understanding the assessor’s healthcare background (e.g. experience and expertise)
- non-verbal and verbal communication
- tailoring of questions to ensure relevance
In the survey, you mentioned that you found the assessment [easier/more difficult] than expected. Could you tell me a bit more about why that was? [Probe on all reasons why, including any impact on channel]
- [Found it more difficult] What could have been done to make the experience easier for you?
- [Found it easier] What could DWP have told you in advance to reassure you?
[If they changed mind on suitability of channel] I can also see that you initially thought your condition would not be accurately assessed using [channel type] and after found that it was. Could you tell me a bit more about why you changed your mind? [Probe on what they found better during the assessment vs initial concerns]
[If changed their mind on suitability of channel AND appealed outcome] Has your opinion on the suitability of [channel type] changed since receiving your decision outcome and appealing this? [If they know the outcome of their claim] How do you feel about the outcome of your claim?
- how does this relate to your experience in the assessment?
- how does this relate to how your assessment was conducted (i.e. assessment channel type)?
[If outcome was appealed] What were your reasons for appealing your outcome decision? [Probe on reasons why]
- what impact do you think having your assessment using another channel would have had on your experience?
- and what impact would this have had on your decision to appeal your claim? [Probe on reasons why/why not]
Overall, what one change would have improved the assessment experience for you?
Channel perceptions and preferences
Timings: 15 to 18 minutes
This section explores claimant’s perception on the ways the provision of some health services have changed.
In this section, I’d like to explore your opinion on the ways in which some health services/ assessments are delivered…
What types of appointments (outside of in person) have you had for other health services? [Probe on possible use of telephone and/or video calls for other health services e.g. GP, hospital]
- how did you find it?
- what would you think about having appointments in this way in the future?
There are 3 different ways a health assessment for [benefit type] can be carried out at the moment: telephone, face to face and online video call. I’d like to explore your thoughts on each of these. For each channel explore:
- how would this assessment type be suited to having a health assessment?
- what would need to be considered?
- would you have any concerns about having an assessment using this method? How could these be addressed?
What are the relative benefits of each channel – are there any ways in which telephone is better than person? Or online? [Explore for all (online vs telephone and in person)]
Overall – how would you prefer to have any future health assessments? Why?
Channel choice
Timings 10 minutes
Thinking about appointments for DWP health assessments in the future, what would you say is important to you?
Probe on:
- channel choice (i.e. perceived accessibility and accuracy of assessment)
- how quickly an assessment is held
- an assessor who specialises in your health condition
- amount of notice
- being able to take someone with you
Which of these is most important to you? Why?
Which of these is least important to you? Why?
If you had to choose, would you prefer to have the next available appointment or wait to have an assessment via your preferred channel?
Probe on reasons why
If you had to choose, would you prefer to have the next available appointment or wait to have an assessor who specialises in your health condition?
Probe on reasons why
If you had to choose, would you prefer to have your assessment via your preferred channel, or see an assessor who specialises in your condition?
Probe on reasons why
How much of a difference do you think having a choice of channels would make to the assessment experience?
- [If no difference] Why not? What do you think would make the most positive impact on the health assessment experience?
- [If would make a difference] Why? What kind of difference would it make to you?
What type of information would be useful to help you make an informed decision about the channel type to have a DWP health assessment?
Summary and wrap up
Timings 5 minutes
Thank participant for sharing their thoughts and opinions and close.
1. Moderator: Thank you for your time today. Is there anything we haven’t discussed that you would like to? Any further questions?
2. Remind participant that everything they told us today will remain confidential. Explain next steps in the research.
Signposting: If needed, signpost to further information and support available for individuals:
See Citizen’s advice (free advice for financial support)
Freephone: 0800 144 8848 (England)
0800 702 2020 (Wales)
0800 915 4604 (Northern Ireland). Monday to Friday 9am to 5pm for all locations.
Closed on public holidays.
If participant cannot hear or speak on the phone, they can type what they want to say. Text 18001 then 0800 144 8884. They can use Relay UK services with an app or a text phone. There’s no extra charge to use it.
See MIND (mental health)
3. Bring the interview to a close. Remind them of the £40 voucher incentive for taking part.