Analysis of acute flaccid paralysis and myelitis: analysis of data up to 2025
Published 2 June 2026
Applies to England

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/acute-flaccid-paralysis-and-myelitis-afpm-in-england/analysis-of-acute-flaccid-paralysis-and-myelitis-analysis-of-data-up-to-2025
Analysis
2025 data
In 2025, 10 AFP/M cases not explained by a non-infectious cause were notified in England; an incidence rate of 0.02 per 100,000 population. Eight of these occurred in children under 15 years of age; a rate of 0.08 per 100,000 under 15 population [Note 1].
AFP/M cases were reported sporadically throughout 2025. The month with the highest number of cases was December (n=3). Of the 10 cases in 2025, most (70%) were between 5 and 14 years of age. All cases with a known vaccination status were fully vaccinated for age and 50% reported international travel within 30 days preceding symptom onset.
As per UKHSA guidance, it is important that all AFP/M cases are appropriately investigated and samples sent to the Enteric Virus Unit (EVU) or Polio Reference Service (PRS) for testing on an E72 report form. ‘Adequate’ sampling is defined as 2 stool specimens of sufficient quantity for laboratory analysis, collected at least 24 hours apart, within 14 days after the onset of paralysis (WHO guidance for AFP surveillance). In 2025 this was not achieved for any of the reported cases. However, at least one stool specimen was received for 60% of cases, all of which underwent culture with no poliovirus isolated. Three cases (30%) had enterovirus PCR-reactive samples [Note 2], identified through either local testing or at UKHSA but no enterovirus genotypes were identified in any of these cases.
Figure 1. Notified AFP/M cases by month of AFP/M symptom onset and testing results, England: 2025

Historical data
Although AFP/M (not explained by a non-infectious cause) was only made notifiable in April 2025, clinicians have historically reported cases to UKHSA that required a risk assessment for polio or where NPEVs were suspected to be a cause. These data are reported here. In 2018, the UK experienced an increase in reports of cases of AFP that was temporally associated with an upsurge in EV-D68 activity. During the COVID-19 pandemic, reporting of AFP declined to very low levels due to public health measures reducing transmission [Note 3].
Figure 2. Notified AFP/M cases by year of AFP/M symptom onset, England: 2018 to 2025. [Note 3] [Note 4]
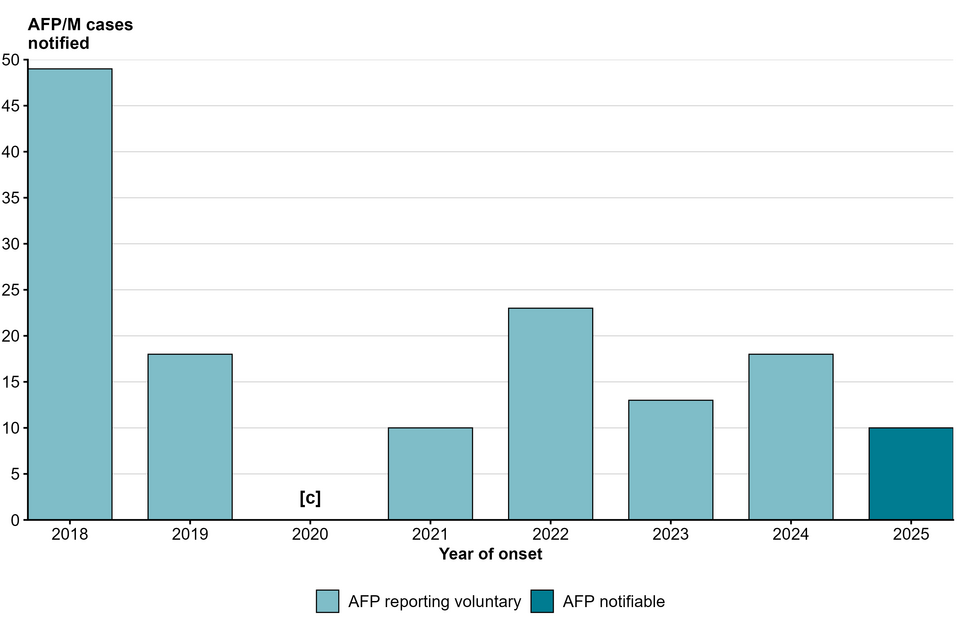
The WHO anticipates that polio-free countries should have a background rate of at least 1 AFP/M case per 100,000 population, of children under the age of 15 years (WHO guidance for AFP surveillance). Based on 2024 ONS population estimates, we would expect around 100 cases per year in the UK, suggesting that there may be significant under reporting of AFP/M.
Table 1. Overall and under 15 counts and rates of notified AFP/M cases by year of AFP/M symptom onset, England: 2018 to 2025. [Note 1] [Note 3] [Note 4]
| Age group | Year | Cases (n) | Population | Rate per 100,000 population |
|---|---|---|---|---|
| All ages | 2018 | 49 | 55,924,528 | 0.09 |
| All ages | 2019 | 18 | 56,230,056 | 0.03 |
| All ages | 2020 | [c] | 56,325,961 | [c] |
| All ages | 2021 | 10 | 56,554,891 | 0.02 |
| All ages | 2022 | 23 | 57,144,395 | 0.04 |
| All ages | 2023 | 13 | 57,932,470 | 0.02 |
| All ages | 2024 | 18 | 58,620,101 | 0.03 |
| All ages | 2025 | 10 | 58,620,101 | 0.02 |
| Under 15 | 2018 | 31 | 9,938,418 | 0.31 |
| Under 15 | 2019 | 9 | 9,929,507 | 0.09 |
| Under 15 | 2020 | [c] | 9,880,230 | [c] |
| Under 15 | 2021 | 7 | 9,818,116 | 0.07 |
| Under 15 | 2022 | 11 | 9,909,083 | 0.11 |
| Under 15 | 2023 | 6 | 9,994,919 | 0.06 |
| Under 15 | 2024 | 7 | 10,055,699 | 0.07 |
| Under 15 | 2025 | 8 | 10,055,699 | 0.08 |
Note 1: Population denominators were derived using the Office for National Statistics nomis tool. Estimates for 2025 were assumed to be the same as those for 2024, as updated estimates were not available at the time of publication.
Note 2: Striated lines represent a reactive PCR result through either local testing or at the Enteric Virus Unit (EVU) at UKHSA. Due to cross-reactivity in PCR assays, these results may indicate either enterovirus or rhinovirus detection.
Note 3: Where counts are small, trends should be interpreted with caution. Small changes in case counts can lead to large changes in rates or percentages and may not indicate real changes in incidence.
Note 4: Small counts under 5 have been suppressed and are denoted by [c].
Data sources and methodology
AFP/M cases
AFP/M cases are notified through reporting to local health protection teams (HPTs). Following notification, managing clinicians are asked to complete an enhanced surveillance questionnaire (ESQ), which queries patient administrative information, vaccination and travel history, clinical status and local testing and diagnostics. Samples, as specified in How to report a case of acute flaccid paralysis or acute flaccid myelitis, are requested to be forwarded to the Polio Reference Service (PRS), along with an E72 report form for testing. The data extracted for this report includes cases with an onset date between January 2018 and December 2025. Of note, the number of AFP cases presented in this report may vary from the notifications of infectious diseases (NOIDs) publications. Some AFP/M cases notified via NOIDs may subsequently be discarded following investigation if the most compatible diagnosis is determined to be non-infectious, such as Guillain–Barré syndrome (GBS).
Linkage to other data sources
AFP cases were linked to UKHSA Laboratory Information Management System (LIMS) system, MOLIS, to ascertain testing information from samples forwarded to the PRS, using a combination of NHS number, name and date of birth. Using the same methodology, cases were linked to the Second Generation Surveillance System (SGSS) to gather local testing data. Onset date was derived using a hierarchical algorithm; clinician-reported onset date from the ESQ was used where available. If it was not available, the first sample collection date was used, followed by the date of report to the HPT.
Denominators
Mid-year population denominators were derived using the Office for National Statistics Nomis tool. Estimates for 2025 were assumed to be the same as those for 2024, as updated estimates were not available at the time of publication.
Further information and contact details
Feeback and contact information
Feedback and specific queries about this report are welcome via phe.afp@nhs.net.
Acknowledgements
These reports would not be possible without the contributions from clinicians and microbiology colleagues in laboratories across England, without whom there would be no surveillance data.