Explainer: Infected Blood Compensation Scheme (HTML)
Updated 8 July 2026

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/infected-blood-compensation-scheme/government-update-on-the-infected-blood-compensation-scheme-html
Purpose of the document
This document explains how the Infected Blood Compensation Scheme (the Scheme) works and summarises the different compensation awards available.
The Scheme is established in law which gives the Infected Blood Compensation Authority (IBCA) the power to make compensation payments in line with the Scheme’s design. The awards outlined in this document are intended to give an idea of the compensation that eligible people may receive. Whether a person is eligible for compensation, and how much compensation they receive, will depend on IBCA’s assessment of the person’s circumstances. IBCA’s assessment will always be made in line with the design of the Scheme as set by the law.
This page was last updated on 18 June 2026 to include the changes made to the Scheme as a result of the draft 2026 regulations.
Related content
This section lists additional sources of information about the Scheme that may be helpful to review alongside this document:
- The Infected Blood Compensation Authority (IBCA) webpage is updated with the latest information about the Scheme, including how to apply
- IBCA’s compensation calculator can help people understand how much compensation they are likely to receive
- More information about interim compensation payments
- The Government’s response to the public consultation can help people to understand the most recent changes made to the Scheme
- The Technical Expert Group (TEG) report can help people to understand the expert advice on which the latest changes to the Scheme were based
Background to the Scheme
Over eight years, the Infected Blood Inquiry (the Inquiry), led by Sir Brian Langstaff, investigated the circumstances which led to and were caused by people being given infected blood (or blood products) by the UK’s National Health Services (NHS), most notably between 1970 to 1998. The Inquiry issued its Second Interim Report in April 2023, in which it made recommendations for the design of a scheme to compensate victims, and its final report in May 2024.
On 21 May 2024, the Government announced plans for the Infected Blood Compensation Scheme (the Scheme), which would be operated by a new arm’s length body called the Infected Blood Compensation Authority (IBCA).
The Government had to make regulations to formally establish the Scheme and give IBCA the powers to pay compensation. The first set of regulations came into force in August 2024, which enabled IBCA to start making core compensation awards to infected people. A second set of regulations then came into force in March 2025, increasing IBCA’s powers to make compensation payments, including paying compensation to affected people (like partners or children) and paying supplementary compensation to infected people.
In March 2025, the Inquiry announced its intention to publish an additional report to “consider the timeliness and adequacy of the Government’s response on compensation”. The Inquiry published its Additional Report in July 2025 which made a number of recommendations for IBCA and the Government in relation to the operation and design of the Scheme.
In December 2025, a third set of regulations came into force to implement some of the changes recommended by the Inquiry’s Additional Report. The Government then launched a public consultation to seek views from the infected blood community on how best to implement the remaining changes recommended by the Inquiry. The Government published its response to the consultation in April 2026, and a fourth set of regulations were made to bring the changes into law on 18 June 2026.
The Inquiry formally closed on 31 March 2026. All victims of the infected blood scandal can now register their intent to claim compensation.
Key information about the Infected Blood Compensation Scheme
This section provides an overview of key information to help readers understand some of the most important information about how the Scheme works.
- The Scheme provides financial compensation to victims of the infected blood scandal.
- The Scheme is UK-wide and operated by an independent arm’s length body called the Infected Blood Compensation Authority (IBCA).
- The Scheme is open both to those who were directly or indirectly infected, and to those who are affected through their relationship with an infected person.
- Compensation is awarded through two main ‘routes’: the core route and the supplementary route. Everyone eligible for compensation will receive a core compensation offer. Supplementary compensation awards are available in exceptional cases where the level of core compensation does not reflect the financial losses or care costs a person may have experienced.
- The Scheme has five award categories, each of which provides compensation for the harm someone suffered in different aspects of their life. The award categories, and what they provide compensation for, are: Injury (for physical and mental injury and emotional distress); Social Impact (for stigma and social isolation caused by the infection); Autonomy (for the impact of the infection on personal life, for example on relationships); Care (for past and future care costs); and, Financial Loss (for past and future financial losses, for example loss of earnings).
- Core route compensation is calculated using set payment rates called tariffs. People’s personal circumstances (like the severity of their infection, or their relationship to an infected person) are used to work out what tariff of compensation they should receive. Tariffs reduce the information that people applying to the Scheme need to provide and enable compensation to be paid more quickly.
- In exceptional cases, higher compensation awards are available for infected people through the supplementary route for the Autonomy, Care and Financial Loss award categories. Higher Financial Loss awards are also available to some affected people through the supplementary route.
- A person can choose to receive their compensation as a lump sum or series of regular payments over 5, 10 or 25 years.
- All compensation paid through the Scheme is exempt from income, capital gains and inheritance tax, and does not affect a person’s eligibility for means tested benefits.
- Accepting compensation from IBCA does not remove a person’s rights to pursue a claim in court.
- For most people, the Scheme will be open to applications for compensation until 31 March 2031. See section on time limits for application for further detail, including exceptions to this deadline for applications.
Working with others to design the Scheme
The Scheme is based on recommendations made by the Infected Blood Inquiry (the Inquiry) and guided, but not limited, by the practice in UK courts. The aim of the Scheme is to deliver fair and comprehensive compensation to victims of the infected blood scandal, with minimal delay.
A group of legal, clinical and actuarial experts, chaired by Professor Sir Jonathan Montgomery, has advised Government throughout the development of the Scheme. This group was first set up in January 2024, and was known as the Expert Group. In July 2025, the Government sought further expert advice to help it make the changes to the Scheme that the Inquiry recommended in its Additional Report. Additional experts in transfusion medicine, haematology and psychological medicine were asked to join the group. This new group was known as the Technical Expert Group (TEG). The advice provided by the EG and TEG can be found here and also here.
Representatives of the infected blood community have generously given their time to provide feedback on the Scheme’s design, including through the public consultation that closed in early 2026.
Applying to the Scheme
Victims of the infected blood scandal can register their intent to claim compensation on IBCA’s website.
Eligibility
The Scheme provides financial compensation to both infected and affected victims of the infected blood scandal. Where an eligible infected or affected person has died, the personal representative of their estate may be able to claim compensation.
Infected people
Infected people are those who have been either directly or indirectly infected, as summarised in the table below.
A directly infected person is someone who through the use of NHS-supplied blood, blood products and/or tissue is or was infected with:
- HIV;
- acute or chronic Hepatitis C;
- chronic Hepatitis B;
- acute Hepatitis B and died from acute liver failure within 12 months of the infection (or within 12 months of the reactivation of infection).
An indirectly infected person is someone who was infected:
- by a person who is or was directly infected (e.g. a person infected by their partner);
- by a person who was infected by someone who was directly infected (e.g. a child infected by their mother who was infected by her partner).
An infected person who has recovered from or ‘cleared’ their infection can still apply for compensation.
People who were infected after blood screening was introduced may be asked to provide additional evidence to IBCA. This is because blood screening significantly reduced the risk of getting an infection from a blood transfusion or blood product, so IBCA will need to establish that, on the balance of probabilities, the infection came from NHS blood products rather than another source. The dates when blood screening was introduced for different infections are listed below:
- HIV infection - November 1985;
- Hepatitis C infection - September 1991;
- Hepatitis B infection - December 1972.
People registered on a current UK Infected Blood Support Scheme (IBSS) and those who were in receipt of support payments from one or more of the Alliance House Organisations (AHO)[footnote 1] are considered automatically eligible for compensation through the Scheme, but may need to provide some additional information for IBCA to accurately calculate their compensation award.
Infected organs transplant scheme
People who knowingly accepted an infected organ transplant through the NHS Transplant Scheme cannot claim compensation for that infection. They may be eligible if, however, that transplant caused a separate, unexpected infection.
Affected people
Affected people are those who have suffered the impacts of infected blood because of their relationship with an infected person. Affected people whose loved one had an acute Hepatitis C infection are not eligible for compensation through the Scheme.
Partners of eligible infected people include:
- spouses;
- civil partners;
- partners who lived with their infected partner for at least one year following infection.
If an eligible infected person has had more than one partner whilst infected, all of those partners can apply for compensation in their own right. Partners who separated from the infected person before infection are not eligible for compensation.
Parents of an eligible infected person, include:
- biological parents;
- adoptive parents;
- others acting in the capacity of a parent as described below (e.g. step parents, grandparents);
Parents must have cared for and lived with the infected person for at least a year while they were under 18. Parents of infected children are eligible no matter the age at which their child was infected, but compensation rates are higher for parents of children infected under the age of 18.
Children of an eligible infected person, include:
- biological children;
- adoptive children;
- others in the position of a child as described below (e.g. step children);
Children must have been cared for and living with their eligible parent for at least a year while under the age of 18. Children of infected parents are eligible regardless of whether they were living with the parents at the time of infection, but compensation rates are higher for children whose parent was infected while they were under the age of 18.
Siblings of eligible infected people, include:
- biological and adoptive siblings;
- step siblings;
- others in the position of a sibling as described below;
Siblings must have lived with their infected sibling for at least two years while under the age of 18. Siblings of infected people are eligible no matter how old they were when their sibling was infected, but compensation rates are higher for siblings who were under 18 at the time of infection.
Carers are people who have provided significant, unpaid care to an infected person. To be eligible for the Scheme, a carer must have provided an average of 16.5 hours of care per week to an eligible infected person for a minimum of six months after they were infected.
Estate applications
If an eligible infected person has died before receiving their compensation, the person managing their estate can apply for compensation.
If an eligible affected person dies between 21 May 2024 and 31 March 2031 and before receiving their compensation, the person managing their estate can apply to receive their compensation.
Applications on behalf of a child or person who lacks capacity
For children under 18, compensation will be paid to the person with parental responsibility for them. For people who lack mental capacity, compensation will be paid to the person with power of attorney or other legal authority to act on their behalf.
Multiple claims
Some people may be able to make multiple claims for compensation. This could be, for example, if they have more than one infected family member. Another example is if a person is both infected themselves and affected by the infection of a loved one. Further detail can be found in the section Compensation awards where an applicant has multiple claims.
Design of the Scheme
This section explains the basic features of the Scheme’s design to help people understand how their or their loved one’s circumstances are assessed in order for compensation to be calculated.
Tariffs
The Scheme uses set payment rates called tariffs to calculate compensation. Tariffs minimise the amount of personal information that people need to provide to receive compensation and help compensation to be paid quicker than would be possible if individual assessments were needed. The tariffs used in the Scheme have been informed, but not limited, by the current practice in UK courts.
Core and supplementary routes
The Scheme has two routes for awarding compensation: the core route and the supplementary route.
Everyone who is eligible for the Scheme will receive compensation through the core route.
In some exceptional cases, after core compensation has been awarded, people may be eligible to receive additional compensation through the supplementary route. For infected people, this may be because they had a very high income before they were infected, or if their particular health condition meant they needed more care than covered by their core compensation award. For bereaved affected people, this may be because they were financially dependent on their infected loved one and did not receive compensation reflecting this as part of their core route compensation award.
The below section ‘Award categories’ sets out the different awards available through the core route.
Award categories
There are five categories of award available through the core route. Each award provides compensation for the different impacts of infected blood on people’s lives. The table below explains the awards available through the core route.
| Category of Award | Description | How the award works for an infected person | How the award works for an affected person |
|---|---|---|---|
| Injury award | Recognises the physical and mental injury, emotional distress and injury to feelings caused by infected blood and related medical treatments, the death of an infected person, or the likely death of a loved one in the future. | A fixed financial award based on the type of infection and its progression. | A fixed financial award based on the affected person’s relationship with the infected person, their infection and its progression. |
| Social Impact award | Recognises the social impact of infected blood that victims may have suffered, for example, stigma and social isolation. | A fixed financial award based on whether the infected person suffered from one infection or multiple infections and if these infections were chronic or acute. | A fixed financial award based on the affected person’s relationship with the infected person. |
| Autonomy award | Recognises the impact of infection on family and private life (e.g. loss of marriage or partnership, loss of opportunity to have children). | A fixed financial award based on the type of infection, infection progression and the person’s age at the time of infection. | Only available to affected partners, parents and children. A fixed financial award based on the affected person’s relationship with the infected person. |
| Care award | Recognises the cost of past and future care needs for infected people. | Calculated based on typical past and future care needs for the type of infection and its progression. | Not available to affected people in their own right. Infected people can choose to pay some or all of their Care award to affected people. |
| Financial Loss award | Recognises the past and future financial losses caused by infection. | All infected people receive £12,500 and most will be eligible for more. The amount depends on the type of infection, its progression, the person’s healthy life expectancy, years at working age and pension age, and in some cases the dates that effective treatment started. | Only available to some bereaved affected people who were dependent on the infected person’s income. Calculated from the year the infected person died to their estimated healthy life expectancy. |
There are an additional four types of award available through the supplementary route. These awards are available in exceptional cases to people after they have received their core route compensation offer. The table below explains the awards available through the supplementary route.
| Category of Award | Description | How the award works for an infected person | How the award works for an affected person |
|---|---|---|---|
| Unethical research award | Compensates infected people who were likely to have been victims of unethical research. | Any infected person treated for a bleeding disorder in the UK before 1986 is automatically eligible. Higher awards are given to people treated whilst under 18, or whilst a student at Lord Mayor Treloar’s school between 1970 and 1983. | Not available for affected people. |
| Severe Health Condition award | Compensates infected people who have developed uncommon and severe health conditions as a result of their infection which are not covered already through the core route. | This award may give higher Financial Loss and Care awards to people with a qualifying severe health condition. This is to recognise that a person with a severe health condition is likely to be less able to work and have higher care needs. | Not available for affected people. |
| Exceptional Loss award | Compensates infected people who have experienced higher financial loss and care costs than recognised through the core route. | Awards for Exceptional Financial Loss are typically calculated based on records of actual earnings. A separate £60,000 award is available for people in high-paying careers who would have earned highly if not for their infection. Awards for care costs are based on records of paid-for professional care. |
Not available for affected people. |
| Supplementary Financial Loss award for affected people | Compensates bereaved affected people who were financially dependent on an infected person before they died. | Not available for infected people. | Affected siblings and parents who can show they were financially dependent on their infected loved one before they died can receive Financial Loss awards. Bereaved disabled children who would have continued to be financially dependent in adulthood can receive additional Financial Loss awards. |
Infection severity
The amount of compensation a person is eligible for depends on the severity and progression of their infection, or their loved one’s infection. The severity of a person’s infection is categorised in the Scheme using infection severity bands. In general, the more severe someone’s infection, the more compensation they are likely to receive. These bands are based on clinical diagnostic markers so that a person’s infection severity can be easily determined from their medical records. There are different levels of infection for Hepatitis B and C infections, and single severity bands for HIV infections. The infection severity bands are listed in the table below. More detailed descriptions can be found at Annex C.
| Infection severity band | Description of infection |
|---|---|
| Level 1 Hepatitis | Acute Hepatitis C infection |
| Level 2 Hepatitis | Chronic Hepatitis C and / or Chronic Hepatitis B infection |
| Level 2B Hepatitis | Chronic Hepatitis C and / or Chronic Hepatitis B infection, where the infection has been treated with Interferon |
| Level 3 Hepatitis | Hepatitis C and / or Hepatitis B infection, where the infection has caused cirrhosis |
| Level 4 Hepatitis | Hepatitis C and / or Hepatitis B infection, where the infection has caused decompensated cirrhosis, liver cancer and/or liver transplant |
| Level 5 Hepatitis | Acute Hepatitis B infection where the person has died from acute liver failure within 12 months of infection or the reactivation of infection |
| HIV | HIV infection only |
| Co-infection including HIV | HIV, with Hepatitis B or Hepatitis C infection |
Calculating compensation awards
The amount of compensation a person is eligible for depends on a range of factors. IBCA has developed a calculator which can be used to provide an estimate of how much compensation a person may be entitled to based on their circumstances.
This section explains all the awards available through the Scheme’s core and supplementary routes. The tables at Annex A set out the value of the awards in further detail.
Understanding the core route awards
Injury awards
Injury awards provide compensation for the physical and mental harm a person has suffered due to infected blood.
They are:
- Available to all infected and affected people through the core route.
- Fixed rate financial compensation awards.
- For infected people, Injury awards are based on infection severity.
- For affected people, Injury awards are based on infection severity, the relationship between the infected and affected person, and the affected person’s age at the time of their loved one’s infection.
- Not available through the supplementary route.
The tables at Annex A set out the rates of core route Injury awards.
Social Impact awards
Social Impact awards provide compensation for the stigma, isolation and disruption to social life that a person may have suffered as a result of infected blood.
They are:
- Available to all infected and affected people through the core route.
- Fixed rate financial compensation awards.
- For infected people, Social Impact awards are higher for co-infections.
- For affected people, Social Impact awards are higher for people affected whilst under 18.
- Not available through the supplementary route.
The tables at Annex A set out the rates of core route Social Impact awards.
Autonomy awards
Autonomy awards provide compensation for the impact of infected blood on a person’s family and private life.
They are:
- Available to all infected people through the core route.
- For infected people, Autonomy awards are based on infection severity.
- Higher Autonomy awards are available for people who were infected under 18 given the disruption to childhood.
- Additional Autonomy awards are available through the supplementary route for infected people subjected to unethical research practices.
- Autonomy awards are available to affected people assumed to have suffered the greatest impact on their autonomy, including partners, children and parents of infected people. Siblings and carers of infected people are not eligible for Autonomy awards.
The tables at Annex A set out the rates of core and supplementary route Autonomy awards.
Care awards
Care awards provide compensation for the cost of past and future care needs of infected people.
They are:
- Available to all infected people through the core route.
- For infected people, core route Care awards are based on infection severity and the assumed care needs for people with that level of infection.
- Based on the average commercial care costs in the UK.
- Care awards for the estates of an infected person are discounted by 25% on the assumption that this care was given free of charge by loved ones and therefore exempt from taxes. If an infected person paid for professional care in the past, the 25% deduction may be removed or higher Care awards may be available through the supplementary route.
- Affected people are not eligible for their own Care award. However, an infected person can choose for some or all of their Care award to be paid directly to the affected people who cared for them.
The tables in Annex A and Annex B set out the rates of core and supplementary Care awards.
Financial Loss awards
Financial Loss awards provide compensation for the past and future financial losses suffered due to infected blood.
They are:
- Available to all infected people through the core route.
- Available only to bereaved partners and children under 18 at the time of their infected parent’s death through the core route. Other bereaved affected people may be able to apply for a Financial Loss award through the supplementary route if they were financially dependent on their infected loved one when they died.
- Higher Financial Loss awards are available through the supplementary route for infected people who have suffered greater loss of earnings or paid more in care costs than covered by the core route.
Financial Loss awards for infected people
- All infected people are eligible for a flat-rate award of £12,500 to cover miscellaneous expenses associated with infection, for example, costs of travelling to appointments. Where a person died due to an acute Hepatitis B infection (Level 5 or HIV / Level 5 Hepatitis co-infection), this award increases to a flat-rate of £17,500.
- In addition to this flat-rate award, with the exception of acute infections, infected people are compensated for the earnings they have lost and may in future continue to lose due to infection and treatment. To calculate lost earnings, the Scheme takes into account factors such as the severity of a person’s infection and whether effective treatment was available that may have improved their health and increased their ability to earn.[footnote 2]
- For each year that a person is infected at working age - between 16 years old and 65 years old, years inclusive - they can be eligible for up to £29,657. This maximum award, which is based on the net median UK earnings in 2023[footnote 3] + 5%, is available where the assumption is that the infected person could not work at all due to infection. For every year between retirement age (from 66 years old) and a person’s healthy life expectancy[footnote 4] they are eligible for 50% of their working age rate, to reflect a pension payout.
- For HIV and HIV/Hepatitis co-infections, people may not have experienced symptoms for some time after infection, so compensation is paid from the date of infection and increases from the date of diagnosis.
Financial awards for affected people
- Bereaved partners and children who were under 18 when their infected parent died are automatically eligible for core route Financial Loss awards. This is because they are assumed to have some level of financial dependency on their infected loved one.
- Other bereaved affected people may be eligible for supplementary route Financial Loss awards if they can show they were financially dependent on their infected loved one for at least six months before they died.
Paying Financial Loss awards
- Where an infected person is living, the Financial Loss award is paid to the infected person.
- Where an infected person has died, the portion of the award that compensates for past financial loss (i.e. from the point of infection to death) is paid to the estate of the infected person. Bereaved partners and children under 18 receive a Financial Loss award to compensate for the years that they would likely have otherwise been financially supported by the infected person.
Understanding the supplementary route awards
This section explains the supplementary route awards available to infected and affected people.
People can only apply for supplementary route compensation after their core route assessment is complete. This is because some of the awards build on the core compensation offer.
Unethical Research award
This award gives additional compensation to infected people who have been victims of unethical research practices.
Anyone who was treated for a bleeding disorder in the UK before 1986 is eligible for this award. People who were adults at the time of treatment will receive an award of £30,000, while people treated as children will receive £45,000.
Children who were treated for a bleeding disorder between 1970 and 1983 whilst attending Lord Mayor Treloar College are eligible for an award of £60,000.
These awards do not stack. A person will only receive one Unethical Research award, which will be the highest award their circumstances makes them eligible for.
Severe Health Condition awards
This award offers higher Financial Loss and Care awards for infected people who have developed specific rare conditions linked to their infection that are not fully compensated in core route compensation.
To qualify for a Severe Health Condition award, an infected person (or their estate representative) needs to show they have been diagnosed with a health condition in one of the following groups (see Annex D for more detailed descriptions of qualifying conditions):
- Group One - Severe visual impairment;
- Group Two - Neurological disorder resulting in long-term severe physical or mobility disability;
- Group Three - Neurological disorder resulting in long-term severe neurocognitive impairment;
- Group Four - Severe psychiatric disorder, potentially resulting in inpatient psychiatric care;
- Group Five - End-stage kidney disease requiring renal replacement therapy;
- Group Six - Other hepatic disorders caused by Hepatitis B or Hepatitis C resulting in long-term severe disability;
- Group Seven - Special Category Mechanism (SCM)
If an infected person has suffered a qualifying severe health condition as a result of their infection, further compensation may be available for the associated care costs and financial loss they experienced. This award does not change the value of a person’s Injury, Social Impact or Autonomy awards. The exact amount of additional compensation a person receives will depend on the amount they are already eligible for through their core route compensation. This is because the Financial Loss and Care awards available through the Severe Health Condition award act as ‘top up’ awards. If a person’s core route compensation for the years following their diagnosis with a severe health condition is lower than the amounts available through the Severe Health Condition awards, the person’s compensation will be increased by the difference. If a person is already receiving the same or higher compensation through the core route, the value of their compensation will not change.
Key points on eligibility:
- HIV: People with HIV who qualify for a Severe Health Condition award will generally not receive higher Financial Loss awards. This is because they already receive the maximum Financial Loss award through the core route, based on the assumption they are unable to work at all after diagnosis. Higher Care awards may be available.
- Retirement age: If a person is diagnosed with a qualifying severe health condition in the year they turn 66, they are not eligible for increased Financial Loss awards as their condition would not have affected their ability to earn.
- IBSS: People who receive SCM payments (or an equivalent) through an IBSS will continue to do so if they choose to continue receiving Support Scheme payments for life without needing to provide further evidence of meeting the Severe Health Condition award eligibility criteria.
- Estates: Where a person who would have qualified for a Severe Health Condition award has died, their estate representative can apply for this award. Estates of infected people in Group 7 can only receive an award if the infected person was receiving SCM payments before they died. Care awards for estates are 25% lower than for living infected people on the assumption that care in the past was given free of charge by loved ones and therefore exempt from taxes.
The table below explains the Financial Loss and Care awards available for each severe health condition.
Qualifying severe health conditions
| Severe health conditions | Infection severity band | Potential Financial Loss award adjustment | Potential Care award adjustment |
|---|---|---|---|
| Group 1 Severe visual impairment |
HIV | No additional award possible - core route already gives the maximum Financial Loss award based on 0% ability to work. | Living infected person: £5,460 per year from date of severe health condition diagnosis (Level 1 care band). Estate of infected person: £4,095 per year from date of severe health condition diagnosis to death of infected person. |
| Group 2 Neurological disorders resulting in long-term severe physical or mobility disability |
HIV and Level 4 Hepatitis | No additional award possible - core route already gives the maximum Financial Loss award based on 0% ability to work. | Living infected person: Up to £23,424.72 per year from date of severe health condition diagnosis (Level 2 care band). Estate of infected person: Up to £17,568.54 per year from date of severe health condition diagnosis to death of infected person. |
| Group 2 Neurological disorders resulting in long-term severe physical or mobility disability |
Level 2, 2B and 3 Hepatitis | If the person can show they were unable to work for all or part of the year, their award may be adjusted to £29,657 per year from year of severe health condition diagnosis until the year they turn 65. Award then reduces to £14,828.50 per year to reflect retirement to healthy life expectancy. | Living infected person: Up to £23,424.72 per year from date of severe health condition diagnosis (Level 2 care band). Estate of infected person: Up to £17,568.54 per year from date of severe health condition diagnosis to death of infected person. |
| Group 3 Neurological disorders resulting in long-term severe neurocognitive impairment |
HIV and Level 4 Hepatitis | No additional award possible - core route already gives the maximum Financial Loss award based on 0% ability to work. | Living infected person: Up to £23,424.72 per year from date of severe health condition diagnosis (Level 2 care band). Estate of infected person: Up to £17,568.54 per year from date of severe health condition diagnosis to death of infected person. |
| Group 4 Severe psychiatric disorder |
HIV | No additional award possible - core route already gives the maximum Financial Loss award based on 0% ability to work. | Living infected person: £5,460 per year from date of severe health condition diagnosis (Level 1 care band). If a person can provide a social services needs assessment showing that they require higher levels of care in line with the Level 2 care band, they may be entitled to an adjusted award of up to £23,424.72 per year. Estate of infected person: £4,095 per year from date of severe health condition diagnosis to death of infected person. Up to £17,568.54 per year if the person was assessed as needing Level 2 care. |
| Group 4 Severe psychiatric disorder |
Level 2, 2B, 3 and 4 Hepatitis | If the person can show that they were unable to work for all or part of the year, their award may be adjusted to £29,657 per year from severe health condition diagnosis to the year the person turns 65. Award then reduces to £14,828.50 per year to reflect retirement to healthy life expectancy. | Living infected person: £5,460 per year from date of severe health condition diagnosis (Level 1 care band). If a person can provide a social services needs assessment showing that they require higher levels of care in line with the Level 2 care band, they may be entitled to an adjusted award of up to £23,424.72 per year. Estate of infected person: £4,095 per year from date of severe health condition diagnosis to death of infected person. Up to £17,568.54 per year if the person was assessed as needing Level 2 care. |
| Group 5 End-stage kidney disease requiring renal replacement therapy (RRT)* |
HIV | No additional award possible - core route already gives the maximum Financial Loss award based on 0% ability to work. | Living infected person: £5,460 per year from date of severe health condition diagnosis (Level 1 care band). Estate of infected person: £4,095 per year from date of severe health condition diagnosis to death of infected person. |
| Group 5 End-stage kidney disease requiring renal replacement therapy (RRT)* |
Level 2, 2B, 3 and 4 Hepatitis | Award adjusted to £29,657 per year from year of severe health condition diagnosis to the year the person turns 65. Award then reduces to £14,828.50 per year to reflect retirement to healthy life expectancy. | Living infected person: £5,460 per year from date of severe health condition diagnosis (Level 1 care band). Estate of infected person: £4,095 per year from date of severe health condition diagnosis to death of infected person. |
| Group 6 Other Hepatic disorders resulting in long-term severe disability |
Level 2, 2B, 3 and 4 Hepatitis | Living person with Hepatitis B: For people born in or before 1953: £20,760 per year. For people born after 1953: £20,760 per year before availability of effective treatment (up to and including 2008); £17,794 per year after effective treatment (from 2009 onwards). Living person with Hepatitis C: For people born in or before 1961: £20,760 per year For people born after 1961: £20,760 per year before availability of effective treatment (up to and including 2016); £17,794 per year after effective treatment (from 2017 onwards). Estate of infected person: Fixed award of £71,178. |
Living infected person: £5,460 per year from date of severe health condition diagnosis (Level 1 care band). Estate of infected person: Up to £40,950 (10 years of Level 1 care band). |
| Group 7 Special Category Mechanism |
Level 2, 2B, 3 and 4 Hepatitis | Living person with Hepatitis B: For people born in or before 1953: £20,760 per year. For people born after 1953: £20,760 per year before availability of effective treatment (up to and including 2008); £17,794 per year after effective treatment (from 2009 onwards). Living person with Hepatitis C: For people born in or before 1961: £20,760 per year. For people born after 1961: £20,760 per year before availability of effective treatment (up to and including 2016); £17,794 per year after effective treatment (from 2017 onwards). Estates of people on SCM through IBSS: If the infected person was receiving SCM payments through an IBSS before they died, their estate will be eligible for the same awards as a living infected person, as outlined above. |
Living infected person: £5,460 per year (Level 1 care band) from date of IBSS SCM assessment, or from 2017 for new SCM applicants. Estate of infected person: If the infected person was receiving SCM payments through an IBSS before they died: £4,095 per year from date of IBSS SCM assessment to death. |
*If a person who qualifies for Group 5 has a successful kidney transplant prior to claiming compensation, they will only be eligible for the Severe Health Condition award for the years prior to and including the year of their successful transplant.
Exceptional Loss awards
Exceptional Loss awards give additional compensation to infected people (or their estate) who have suffered higher financial loss and/or care costs than the core route compensates for as a result of their infection.
An infected person may be eligible for an Exceptional Loss award if they:
- were a particularly high earner before they were infected and had to reduce or give up this work;
- had started or been offered a job in a career where the average salary was over £38,504;[footnote 5]
- paid for professional care in the past to support them with their infection.
Exceptional Loss awards are based on a person’s individual circumstances. IBCA will therefore need to ask for more detailed evidence so they can accurately calculate the appropriate compensation. Examples of records a person may be able to use as evidence for this award include but are not limited to: records of earnings, invoices of care costs, employment offers, and evidence of early medical retirement.
There are five types of Exceptional Loss award: three for exceptional loss of earnings, and two for exceptional care costs. The five awards are set out in the tables below.
Awards for Exceptional Loss (Earnings)
The three awards available for exceptional loss of earnings are below. The type of award a person may be eligible for will depend on their circumstances. A claimant can only receive one of the three awards.
| Award | Who? | What the award covers | Value of award | Evidence required |
|---|---|---|---|---|
| Exceptional Financial Loss: PAYE earnings | Infected people who were employees and can evidence earnings above the core route before infection. | Any income covered by PAYE (e.g. basic pay and overtime pay). Assumed salary progression (i.e. the pay increases that a person might have had over their career lifetime if they had not been infected). A pension award, set at a 6.1% contribution rate to reflect private sector pension contributions. |
Calculated based on the person’s actual earnings. The highest award available equates to a gross salary of £76,249 per year. | Evidence of annual earnings from the point that earnings first reduced until the year they applied to the Scheme or turned 65. Evidence of salary in the year prior to infection. |
| Exceptional Financial Loss: self-employment earnings | Infected people who were self-employed and can evidence earnings above the core route before infection. | Any income covered by PAYE (e.g. basic pay and overtime pay). No pension award is given as self-employed people would not have received employer contributions to a pension. |
Calculated based on the person’s actual earnings. The highest award available equates to a gross salary of £76,249 per year. | Evidence of annual earnings from the point that earnings first reduced until the year they applied to the Scheme or turned 65. Evidence of salary in the five years prior to infection. |
| Exceptional Financial Loss: Potential earning capacity | Infected people who do not have evidence of earning more than the core route but can show they had a job (or job offer) in a career where the average salary was above £38,504. | A flat rate award to recognise the probability that infected people already on the path to a high-earning career would likely have earned above the core route if they had not been infected. | £60,000 one-off award. | Evidence of either being employed in or having a job offer for a career where the average salary was above £38,504. Evidence must date from before the infected person turned 66. For evidence of employment, the work must have occurred within 10 years of infection. For evidence based on a job offer that was not taken up, that offer must have been made within one year of infection (unless there were extenuating circumstances). |
Awards for Exceptional Loss (Past care costs)
The two awards available for exceptional loss due to past care costs are below. A claimant can only receive one of the two awards.
Both awards offer additional compensation for infected people (or their estates) who can show that they paid for professional care before 1 April 2025. Which award a person may be eligible for depends on the cost and duration of the professional care they have received.
| Award | Who? | Value of award | Evidence required |
|---|---|---|---|
| Exceptional Loss: Excess deemed care costs | Estates of infected people or living infected people who have received treatment with Interferon and who can show they paid for care for at least six months. | The amount of care that the person paid for will be matched to the relevant care band (see Annex B). The value of the award will be calculated based on 25% of the relevant care band value (the remaining 75% will have already been given through the core route). | Evidence of six months of paid-for care, detailing the care provided. |
| Exceptional Loss: Excess actual care costs | Any infected person who can show that the cost of their past care exceeded the compensation provided through the core route (and Severe Health Condition award, where appropriate). | The value of the award will reflect the additional amount that a person paid for care beyond the core Care award (and Severe Health Condition award, where appropriate). The maximum value of the additional award is 25% of the person’s core past Care (and Severe Health Condition, if appropriate) award. | Evidence of all past care costs. |
Supplementary route Financial Loss award for affected people
The only groups of affected people eligible for a core route Financial Loss award are bereaved partners and children. This is because they are assumed to have been financially dependent on the infected person when they died.
The Supplementary Financial Loss award allows other groups of bereaved affected people who were financially dependent on their infected loved one before they died to apply for a Financial Loss award. It also enables bereaved children who would likely have continued to be financially dependent on their infected parent in adulthood due to disability to receive additional Financial Loss compensation.
These awards work in the same way as Financial Loss awards for infected people and are calculated based on the anticipated ‘working lifetime’ of the infected person. Awards are therefore higher for any years that the infected person would have been at working age, and reduce by 50% from the year they would have turned 66 to reflect a pension income that continues until the infected person’s healthy life expectancy.
The table below sets out the supplementary Financial Loss awards available for affected people.
| Who? | Eligibility | Award amount |
|---|---|---|
| Bereaved dependent parents | To be eligible, a person will need to show they were financially dependent on their infected child at the time of, and for six months prior to death. Evidence could include the provision of housing or meals. | £5,561 per year from the year after the infected person’s death to the year the infected person would have turned 65. £2,780.50 per year from the year the infected person would have turned 66 (retirement age) to their healthy life expectancy. |
| Bereaved dependent siblings | To be eligible, a person will need to show they were financially dependent on their infected sibling at the time of, and for six months prior to death. Evidence could include the provision of housing or meals. | £5,561 per year from the year after the infected person’s death to the year the infected person would have turned 65. £2,780.50 per year from the year the infected person would have turned 66 (retirement age) to their healthy life expectancy. |
| Bereaved children with a disability that leads to financial dependence on a parent in adulthood | Disabled people with a relevant disability under Section 6 of the Equality Act 2010. | £5,561 per year from the year after the infected person’s death to the year the infected person would have turned 65. £2,780.50 per year from the year the infected person would have turned 66 (retirement age) to their healthy life expectancy. If the bereaved child lost both parents to infected blood while under 18, higher awards are available: £22,243 per year from the year after the infected person’s death to the infected person’s estimated healthy life expectancy; £16,682.25 for years where one parent would have been 66 or older; £11,121.50 for years where both parents would have been 66 or older. Any core route Financial Loss awards will be deducted from the above totals. |
Compensation awards where an applicant has multiple claims
There are some instances where a person may be eligible to make multiple claims for compensation.
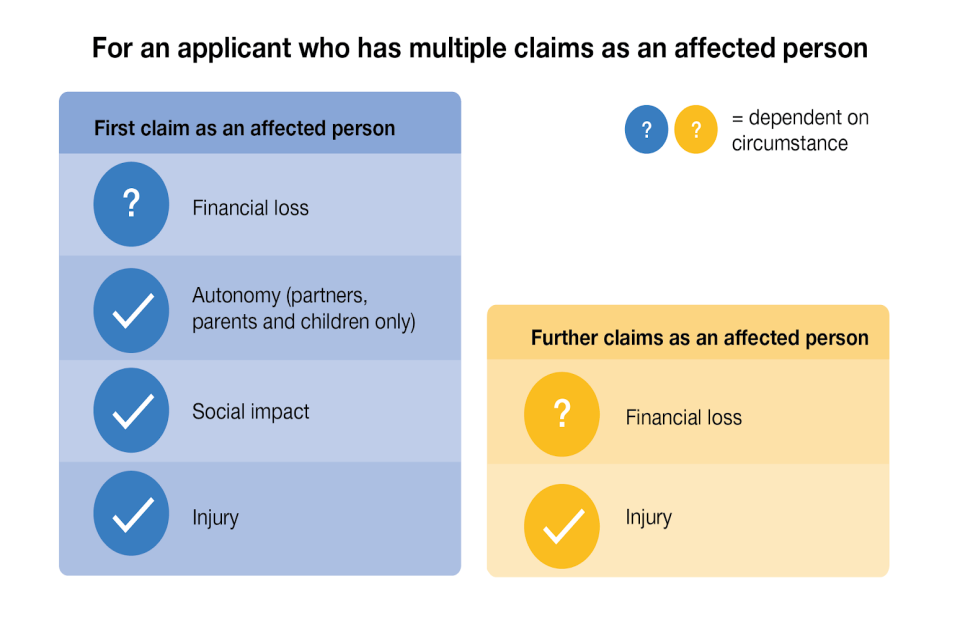
One example is where someone has multiple loved ones who have been infected (for example, where a parent and a sibling have been infected). In this case, IBCA will review all the claims at once and provide a single, comprehensive compensation award. In this scenario, through the core route the affected person would be entitled to multiple Injury awards, one for each claim. They may also be eligible for multiple Financial Loss awards, depending on their circumstances. Regardless of how many claims the person is making, they will only ever receive one Social Impact and Autonomy award. This is shown in the diagram below.
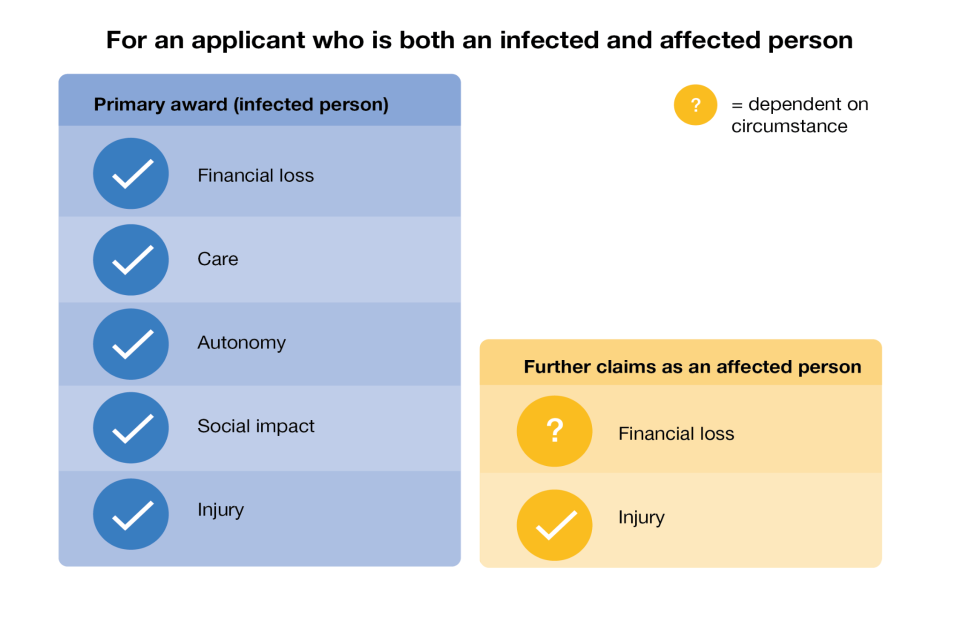
Another example where a person may be eligible for multiple claims is if they are both an infected and an affected person (for example, if the person is infected themselves and has an infected family member). In this case, IBCA will need to review and assess each claim separately as it is made. A person in this situation would be eligible for all the awards available to infected people, as well as an additional Injury award based on the number of affected claims. Additional Financial Loss awards may be available depending on circumstance. This is shown in the diagram below.
Infected Blood Support Scheme (IBSS) Payments
All eligible infected people or their bereaved partners who were registered with an IBSS before 1 April 2025 will continue to receive Support Scheme payments for life, should they choose to do so. If an infected person dies after 1 April 2025 and before receiving compensation from IBCA, their bereaved partner can still register for IBSS and choose to receive Support Scheme payments for life if they wish.
Responsibility for making support payments will transfer from the IBSS to IBCA from the following dates in early 2027. This transfer will not have any impact on the regular payments that a person receives.
- Wales Infected Blood Support Scheme: 15 January 2027
- Scotland Infected Blood Support Scheme: 1 February 2027
- Infected Blood Payment Scheme for Northern Ireland: 1 February 2027
- England Infected Blood Support Scheme: 23 March 2027
For IBSS beneficiaries who choose to continue receiving Support Scheme payments for life, Support Scheme payments will not be taken into account when assessing an applicant’s Injury, Social Impact, or Autonomy awards, or in relation to past Financial Loss or past Care awards. Applicants will be able to access these parts of their compensation as a lump sum or periodic payment over 5, 10 or 25 years.
Any Support Scheme or discretionary payments made on or after 1 April 2025 will be taken into account when IBCA calculates the compensation awards relating to a person’s future financial loss and care costs. This is because both awards are providing compensation for the financial loss and care needs that a person is expected to experience in future. Pre-payment prescription certificates or grants for talking therapy will not be taken into account when compensation awards are calculated.
For infected IBSS beneficiaries, IBCA will compare their future Financial Loss and future Care awards with the Support Scheme payments that they could expect to receive through their lifetime. If the infected person would have received more money through the Scheme, a ‘top up’ award will be given. If the awards under the Scheme would be lower than the amount the person could expect to receive through future Support Scheme payments, this will have no impact and the person will continue to receive Support Scheme payments at the same rate, increasing annually in line with CPI. Bereaved partners are not eligible for this ‘top up’ award.
If an IBSS beneficiary chooses to stop receiving Support Scheme payments and to instead receive all their compensation through the Scheme, they will need to de-register from IBSS (or opt out once IBCA takes responsibility for making the payments).
Managing money received through compensation awards
Living infected and affected people can choose to receive their compensation as:
- a single lump sum payment;
or
- a series of regular payments (instalments) over a 5, 10 or 25 year period, which are uplifted annually in line with CPI.
Individuals are able to, after receiving compensation, switch from their Support Scheme payments to a core award, and from periodic payments to a lump sum, if they wish to.
Where the infected person has died, estate representatives will receive compensation as a single lump sum payment which can then be distributed to beneficiaries of the estate as appropriate.
Where an affected person has died after accepting a claim but before receiving the full balance of their compensation, their estate will receive the remainder of the compensation as a single lump sum payment which can then be distributed to beneficiaries of the estate as appropriate.
IBCA provides financial advice and support that can assist people awarded compensation with managing their compensation awards, accessing financial services, and accessing benefits advice where relevant.
Returning to the Scheme for reassessment due to health deterioration
The compensation awards are designed in a way that accounts for the severity of a person’s infection, as well as the likely progression of their infection over time. For example, Care awards take into account the different care needs that someone will be expected to have across their whole life, on the basis of their infection severity.
However, there will be times where an infected person’s health deteriorates so that they change severity banding, or develop a new severe health condition after receiving their initial compensation award. Depending on their exact circumstances and how much they have previously been awarded by the IBCA, an infected person in this situation may be eligible for more compensation in recognition of the impact this health deterioration is likely to have on their future life. This is known as a ‘return to the Scheme’.
The table below sets out the two circumstances in which someone can return to the Scheme for reassessment, and what the options are for each circumstance.
| Type of health deterioration | Infected people | Affected people |
|---|---|---|
| Infection severity band change | If an infected person’s health deteriorates and they are diagnosed with a new condition that changes their severity band, they will be able to return to the Scheme for reassessment. An infected person can return to the Scheme for reassessment as many times as their condition changes severity band. Returning to the Scheme for a severity band change will result in a further core award payment. Return to scheme for a severity band change may also enable an infected person to apply for an Exceptional Loss award via the supplementary route. After their first application, an infected person will only be able to have their supplementary award reassessed once. |
An affected person’s compensation does not change if an infected person returns to the Scheme. |
| Development of new Severe Health Condition | If an infected person’s health deteriorates and they develop a new severe health condition (regardless of whether they were previously assessed to have a severe health condition), they may be able to return to the Scheme. Where an infected person develops a new severe health condition as a result of their infection, they can only return to the Scheme once. |
An affected person’s compensation does not change if an infected person returns to the Scheme. |
If an infected person receives their core route compensation from IBCA, then returns to IBCA to be assessed for a supplementary route award, this will not be considered a return to the Scheme.
Returning to the Scheme for a reassessment following a health deterioration will be possible regardless of the amount of time that has passed since a person’s initial assessment and award of compensation by IBCA. However, the reassessment does need to happen within six years of the diagnosis of the new health deterioration.
Death during the application process
Death of an infected person:
- If an infected person has accepted their compensation offer and dies before receiving their payment, their compensation will be paid to the personal representative of their estate.
- If an infected person dies before they have accepted their compensation offer, their personal representatives will need to start a new application. IBCA will use the evidence submitted for their original application so this does not have to be provided again.
- If an infected person is receiving support payments or periodic compensation payments at the time of their death, their support payments will stop and the outstanding balance of their total compensation award will be paid to the personal representative of their estate.
Death of an affected person:
- If an affected person dies between 21 May 2024 and 31 March 2031 and before receiving their compensation, the personal representative of their estate will be able to apply to receive their compensation.
- Where an affected person has died after accepting a claim but before receiving the full balance of their compensation, their estate will receive the remainder of the compensation as a single lump sum payment which can then be distributed to beneficiaries of the estate as appropriate.
Time limits for application
Infected people and their estate representatives:
- For people diagnosed before 1 April 2025, the Scheme will be open to applications for compensation until 31 March 2031. This closing date will be reviewed by 31 March 2028 to ensure it remains appropriate based on the numbers of applications and expected processing times.
- For people diagnosed after 1 April 2025, the Scheme will be open to applications for six years from their date of diagnosis.
Affected people:
- An affected person can only apply for compensation once their infected loved one is confirmed as eligible for the Scheme.
- Where an infected person is diagnosed before 1 April 2025, the Scheme will be open to their affected loved ones until 31 March 2031.
- Where an infected person is diagnosed after 1 April 2025, the Scheme will be open to their affected loved ones for six years from the infected person’s date of diagnosis.
Estate representatives of affected people:
- Where an affected person dies between 21 May 2024 and 31 March 2031 before receiving their compensation, their estate representative can apply for compensation until the Scheme closes on 31 March 2031.
Effect of other payments on compensation awards
Infected Blood Support Schemes (IBSS) and Alliance House Organisations (AHO)
The Scheme is separate from the existing UK IBSS. Any support or discretionary payments a person received through the IBSS or AHO[footnote 6] before 1 April 2025, will not be deducted from compensation paid through the Scheme. Payments made on or after 1 April 2025 are deducted from a person’s compensation for future financial loss and care costs, with the exception of payments for pre-payment prescription certificates or grants for talking therapy which are not taken into account.
Interim compensation payments
If a person or estate has previously received interim compensation payments, these are automatically deducted from the compensation award paid through the Scheme.
Other compensation awards
If a person has previously received compensation for their infection outside of the Scheme (e.g. through court), the value of this compensation will be deducted from awards made through the Scheme. This does not include any awards made by an AHO.
Should a person choose to pursue litigation after receiving compensation through the Scheme, compensation amounts previously awarded through the Scheme are likely to be deducted from any awards made by the courts.
Impact on tax and benefits
Taxation
Compensation paid through the Scheme is exempt from income, capital gains and inheritance tax.
People who receive compensation on or after 4 December 2025 have a two-year window from the date they receive compensation in which they can gift some or all of their compensation to another person without paying inheritance tax.
Means tested benefits
Compensation awarded through the Scheme will not adversely impact means tested benefits that an infected or affected person receives.
Where a person receives compensation as an estate beneficiary, this will not impact any entitlement to means tested benefits.
Reviews and appeals
If a person is dissatisfied with the outcome of their application to the Scheme, they can request an internal review and have the right to an appeal within three months of receiving their original decision from IBCA. IBCA’s internal review process must be exhausted before the applicant can submit an appeal application. IBCA must take reasonable steps to ensure the review is carried out by a staff member who was not involved in the original decision. IBCA must explain the reason behind the internal review outcome. If a person is dissatisfied, they can appeal the decision through the First-tier Tribunal, administered by HM Courts and Tribunals Service.
Rights to litigation
The Scheme is designed to compensate victims of infected blood without the need to go through a court or tribunal process. However, accepting compensation through the Scheme does not remove a person’s right to pursue litigation.
Raising concerns about the Scheme
People can raise concerns about the design or delivery of the compensation scheme by emailing: feedbackandconcerns@ibca.org.uk. Concerns or issues raised will be considered by the Cabinet Office and IBCA. Both organisations publish quarterly summaries of feedback received on the compensation scheme design and delivery, and any action being taken as a result.
Annex A: Award tables
The below tables provide an overview of the compensation awards for people based on infection severity and the availability of effective treatments. As a reminder, infection severity bands are as follows - a full description of infection severity bands is at Annex C:
- Level 1: Hepatitis C (Acute)
- Level 2: Hepatitis B and/or C (Chronic)
- Level 2B: Hepatitis B and/or C (Chronic, treated with Interferon)
- Level 3: Hepatitis B and/or C (Cirrhosis)
- Level 4: Hepatitis B and/or C (Decompensated cirrhosis; liver cancer; liver transplantation)
- Level 5: Hepatitis B (Acute, fatal)
- HIV
- Co-infection with HIV
Core route awards for infected people and estates of deceased infected people
Table 1: Core awards for an infected person with a single infection (or their estate)
| Category of Award | Level 1 Hepatitis | Level 2 Hepatitis | Level 2B Hepatitis | Level 3 Hepatitis | Level 4 Hepatitis | Level 5 Hepatitis | HIV |
|---|---|---|---|---|---|---|---|
| Injury award | £10,000 | £60,000 | £70,000 | £120,000 | £180,000 | £180,000 | £180,000 |
| Social Impact award | £5,000 | £50,000 | £50,000 | £50,000 | £50,000 | £50,000 | £50,000 |
| Autonomy awardⱽ | £10,000 | £40,000 | £40,000 | £40,000 | £50,000 | £50,000 | £60,000 |
| Financial Loss award | £12,500 | Annual Financial Loss award* | Annual Financial Loss award* | Annual Financial Loss award* | Annual Financial Loss award* | £17,500 | £12,500, plus annual Financial Loss award: £14,829 per year before diagnosis; £29,657 per year from diagnosis |
| Care award | £500 | See Annex B | See Annex B | See Annex B | See Annex B | £41,188.49 | See Annex B |
*£12,500, plus annual Financial Loss award which varies based on infection severity and the infected person’s age when effective treatments became available - see Financial Loss award tables.
ⱽ Where a person was infected under 18, they will be eligible for a 50% uplift to the Autonomy award for the highest infection severity band reached during childhood.
Table 2: Core awards for an infected person with HIV & Hepatitis C/B co-infection (or their estate)
| Category of Award | HIV and Level 1 Hepatitis | HIV and Level 2 (or Level 2B) Hepatitis | HIV and Level 3 Hepatitis | HIV and Level 4 Hepatitis | HIV and Level 5 Hepatitis |
|---|---|---|---|---|---|
| Injury award | £182,500 | £195,000 | £240,000 | £270,000 | £270,000 |
| Social Impact award | £70,000 | £70,000 | £70,000 | £70,000 | £70,000 |
| Autonomy awardⱽ | £70,000 | £70,000 | £70,000 | £70,000 | £70,000 |
| Financial Loss award* | £18,536 per year before HIV diagnosis; £29,657 per year from diagnosis | £18,536 per year before HIV diagnosis; £29,657 per year from diagnosis | £22,243 per year before HIV diagnosis; £29,657 per year from diagnosis | £22,243 per year before HIV diagnosis; £29,657 per year from diagnosis | £14,829 per year before HIV diagnosis; £29,657 per year from diagnosis |
| Care award | See Annex B | See Annex B | See Annex B | See Annex B | See Annex B |
The awards a person is eligible for depends on the severity of their Hepatitis infection at the point of application to IBCA, rather than the severity of their infection at the time they were diagnosed with HIV.
*In addition to the per year Financial Loss awards given in Table 2, infected people with a coinfection of HIV and Level 1-4 Hepatitis receive a £12,500 award, while infected people with HIV and Level 5 Hepatitis coinfection receive a £17,500 award.
ⱽ Where a person was infected under 18, they will be eligible for a 50% uplift to the Autonomy award based on the highest infection severity band reached before they turned 18.
Table 3: Core awards for an infected person with chronic Hepatitis C & Hepatitis B co-infection (or their estate)
| Category of Award | Level 2 Hepatitis coinfection | Level 2B Hepatitis coinfection | Level 3 Hepatitis coinfection | Level 4 Hepatitis coinfection |
|---|---|---|---|---|
| Injury award | £75,000 | £85,000 | £150,000 | £225,000 |
| Social Impact award | £70,000 | £70,000 | £70,000 | £70,000 |
| Autonomy awardⱽ | £70,000 | £70,000 | £70,000 | £70,000 |
| Financial Loss award | * | * | * | * |
| Care award | See Annex B | See Annex B | See Annex B | See Annex B |
*£12,500, plus a Financial Loss award which varies based on infection severity and the infected person’s age when effective treatments became available - see Financial Loss award tables.
ⱽ Where a person was infected under 18, they will be eligible for a 50% uplift to the Autonomy award based on the highest infection severity band reached before they turned 18.
Core awards for affected people or eligible estates of affected people
Table 4: Core awards for affected people (or eligible estates of affected people) where the infected person had Level 3 Hepatitis, Level 4 Hepatitis, Level 5 Hepatitis, HIV or a Hepatitis C and B co-infection at Level 3 or above
| Category of Award | Partner | Child (under 18 when parent was infected) | Parent (of child infected under 18) | Siblings (under 18 when living with infected person) | Carers; Parent (of child infected age 18 or over); Child (aged 18 or over when parent was infected); All other eligible siblings |
|---|---|---|---|---|---|
| Injury award | £86,000* | £60,600ⱽ (£50,400ⱽ if parent had Level 2 or 2B Hepatitis infection while child was under 18) |
£65,400+ | £33,000ⱽ (£32,000ⱽ if infected sibling had Level 2 or 2B Hepatitis infection while affected sibling was under 18) |
£22,000 |
| Social Impact award | £12,000 | £12,000 | £12,000 | £12,000 | £8,000 |
| Autonomy award | £16,000 | £6,600 | £6,600 | N/A | N/A |
| Financial Loss award | See Financial Loss award tables | See Financial Loss award tables | N/A | N/A | N/A |
| Care award | N/A | N/A | N/A | N/A | N/A |
*For partners bereaved before 14 April 2026, and bereaved partners on IBSS, the core route Injury award is 50% higher.
- For parents of a child who passed away whilst under 18 and before 14 April 2026 the core route Injury award is 50% higher.
ⱽ This figure is inclusive of the 50% uplift given to children and siblings affected whilst under the age of 18.
Table 5: Core awards for affected people (or eligible estates of affected people) where the infected person had Level 2 (or Level 2B) Hepatitis infection
| Category of Award | Partner | Child (under 18 when parent was infected) | Parent (of child infected under 18) | Siblings (under 18 when living with infected person) | Carers; Parent (of child infected age 18 or over);Child (aged 18 or over when parent was infected); All other eligible siblings |
|---|---|---|---|---|---|
| Injury award | £34,000* | £30,000ⱽ | £20,000 | £30,000ⱽ | £20,000 |
| Social Impact award | £12,000 | £12,000 | £12,000 | £12,000 | £8,000 |
| Autonomy award | £16,000 | £6,600 | £6,600 | N/A | N/A |
| Financial Loss award | See Financial Loss award tables | See Financial Loss award tables | N/A | N/A | N/A |
| Care award | N/A | N/A | N/A | N/A | N/A |
*For bereaved partners on IBSS, the core route Injury award is 50% higher.
ⱽ This figure is inclusive of the 50% uplift given to children and siblings affected whilst under the age of 18.
Affected people whose loved one had a Level 1 Hepatitis infection are not eligible for compensation through the Scheme.
Financial Loss award tables
Core Financial Loss awards for infected people
The tables below set out the Financial Loss awards for infected people. Where the infected person has died, the relevant Financial Loss awards below will be paid to the estate representative for the years between the infected person’s infection and their death, inclusive of both years.
Table 6: Core Financial Loss award based on disease progression and availability of effective treatment (Hepatitis B)
| Milestones for the introduction of major treatments | Level 2 or Level 2B | Level 3 | Level 4 |
|---|---|---|---|
| For people born after 1953: Pre effective treatment (2008 and earlier) | £11,863 per year+ | £23,726 per year | £29,657 per year |
| For people born after 1953: Effective management from 2009 | £5,931 per year+ | £17,794 per year | £29,657 per year |
| For those born in or before 1953 | £11,863 per year+ | £23,726 per year | £29,657 per year |
+For people on Level 2B, the yearly Financial Loss rate will be uplifted to £23,726 for two years for each separate round of Interferon treatment where treatment was two years apart.
Table 7: Core Financial Loss award based on disease progression and availability of effective treatment (Hepatitis C or Hepatitis co-infection)
| Milestones for the introduction of major treatments | Level 2 or Level 2B | Level 3 | Level 4 |
|---|---|---|---|
| For people born after 1961: Pre-effective treatment (2016 and earlier) | £11,863 per year+ | £23,726 per year | £29,657 per year |
| For people born after 1961: Effective management from 2017 | £5,931 per year+ | £17,794 per year | £29,657 per year |
| For people born in or before 1961 | £11,863 per year+ | £23,726 per year | £29,657 per year |
+For people on Level 2B, the yearly Financial Loss rate will be uplifted to £23,726 for two years for each separate round of Interferon treatment where treatment was two years apart.
Core and supplementary route Financial Loss awards for bereaved affected people
Table 8: Core and supplementary Financial Loss awards available to bereaved affected people
| Affected cohort | Route | Financial Loss award per year following the death of the infected person |
|---|---|---|
| Bereaved partner | Core route | £16,682 per year from the year after the infected person’s death until the year the infected person would have turned 65, then £8,341 from the year the infected person would have turned 66 to their healthy life expectancy. |
| Bereaved child under 18 when parent(s) dies | Core route | £5,561 per year for years the child would have been under 18 while the infected person would have been under 66. £2,780.50 per year for any years where the infected person would have been 66 or older while the child was under 18. If the child lost both parents to infected blood while under 18: £22,243 per year for years the child was under 18 where both infected parents would have been under 66. This amount reduces to £16,682.25 if one infected parent would have been 66 or older while the child was under 18; or, £11,121.50 if both parents would have been 66 or older while the child was under 18. |
| Bereaved dependent parent | Supplementary route | £5,561 per year from the year after the infected person’s death until the year the infected person would have turned 65. £2,780.50 per year from the year the infected person would have turned 66 to their healthy life expectancy. |
| Bereaved dependent sibling | Supplementary route | £5,561 per year from the year after the infected person’s death until the year the infected person would have turned 65. £2,780.50 per year from the year the infected person would have turned 66 to their healthy life expectancy. |
| Bereaved child with a disability causing financial dependence on parent(s) in adulthood | Supplementary route | £5,561 per year from the year after the infected person’s death until the year the infected person would have turned 65. £2,780.50 per year from the year the infected person would have turned 66 to their healthy life expectancy. If the child lost both parents to infected blood while under 18, higher awards are available: £22,243 per year from the year after the infected person’s death to the infected person’s estimated healthy life expectancy; £16,682.25 for years where one parent would have been 66 or older; £11,121.50 for years where both parents would have been 66 or older. Any core route Financial Loss awards will be deducted from the above totals. |
Annex B: Care bands and assumed care requirements based on infection severity
Care band descriptors and costs
Table 1: This table shows the compensation amounts for different care bands. These are used, together with the assumed care requirements in Table 2, to calculate a person’s Care award.
| Care band | Description | Care award compensation per year |
|---|---|---|
| General support around the home (Level 1 Care) | 6 hours per week Support with heavier domestic tasks, attending medical appointments and household maintenance |
£5,460 |
| Low Care (Level 2 Care) | 16.5 hours per week (equates to 6 hours per week general support + 1.5 hours per day personal care) General support around the home, alongside part-time help with personal care (e.g. washing and dressing) |
£23,424.72 |
| Moderate Care (Level 3 Care) | 34 hours per week (equates to 6 hours per week general support + 4 hours per day agency home care) General support around the home, with more frequent or daily help (e.g. increased personal care and help with meals) |
£51,285.92 |
| High Care (Level 4 Care) | 41 hours per week (equates to 6 hours per week general support + 5 hours per day agency home care) General support around the home, alongside significant help daily with personal care and meals |
£62,742.40 |
| End-of-Life Care (Level 5 Care) | 24-hour support | £109,835.96 |
Assumed care requirements based on infection severity
Table 2: This table shows the assumed level and duration of care (in years) required for different infection severities. These are used, together with the care bands in Table 1, to calculate a person’s Care award.
| Infection severity band | End of life (Level 5 care band) | High care (Level 4 care band) | Moderate care (Level 3 care band) | Low care (Level 2 care band) | General support around the home (Level 1 care band) |
|---|---|---|---|---|---|
| HIV | 0.5 | 1.5 | 7 | 5 | 10 |
| HIV and Level 1 Hepatitis | 0.5 | 1.5 | 7 | 5 | 10 |
| HIV and Level 2 Hepatitis | 0.5 | 1.5 | 7 | 5 | 10 |
| HIV and Level 3 Hepatitis | 0.5 | 1.5 | 7 | 5 | 10 |
| HIV and Level 4 Hepatitis | 0.5 | 1.5 | 7 | 5 | 10 |
| Level 1 Hepatitis | N/A | N/A | N/A | N/A | N/A |
| Level 2 Hepatitis | N/A | N/A | N/A | N/A | 10 |
| Level 2B Hepatitis | N/A | N/A | N/A | 1* | 10 |
| Level 3 Hepatitis | N/A | N/A | N/A | 6 | 10 |
| Level 4 Hepatitis | 0.5 | 1.5 | 2 | 6 | 10 |
| Level 5 Hepatitis | 0.5 | N/A | N/A | N/A | N/A |
*The table shows the care requirements for a person with a Level 2B Hepatitis infection who received one round of treatment with Interferon. For every additional round of treatment with Interferon, an additional year of Level 2 Low Care is added.
Annex C: Infection severity band descriptions
This table provides a detailed description of the clinical markers of infection severity for each infection severity band.
| Infection severity | Infection type | Description of infection |
|---|---|---|
| Level 1 Hepatitis | Hepatitis C (Acute) | Transient, self-cleared infection usually within 6-12 months of exposure. |
| Level 2 Hepatitis | Hepatitis C and / or Hepatitis B (Chronic) | Chronic infection characterised by: (a) Hepatitis B - infection with confirmed Hepatitis B surface antigen (HBsAg) positivity for longer than 6 months with detectable Hepatitis B virus DNA on a polymerase chain reaction test, if not on antiviral therapy. (b) Hepatitis C - infection with replicating Hepatitis C virus RNA. |
| Level 2B Hepatitis | Hepatitis C and / or Hepatitis B (Chronic, treated with Interferon) | As per Level 2 Hepatitis, where a person has had their infection treated with Interferon. Anyone treated with Interferon, regardless of how long that treatment was endured, is considered eligible for Level 2B compensation awards. Additional compensation is available for people who have had multiple rounds of treatment with Interferon. |
| Level 3 Hepatitis | Hepatitis C and / or Hepatitis B (Cirrhosis) | Characterised by serious scarring (serious fibrosis) of the liver caused by long-term liver damage caused by infection; Treatment of B-cell non-Hodgkin’s lymphoma caused by infection - single round treatment (first line therapy); Type 2 or 3 cryoglobulinemia caused by infection accompanied by membranoproliferative glomerulonephritis (MPGN). |
| Level 4 Hepatitis | Hepatitis C and / or Hepatitis B (Decompensated cirrhosis; liver cancer; liver transplantation) | Decompensated cirrhosis caused by infection is characterised by the presence of: hepatic encephalopathy (confusion due to liver damage); ascites (accumulation of fluid in the abdomen); variceal haemorrhage (bleeding from dilated veins in the gullet or stomach); or, a Child-Pugh score greater than 7.Treatment of B-cell non-Hodgkin’s lymphoma caused by infection - multiple round treatment (second line therapy). |
| Level 5 Hepatitis | Hepatitis B (Acute, fatal) | Infection resulting in death from acute liver failure within 12 months of infection or within 12 months of a reactivation of the infection. |
| HIV | N/A | HIV infection only. |
| Co-infection including HIV | N/A | HIV co-infection with Hepatitis B or Hepatitis C. |
Annex D: Severe Health Condition descriptions
This table sets out in detail the health conditions that may make someone eligible for a Severe Health Condition award.
| Severe Health Condition | Description |
|---|---|
| Group 1. Severe visual impairment. Related to HIV | Applicants would need to be registered as severely sight impaired (blind) and have evidence of one of the following opportunistic infections secondary to advanced HIV disease: A. Cytomegalovirus retinitis B. Varicella zoster virus necrotising retinitis C. Herpes simplex virus necrotising retinitis D. Toxoplasmosis chorioretinitis E. Optic neuropathy secondary to cryptococcal meningitis F. Cortical blindness secondary to Progressive Multifocal Leucoencephalopathy (PML) |
| Group 2 Neurological disorders resulting in long-term severe physical/ mobility disability Related to HIV and/or Level 2, Level 3 or Level 4 Hepatitis infections |
All applicants would need to provide evidence of a social services needs assessment confirming requirement for long-term personal and domestic care as defined by scheme in the low care band (Level 2) for a physical or mobility disability. AND Applicants with an HIV infection would need to provide evidence of: A. One of the following central nervous system (CNS) opportunistic infections and neoplasia secondary to advanced HIV disease: 1. Cerebral toxoplasmosis 2. CNS Tuberculosis 3. Cytomegalovirus encephalitis 4. Varicella zoster virus encephalitis 5. Herpes simplex virus encephalitis 6. Epstein Barr virus encephalitis 7. Progressive multifocal leucoencephalopathy 8. Cryptococcal meningitis 9. Primary CNS lymphoma 10. Thromboembolic disease secondary to bacterial / fungal endocarditis B. One of the following CNS conditions secondary to or associated with HIV infection: 1. HIV vacuolar myelopathy 2. Transverse myelitis 3. Thrombotic thrombocytopaenic purpura 4. Cerebrovascular ischaemic/ Haemorrhagic stroke 5. Coagulopathies: Antiphospholipid syndrome C. One of the following peripheral nervous system and myopathic conditions secondary to or associated with HIV infection: 1. Chronic inflammatory demyelinating polyneuropathy 2. Cytomegalovirus polyradiculopathy 3. HIV myopathy Applicants with a Hepatitis C infection would need to provide evidence of: A. Cryoglobulinaemic vasculitis induced neurological disease that results in severe mobility disability B. Peripheral neuropathy caused by mixed cryoglobulinaemic vasculitis that results in severe mobility disability Applicants with a Hepatitis B infection would need to provide evidence of: A. Peripheral neuropathy caused by mixed cryoglobulinaemic vasculitis that results in severe mobility disability B. Peripheral neuropathy occurring in the context of Hepatitis B associated polyarteritis nodosa (PAN) |
| Group 3 Neurological disorders resulting in long-term severe neurocognitive impairment and/or behavioural disorders Related to HIV and/or Level 4 Hepatitis B or C |
All applicants would need to provide evidence of a social services needs assessment confirming requirement for long term personal and domestic care as defined by scheme in the low care band (Level 2) for a neurocognitive impairment. AND Applicants with an HIV infection would need to provide evidence of one the following conditions for which HIV infection is considered the main underlying cause or is a major contributing factor: A. HIV brain and/or cerebrovascular disease resulting in neurocognitive impairment (dementia) and/or behavioural disorders B. Legacy opportunistic CNS infections secondary to advanced HIV disease, (for example Post infectious encephalitis or Progressive Multifocal Leucoencephalopathy (PML), resulting in neurocognitive impairment (dementia) and or behavioural disorders Applicants with a Hepatitis B or Hepatitis C infection would need to provide evidence of the following conditions: A. Chronic hepatic encephalopathy in association with a decompensated cirrhosis diagnosis of duration in excess of 4 years (the first four years being covered in the core award) |
| Group 4 Psychiatric disorders resulting in long term mental health disability Related to HIV and Level 2, Level 3 and/or Level 4 Hepatitis infections |
Applicants with a Hepatitis B and/or Hepatitis C and/or HIV infection would need to provide evidence of a diagnosis by a psychiatrist of one of the following conditions: A. Mood disorders: i. Depressive disorders ii. Bipolar disorders when brought forward by the blood infection or Interferon treatment B. Anxiety and stress related disorders: i. Generalised anxiety and panic disorders ii. Post traumatic stress disorders iii. Adjustment disorders C. Psychotic disorders: i. Secondary psychotic disorders due to HIV brain disease, HIV related CNS opportunistic infection or neoplasia, or Interferon treatment Supporting evidence For an uplift award to reflect provision of domestic care, all of the following must be provided as supporting evidence: A. Report from a consultant psychiatrist confirming (i) the diagnosis; (ii) the major role of blood borne infection or Interferon treatment in the aetiology and / or course of the mental health disorder AND B. One of the following: i. Report from a consultant psychiatrist confirming the patient received consultant-led secondary mental health treatment for six months or more ii. Evidence of inpatient admissions for treatment of mental health disorder iii. Evidence of history of sectioning under the Mental Health Act For an applicant to receive an uplift award to reflect provision of low care the applicant must satisfy criteria A, B; and C. Social services needs assessment confirming requirement for long-term personal and domestic care as defined by scheme in the low care band (Level 2) |
| Group 5 End-stage kidney disease requiring renal replacement therapy (RRT) Related to HIV and Level 2, Level 3 and/or Level 4 Hepatitis infections |
Applicants with an HIV infection would need to provide evidence of an end-stage kidney disease listed below which has required renal replacement therapy (RRT) for minimum of 3 months: A. HIV associated nephropathy B. HIV associated immune complex chronic kidney disease C. Drug associated kidney disease in conjunction with treatment with foscarnet sodium or cidofovir or tenofovir disoproxil Applicants with a Hepatitis B infection would need to provide evidence of condition below in addition to renal replacement therapy (RRT) for a minimum of 3 months: A. Membranous Nephropathy B. Membranoproliferative glomerulonephritis including in the presence of mixed cryoglobulinaemic vasculitis C. IgA nephropathy D. Tenofovir disoproxil induced renal failure Applicants with a Hepatitis C infection would need to provide evidence of condition below in addition to renal replacement therapy (RRT) for a minimum of 3 months: A. Membranoproliferative glomerulonephritis including in the presence of mixed cryoglobulinaemic vasculitis |
| Group 6 Other Hepatitis-associated disorders resulting in long-term severe disability Related to Level 2, Level 3 and/or Level 4 Hepatitis infections |
Applicants with a Hepatitis C infection would need to provide evidence of one of the following autoimmune diseases caused by or exacerbated by Interferon treatment for Hepatitis C: A. Coombs positive haemolytic anaemia B. Idiopathic fibrosing alveolitis of the lung C. Rheumatoid arthritis Applicants with a Hepatitis C infection would need to provide evidence of one of the following: A. Sporadic porphyria cutanea tarda causing photosensitivity with blistering B. Immune thrombocytopenic purpura C. Type 2 or 3 mixed cryoglobulinaemia accompanied by: cerebral vasculitis; dermal vasculitis; or, peripheral neuropathy with neuropathic pain Applicants with a Hepatitis B infection would need to provide evidence of one of the following autoimmune diseases: A. Coombs positive haemolytic anaemia – caused by or exacerbated by Interferon treatment for Hepatitis B B. Idiopathic fibrosing alveolitis of the lung – caused by or exacerbated by Interferon treatment for Hepatitis B C. Rheumatoid arthritis – either related to the virus directly or caused by or exacerbated by Interferon treatment for Hepatitis B D. Aplastic anaemia where treatment results in long term severe disability |
| Group 7 Special Category Mechanism (SCM) Related to Level 2, Level 3 and/or Level 4 Hepatitis infections |
Applicants already assessed as SCM under the Support Schemes will be automatically eligible. New applicants would need to provide evidence of eligibility, consistent with the EIBSS criteria for SCM. IBCA will determine how best to assess applicants against these criteria. |
-
The Macfarlane Trusts, the Eileen Trust, the Skipton Fund, the Caxton Foundation and MFET Ltd ↩
-
If a person was 55 years or older when effective treatment was introduced, this is not taken into account given they are less likely to have returned to work even if their health improved. Effective treatment dates are: Hepatitis B in 2008; Hepatitis C in 2016; Hepatitis B and C co-infection in 2016. ↩
-
Median salary according to Annual Survey of Household Earnings (all occupations) published by the Office of National Statistics in 2023. The median salary is then deducted for Tax and National Insurance contributions. ↩
-
Healthy life expectancy is determined using the Ogden Tables 8th Edition (PDF, 4.5MB). ↩
-
£38,504 reflects a salary that is 10% above the median gross salary in April 2023, based on data from the Office for National Statistics. ↩
-
The Macfarlane Trust, the Eileen Trust, the Skipton Fund, the Caxton Foundation and MFET Ltd ↩