HPR volume 14 issue 13: news (14 and 21 July)
Updated 23 December 2020

© Crown copyright 2020
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/health-protection-report-volume-14-2020/hpr-volume-14-issue-13-news-14-and-21-july
COVID-19 surveillance and guidance update
Enforcement powers became available to local authorities this month underpinning the Department of Health and Social Care’s (DHSC’s) new guidance for local decision makers on containing and managing local COVID-19 outbreaks. The guidance, known as the Contain Framework, outlines a range of measures that local authorities, the NHS, Public Health England (PHE) and others can take in response to localised coronavirus outbreaks.
Local authorities’ new enforcement powers (under the Health Protection (Coronavirus, Restrictions) (England) Regulations 2020) are summarised in Appendix 2 of the Contain Framework. The Department of Health and Social Care (DHSC) press release has more information.
The shift of focus to more localised COVID-19 infection prevention and control activity was reflected in the latest PHE National Weekly Surveillance Report (NWSR) that now includes a section covering local data and local control interventions.
National Weekly Surveillance Report (NWSR)
Summarising the national epidemiological picture, the latest NWSR (including data to 12 July) states:
“COVID-19 activity continued to decline or remain stable in England across the majority of surveillance indicators during week 28. Case detections are highest in the East and West Midlands and Yorkshire and Humber. There has been a small increase in detections in the West Midlands through both ‘Pillar 1’ and ‘Pillar 2’ testing [see below]. At a local authority level, activity remains highest in Leicester, though the weekly incidence of confirmed cases continues to decrease. There have been increases in Blackburn and Darwen, Bradford, Luton and Peterborough. Case detections are highest in adults aged 85 and over. There has been an increase in the proportion of cases from the Asian and Asian British ethnic group, this is likely to reflect larger populations from this ethnic group in areas that are currently seeing higher incidence.”
In the new section, Contain Framework Local Authority Watchlist, the NWSR now provides more detail of geographical areas of most concern, taking account of a range of factors including high weekly infection incidence rates, the incidence trend, test positivity, local response and plans, and the trend of other metrics such as healthcare activity and mortality. In week 28, a dozen local authorities were listed with status ranging from ‘of concern’ to ‘for national intervention’. Ten lower-tier local authorities are listed as ‘of concern’ on the basis of incidence rates only.
As far as institutional outbreaks were concerned, in week 28, the overall number of acute respiratory infection incidents in England remained similar to the previous week, with small declines in the number of incidents in educational, workplace and other institutional settings. It was noted that, since Pillar 2 testing became open to everyone during week 21, more outbreaks of mild disease have been detected in settings with healthy younger populations.
The NWSR is published on Thursdays, presenting data as at 9:30am on the previous Wednesday of each publication week. It distinguishes between data from Pillar 1 testing (swab testing in PHE labs and NHS hospitals for those with a clinical need, and the most critical health and care workers) and Pillar 2 testing (mass-swab testing for critical key workers in the NHS, social care and other sectors).
The infographic that accompanies the NWSR provides more detailed trend information, across a wider range of parameters than the Coronavirus Cases in the UK: Daily Updated Statistics webpage.
The epidemic curve for England, including week 28 data (up to 15 July):
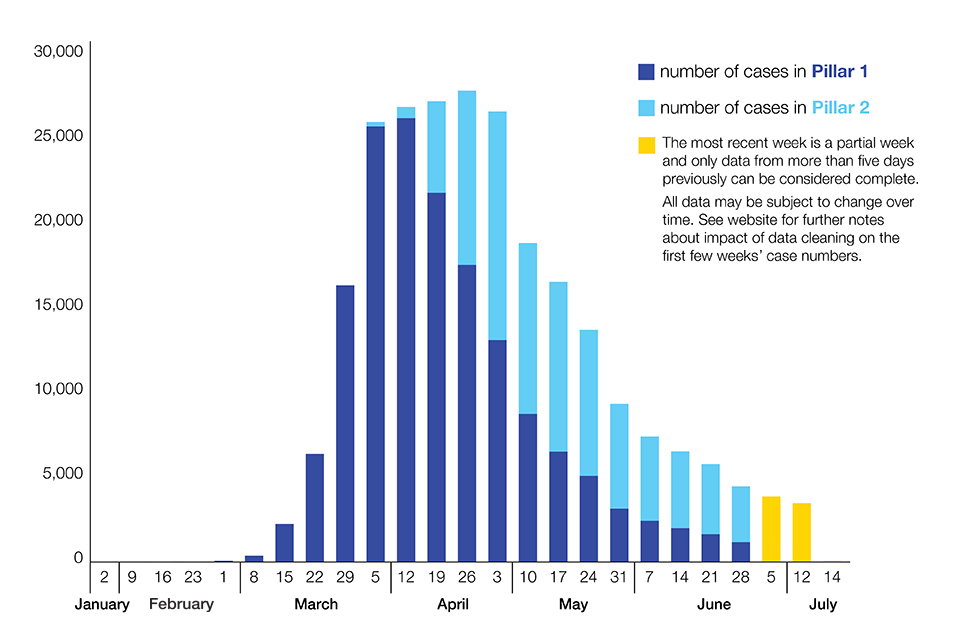
Laboratory-confirmed COVID-19 cases (England) as at 15 July 2020 (by date of specimen collection).
Coronavirus Infection Survey
The Office for National Statistics-led (ONS) Coronavirus Infection Survey (CIS) is a ‘household survey’ that collates results from testing nose and throat swabs, and blood samples, taken from a cross-sectional sample of the population in England who live or work outside of institutional settings and would not otherwise be candidates for testing.
It aims to determine the proportion of the population infected, with or without symptoms, at a particular point in time, the number of new infections occurring over a given time period and the proportion of the population that have developed antibodies.
The latest pilot data report, released on 17 July, indicates that, at both national and regional level, the decreasing number of people testing positive in England, that had been seen in earlier reporting periods, had levelled off (although changed methodology means that the latest data cannot be directly compared with those in previous CIS reports).
ONS provisionally estimates that for the week 6 July to 12 July, 24,000 people on England had COVID-19 (95% confidence interval: 15,000 to 34,000), equivalent to 0.04% of the population in England or about 1 in 2,300 individuals.
On disease incidence (using ONS’ new ‘exploratory modelling’ approach), the CIS report indicates that during the week 6 July to 12 July around 1,700 people became newly infected with COVID-19 per day (95% confidence interval: 700 to 4,200); indicating that the decreasing rate of new infections recorded since mid-May had levelled off.
On antibody status, the latest report notes that, as of 29 June, 6.3% (95% confidence interval: 5.0% to 7.8%) of adults from whom blood samples were taken tested positive for COVID-19 antibodies, equivalent to 1 in 16 people, or 2.8 million people, in England.
COVID-19 guidance update
On 17 July, updated guidance was published jointly by PHE and the Ministry of Justice, on Preventing and controlling outbreaks of COVID-19 in prisons and places of detention. This is intended to assist staff in the prisons estate, local PHE Health Protection Teams and other stakeholders in responding to COVID-19 incidents in prisons and places of detention (PPDs), including when staff or prisoners display symptoms, when there are requirements for cohorting affected groups and limiting spread. The guidance is advisory and does not supersede relevant primary legislation.
Joint DHSC and PHE guidance, updated on 14 July, for commissioners and providers of services for people who use drugs or alcohol, takes account of NHS test and trace service arrangements and stresses the importance of continued operations of needle and syringe programmes and opioid substitution treatments. The guidance is advisory and does not supersede relevant primary legislation.
The Health and Safety Executive has published Air conditioning and ventilation during the coronavirus outbreak which provides general ventilation advice and specific recommendations.
This states that the risk of air conditioning spreading COVID-19 in the workplace is extremely low as long as there is an adequate supply of fresh air and ventilation. In the case of a centralised ventilation systems, where air is removed and circulated to different rooms, it is recommended that recirculation is turned off and fresh air supply maximised. Systems that mix extracted air with fresh air before recirculation are satisfactory; as are those operating within individual rooms, such as portable units.
Country-specific travel guidance
General advice on Safer air travel for passengers is regularly updated by the Department for Transport.
Comprehensive, country-specific travel advice, taking account of changing quarantine rules, is provided by the PHE-sponsored TravelHealthPro website, consolidating advice from the National Travel Health Network and Centre (NaTHNaC), the Foreign and Commonwealth Office and PHE.
TravelHealthPro website includes a general risk assessment guide and a comprehensive set of Country information pages where each country is now classified as high, moderate or low risk of exposure to COVID-19 based on currently available information assessed by PHE and NaTHNaC.
Travellers are advised against all non-essential travel to countries or areas classified as high risk. Those at increased risk of severe COVID-19 are advised to discuss travel plans with a health professional, even for travel to moderate risk areas.
Check the current Foreign and Commonwealth Office (FCO) travel advice before travel.
The Cabinet Office guidance Coronavirus outbreak FAQs: what you can and can’t do was updated on 17 July.
Antimicrobial resistance: third WHO GLASS report published
The third World Health Organization report on the Global Antimicrobial Resistance and Use Surveillance System (GLASS) was published on 26 May 2020.
The report describes the development of GLASS and the status of antimicrobial resistance (AMR) surveillance activities globally and summarises 2018 AMR data from participating countries. Despite limitations in interpretation of the data, high levels of resistance to commonly used antibiotics are observed.
Global AMR surveillance systems for other pathogens – HIV, tuberculosis and malaria – as well as environmental surveillance of AMR, are also described.
UK AMR data from 2018 is included from blood, urine, and genital specimens, that is Streptococcus pneumoniae, Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae and Acinetobacter spp. isolated from blood cultures; E. coli and K. pneumoniae from urine specimens; and Neisseria gonorrhoeae from urethral and cervical swab specimens.
The English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) report 2019 to 2020 will be published in autumn 2020 and will include AMR data for England covering the period from 2015 to 2019.
Infection reports in this issue of HPR
Pneumococcal Polysaccharide Vaccine (PPV) coverage report, England, April 2019 to March 2020.