Disability Assessor Recruitment and Retention
Published 29 January 2026

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/disability-assessor-recruitment-and-retention/disability-assessor-recruitment-and-retention
January 2026
DWP research report no. 1056
A report of research carried out by The Social Agency (formerly Basis Social), in partnership with London Economics on behalf of the Department for Work and Pensions.
Crown copyright 2026.
You may re-use this information (not including logos) free of charge in any format or medium, under the terms of the Open Government Licence. To view this licence, visit National Archives
or write to:
Information Policy Team
The National Archives
Kew
London
TW9 4DU
or email: psi@nationalarchives.gov.uk
This document/publication is also available on our website at:
If you would like to know more about DWP research, email: socialresearch@dwp.gov.uk
First published January 2026.
ISBN 978-1-78659-908-7
Views expressed in this report are not necessarily those of the Department for Work and Pensions, any other government department, or any health assessment providers.
Executive summary
This research was conducted in February to April 2022. Statistics and views reported were accurate in relation to the health assessment providers at that point in time.
Background
DWP commissioned The Social Agency (formerly Basis Social), working in partnership with London Economics, to undertake research into barriers to the recruitment and retention of health and disability benefit assessors (HDAs). The Department makes around 1.9 million assessments for disability benefits each year, working alongside three providers for delivering Work Capability Assessments (WCA) and Personal Independence Payment (PIP) assessments (IAS, CHDA and Capita). Ensuring the supply of health and disability assessments adequately matches demand has always been a challenge for DWP, in part due to inadequate levels of HDA recruitment and retention.
The research design consisted of three methodological strands, to triangulate insights and provide a robust rationale for any potential changes that address recruitment and retention:
-
Economic analysis of supply and demand issues around employment of health care professionals and the implications for assessor employment. This was led by London Economics who produced Annex A.
-
An evidence review into best practice around delivering services in ways that support retention and wellbeing across similar public services.
-
Qualitative research with DWP agents, assessors, provider executives, and recruiters involved in the recruitment of health and disability assessors to contracted providers. A total of 35 interviews were undertaken between February and April 2022.
Health and disability assessor recruitment
(Section 2 of the report)
Over the course of 2021, there was a modest growth of the HDA workforce through recruitment efforts, largely driven by one organisation (IAS) while it declined for CHDA. A key factor influencing the pressures on recruitment is that workforce retention is a very serious issue for all assessment providers (APs). An average of 4.3% of assessors left the occupation each month throughout 2021; in annual terms, this is equivalent to an attrition rate of 52%. Approximately, 40% of new recruits also leave during the training period. Due to these levels of attrition, very high recruitment levels are required to maintain the workforce required to meet assessment targets (for instance, between 2,000 and 3,000 FTE assessors per year, which is approximately 60% to 90% the size of the HDA workforce at the time of writing).
One issue around the identified recruitment and retention issues could be that the skills required and work activities performed by HDAs differ from those of healthcare professionals (HCPs) more generally, meaning HCPs might both not be attracted to HDA roles and may struggle to adapt to the HDA remit. The HDA role can be considered a combination of two discrete occupations: healthcare professional and benefits assessor. In both roles there is often a need for strong interpersonal and communication skills, critical thinking skills, resilience and rigour. The HDA role has aspects of a HCPs role in using medical knowledge to understand health conditions, however this is to aid judgements of functioning and not to diagnose or deliver therapeutic care. The HDA role also incorporates some aspects of a benefits assessor role in respect of the need to assess against functional criteria and to write reports. Good clerical and administrative skills were seen as critical to completing daily assessment targets; detailed report writing is not a key feature of HCPs work. One additional key difference is that the range of tasks and activities undertaken by a HDA to fulfil their role is much more limited than is the case for HCPs.
In discussions with assessors, APs and recruiters it was clear that not all professions were equivalent in the extent to which they prepared people for performing a role as an HDA. Given the variety of presenting disabilities (and impacts on functioning) there was a general view that more generalist HCPs are better suited to the role, given their familiarity with a wider set of conditions. These included GPs, nurses and paramedics.
Within the five HCP professions at the time of writing eligible to become assessors, there were 1.18 million registered HCPs in 2021. In the last 6 to 8 months, DWP contract managers and executives from Capita and IAS reported that recruitment has significantly improved, such that there are full training HDA cohorts. Several factors were seen to have driven this improvement in the supply of HDAs:
-
people leaving the NHS due to the increased stress of working through the COVID-19 pandemic
-
the flexibility for HDAs (in Capita and IAS) to work from home to conduct assessments because of COVID-19
-
reducing the clinical experience requirement to 12 months, attracting newly qualified HCPs
-
IAS aligning salaries with other providers
-
introducing testimonials as part of the recruitment materials used to attract new HDAs
While there has been some recent strengthening of the recruitment pipeline for HDAs the wider trends – low unemployment, record job vacancies for HCPs and comparably lower salaries - suggest the labour market will be very challenging for recruitment. To attract potential recruits to become HDAs, the economic analysis suggests that the APs should be offering wages to HDAs of at least £38,000 per year outside London. However, offering a higher starting salary than that (closer to £45,000) would be required to financially attract approximately 30% more of the full-time nursing, physiotherapist and occupational therapist workforce. Those interviewed as part of this research were clear that it was the overall package which was important, and salary was only one part of that. Additionally important motivators were the opportunity to have a fixed working pattern, the flexibility to work from home, to continue to use their medical experience as part of their role and to have access to professional development opportunities which kept their medical expertise up-to-date.
Aside from the competitive recruitment landscape there are various other challenges for recruitment, including:
-
recruitment criteria are narrowly defined, requiring medical qualifications and specific clinical experience, effectively forming a HDA ‘micro-market’
-
candidates do not get a clear enough picture of the HDA role during the recruitment process, with a mismatch of expectations and motivations and the realities of the role
-
the lack of part-time training and flexibility in working arrangements
-
HCPs were attracted to their therapeutic roles because of a desire to help people who were ill or hurt; the HDA role does not deliver this and the wider perception (the ‘negative press’) is that it is a role which does not help people
-
the disability assessment sector offers limited opportunities for career progression
-
the recruitment process is time consuming
Based on the evidence gathered through this research, opportunities to consider for improving HDA recruitment (outside of simply increasing financial incentives) can be seen to include:
-
increased transparency about what the HDA role involves, to ensure expectations are more aligned with experiences
-
re-structuring the training process and supporting greater flexibility in HDA roles to accommodate different working preferences
-
offering a clear career path, or at the least opportunities to take on responsibilities beyond assessments to provide variety and progression
-
tackling the negative perceptions around the HDA role (for example, through client and HDA testimonials) to help reposition the role
-
considering broadening the scope for qualifying roles to other HCPs (for example, prescribing pharmacists
Health and disability assessor retention
(Section 3 of the report)
The training and onboarding process for HDAs encompasses four stages, after which HDAs are then on a probationary period before being confirmed fully in post. This process differs in length depending on a range of factors including the qualifications which HCPs enter the process with, whether parts of the process are undertaken part-time or full-time, and how quickly people progress through each stage. In theory it could take as little as 2 to 3 months to be approved but in many cases it is taking 6 months, and some report instances of 12 to 18 months.
For those HDAs who make it through this training and go on to work as a HDA the role can deliver against many of the expected benefits detailed in Section 3, though there is recognition it is not for everyone and that you have to be both resilient, self-directed and comfortable with the level of scrutiny that comes with the role. There is a view that contract providers deliver sufficient support for HDAs and that there are progression opportunities for those that seek additional responsibilities and demonstrate an aptitude for the role.
However, there is an acknowledgement that a high proportion of HCPs do not make it through the training process or, where they do, do not stay in post very long. The qualitative research suggests that there is an expectation that most HDAs will leave their role within just 2 to 3 years. There are various challenges found to be impacting retention:
-
the mismatch of people’s incoming expectations and their experience of the role. In particular that it is not a ‘wind-down’ or ‘easy’ option or that it will involve some use of their therapeutic or care-giving skills
-
the assessment process is very different to what HDAs are used to as a HCP, with the focus on justifications quite alien compared to providing a diagnosis, and high degree of emotional burden through having to listen but with limited opportunity to act (and deliver care)
-
the training and onboarding processes are relatively lengthy and the auditing elements (especially during the latter stages) can be highly pressurised and stressful
-
the role itself is relatively repetitious and offers limited variety to keep people engaged and motivated; similarly there is a lack of clear career progression opportunities, particularly compared to the healthcare sector
-
HCPs have skills which are still very much in demand so tend to have a wide range of opportunities to leave their HDA role to satisfy their work-related needs
While not the focus of this research, we did identify a range of actions that were being taken by both DWP and APs to address retention and there was a healthy, honest and supportive relationship reported between DWP and APs in discussing these issues. These range from changes to the assessment processes themselves (for example, reducing the expected number and length of PIP assessments) and piloting of WCA assessments to be undertaken remotely through to support measures by APs largely focusing on trying to establish more of a culture of learning and coaching during the training and onboarding process.
Based on the evidence gathered through this research, opportunities to consider for improving HDA recruitment (outside of simply increasing financial incentives) can be seen to include:
-
ensuring that recruitment processes are fit for purpose, including clarity on the HDA role and testing for competencies required
-
tailoring support so that trainee HDAs at the latter stages of the training process feel adequately supported and minimising the degree to which trainee HDAs feel they are being ‘audited’
-
looking at opportunities to offer HDAs alternative roles and remits (including mentoring, case file analysis, training delivery, management roles) to stem the departure of HDAs after 2 to 3 years
-
supporting work/life balance desires by ensuring that remote working is or remains possible across both WCA and PIP in future
Acknowledgements, Authors and Contacts
Acknowledgements
The Department for Work and Pensions (DWP) commissioned The Social Agency (formerly known as Basis Social) in partnership with London Economics to undertake this research. We would like to thank the authors of the report: Dan Clay, Leyla Hart-Svensson, James Cannings and Dr Gavin Conlon.
Authors
Dan Clay Managing Partner, The Social Agency
Leyla Hart-Svensson The Social Agency
James Cannings Economic Consultant, London Economics
Dr Gavan Conlon Partner, London Economics
Department for Work and Pensions
Contacts
For queries about the content of this document, please contact: Dan Clay dan.clay@thesocialagency.co.uk
The Social Agency
The Fisheries,
1 Mentmore Terrace,
London,
E8 3PN
Telephone: +44 (0)7841 775192
For Annex A:
London Economics Head Office
Somerset House,
New Wing,
Strand,
London,
WC2R 1LA,
United Kingdom
Website: www.londoneconomics.co.uk
Email: info@londoneconomics.co.uk
Twitter: @LondonEconomics
Telephone: +44 (0)20 3701 7700
Fax: +44 (0)20 3701 7701
Press enquiries should be directed to the Department for Work and Pensions Press Office: Media enquiries: 0203 267 5129; Out of hours: 0203 267 5144; Website www.dwp.gov.uk. Follow us on Twitter: www.twitter.com/dwppressoffice
1. Research background and context
This research was conducted in February to April 2022. Statistics and views reported were accurate in relation to the health assessment providers at that point in time.
The Department makes around 1.9 million assessments for disability benefits each year. Ensuring the supply of health and disability assessments (delivered through the contracted providers: IAS, CHDA and Capita) adequately matches the demand for health and disability assessments, has always been a challenge for DWP. This has been driven in part by inadequate levels of assessor recruitment and retention, as previous investigations into this issue (available to DWP internally) have shown.
DWP commissioned The Social Agency (formerly Basis Social) to undertake research to obtain insight into barriers to the recruitment and retention of health and disability benefit assessors. This evidence will be used to inform measures to improve recruitment and retention of assessors, therefore improving providers’ assessment capacity (and DWP’s ability) to meet demand for assessments - potentially leading to better service, and better value for money for DWP.
The research design consists of three methodological strands, to triangulate insights and provide a robust rationale for any potential changes that address recruitment and retention:
1. Economic analysis of supply and demand issues around employment of health care professionals and the implications for assessor employment. This strand was led by consultants at London Economics and involved assessing:
a) The state of supply of potential assessors, including recent labour market trends and key drivers of change in labour market supply
b) A comparison of skills and work activities for healthcare professionals (HCPs) and assessors
c) The challenge in recruitment and retention of assessors, and assessor needs to meet demand for WCA and PIP assessments
London Economics produced Annex A to support the main report. The annex uses evidence from the Labour Force Survey to determine the size and characteristics of the population of healthcare professionals and those with relevant qualifications, from which assessment providers (APs) might recruit. It also compares the salaries offered by APs with those of relevant healthcare professionals (using the Annual Survey of Hours and Earnings), as well as salaries associated with agency or bank nurses. The annex draws on data from a United States occupational classification database (known as O*NET) to compare the skills and work activities of healthcare professionals and assessors.
Finally, the annex uses data provided by DWP and APs to analyse retention issues and the levels of recruitment that would be required to meet demand for WCA and PIP assessments.
2. An evidence review into best practice around delivering services in ways that support retention and wellbeing across similar public services. This involved a review of publicly available information to assess:
a) Whether DWP’s health assessment providers face barriers to assessor recruitment and retention, relative to comparable examples in the public sector, and the extent to which these were driven by different factors
b) Whether public sector contractor’s characteristics (for example, age, region, job seniority, clinical profession, working patterns) are relevant factors in supporting recruitment and retention
c) Examples of successfully mitigating against identified barriers in the public sector and whether these are transferable to DWP
From an initial phase of ‘discovery’ of circa 60 publicly available sources, the evidence presented a challenge in a lack of recruitment and retention experiences that felt analogous to the context of disability benefit assessors. The discovery phase consisted of reading a small range of documents supplied by DWP, with most other sources found online, across range of articles, and academic and public policy documents. The online search used the following search terms or phrases:
-
HCP or healthcare staffing, recruitment, retention; coupled with named healthcare ‘sector experts’ for example, the Health Foundation, Kings Fund and Nuffield Trust
-
recruitment, retention, experiences of other Assessor roles for example, ESA / UC
-
recruitment and retention issues or barriers for health care professionals (nurses, doctors, occupational therapists, physiotherapists, paramedics - not a great deal on the last three)
-
recruitment and retention issues or barriers in the public sector
-
research into contractors outsourcing in the public sector
-
recruitment and retention of healthcare workers in EU, Scandinavia and America
-
best practice recruitment (general)
-
best practice retention (general)
-
best practice regarding recruitment and retention of healthcare professionals domestically and internationally
The ‘contracted-in’ nature of HCPs to APs is a specific type of recruitment and employment experience, and the job of an HDA is a very different to how HCPs would have been working in their prior clinical professions. After discussion with DWP on the limitations of the evidence review, it was agreed that the qualitative element of the research could best interrogate questions on both public sector contract processes, and how characteristics of those HCPs who become assessors impact recruitment and retention. The evidence review, therefore, focusses on the overarching ‘best practice’ element of the research objectives, interrogating relevant contexts such as NHS, Education, and general recruitment and retention practices, to understand what strategies are used - or advised - to recruit and retain talent, and whether any learnings are transferable to the context of disability benefit assessors.
3. Qualitative research with DWP agents, assessors, provider executives, and recruiters involved in the recruitment of health and disability assessors to contracted providers. The aims of this research included:
a) the barriers to the recruitment and retention of assessors, including variation across WCA and PIP assessments
b) understanding potential changes which could mitigate against these barriers
c) whether assessor characteristics (for example, age, region, job seniority, clinical profession, occupational history, working patterns) are relevant factors in determining the likelihood of recruitment and retention
DWP staff, assessor and provider executive sample was provided to the research team by DWP. Across the assessor and provider sample we looked to achieve an equal spread of representation across IAS, CHDA and Capita however this was dependent on the volume of sample received, which was not equal across providers.[footnote 1] Recruiters working for firms which themselves recruit disability assessors on behalf of contracted providers were recruited via a professional, independent research recruiter (Acumen). Participants received incentives of between £50 to recognise their time and expertise in contributing to the research.
A total of 35 interviews were undertaken between February and April 2022. The sample achieved was as follows:
-
DWP Contract Management staff (n 8)
-
Senior Provider Executives (n 3)
- Assessors
- IAS (n 9)
- CHDA (n 5)
- Capita (n 5)
- Recruiters working on behalf of contracted providers (n 5)
A standardised topic guide was developed for use with each of the four stakeholder groups. These are included in Annexes C,D,E and F. This variously covered motivations and expectations of assessors, views toward the recruitment and approval process, core competencies for HDAs, the job market for HDAs (including supply and demand), drivers of attrition, and the challenges and opportunities to improve recruitment and retention. All interviews were recorded and transcribed. The research team used framework analysis as a method for organising and managing data through a process of summation and synthesis, resulting in a series of themed matrices tied to the topic guides (and aims for the research).
This research report brings together these three inter-related research activities, with evidence triangulated and presented under two chapters: one relating to recruitment and one relating to retention.
2. Health and disability assessor recruitment
2.1. The recruitment challenge
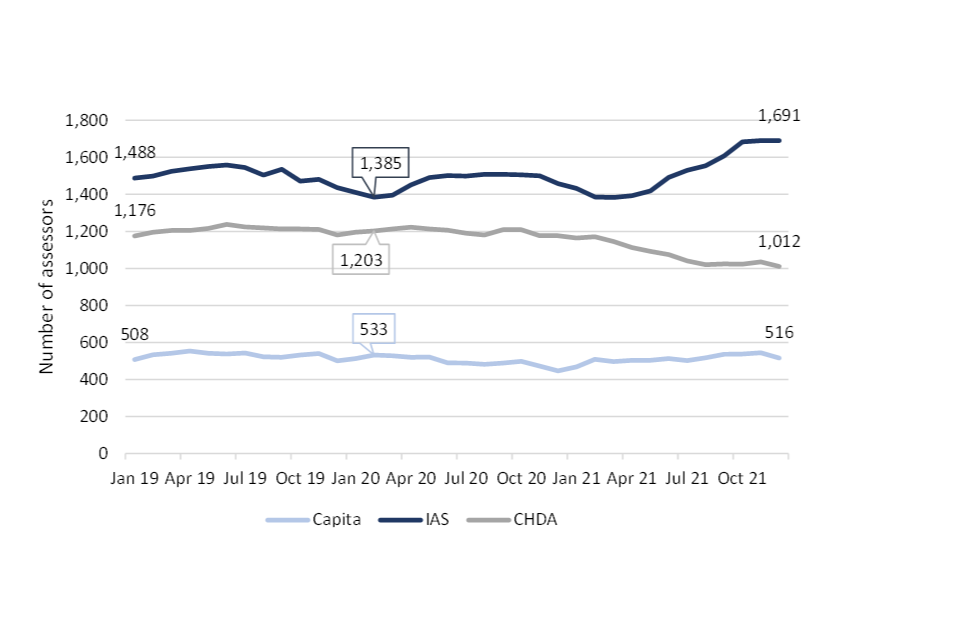
There were 3,219 full-time equivalent (FTE) health and disability assessors (HDAs) in December 2021 (the most recent data available at the time of writing) based on the data provided by the three APs contracted to deliver health and disability assessments: Capita and IAS (both delivering Personal Independent Payment assessments) and CHDA (delivering Work Capability Assessments). This is approximately 50 more FTE assessors than there were in total in January 2020 and around 100 more than in February 2020 immediately before the COVID-19 pandemic. Although there was an increase in the number of assessors in the first 6 months of the pandemic (to September 2020), there was a significant reduction in the number of assessors across all APs between October 2020 to the beginning of 2021. However, since April 2021, modest levels of growth have taken place (largely driven by IAS), with approximately 200 more assessors becoming available (3,010 in April 2021 compared to 3,219 in December 2021).
The availability of assessors since January 2019 has been varied across the 3 APs see Figure 1). The number of FTE assessors at IAS increased by 14% from 1,488 in January 2019 to 1,691 in December 2021. However, underneath this upward trend, IAS lost around 100 assessors between January 2019 and February 2020, so their growth has been 22% since February 2020. For CHDA, the number of FTE assessors was broadly stable from January 2019 to October 2020, then declined by 16% in the months to December 2021 (from 1,210 to 1,012). For Capita, there were approximately the same number of assessors in January 2022 as in January 2019.
Figure 2.1: Number of FTE health and disability assessors, by provider, January 2019 to December 2021[footnote 2]
Workforce retention is a very serious issue for all APs. Across all providers an average of 4.3% of assessors left the occupation each month throughout 2021 (which compares to an estimate of 3.5% per month in both 2019 and 2020). In annual terms, this is equivalent to an attrition rate of 52% in 2021: 4 to 5 times higher than ‘source’ occupations in the NHS[footnote 3]. Approximately, 40% of new recruits also leave during the training period. Due to these levels of attrition, very high recruitment levels are required to maintain the workforce required to meet assessment targets (for instance, between 2,000 and 3,000 FTE assessors per year, which is approximately 60% to 90% the size of the HDA workforce at the time of writing).
There’s a shelf life with this role.
(Senior stakeholder – AP)
By understanding how to address retention issues amongst both new recruits and more experienced staff this will help initiate actions that will moderate the recruitment demand among APs, while also improving operational capacity to deliver against targets. While recruitment and retention are bound up with one another in terms of APs ability to meet demand for health and disability assessments, there are also clear learnings in relation to both which are separated in this report for clarity. This section (Section 2) focuses on recruitment, while Section 4 focuses on retention.
2.2. Competencies of a ‘good’ assessor
HDAs must be registered healthcare professionals with at least 1 to 2 years’ UK experience (depending on the job specification). The following healthcare professions are eligible to become assessors:
- Doctors
- Nurses
- Physiotherapists
- Occupational therapists
- Paramedics (only for PIP)
One issue around the identified recruitment and retention issues could be that the skills required and work activities performed by HDAs differ from those of healthcare professionals more generally, meaning HCPs may struggle to adapt to the different nature of the HDA remit, and not be attracted to the core assessment role of the HDA.
HDAs are recruited primarily using a qualifications-based approach. Namely, assessors are required to be trained as doctors, nurses, occupational therapists, physiotherapists or paramedics with at least one to two years’ UK experience. This recruitment strategy is designed to ensure that assessors have the required medical knowledge for the job. However, there are elements of an assessor’s job that differ from the healthcare professions from which they are recruited. For example, a key part of an assessor’s job is to write 3,000 to 4,000-word reports detailing the assessment undertaken and relevant recommendations, which is something rarely done by nurses (for example).
In Annex A (section A.4), London Economics looked into the similarity between HCPs and the assessment element of the HDA role using the Occupational Information Network (O*NET).[footnote 4] We summarise some of the key findings here.
The HDA role can be considered a combination of two discrete occupations: healthcare professional and benefits assessor. The role has aspects of a healthcare professional’s role in using medical knowledge to understand health conditions. However, the role differs from that of an HCP in the sense that assessments require an appraisal against criteria, rather than diagnosing medical conditions. The assessor role also does not have the ongoing caring role of healthcare professionals, as their role is only of initial assessment. The HDA role also incorporates some aspects of a benefits assessor role in respect of the need to assess against functional criteria and to write reports. However, it differs from a traditional benefits assessor role as HDAs do not make the final decision on benefits eligibility. HDAs also need to use medical knowledge, which is not required in a traditional benefits assessor role.
Using information from O*NET, London Economics were able to identify the skills and work activities that are similar and different, helping to understand what core competencies are likely to be relevant to HDA roles:
-
HCP roles require a wider variety of skills than those required by benefits assessors. This finding suggests that HCPs may be over-qualified for the assessment element of the HDA role
-
Many interpersonal skills and analytical skills are more important for HCPs than for benefits assessors. However, speaking and active listening skills are generally more important for benefits assessors than for HCPs
-
Benefits assessors undertake tasks that are generally more desk-based than those undertaken by HCPs, such as administrative activities and working with computers
-
HCP roles require undertaking more abstract tasks (such as creativity and problem solving), more management, training and team-related tasks, and fewer planning tasks (such as organising, planning, and prioritising work) than benefits assessors
-
Delivering therapeutic care is an essential part of an HCP role, but is not part of the assessor role.
From the qualitative research, a set of HDA ‘core competencies’ were informally reported by those who work in the role themselves, those who have oversight of assessors in APs, DWP contract management and HDA recruiters. These core competencies were described as:
- Excellent interpersonal and communication skills
- Critical and objective thinking skills, coupled with an investigative mindset
- Broad grounding in clinical practice - for instance, those who are experienced and work across a range of cases/people (for example, nurses, doctors, paramedics)
- Good time management and organisational skills
- Good clerical and administrative skills, including solid IT literacy
- Detail oriented, with the ability to record and report a lot of information
- Resilient (needed for both dealing with customers and receiving performance feedback)
- Ability to work independently, self-starting attitude
- Ability to embrace repetitive tasks (regarding the nature of the assessment and reporting process)
- Analytical rigour (needed for assessing against functional criteria to individual customer cases)
Another way of looking at what soft and hard skills are needed for HDA roles is to look at the type of person the role is most or least suited to. There was a high degree of consistency in the feedback received from all of the different participants interviewed as part of this research, as well as with the O*NET analysis undertaken by London Economics.
Table 2.1 Attributes, skills, and experience of those most and least suited to HDA role.
| Area | HDA role most suited to those who… | HDA role least suited to those who… |
|---|---|---|
| Experience | 1) Have had exposure to a wide range of disabilities and presenting conditions 2) Are comfortable to work across diverse cases including physical and mental health conditions | 1) Have operated in more specialist roles or settings (for example, managerial staff, anaesthetists, care home nurses etc.) where they have been exposed to a narrower breadth of issues/experiences 2) Do not have enough clinical experience - newly qualified staff will probably be able to pass training relatively quickly but often don’t have breadth of experience required to excel in role (and achieve the quality competencies) |
| Motivations and expectations for role | 1) Want the standard ‘9 to 5’ working arrangement verses an NHS shift pattern (perhaps to suit family commitments) 2) Are prepared to work full time (in the main HDA roles are FT) 3) Are happy to work from home, if primarily doing telephone assessments | 1) Are looking to ‘wind down’ in their career. The HDA role is demanding and taps into new skills that HCPs may need to sharpen (clerical, analytical, technological) 2) Are more stuck in their ways and not willing or able to reskill |
| Resilience | 1) Are happy to receive feedback on the quality of their reports and act on this 2) Can cope with repetitive tasks 3) Can cope with the sometimes emotionally demanding nature of the work | Are less able to deal with the emotional toll of dealing with customer claims, for example, having to hear about the impact of physical/mental conditions as on a daily basis |
| Interpersonal skills | 1) Enjoy communicating with people 2) Have empathy and patience, key for assessing customers with different needs and issues | |
| Assessment-related skills | 1) Used to performing assessments and writing reports in their previous HCP role, and handing those over to other professionals (OT’s, physiotherapists and paramedics are deemed to fit this most) 2) Can understand the benefit criteria and objectively ground their assessment approach within this 3) Can comfortably go ‘off-script’ and probe into a customer’s answers 4) Are happy to engage with a clerical role due to the central need to record and report data on customer disabilities 5) Are digitally savvy, feeling confident around computer software and systems | 1) Focus more on a customer’s conditions rather than the functional impact of those conditions on their daily living, mobility, or capability to work as per the benefit criteria 2) Struggle with or dislike clerical tasks and cannot type quickly 3) Struggle with technology (working with multiple systems and programmes is part of the training, assessment and reporting process) 4) Are not as comfortable with data collection (some HCP roles, for example, doctors, are used to taking patients’ clinical history verses nurses who are more aligned with care and treatment) 5) Do not like working with virtual channels, for example, telephone and video (although face to face assessments happen, pandemic working has necessitated the use of telephone in the main) |
Knowledge, in the form of being a qualified doctor, nurse, occupational therapist, physiotherapist or paramedic, is a pre-requisite for HDAs. In discussions with assessors, APs and recruiters it was clear that not all professions were equivalent in the extent to which they prepared people for performing a role as an HDA. Given the variety of presenting disabilities (and impacts on functioning) there was a general view that more generalist HCPs are better suited to the role, given their familiarity with a wider set of conditions. These included GPs, nurses and paramedics. This is supported by the wider literature that some HDAs do not have enough specific knowledge to carry out health and disability assessments. For example, physiotherapists may not have sufficient medical knowledge on non-physical conditions, such as mental health conditions. Disability charity Scope ran a survey of disabled people and their carers in 2021, which found that over two thirds of survey respondents felt that their assessor did not understand their condition or impairment.[footnote 5] Only 12% of respondents felt that the assessor understood their condition or impairment.
The reality of who comes through the recruitment process does not always fully match this ideal list of HDA core competencies, due to a combination of unclear communications of these competencies and understanding of what the job entails - which can sometimes become apparent only when into the training and onboarding process, or commencing work as an HDA. This disconnect is explored further in Sections 3 and 4 of the report.
If potential HDAs do not have the required knowledge, skills and abilities for the tasks that they are expected to perform, then it is likely to lead to job dissatisfaction and therefore to poor assessor retention. Similarly, if potential assessors do not feel that they have the required knowledge, skills and abilities to become an assessor, then they are unlikely to apply to become one.
2.3. Supply of potential assessors
As previously described, there are five healthcare professions eligible to become assessors at the time of writing: doctors, nurses, physiotherapists, occupational therapists and paramedics (only for PIP). Based on data on the number of healthcare professionals registered in the professions from which HDAs are recruited, there is a large supply of registered healthcare professionals as well as appropriately qualified individuals working in other occupations.
The total number of registered HCPs increased by around 180,000 (18%) between 2013 and 2021, from around 1 million to 1.18 million. Nurses made up the largest proportion of healthcare professionals, standing at approximately 59% in 2021 (corresponding to approximately 700,000 registered nurses). Doctors made up the second largest proportion of the HCP population in 2021 (30%), which increased from 26% in 2013. Approximately 350,000 doctors were on the register in December 2021. The other occupations only make up around 11% of the HCP population between them (4% for occupational therapists, 3% for paramedics and 5% for physiotherapists). However, the other occupations saw substantial growth between 2013 and 2021, particularly paramedics. The pool of occupational therapists grew by 25%, paramedics by 62% and physiotherapists by 24%. In September 2021, there were around 60,000 registered physiotherapists, 42,000 registered occupational therapists and 31,000 registered paramedics. Most of those qualified as HCPs choose to work in health-related fields, but there are a modest proportion of individuals – approximately 600,000 - who work in other occupations.[footnote 6]
Despite recent growth in the economically inactive population during the COVID-19 pandemic, the number of appropriately qualified individuals that are economically inactive who are likely to return to work is relatively small. As unemployment is also relatively low (as of February 2022), APs are likely to mostly recruit from those already in work. More detail is available in Annex A.
Within the last 6 to 8 months, DWP contract managers and executives from APs report that recruitment has significantly improved (notably for Capita and IAS)[footnote 7], such that there are full training HDA cohorts for months ahead – a marked difference to the recruitment situation at a similar point in 2021. Several factors were seen to have driven this improvement in the supply of HDAs:
1. A key external driver causing a flush of supply into the market has been people leaving the NHS due to the increased stress of working through the COVID-19 pandemic[footnote 8], and to a lesser extent the resulting cultural shift spurring desire for a career change. Recruiters have historically seen plenty of applications for HDA roles from HCPs who “feel despondent with the hands-on nature of their role”, although this has not guaranteed that the candidates were right for the role (regarding profession, experience, and role ‘fit’), and therefore this has not always translated to ‘quality’ supply.
You see two brackets of [HCPs] who apply: ones in busy hospital environments who are totally burnt out and the other bracket is the ones who want to work from home…the second one is about more flexibility – it’s all about work/life balance.
(HDA Recruiter)
2. Assessments have moved from face-to-face to telephone as a result of COVID-19, and those providers with the ability to set HDAs up to work from home (IAS, Capita) have been able to offer a more attractive proposition to those HCPs who desire greater flexibility in where they work. This change of assessment channel broadened the recruitment pool from those living around a specific location (to manage clinic and home consultations) to potentially across the whole of the UK. CHDA has been less able to take advantage of this as – at the point of this research – had yet to implement working from home for HDAs, and despite paying higher salaries, are attracting comparatively less candidates.[footnote 9]
We have got an extremely healthy pipeline. Now, if we were having this conversation this time twelve months ago it would have been a completely different story so there’s been a lot of things that have changed over the last twelve months that has allowed us to cast our net a little bit wider and the main thing that has changed has been the fact that we can recruit our practitioners anywhere across the country because of the telephone assessment approach.
(AP Executive)
The game changer has been home working and hybrid working approach.
(DWP Contract Manager)
It’s not just about pay. CHDA pay more than IAS and Capita, but they aren’t recruiting the same numbers. CHDA don’t have so much working from home.
(DWP Contract Manager)
3. Further broadening the pool of prospective talent was a change to who could apply to become an HDA. Previously restricted to those HCPs with two years of clinical experience, this has now been reduced to 12+ months of experience, attracting those who are newly qualified into HDA roles.
4. In the case of IAS, in April 2021 salaries were aligned with other providers, which Account Executives believe to be a secondary driving factor for increased recruitment to their PIP assessor roles.
5. IAS also felt that the recent introduction of testimonials from experienced HDAs in the recruitment process has provided a better sense of what the role is like for potential recruits, encouraging them to move forward with the application process.
We did things like telling stories of HPs so we’d get a HP that had been recruited in Hull as an example, talking about where she’d come from, how she’s transitioned into the role, how she found it and it was a bit like a testimonial sort of advertising campaign where other practitioners could see it and think do you know what I am a mental health nurse and actually I could apply these skills to that role and she seems to be enjoying it.
(AP Executive)
The analysis in Annex A by London Economics highlights that recent wider labour market trends since the beginning of COVID-19 have been characterised declining employment levels and a move towards economic inactivity. Research by the Institute for Employment Studies claims that the number of individuals actively participating in the labour force is approximately 1.15 million lower than it would have been if pre-pandemic growth had continued.[footnote 10] Around three-fifths of this difference is due to increased economic inactivity, particularly amongst women, while the remaining two-fifths is as a result of limited population growth. The decreased labour force participation rate is likely to decrease the size of the potential HDA workforce going forward.
While participation rates in the labour force have decreased, unemployment remains low (as of February 2022), at 4.1%, which is 0.1 percentage points higher than pre-pandemic levels.[footnote 11] At the same time, there were approximately 1.3 million job vacancies in February 2022, which is the highest on record.[footnote 12] Without even considering the extent of either skills mismatch or geographic disparities, the ratio of job vacancies to claimant count the lowest on record.[footnote 13] This combination of factors, and in particular the plentiful supply of outside options for healthcare professionals, makes the labour market exceptionally challenging for recruitment at the time of writing.
2.4. Demand for Health Care Practitioners (HCP)
It is well documented that as we come out of the COVID-19 pandemic, the UK labour market is experiencing considerable upheaval, with pressure on hiring growing, with significant skills and talent gaps across many roles.[footnote 14] CIPD’s Resourcing and talent planning survey (with responses from a broad mix of private and public sector organisations including public administration, education and health) heard that 45% of respondents believe that competition for well-qualified talent has increased, and a similar proportion of employers who attempted to recruit had difficulties attracting suitable candidates.[footnote 15]
The level of vacancies at the time of writing is a particular challenge in healthcare. There were 206,000 vacancies in the human health and social work activities sector in November 2021 to January 2022, which is approximately 5.1 vacancies for each 100 employee jobs in the sector, compared to 3.4 before the pandemic. The statistic is also higher than the overall average of 4.3 across all economic sectors. Vacancies are also persistently high in the NHS, particularly in nursing (see Annex A for more detail). Given the fact that the supply of newly qualified nurses is based on NHS estimates of patient demands, and increasing the training pipeline is both hugely expensive and takes a considerable length of time to realise, competition for HCPs is likely to remain high. This will make recruitment by APs extremely challenging in the short and medium term (even in the presence of competitive wage offers).
APs generally offer a range of salaries, which depend on (a) the location of the role, and (b) the type of role. Generally, higher salaries are offered in Greater London and areas around London (such as the South East)[footnote 16]. As Table 2.2 shows, the variation in advertised salaries is relatively wide across the APs, ranging from £34,000 to £46,200. Generally, salaries for PIP assessors (PIP assessments are provided by Capita and IAS) are lower than salaries for WCA assessors (WCAs are provided by CHDA).
Table 2.2 Annual advertised starting salaries offered by APs in 2021.[footnote 17]
| Assessment provider | Low | High | Other salaries found |
|---|---|---|---|
| Capita | £34,000 | - | - |
| IAS | £35,000 | £42,000 | £46,200 |
| CHDA | £39,500 | £46,300 | £72,000 - £84,200 |
Note: The only salary that can be found through the Capita vacancy page is £34,000. On the IAS website, salaries of £35,000 to £42,000 are advertised, but salaries for IAS PIP assessors in London are advertised elsewhere as up to £46,200. The low salary for CHDA is for outside London, while the high salary relates to positions based in London. The other salaries found for CHDA assessors are for doctors only - £72,000 is the figure for outside London, and £84,200 is the figure for within London.
The starting salaries offered by APs are put into context in Figure 2, which shows where the starting salaries offered by the APs rank in terms of the percentile of gross earnings of full-time employed HCPs. The starting salaries offered by APs are not particularly competitive, as shown by the relatively high proportion of HCPs that are already earning more than the HDA starting salary. The highest salary offered outside of London is at the 58th percentile for full-time nurses, the 60th percentile for full-time physiotherapists and the 75th percentile for full-time occupational therapists.[footnote 17]
This means that many full-time workers (42% of nurses, 40% of physiotherapists and 25% of occupational therapists) in those healthcare professions will already be earning more than the salary offered by the APs. In fact, the lowest salary offered by providers is below the median salary for full-time employees in every profession studied. The lower salaries offered by APs are similar to the total level of pay achieved by an NHS healthcare professional with approximately 4+ years’ experience positioned towards the top of Band 5. While the assessment provider salaries studied refer to starting salaries for HDAs and are compared to salaries for experienced HCPs, it is these experienced HCPs that APs are looking to attract, so this is a relevant comparison.
Persistent unpaid overtime in the HDA role (if it occurs) would also make the salary even less attractive, particularly given the option to take on extra hours for additional pay in HCP roles, such as nursing (either directly through the NHS or indirectly though agency work).
Figure 2: Yearly gross earnings percentiles of starting salaries offered by APs in 2021 (full-time employees)[footnote 18]
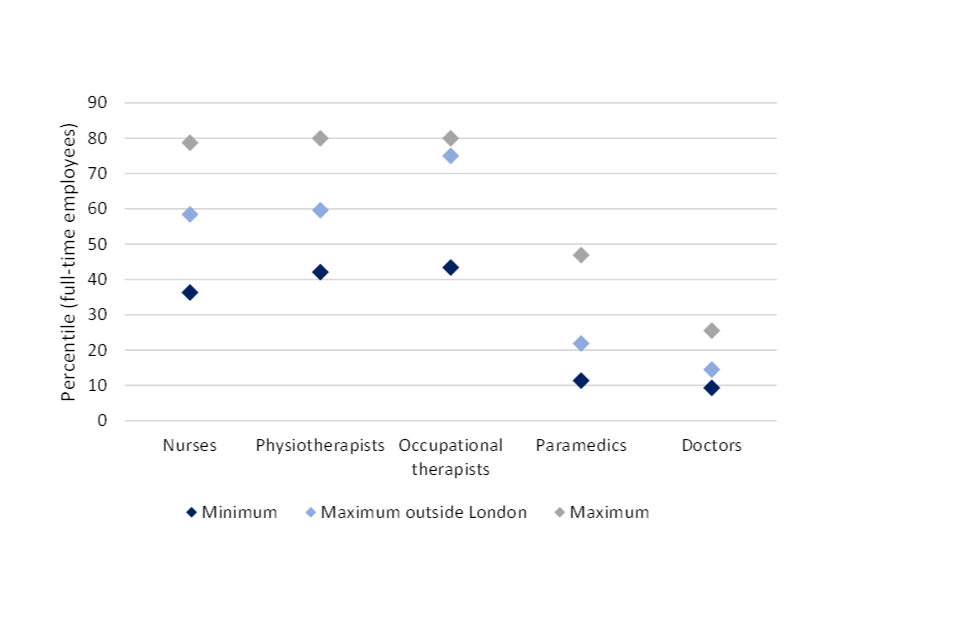
Note: Based on gross yearly earnings for full-time workers in each occupation. Only refers to salaries for regular health and disability assessors (for instance, does not include data on occupation-specific roles). Salaries considered are: Minimum: £34,000, Maximum outside London: £39,500, Maximum: £46,200. The highest percentile recorded for physiotherapists and occupational therapists in the ASHE data is the 80th percentile, so the true percentile of the highest salary is likely to be higher than that. Refers to starting salaries of APs only.
To attract potential recruits to become HDAs, this analysis suggests that the APs should be offering higher wages to HDAs, of at least £38,000 per year outside London (some APs already offer more than this). However, offering a higher starting salary than that (closer to £45,000) would be required to even start to financially attract approximately 30% more of the full-time nursing, physiotherapist and occupational therapist workforce. These salaries reflect 2021 prices, so due to high inflation in late 2021 and 2022, the nominal salaries required may be higher. See Annex A for more detail.
The qualitative research confirmed that the key competition for HDAs was the NHS, or roles in the private healthcare sector. Due to the ongoing availability of roles (permanent and contract), the relatively high salaries, and the familiarity of these roles to qualified HCPs working as HDAs, there is always a danger that HDAs are attracted back into therapeutic roles even after leaving the NHS. COVID-19 was also felt to be a bit of a ‘call to arms’ for the healthcare profession, so while many people may have left due to the pressures of delivering care in the pandemic, it may also have resulted in practitioners going back into the NHS.
Some leave because, you know, their heart, actually they realise their heart belongs back in whatever they were doing before.
(DWP Contract Manager)
Recruiters mentioned other smaller areas of demand for HCPs as: alternative disability assessor roles outside of PIP and WCA, health assessors in local authorities, or assessing people for claims in the travel industry (which apparently pays a little more than an HDA salary). Although levels of demand are reportedly not quite as high for these roles, they may seem like an attractive alternative to HDA roles as there is less (negative) stigma attached as compared to health disability assessment for DWP resulting from the negative press around disability benefits and the role itself.
2.5. HCP expectations/motivations regarding Health and Disability Assessor roles
As described in the previous section a key external driver for increased supply of HCPs into the HDA job market is ‘burnout’, an issue exacerbated by the COVID-19 pandemic. Focussing rather on what the HDA role offers candidates, interviews across the qualitative research sample revealed a consensus on the motivations for HCPs to consider the HDA role. These motivations can be listed in descending order of importance to HCPs (who, as previously stated, often come from roles in the NHS):
1. Fixed working pattern: Most HCPs who tend to consider the HDA role have experienced frequently changing patterns of shift work, work on weekends and bank holidays, long hours and unpaid overtime. To them, the prospect of a classic ‘9 to 5’ and a 40-hour work week (which is how the HDA role is positioned by providers) is an attractive proposition. Also, it was reported that this is especially attractive to HCPs who have family commitments and seek more regularity (for example, working when kids are at school) and less reliance on childcare.
2. Flexibility and work/life balance: Flexibility speaks to the potential for homeworking and hybrid working, as offered primarily by PIP APs, since the change to the assessment operational model under COVID-19 easement. Combining this flexibility with the fixed working pattern is highly motivating as it is believed to provide a less stressful and better work/life balance as compared to what HCPs might be experiencing in their healthcare roles.
The fact that if they’re working in a hospital, they might have to work Saturdays and Sundays and nights but you don’t have to do that when you’re working on PIP and actually it’s a different environment from an NHS environment.
You’re not walking like a zombie all night like you were on the night shift.
(HDA)
I didn’t get into nursing originally to get into assessing… it is something I reflect on and struggle with actually… but actually it is just too difficult [nursing].
(HDA)
3. Salaries are relatively attractive: While not providing a salary bump to all HCPs, the HDA salary range was seen as being competitive with the salaries of HCPs who may be applying for the role. For those who are early on in clinical career or working at a junior level (for example. a band 5/6 nurse), the salary offered against the stated hours in the contract was felt to be adequate. The salary is also wrapped up in an overall benefits package (which may differ across APs) offering for example, pension, healthcare, life assurance, and a retail discount programme.
The money side of it is better than the NHS.
(HDA)
I am now on the same wage as top band 6, if not more.
(HDA)
4. Development (or maintenance) of medical knowledge: HDAs need to be able to assess a wide range of physical and mental health conditions that HCPs may not have been previously exposed to. The training programme and commitment to ongoing CPD offered by APs helps to build a broad base of medical knowledge and to keep this up-to-date. This is particularly important given the potential for HDAs to move back into HCP roles.
5. The job has an altruistic element for some: Having worked in a job caring for others, HCPs can recognise the HDA role as helping those who are vulnerable and most in need, listening to them and enabling them to get the right benefits.
Health Professionals can still do what they’re passionate about [healthcare] but maybe in a less – in a different environment from what they’re used to, potentially, in the NHS.
(DWP Contract Manager)
We are the people for last port of call [for the claimants].
(HDA)
Overall, it was not one specific benefit that was the primary driver toward applying to become an HDA, but rather the combination of each of the above. Amongst those attracted by the role it was seen as less demanding versus the NHS, offering a better work/life balance, with no more shifts and nights, all matched with an attractive (or comparable) salary. HDA recruiters reported that nurses were especially attracted to the role.
The overall package is a motivator.
(DWP Contract Manager)
These motivations translate to set of expectations that HCPs have going into the HDA role. The following section will explore the how the reality of the HDA role does not always live up to these expectations and the drivers for this disconnect.
2.6. Challenges for recruitment
The qualitative research revealed strong perceptions that the majority of issues regarding the maintenance of the HDA workforce are more clearly attributed to ‘retention’, once HCPs had started training or were working in the role. However, 6 key recruitment challenges were also identified.
2.6.1. The HDA ‘micro-market’ created by DWP is limited in scope to recruit
The HDA workforce is a secondary job market of HCPs, tapping into the already highly competitive primary market for qualified and experienced HCPs in NHS and private healthcare roles (see also Sections 3.3 and 3.4). As recruitment criteria are narrowly defined, requiring medical qualifications and clinical experience, there is limited scope to recruit HDAs, and effectively DWP have designed a ‘micro-market’ of HDA labour. DWP Contract Managers noted the limitations of this situation, questioning whether ongoing staff shortages are indeed endemic to this type of market arrangement.
The Disability Assessor market is a construct of DWPs making. There is a finite number of assessors.
(DWP Contract Manager)
One of the issues with recruitment and retention is that DWP are creating a micro-market…if one provider increases salaries you get movement between agencies. That’s not wholesale or big numbers but it is a factor.
(DWP Contract Manager)
Another factor impacting the scope to recruit is the limitation on the range of qualifying roles to become an HDA. Naturally, contract obligations will play a role in defining who is eligible to be an HDA, but APs question the rationale for not including other relevant health professionals, for example, pharmacists (who assess and prescribe) and midwives, thus broadening the pool from which they can recruit. It seems as if there may be room to both open the market and rationalise it across providers, so that each provider is not so clearly in competition with one another, impacting the recruitment pipeline and consistency of service delivery.
Is there a point that the DWP or whoever’s doing this sort of service needs to understand, actually, you know, the capacity is likely to be X and therefore you’re going to have to design to that capacity?
(DWP Contract Manager)
Why can’t we recruit pharmacists? They can assess and prescribe. And what about midwives?
(Senior Stakeholder – AP)
Further effecting the dynamics of the HDA job market are the range of salaries offered by different APs, sometimes resulting in a situation of HCPs moving between the different APs to receive an increase for effectively the same position. This kind of movement causes instability and raises a question on how salaries are determined by DWP and APs. Although it should be noted, as per Section 3.5, that salary is not the only motivator for selecting an HDA role, rather playing a part in the overall package, where flexibility and working pattern are also strong motivators for job choice.
If one provider increases salaries you get movement between agencies.
(DWP Contract Manager)
2.6.2. Candidates do not get a clear enough picture of the HDA role during the recruitment process
While the effects of this tend to play out as a retention issue (discussed fully in Section 3.3), a lack of awareness of the reality of the HDA role is, in part, attributed to the recruitment process. Although candidates seemed to understand the nature of the HDA role at the recruitment stage (assessing the functional impact of a disability and reporting this assessment), the pressures and demands of the role were not felt to be adequately communicated. The impact of this is that candidates who are unsuited for the role still progress past interview stage, as they may have the basic clinical skills required and are able to pass the relevant communication and clerical tests.
Qualitative feedback from across the sample was that some HCPs do not understand key aspects of the role:
-
that they will be translating their clinical skills into a very different kind of work product, one which is both not care-focussed and which has a degree of repetition that may not align with expectations
-
the need for good clerical skills and tech-savviness which they may not have used/developed in previous healthcare roles
-
a resilience to deal with both the emotional demands of assessing claimants and the consistent level of scrutiny and feedback on the ‘quality’ of their work
The idea that they would want to be on a treadmill of collecting details but not intervening is alien to a significant proportion of the health sector. A lot of people that apply for roles don’t understand this point. They arrive. Have rigorous training and penny drops that this is what role is.
(DWP Contract Manager)
One of the first things I would say is someone needs to be resilient, it’s not an easy role, it is very difficult not to allow the stories they hear through the PIP assessments to be absorbed, and not start affecting their mental health - and the way they feel about the role.
(Senior Stakeholder - AP)
I think we do find that people predominantly find this role very, very tough and they’ve got to be a certain kind of robust person.
(Senior Stakeholder - AP)
They should probably recruit the right people who can type when they are talking.
(Recruiter)
Sometimes these challenges were not clear until they progressed to the latter stages of the training and approval process, and when they were actually in a ‘room’ (virtual or face-to-face) with a real claimant, having to write up numerous reports in their contracted 40-hour weeks and having this performance audited.
In an NHS nurse role, get what is expected from you…people don’t realise it is gonna different be from the NHS.
(HDA)
I thought I would be a bit more clinical.
(HDA)
It was reported that some HCPs feel that they may have been mis-sold on the role, with recruiter’s keen to communicate an attractive package of work/life balance and competitive salary, rather than focus on the core competencies necessary to actually succeed in the role – which are somewhat more nuanced than simply having clinical experience. While IAS have recently started using some testimonials from long-standing members of staff on their ‘Recruitment Hub’, there has been limited opportunity for candidates to hear about the nuanced reality of the role – and crucially how it differs to one in healthcare.
When you go through recruitment they say you will pick it up pretty easy…the assessments are quite easy…but they are probably the polar opposite.
(HDA)
They don’t advertise the hard bit before the good bit.
(HDA)
The recruitment process could be clearer on what is expected…more detail on what is involved.
(HDA)
2.6.3. Lack of part-time and flexible opportunities
While the HDA role is often sold as having the benefit of flexibility this didn’t necessarily translate into reality in either the training and approval process, or in the role itself.
Aside from CHDA there did not appear to be the opportunity to carry out HDA training on a part-time basis, even when applying for a part-time role. Both recruiters and DWP contract managers question why a full time commitment is necessary for training and the ongoing job, as this restriction closes out key potential groups from recruitment, especially those who have family commitments and want to work part-time to manage these, or those HCPs who might be towards the end of their career and would like to step away from healthcare in to a related role that offered more of a ‘wind-down’ in pace. With the full-time training commitment this can be a barrier for some who feel that this is too big a trade-off without a guaranteed position, considering the level of competency that must be reached within a relatively short time frame, and prevents them taking flexible work during the training period (for example, NHS ‘bank’ shifts).
If they offer more flexibility and part-time they would attract a bigger audience.
(Recruiter)
In addition, ‘full time’ tends to mean the traditional ‘9 to 5’, and feedback included whether this could be structured more flexibly to attract a wider pool, for example, offering condensed hours, or the ability to independently structure time and do less time-sensitive tasks like report writing in the evening. It appeared that APs were variously developing and piloting a range of initiatives to provide this degree of flexibility (for example, for working parents who needed to work around school drop-off and pick-up).
2.6.4. HDA role not aligning with ‘calling’ to deliver therapeutic care
The qualitative interviews revealed a key emotional barrier preventing HCPs from considering the HDA role – or delaying application until feeling there was no other option but to leave the NHS: the concern at not being able to apply their clinical skills to deliver therapeutic care. Disability assessments are not what HCPs are trained to do, despite their clinical skills being uniquely required for that role. In fact the HDAs may see themselves as transitioning from a role where they are high respected to one where they are despised (or at the very least, stigmatised).
They didn’t intend to be 9 to 5 in an assessment centre day in day out…HCPs, like teachers, it’s a calling a need to care and look after.
(DWP Contract Manager)
HCPs train for long periods to achieve degree-level qualifications and/or sufficient levels of experience to qualify as a nurse, occupational therapist, doctor, paramedic etc., which would also have required a significant financial investment. They have tended to pursue their particular healthcare career due to more than simply the need for a job they enjoy – there is also the stronger, more emotional element of the role, and some HCPs describe a ‘calling’ to the profession driven by the altruistic desire to care for others. Even in the face of long hours, unsociable shifts and pandemic stress, the majority of HCPs (and those that work with them in the disability assessment sector) identify a strong connection with the ‘care’ elements of healthcare roles. There is also the perception that - despite the CPD offered to HDAs - being out of clinical practice compromises their ability to get back into clinical practice, actualised by a two-year ‘hard deadline’ out of clinical practice, at which point they lose their licence.
You are de-skilling yourself clinically.
(HDA)
Put it like this…did you train to become a nurse in order to do health assessments? I think probably in many cases generally probably not.
(DWP Contract Manager)
So let’s say you’re a nurse or a physio, you’ve probably done that from when you were eighteen or nineteen, you’ve done a degree for three or four years, you’ve done all this work to get to that point and then I think it’s very scary then to leave.
(HDA)
We all got in healthcare for altruistic reasons and that maybe isn’t the case in this job… you’re a cog in the machine doing bureaucratic work.
(HDA)
Disability assessment, in addition to being an appropriation of their clinical skills, is also compared unfavourably with the healthcare profession. This is largely due to the binary nature of the outcome, where their assessment of the functional impact of a claimant’s disability decides whether they will receive financial support. Even though HDAs are talking to and assessing claimants, trying to understand their daily struggles, the outcome is not always positive – for example, if that individual’s level of restriction does not ‘meet the criteria’ to receive the benefit. In addition to this, HDAs hear much about the impact of people’s physical and mental conditions daily, and at the end of a short assessment they cannot intervene or provide care to that person. It must also be noted that that distrust and negative perceptions of the assessment process are likely to be part of an individual’s broader perceptions and feelings towards policy direction and the government.
The negative emotional perceptions of the HDA role can prevent HCPs from applying, even if they are attracted by the overall package it offers. But a key issue exacerbating this barrier is the ‘negative press’ around APs and the role itself, where bad reviews from former HDAs are easily found on job websites. When this negativity is seen in black and white – with nothing positive and compelling to counter it - it serves to confirm their already negative perceptions of the role. Aligned to this was a view that the roles were always advertised, implying that they couldn’t be filled, again sowing seeds of doubt in people’s minds.
When you go onto Indeed and read really bad reviews for IAS…at first you think…well, you wouldn’t touch them.
(HDA)
Lots of people think about the job and then read these [reviews] and just shelve thinking about the job for a year… or just disregard the job.
(Recruiter)
Despite this broad concern around the reputation of the HDA role and the APs, some former HCPs positively described the role as having a ‘duty of care’, which aligns with the more human and emotional nature of healthcare – as they can help vulnerable people get the support they need. However, it is reported that this does not feature largely in the ‘selling’ of the role during the recruitment stage, despite some HCPs reporting it as motivating once in the role.
Sometimes the job is just not for everybody, sometimes it’s hard to remove yourself from that caring role and be a bit more critical.
(HDA)
2.6.5. The disability assessment sector offers limited opportunities for career progression
Views from across the qualitative research sample were that the HDA career path, and opportunities for progression from the role, seem limited and can reduce the attraction of the HDA role. It was widely acknowledged that the role could be perceived as a bit of a ‘dead end job’ or where you go to finish your career, with nowhere to progress to apart from becoming more senior in the assessment process (for example, a CSL or managerial role). HCPs, especially those in the NHS, are used to a clearly defined path of progression with established pay band scales and have access to a wide variety of opportunities and specialisms to try. The perception was that for some HCPs who were in the later stage of their career, the more flexible and standardised nature of the role might be acceptable, but for those who were earlier in their career this lack of progression was an inhibiting factor.
I don’t want to feel like I’m at a standstill.
(HDA)
The opportunities for job promotion are few and far between.
(HDA)
I don’t want to plateau at this time of my career.
(HDA)
Communications at the recruitment stage do not seem to tackle this issue, with job specs having limited scope for change when supplied to recruiters and expressing only a general sense of progression and opportunity outside the HDA role: for example, “Becoming a Disability Assessor is an excellent way to broaden your field of expertise and gain valuable experience that will open doors in your career – whether that’s management roles in the PIP team, working elsewhere in Capita, or wherever your career takes you.”[footnote 19] And as identified in the evidence review in Section 4.5 of this report, a core principle of ‘best practice’ retention is around clarity: to offer employees ‘clear career progression with opportunities to move within the organisation to expand skills and experience’.
2.6.6. Time-consuming recruitment process
Feedback from recruiters was that the recruitment process was off-putting for some and could be improved from an efficiency perspective. Typically, an HCP will apply via an online ad and submit their CV, then they will have an introductory interview with the recruiter. After this, candidates must go to the Assessment provider’s portal to complete a set of online competency assessments (for example, for IAS four tests are completed in one sitting) including an online typing test, tests designed to assess their clinical skills and knowledge, their observational skills, open questioning skills etc, all within the context of the disability assessment process. Assuming they pass the tests, candidates will progress for an interview with the assessment provider before being then offered the role (subject to passing the approval process). It was noted by recruiters that so many candidates find the test stage difficult, with a high rate of failure. Although that was seen as helping to remove inappropriate candidates it could be off-putting for encouraging applicants.
It’s a really lengthy process - can it be shortened? There are a lot of hoops to jump through. The majority fail online tests - if we could do this [establish competency] quicker it might be more efficient. I could establish are they suitable and then they can go through to do the test.
(Recruiter)
You might have less people accepting offers - but those people wouldn’t continue anyway…yes it would effect recruitment, but it would be a better outcome in the long term.
(DWP Contract Manager)
Really sort of, make sure that the upfront messaging means that only the right people want to [become assessors].
(DWP Contract Manager)
2.7. Best practices
From the evidence review, much of the documentation pertaining to ‘recruitment and retention’ provided a similar picture of the key elements which drive success, and some of those elements (for example, access to flexible working and fair reward) sit across both areas, being considered necessary to attract and retain staff. Below is a summary of core principles of a successful recruitment strategy, synthesised from evidence drawn from a range of sources, including:
-
Recruitment: an introduction (CIPD) [footnote 20]
-
‘Inspire, Attract and Recruit toolkit: Resources and guidance to support your workforce supply’ (NHS Employers)[footnote 21]
-
‘Wellbeing at work’ (CIPD)[footnote 22]
-
‘Recruitment and retention in adult social care: secrets of success Learning from employers what works well’ (Skills for care)[footnote 23]
Core principles of a successful recruitment strategy
1. Understanding your target workforce
Identifying and understanding the needs of target staff groups and how those needs may vary across different target demographics. Harnessing this knowledge can help tailor job advertising to maximise reach.
2. Designing a recruitment campaign that is tailored to attract your target workforce
Please see a best practice example ‘The Big Thank You’ at King’s College Hospital (KCH) in the annex of this document.
3. Recruiting via your existing workforce
Existing staff are ideally placed to talk about their careers and the benefits of working for an organization and are a useful way to attract new candidates through word-of-mouth advocacy. Through this approach, recruitment costs can be saved, and employees potentially incentivised to spread the word through referral reward schemes.
4. A recruitment process governed by principles of diversity and inclusion
The UK workforce is now more diverse than ever, reflecting changes in society and demographics of the population. The overarching values and strategy of an organization should work to promotes diversity and inclusion, with this cascading through the organisation into recruitment practices
5. Use of Values-based recruitment
Values-based recruitment (VBR) can help attract and select future employees whose personal values and behaviours align with that of the organisation.
6. Offering flexible working
Prior to the pandemic many workers across sectors chose to work part-time. Analysis from the Office for National Statistics shows that the proportion of part-time workers grew by around 50% from 2008 – 2018.[footnote 24] Flexible working also now implies how we work when at work, for example, is the nature of a role eligible for compressed hours or flexible work over the day or evening?
7. Being a ‘leading employer’
Demonstrating a good reputation and culture, a strong health and wellbeing approach, to communicating your reward package effectively, a strong employer brand is incredibly important in a competitive environment.
8. Communicating an attractive reward package
Developing a comprehensive package with attractive pay and benefits, and ensuring this is communicated at recruitment stage.
9. Induction and onboarding
The first six months in a new role typically influences whether an employee stays for the long term, making induction and the onboarding process crucial. An effective induction can help employees to perform at their best from the start. And during this period effective mentoring, senior support, structured appraisals, and a supportive learning environment can help retain staff.
2.8. Opportunities for improving recruitment
Based on qualitative feedback and reflection on ‘best practice’ for effective recruitment, five key opportunities areas were identified to improve recruitment of HDAs. However, it should be noted that they focus more on actions that could be taken by the actors in the disability assessment ecosystem (DWP and APs), being mindful that there are external market factors that can limit the available pool of HCPs.
Figure 3: Summary of opportunities to improve HDA recruitment
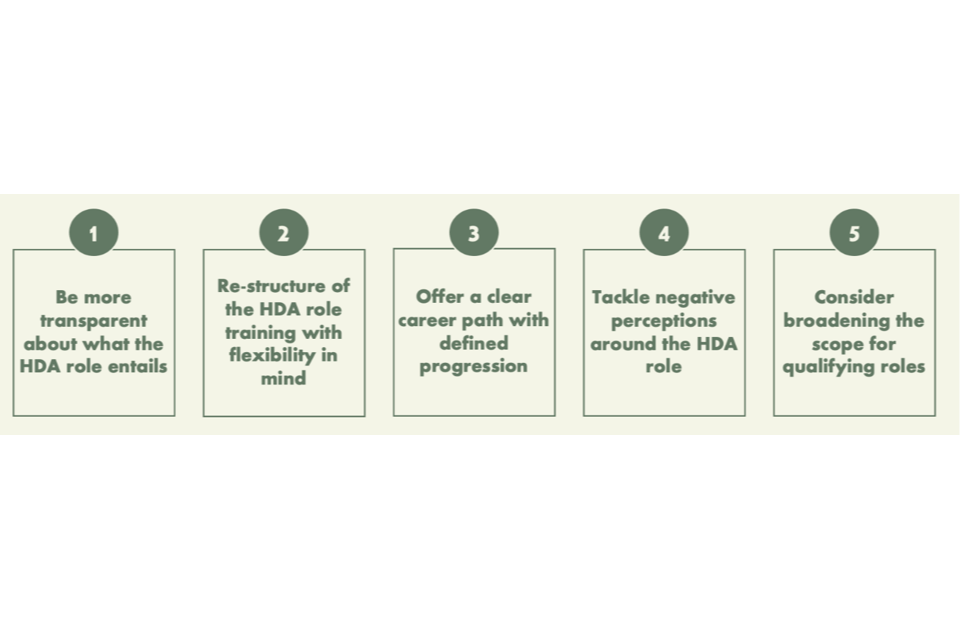
1. Be more transparent about what HDA the role entails
An improvement focussed on communications, more clarity is required so that HCPs feel fully informed about the role, reducing a mismatch of expectations when they start training and progress to being ‘on the job’, around the following areas:
-
The HDA role should be positioned as a new challenge, with quite a steep learning curve and ongoing targets to meet, busting any myth that it is a ‘wind down’ role
-
Recruiters need to be able to transparent and honest about the realities of the role and talk to the core competencies that make a good fit – and crucially be able to be honest if a candidate doesn’t seem right, rather than sending everyone through to the lengthy online competency tests and interview process
-
Focus on the importance of clerical skills and the need for technical proficiency, which are necessary for the use of different IT systems, timely management of data, and report writing. This is a big part of the role, very different to what some HCPs will be used to, and as we will see in the next section on retention is where many new HDAs can stumble and ultimately, leave
-
Provide clarity on how the HDA role differs to an HCP role. HCPs might be uniquely eligible for the role but need to be advised on what the transition to assessor will be like, especially regarding the reframing of patients into customers. HDAs need to be empathetic but must be prepared for the emotional reality of assessing the functional impact of a claimant’s disability, rather than their purpose being to intervene or offer care – and that they will be faced with lots of challenging conversations daily
-
Highlight the demands of the training process. The training can feel very intense due to the amount of learning required over a short period, which new recruits could be better prepared for
-
Utilise personal stories from existing staff to bring all of these elements to life. The use of testimonials (which IAS have started recently) and open days can communicate the human side of the HDA experience, the core competencies required, and the demands and benefits of the role – ultimately helping potential candidates to understand if the role is right for them. The aim here is to improve the quality of the intake, recruiting people who are a better fit for the role, who therefore have the power to ‘go the distance’
There is a reason on there for why people leave and the main reason is around performance and also expectations of the role.
(AP Executive)
We designed this [Recruitment Hub with testimonials]… to give people the opportunity to withdraw themselves from the process so, as they’re going through this they think, ‘actually this isn’t what I thought it was going to be so I’m going to take myself out of this’, so that the ones that we do get through to interview and offer stage, are the ones that we know are, kind of, really committed and very aware of what the role is going to be and I think that we’ve managed to do that. I still think that the one thing we’re not able to fully prepare somebody for is what it’s like being sat in front of a claimant with all of this new learning that you’ve then got to put into practice.
(AP Executive)
I think it can be a bit wishy washy with the disability assessors of where they can progress to what can they do next.
(Recruiter)
As a nurse, every day is different. Speaking to four or five people a day, then writing up a report, that’s how their day is set up. I know everybody is different, but how long I could do that for, you know it it’s quite repetitive.
(Recruiter)
2. Re-structure the HDA role training with flexibility in mind
One of the key barriers to recruitment is the full-time requirement for most training programmes (and in some cases their ongoing employment). Perceived as an ‘easy win’ to attract more candidates who cannot / do not want to work full time, could the structure be reconsidered, for example, offering part time training and delivery, or condensed hours? This could also be positioned as enabling HDAs to keep a hand in medical practice to both provide additional variety and to address any concerns about time away from the profession impacting their ability to return to therapeutic practice.
A flexible training process that might make the onboarding quicker.
(DWP Contract Manager)
Those in DWP Contract Management noted that the lack of being able to offer work from home for WCAs made CHDA less attractive compared to other APs who can facilitate hybrid working – and felt that the technology and mindset regarding flexibility needed to be in keeping with the change seen in post-pandemic working practices. It was noted by both some DWP stakeholders and Assessment Provider Executives that a threat to the recruitment pipeline may arise if there was a shift back to a model where face-to-face assessments would once again become the key mode of delivery. Hybrid working has proven to be very popular (although full time work from home during the pandemic less so) and a key recruitment driver.[footnote 25]
It’s so important to see different channels of assessment offered – but the formal channel mix needs to come from DWP.
(DWP Contract Manager)
If we keep the hybrid model of assessments then it [recruitment] will continue to work fine. If we move forward and it goes primarily to face-to-face then will have to go back to recruiting by geography which will turn all the positive recruitment on head.
(Senior Assessment Executive)
The key factor is allowing for flexibility for hybrid working and not tying them to assessment centres.
(DWP Contract Manager)
The game changer has been home working and the hybrid working approach.
(DWP Contract Manager)
3. Offer a clear career path with defined progression
One of the key elements of best practice retention is making employees feel confident that they have a positive future with an organisation and that this future will offer them opportunities to develop their skills and progress. Building this confidence should start right at the beginning of the recruitment stage, countering the perception that being an HDA is a bit of a ‘dead-end role’:
-
Clarify the softer and alternative skills which can be developed in the HDA role - communication, technical, analytical and report writing skills are layered on to clinical skills, and are a key benefit to other job opportunities outside of the disability assessment context
-
APs should consider how the HDA role might be positioned as a career with progression opportunities. At the time of writing, apart from becoming a quality lead or supervisor, the path does not feel clear - what is the exact scope for widening roles, progressing into management or branching out into other part of the AP organisation (for example, Capita has a very broad scope outside of being a disability assessment provider)? The role would be more attractive to candidates – particularly those at earlier stages of their career - if they could visualise what the HDA role will look like in 3 to 5 years and beyond
-
Provide greater clarity around salaries and ongoing incentives. As established, if in the NHS, HCPs are used to the progressive pay band structure, so can APs clarify opportunities to reach a higher pay band, other than through incentive schemes/overtime? In addition to this, could a loyalty bonus scheme be attached to the role, for example, for 2/3/5 years loyalty, to drive appeal?
It’s easy to notice the skills and attributes in a particular healthcare professional and go yes, you’re the right kind of person to be an auditor let’s say.
(DWP Contract Manager)
Make sure that the upfront messaging means that only the right people want to [become assessors].
(DWP Contract Manager)
4. Tackle negative perceptions around the HDA role
It is undoubtedly a difficult task to rebrand the disability benefits system and assessment service – the negative press goes further than poor online reviews for APs, with a perception that the prevailing sentiment is that the system is unfair and unpopular. However, work can be done (potentially in mainstream or social media) to address myths about disability assessment, that HDAs are not there to take away people’s benefits, but are genuinely there to help them to get the correct level of entitlement based on their restrictions, hence using best possible people to help assess this: HCPs.
Senior stakeholders from APs were passionate about the quality of the service and reported that feedback is consistently collected, evidencing that from the claimant’s perspective the process is largely helpful. Is there also a place in a refreshed communications strategy to give voice to the majority who get the award, and how a good claimant experience can be delivered?
Customers complete customer satisfaction forms and 90% of customers are satisfied…we know that this service is a good service.
(DWP Contract Manager)
As mentioned above, testimonials from existing, experienced HDAs can play a powerful role in illuminating what the role really involves, helping to humanise it. There is broad scope to think about re-branding the HDA profession and a refreshed communications strategy to support recruitment.
The main things [DWP can do] are around the perceptions of the service.
(DWP Contract Manager)
I think we can do more in promoting our support for claimants.
(DWP Contract Manager)
5. Consider broadening the scope for qualifying roles
Is there scope to expand out to other relevant HCP professions, for example, pharmacists and midwives, to help broaden the pool of recruitment in an already hamstrung market?
What you could potentially look at is people that are not necessarily qualified professionally but have got that experience, you know, of being able to triage, you know, cases and kind of point them in the right direction, especially if they’ve got some tools, for example, that will help them do that so I think that there are some opportunities in the very initial stages of when the claims come through to IAS to have a group of non-clinicians, if you like, that can triage the cases to put them into the right queue.
(AP Executive)
Considerations for DWP and Assessment Providers to improve HDA recruitment
Considerations for DWP
-
Agree and formalise HDA core competencies with APs
-
Define assessment channel mix to futureproof a wide catchment for recruitment (and retention)
-
Prioritise a discussion with APs on part-time training and employment (it is understood that this comes under contract negotiations)
-
Consider some simple re-branding activities to reframe the HDA profession supported by a refreshed communications strategy
-
Rationalise and extend the qualifying roles for HDAs across PIP and WCA to help level out the recruitment playing field within the market
Considerations for assessment providers
-
Recalibrate any job specs around agreed HDA core competencies and encourage recruiters to discuss the realities of the role, to help candidates to judge whether they are a genuine or potential fit
-
Empower a more efficient recruitment process by allowing recruiters to do an initial sift based on informal assessment of competency, preventing any unsuitable candidates from going through to the online test stage
-
Position the job as a career, with a clearly defined path and progression, opportunities to broaden out from the role
-
Build the value-add skills in to advertising the benefits of the job, for example, communication, technical, analytical, and writing
-
Work with DWP on executing refreshed communications for the HDA profession
-
Increase the use of the ‘voice of the assessor’ to bring the HDA role to life for potential candidates, helping them to understand both what it needs – and what they can get from it
3. Health and Disability Assessor retention
3.1. Summary of onboarding and approval process
Through discussions with HDAs and senior stakeholders within CHDA and IAS we developed a picture of the training and onboarding that HCPs go through to become approved by the Secretary of State to undertake consultations. The training process appears to be relatively similar across WCA and PIP providers, however these were not the substantive focus of discussions so should be taken as indicative of the training and approval process.
The process is summarised in the ‘summary of HDA training process’ (below) and encompasses four stages, after which HDAs are then on a probationary period before being confirmed fully in post. This process differs in length depending on a range of factors including the qualifications which HCPs enter the process with, whether parts of the process are undertaken part-time or full-time, and how quickly people progress through each stage. In theory it could take as little as 2 to 3 months to be approved but in many cases it is taking six months, and some report instances of 12 to 18 months.
Summary of HDA training process
Stage 1
Stage 1 involves distance learning online learning modules delivered over 3 days to introduce trainee HDAs to the role.
Stage 2
Stage 2 historically involved a training event that was run regularly at a central location. The length of the training varied depending on the level of qualification that the trainee HDAs were coming in with: from 8 working days for qualified doctors through to 18+ working days for general nurses or physios, for example. Following this training there is an open-book MCQ exam. While it was possible to fail at this stage, relatively few HDAs were seen to do so, and training could be sat again.
With COVID-19, all training has moved online and been run remotely. This can involve a mixture of self-directed modules and training from a national pool of trainers. Online training is not yet felt to be as good as that delivered face-to-face as participants miss out on the same level of interaction and peer-to-peer learning as happens face-to-face. While it does incorporate practice role playing with actor claimants, with oversight from trainers, the content has not been fully developed for online delivery. As with face-to-face there is an open-book MCQ exam at the end of the training, and this can be re-sat multiple times if needed.
Stage 3
Stage 3 is where trainee HDAs progress into more of a ‘live’ environment in which they receive 1-2-1 support in managing one live ‘short’ case (simpler and more straightforward claims) per day. Over a period of 8 to 10 working days they are also shadowing a mentor, responding to scenarios, taking part in examinations and consolidating learning. During this time they have to demonstrate the competencies desired from a HDA and provide assurance that they can complete an assessment without supervision and achieve the right outcome. If they are not felt to meet the requirements at this point there can be a three-day extension to this stage.
Senior assessment executives from both CHDA and IAS have recognised that there is a big leap between Stage 2 and Stage 3, a point where trainee HDAs go from role plays to a live environment in which they are constantly being assessed.
Stage 3 is when APs report that there starts to be more significant issues with HCPs dropping out from the approval process due in part to the pressures of the assessment process, but also due to lack of perceived competencies to perform the role.
Stage 4
The final stage in the approval process is to show competency independently undertaking assessments across a mixture of cases, with all cases audited by a Clinical Support Lead. Across approximately 20 cases there is a need for trainee HDAs to achieve four A grades and no more than one B grade in a row. If this is not achieved, then a meeting is held to discuss performance and the trainee HDA is given another 10 cases in which to show improvement. During this period additional support is put in place but if significant improvements are not demonstrated then this can lead to someone being terminated. Only once they are able to demonstrate consistent competency will be put forward for approval.
Stage 4 is the main point at which HCPs are seen to ‘wobble’ and fail because of the increased pressure and weight of expectations. For most trainee HDAs who are leaving at this stage it is because they are unable to demonstrate the consistency of competencies needed.
The majority of the people, 90% of the people who leave the business will be either in Stage Four when they are waiting to be approved or immediately after when the expectation in terms of productivity, the number of assessments per day increases on a regular basis.
(HDA)
As highlighted in Section 3.1., analysis from London Economics revealed that retention of HDAs is a key issue: attrition in the initial training period is exceptionally high, with around 40% of new recruits leaving during 3-month training; and monthly attrition for other staff is also very high at around 3%, suggesting that nearly 40% of the HDA workforce leave each year. This figure looks even more stark in comparison with the NHS, where the comparable annual workforce retention figure is around 10% for nursing staff. This challenging retention context presents a recruitment challenge – as high levels of recruitment are required to consistently replenish the workforce.
3.2. Factors influencing HDAs to remain in role
Senior stakeholders in APs describe a ‘lightbulb moment’ for HDAs, which happens around twelve months - when a certain level of confidence and competence is achieved, where HDAs feel fully settled in and able to cope with the demands of the role. And from a more emotional perspective, once HDAs have undertaken a reasonable amount of assessments they have a greater degree of understanding and appreciation of how their role is supportive of people, albeit in a different way to an HCP.
I think when you understand it more, it’s really about making sure people have the right kind of support.
(HDA)
The HDAs who were part of the qualitative research sample were well placed to describe their motivations for staying, all having been in their roles for more than a year. Those who find the job engaging enjoy speaking to people and are positive about the assessment channel mix, providing variety in their role – with the recent increase in face-to-face assessments being a welcome shift from 100% telephone during the pandemic.
I enjoy learning about different conditions – you need do your research; it keeps you on your toes…there’s always something you don’t know.
(HDA)
The assessment centre is only ten minutes from my house…so that works for me – I enjoy doing the face-to face assessments more.
(HDA)
From a support perspective, they feel they have the right amount to succeed in their job, with great relationships with their teams and immediate colleagues and management who are supportive of their clinical judgement and readily available to talk through problems. They speak positively of receiving ongoing clinical training and helpful feedback from quality leads, providing feedback on what they have done well, as well as where they need to improve. HDAs across APs describe a recent increase in ‘buddy’ (peer) support for new starters, once their training periods have finished. HDAs also report that their feedback on issues with assessment process has been listened to, and welcome the increase in peer-to-peer support via Teams channels during remote working.
Some HDAs feel that career progression is clear and available to them, with the ability to become a quality lead providing the stretch and direction they desire, or opportunities to carry out other roles and responsibilities such as file work or mentoring other HDAs.
I have really good friendships here, with CSL and colleagues.
(HDA)
3.3. Challenges for retention
It is important to note that no former HDAs were interviewed as part of the qualitative research. However, a strong and consistent view of the reasons for leaving was gained from those HDAs who have experienced colleagues leaving, senior AP stakeholders who oversee areas such as ‘people’ and engagement’, and recruiters who have received feedback from HDAs they have placed who leave their roles.
3.3.1. Mismatch of perceptions / expectations around the role
The qualitative feedback pointed to this as a key retention challenge, however, as explored in Section 2.6.2 the issue is rooted in ‘recruitment’: that candidates do not get a clear enough picture of the HDA role during the recruitment process.
Two key themes are evident:
1. A realisation that the HDA role is not a ‘wind-down’ or ‘easy’ option after healthcare
This challenge tends to happen over two distinct waves in the first 12 months of the role: first during the training and onboarding process (covered in more detail in Section 3.3.3. below); and then when HDAs become qualified and start to manage their caseload themselves. The key issue is that many HCPs looking to step away from the stress of their healthcare role, expect the ‘desk-based’ and ‘9 to 5’ nature of the HDA role to be much easier and more relaxed, when in fact there is a focus on targets and the requirement for a high degree of focus, discipline and clerical skills needed to achieve the required output within a 9 to 5 day.
Reason for leaving is around performance and around different expectations for role. Can think it is a nice wind down role from being in a busy environment. While the environment is like that the job is challenging.
(Senior stakeholder – AP)
The clerical nature of the role implies an ability to carry out assessments over the phone and in person; record lots of information about a claimant at speed, while simultaneously assessing them; and then to analyse and calibrate that information into a report – with the expectation that this should be done for three assessments per day. Some HDAs experience stress and anxiety with this shift from a role that uses their clinical and care skills, to a role which requires more in the way of clerical and interpersonal skills. Reportedly, HDAs have an under-appreciation of amount of administration and writing involved in the job, and this impacts how they manage their time, with those who leave claiming they are unable to do the job in the hours they have to do it. The material impact of this is that what may have looked like a more financially attractive proposition than their HCP role can become less-well paid when aggregated over the number of hours worked – which is made starker when coming from a job environment where overtime is paid reasonably well (for example, on ‘bank’ shifts).
It’s a misrepresentation of the hours, I hear tales of them working 60 hour weeks and working weekends to catch up on writing 4000 word reports.
(Recruiter)
They [HDAs who leave] just can’t keep up with the demands of the job.
(HDA)
It is a LOT of writing.
(HDA)
A big contributing factor here is how adept an HDA is with technology. The role requires a lot of online training and communication, and use of systems and programmes to carry out tasks. As they have been more used care-focussed and less tech-reliant mode of delivery as an HCP this shift can cause some to struggle, if not naturally tech savvy – an issue that was reported to be more acute for those HDAs who were at a later stage in their career, where technology had not played a key role in their day-to-day.
In addition to the everyday demands of the role, there is also a requirement for ongoing CPD which is not factored into the working week. For IAS this is one hour of CPD a month, plus the ‘my learning journey’ online programme, an expectation to listen to clinical podcasts, and whenever HDAs feel they need to do deeper research into conditions they are not so familiar with.
2. An expectation that because they have been recruited for their clinical skills, the HDA role will be like that of an HCP
Similarly, at the recruitment stage, the key differences between the roles do not seem to be communicated. HCPs have a care focus, however, the nature of the HDA role is quite different. While requiring that an HDA be empathetic and use their clinical skills to assess claimants, the output is to decide on the level of functional impact of their physical/mental restrictions and then move on to the next case. From an emotional perspective this can be very challenging for people who are trained in caregiving to adapt to.
A teacher goes through teacher training, lands in the classroom and decides they don’t like kids…it’s the same here.
(DWP Contract Manager)
I don’t deal well with conflict or complaints…when I get a complaint I take it heart – they tend to be the claimants who don’t get the benefit.
(HDA)
Most HCPs who become HDAs are used to being part of a big team with lots of variety in the work they do. The HDA assessment process, despite providing some variety in the types of claimant conditions they see, is very repetitive as a process. The job can also be isolating, as the process requires the HDA to work independently (they may be part of a team and consult with colleagues, but the assessment and report side must be conducted individually). Naturally, this isolation was exacerbated for those who were doing purely telephone assessments during the COVID-19 pandemic, especially if homeworking was the only option with the assessment provider they worked for.
The idea that they would want to be on a treadmill of collecting details but not intervening is alien to a significant proportion of the health sector. A lot of people that apply for roles don’t understand this point. They arrive, then have rigorous training and the penny drops that this is what role is.
(DWP Contract Manager)
Other operational differences to the HCP role can have a negative impact on perceptions of the HDA role, namely the use of target-setting and audit feedback. The commercial contracts held between APs and DWP necessitate a certain level of productivity and quality in output, to ensure a good service is being provided to the ‘customers’ who access the PIP and ESA/UC benefits system. HCPs are not as used to working to defined productivity targets, rather the ad hoc nature of healthcare, defined by individual needs, and can find this switch cognitively challenging. In addition, even after the training and onboarding is completed, the audit process remains central to the work, requiring a personal resilience for absorbing and acting on feedback. And it is the case that issues arise when some newly qualified HDAs, who may have performed well in the earlier stages of training, start to become audited.
They can’t keep up with the workload - lots of pressure. It is a tough role, lot of info, it’s regimented and strict very different environment verses what they are used to.
(Recruiter)
In an NHS nurse role, get what is expected from you…people don’t realise it is gonna be different from the NHS.
(HDA)
It’s a job you always feel a little bit insecure in because it’s a very feedback heavy role and you get a lot of negatives and when you’re used to being a clinician you get a lot of positive stuff all of the time from your patients.
(HDA)
3.3.2. HDAs experience specific issues with the assessment process
Qualitative feedback highlights that HCPs are used to feeling highly confident in their skills and competent to deliver in their specific healthcare roles. The differences to the HDA role and the sense of ‘starting over’ is reported to ‘knock their confidence’, with elements of the assessment process presenting specific challenges.
The new challenge of the clerical nature of the role has already been established, but digging a bit deeper into this, feedback from senior stakeholders at APs suggests that some HDAs lack interest in writing the ‘justifications’ in their reports. They lack a sense of self efficacy in making justifications against the assessment criteria, as the judgement required for this is not the same as making a medical diagnosis (for instance, the evidence and decision is more subjective). In addition to this, they need to be highly self-directed in their role, needing to actively ask for help from quality leads and supervisors when they need it.
They’re learning this whole new skill set around…sort of, report writing and probing of questions and how to pull that information out but then without having the responsibility of an outcome of that.
(Senior stakeholder – AP)
From a channel perspective, some HCPs can struggle to keep questions sharp during telephone assessments, due to the lack of visual cues to direct a conversation, impacting productivity.
It’s much more detective-based than it would be if its face-to-face. I have to use my judgement on what to ask for more information on and I want to be thorough, so it ends up taking longer.
(HDA)
The assessment process can also be a stressful and exhausting experience, listening to the most negative elements of people’s lives on an ongoing basis. It is reported to be emotionally taxing, not being able to offer support or to ‘fix’ people.
You’ll see a 16 year old boy with a stoma bag – but as he can do crutches he won’t get the mobility part [of the benefit criteria] …I don’t like this part of the job.
(HDA)
The ongoing need for emotional resilience, cognitive focus and flexibility of approach are reported to leave HCPs feeling fatigued with the assessment process.
[I imagine] they can feel like all day-counsellor.
(DWP Contract Manager)
3.3.3. Training and onboarding are long, highly pressurised processes
Anecdotal qualitative feedback from senior stakeholders in IAS is that overall HDA attrition is around 3% per month (similar to that in London Economics analyses), with 30 to 50 HDAs leaving their posts. However, 50% of assessors leave within first six months of joining. This is when they are still either going through the approval process or newly approved and therefore still learning the role (and where their previous role is still a live option to return to).
If you have 12 on training, you are lucky if you see 3/4 past the first 3 months on the job.
(Recruiter)
At first this job is really difficult. Initially, every day is a bad day, then slowly…you find that the good days become the majority.
(HDA)
Becoming a qualified HDA requires an intensive and lengthy training process, and there is no guarantee of a job at the end as this is dependent on approval. There is a significant full-time commitment required, and four different stages to complete before becoming approved. HDAs reported needing to do a lot of revision outside of set training hours and that this was an exhausting and highly stressful process. Due to COVID-19 the initial training moved from face-to-face to online, upping the intensity for new joiners having to learn remotely by themselves and feeling a lack of tangible support. Even when delivered face-to-face, trainee HDAs had to travel considerable distances to training centres, meaning travel there and back over weekends and lots of time away from their families. The time commitment required is significant.
That’s what put me off initially…lots of revising – and doing that outside of training hours, staying away from home, and knowing you had to do roleplay assessment at the end of the week…also 6-8 hours to travel for the weekend home.
(HDA)
Aside from the time commitment and intensity of learning requirements, a large part of the training is continuous assessment and auditing, where trainees can feel a lack of confidence in their capability, and progress undermined. This is especially challenging when they are coming from an environment where they are skilled, trained, competent and confident - they are not used to ‘failing’, not used to the same level of scrutiny and possibly less accepting of critical feedback. Exacerbating the feedback issue is that there is seemingly no consistency, with each claimant case that is audited presenting with different conditions and circumstances, making it very difficult to assess impact on functioning consistently.
The main points at which HCPs undergoing training begin to leave the process is during Stages Three and Four, when their cases and practices are consistently audited. This is the point at which trainee HDAs begin to be formally assessed and where judgements are made around their competencies, after already having been involved in between two and four weeks of training. As referenced in the earlier economic analyses, many HCPs were seen to leave the process at this point due to the pressure of being audited and not being able to demonstrate a consistently high level of competency in their assessments. The feedback from senior executives at the APs and DWP Contract Managers is that this level of pressure makes trainee HDAs nervous and to question their decision to take on a role as an HDA. This at a time where alternative roles within the NHS, often comparatively well paid, are available for them to return to.
They cannot cope with the pressure of the job being on the line every 10 cases because let’s not forget, if you don’t get it within 20 cases, every 10 cases your manager will be on your door and say ‘you haven’t achieved approval, I don’t see any improvements in the grades, we’ve put a lot of work in to this to support you’, okay, the procedure prompts them to get in touch with the HR business partner and say we cannot keep them in the business.
(HDA)
I think the approval process is definitely the crux of it because that is where we do see people leaving and that is in the front office space and in the back-office space so this is something across both areas that the HPs find really, really challenging. And you know I don’t know what the magic recipe is to change that. I genuinely don’t because I think you can’t bad mark every HP that comes through the business, hand hold them to a degree where it is absolutely unfeasible, and you know. But that is where people fold, 100%.
(DWP Contract Manager)
3.3.4. Once trained, HDAs start to lack a sense of variety in their role, and become concerned about career progression
As noted in the Section 2.6., offering ‘clear career progression with opportunities to move within the organisation to expand skills and experience’ are a key part of best practice for the successful retention of staff. At the time of writing, health assessment can feel limiting in terms of the variety the role provides, and in terms of future progression.
In their former healthcare roles, HCPs are used to working within a sector where there is huge variety of different opportunities to use and develop their clinical skills. And that sense of variation is mirrored in their ‘day-to-day’ where they will often see different types of cases and be called to be creative in their approach. Even though each claimant’s situation will be unique, the assessment and reporting process is fixed, with a prescribed set of criteria determining the outcome.
In terms of progression, it has already been noted that those HCPs who worked in the NHS will be used to the progression of the grade and pay band structure, offering a clear, if not somewhat prescribed, path. In contrast the HDA role appears to offer very limited progression opportunities and can be perceived as a dead end in terms of their career. While this may be less of an issue for those in the latter stages of their working lives who may be looking to retire, this is described as unappealing for younger people who want to see a career offering a bright and challenging future.
A lot of people will go back to their previous roles. It’s a vulnerable time as there is a huge demand for HCPs.
(Senior stakeholder – Assessment provider)
There’s a high demand for their skills…and [healthcare] offers them that familiar culture they are used to – also if they are out of it for too long, they lose their right to work.
(Recruiter)
Most interviewees highlighted that the HDA role, in the absence of additional responsibilities, was one which had a very limited “shelf life”, and that realistically there was an expectation that people would only perform it for 2 to 3 years before they get fatigued and move on. The important thing for contract providers is to look at what additional responsibilities or progression opportunities could help to increase this length of service.
There’s a shelf life for assessors…there’s a smaller number who have been there for many years.
(DWP Contract Manager)
COVID has opened that [variation] up with [different] channels but ultimately it’s a defined role.
(DWP Contract Manager)
3.3.5. There is always a ‘way out’
Qualitative feedback from the various groups of participants noted the vulnerability of the health assessment market due to the consistently huge demand for HCPs, recently exacerbated by the COVID-19 pandemic and impact of Brexit. Due to demand, and the fact that healthcare is their familiar territory, HCPs have an awareness that there is a job waiting for them if being an HDA doesn’t work out. This draw back to what they know is reported to happen at three key points:
-
Early in the training process if it is deemed to be too challenging
-
After they qualify and realise that the day-to-day doesn’t live up to their expectations
-
Around the two-year mark when HDAs they feel that the job has run its course. It is not a co-incidence that this two-year mark is also the limit for an HCP to be out of clinical practice before they lose their licence.
Another minor factor in retention is dictated by market structure, consisting of multiple APs. It is noted by AP’s that competition between providers drives HDA movement, as HDAs are aware that they can essentially do the same job but receive a small salary increase by moving.
Some leave because, you know, their heart, actually they realise their heart belongs back in whatever they were doing before.
(DWP Contract Manager)
When people have options they tend to move.
(DWP Contract Manager)
WCA is struggling a bit more and some people are jumping ship.
(DWP Contract Manager)
If at point where feeling confidence has been knocked due to new role then easiest thing is they go back to what they know. Feel just not going to get it.
(Senior stakeholder – AP)
3.4. Actions taken to address retention
Senior assessment executives and more experienced HDAs with remits that went beyond the core role of completing assessments were all exceedingly positive toward the relationship with DWP. There was a view that there existed a spirit of collaboration between DWP and the contracted providers, with a key focus being addressing the recruitment and retention issues to help also address a backlog of assessments. While it was not possible to get an exhaustive picture of the range of actions being taken to address retention issues, we were able to identify some of the actions being taken at the time, some of which required changes sanctioned by DWP, and others which were more internally driven and focussed.
There have been a number of changes to the assessment processes themselves, including the move from requiring HDAs to complete four PIP assessments per day down to three and removing the need to summarise all evidence (relevant and irrelevant) submitted with claims. These changes have helped to reduce the time pressures on HDAs, enabling more work to be completed within the core working hours. There have also been changes put in place to enable the piloting of WCA assessments to be undertaken remotely, enabling HDAs to work at home rather than in a centralised setting. This in turn was seen to be helpful both in increasing scope for recruitment but also providing staff with more flexibility, encouraging retention.
Outside of these changes DWP Contract Managers interviewed as part of this research felt there was little more that could be done to alter processes further without wholesale transformation. The issue was seen as more to do with the high levels of demand for the benefits as opposed to the service itself.
My view is there are limited opportunities unless they are transformational.
(DWP Contract Manager)
We can’t be making wholesale changes at this point.
(DWP Contract Manager)
In addition to the above changes, individual contract providers were themselves putting in place a wide range of support measures to try and improve retention, largely focusing on trying to establish a culture of learning and coaching. These variously included:
-
high levels of internal scrutiny and analysis over HDA performance to identify individuals that are struggling and to put in place personalised support packages (with a focus on coaching and supporting) to help promote retention. This has included the production of a retention toolkit for managers to use in supporting conversations with trainee HDAs
-
piloting ‘soft’ Stages 3 and 4 where additional time is factored into the run-up to Stages 3 and 4 to aid the transition between stages. This includes extra days with a Clinical Support Lead where trainee HDAs can go through some of the elements that they most struggle with (largely descriptors, risk and procedural issues (for instance, unexpected findings)), and trial case audits which don’t count toward the final assessments
-
increased ‘buddy support’ for those that have finished their training
-
offering opportunities for HDAs to take on additional responsibilities, for example, file work, mentoring, and taking customer advice calls
-
internal colleague-led feedback loop so when HDAs do leave that learnings are shared to help address issues going forward
I think there’s something that we can do in that nought to six months space that just makes it feel easier…then I think we’ll stop a lot of attrition because once people get into this role they really, really enjoy it.
(Senior Stakeholder – AP)
While all stakeholders spoken to within the contracted providers reported that more could and was being done to understanding individual priorities and tailoring the work environment to these, HDAs were also largely very positive about the support that they were able to access in their organisation.
3.5. Best practices
Underpinning retention is the requirement to understand an employee’s needs from a job, and when those needs are identified, retention activities can be crafted to support them. In ‘The courage of compassion’, The Kings Fund identified three core needs to help nurses flourish and thrive at work:
1. autonomy – the need to have control over their work lives, and to be able to act consistently with their values
2. belonging – the need to be connected to, cared for, and caring of others around them at work, and to feel valued, respected and supported
3. contribution – the need to experience effectiveness in what they do and deliver valued outcomes[footnote 26]
In ‘Caring for doctors, caring for patients’ a similar set of needs were also identified (although ‘contribution’ was swapped out for ‘competence’, with a similar intention) to ensure wellbeing and motivation at work, and to minimize workplace stress.[footnote 27]
When thinking about retention, it is worth expanding briefly on the increasing prioritization of employees’ health and wellbeing at work, the focus on which has been accelerated by pressures and changes to work practices attributed to the COVID-19 pandemic. Much of the evidence centralises the prioritisation of health and wellbeing as essential to retaining employees, with a wealth of best practice available from various organisational strategies (please see examples in the following pages and in Annex A). It is interesting that health and wellbeing seems to be a collective outcome of various retention principles, for example, being recognised and rewarded, access to learning and development opportunities, working in a compassionate and inclusive environment and having a voice and way to influence. CIPD explains that investing in employee wellbeing can lead to increased resilience, better employee engagement, reduced sickness absence and higher performance and productivity.[footnote 28] In CIPD’s Resourcing and Talent Planning Survey, it is reported that, in 2020 the top step by organisations taken to improve employee retention was “improved support for employee wellbeing” (57%) with the next highest steps, arguably influencing wellbeing, being: improving work–life balance (49%), introducing/enhancing flexible working options (48%), and improving support for homeworkers (43%).
Below is a summary of core principles of a successful retention strategy, synthesised from evidence drawn from a range of sources, including:
-
Improving staff retention’ (NHS Employers)[footnote 29]
-
‘Top tips for retention’ – A briefing for adult social care providers’[footnote 30]
-
‘Recruitment and retention: Secrets of success’ (skills for care)[footnote 31]
-
‘NHS People Promise’[footnote 32]
-
‘Wellbeing at work’ (CIPD)[footnote 33]
Core principles of a successful retention strategy
- Good work/life balance
- Flexible working (part-time, flexible hours)
- Fair reward and attractive overall remuneration package
- A culture of health and wellbeing (with initiatives that staff have consulted on)
- Compassionate and nurturing leadership
- A safe, inclusive culture that champions diversity
- Clear career progression with opportunities to move within the organisation to expand skills and experience
- Investment in flexible training and staff development, with opportunities for mentorship
- Mechanisms for staff voices to be heard – opportunities to influence culture, processes, and decisions (for example, staff surveys, routes for ongoing staff feedback)
- Strong company and brand values
- Recognition of staff efforts and achievements, for example, shared praise or celebration
- Understanding the needs of the workforce and why people leave (conducting ‘stay interviews’ can help spot the signs of leavers before they go)
A wealth of case studies exist across the NHS and the public sector, bringing to life how organisations’ best practice around retention, measure their success, and learn from the experience. However, some remain as ‘work in progress’ examples. Below are some selected examples to bring some of the core principles of successful retention to life, with more case studies available in Appendix B.
An overarching people strategy: The NHS People Plan 2020/2021 and People Promise[footnote 34]
The strapline of the NHS People Plan 2020/2021 is ‘More people, working differently, in a compassionate and inclusive culture’, and seeks to build the resilience of a fragile and exhausted NHS. A broad range of actions and commitments to staff, to be disseminated through the national network of Integrated Care Systems, are organised around four pillars:
-
looking after our people – with quality health and wellbeing support for everyone
-
belonging in the NHS – with a particular focus on tackling the discrimination that some staff face
-
new ways of working and delivering care – making effective use of the full range of our people’s skills and experience
-
growing for the future – how we recruit and keep our people, and welcome back colleagues who want to return.
The People Promise is an interesting commitment to enacting the plan, based around seven promise pillars, very much aligned to the core principles of successful retention identified above. In reference to principle number 9 and 12 above, the People Promise was developed through consultation with those who work in the NHS. People in different healthcare roles and organisations were asked what matters most to them, and what would make the greatest difference in improving their experience in the workplace. The annual NHS Staff Survey is to be realigned to map to the seven components of the promise, and metrics put in place to evaluate progress and performance across these components.
The People Promise and the promise pillars.
The ‘NHS People Plan’ and ‘People Promise’ are interesting examples of best practice, as they encapsulate a broad-ranging retention strategy where staff consultation is the central feature, and their needs developed into a strong commitment – the ‘promise’. This use of a promise is more engaging and emotive than a simple set of retention principles and actions. Most importantly, a promise speaks to accountability – as it must be delivered. However, since this is a new strategy, data from subsequent NHS Staff Surveys will bear out the success of its implementation across the NHS.
The Education Staff Wellbeing Charter 2021: Department for Education (DfE)[footnote 36]
Focussing on the importance of staff wellbeing, the Education Staff Wellbeing Charter commits DfE, Ofsted and schools, colleges or academy trusts to sign up to a two-way charter on staff wellbeing. The DfE make improved wellbeing among staff a key outcome for education policy, describing staff as a ‘precious resource’ and describing a duty to valuing them, their wellbeing and mental health.
The charter defines wellbeing as “A state of complete physical and mental health that is characterised by high-quality social relationships”. In it, DfE makes nine policy commitments to support staff wellbeing; Ofsted describes its three commitments; and educational organisations are asked to sign up to 11 commitments to their staff. Measurement of and accountability for staff wellbeing is a key part of the charter. In addition, the charter is supported by a set of ‘principles of shared understanding’ around wellbeing.
National GP Retention scheme[footnote 37]
With a focus on flexible working and understanding the needs of doctors at various life-stages, the National GP Retention scheme is aimed at doctors who are seriously considering leaving or have left general practice due to personal reasons (caring responsibilities or personal illness), approaching retirement or requiring greater flexibility due to family or career needs. The scheme enables doctors to do a maximum of four sessions per week and still be a doctor. As an RGP (retained GP), the doctor gets more flexibility and educational support than they would in a ‘regular’ salaried GP post. The scheme gives financial support to both the RGP and the practice employing them, for the fact that the role differs from ‘regular’ part-time posts.
3.6. Opportunities for improving retention
Before focussing on opportunities to improve retention of HDAs, a qualitative assessment of ‘how we are doing’ against the core principles of best practice retention highlights key areas that require consideration:
Performance against core principles of best practice
| Feature of ‘best practice’ retention | Performance [footnote 38] | Rationale for performance rating |
|---|---|---|
| Good work/life balance | Average | Work/life balance is impacted by the cognitive and clerical demands of assessment targets and report writing, with some HDAs needing to spend extra time outside of allotted 9 to 5 |
| Flexible working (part-time, flexible hours) | Requires improvement | Although hybrid working is offered by IAS and Capita, an issue is the narrowly defined (and outdated) perception that the HDA role requires a full time, 9 to 5 commitment – narrowing the market for recruitment and impacting ability to retain talent |
| Fair reward and attractive overall remuneration package | Average | Although salaries are relatively attractive, this is impacted by the perception of working ‘unpaid overtime’ due to the administrative and clerical demands of the job - a challenge when many HCPs can be used to well-paid overtime shifts |
| A culture of health and wellbeing | Average | Not cited as a key issue during the qualitative research. The assessment process does have an impact on mental health, which HDAs can find stressful and upsetting. Although there are reports from existing HDAs of good camaraderie within teams, which should be noted as a positive |
| Compassionate and nurturing leadership | Average | Reports of feedback being listened to and acted on by leadership, although some perception that non-clinical leadership lack an appreciation for some of the complexities of the assessment process (around people and their conditions), with too strong a focus on commercial targets |
| A safe, inclusive culture that champions diversity | N/A | Not cited in the research as an issue / asset |
| Clear career progression with opportunities to move within the organisation to expand skills and experience | Requires improvement | Distinct issues around role variety and career progression to be addressed to improve retention |
| Investment in flexible training and staff development, with opportunities for mentorship | Requires improvement | Distinct issues around role variety and career progression to be addressed to improve retention |
| Mechanisms for staff voices to be heard – opportunities to influence culture, processes, and decisions | Good | Reported as working well (although the caveat is that this is the perception of existing HDAs who have stayed in their role, and AP’s) |
| Strong company and brand values | Requires improvement | Clear ‘category issue’ around the perception of the disability benefit system and assessment service. This arguably effects recruitment into the HDA role more, but a strong and emotive sense of purpose around the assessment process as one that is helping the most vulnerable could help to retain HCPs in the role |
| Recognition of staff efforts and achievements | N/A | Not cited in the research as an issue or asset outside of salary and benefits package |
| Understanding the needs of the workforce and why people leave | Good | Being explored in depth in this programme of DWP health transformation research to understand and address key issues at the time of writing |
The research suggests that there is a strong connection between the optimisation of recruitment and retention, neither of which can be considered in isolation when building a future workforce strategy. Four key areas are evident in relation to improving retention:
1. Good recruitment is fundamental to retention
An in-depth understanding of what the HDA role entails and whether a potential employee will fit (regarding competency) can be most effectively managed at the recruitment stage, as explored fully in Section 3.8. In summary, a clearer representation of a typical day or week for a disability assessor, brought to life by HDA testimonials, is crucial to manage expectations. Detailed competency questions, zeroing in on clerical and technical skills, will help to screen out people that will struggle to complete volume of assessments required and those that may not have the resilience for continuous feedback and the emotional demands of dealing with claimants’ needs and issues on a daily basis.
2. Consider where support is most needed – and how feedback is delivered
A high-level of support is required by those in the training process, and must temper the ongoing nature of audit feedback, which can undermine confidence and sense of competency when learning a range of new skills, at speed. This has been hampered by the need to conduct training online, increasing trainees’ sense of isolation in the process. Peer-to-peer training and support can help engage and empower trainees, reducing isolation during a stressful time, but overall, knowing that there is mentorship and a strong sense of support from ‘day 1’ is key, especially when the initial stages of engaging with the role are online.
When trainees reach Stage 4 and must achieve a minimum four grade As and one grade B in a row of five assessments, this is a highly daunting moment, with qualification hanging in the balance. This is when the highest level of support is required, giving trainees the confidence to get ‘over the line’, however is there scope to reduce the demand of this stage, with the awareness that fear and anxiety are amplified by the need for five high grades in succession?
Audit feedback is a clear issue impacting HDA’s perception of the role, feeding into retention; how frequently it is delivered, how varied it can be, and the capacity for new trainees - as well as those who are qualified - to receive it positively and act on it. Perhaps there is room to reframe the necessary task of auditing as a ‘safety net’ for HDAs, helping them to ensure quality, rather than feeling like a punitive activity, as it seems to be perceived at the time of writing?
Given the high level of feedback HDAs must absorb and the need for support as trainees and post-qualification, Clinical Support Leads must have their time protected to provide continued point of support and mentoring to HCPs going through the process. In addition to this, what scope is there to offer tailored support to individual needs if, for example, tech, typing, or report-writing skills are clear areas for development, could there be specific programmes to target and boost performance in these areas?
People failed within the first week and were asked to leave the company… they had just left HCP roles for this… it unnerved me for months.
(HDA)
Amendments are really challenging and really hard to get your head around… that is where I could’ve done with more support.
(HDA)
3. Job variety and career progression can tackle the ‘shelf life’ of the HDA role
A sense of stretch and challenge need to be built into the existing HDA role to extend its potential as a career. This can be achieved both internally within providers and offering flexibility in how employees work. Within the assessment provider, is there potential for HDAs to take on other tasks and responsibilities alongside assessments, for example, include file work, mentoring, advice calls? From an external perspective, if HDAs were able to work more flexibly (part-time or condensed hours) they could possibly ‘keep their hand in’ clinical practice, doing freelance or bank shifts? This could enable them to maintain their clinical skills, prevent the feeling they have gone ‘all in’ in a job that is so different from their calling as an HCP, and obviate the need to leave after two years due to concern about losing their licence.
Strategy around career progression must consider pathways for employees based on their competencies and interests, with some consideration of ‘what next’ after the HDA role (also key to communicate this during the recruitment stage). And including employees in this conversation – understanding what they would like to do - will help to increase their engagement.
Finally, could there be increased financial recognition for HDAs who have been in post for a while, for example, two years and five years, also serving to provide a sense of progression. Anecdotally, research feedback suggests that those who have been in post for a while are often getting paid less than new entrants despite having broader range of responsibilities.
So long as the opportunities are there I’m more than happy [to stay].
(HDA)
Maximus are a massive company - could there be progression through wider company and subsidiaries?
(DWP contract Manager)
Can [HDAs] feed in to shaping the future of the profession? That helps them see what’s coming next.
(DWP contract Manager)
4. A flexible approach to work can provide autonomy and a better work/life balance
Research feedback has established that the hybrid working model is a key motivator for HCPs looking for a role that will improve their work/life balance, and retaining the opportunity to work from home is critical for ongoing retention. It may be helpful to establish a provider-wide delivery model to even out competition for roles, allowing for the assessment channel mix can be tailored to the workforce in certain areas and potentially incentivising working from a central location.
If that [WFH] changed I’ll rethink my job options.
(HDA)
There’s the potential to move to 70% telephony, 20% face-to-face and 10% video for each assessor. If we could recruit into areas but use those areas as just telephony assessors - telephony or video – this would be a massive win… People might be willing to travel in to work as it would only be for 20% [of their time].
(DWP Contract Manager)
Considerations for DWP and Assessment providers to improve HDA retention
Considerations for DWP
-
Formalise a joined-up recruitment and retention strategy that identifies activities which are necessary to boost both areas
-
Discuss refinement of recruitment process with APs to ensure competency and role fit is achieved
-
Consider parameters for qualification as an HDA, can these be recalibrated to make the training process more manageable?
-
Work with APs to understand stretch and progression opportunities after being an HDA, what can DWP do to help this process?
-
Make long-service bonuses part of the remuneration conversation with contractors
-
Prioritise flexible working as part of ongoing contractor discussions, as it is vital to sure up retention
Considerations for assessment providers
The above DWP considerations are also key for APs, but internal assessment provider consideration needs to be given to the training and auditing process to reduce anxiety and negative perceptions. It is understood that more attention is being paid to this area, however progress must be continuously monitored, with employees engaged to understand what is working/not and where more support is required.
4. Discussion and conclusions
The size of the health and disability benefit assessor (HDA) workforce is not sufficient for meeting the assessment targets of PIP and WCA at the time of writing. DWP commissioned this research to obtain insight into barriers to the recruitment and retention of HDAs. What we found through this process was that the pipeline of new HDA recruits has been shored up – at least for IAS and Capita - over the course of the last 12 to 18 months, in part because COVID-19 has led to many HCPs working in the national health service to seek alternative roles, but also because COVID-19 has led to the opportunity to deliver the HDA role remotely (at least for PIP assessments). This means that contract providers (most notably IAS and Capita) have had a healthier quantity of HCPs progressing through their training process than in previous years. However while recruitment has been bolstered in the short-term the real issue for contract providers is the high rates of attrition: over 50% in 2021. Approximately two-in-five trainee HDAs leave during the training period (which itself lasts approximately 3 months). A huge amount of investment is made in the training and onboarding of individuals who leave the profession within 6 to 24 months, if not sooner.
The issues with retention are bound up with recruitment. HDAs are recruited from a relatively narrow pool of HCPs who qualify to perform the role. While HCPs bring with them clinical skills that are relevant to deliver health and disability benefit assessments, there are also a range of other skills that are not necessarily present, notably those relating to clerical and administrative skills. There is also a very different working environment moving from the variety offered by inter-disciplinary team-based therapeutic care to independently managing a rigorous and repetitive assessment process. At the time of writing, there is insufficient clarity during the recruitment process as to what the HDA role involves, who it is best suited to, and what the progression opportunities are within contract providers. As a result HCPs can both struggle to complete the training process, and those that are approved into a HDA role can find the repetitive and bounded nature of the role wears them down relatively quickly.
Sitting alongside this lack of adequate expectation setting is a training and approval process which is both lengthy, largely excluding of those wanting or needing to work part time, and which is experienced as a relatively punitive and stressful experience. The initial stages of training are not seen to adequately prepare trainee HDAs for the reality of conducting real assessments during Stages 3 and 4 of the training process, or the level of scrutiny that they will come under in assessing how disabilities impact an individual’s functioning. Again it is worth reinforcing how massive the shift that HCPs experience in transitioning into performing a HDA role within these conditions – from being a highly trained practitioner of therapeutic care where judgements were respected into a role where decisions (based on evidence perceived to be highly subjective) were scrutinised against some objective reality that trainees could find hard to grasp.
Once in role HDAs are required to achieve targets of 3 (PIP) or 5 (WCA) assessments per day; if not sufficiently efficient in typing reports quickly and accurately it can be difficult to meet targets within the core working hours, meaning unpaid overtime can be more common than was expected. The reality of the role for many people is one which is quite repetitious, and due to the nature of the conversations, has the potential to be emotionally draining. The repetitive nature of the role and the lack of diversity of tasks or opportunities for progression mean that some HDAs can become frustrated relatively quickly, especially if they are earlier in their careers.
That there is an expected 2 to 3 year ‘shelf-life’ for an HDA is telling and directly linked to the issues identified here by all stakeholder groups.
Many HCPs leaving HDA roles were reported to have returned into therapeutic practice, taking advantage of their networks and knowledge of the health system. Because expectations of both the training and the role do not always align with experience – both of a relatively stressful and intensive training process, and the repetition, emotional toll and administrative requirements in delivering assessments - this helps contribute toward a situation where there are (seemingly) constant vacancies and the role is not held in much esteem.
On the basis of this research the barriers to recruitment and retention appear to be that:
-
HCP motivations and expectations don’t align with their experiences of the HDA role
-
the HDA training process is seen to be overly onerous
-
the HDA role is limited in scope and limiting HDAs sense of satisfaction or progression in their employment
From the documentary evidence it was noticeable that as well as recruitment and retention going ‘hand in hand’ to create a resilient workforce, a defined workforce planning strategy provides the foundation for most other activities concerned with acquiring, developing, and deploying people. Workforce planning is a core business process which aligns changing organisation needs with people strategy and is considered to be one of the most effective activities an organisation can engage in.
There is clearly a lot of work that has taken place to improve the experience of HDAs both from DWP and from contracted providers. This ranges from substantive changes to the assessment process through to marketing initiatives that are directed at a more informed pipeline of HDA recruits and processes to personalise support for HDA trainees. Question marks were raised at what more could be done, in particular from the perspective of DWP, without wholescale changes to disability assessments to alleviate demands on the system. While it is unclear whether it will meet the required demand to address the backlog at the time of writing, there do appear to be some opportunities for improving retention and recruitment issues, namely:
-
consider expanding the range of HCP professions that can qualify as HDAs to include, for example, prescribing pharmacists
-
ensure contract providers and recruiters provide a positive but realistic picture of the HDA role, including the importance of skills required beyond the HCP qualification
-
explore the potential for revising the recruitment and training processes to:
-
build in greater flexibility to accommodate different personal preferences and circumstances (for example, part-time study)
-
enable trainee HDAs to get a stronger sense of the role earlier in the process and their suitability for this
-
create more of a supportive environment such that trainees do not feel so disempowered through the auditing and assessment stages of the approval process
- Look at opportunities to create more variety in HDA roles, and progression opportunities within APs relative to skills and career aspirations. This could include:
-
developing partnerships with NHS trusts to enable HDAs to deliver therapeutic care on a part-time basis, alongside their HDA role
-
ensuring HDAs have the opportunity to work across different types of task (and potentially benefits). This could also include the opportunity to take on different responsibilities while performing their HDA role, such as mentoring
- Consider different incentive structures to promote HDAs remaining in role post 12 to 24 months.
Annex A: Research into recruitment and retention of health and disability assessors
London Economics to The Social Agency (formerly Basis Social) for the Department for Work and Pensions
Context Note
This report was originally commissioned by the Department for Work and Pensions (DWP) and written in 2022. It formed one part of a wider project on the recruitment and retention of health and disability assessors (HDAs). As such, the findings within this annex are relevant to the climate of the time.
The wider project was led by The Social Agency (formerly Basis Social), who have undertaken an evidence review and qualitative research with DWP agents, existing HDAs and former HDAs. This report is designed to be considered alongside the work undertaken by The Social Agency. This annex exists as a consolidated version of the original London Economics report as a final deliverable for this project.
A1 Key Findings
There is a large supply of registered healthcare professionals (HCPs) as well as appropriately qualified individuals working in other occupations.
Most of those qualified as HCPs choose to work in health-related fields, but there are a modest proportion of individuals who work in other occupations. Assessment providers could target these individuals by providing a path to revalidation as HCPs through re-training.
Despite growth in the economically inactive population during the COVID-19 pandemic, the number of appropriately qualified individuals that are economically inactive who are likely to return to work is relatively small.[footnote 39] As unemployment is also relatively low (as of February 2022)[footnote 40], assessment providers are likely to mostly recruit from those already in work.
However, external demand for HCPs is very high. The NHS is the main employer of HCPs and there have been persistently high vacancies for more than a decade. Given the fact that the supply of newly qualified nurses is based on NHS estimates of patient demands, and increasing the training pipeline is both hugely expensive and takes a considerable length of time to realise, competition for HCPs is likely to remain high. This will make recruitment by assessment providers extremely challenging in the short and medium term.
Salaries of HCPs are not as competitive as they may initially appear. Amongst some assessment providers, advertised salaries are lower than the median salary for HCPs.
Workforce retention is a very serious issue for assessment providers. Due to elevated levels of attrition, very high recruitment levels would be required in order to maintain the workforce required to meet existing assessment targets.
Many of the skills required and work activities performed by Health and Disability Assessors (HDAs) in the assessment aspect of their role are fundamentally different from those of HCPs. As a result, HCPs may struggle to adapt to the different nature of the HDA role and not be attracted to the core assessment aspect of the HDA role.
The most similar healthcare-related roles to HDAs are ones that are more desk-based, administrative, or require gathering and processing information. These could be medical support roles, but these individuals are unlikely to have the adequate levels of knowledge or clinical experience required for the role.
The lack of similarity between the roles will put increased pressure on the financial compensation offered to recruit and retain healthcare professionals by assessment providers (as well as the nature of the working conditions).
A2 Supply of potential assessors
HDAs must be registered healthcare professionals with at least 1 to 2 years’ UK experience (depending on the job specification). The following healthcare professions are eligible to become assessors:
-
Doctors
-
Nurses
-
Physiotherapists
-
Occupational therapists
-
Paramedics (only for PIP)
This section looks at the number of healthcare professionals that are registered across the United Kingdom and the number of trained healthcare professionals in work at the time of writing (either as healthcare professionals or not), as well as the number of trained healthcare professionals out of work (for reasons of unemployment or economic inactivity). This approach identifies those who are eligible to become HDAs, as well as those who could potentially become HDAs through revalidation.
A2.1 Size of the pool of healthcare professionals
Professional registration bodies provide data on the number of healthcare professionals that are registered in the professions from which HDAs are recruited at the time of writing. For nurses, the relevant organisation is the Nursing and Midwifery Council (NMC); for doctors, it is the General Medical Council (GMC); for occupational therapists, paramedics and physiotherapists it is the Health & Care Professions Council (HCPC). The number of registered professionals shows the size of the pool of individuals who, are at the time of writing, eligible to become HDAs.[footnote 41] There will also be a pool of individuals who were previously registered, who could revalidate and become HDAs, but these are not shown in these statistics.
Registration with the NMC, GMC or HCPC is a pre-requisite to become an HDA. However, being registered with a professional body does not guarantee that individuals are practising in the profession: they may be in another profession, unemployed or outside the workforce (economically inactive). However, registration bodies require revalidation – for nurses this is every 3 years; for doctors it is usually every 5 years; for other professions it is every 2 years. Revalidation generally requires that nurses have been practising for at least 450 hours (in total) in the past 3 years, while occupational therapists, paramedics and physiotherapists need to have demonstrated that they have practised at some point in the previous two years. Doctors are assessed (usually by “responsible officers” within their own organisation) for their fitness to practise based on yearly appraisals. It is also possible for HCPs who have not recently practised to revalidate, but it usually requires a course to be taken.
As a result of the revalidation processes, there may be a lag between employment trends and registration trends. For example, if a nurse were to revalidate (or originally register), then drop out of the labour force immediately, then they would still appear in registration statistics three years later when it would be time to revalidate. Additionally, this data cannot capture any changes in the mode of employment (for example, moving from full-time to part-time employment). It will also not immediately capture emigration (as this will only show when individuals are required to revalidate to remain on the register). However, the register does give an accurate picture of the potential number of HCPs that DWP could recruit from.
A2.1.1 Total number of registered HCPs
The total number of registered HCPs increased by around 180,000 (18%) between 2013 and 2021, from around 1 million to 1.18 million (Figure 1).[footnote 42] Nurses made up the largest proportion of healthcare professionals, standing at approximately 59% in 2021 (corresponding to approximately 700,000 registered nurses[footnote 43]). This percentage fell from 64% in 2013, even though the number of nurses increased by 57,000 (9%).[footnote 44] Doctors made up the second largest proportion of the HCP population in 2021 (30%), which increased from 26% in 2013. Approximately 350,000 doctors were on the register in December 2021.[footnote 45] The population of doctors increased by 93,000 from 2013 to 2021 (a 36% rise). The other occupations only make up around 11% of the HCP population between them (4% for occupational therapists, 3% for paramedics and 5% for physiotherapists). However, the other occupations saw substantial growth between 2013 and 2021, particularly paramedics. The pool of occupational therapists grew by 25%, paramedics by 62% and physiotherapists by 24%. In September 2021, there were around 60,000 registered physiotherapists, 42,000 registered occupational therapists and 31,000 registered paramedics.[footnote 46]
Figure 1: Number of registered healthcare professionals (nurses, occupational therapists, paramedics and physiotherapists)

Source: London Economics’ analysis of Health & Care Professions Council, Nursing & Midwifery Council and General Medical Council data.
Note: Data on doctors includes provisional and temporary registrations. As data was not consistently available within the same months, Figure 1 was linearly interpolated to provide a like-for-like comparison.
A2.2 Trained healthcare professionals by work status
Trained healthcare professionals are not necessarily working in the field in which they are trained. They may be working in different occupations, be unemployed, or be economically inactive. Those who are not working in the field in which they are trained may not have active registration, so would not show up in the registration statistics. Therefore, the pool of potential HDAs could be wider than the number of registered HCPs (although non-registered former HCPs may need to be provided support to revalidate). Similarly, not all registered HCPs will be in work.
A2.2.1 Economically inactive Healthcare Professionals
According to the Labour Force Survey (LFS), the main reasons for inactivity[footnote 47] among individuals with a medical-related or nursing qualification (Figure 2) are retirement from paid work, being long-term sick or disabled and looking after family at home[footnote 48]. In total, there are around 185,000 medically-qualified or nursing-trained individuals who are out of work due to early retirement from paid work or because they are looking after family at home. In addition, there are more than 90,000 who self-describe their circumstances as being inactive for long-term health-related reasons and over 60,000 who are looking after family at home.
The LFS gives insight into distance from the active labour market, through providing data on whether individuals would like a paid job.[footnote 49] It may be particularly challenging to help those with medical-related or nursing qualifications out of economic inactivity, as they are less likely than other economically inactive individuals aged 16 to 65 to want a paid job (14% compared to 19%). Overall, around 46,000 inactive individuals with medical-related or nursing qualifications would like to work and only 22,000 of those have a qualification that is Level 6 (degree level) or above.
In part, this is because, compared to the rest of the economically inactive population, those with medical-related or nursing qualifications are more likely to be retired from paid work by 65 (35% compared to 20%). Only 1% of retired individuals aged 16 to 65 with a medical-related or nursing qualifications want a paid job (compared to 3% of non-qualified individuals that are defined as economically inactive).
However, economically inactive individuals with medical-related or nursing qualifications are less likely to be long-term sick or disabled or looking after family at home than other economically inactive individuals. Within those categories, 25% of the long-term sick and disabled and 17% of those looking after family report that they would like a paid job. Therefore, it is possible that offering flexible or part-time work may help move these individuals back into work. These individuals may need to be helped back into work through revalidation if their professional registration has expired.
Figure 2: Number of individuals with any medical-related or nursing qualification who are economically inactive, by reason for inactivity (aged 16-65)

Note: Does not include students, who are classified separately from the remainder of the inactive population in the LFS.
Source: London Economics’ analysis of Q3 2021 of the Labour Force Survey.
A2.2.2 Healthcare professionals in-work
The Labour Force Survey (LFS) has been used to estimate the number of individuals in the UK who are trained HCPs and in work. The identification of trained HCPs is not straightforward, as the definition of subjects is wider than desired, for example, dentistry within the “Medicine and Dentistry” category, so risks including subjects that are not relevant. Furthermore, certain individuals have not recorded their subject of study, so cannot be identified. As a result, the group of individuals identified is likely to include some individuals who do not have the relevant qualifications and exclude some individuals who do have the relevant qualifications. However, the analysis does provide an indication of where trained individuals are located within the labour force.
The following subjects were classified as medical or nursing-related for academic qualifications:
-
Medicine & dentistry (general)
-
Pre-clinical medicine
-
Clinical medicine
-
Other in medicine & dentistry
-
Subjects allied to medicine (general)
-
Anatomy, physiology & pathology
-
Nursing (excluding dental nursing)
-
Occupational health
-
Occupational therapy
The following vocational subjects were classified as medical or nursing-related for vocational qualifications:
-
Health broad programmes
-
Medicine
-
Nursing and caring
-
Medical diagnostic and treatment techniques
-
Therapy and rehabilitation
Further to this, anybody who was deemed to have a nursing qualification (there is a specific field for this, although it does not identify all nurses) was classed as having a medical-related or nursing qualification.
The classification has a high level of identification of relevant HCPs: it identifies 78% of nurses, 80% of physiotherapists, 77% of occupational therapists, 63% of paramedics and 63% of doctors. It also does well to avoid identifying irrelevant occupations: it only identifies 14% of dental practitioners and 24% of dental nurses.
This subject classification does not identify the level of qualification, so does not guarantee that individuals are eligible to work as HDAs.
Consequently, the number of individuals identified is an estimate and should be treated with some caution. However, this analysis helps to better understand whether those with medical or nursing-related qualifications are in the labour force at the time of writing.
-
Based on analysis of the LFS, approximately 1.86 million employed individuals were identified as having medical-related or nursing qualifications in Q3 of 2021.[footnote 50]
-
Most individuals were employed in occupations where it would be expected to find trained HCPs, with 74% being employed in professional occupations, or caring, leisure and other service occupations (Figure 3). These broad occupations include nurses, doctors, care workers and home carers, nursing auxiliaries and assistants, physiotherapists, midwives, and occupational therapists.
-
Around 9% of employed individuals with medical-related or nursing qualifications were employed in associate professional and technical occupations. This occupation group contains health associate professionals and paramedics.
-
Around 4% of employed individuals with medical-related or nursing qualifications were employed as managers, directors, or senior officials, but most of them were employed as medical-related managers.
-
The remaining 13% of employed individuals with medical-related or nursing qualifications are not employed in health-related fields. In most cases, there is a small proportion of individuals with medical-related or nursing qualifications working in occupations (relatively or entirely) unrelated to the original field of qualification. For example, around 23,000 sales and retail assistants possess a medical-related or nursing qualification (making up around 3% of all sales and retail assistants).
Figure 3: Proportion of the employed population with medical-related or nursing qualifications found in each SOC2010 major group occupation

Source: London Economics’ analysis of Q3 2021 of the Labour Force Survey.
Not all those with medical-related or nursing qualifications will have qualifications to a sufficiently high level to work as HDAs. Around 1.21 million[footnote 51] (65%) of the 1.86 million individuals with medical-related or nursing qualifications have a Level 6 qualification (degree level equivalent) or above, so should be sufficiently qualified.[footnote 52] Of those, around 588,000 are working outside the relevant healthcare professions (compared to approximately 1.17 million outside the relevant healthcare professions at all qualification levels). The number of qualified HCPs may be higher, as some individuals may have obtained a nursing qualification before it became a degree-level subject. Around 260,000 (14%) individuals in employment with a medical-related or nursing qualification have a Level 4 or 5 qualification[footnote 53] as their highest qualification. Those with medical or nursing qualifications below Level 4 are concentrated in certain professions: approximately 25% of care workers and 69% of nursing auxiliaries and assistants with a medical or nursing-related qualification have a qualification of Level 4 or above. These two professions make up around half of the group with medical-related or nursing qualifications who have their highest qualification below Level 4.
In summary, the pool of potential HDA supply outside of the professions from which they are recruited is much smaller than it initially appears, as around half of those with medical-related or nursing qualifications do not have qualifications to a sufficiently high level to be eligible to become HDAs. There are potentially around 600,000 employed individuals with relevant qualifications who are not working as HCPs at the time of writing. However, this estimate should be considered an upper bound, as the measure of ‘relevant qualifications’ may capture adjacent medical-related qualifications (for example, in subject allied to medicine) which do not provide eligibility to become HDAs.
Breakdown by sector
Figure 4 illustrates the breakdown of those with medical-related or nursing qualifications by industry sector. Most qualified individuals (70%) work in human health and social work activities, which matches the findings by occupation. However, this still means that approximately 30% work in other sectors of the economy, which suggests that assessment providers could recruit from outside healthcare for those who may be qualified but not registered, such as occupational therapists (around 4% of HCPs are occupational therapists, compared to 1% of HDAs amongst the Centre for Health and Disability Assessments (CHDA) HDA assessor workforce in 2022). The results below are broadly similar if just looking at those with Level 6 qualifications or above.
Figure 4: Percentage of employees with medical-related or nursing qualifications in each SIC 2007 sector

Note: Definition of medically- or nursing-trained population is in Section A2.2.2. ‘Other’ contains: ‘agriculture, forestry and fishing’ (0.2%), ‘mining and quarrying’ (0.1%), ‘manufacturing’ (1.2%), ‘water supply; sewerage, waste management and remediation activities’ (0.1%), ‘construction’ (0.4%), ‘transportation and storage’ (0.9%), ‘accommodation and food service activities’ (1.4%), ‘information and communication’ (0.6%), ‘financial and insurance activities’ (0.9%), ‘real estate activities’ (0.3%), ‘arts, entertainment and recreation’ (0.6%), ‘households as employers’ (0.1%), ‘activities of extraterritorial organisations and bodies’ (0.1%).
Source: London Economics’ analysis of Q3 2021 of the Labour Force Survey.
A2.2.3 Vacancies, tight supply, and recent labour market trends
Decreased labour force participation and unemployment
Recent wider labour market trends since the beginning of COVID-19 have been characterised by declining employment levels and a move towards economic inactivity. Research by the Institute for Employment Studies claims that the number of individuals actively participating in the labour force is approximately 1.15 million lower than it would have been if pre-pandemic growth had continued.[footnote 54] Around three-fifths of this difference is due to increased economic inactivity, particularly amongst women, while the remaining two-fifths is a result of limited population growth. The decreased labour force participation rate is likely to decrease the size of the potential HDA workforce.
While participation rates in the labour force have decreased, unemployment remains low (as of February 2022), at 4.1%, which is 0.1 percentage points higher than pre-pandemic levels.[footnote 55] At the same time, there were approximately 1.3 million job vacancies in February 2022, which is the highest on record.[footnote 56] Without even considering the extent of either skills mismatch or geographic disparities, the ratio of job vacancies to claimant count the lowest on record.[footnote 57] This combination of factors, and in particular the plentiful supply of outside options for healthcare professionals, makes the labour market exceptionally challenging for recruitment.
Vacancies
The level of vacancies is a particular challenge in healthcare. There were 206,000 vacancies in the human health and social work activities sector in November 2021 to January 2022[footnote 58], which is approximately 5.1 vacancies for each 100 employee jobs in the sector, compared to 3.4 before the pandemic. The statistic is also higher than the overall average of 4.3 across all economic sectors. Vacancies are also persistently high in the NHS, particularly in nursing. Within the NHS, it is possible to look at the total number of vacancies and the vacancy rate overall and for nurses specifically (Figure 5 and Figure 6).[footnote 59] Vacancy rates are higher in nursing than in other parts of the NHS, standing at 10.5% in September 2021, compared to 7.6% overall (Figure 5). Although vacancy rates have fallen in nursing since June 2018 (when they were 12.0%), the number of nurse vacancies in the NHS in September 2021 stood at approximately 39,800 (Figure 6).
Figure 5: Vacancy rate in the NHS for all workers and nurses, June 2018 to September 2021 (England)

Note: Dates refer to the date at the end of the quarter for which the data was collected.
Source: London Economics’ analysis of NHS Digital data.
Figure 6: Number of vacancies in the NHS for all workers and nurses, June 2018 to September 2021 (England)

Note: Dates refer to the date at the end of the quarter for which the data was collected.
Source: London Economics’ analysis of NHS Digital data.
A2.2.4 Salaries offered by assessment providers
The basic annual advertised starting salaries for HDAs are provided in Table 1 below. The salaries have been gathered through job adverts for HDAs found online, as no salary data from the assessment providers was provided to London Economics. These job adverts were primarily found through the assessment providers’ websites, but some have been added from other job adverts found elsewhere. As these salaries are those advertised, they only show starting salaries and do not give insight into salary progression. However, some job adverts do advertise a small salary uplift on completion of training as well as performance-related bonuses.
Assessment providers generally offer a range of salaries, which depend on (a) the location of the role; and (b) the type of role. Generally, higher salaries are offered in Greater London and areas around London (such as the South East). There is an uplift of around 20% for salaries within Greater London.[footnote 60] No regional variation could be found for Capita, but this may be because they do not offer assessments in the areas around London. Assessment providers generally advertise jobs for doctors separately to those of other professions and offer a substantially higher salary than for other professions. CHDA also offer a salary uplift of around 5% for physiotherapists.
As Table 2.3 shows, the variation in advertised salaries is relatively wide across the assessment providers, ranging from £34,000 to £46,200. To some extent, this difference is due to regional variation[footnote 61], but the highest basic salary outside of London (£39,500) is still approximately £5,500 per year higher than the lowest salary offered. Generally, salaries for PIP assessors (PIP assessments are provided by Capita and Independent Assessment Services (IAS)) are lower than salaries for WCA assessors (WCAs are provided by CHDA).
Table 2.3: Annual advertised starting salaries offered by assessment providers in 2021
| Assessment provider | Low | High | Other salaries found |
|---|---|---|---|
| Capita | £34,000 | - | - |
| IAS | £35,000 | £42,000 | £46,200 |
| CHDA | £39,500 | £46,300 | £72,000 - £84,200 |
Note: The only salary that can be found through the Capita vacancy page is £34,000. On the IAS website, salaries of £35,000 to £42,000 are advertised, but salaries for IAS PIP assessors in London are advertised elsewhere as up to £46,200. The low salary for CHDA is for outside London, while the high salary relates to positions based in London. The other salaries found for CHDA assessors are for doctors only - £72,000 is the figure for outside London, and £84,200 is the figure for within London.
Source: London Economics’ analysis of Capita, IAS, CHDA and Totaljobs websites.[footnote 62]
The starting salaries offered by assessment providers are put into context in Figure 7, which shows where the starting salaries offered by the assessment providers rank in terms of the percentile of gross earnings of full-time employed HCPs. The starting salaries offered by assessment providers are not particularly competitive, as shown by the relatively high proportion of HCPs that are already earning more than the HDA starting salary. The highest salary offered outside of London is at the 58th percentile for full-time nurses, the 60th percentile for full-time physiotherapists and the 75th percentile for full-time occupational therapists.[footnote 63] This means that many full-time workers (42% of nurses, 40% of physiotherapists and 25% of occupational therapists) in those healthcare professions will already be earning more than the salary offered by the assessment providers. In fact, the lowest advertised salary offered by providers is below the median salary for full-time employees in every profession studied. The lower salaries offered by assessment providers are similar to the total level of pay achieved by an NHS healthcare professional with approximately 4+ years’ experience positioned towards the top of Band 5 at the time of writing. While the assessment provider salaries studied refer to starting salaries for HDAs and are compared to salaries for experienced HCPs, it is these experienced HCPs that assessment providers are looking to attract, so this is a relevant comparison.
To attract potential recruits to become HDAs, this analysis suggests that the assessment providers should be offering higher wages to HDAs, of at least £38,000 per year outside London (some assessment providers already offer more than this). However, offering a higher starting salary than that (closer to £45,000) would be required to even start to financially attract approximately 30% more of the full-time nursing, physiotherapist and occupational therapist workforce. These salaries reflect 2021 prices, so due to high inflation in late 2021 and 2022, the nominal salaries required may be higher.
The basic salaries offered by assessment providers will also be unlikely to attract paramedics: even the maximum salary offered[footnote 64] is below the median salaries for paramedics. If assessment providers are looking to attract paramedics, then salaries would need to be raised to at least £47,200 per annum: this could be done specifically for paramedics, mirroring the approach that CHDA have adopted for physiotherapists.
The highest regular assessor salary is clearly well below median earnings for doctors. However, the specific salaries paid to doctors are at the 72nd percentile for the salary outside London and 81st percentile for the Greater London salary.
Figure 7: Yearly gross earnings percentiles of starting salaries offered by assessment providers in 2021 (full-time employees)

Note: Based on gross yearly earnings for full-time workers in each occupation. Only refers to salaries for regular health and disability assessors (for instance, does not include data on occupation-specific roles). Salaries considered are: Minimum: £34,000; Maximum outside London: £39,500; Maximum: £46,200. The highest percentile recorded for physiotherapists and occupational therapists in the ASHE data is the 80th percentile, so the true percentile of the highest salary is likely to be higher than that. Refers to starting salaries of assessment providers only.
Source: London Economics’ analysis of Capita, IAS, CHDA and Totaljobs websites and Annual Survey of Hours and Earnings data.[footnote 65]
A2.2.5 Working overtime
The ability to recruit from healthcare professions also depends on job satisfaction within healthcare professions. Every healthcare profession analysed in the Labour Force Survey had a higher-than-average incidence of overtime (as seen in Figure 8). Survey evidence from other sources also provides evidence on job satisfaction of HCPs in conjunction with their working patterns. The Royal College of Nursing’s 2021 Employment Survey reported that over 90% of nurses worked additional hours. 55% of nurses reported that they worked additional hours several times a week or every shift[footnote 66], while 53% of nurses working overtime reported that they were not paid for their overtime. Crucially however, despite the high incidence of overtime (sometimes unpaid), around half of nurses reported that they were happy with their working hours, with only around a quarter reporting that they were dissatisfied[footnote 67] (though it is unclear whether this dissatisfaction was in respect of working too few or too many hours). Interestingly, nurses also mentioned high levels of work intensification, with around two-thirds of nurses reporting that they were under too much pressure at work. Over-working, particularly during the COVID-19 pandemic, may push a number of HCPs to leave their profession. A 2020 survey by the Royal College of Nursing found that 33% of nurses reported that they worked longer hours during the pandemic, compared to 6% working shorter hours.[footnote 68]
Figure 8: Percentage of employees who ever work overtime in each healthcare profession and overall in the UK

Note: “UK average” refers to all occupations (for instance, not just healthcare professionals).
Source: London Economics’ analysis of Q3 2021 of the Labour Force Survey.
A3. Analysis of DWP and assessment provider data
A3.1 Staff turnover and retention
A3.1.1 Staff turnover
Staff turnover is a key indicator of workforce retention. Data from CHDA, IAS and Capita shows that workforce turnover is very high for health and disability assessors. An average of 4.3% of assessors left the occupation each month throughout 2021 (which compares to an estimate of 3.5% per month in both 2019 and 2020). In annual terms, this is equivalent to an attrition rate of 52% in 2021 (compared to 42% in 2020 and 43% in 2019).[footnote 69] In comparison, the annual turnover rate for NHS nurses and health visitors was between 9.0% and 10.5% each year from 2014 to 2020.
This data suggests that retention is a hugely noteworthy problem for assessment providers, as staff turnover is approximately four to five times higher than the main ‘source’ occupation categories in the NHS. While data before 2019 was not available for the other assessment providers, CHDA data suggests that retention issues have been a long-standing issue, illustrated by the 3.1% monthly turnover in 2018.
Turnover rates differ across assessment providers but are not directly comparable as different measures are used by each provider. Despite this, an upward trend in turnover is apparent. In particular, monthly turnover rates for each of the three providers ranged from 3.0% to 3.8% in 2019, stabilising or decreasing to between 2.2% and 3.9% in 2020, but increasing to between 3.6% and 6.9% in 2021. It is difficult to identify whether there is a link between salaries and turnover rates, as data was not provided on historical salaries and each assessment provider’s ranking changes each year.[footnote 70] However, there is a relationship between the 2021 staff turnover figures, and the salaries offered: the assessment provider with the lowest salary offered had the highest staff turnover and vice-versa.
A3.1.2 Turnover of staff during training
Data from CHDA allows for analysis of the level of accumulated experience of those leaving their jobs as assessment providers. The analysis identifies a particular issue relating to the retention of those in training. In 2021, 30% of new recruits left during their training period (3 months for non-doctors or 1 month for doctors), although this represented a reduction from 40% in 2018.[footnote 71] Following the completion of training, an average of 8% of newly-accredited[footnote 72] assessors left each month, which was higher than the 6% monthly attrition rate that existed in 2019 and 2020. In total, only around 44% of those recruited in 2021 could be expected to reach the stage of being classified as ‘experienced’ HDAs (requiring 9 months for non-doctors or 7 months for doctors). This result was similar across all years analysed.
Monthly training attrition is higher for non-doctors than for doctors. Based on the data provided, around 40% of non-doctors hired in 2021 would be expected to have become experienced, compared to 62% of doctors. In part, this finding is likely to be a result of the fact that doctors have a relatively shorter training period, but even once that is taken into account, their training attrition is still lower than for non-doctors.
A.3.1.3 Costs of high staff turnover
These early-career retention issues are likely to cause considerable issues for recruitment, as around 2.3 staff must be hired for each experienced staff member required. The extra recruitment required to fill the HDA pipeline will be accompanied by particularly high costs for assessment providers. On average, it costs approximately £3,000 to hire an employee (not including training costs).[footnote 73] Assessment providers must also pay the wages of staff while they are training and during their period of new accreditation, when they are less productive. In addition, assessment providers need to pay training costs and use the time of more experienced staff to train and supervise new employees. Therefore, the costs of staff turnover are very high for assessment providers with retention being the key issue to address.
Reducing attrition could also help reduce other staff costs incurred by assessment providers. Clinical Standards Leads (CSLs) are experienced assessors who spend most of their time training and providing support to staff, rather than directly assessing claims. The high training attrition and the high levels of recruitment in consequence means that these staff have to devote substantially more time to training new employees (rather than assessing) than might be otherwise warranted.
A4. Comparison of skills and work activities for healthcare professionals and assessors
A4.1 Similarity of skills and work activities of HCPs and the assessment element of the HDA role
A4.1.1 Overall similarity
The overall similarity of the skills and work activities of doctors, physiotherapists, occupational therapists, nurses and benefits assessors are shown in Table 4.1 – Skills and Table 4.2 – work activities. For each column in the table, a ranking x means that the occupation in the same row is the xth most similar to the occupation in the column heading characterised declining employment levels out of the 873 occupations analysed. For example, taking the example of physiotherapists (Table 4.1), a nurse is estimated to be the 4th closest occupation in terms of skills similarity, while physiotherapist is estimated to be the 12th closest occupation to a nurse.
The results show healthcare professions are similar to each other for both the skills required and the work activities performed. In particular, there is strong similarity between physiotherapists, occupational therapists and nurses on both dimensions. However, both the skills and work activities of benefits assessors are very different from those required for healthcare professionals. Benefits assessors rank over 400 in terms of skills similarity and between 204 and 430 in terms of work activities. These results suggest that healthcare professionals would not have the correct skills for, and would be unlikely to move into, a regular benefit assessor role due to the level of dissimilarity of the roles. Healthcare professionals are likely to be unused to the types of tasks that they are required to perform as an assessor and may not possess the correct skills required for the assessment component of their role.
An important caveat to note is that the analysis compares a ‘typical’ HCP with a ‘typical’ HDA. All individuals within an occupation are considered to have the same skills and to perform the same work activities as each other. While on average the work of benefits assessors is dissimilar from that of HCPs, it may be the case that HCPs of different levels of experience perform different tasks and therefore might be closer to the assessor role. This distinction between workers within the same occupation cannot be detected within this data, but it is an important consideration when looking in the following sections into the exact differences in the skills used and work activities performed.
Table 1: Ranking of skills similarity between doctors, physiotherapists, occupational therapists, nurses, and benefits assessors
| Doctors | Physiotherapists | Occupational therapists | Nurses | Benefits assessor | |
|---|---|---|---|---|---|
| Doctors | - | 29 | 20 | 10 | 310 |
| Physiotherapists | 48 | - | 4 | 12 | 261 |
| Occupational therapists | 49 | 6 | - | 25 | 386 |
| Nurses | 14 | 4 | 7 | - | 310 |
| Benefits assessor | 412 | 472 | 462 | 484 | - |
Note: Based on 873 occupations. Ranking refers to the ranking of the occupation in the row in the occupation in the column. For example, the bottom left cell indicates that benefits assessors are the 412th most similar occupation to a doctor, but the top right cell indicates that doctors are the 310th most similar occupation to a benefits assessor. Occupational definitions are detailed in Table 4.2 below. Doctors and nurses have the same rank for benefits assessors, as the ranking is of where they would place in the ranking of US occupations, which happens to be in the same place as both have similarity scores that are close to each other.
Source: London Economics’ analysis of O*NET data.[footnote 74]
Table 4.2: Ranking of work activities similarity between doctors, physiotherapists, occupational therapists, nurses, and benefits assessors
| Doctors | Physiotherapists | Occupational therapists | Nurses | Benefits assessor | |
|---|---|---|---|---|---|
| Doctors | - | 28 | 20 | 12 | 95 |
| Physiotherapists | 40 | - | 2 | 14 | 334 |
| Occupational therapists | 24 | 2 | - | 8 | 339 |
| Nurses | 7 | 3 | 3 | - | 307 |
| Benefits assessor | 204 | 395 | 427 | 430 | - |
Note: Based on 873 occupations. Ranking refers to the ranking of the occupation in the row in the occupation in the column. For example, the bottom left cell indicates that benefits assessors are the 204th most similar occupation to a doctor, but the top right cell indicates that doctors are the 95th most similar occupation to a benefits assessor. Occupational definitions are detailed in Table 4 below.
Source: London Economics’ analysis of O*NET data.
Table 4.3: Classification used for O*NET occupations
| Classification used for analysis | O*NET occupation |
|---|---|
| Doctors | General Internal Medicine Physicians |
| Doctors | Family Medicine Physicians |
| Doctors | Hospitalists |
| Doctors | Paediatricians, General |
| Doctors | Preventive Medicine Physicians |
| Doctors | Obstetricians and Gynaecologists |
| Doctors | Urologists |
| Doctors | Dermatologists |
| Doctors | Allergists and Immunologists |
| Doctors | Neurologists |
| Physiotherapists | Physical Therapists |
| Occupational therapists | Occupational Therapists |
| Nurses | Licensed Practical and Licensed Vocational Nurses |
| Nurses | Registered Nurses |
| Nurses | Critical Care Nurses |
| Nurses | Acute Care Nurses |
| Nurses | Advanced Practice Psychiatric Nurses |
| Nurses | Clinical Nurse Specialists |
| Nurses | Nurse Practitioners |
| Benefits assessor | Eligibility Interviewers, Government Programs |
Source: London Economics’ analysis based O*NET and LMI For All.[footnote 75]
A4.1.2 Breakdown of similarity
Behind the overall dissimilarity between HCPs and benefits assessors, it is possible to break down the skills and work activities that are similar and different. The main findings are below, with detailed findings to follow:
-
HCP roles require a wider variety of skills than those required by benefits assessors. This finding suggests that HCPs may be over-qualified for the assessment element of the HDA role.
-
Many interpersonal skills and analytical skills are more important for HCPs than for benefits assessors. However, speaking and active listening skills are generally more important for benefits assessors than for HCPs.
-
Benefits assessors undertake tasks that are generally more desk-based than those undertaken by HCPs, such as administrative activities and working with computers.
-
HCP roles require undertaking more abstract tasks (such as creativity and problem solving), more management, training and team-related tasks, and fewer planning tasks (such as organising, planning, and prioritising work) than benefits assessors.
-
Assisting and caring for others is an essential part of an HCP role but is only mildly important for benefits assessors.
A4.1.3 Alternative similar occupations to assessors
While benefits assessors are broadly dissimilar to HCPs, it is possible to find out which other occupations are similar to benefits assessors.
Considering healthcare-related occupations, in terms of work activities performed, the occupations that are most similar to benefits assessors are ones that are more desk-based, administrative, or require gathering and processing information. Similar healthcare-related occupations to benefits assessors include medical transcriptionists, patient representatives, dieticians and nutritionists, speech and language therapists and pharmacy technicians.
Considering the skills required, the healthcare-related jobs that are most similar to benefits assessors are those that require skills such active listening, reading comprehension, speaking, but do not require physical skills. Some medical support roles require similar skills to benefits assessors, such as some types of care workers and nursing auxiliaries.
Looking beyond healthcare-related roles, the jobs most similar to benefits assessors are generally office and administrative support occupations and business and financial support occupations. Similar jobs often involve clerical work, such as pensions and insurance clerks, bank and post office clerks. Other routine government roles are also similar, such as tax examiners and collectors. Other similar occupations include those human resources, paralegals, interpreters and translators, reporters and journalists, secretaries and receptionists. The most similar occupations to benefits assessors are very different to the roles of HCPs. Individuals working in these similar roles are likely to possess some of the skills required to be an HDA but are unlikely to have sufficient medical training to undertake functional assessments. It is possible that instead of giving assessor training to the limited pool of highly sought-after healthcare professionals, consideration might be given to widening the pool to assessor-type occupations, or more routine healthcare support roles, and providing them with more extensive functional assessment training. This option may be particularly attractive given the fact that clerical roles are some of the most at-risk of automation and therefore demand from firms for those types of roles is likely to naturally decrease over time. However, the level of training required would be much greater (and more expensive) than the assessor training given to HCPs by assessment providers at the time of writing, as it would require substantial medical training.
Appendix B
Further examples of best practice in recruitment and retention
An award-winning recruitment campaign: The Big Thank You at King’s College Hospital (KCH) NHS Foundation Trust[footnote 76]
KCH partnered with a recruitment agency to create an award-winning recruitment campaign built on extensive staff engagement. 166 staff were celebrated for their contribution and were photographed and filmed for the campaign, in which they spoke of their pride in working for the trust.
The trust saw tangible outcomes from the campaign: increasing its nursing establishment in a 6-month period, staff reported feeling valued and that the engagement campaign had boosted morale, and the profile of the trust was raised through winning two recruitment awards.
Embedding employee wellbeing as a strategic priority: Essex County Council (ECC)[footnote 77]
In September 2020 ECC launched its five-year, prevention-focused Wellbeing Strategy. During its development the council carried out a wellbeing audit and ran focus groups to ensure the strategy reflected the needs and views of its workforce. The strategy focusses on specific pillars of wellbeing: mental, physical, social and financial and encourages employees to take personal responsibility for their own wellbeing through an internal ‘My Wellbeing’ brand. This sense of accountability is matched through commitment to the strategy from council leadership, and training for managers so they can feel confident and capable to support employee wellbeing.
ECC are committed to evaluating the impact of their range of wellbeing programmes and are using a range of ‘hard’ and ‘soft’ metrics to measure the impact of its actions. Impact on recruitment and retention rates are one of the hard metrics, collected through quantitative approach with staff.
Improving staff retention through creating sustainable career pathways: Warrington and Halton Teaching Hospitals NHS FT[footnote 78]
To improve recruitment and retention the trust took a multi-step approach. First, workforce data was analysed, revealing gaps by age and profile. Further analysis revealed ‘limited career progression’ and ‘limited continual professional development’ as the two main reasons for nurses leaving. The trust held a series of physical and virtual engagement sessions where staff told them what they wanted and with this feedback, they then developed a clinical career pathway. A Nursing and Midwifery Recruitment and Retention group was established, chaired by the chief nurse, which provided strategic oversight and a governance structure for the programme.
In the 12-month period after implementing the career development pathway the trust experienced a reduction in registered nurse turnover by 2.55%, and an increase in the number of internal promotions.
Improving retention at all stages of nurses’ careers: United Lincolnshire Hospitals NHS Trust[footnote 79]
The trust faced increasing nurse turnover rates in 2018. A commissioned report highlighted to the trust that a ‘one size fits all’ approach to tackling turnover would not work and that they needed to look at retention initiatives targeted at staff groups with differing motivations and needs. At the time of the report 20.9% of the trust workforce were aged 55 or over and within 5 years this was expected to increase to 36.8%. Through staff consultation key across different workforce age groups needs were identified:
-
Baby boomers (50+ years) - look for a workplace that compliments their attitude to team working, and value leadership and mentoring positions for continued workplace learning.
-
Generation X (35 to 50 years) – generally seen as adaptable and great at collaboration, they want to learn more skills to stay competitive and highly value work/life balance.
-
Millennials (18 to 34 years) – important to have a workplace that aligns with their values and flexibility to sustain a good work/life balance, with ongoing feedback to help them progress.
The trust set up a retention project team and developed a framework that helped bring focus to the retention initiatives, based on the above identified groups within the workforce. Retention actions taken were:
-
Enhancing the quality of data around nurse turnover to understand the reasons behind staff leaving and staying.
-
Develop a formal and consistent approach to flexible working including the option to retire and return.
-
Enhance awareness of the development opportunities and career pathways available for staff.
As part of the retention strategy, ‘itchy feet conversations’ were launched to understand reasons for staff wanting to leave, including a dialogue on how to keep them. In the first 6 months of the initiative, 26 members of staff requested a conversation, and all were retained.
Diversity and inclusion: West Yorkshire and Harrogate Partnership (ICS) - Moving diverse leadership forward[footnote 80]
West Yorkshire and Harrogate Partnership (WY&HP) put diverse leadership at the heart of its ICS workforce strategy, to address the disproportionately high poor experiences in the workplace for BAME staff. A BAME Staff Network was designed an important part of turning this ambition into reality, with commitment and full support from the partnership’s leadership groups. The network is comprised of colleagues at all levels across the Partnership, working to support the partnership’s response to:
- leadership development
- communication
- health and wellbeing resources for staff
- involvement in shaping and contributing to research
- involvement in decision-making
- supporting staff with risk assessments
The network started a conversation on how the Partnership should collectively and visibly change its position on inclusion and diversity by organising a BAME staff talent takeover in October 2019. The takeover showcased a series of 90-second film clips asking bold questions of leaders across the partnership. This was supported by colleagues in senior leadership positions sharing their personal career progression experiences. The BAME staff network has been empowered with a strong voice across the Partnership is also represented on the Partnership’s People Board, system leadership executive group, clinical forum and the health inequalities network.
Increasing recruitment and retention through reward: Sherwood Forest Hospitals NHS Foundation Trust[footnote 81]
The trust developed a comprehensive reward package to play a vital role in its recruitment and retention campaign. It began looking into its staff survey results to focus on the areas which needed the most improvement. From this the organisation developed a recruitment and retention campaign. Working with numerous departments across the trust, the benefits booklet was revamped and featured new and relevant benefits. The newly published benefits booklet was distributed to existing staff and a communications campaign was launched to advertise the benefits package.
Long-service awards were introduced as part of the retention strategy. The trust holds afternoon tea sessions where staff receive a signed letter from the chief executive. Up to 250 staff would attend each session and events have received great feedback, with staff saying it improved morale and made them feel valued. There is also an annual recognition week held once a year where staff are thanked for their service. The trust also has thank-you cards for staff to complete for one another which are sent throughout the year. These recognition methods are included in the benefits booklet which shows staff they are supported and valued by the organisation. The key outcomes of these retention activities have been a one third reduction in registered nurse vacancies since 2020, an increase in retention rates have increased and decline in turnover rates.
Appendix C
DWP recruitment and retention research
Topic guide for assessors
February 2022
Note to researcher
DWP have commissioned The Social Agency (formerly Basis Social) to undertake research to understand the barriers to recruitment and retention of health and disability benefit assessors. The rationale for commissioning this research is to inform changes to DWP’s contracting processes, such that assessor recruitment and retention is improved, and providers’ assessment capacity is better suited to meet demand. Ensuring the supply of health and disability assessments (delivered through the contracted providers) adequately matches the demand for health and disability assessments, has always been a challenge for DWP. This has been driven in part by inadequate levels of assessor recruitment and retention, as previous investigations into this issue have shown.
50 to 60 qualitative interviews with current and former assessors, DWP contract managers and senior assessment agents will provide insight into the perceived barriers to the recruitment and retention of assessors, from the perspective of
- Current and former assessors
- Provider executives (from Capita, IAS, CHDA)
- DWP Senior Civil Servants managing assessment contracts, as well as opportunities to overcome these barriers
Research objectives
-
What are the current barriers to the recruitment and retention of assessors, from the perspective of a) current and former assessors, b) provider executives (from Capita, IAS, CHDA) executives and c) DWP Senior Civil Servants managing assessment contracts
-
Are there any potential changes which could mitigate against these barriers, from the perspective of a), b) and c) (above).
-
Do these barriers, as identified a), b) and c) (above), vary across different health and disability assessments? (for instance, PIP assessments, WCA and IIDB)
-
Are assessor characteristics (for example, age, region, job seniority, clinical profession, occupational history, working patterns), relevant factors in determining the likelihood of recruitment and retention, from the perspective of a), b) and c) (above).
This guide is only for use with Current Assessors.
Discussions will last 45 minutes.
Any queries about this discussion guide should be raised with the Project Lead.
Topic guide for current assessors
Content (timings 0 to 5 minutes)
Moderator to introduce the session.
My name is XXX. I work on behalf of Basis Social. We are an independent research agency who have been asked to carry out this research with you on behalf of DWP.
DWP have commissioned this research to understand some of the challenges to the recruitment and retention of health and disability benefit assessors, and the opportunities to improve recruitment and retention.
We’re speaking to a) a range of current and former assessors, b) provider executives (from Capita, IAS, CHDA) and c) DWP Senior Civil Servants managing assessment contracts.
The interview will last 40 to 45 minutes.
We have a lot to get through so please excuse me if I move the conversation on at times.
There are no right or wrong answers to the questions we will be asking. If any questions seem obvious, it’s because we don’t want to assume what you are thinking, we want to hear it in your own words. You don’t have to answer any question if you don’t want to, you can just ask us to move on.
As mentioned during recruitment, we would like to record this discussion but only if you are happy with this. This recording would only be reviewed by members of the Basis Social research team and will not be shared with DWP or your employer. Do you have any concerns or worries about this? If so, please don’t hesitate to raise these now – it won’t affect your participation in this research as I can take notes. If you are happy, I’ll start recording the session now.
The research will be used by DWP to inform service development. While the work may be published, all responses will remain anonymous.
Finally, Basis are a company partner of a body called the Market Research Society and abide by their code of conduct. Participation in this discussion is completely voluntary and you are able to withdraw your consent to participate at any point in the process. This includes during this discussion, or even afterwards.
Any questions before we start?
About them and their role (timings 5 to 10 minutes)
1. Could you briefly tell me about your role and responsibilities?
Probe if needed:
-
Which provider do they work for?
-
Do they undertake WCA and/or PIP assessments?
2. Where are you located?
3. What is your clinical background? (nurse, doctor, physio etc.)
4. How long have you worked as WCA/PIP assessor?
5. How long have you worked for [name of employer]?
6. Do you specialize in assessments for a specific type of claimant in terms of their presenting needs/conditions? (Note: that there are some Assessors who are champions n respect of different conditions)
7. How many assessments are you expected to carry out per week?
-
Has this workload changed over the course of the COVID-19 pandemic? Probe: How/why?
-
What do you think about these expectations? Are they reasonable?
8. What working pattern do you have? For example, 9 to 5
- Is overtime common or expected?
9. Are you working from home or have you been over the pandemic?
-
Moderator explore what proportion of time is spent working from home versus elsewhere.
-
How would you feel about returning full time to face to face assessments?
Recruitment to role of assessor (timings 10 to 15 minutes)
1. What did you do before becoming an assessor?
2. What motivated you to take on a role as a WCA/PIP assessor?
3. What were their expectations of the role?
- Key benefits that they perceived the role would offer?
4. To what extent have your expectations have been met so far?
- Explore how or why not met (if mentioned)
5. Could you tell me a little about the recruitment process?
- Was it easy or challenging?
- What support did you receive?
- Are there any ways in which the recruitment process could be improved?
Assessment process (timings 15 to 20 minutes)
1. What are your thoughts on the WCA / PIP assessment process more broadly? Explore:
-
What do you see as being the purpose of the assessment process?
-
Whether seen to be an effective and/or efficient process from the point of view of (1) assessors and (2) claimants? Why or why not?
-
[Where relevant] Whether any differences in views between WCA or PIP assessments?
2. What are the key challenges you face as a WCA / PIP assessor?
- How do these challenges make you feel about the role?
3. Where do you feel there are opportunities to improve the effectiveness or efficiency of the WCA / PIP assessment process?
Training and guidance (timings 20 to 25 minutes)
1. Can you briefly talk me through the training you received when you started? And any training that you received during your time as an assessor?
-
Have you received any specific training to assist with a specific condition a claimant may have?
-
How effective was this training in preparing you for your role?
-
On reflection, how might the training be improved?
2. What about broader support? For example, in terms of line management and pastoral care? How effective is this in enabling you to perform your role?
3. What support do you have access to if you are presented with a challenging case? For example:
-
Difficulty with the claimant (language, behaviour, anxiety)
-
Unclear or ambiguous evidence
4. In practice, how easy/difficult is it to access this support?
5. Is there guidance on claimants with acute conditions? If so, how helpful and/or clear is this?
-
‘Invisible illness’ – fibromyalgia, ME, mental health etc.
-
Rare or uncommon disabilities that may require specialist treatment
6. How important is training and support in how you feel about your job?
Perceptions of the role and looking forward (timings 25 to 35 minutes)
1. What do you enjoy most about:
-
Your role as an assessor
-
Working for [provider]
2. What do you enjoy least about:
-
Your role as an assessor
-
Working for [provider]
3. What kind of person is the role of assessor best suited to? Why? (Moderator note any mention of clinical profession, occupational history, age, job seniority, desire for specific working pattern)
4. And what kind of person is the role of assessor least suited to? Why? (Moderator note any mention of clinical profession, occupational history, age, job seniority, desire for specific working pattern)
5. Do you see yourself working as a (PIP/WCA) assessor for the long term (say for next 12 months)?
6. Have you considered leaving the profession at any point over the last 12 months? If so, why?
7. What do you think are some of the main reasons why practitioners leave their role as an assessor?
- And conversely, what makes people stay in these roles?
8. What changes could made to make the profession more attractive to potential employees in the future?
Final summary probes on:
- Recruitment
- Remuneration
- The day to day of the job
- Training and support
Final thoughts and close (timings 35 to 40 minutes)
1. Finally would you mind confirming your age, gender and how long you have been working in this role?
2. Any final thoughts you would like to share?
3. Thank and close.
Appendix D
DWP recruitment and retention research
Topic guide for former assessors
February 2022
Note to researcher
DWP have commissioned Basis Social to undertake research to understand the barriers to recruitment and retention of health and disability benefit assessors. The rationale for commissioning this research is to inform changes to DWP’s contracting processes, such that assessor recruitment and retention is improved, and providers’ assessment capacity is better suited to meet demand. Ensuring the supply of health and disability assessments (delivered through the contracted providers) adequately matches the demand for health and disability assessments, has always been a challenge for DWP. This has been driven in part by inadequate levels of assessor recruitment and retention, as previous investigations into this issue have shown.
50 to 60 qualitative interviews with current and former assessors, DWP contract managers and senior assessment agents will provide insight into the perceived barriers to the recruitment and retention of assessors, from the perspective of:
- Current and former assessors
- Provider executives (from Capita, IAS, CHDA)
- DWP Senior Civil Servants managing assessment contracts, as well as opportunities to overcome these barriers.
Research objectives
-
What are the current barriers to the recruitment and retention of assessors, from the perspective of a) current and former assessors, b) provider executives (from Capita, IAS, CHDA) executives and c) DWP Senior Civil Servants managing assessment contracts
-
Are there any potential changes which could mitigate against these barriers, from the perspective of a), b) and c) (above).
-
Do these barriers, as identified a), b) and c) (above), vary across different health and disability assessments? (for instance, PIP assessments, WCA and IIDB)
-
Are assessor characteristics (for example, age, region, job seniority, clinical profession, occupational history, working patterns), relevant factors in determining the likelihood of recruitment and retention, from the perspective of a), b) and c) (above)
This guide is only for use with Former Assessors.
Discussions will last 45 minutes.
Any queries about this discussion guide should be raised with the Project Lead.
Topic guide for former assessors
Content (timings 0 to 5 minutes)
Moderator to introduce the session. My name is XXX. I work on behalf of Basis Social. We are an independent research agency who have been asked to carry out this research with you on behalf of DWP.
DWP have commissioned this research to understand some of the challenges to the recruitment and retention of health and disability benefit assessors, and the opportunities to improve recruitment and retention.
We’re speaking to a) a range of current and former assessors, b) provider executives (from Capita, IAS, CHDA) and c) DWP Senior Civil Servants managing assessment contracts.
The interview will last 40 to 45 minutes.
We have a lot to get through so please excuse me if I move the conversation on at times.
There are no right or wrong answers to the questions we will be asking. If any questions seem obvious, it’s because we don’t want to assume what you are thinking, we want to hear it in your own words. You don’t have to answer any question if you don’t want to, you can just ask us to move on.
As mentioned during recruitment, we would like to record this discussion but only if you are happy with this. This recording would only be reviewed by members of the Basis Social research team and will not be shared with DWP or your employer. Do you have any concerns or worries about this? If so, please don’t hesitate to raise these now – it won’t affect your participation in this research as I can take notes. If you are happy, I’ll start recording the session now.
The research will be used by DWP to inform service development. While the work may be published, all responses will remain anonymous.
Finally, Basis are a company partner of a body called the Market Research Society and abide by their code of conduct. Participation in this discussion is completely voluntary and you are able to withdraw your consent to participate at any point in the process. This includes during this discussion, or even afterwards.
Any questions before we start?
About them (timings 5 to 15 minutes)
1. Could you briefly tell me about your role and responsibilities when you were an assessor?
Probe if needed:
- Which provider did they work for?
- Did they undertake WCA and/or PIP assessments?
2. How long did you work as WCA/PIP assessor for? And how long had you worked for [name of former employer]?
3. When did you stop your work as an assessor?
4. Where were you located while working as an assessor?
5. What is your clinical background? (nurse, doctor, physio etc.)
6. Were you a specialist or did you only conduct assessments for a specific type of claimant?
7. How many assessments were you expected to carry out per week?
-
[If relevant] Did this workload change over the course of the COVID-19 pandemic? Probe: How and why?
-
What did you think about these expectations? Were they reasonable?
8. What working pattern did you have? For example, 9 to 5 * Was overtime common or expected?
9. [If working as an assessor during the pandemic] Were you working from home over the pandemic? Explore what proportion of time was spent working from home versus elsewhere.
10. Thanks, and can I ask what you do now?
Recruitment to role of assessor (timings 15 to 20 minutes)
1. What did you do before becoming an assessor?
2. What motivated you to take on a role as a WCA/PIP assessor?
3. What were their expectations of the role?
- Key benefits that they perceived the role would offer?
4. To what extent were your expectations met?
- Explore how and why not met (if mentioned)
5. Could you tell me a little about the recruitment process?
-
Was it easy or challenging?
-
What support did you receive?
-
Are there any ways in which the recruitment process could be improved?
Assessment process (timings 20 to 25 minutes)
1. What are your thoughts on the WCA / PIP assessment process more broadly? Explore:
-
What do you see as being the purpose of the assessment process?
-
Whether seen to be an effective and/or efficient process from the point of view of (1) assessors and (2) claimants? Why or why not?
-
[Where relevant] Whether any differences in views between WCA or PIP assessments?
2. What are the key challenges you faced as a WCA / PIP assessor?
- How did these challenges make you feel about the role?
3. Where do you feel there are opportunities to improve the effectiveness or efficiency of the WCA / PIP assessment process?
Perceptions of the assessor role (timings 20 to 25 minutes)
1. What did you enjoy most about:
-
Your role as an assessor
-
Working for [provider]
2. What did you enjoy least about:
-
Your role as an assessor
-
Working for [provider]
3. What kind of person is the role of assessor best suited to? Why?
Moderator note any mention of clinical profession, occupational history, age, job seniority, desire for specific working pattern
4. What kind of person is the role of assessor least suited to? Why?
Moderator note any mention of clinical profession, occupational history, age, job seniority, desire for specific working pattern
Reasons for leaving (timings 25 to 35 minutes)
Thinking back to your expectations and motivations for taking on the assessor role initially:
1. What, if any, aspects of the assessor role did not live up to your expectations?
2. Were there any key challenges you faced in role?
- How did you manage them?
3. Did you receive sufficient training and support to enable you to perform your role?
- If not, what other training or support would have been useful?
4. May I ask, why did you decide to leave the role?
Probe satisfaction with:
- nature of work
- job satisfaction
- benefits and financial reward
- support
- progression
- development and training
- support
- colleagues
- workplace culture
5. Upon resigning did you have an exit interview? If so, explore:
-
Were you asked about your reasons for leaving the role?
-
Were you given the opportunity to feedback on any issues you had during your time as an assessor?
-
What issues did you share?
6. More broadly, why do you think there is high staff turnover observed across the assessor or HCP profession?
7. Can I ask if you are currently in employment? If so, what do you do?
If employed:
- What was your motivation for taking on this role?
- How does your current role compare to your previous role as an assessor?
(Moderator ensure to be sensitive in asking this question as could be highly personal – make sure they know they only have to answer if they feel comfortable)
Recommendations (timings 35 to 40 minutes)
1. What advice would you give to someone considering becoming an assessor?
2. Are there any changes that could be made that would make it more attractive for Assessors to remain in their roles?
Probe on:
- pay and benefits
- career progression
- development and training
- support
- colleagues
- workplace culture
3. Would you ever consider returning to the profession in future? Why or why not?
Final thoughts and close (timings 40 to 45 minutes)
1. Finally, would you mind confirming your age, gender
2. Any final thoughts you would like to share?
3. Thank and close
Appendix E
DWP recruitment and retention research
Topic guide for Senior Assessment Agents/Executives
February 2022
Note to researcher
DWP have commissioned Basis Social to undertake research to understand the barriers to recruitment and retention of health and disability benefit assessors. The rationale for commissioning this research is to inform changes to DWP’s contracting processes, such that assessor recruitment and retention is improved, and providers’ assessment capacity is better suited to meet demand. Ensuring the supply of health and disability assessments (delivered through the contracted providers) adequately matches the demand for health and disability assessments, has always been a challenge for DWP. This has been driven in part by inadequate levels of assessor recruitment and retention, as previous investigations into this issue have shown.
50 to 60 qualitative interviews with current and former assessors, DWP contract managers and senior assessment agents will provide insight into the perceived barriers to the recruitment and retention of assessors, from the perspective of:
- Current and former assessors
- Provider executives (from Capita, IAS, CHDA)
- DWP Senior Civil Servants managing assessment contracts, as well as opportunities to overcome these barriers
Research objectives
- What are the current barriers to the recruitment and retention of assessors, from the perspective of a) current and former assessors, b) provider executives (from Capita, IAS, CHDA) executives and c) DWP Senior Civil Servants managing assessment contracts
-
Are there any potential changes which could mitigate against these barriers, from the perspective of a), b) and c) (above)
-
Do these barriers, as identified a), b) and c) (above), vary across different health and disability assessments? (for instance, PIP assessments, WCA and IIDB)
- Are assessor characteristics (for example, age, region, job seniority, clinical profession, occupational history, working patterns), relevant factors in determining the likelihood of recruitment and retention, from the perspective of a), b) and c) (above)
This guide is ONLY for use with Senior Assessment Executives.
Discussions will last 45 minutes.
Any queries about this discussion guide should be raised with the Project Lead.
Topic guide for senior assessment executive/associates
Content (timings 0 to 5 minutes)
Moderator to introduce the session.
My name is XXX. I work on behalf of Basis Social. We are an independent research agency who have been asked to carry out this research with you on behalf of DWP.
DWP have commissioned this research to understand some of the challenges to the recruitment and retention of health and disability benefit assessors, and the opportunities to improve recruitment and retention.
We’re speaking to a) a range of current and former assessors, b) provider executives (from Capita, IAS, CHDA) and c) DWP Senior Civil Servants managing assessment contracts.
The interview will last 40 to 45 minutes.
We have a lot to get through so please excuse me if I move the conversation on at times.
There are no right or wrong answers to the questions we will be asking. If any questions seem obvious, it’s because we don’t want to assume what you are thinking, we want to hear it in your own words. You don’t have to answer any question if you don’t want to, you can just ask us to move on.
As mentioned during recruitment, we would like to record this discussion but only if you are happy with this. This recording would only be reviewed by members of the Basis Social research team and will not be shared with DWP or your employer. Do you have any concerns or worries about this? If so, please don’t hesitate to raise these now – it won’t affect your participation in this research as I can take notes. If you are happy, I’ll start recording the session now.
The research will be used by DWP to inform service development. While the work may be published, all responses will remain anonymous.
Finally, Basis are a company partner of a body called the Market Research Society and abide by their code of conduct. Participation in this discussion is completely voluntary and you are able to withdraw your consent to participate at any point in the process. This includes during this discussion, or even afterwards.
Any questions before we start?
About them (timings 5 to 10 minutes)
1. Which provider do you work for?
2. Can you tell me a little bit about your role and what it involves?
3. Are you Involved specifically with the WCA or PIP assessment workforce?
4. What is your professional background?
Probe whether any experience as an assessor or clinical practitioner?
5. How long have you worked as an [role] with [provider]?
Assessment process (timings 10 to 20 minutes)
1. What are your thoughts on the WCA / PIP assessment process more broadly?
Explore:
- Whether seen to be an effective and/or efficient process? Why or why not?
- [Where relevant] Whether any differences in views between different types of assessments for example, PIP versus WCA?
2. What are the key challenges faced by WCA / PIP assessors?
-
What impact did this have on the assessors?
-
Does this impact your role? How?
3. Where do you feel there are opportunities to improve the effectiveness or efficiency of the WCA / PIP assessment process?
-
For claimants
-
For assessors
-
For your organisation
Assessor recruitment (timings 20 to 30 minutes)
1. What do you think motivates health care professionals to apply to be a WCA/PIP assessor?
Probe on what they perceive as the key benefits, and touch on:
- salary
- progression
- sense of purpose or job satisfaction
- work/life balance
- Remaining in a person-facing role in an alternative context
2. What do you consider to be the core competencies of a good assessor?
3. What kind of person is the role of assessor best suited to? Why?
Moderator note any mention of clinical profession, occupational history, age, region, job seniority, desire for specific working pattern
4. What kind of person is the role of assessor least suited to? Why?
Moderator note any mention of clinical profession, occupational history, age, region, job seniority, desire for specific working pattern
5. Do you see the right kind of talent ‘walking through the door’ or applying for the roles? Why or why not?
6. What is the job market like for assessors?
Probe specifically on:
- Levels and quality of ‘supply’
- Levels of market demand and competition for individuals who qualify as assessors
7. In your view, what factors are driving the current job market situation?
8. How has the job market for assessors changed over the course of the pandemic?
- Explore driving factors
9. What are the key challenges in the successful recruitment of assessors?
10. What do you consider to be key opportunities for increasing recruitment WCA/PIP assessor roles? What needs to improve?
Assessor retention (timings 30 to 40 minutes)
1. Do you conduct exit interviews with assessors who chose to leave?
-
If so, do you explore the reasons behind why an assessor has chosen to leave?
-
What kind of reasons for leaving do you typically hear from assessors?
2. More generally, what do you see as the reason(s) for the high staff turnover observed across the assessor or HCP profession?
Probe relative weight given to following aspects:
- salary
- progression
- job satisfaction
- support
- job security etc.
- moved to telephone or online assessment during the pandemic
- pandemic causing shift in job perceptions
3. What are the key opportunities for increasing retention of WCA/PIP assessors?
- Which of these opportunities are most feasible to implement (for instance, accounting for what is within power of DWP verses their organisation)
Final thoughts and close (timings 40 to 45 minutes)
4. Finally, would you mind confirming your age and gender?
5. Any final thoughts you would like to share?
6. Thank and close
Appendix F
DWP recruitment and retention research
Topic Guide for Senior DWP Agents/Contract Managers
February 2022
Note to researcher
DWP have commissioned Basis Social to undertake research to understand the barriers to recruitment and retention of health and disability benefit assessors. The rationale for commissioning this research is to inform changes to DWP’s contracting processes, such that assessor recruitment and retention is improved, and providers’ assessment capacity is better suited to meet demand. Ensuring the supply of health and disability assessments (delivered through the contracted providers) adequately matches the demand for health and disability assessments, has always been a challenge for DWP. This has been driven in part by inadequate levels of assessor recruitment and retention, as previous investigations into this issue have shown.
50 to 60 qualitative interviews with current and former assessors, DWP contract managers and senior assessment agents will provide insight into the perceived barriers to the recruitment and retention of assessors, from the perspective:
-
current and former assessors
-
provider executives (from Capita, IAS, CHDA)
-
DWP Senior Civil Servants managing assessment contracts, as well as opportunities to overcome these barriers.
Research objectives
-
What are the current barriers to the recruitment and retention of assessors, from the perspective of a) current and former assessors, b) provider executives (from Capita, IAS, CHDA) executives and c) DWP Senior Civil Servants managing assessment contracts
-
Are there any potential changes which could mitigate against these barriers, from the perspective of a), b) and c) (above)
- Do these barriers, as identified a), b) and c) (above), vary across different health and disability assessments? (for instance. PIP assessments, WCA and IIDB)
- Are assessor characteristics (for example, age, region, job seniority, clinical profession, occupational history, working patterns), relevant factors in determining the likelihood of recruitment and retention, from the perspective of a), b) and c) (above).
This guide is ONLY for use with senior DWP agents.
Discussions will last 35 minutes.
Any queries about this discussion guide should be raised with the Project Lead.
Topic guide for senior DWP agents/contract managers
Content (timings 0 to 5 minutes)
Moderator to introduce the session.
My name is XXX. I work on behalf of Basis Social. We are an independent research agency who have been asked to carry out this research with you on behalf of DWP.
DWP have commissioned this research to understand some of the challenges to the recruitment and retention of health and disability benefit assessors, and the opportunities to improve recruitment and retention.
We’re speaking to a) a range of current and former assessors, b) provider executives (from Capita, IAS, CHDA) and c) DWP Senior Civil Servants managing assessment contracts.
The interview will last 30 to 35 minutes.
We have a lot to get through so please excuse me if I move the conversation on at times.
There are no right or wrong answers to the questions we will be asking. If any questions seem obvious, it’s because we don’t want to assume what you are thinking, we want to hear it in your own words. You don’t have to answer any question if you don’t want to, you can just ask us to move on.
As mentioned during recruitment, we would like to record this discussion but only if you are happy with this. This recording would only be reviewed by members of the Basis Social research team and will not be shared with DWP or your employer. Do you have any concerns or worries about this? If so, please don’t hesitate to raise these now – it won’t affect your participation in this research as I can take notes. If you are happy, I’ll start recording the session now.
The research will be used by DWP to inform service development. While the work may be published, all responses will remain anonymous.
Finally, Basis are a company partner of a body called the Market Research Society and abide by their code of conduct. Participation in this discussion is completely voluntary and you are able to withdraw your consent to participate at any point in the process. This includes during this discussion, or even afterwards.
Any questions before we start?
About them (timings 5 to 10 minutes)
1. Can you tell me a little bit about your role and what it involves?
2. How does your role relate to the management or oversight of assessors and/or provider executives?
- Which providers do you have management or oversight of?
3. How long have you worked for DWP? And how long in this role specifically?
4. How would you describe your relationship with [named] providers?
-
What works well and when does it work well?
-
What challenges do you experience in managing these relationships?
Assessment process (timings 10 to 15 minutes)
1. What are your thoughts on the WCA / PIP assessment process more broadly?
Explore:
- Whether perceived as an effective and/or efficient process? Why or why not?
- [Where relevant] Whether any differences in views between different types of assessments?
2. What are the key challenges faced by WCA / PIP assessors?
- What impact do these challenges have more broadly for example, on DWP, and more specifically, to you in your role?
3. Where do you feel there are opportunities to improve the effectiveness or efficiency of the WCA / PIP assessment process?
-
For claimants
-
For assessors
-
For DWP as a whole
Assessor recruitment and retention (timings 15 to 30 minutes)
1. What do you think motivates people to become a WCA/PIP assessor?
Probe on what they see as the key benefits, and touch on:
- salary
- progression
- purpose or job satisfaction
- sense of purpose or job satisfaction
- remaining in a person-facing role in an alternative context
2. What do you consider to be the core competencies of a good assessor?
Focus on recruitment
3. What do you consider to be the key challenges regarding the recruitment of assessors into provider organisations?
4. What do you consider to be key opportunities for increasing recruitment of WCA/PIP assessor roles?
- What would you like to see from assessment providers to facilitate recruitment?
Focus on retention
5. What do you understand as the reason(s) for the high staff turnover observed across the assessor profession?
6. What do you consider to be key opportunities for increasing retention of WCA/PIP assessors?
- What would you like to see from assessment providers to facilitate retention of Assessors?
7. What role, if any, do you think DWP has in supporting providers to address some of the recruitment and retention challenges highlighted in this interview?
Explore:
- Are there alternatives to the current provider model (including pros and cons of these)
- Knowledge sharing
- More communication between assessors and DWP
Final thoughts and close (timings 30 to 35 minutes)
1. Finally would you mind confirming your age and gender?
2. Any final thoughts you would like to share?
3. Thank and close
Bibliography
1. Research into recruitment and retention of health and disability assessors; London Economics; 2022
2. Resourcing and talent planning survey 2021; CIPD; 2021
3. www.nhsemployers.org/publications/improving-staff-retention
4. WE ARE THE NHS: People Plan 2020/21 - action for us all; NHS; 2020
7. Recruitment and retention in adult social care: secrets of success Learning from employers what works well; Skills for Care; 2017
8. Labour Market Overview, UK, ONS
12. The Cost of Brain Drain: Understanding the financial impact of staff turnover; Oxford Economics; 2014
13. The courage of compassion; The Kings Fund; 2020
14. Caring for doctors, caring for patients; West, M. & Cola, D.; 2019
16. www.local.gov.uk
17. NHS Improving staff retention
20. The Education Staff Wellbeing Charter; Department for Education; 2021
21. www.england.nhs.uk retaining the current medical workforce
23. Health and Wellbeing at Work 2021, Case studies; CIPD; 2021
24. Creating a sustainable career pathway
25. www.nhsemployers.org improving retention
26. www.england.nhs.uk - moving diverse leadership forward
27. NHS - increasing recruitment and retention through reward
28. Workforce burnout and resilience in the NHS and social care; House of Commons Health and Social Care Committee; 2021
-
DWP were able to provide 41 named contacts in total, of which interviews were undertaken with 30 people. All contacts were invited to participate in the research and contacted up to three times. ↩
-
London Economics’ analysis of data from Capita, IAS and CHDA. Provided by DWP. ↩
-
NHS Workforce statistics December 2021: NHS Workforce Statistics - December 2021 (Including selected provisional statistics for January 2022) - NHS England Digital. ↩
-
O*NET is a tool from the United States, where nearly 1,000 occupations are classified according to the knowledge, skills and abilities required for the job, alongside the activities and tasks performed. Available at: onetcenter.org. ↩
-
Scope. (2021). Health assessments for benefits (Work and Pensions Committee HAB0079). House of Commons. Available at: Pensions Committee HAB0079. ↩
-
This estimate should be considered an upper bound, as the measure of ‘relevant qualifications’ may capture adjacent medical-related qualifications (for example, in subject allied to medicine) which do not provide eligibility to become HDAs. ↩
-
CHDA hold responsibility for WCA which at the point of the research still required HDAs to work from specific sites rather than from home, limiting the pool from which HCPs could be drawn. ↩
-
Stress and burnout in the NHS, exacerbated by the demands of the COVID-19 pandemic, is an acknowledged issue driving HCPs to leave their jobs (as detailed in “Workforce burnout and resilience in the NHS and social care”; House of Commons Health and Social Care Committee; 2021). London Economics accompanying report highlights that every healthcare profession analysed in the Labour Force Survey had a higher-than-average incidence of overtime and that around one-quarter of nurses responding to the Royal College of Nursing’s 2021 Employment Survey reported they were dissatisfied with their working hours. ↩
-
As of April 2022, CHDA were not offering full WFH capability for HDAs delivering WCA, although pilots are underway. ↩
-
Institute for Employment Studies (2022). Labour Market Statistics, February 2022. Available at: employment-studies.co.uk. ↩
-
Office for National Statistics (2022). Employment in the UK: February 2022. Available at: www.ons.gov.uk. ↩
-
Office for National Statistics (2022). Vacancies and jobs in the UK: February 2022. Available at: www.ons.gov.uk. ↩
-
Institute for Employment Studies (2022). Labour Market Statistics, February 2022. Available at: www.employment-studies.co.uk. ↩
-
Resourcing and talent planning survey 2021; CIPD; 2021 ↩
-
ibid ↩
-
We should acknowledge this data is based on advertised, not actual salaries ↩
-
The percentiles are likely to be higher if one only looked at percentiles HCP salaries outside London, but this data is not available through the ASHE (the regional income deciles for HCPs are sparsely-populated or non-existent due to small sample sizes). ↩ ↩2
-
London Economics’ analysis of Capita, IAS, CHDA and Totaljobs websites and Annual Survey of Hours and Earnings data. ↩
-
Recruitment and retention in adult social care: secrets of success; Skills for care; 2017 ↩
-
Labour market overview, UK , Office for National Statistics (ons.gov.uk) ↩
-
At the time of writing the future assessment channel strategy is under review by DWP and Treasury, due to the end of ‘COVID-19 easement’ ↩
-
The courage of compassion; The Kings Fund; 2020 ↩
-
Caring for doctors, caring for patients; West, M. & Cola, D.; 2019 ↩
-
Top tips for retention , A briefing for adult social care providers ↩
-
The Education Staff Wellbeing Charter; Department for Education; 2021 ↩
-
NB this is a qualitative assessment framework based on secondary analysis of feedback from the qualitative sample of HDAs, DWP contract managers, senior stakeholders in assessment providers and recruiters ↩
-
Institute for Employment Studies 2022 - Labour Market Statistics, February 2022. ↩
-
Office for National Statistics 2022 - Employment in the UK February 2022. ↩
-
The figures include a small number of recently trained HCPs who will not yet have the required number of years of clinical experience. ↩
-
Health & Care Professions Council. (2021). Registrant data and statistics ↩
-
September 2021 Mid-year report, Registration data reports, Nursing and Midwifery Council ↩
-
Register data over time, December 2021, General Medical Council ↩
-
Registrant snapshot 1 September 2021, Health and Care Professions Council ↩
-
Based on Labour Force Survey data. The definition of inactivity in the LFS does not include students. ↩
-
Office for National Statistics (ONS), released 8 December 2022, ONS website, statistical bulletin, Economic activity status, England and Wales: Census 2021 ↩
-
Office for National Statistics, Northern Ireland Statistics and Research Agency. (2021). Quarterly Labour Force Survey, July - September, 2021. UK Data Service. SN: 8872, DOI: 10.5255/UKDA-SN-8872-1 ↩
-
Office for National Statistics, Northern Ireland Statistics and Research Agency. (2021). Quarterly Labour Force Survey, July - September 2021. UK Data Service. SN: 8872, DOI: 10.5255/UKDA-SN-8872-1 ↩
-
Office for National Statistics, Northern Ireland Statistics and Research Agency. (2021). Quarterly Labour Force Survey, July - September, 2021. UK Data Service. SN: 8872, DOI: 10.5255/UKDA-SN-8872-1 ↩
-
The majority of job advertisements identified indicate that individuals should have a professional registration in the relevant healthcare professions. Although this normally is associated with a Level 6 qualification, in a number of interviews undertaken by The Social Agency (formerly Basis Social) for this project, Level 5 qualifications have been referenced as being sufficient. ↩
-
A Level 4 or 5 qualification is a post-18 qualification, which is below degree level. ↩
-
Institute for Employment Studies (2022). Labour Market Statistics, February 2022. ↩
-
Office for National Statistics (2022). Employment in the UK: February 2022. ↩
-
Office for National Statistics (2022). Vacancies and jobs in the UK: February 2022. ↩
-
Institute for Employment Studies (2022). Labour Market Statistics, February 2022. ↩
-
Office for National Statistics (2025). VASC02: Vacancies by industry ↩
-
NHS Digital (2021). NHS Vacancy Statistics England April 2015 – September 2021 Experimental Statistics. ↩
-
Based on the CHDA salary uplift for Greater London (17%) and the difference between the highest and lowest salary advertised (20%) on the IAS website. ↩
-
Data on variation in regional pay is relatively sparse for healthcare professionals. The Annual Survey of Hours and Earnings (ASHE) provides details on median salaries of healthcare professionals in 11 UK regions. However, due to the relatively limited number of healthcare professionals in each region, the precision of the estimates are relatively low, so limited conclusions can be drawn from the data. Available at: Office for National Statistics. (2021). Earnings and hours worked, region by occupation by four-digit SOC: ASHE Table 15 ↩
-
Totaljobs. (2022). Disability Assessor Jobs ↩
-
The percentiles are likely to be higher if one only looked at percentiles HCP salaries outside London, but this data is not available through the ASHE (the regional income deciles for HCPs are sparsely-populated or non-existent due to small sample sizes). ↩
-
Incidentally, the highest salary offered is not available to paramedics, as paramedics are not eligible to become WCA assessors. ↩
-
Office for National Statistics. (2021). Earnings and hours worked, occupation by four-digit SOC: ASHE Table 14 ↩
-
Royal College of Nursing (2021). Employment Survey 2021. ↩
-
Ibid. ↩
-
Royal College of Nursing (2020). Building a Better Future for Nursing: RCN members have their say. ↩
-
Calculated as the total number of leavers in the year divided by the average number of FTE staff during the year. ↩
-
For each provider, the annual turnover rate was first calculated and then converted to an average monthly turnover rate per provider, per year. ↩
-
Data was only available from March to December 2018. ↩
-
Doctors employed for 2 to 6 months or non-doctors employed for 4 to 8 months. ↩
-
The analysis uses the US measure of skills and work activities from the Occupational Information Network (O*NET). O*NET also includes data on other measures such as knowledge, abilities and work context, but only skills and work activities are used for this analysis. ↩
-
As O*NET is based on US occupations, the first stage required was to convert the relevant US occupations to UK occupations. We did not have access to a full crosswalk between the US and UK occupational classification, but there was access to the online LMI For All tool which allows one to individually search for matches between UK and US occupational codes. ↩
-
The Big Thank You at King’s College Hospital NHS Foundation Trust ↩
-
Health and Wellbeing at Work 2021, Case studies; CIPD; 2021 ↩