Acute hepatitis B: national enhanced surveillance report January to September 2020
Updated 3 February 2026
Applies to England

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/acute-hepatitis-b-england-enhanced-surveillance-reports/acute-hepatitis-b-national-enhanced-surveillance-report-january-to-september-2020
Background
The quarterly reporting of enhanced molecular surveillance of acute hepatitis B is based on clinical reports of acute cases to UK Health Security Agency (UKHSA) being entered on HPZone and corresponding samples being submitted to UKHSA Blood Borne Virus Unit (BBVU) in the Virus Reference Department (VRD) at Colindale.
In 2016, VRD reintroduced anti hepatitis B core avidity testing alongside genotyping of samples from patients diagnosed with acute hepatitis B, a service which is offered free of charge.
Hospital microbiology and virology departments are requested to send samples to Colindale for confirmation, avidity testing and genotyping as part of the national enhanced surveillance of acute hepatitis B (see Acute hepatitis B: guide to national enhanced surveillance).
Following the reporting of clusters of acute hepatitis B in 2016, an HPZone context ‘Acute hepatitis B’ was added for monitoring of acute cases.
Impact of SARS-CoV-2 (COVID-19)
Following the first cases of SARS-CoV-2 detected in England at the end of January 2020, social and physical distancing measures were introduced in March, requiring people to stay at home, closing businesses and venues. These measures and the redeployment of health staff led to a reduction and/or re-configuration of testing among those at high risk of blood borne viruses and clinical serves providing care.
Causes of declines in testing and diagnoses are multifactorial: including but not restricted to deployment of staff, disruption to services, impact of social and physical distancing measures resulting in fewer opportunities for onward transmission, and disruption to laboratory consumables due to increases in demand during the pandemic.
Methods
Acute hepatitis B cases recorded in 2 different ways and entered on HPZone between January 2020 and September 2020 were extracted. HPZone Context ‘Acute Hepatitis B’ data includes personally identifiable information, which therefore allows for the rapid identification of cases and request of samples directly from laboratories for avidity and molecular characterisation at VRD, Colindale.
HPZone data without personally identifiable information (HPZone dashboard) on acute cases was matched to HPZone context data using a unique identifier. The ‘Acute Hepatitis B’ Context data was matched to laboratory testing data from the VRD using Microsoft Access algorithms comparing combinations of the following variables: surname, first name, date of birth, sex, and NHS number.
Results
Between January and September 2020, 155 cases of acute hepatitis B were reported onto HPZone dashboard across England (confirmed, probable and possible), the number of reported cases is lower than observed in previous years, likely to be associated with the impact of the SARS-CoV-2 pandemic.
Overall, the cases entered on HPZone dashboard have been declining since 2011 from 513 compared to 287 in 2019. Monthly cases since 2010 in England are shown in Figure 1. In 2015 there was a slight increase in cases likely caused by the outbreak of acute hepatitis B in men who have sex with men who identify as heterosexual.
Figure 1. Cumulative cases of acute hepatitis B in England entered on HPZone dashboard 2010 to September 2020. (Please be aware that 2020 data is provisional)
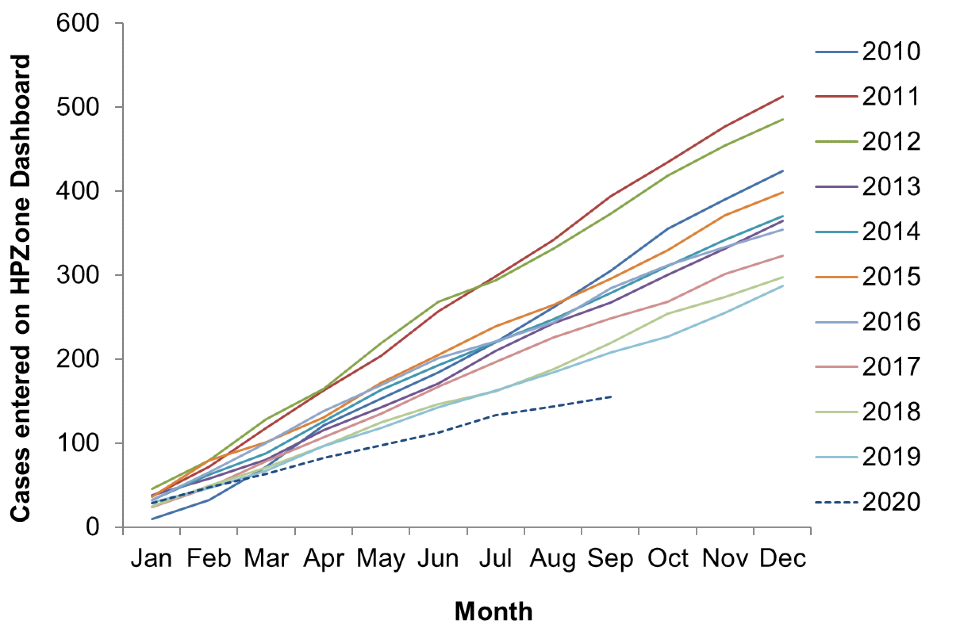
Figure 2. January to September 2020 cases entered onto HPZone dashboard. The line graph (right axis) shows the proportion of HPZone context cases that had a sample forwarded to the VRD
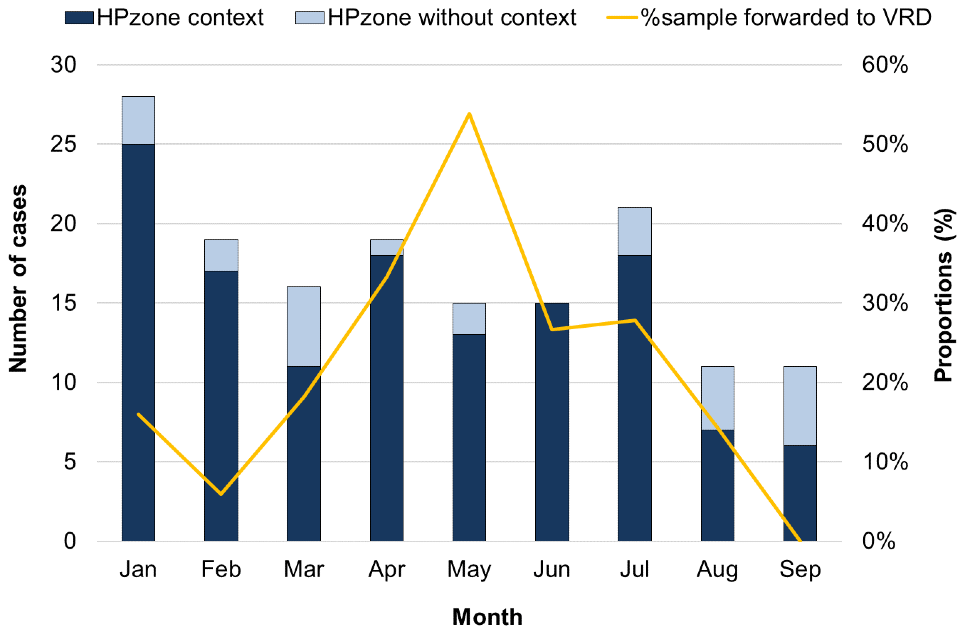
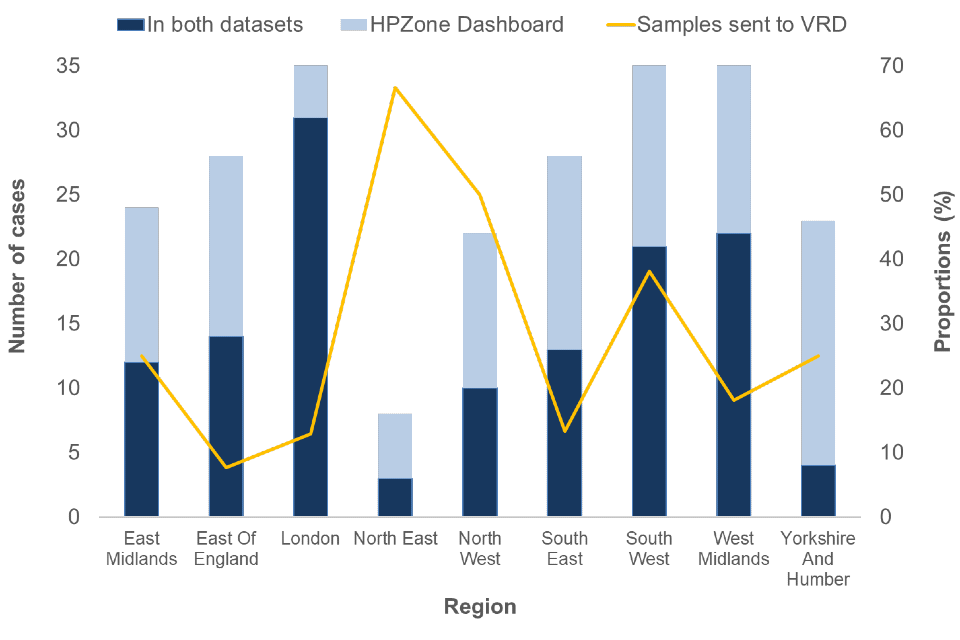
Figure 3. January to September 2020 cases entered onto HPZone Context and/or entered onto HPZone dashboard by UKHSA regions. The line graph (right axis) shows the proportion of HPZone context cases that had a sample forwarded to the VRD
For the 2020 January to September HPZone context data set and the 2020 January to September HPZone dashboard data set, age and sex was well reported (>99.4%). Where sex was known males accounted for 69% of cases (153 out of 155). The median age of persons with acute HBV was 41 years old (IQR: 28 to 53): 43 (IQR: 30 to 57) for males and 34 (IQR: 22 to 50) for females. The age distribution by sex is presented in Table 1. The highest proportion of cases were in the 25 to 34 and 35 to 44 years age groups. The highest proportion in males was in the 35 to 44 year group, whilst in females the highest proportion was among those between 15 and 24 years of age.
Table 1. Number and proportion of acute HBV cases from HPZone dashboard by sex and age group during January to September 2020
| Age group | Female | Male | Unknown | Total |
|---|---|---|---|---|
| Under 15 | 1 (2.2) | 4 (3.7) | 0 | 5 (3.2) |
| 15 to 24 | 13 (28.3) | 12 (11.2) | 0 | 25 (16.1) |
| 25 to 34 | 11 (23.9) | 18 (16.8) | 1 (100) | 30 (19.4) |
| 35 to 44 | 6 (13.0) | 24 (22.4) | 0 | 30 (19.4) |
| 45 to 54 | 10 (21.7) | 17 (15.9) | 1 (100) | 28 (18.1) |
| 55 to 64 | 2 (4.3) | 18 (16.8) | 0 | 20 (12.9) |
| 65 and over | 3 (6.5) | 14 (13.1) | 0 | 17 (11.0) |
| Total: | 4 | 107 | 2 | 155 |
Avidity testing and molecular characterisation investigations were undertaken on samples linked to cases to confirm the acute hepatitis B diagnosis with additional genotyping and phylogenetic analysis to inform on the diversity of the circulating viruses.
Of the 54 samples submitted to the VRD as part of the enhanced surveillance programme, 9 (17%) samples were confirmed to be from individuals with chronic hepatitis B and 26 (48%) were confirmed to be from individuals with acute hepatitis B infection. The avidity testing in the remaining 17 samples was classified as undetermined where it was not possible to confidently assign an HBV infection status and 2 samples were not tested.
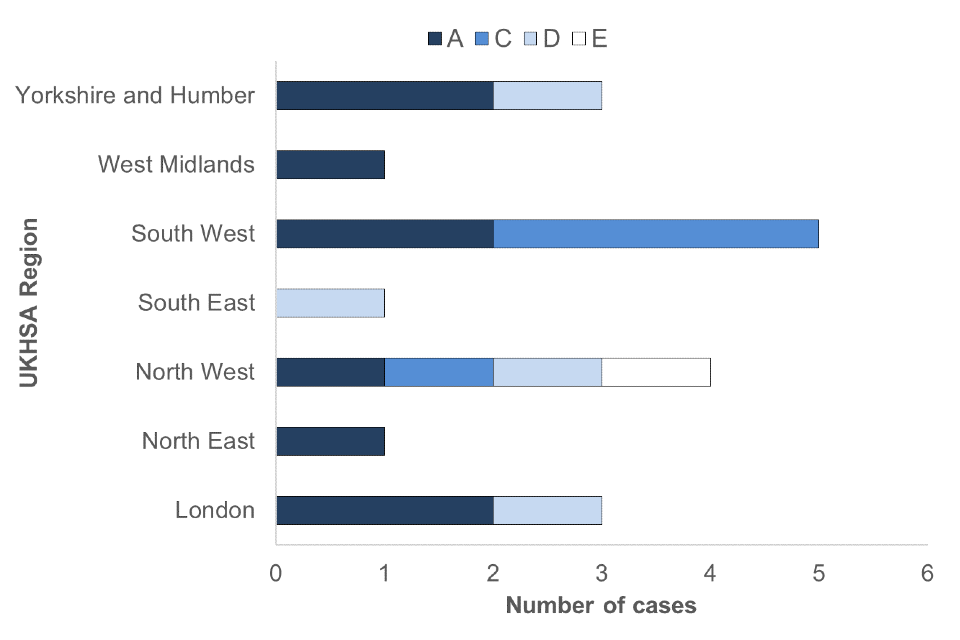
A total of 20 confirmed acute cases could be genotyped during January to September 2020. The distribution of genotypes is shown in Table 2. Consistent with trends seen in 2018 and 2019, genotype A was the most commonly reported genotype with 55.0% of cases (see Acute Hepatitis B (England): annual report for 2018). Additional sub genotype analysis of the A viruses indicated 3 to be A1 and 8 to be A2. The distribution of genotypes seen in UKHSA regions is shown in Figure 4.
Table 2. Genotype distribution and proportions of acute hepatitis B cases tested at VRD in January to September 2020
| Acute genotype | Number of cases | Proportion of cases |
|---|---|---|
| A | 11 | 55.0 |
| B | 0 | 0.0 |
| C | 4 | 20.0 |
| D | 4 | 20.0 |
| E | 1 | 5.0 |
| F | 0 | 0.0 |
| Unknown | 6 | – |
| Total: | 26 | – |
Figure 4. Genotypes of acute samples sent to VRD by UKHSA region
Discussion
Quarterly publication of enhanced molecular surveillance using matched HPZone and reference laboratory confirmatory and typing data with a regional breakdown allows real-time monitoring of acute hepatitis B transmission. The number of acute hepatitis B cases in January to September 2020 remained low and consistent with annual trends for the same timeframe. Molecular analysis provides insight into the current hepatitis B genotypes circulating in England, although interpretation is limited by the small proportion of samples submitted to VRD. The A2 ‘prisoner variant’ is one of the most common strains and is known to be well-established in the UK MSM population.
Other genotypes can indicate a geographical origin which can help provide an understanding of sources of infection and transmission routes. For example, genotype D is associated with South Asia. Timely assignment of cases to the HPZone context and improved submission of samples for molecular characterisation will allow for more comprehensive monitoring of acute hepatitis B infection in England.