National norovirus and rotavirus report, week 43 report: data up to week 41 (16 October 2022)
Updated 10 August 2023
Applies to England

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/statistics/national-norovirus-and-rotavirus-surveillance-reports-2022-to-2023-season/national-norovirus-and-rotavirus-report-week-43-report-data-up-to-week-41-16-october-2022
This weekly report covers the 2 week period between 3 and 16 October 2022 (reporting weeks 40 and 41, 2022) and is the second Official Statistics report of the 2022/2023 season.
Data reported here provide a summary of norovirus and rotavirus activity (including EV outbreaks) in England up to reporting week 41 of the 2022/2023 season.
The main messages of this report are:
- The UK Health Security Agency (UKHSA) has relaunched the Official Statistics National Norovirus and Rotavirus Report after it was temporarily suspended and replaced by the National Norovirus and Rotavirus Bulletin between December 2020 and October 2022 to continue to provide an overview of norovirus and rotavirus activity in England.
- Norovirus laboratory reporting has increased in recent weeks, however reported enteric virus (EV) outbreaks have been lower than the 5-season average of the same period (2014/2015 to 2018/2019).
- Norovirus laboratory reports during weeks 40 and 41 of the 2022/2023 season were 19% higher than the 5-season average of the same period prior to the emergence of COVID-19 (2014/2015 to 2018/2019).
- During weeks 40 to 41, 2022, laboratory reports of rotavirus were 22% higher than the 5-season average (2014/2015 to 2018/2019) for the same 2-week period pre-COVID-19.
- The number of reported enteric virus (EV) outbreaks has been stable in recent weeks (40 and 41) but overall remains 33% lower than the 5-season average of the same 2-week period before the pandemic.
- So far this season, reports of EV outbreaks in hospital and care home settings remain notably lower than during the same period in the 5 seasons pre-COVID-19, however EV outbreaks in educational settings have returned to comparable levels for this point in the season.
- During the 2022/2023 season to date the majority (69%) of samples characterised were norovirus Genogroup 2 (GII) of which the most frequently identified strain was genotype GII.4 (20%), however due to low numbers of samples submitted for molecular surveillance in the early part of the season, the data should be interpreted with caution.
Background
No single surveillance system fully captures national changes in norovirus or rotavirus activity; therefore this report presents data from 4 systems which collectively describe recent trends. Data is reported by season rather than calendar year, in order to capture the winter peak of activity in one reporting period (please see interpretation of trends section for more details).
The coronavirus (COVID-19) pandemic impacted activity across many gastrointestinal pathogen surveillance indicators for England in 2020 and 2021, and reduced norovirus reporting continued into 2022. The reasons for the reduction in norovirus reporting are considered to be multifactorial. The pandemic led to many changes which have likely had a negative impact on surveillance indicators, but which have likely also resulted in reduced norovirus and rotavirus (and other enteric virus) transmission. Following the lifting of COVID-19 restrictions norovirus and rotavirus activity began to increase but has not followed the pre-COVID-19 seasonal trends (based on the 5-season period of the 2014/2015 to 2018/2019 seasons, data covering this time period is available at National norovirus and rotavirus bulletins 2021 to 2022: management information).
Following the introduction of the rotavirus vaccine in July 2013 the total number of laboratory-confirmed rotavirus infections each season has remained low compared to the pre-vaccine period. A 77% decrease in laboratory-confirmed rotavirus infections in infants was observed in the first season following vaccine introduction (1).
UKHSA routinely undertakes norovirus characterisation as part of national surveillance to monitor the diversity of circulating strains. This molecular surveillance enables detection of novel strains or emergence of existing strains that could lead to strain replacement event and which have previously been associated with a temporal shift in norovirus activity (2). Norovirus activity varies from season to season and therefore differences will be observed between every season.
Worldwide the most commonly detected norovirus genotype is genogroup II- genotype 4 (GII.4). Historically between 1995 and 2013 there have been 5 global GII.4 strain replacements events (3, 4). Since the winter of the 2012/2013 season and prior to the emergence of COVID-19 in England the most frequently detected strain was Norovirus/GII.4/Sydney/2012 or GII.4 Sydney2012-like variants (5).
To enable effective molecular surveillance, it is crucial that samples are obtained from suspected norovirus cases or outbreaks for laboratory confirmation and then norovirus-positive samples are referred on to the Enteric Virus Unit (EVU) for characterisation.
Laboratory surveillance
Data presented here is derived from the Second-Generation Surveillance System (SGSS). Please see data sources and reporting caveats sections for more information, for guidance on interpretation of trends and the impact of the COVID-19 pandemic.
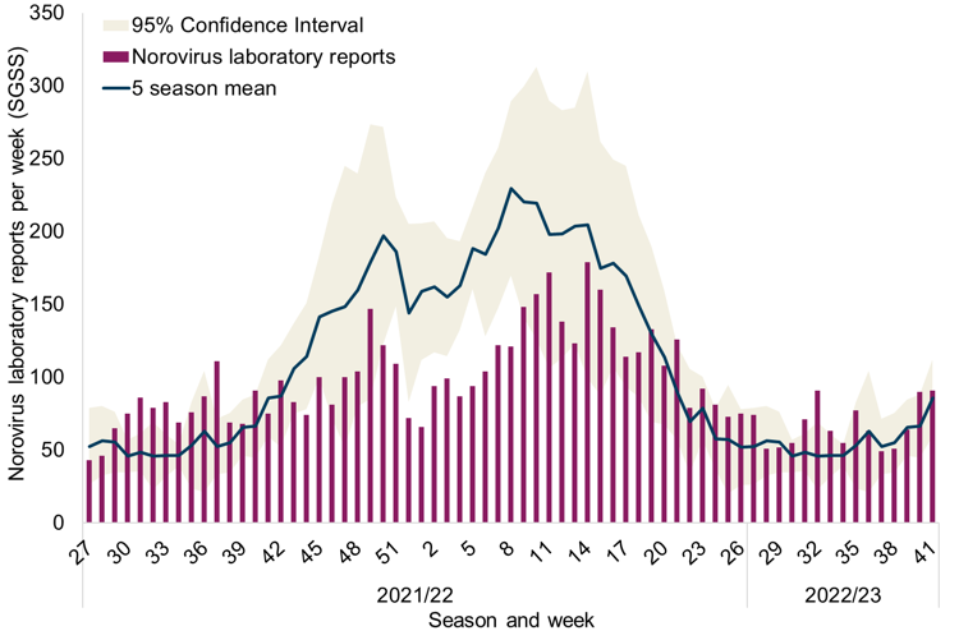
Following a sustained period of unusually low activity from March of the 2019/2020 season and throughout the 2020/2021 season norovirus reporting began to increase from week 25 of 2021(data covering this period is available at National norovirus and rotavirus bulletins 2021 to 2022: management information), although not returning to the overall seasonal trend observed pre-pandemic during the 2021/2022 season. So far the weekly number of norovirus laboratory reports has fluctuated week to week during the 2022/2023 season (Figure 1). It is likely that unusual norovirus activity will continue throughout the 2022/2023 season.
This season the cumulative number of positive norovirus laboratory reports in England to week 41 (997 laboratory reports) was 19% higher than the 5-season average for the same period prior to the pandemic (2014/2015 to 2018/2019) (838 laboratory reports).
Overall, norovirus activity increased during weeks 40 and 41 and total norovirus laboratory reports during this period (181 laboratory reports) were 19% higher than the 5-season average (152 laboratory reports) for the same 2 week period (Figure 1).
Figure 1. Norovirus laboratory reports in England by week during 2021/2022 and 2022/2023 seasons, compared to 5-season average
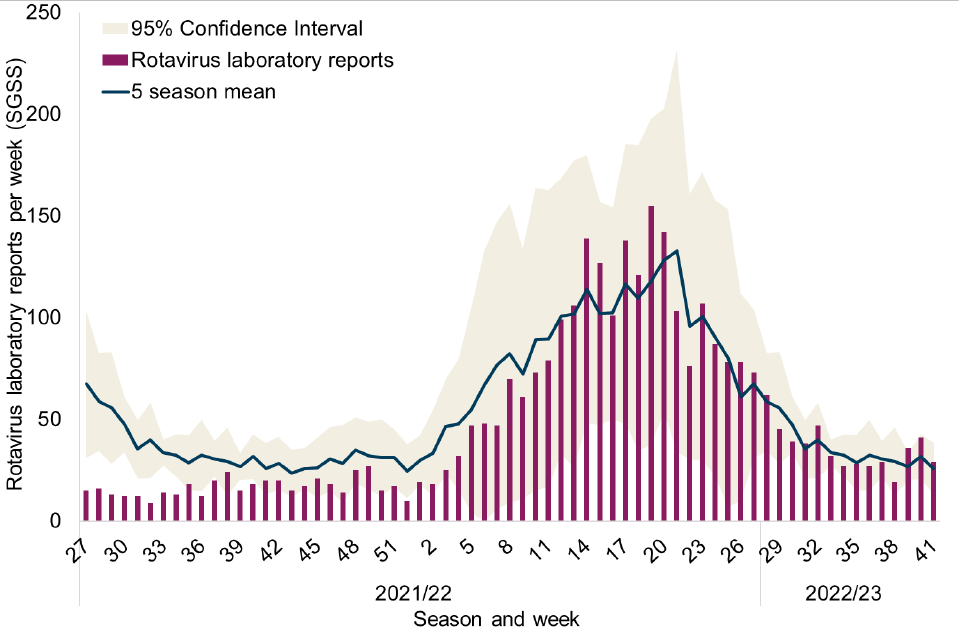
Similar to norovirus there was a notable reduction in rotavirus activity from March 2020 onwards. Reported rotavirus activity remained low throughout the whole 2020/2021 season (data covering this period is available at National norovirus and rotavirus bulletins 2021 to 2022: management information) and into the first half of the 2021/2022 season. Reporting returned to levels comparable to the 5-season average of the same period pre-COVID-19 in 2022 (Figure 2), generally following the historical pre-COVID-19 seasonal trend from week 13 onwards.
The cumulative number of positive rotavirus laboratory reports in England to week 41 of the current season (572 laboratory reports) was comparable to the 5-season average (2014/2015 to 2018/2019, post-vaccine and pre-COVID-19) for the same period (575 laboratory reports).
Overall rotavirus activity for the 2-week period of weeks 40 and 41, 2022 (70 laboratory reports) was 22% higher than the 5-season average (57 laboratory reports) for the same period.
Figure 2. Rotavirus laboratory reports in England by week during 2021/2022 and 2022/2023 seasons, compared to 5-season average
Outbreak surveillance
Data presented here is derived from HPZone and the Hospital Norovirus Outbreak Reporting System (HNORS). Please see data sources and reporting caveats sections for more information, for guidance on interpretation of trends and the impact of the COVID-19 pandemic.
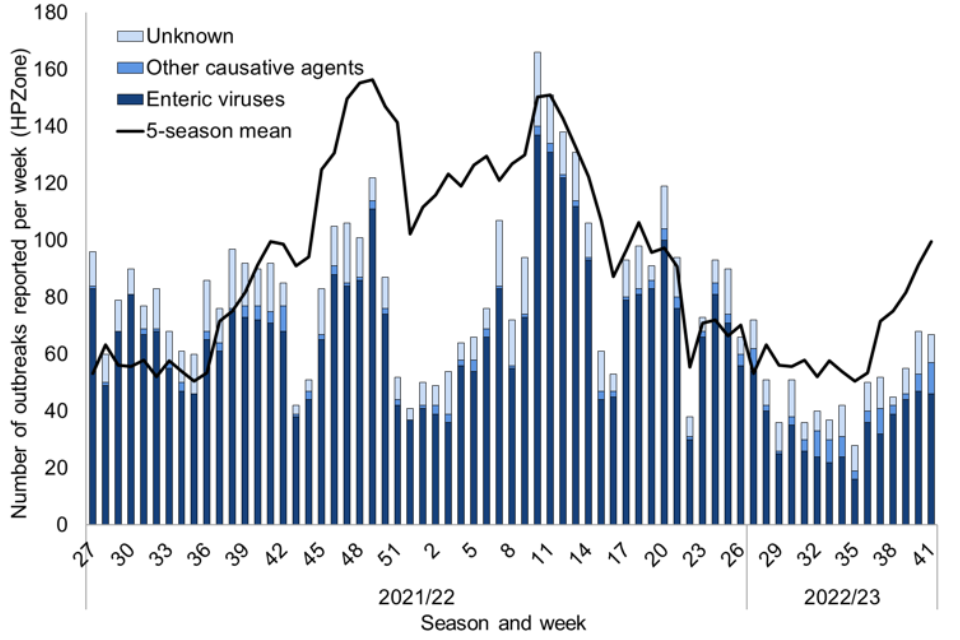
There was also a substantial and sustained drop in the number of EV outbreaks reported to national surveillance following the emergence of COVID-19 in March 2020, with an 83% decrease in total reported EV outbreaks across the entire 2020/2021 season (data covering this period is available at National norovirus and rotavirus bulletins 2021 to 2022: management information) compared to the pre-pandemic 5-season average (2014/2015 to 2018/2019). Across the 2021/2022 season and into the 2022/2023 season the number of reported EV outbreaks varied in comparison with the 5-season average.
Up to week 41 of the 2022/2023 season the cumulative number of EV outbreaks reported to HPZone was 33% lower than the pre-pandemic 5-season average (2014/2015 to 2018/2019), 510 and 755 outbreaks respectively Figure 3).
Although the total number of reported EV outbreaks increased during weeks 40 and 41 of the 2022/2023 season (93 outbreaks) compared to the previous 2-week period of weeks 38 and 39 (83 outbreaks), the total number of reported EV outbreaks was 40% lower than the 5-season average for the same 2-week period (154 outbreaks).
Figure 3. Gastroenteritis outbreak reports by causative agent and week of declaration in England, 2021/2022 and 2022/2023 seasons compared to the 5-season average of total reported outbreaks
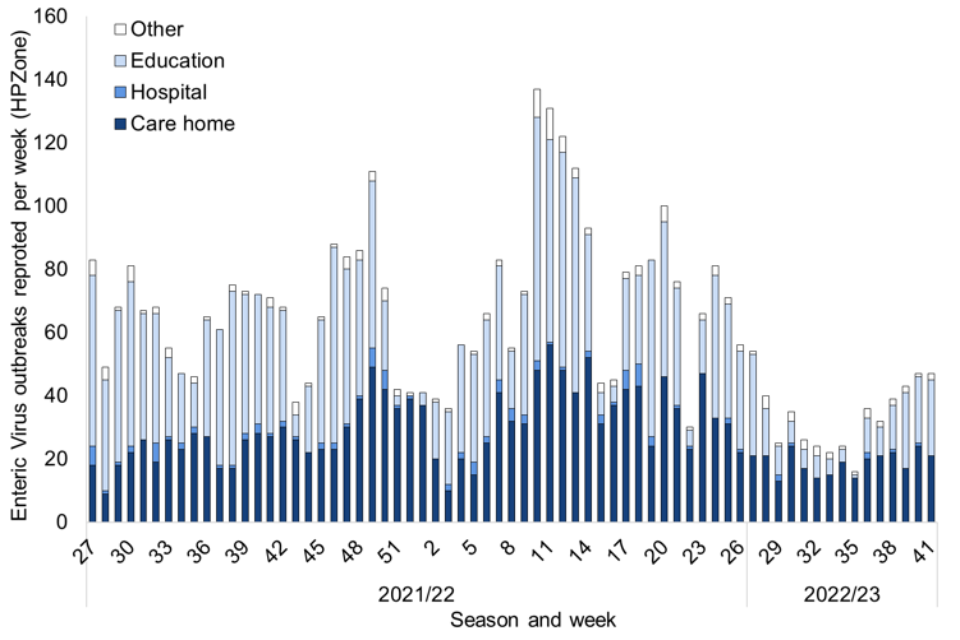
During the 2020/2021 and 2021/2022 seasons there was a shift in the most frequently reported settings of EV outbreaks. Prior to the emergence of COVID-19 the majority of outbreaks reported to HPZone were reported in hospital and care home settings, however in the 2020/2021 and 2021/2022 seasons outbreaks were most frequently reported in educational settings (data covering the 2020/2021 period is available at National norovirus and rotavirus bulletins 2021 to 2022: management information).
In the 2 week period of weeks 40 and 41, 2022 the majority of reported EV outbreaks (all suspected or confirmed as norovirus) have occurred in educational and care home settings, both 48% (Figure 4). During this 2-week period the number of outbreaks in educational settings remained at levels comparable to the 5-season average (2014/2015 to 2018/2019), however the number of outbreaks reported in care home settings was lower than the 5-season average pre-COVID-19.
Figure 4. Enteric virus outbreaks reported to HPZone in England by setting during the 2021/2022 and 2022/2023 seasons
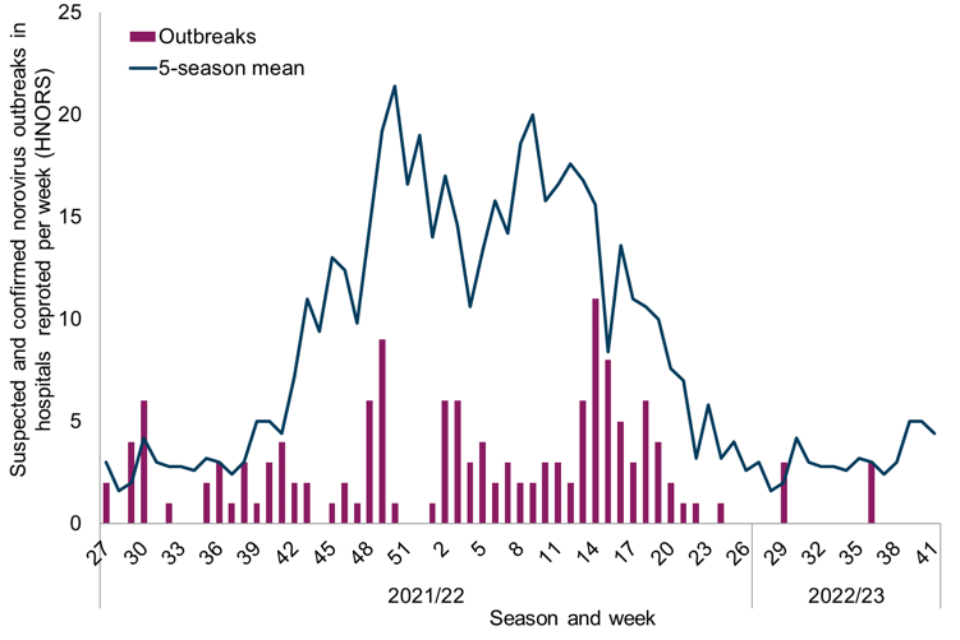
Throughout the 2021/2022 and 2022/2023 seasons to date, reports of suspected and confirmed norovirus outbreaks in hospitals (captured by HNORS), have been substantially lower than the 5-season average. Up to week 41 of the 2022/2023 season 6 outbreaks have been reported (Figure 5), an 88% decline in reporting compared to the pre-COVID-19 5 season average for the same period (48 outbreaks). All 6 outbreaks were laboratory confirmed as norovirus.
Figure 5. Suspected and confirmed norovirus outbreaks reported to HNORS in England by week of occurrence during the 2021/2022 and 2022/2023 seasons compared to the 5-season average
Molecular surveillance for norovirus
Data presented here is provided by UKHSA’s Enteric Virus Unit (EVU). The drop in norovirus reporting to national surveillance during the 2019/2020 and 2020/2021 seasons lead to a period of low referral of norovirus-positive samples for characterisation, therefore this data is not presented. Please see data sources and reporting caveats sections for more information, for guidance on interpretation of trends and the impact of the COVID-19 pandemic.
During the 2021/2022 season, 572 norovirus positive samples were characterised of which 90% were genogroup 2 (GII), 8% were genogroup one (GI) and 2% were mixed. The 3 most frequent norovirus GII genotypes identified were GII.4 (48%), GII.3 (13%) and GII.2 (10%) and the most frequently identified norovirus GI genotypes were GI.3 (3%) and GI.6 (3%).
Of the 158 norovirus positive samples characterised during the 2022/2023 season to date, 69% (108 out of 158) were genogroup 2 (GII) 30% (48 out of 158) were genogroup 1 (GI) and 1% were mixed (2 out of 158). The 3 most frequent norovirus GII genotypes identified were GII.4 (20%), GII.6 (13%) and GII.17 (13%) and the most frequently identified norovirus GI genotypes were GI.3 (13%) and GI.2 (10%).
Data sources
- The Second-Generation Surveillance System (SGSS) is the national laboratory reporting system, recording positive laboratory reports of norovirus and rotavirus.
- The Hospital Norovirus Outbreak Reporting System (HNORS) is a web-based scheme for reporting suspected and confirmed norovirus outbreaks in Acute NHS Trust hospitals, and captures information on the disruptive impact these outbreaks have in hospital settings.
- HPZone is a web-based case and outbreak management system used by Health Protection Teams (HPTs) to record outbreaks they are notified of and investigate. In England, suspected and confirmed EV outbreaks (norovirus, rotavirus, astrovirus and sapovirus) are reported as ‘Gastroenteritis’ outbreaks.
- Norovirus characterisation data is produced by the Enteric Virus Unit and is used to monitor the diversity of circulating strains of norovirus in England.
Reporting caveats
Interpretation of trends
In order to capture the winter peak of activity in the reporting period the norovirus and rotavirus season runs from week 27 in year 1 to week 26 in year 2, that is, week 27 2021 to week 26 2022, July to June. The 2021/2022 and 2022/2023 seasons are compared to the 5-season average calculated from the 5-season period of 2014/2015 to 2018/2019. The 2019/2020 and 2020/2021 seasons are not included in this calculation due to the adverse impact of the emergence of COVID-19 on surveillance part way through the 2019/2020 season and the continued impact into the 2021/2022 season. In years with a week 53 (2015 and 2020) data is combined with week 52 data to avoid distortion of the figure.
Under-ascertainment is a recognised challenge in enteric virus surveillance with sampling, testing and reporting criteria known to vary by region. In addition, samples for microbiological confirmation are collected in a small proportion of community outbreaks. Therefore, this report provides an overview of enteric virus activity across England and data should be interpreted with caution.
All surveillance data included in this report is extracted from live reporting systems, is subject to a reporting delay, and the number reported in the most recent weeks may rise further as more reports are received. Therefore, data pertaining to the most recent 2 weeks is not included.
Impact of COVID-19 pandemic on surveillance
The UK Health Security Agency (UKHSA) has relaunched the Official Statistics National Norovirus and Rotavirus Report after it was temporarily suspended due to quality issues with the data from the 4 aforementioned data sources during the COVID-19 pandemic period. Additional analyses of this data has been undertaken and demonstrate the quality of this data is now comparable with the data collected before the pandemic and therefore reporting can resume as an Official Statistic. Between December 2020 and October 2022 the report was replaced by the National Norovirus and Rotavirus Bulletin to ensure an overview of norovirus and rotavirus activity in England continued to be available to the public (data covering the periods 2020/2021 and 2021/2022 is available at National norovirus and rotavirus bulletins 2020 to 2021: management information and National norovirus and rotavirus bulletins 2021 to 2022: management information ).
It is likely that the interventions implemented to control COVID-19 led to a reduction in enteric virus transmission. However, when considering the surveillance data reported here, the magnitude of the reduction is unlikely to be wholly attributable to these control measures alone. It is likely that other factors such as, but not limited to, changes in ascertainment, access to health care services and capacity for testing also contributed to the observed reduction due to changes in ascertainment and varied over time. Therefore, trends for the 2019/20, 2020/2021 and 2021/22 seasons should be interpreted with caution.
SGSS data
SGSS data is England only, week number is calculated from specimen date and location is based on laboratory geography. Norovirus data include faecal and lower Gastrointestinal tract specimen types only. Reporting may be subject to differences in regional ascertainment.
HPZone data
HPZone data utilises week of date of outbreak entry on to HPZone for analyses due to mandatory completion of the field. While this usually reflects the date of notification, batch reporting of outbreaks can occur.
Over the 5 seasons prior to the emergence of COVID-19 (2014/2015 to 2018/2019) an average of 86.1% of gastroenteritis outbreaks reported to HPZone were attributed to EVs (norovirus, rotavirus, sapovirus and astrovirus), 1.8% to other causative agents and 12.0% were of unknown cause. Of the outbreaks attributed to EVs, 98.4% were reported as suspected and confirmed norovirus outbreaks.
During the previous 5 seasons prior to the emergence of COVID-19 (2014/2015 to 2018/2019) 62.7% of all reported outbreaks attributed to EVs (norovirus, rotavirus, sapovirus and astrovirus), occurred in care home settings, 18.7% in educational settings, 13.0% in hospital settings and 5.6% in ‘other’ settings. Of the outbreaks attributed to EVs, 98.4% were reported as suspected and confirmed norovirus outbreaks. Only 13.7% of reported EV outbreaks were laboratory confirmed as norovirus during the previous 5 seasons.
HNORS data
HNORS reporting is voluntary, and variations may reflect differences in ascertainment or reporting criteria by region. National guidance recommends closure of the smallest possible unit in hospitals. Therefore, not all outbreaks reported to HNORS result in whole ward closure (some closures are restricted to bays only) and not all suspected cases are tested. Additionally, not all suspected cases are tested for norovirus, often only a proportion of individuals will be tested in any suspected outbreak.
Week number is calculated from date of first case onset for HNORS data. During the 5 seasons prior to the emergence of COVID-19 (2014/2015 to 2018/2019) 73.6% of outbreaks reported to HNORS were laboratory confirmed as norovirus.
From May to October 2019 and during February 2020 the HNORS website was temporarily offline. The reliance on manual data collation during this period may have negatively impacted ascertainment so trends should be interpreted with caution.
Norovirus characterisation data
Norovirus genotype and GII.4 strain characterisation data from the reference laboratory are subject to a reporting delay, and the numbers reported in any week may rise further additional characterisation data become available.
References
- Atchison and others. ‘Rapid declines in age group–specific rotavirus infection and acute gastroenteritis among vaccinated and unvaccinated individuals within 1 year of rotavirus vaccine introduction in England and Wales’ , The Journal of Infectious Diseases: volume 213, pages 243 to 249 (viewed on 17 October 2022)
- Allen and others. ‘Emergence of the GII-4 norovirus Sydney2012 strain in England, winter 2012–2013’, The Public Library of Science One, volume 2, article: e88978 (viewed on 17 October 2022)
- Allen and others. ‘Characterisation of a GII-4 norovirus variant-specific surface-exposed site involved in antibody binding’ Virology Journal, volume 6, article number: 150 (viewed on 17 October 2022)
- Zakikhany and others. ‘Molecular evolution of GII-4 Norovirus strains’ The Public Library of Science One, volume 7, article: e41625 (viewed on 17 October 2022)
- Ruis C and others. ‘The emerging GII.P16-GII.4 Sydney 2012 norovirus lineage is circulating worldwide, arose by late-2014 and contains polymerase changes that may increase virus transmission’ The Public Library of Science One, volume 6, article: e0179572 (viewed on 17 October 2022)
Further information
Further information about norovirus surveillance can be found at Norovirus: guidance, data and analysis.
Further information about rotavirus surveillance can be found at Rotavirus: guidance, data and analysis.
Acknowledgements
We are grateful to all who provided data used in this report, including NHS Infection Control and Prevention staff (HNORS users), UKHSA local (HPTs) and UKHSA regional teams (Field Services) and UKHSA Regional Public Health and Collaborating Laboratories.
This report was produced by the Gastrointestinal Infections & Food Safety (One Health) Division, UKHSA.
Please direct any queries or comments to NoroOBK@ukhsa.gov.uk.