SPI-M-O: Statement on daily contact testing, 3 March 2021
Updated 13 May 2022

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/spi-m-o-statement-on-daily-contact-testing-3-march-2021/spi-m-o-statement-on-daily-contact-testing-3-march-2021
Summary
1. Daily Contact Testing (DCT) involves the repeat, rapid testing of contacts of confirmed cases for a certain number of days with lateral flow tests (LFTs) and has the potential to be a helpful supplement to, or even a replacement for, less adaptive quarantine strategies.
2. Adherence to such testing strategies determines their effectiveness and needs careful consideration as any changes will alter the findings greatly, possibly to the point of negating any positive impact of DCT. Modelling and sensitivity analysis indicate that the impact of any policy is largely dependent on its acceptability among, and adherence from, the target population. Until these are known, the predictions of impact are very uncertain.
3. 3 modelling groups have considered analyses looking at various aspects of DCT strategies. The possible impacts of DCT for different scenarios are summarised here.
| Scenario | Result |
|---|---|
| An index case tests positive. 3 days later, their contact has been traced and receives a supply of lateral flow tests. | 5 days of sequential testing of the contact matches the effectiveness of 10-days quarantine, if both interventions have the same adherence. (See paragraph 11 and Figure 1). |
| An index case tests positive. On the same day a contact is traced and receives a supply of lateral flow tests. | 7 days of sequential testing at approximately 20% higher adherence matches the effectiveness of 10-days quarantine. (See paragraph 13 and Figure 2). |
| An index case tests positive. Their household is known, and a contact in another household is also identified. The status quo is that both the index case’s household and the other contact quarantine for 10 days. Can daily contact testing improve on the status quo in terms of reducing epidemic growth? | Daily testing of the contact in a different household diminishes the overall epidemic growth rate. There is marginal further slowing of the epidemic growth rate if daily contact testing of the index case’s household is performed in addition to the household’s 10-day quarantine. Replacing quarantine of the index case’s household with daily contact testing increases the epidemic growth rate. (See paragraphs 19 to 22 and Figures 4 and 5). |
| A school aims to minimise infections and school days missed amongst its pupils. | Combining twice weekly mass testing with daily testing of contacts can allow lower prevalence and lower numbers of school days missed, if both uptake and adherence are high. (See paragraph 29 and Figure 6). |
4. Key points from the analyses summarised here include the following.
- Assuming a three-day delay for contact notification and sending of test kits, 5 days of sequential testing may match the effectiveness of 10-day quarantine for the same level of adherence to each. If adherence was better using DCT than quarantine, then more transmission can be averted. Assuming no delay to testing and tracing (for example, testing conducted in a workplace) then greater adherence to DCT than to quarantine is needed to have the same impact on transmission.
- There is little benefit to additional days of sequential testing beyond a certain point.
- One or 2 sequential days of missed tests within a sequence of testing days do not make a large difference to the impact of DCT and could be mitigated against, assuming high levels of adherence.
- DCT has potential advantages of finding more contacts who may go on to become cases earlier, or asymptomatic cases, which can then enter the NHS Test and Trace system.
- DCT strategies could impact the wider growth rate of the epidemic. Assuming 100% adherence to isolation, quarantine, and DCT under certain scenarios, DCT strategies could be more effective than those currently in place for all options considered. The most effective policy at reducing growth rates would be both quarantine and DCT of household contacts; this is only very marginally more effective than quarantine only of household contacts and DCT with no quarantine of non-household contacts.
- DCT strategies could be more effective in reducing the growth rate of the epidemic compared to the current 10-day quarantine strategy for contacts. This could be the case even when both out-of-household and within-household contacts of a case take daily tests instead of quarantining.
- In a school-type setting, mass asymptomatic testing combined with sequential DCT are shown to be more effective at reducing infections than year-group bubble isolation in this analysis.
Context
5. Daily Contact Testing (DCT) involves the repeat, rapid testing of contacts of confirmed cases for a certain number of days with lateral flow tests (LFTs), with the aim of avoiding quarantine (if individuals continually test negative) and only isolating if in receipt of a positive test. As a result, it may provide opportunities to break chains of infection while also reducing absences from work or school, increase adherence to policies, and reduce personal, social, and financial costs for individuals. It could, however, accidentally lead to increased transmission in the case of false negative results or false reassurance, if poorly implemented.
6. The success of such a policy depends on the balance between false negatives against an increase in adherence compared to quarantine alone. The key considerations are as follows.
- How might the proportion of adherence with the complete daily contact testing influences the results?
- How might the speed of contact tracing and different testing schedules influence the results?
- How might the sensitivity of lateral flow tests affect the impact of DCT?
- How might institutional-led testing (such as in schools, workplaces) limit delays in the process or change the efficacy of daily testing?
7. Assumptions on people’s behaviour and willingness to adhere to guidance is critical to any testing strategy. If isolation is a very unattractive prospect, then there is little motivation to test. Behaviour means there is the potential for DCT to perform as well or better than current strategies, however, if adherence is poor, it could lead to worse outcomes than the status quo. Trials to understand behaviour with various DCT protocols, as with other testing strategies, are required and SPI-M-O understand some are ongoing. Until these in-progress trials report, the impact of comprehensive implementation cannot be predicted, without great uncertainty.
8. 3 models have considered the impacts of DCT strategies with different focuses.
General principles for sequential daily testing of contacts of confirmed cases
9. This analysis uses a model that has previously shown that daily contact tracing for 5 days with LFTs is only 12% less effective than 14-day quarantine in averting onward transmission (assuming 50% adherence to quarantine and 67% adherence to self-isolation upon symptoms or a positive test) [footnote 1]. This modelling compares DCT with LFTs to the current policy of 10-day quarantine while varying:
- levels of adherence to each strategy;
- the number of days of sequential tests;
- speed of contact tracing and any associated delays;
- the sensitivity of LFTs; and
- the impact of missing up to 2 sequential days of tests.
10. This model considers viral load trajectories over the course of an infection and estimates the amount of transmission prevented under each strategy, where the likelihood of detecting a case is determined by the Ct value at the time of testing. The effectiveness of a strategy is determined by the proportion of secondary case infectious periods that are spent in quarantine or isolation (following a positive test or symptoms), namely the transmission potential averted.
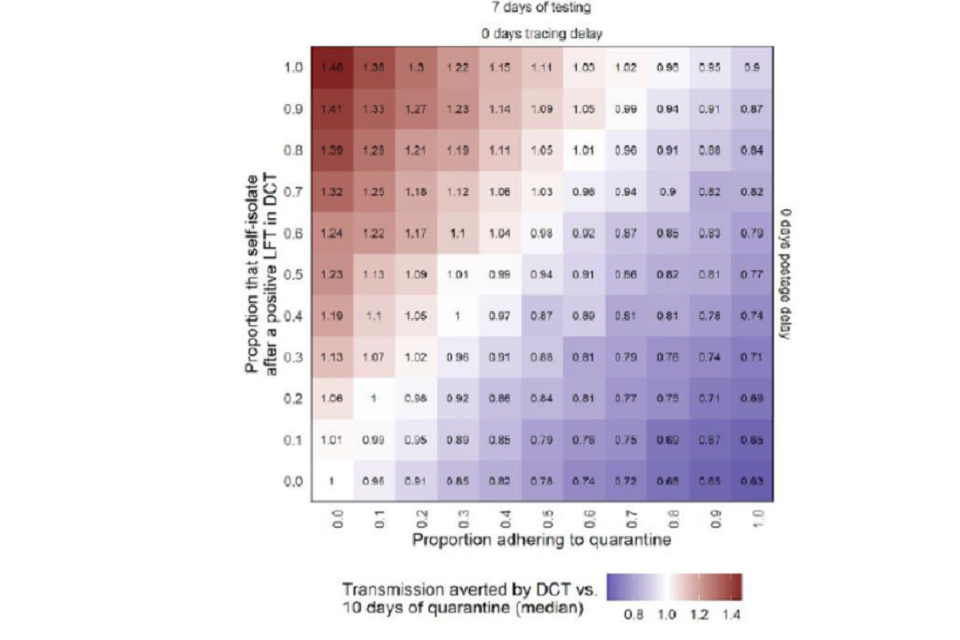
11. If it takes one day to notify contacts and 2 days to send out testing kits, 5 days of sequential testing may closely match the effectiveness of 10-day quarantine for the same level of adherence (Figure 1). If adherence was higher for DCT than for 10-day quarantine, more transmission could be averted. Under these conditions, there is little benefit to additional days of testing beyond five or seven days of DCT and this relation shifts depending on assumptions of test sensitivity. Greater increases in adherence to DCT would be required to exceed the effectiveness of 10-day quarantine, if LFT sensitivity was lower and vice versa.
12. Tracing and postage delays affect which day an infected individual’s test will detect their infection. Longer tracing delays cause a larger proportion of cases to be detected on the initial tests, whereas shortening these delays increases the relative contribution of later tests. Increased postage delays also increases the relative proportion of cases detected by initial tests [footnote 2]. Delays to notification and postage of tests result in individuals being tested later in their infection, with a greater relative proportion detected by the first few tests – shortening these delays increases the utility of more days of testing.
Figure 1: Relative amount of transmission potential averted by 5 days of daily contact testing (DCT) with lateral flow tests (LFTs), including delays due to notifying contacts and sending testing kits, compared to 10-day quarantine, varying by proportion of adherence to quarantine (x-axis) and to self-isolation following a positive test (y-axis). Red = more transmission averted by DCT; Blue = more transmission averted by quarantine.

Grid showing the relative transmission potential averted by 5 days of daily contact testing may be higher than that from 10 day quarantine if the proportion self-isolating following a positive test exceeds that adhering to quarantine, and vice versa.
13. Further conditions with immediate tracing and testing, for example, as might happen in a workplace have been considered. For DCT to match the effectiveness of 10-day quarantine in this situation, adherence to DCT for 7 days would need to be around 20% higher than that for a 10-day quarantine (Figure 2). In reducing contact tracing delays, there is an increase in transmission potential averted, however, more days of sequential testing are needed to ensure the same proportion of possible future cases are successfully detected.
Figure 2: Relative amount of transmission potential averted by 7 days of daily contact testing (DCT) with lateral flow tests (LFTs) on immediate notification compared to 10-day quarantine, varying by proportion of adherence to quarantine (x-axis) and to self-isolation following a positive test (y-axis). Red = more transmission averted by DCT; Blue = more transmission averted by quarantine.
Grid showing relative transmission potential averted by 7 days daily contact testing with no delays is similar/higher to that from 10 day quarantine if proportion self-isolating after a positive test is at least 20% higher than that adhering to quarantine
14. This same method can also consider, for example, missing up to 2 consecutive days in the sequential tests (replicating a weekend or gap in shift patterns). Figure 3 shows that missing these tests has less of an impact on transmission potential averted than taking tests for a longer time.
Figure 3: Relative amount of transmission potential averted by 3, 5, 7, or 10 days of daily contact testing (DCT) with lateral flow tests (LFTs) compared to 10-day quarantine, varying the numbers of tests missed (0 = purple, 1 = blue, 2 = yellow) and the number of days delay in tracing (0 = left, 1 = middle, 2 = right). A zero-day quarantine (no intervention beyond self-isolation on symptom onset) is also shown.
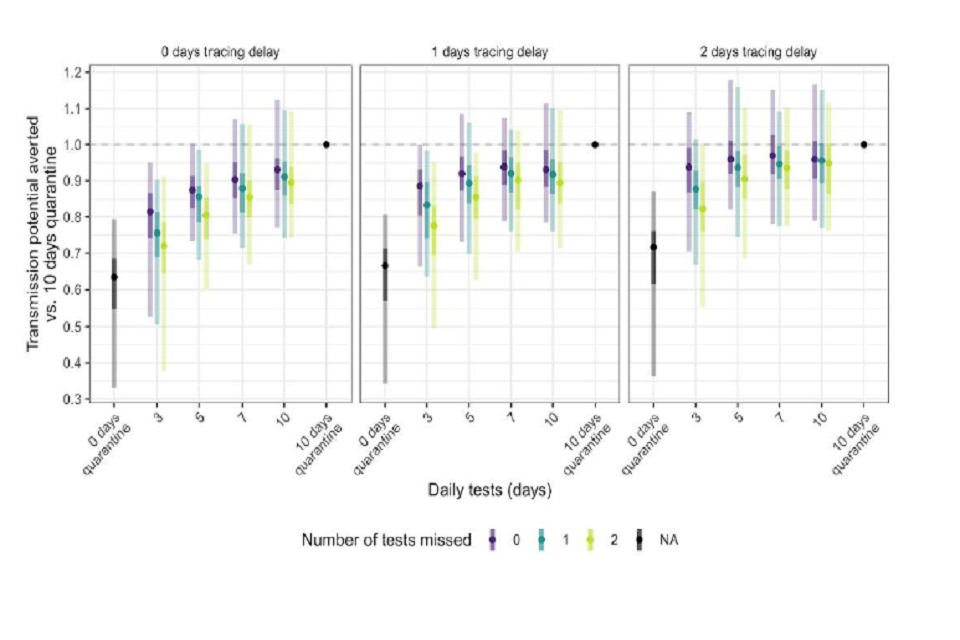
Scatterplots (with ranges) showing the relative transmission potential averted (vs. 10 day quarantine) rises with days of daily contact tracing. Missed tests reduce the transmission potential averted, with this loss smaller with longer daily testing.
15. This modelling relies on the assumption that there is a threshold for infectiousness and that that does not scale with increasing Ct values. This may not be the case and infectiousness may scale differently which would alter the results. Understanding the correlations between Ct values and PCR positive tests, LFT positive tests, and infectiousness is vital to improve this analysis. It also only considers shortening the infectious period, not how this may affect wider chains of transmission.
Comparison of impact on household and out-of-household contacts
16. Another model considered DCT that focused on household (HH) and out-of-HH contacts and assumes contacts that go on to be identified as cases through DCT are entered into the NHS Trace and Trace system with the subsequent tracing, testing, and if necessary, isolation of their contacts. This increases the overall number of cases and contacts identified and entering the system, with a potentially greater impact on wider transmission. Currently, contacts of cases must develop symptoms to be tested (same as anyone else) so contact tracing does not improve the case detection rate [footnote 3]; DCT however could. This model investigates these effects. The findings shown here, however, are not applicable to workplace or school settings, where contact tracing may be conducted outside of the NHS Test and Trace system.
17. In theory, DCT could identify contacts as positive slightly earlier in their infectious period than waiting for symptoms to develop as viral load, and therefore test sensitivity, rises prior to symptom onset. This also means that HH members of the contact-turned-case could quarantine sooner on average. The contact-turned-case also may be able to reduce within-HH transmission by self-isolating or social distancing from their HH members. DCT could also help to identify asymptomatic cases and allow further contact tracing.
18. The current status quo policy involves 10-day isolation of cases and 10-day quarantine of all contacts, both within-HH and out-of-HH. Even with 100% adherence to quarantine, not all transmission is blocked. Contacts of index cases quarantine inside households of individuals who themselves are not quarantining unless the contact in question develops symptoms later and becomes a new index case.
19. 3 DCT strategies for contacts within- and out-of-HH are considered.
- HH contacts quarantine only (no DCT); out-of-HH contacts DCT with no quarantine.
- HH contacts DCT and quarantine; out-of-HH contacts DCT with no quarantine.
- HH contacts DCT only (no quarantine); out-of-HH contacts DCT with no quarantine.
20. This model found that DCT strategies could be more effective compared to the status quo policy for all options, assuming 100% adherence to isolation, quarantine, and daily DCT in all scenarios. Under this assumption, DCT of out-of-household contacts, instead of quarantining these individuals, could lead to reduced simulated growth rates (Figures 4 and 5 – blue compared to all other colours).
21. The most effective strategy to reduce these estimated growth rates appears to be both the quarantine and DCT for HH contacts (Figure 4), although this is only very marginally more effective than only quarantining with no DCT of HH contacts, while out-of-HH contacts DCT and do not quarantine.
Figure 4: Estimated effects of simulated growth rates across a variety of DCT strategies compared to the current policy of 10-day isolation of cases and 10-day quarantine of all contacts (left). All other scenarios assume DCT for all contacts but quarantine for household contacts only.
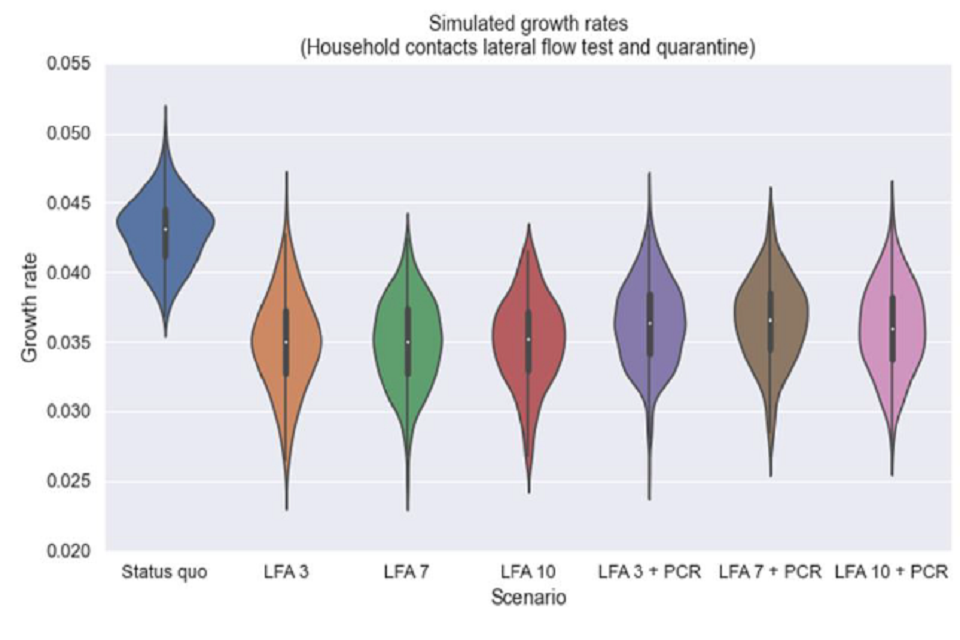
Violin plot showing daily contact testing for 3, 7 and 10 days (with household contacts also quarantining) may be more effective than the status quo, with lower simulated growth rates. Adding confirmatory PCRs slightly reduced effectiveness.
22. Even when HH contacts did not quarantine but did test daily (Figure 5), DCT scenarios showed lower median growth rates compared to the status quo policy, decreasing with duration of daily testing.
Figure 5: Estimated effects of simulated growth rates across a variety of DCT strategies compared to the current policy of 10-day isolation of cases and 10-day quarantine of all contacts (left). All other scenarios assume DCT for household contacts but no quarantine for either household or out-of-household contacts.
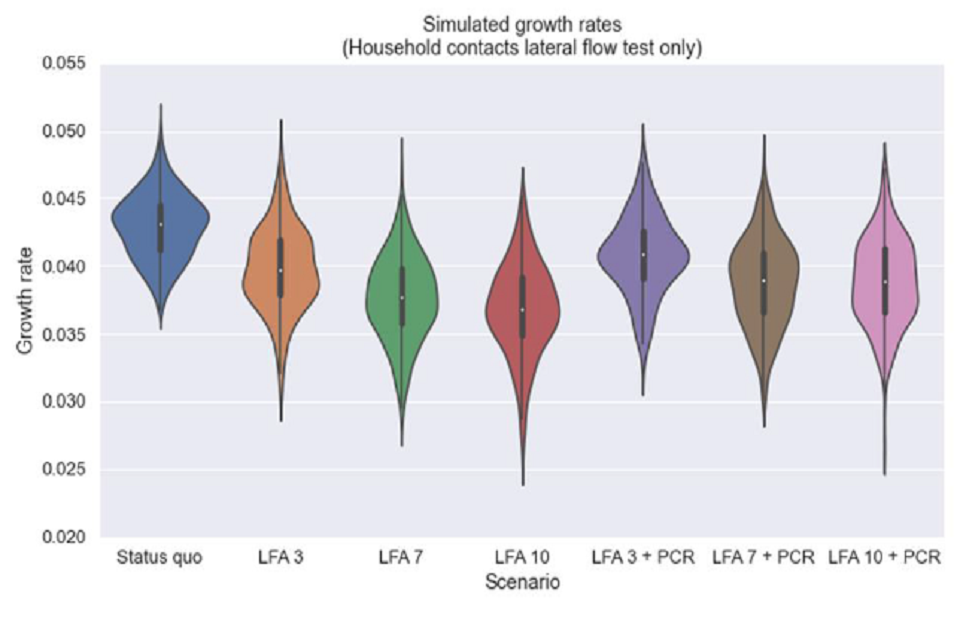
Violin plot showing daily contact testing for may be more effective than the status quo (but less than figure 4), with lower simulated growth rates. Longer periods of DCT are more effective, while adding confirmatory PCRs slightly reduced effectiveness.
23. The importance of the duration of sequential daily tests (whether 3, 7 or 10 days) depends on HH contact policy adopted:
- HH contacts DCT, no quarantine (as for out-of-HH contacts); longer durations of DCT are more effective (Figure 5 – red compared to green compared to orange), supporting analysis from another model (paragraph 13).
- HH contacts DCT and quarantine; duration of DCT makes little difference (Figure 4).
- HH contacts only quarantine, no DCT; duration of DCT makes little difference.
24. Taking these results in combination suggests that the duration of sequential LFTs is more important for HH contacts than for out-of-HH contacts when both are not quarantining.
25. For all HH contact strategies and DCT durations, requiring a confirmatory PCR test to initiate tracing the contacts of those testing positive using an LFT reduced effectiveness (Figures 4 and 5 – purple, brown, and pink compared to orange, green, and red).
Application of rapid testing strategies, including DCT, in school settings
26. As well as considering strategies that could be reflective of DCT in households and workplaces, another model has assessed the impact of different school reopening and testing strategies using LFTs on transmission and absences.
27. Previously, strategies using mass asymptomatic testing or sequential DCT alone were found to be less effective at reducing infections than isolating year-group bubbles but were effective at reducing absences.
28. In this analysis, however, mass asymptomatic testing combined with sequential DCT were shown to be more effective at reducing infections than year-group bubble isolation.
29. At 75% uptake (agreeing to participate in testing), a mass testing strategy alone appears less effective at reducing infections at all levels of adherence (tests actually taken at home) when compared to year-group isolation. Combining mass testing with year-group isolation was the most effective strategy for reducing infections, even at low levels of adherence, followed by mass testing with serial contact testing (Figure 6).
30. Mass testing in combination with either isolation or sequential contact testing can result in high levels of absences.
Figure 6: All plots: orange = isolation of year-group bubbles; blue = sequential daily contact testing; purple = weekly mass asymptomatic testing; green = combined sequential daily contact testing and mass asymptomatic testing; yellow = combined mass asymptomatic testing and year-group bubble isolation. It is assumed those who opt out of mass asymptomatic testing also opt out of sequential daily contact testing. (Left) The relationship between adherence to home tests with transmission, assuming 75% of pupils participate in rapid testing. (Right) The relationship between uptake of mass testing and mean days of school absences.
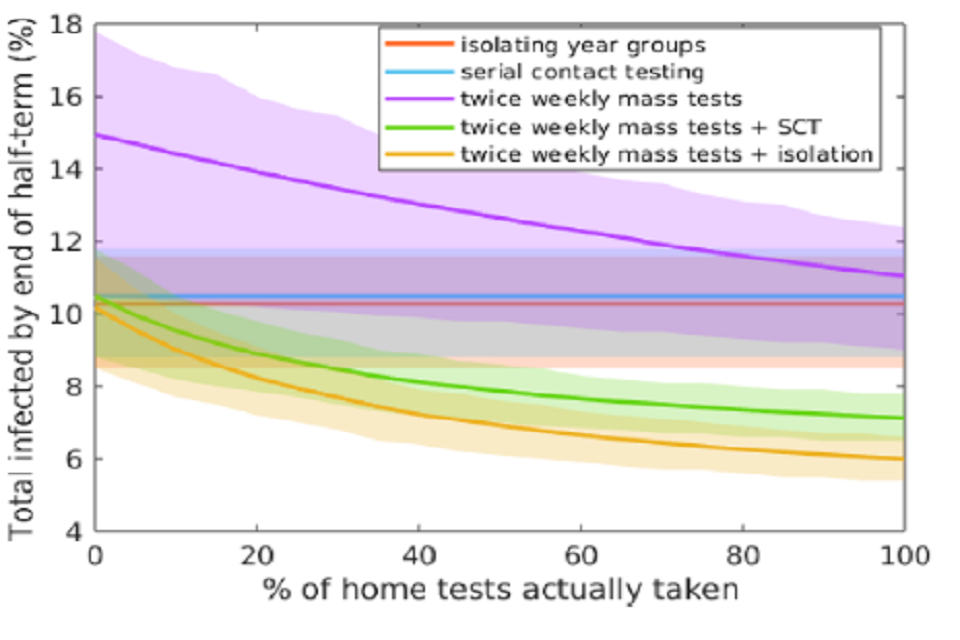
Line chart showing numbers infected by half-term falling with higher adherence to home testing for strategies involving mass testing, for 75% uptake. Mass testing in combination with year-group isolation or serial contact tracing are the most effective.
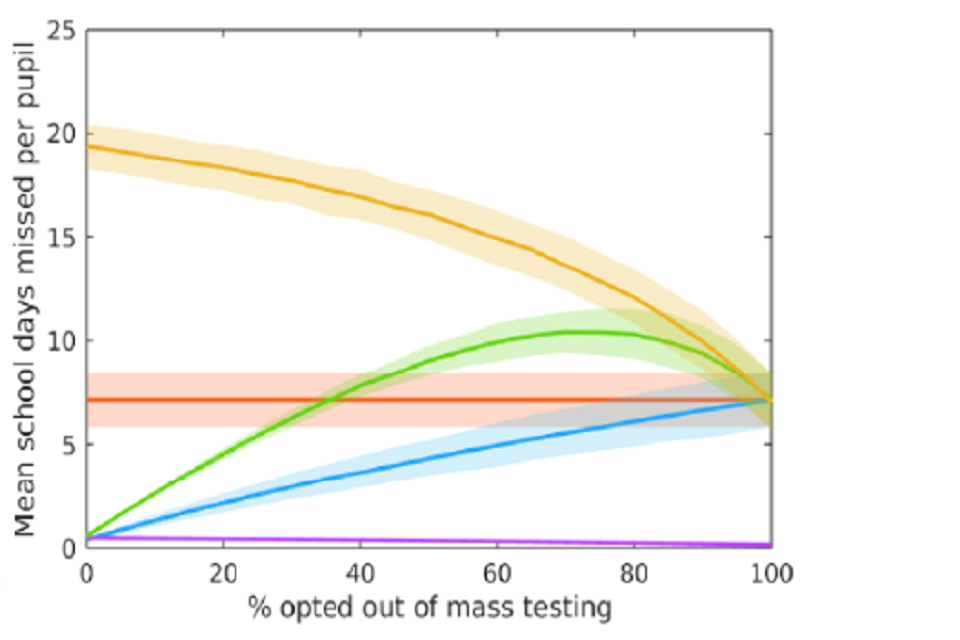
Line chart showing mean absence days per pupil are lowest for mass testing alone, and highest for mass testing in combination with year group isolation. There is a mixed relationship between uptake and absences across strategies.
31. These analyses show that rapid testing could be a helpful supplement but cannot replace existing measures.
Annex: PHIA framework of language for discussing probabilities

0 to 5% remote chance.
10% to 20% highly unlikely.
25% to 35% unlikely.
40% to 50% realistic possibility.
55% to 75% likely or probably.
80% to 90% highly likely.
95% to 100% almost certain.
References
-
Rapid testing strategies for traced contacts: comparing quarantine, quarantine and testing, and daily testing, 16 November 2020 ↩
-
This is due to the assumption that individuals not detected due to tracing delays are as yet unaware that they have been exposed and are hence considered infectious; those not detected due to a longer postage delay are assumed to be in isolation waiting for a test, and hence are considered not infectious. ↩
-
Footnote added for release: all else being equal. ↩