SAGE 38 minutes: Coronavirus (COVID-19) response, 21 May 2020
Published 19 June 2020

© Crown copyright 2020
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/sage-38-minutes-coronavirus-covid-19-response-21-may-2020/sage-38-minutes-coronavirus-covid-19-response-21-may-2020
Thirty-eighth SAGE meeting on COVID-19, 21 May 2020.
Held via Video Teleconference.
Summary
1. SAGE provided advice on sequencing of social distancing NPIs — see paragraphs 9 to 22.
2. SAGE advised that overall public adherence with social distancing measures will likely be diminished by HMG signalling its intent to release even some of the measures.
3. SAGE warned that if the test, trace and isolate (TTI) system begins operating when there is a relatively high level of incidence and prevalence of COVID-19 in the population, the system could very rapidly become overwhelmed.
Reasonable Worst-Case Scenario (RWCS)
4. SAGE reviewed again (as requested by Cabinet Office) the RWCS discussed at the last meeting in which behavioural and social interventions (BSI) easing on 1 June push R to 1.7 for 4 weeks, at which point reversal of BSI easing brings R down to 0.7 until incidence levels are similar to those at 1 June, and R returns to 1 for the rest of 2020.
5. SAGE reiterated that the RWCS model predicts a rise in R to 1.7 due to a lack of rapid detection of increased incidence in the population. Early warning signals, as well as an effective TTI programme, should be designed to prevent R rising to this level (or above 1).
6. SAGE advised that flexible localised capacity planning is required within the NHS to enable it to respond to rises in R.
7. SAGE cautioned that other scenarios, such as a rise in R to 1.2, could be more difficult to detect, and over time lead to a gradual increase in hospitalisations and deaths, and that this scenario should also be planned for.
8. SAGE approved the RWCS paper once changes were made.
Actions:
- SPI-M to update RWCS to include caveats on a) detecting incidences quickly and b) different effects of R above 1, both low as well as high values, so RWCS can be incorporated in return on Cabinet Office commission (by 22 May)
- Welsh Government to reconcile its modelling with SAGE-endorsed RWCS
Sequencing of social distancing NPIs
Situation update
9. The best estimate of R in the UK is between 0.7 and 1.0. While it is highly likely to be under 1, it could be close to it. There is little evidence of regional variation in R. Because the number of cases and deaths is smaller on a subnational level, there is greater uncertainty in these estimates of R. It is likely that R is less than 1 in all UK nations and regions.
10. The number of cases in the community has decreased more quickly than the number in, or seeded from, care homes or hospitals. As a result, hospital or care home cases now represent a higher proportion of total cases, possibly a majority. This means that the rate at which the overall epidemic is shrinking in terms of cases has slowed.
11. Incidence of COVID-19 infection remains uncertain with the latest ONS data suggestion about 8,000 to 9,000 cases per day (0.11 cases/100 people per week or 61,000 new COVID-19 infections per week in England, with wide confidence intervals). Modelling estimates are higher and range from 10,000 to 60,000 new infections per day based on case incidences, ICU admissions and deaths, which represent a larger data set than the ONS sample size. ONS estimates that, between 4 May and 17 May 2020, an average of 0.25% of the community population in England had COVID-19 (95% confidence interval: 0.16% to 0.38%).
Changes to measures
12. It is not yet possible to accurately assess the impact of changes already made to NPIs. Changes in transmission which have happened in the last 2 weeks will not yet be reflected in clinical data.
13. SAGE agreed that the presentation of school reopening options under different track, trace and isolate (TTI) scenarios and with varying levels of work and leisure contacts (for example from reopening non-essential retail) illustrates how the impacts of multiple, separate changes accumulate (graphic below is from paper 4a). With schools closed and R 0.7 to 1.0, as now, there is little headroom with no contact tracing in place. Moreover, the figure does not take into account any changes as a result of phase 1. SAGE noted that the figure is illustrative rather than fully quantitative and should not be used to extract predictions of the impacts of packages of measures. The more modest re-opening options are lower risk, but the level of risk depends on TTI performance. It will be important to know accurately the actual, proven TTI performance at the time when changes are made.
14. SAGE noted that overestimation of TTI capacity could lead quickly to R returning to 1.7 (the reference value in the RWC). It was noted, however, that the summer school holidays would in effect reinstate school closures in July, potentially unwinding the impacts of re-opening, and allowing monitoring of effects if other NPIs remain stable.
15. SAGE advised that either social bubbling or opening both primary and secondary schools had the potential to recreate significant transmission networks, which would have a large effect on the epidemic.
16. SAGE noted the relatively young age profile of parents and teachers, which means that a lower level of risk in general (though some individuals within those groups may be higher risk for other reasons). Further work is needed to understand the proportion of children living with grandparents who are more likely to be in higher-risk age groups.
17. SAGE advised that opening schools or non-essential retail safely would require a significant effort to ensure that environments are appropriate to minimise transmission (for example distancing and hygiene measures, ventilation). Systems to evaluate this, and, potentially, enforcement mechanisms will be required. In this context it was noted that modelling of the effects of opening non-essential retail assume that a modest increase (10% points for work and 10% for leisure) in contacts occur. It is not known with confidence what the change would be in practice and any change would require effective distancing, hygiene and environmental control.
18. SAGE emphasised the importance of very careful monitoring and evaluation of infection in schools after any re-opening. This could begin with a virological and serological study of the current school population and should include serial testing for the virus and antibodies, with the appropriate control study. Jeremy F, ONS and PHE to design a study protocol with DfE to take this forward. CMO and GCSA to facilitate funding. A similar study in the retail sector should also conducted (where there may already be good data on contact patterns in open shops). PHE to lead.
19. Further to this, SAGE noted that the precise impacts of lifting NPIs are not possible to predict accurately. It recommends that any changes are done in such a way that impacts can be measured and evaluated, with systems for this in place at the outset, and that this evaluation is made before any subsequent steps are taken.
20. SAGE considered that the behavioural responses in the event of multiple, simultaneous changes to current restrictions were highly unpredictable and that the possibility of large, unintended, negative consequences with respect to adherence to remaining measures was significant.
- 21. SAGE advised that the lower the number of infections at the point when measures are lifted, the better this would be in terms of managing the epidemic. Not only would there be fewer people being infected, becoming ill and dying but:
- a. Contact tracing and testing capacities are less likely to be overwhelmed. If TTI is overwhelmed, re-imposition of significant NPIs is the only way to regain control of the epidemic. The risks of TTI failure will be greatest in winter and at the start of TTI if the number of cases is still relatively high and the system is not mature.
- b. Fewer people in total will be required to isolate having been identified by TTI as a contact of an infected individual (currently at 10,000 cases per day and 20 to 30 contacts per person very large numbers may need to be isolated).
- c. Individuals are less likely to get multiple ‘stay home’ warnings from contact tracing.
- d. If R does rise above 1, the time window to detect from a lower level of incidences therefore would be longer.
22. It is also important to note that the prevalence of non-COVID-19 respiratory disease in the community is also a critical determinant of the scale of TTI required and may easily swamp the number of COVID-19 cases (for example test capacity and any contact isolation based purely on symptoms will need to take this into account).
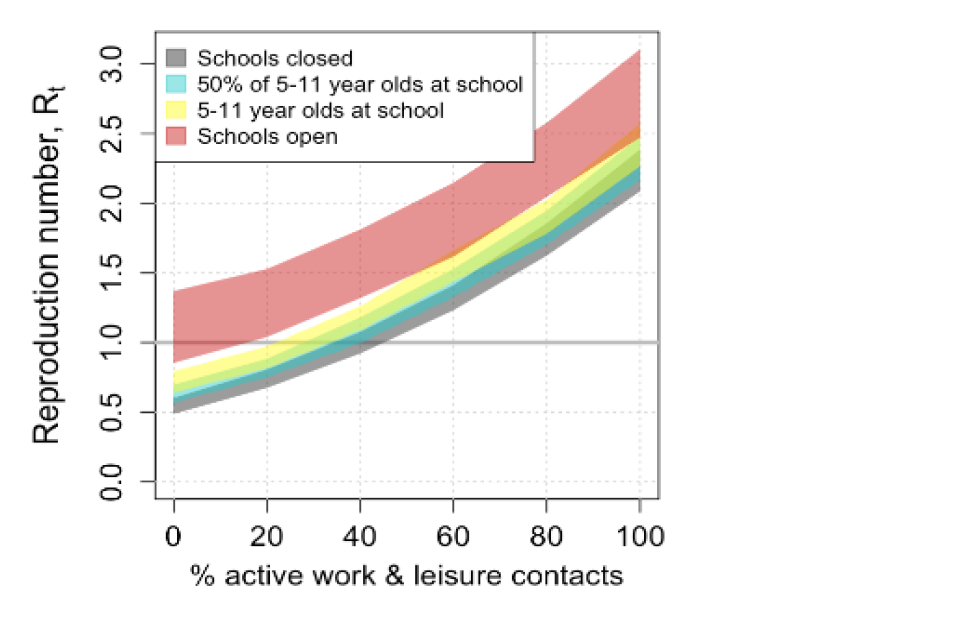
Figure shows the R rate increase predicted with different scenarios of schools closed, 50% of 5-11 year olds at school, all 5-11 year olds at school, and schools open with no contact tracing.The highest figure is 3.0.
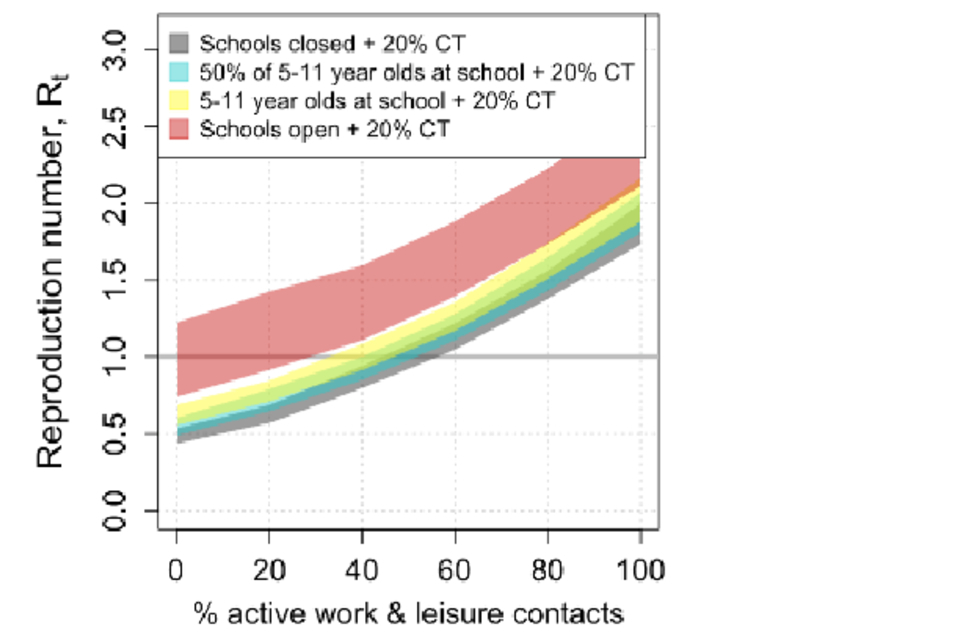
Figure shows the R rate increase predicted with different scenarios of schools closed, 50% of 5-11 year olds at school, all 5-11 year olds at school, and schools open with 20% level of contact tracing.The highest figure is 2.5.
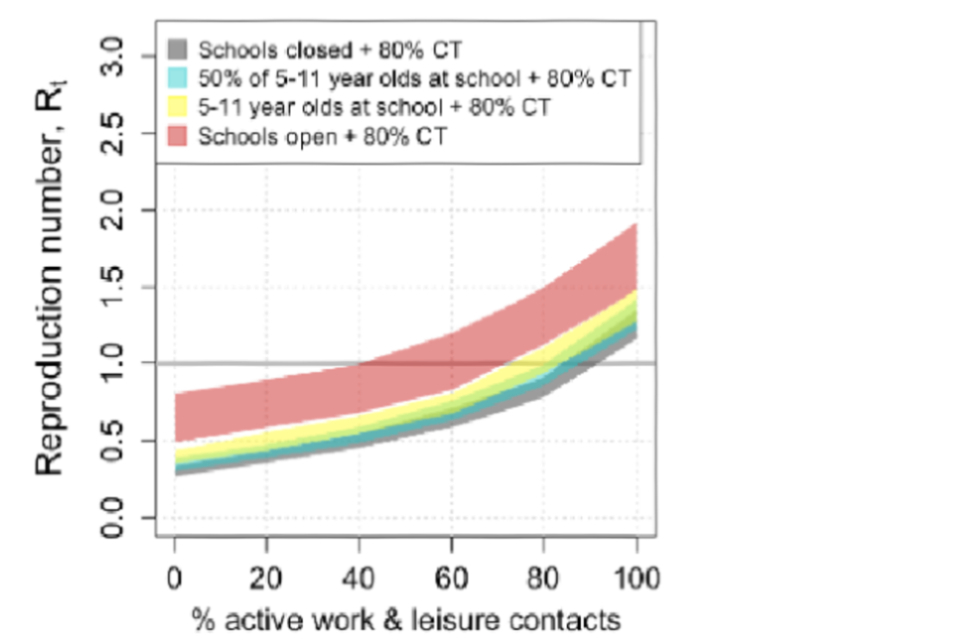
Figure shows the R rate increase predicted with different scenarios of schools closed, 50% of 5-11 year olds at school, all 5-11 year olds at school, and schools open with 80% level of contact tracing.The highest figure is nearly 2.0.
Note: On the x-axis, 0% is full lockdown with household contacts only. The current measures (with key workers etc) have only taken us to -20%. We are currently on the first graph (no TTI) in the pale blue (with children of key workers at school) at R 0.7 to 1.0. These graphs are indicative on changes in R against relaxation of measures for a given level of TTI, they do not represent absolute levels of R. Modelling of the effects of opening non-essential retail assume a modest increase of 10% for work and 10% for leisure; these were treated separately and are not a straight addition in the graphs above. Therefore, the effect in the ready reckoner above, will be somewhere between 10% and 20%.
Actions:
- SAGE secretariat to send summary of SAGE advice on sequencing of NPIs to Cabinet Office (by 22 May)
- Jeremy Farrar and ONS to develop protocol for study to assess prevalence and infection rate among children and teachers currently attending schools (by 26 May)
- PHE to develop protocol for study to assess infection within essential retail that is currently open (by 26 May)
- SPI-B and Children’s Sub-group to identify research questions around understanding behaviours that are influenced by social distancing protocols in schools and options for taking such research forward; Children’s Sub-group to also understand proportion of children living with grandparents in higher-risk age groups (by 28 May)
- SAGE secretariat to provide paper summarising current SAGE understanding of SARS-CoV-2, epidemiology of COVID-19 and mitigations, for example environmental and test, trace and isolation (by 28 May)
Test, Trace, and Isolate (TTI)
23. SAGE was updated on the Joint Biosecurity Centre and TTI, including testing capacity, local authority planning, the development of a JBC scenario ‘playbook’ (which SAGE will support) and the role of the NHSX contact tracing app.
24. The Joint Biosecurity Centre (JBC) will provide insight and analysis to drive the TTI system. A beta version of JBC will be operational by 1 June.
25. Local authorities, with the support of PHE, will be tasked with developing local action plans, to include: supporting care homes, identifying high-risk settings, deploying local testing rapidly, providing sufficient resource for local contact tracing and helping people self-isolate. SAGE was supportive of local areas being empowered to identify infections at local levels and to make decisions to address these, using a clear list of actions and triggers for actions.
26. SAGE highlighted that TTI capacity needs to be scaled according to the number of people who have both COVID-19 and also COVID-19 comparable symptoms (this is a far higher number than for COVID-19 cases alone). At current prevalence and incidence, a test and trace capacity of 10,000 a day will likely not be sufficient, as it does not take into account non-COVID-19 symptoms.
27. SAGE recognised that transparency and early public engagement are essential to ensure public buy-in for TTI. Challenges include conveying to individuals the need to self-isolate if they have come into contact with a positive case. Incentives and protections are required to encourage people to self-isolate on several occasions.
28. SAGE recognised the importance of the JBC and the TTI system improving over time. Collection of data from index cases, including locations and job roles, should improve knowledge of how the disease is transmitted.
29. SAGE recognised the absolute requirement for the JBC to work in tandem with the TTI system and for both to be guided at every level by organisationally embedded science. A challenge will be to reduce the prevalence of COVID-19 to very low levels and for JBC to identify and prioritise data that provide early indications of rising infection levels.
30. SAGE approved a paper on science aspects of the JBC once changes were made. The paper should set out the projected number of deaths if the incidence of COVID-19 in the population is at 100 or 1,000 cases per day. SAGE reiterated its view that incidence should be as low as possible before an effective TTI and JBC system can work. The decision as to what level of incidence to choose is an operational one and not for SAGE.
31. SAGE warned that if the TTI system begins operating when there is a relatively high level of incidence and prevalence of COVID-19 in the population, the system could very rapidly become overwhelmed.
Actions:
- SAGE secretariat to share draft paper on infection transmission in other high-risk environments/disadvantaged settings with Joint Biosecurity Centre
- SAGE secretariat to send SAGE advice on testing requirements for cases and contacts to Joint Biosecurity Centre (by 22 May)
- Joint Biosecurity Centre (Tom Hurd) to ensure its data is available for research purposes
- SPI-B to advise NHSI Team directly on behaviour change required for effective design of TTI
- Ian Diamond to update and circulate Evaluation Subgroup paper on Joint Biosecurity Centre design principles, to reflect discussion on rates and levels of COVID-19 incidences (by 22 May); Evaluation Subgroup to provide ad hoc advice as necessary directly to Joint Biosecurity Centre
- SAGE participants to email SAGE secretariat with recommended names for chief medical and science officer in JBC and TTI programme
- SAGE secretariat to provide a paper summarising the current state of SAGE understanding of SARS-CoV-2
List of actions
- SPI-M to update RWCS to include caveats on a) detecting incidences quickly and b) different effects of R above 1, both low as well as high values, so RWCS can be incorporated in return on Cabinet Office commission (by 22 May)
- Welsh Government to reconcile its modelling with SAGE-endorsed RWCS
- SAGE secretariat to send summary of SAGE advice on sequencing of NPIs to Cabinet Office (by 22 May)
- Jeremy Farrar and ONS to develop protocol for study to assess prevalence and infection rate among children and teachers currently attending schools (by 26 May)
- PHE to develop protocol for study to assess infection within essential retail that is currently open (by 26 May)
- SPI-B and Children’s Sub-group to identify research questions around understanding behaviours that are influenced by social distancing protocols in schools and options for taking such research forward; Children’s Sub-group to also understand proportion of children living with grandparents in higher-risk age groups (by 28 May)
- SAGE secretariat to provide paper summarising current SAGE understanding of SARS-CoV-2, epidemiology of COVID-19 and mitigations, for example environmental and test, trace and isolation (by 28 May)
- SAGE secretariat to share draft paper on infection transmission in other high-risk environments/disadvantaged settings with Joint Biosecurity Centre
- SAGE secretariat to send SAGE advice on testing requirements for cases and contacts to Joint Biosecurity Centre (by 22 May)
- Joint Biosecurity Centre (Tom Hurd) to ensure its data is available for research purposes
- SPI-B to advise NHSI Team directly on behaviour change required for effective design of TTI
- Ian Diamond to update and circulate Evaluation Subgroup paper on Joint Biosecurity Centre design principles, to reflect discussion on rates and levels of COVID-19 incidences (by 22 May); Evaluation Subgroup to provide ad hoc advice as necessary directly to Joint Biosecurity Centre
- SAGE participants to email SAGE secretariat with recommended names for chief medical and science officer in JBC and TTI programme
- SAGE secretariat to provide a paper summarising the current state of SAGE understanding of SARS-CoV-2
Attendees
Scientific experts:
- Patrick Valiance (GCSA)
- Chris Whitty (CMO)
- Andrew Curran (CSA HSE)
- Angela McLean (CSA MOD)
- Brooke Rogers (KCL)
- Calum Semple (Liverpool)
- Carole Mundell (FCO CSA)
- Cath Noakes (Leeds)
- Charlotte Watts (CSA DfID)
- Dido Harding (NHSI)
- Fliss Bennee (Wales Technical Advisory Cell)
- Graham Medley (LSHTM)
- Ian Boyd (St Andrews)
- Ian Diamond (ONS)
- Ian Young (CMO Northern Ireland)
- Jeremy Farrar (Wellcome)
- Jim McMenamin (Health Protection Scotland)
- John Aston (CSA HO)
- John Edmunds (LSHTM)
- Jonathan Van Tam (dCMO)
- Julia Gog (Cambridge)
- Lucy Yardley (Bristol)
- Maria Zambon (PHE)
- Mark Walport (UKRI)
- Mark Wilcox (NHS)
- Michael Parker (Oxford)
- Nicola Steedman (dCMO Scotland)
- Osama Rahman (CSA DfE)
- Paul Cosford (PHE)
- Peter Horby (Oxford)
- Rob Orford (Health CSA Wales)
- Robin Grimes (CSA MOD)
- Sharon Peacock (PHE)
- Stephen Powis (NHS)
- Venki Ramakrishnan (Royal Society)
- Wendy Barclay (Imperial)
- Yvonne Doyle (PHE)
Observers and government officials:
- Ben Warner (No. 10)
- Henry Cook (No. 10)
- lmran Shafi (No. 10)
- Louis Watt (NHSI)
- Vanessa MacDougall (HMT)
SAGE secretariat
- Simon Whitfield
- Stuart Wainwnght
Total participants: 59
4 observers and government officials and 13 Secretariat members redacted.