
Near miss between a passenger train and a van near Millbrook, Bedfordshire, 25 September 2025
Published 16 April 2026

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/safety-digest-042026-millbrook/near-miss-between-a-passenger-train-and-a-van-near-millbrook-bedfordshire-25-september-2025
1. Important safety messages
This incident demonstrates the importance of:
- staff only going on or near the line when accompanied by a controller of site safety, who has given them permission to do so
- ensuring that a clear understanding has been reached when discussing safety-critical information
- challenging unsafe working practices in accordance with recognised rail industry systems.
2. Summary of the incident
At around 23:34 on 25 September 2025, a passenger train travelling at 108 mph (174 km/h) on the Midland Main Line almost struck a van that had been reversed onto the tracks by railway staff at an access point near to Millbrook, Bedfordshire.
The railway at the site of the incident, just north of Ampthill tunnels, has four lines which run generally north to south. From west to east, these are designated as the Down Fast, Up Fast, Down Slow and Up Slow lines. The up lines carry southbound trains towards London, while the down lines carry northbound trains towards Bedford and Leicester.
Bridge number 169 (known locally as Park Farm bridge or ‘water bridge’) carries a single track lane over the railway to allow access to a nearby property. There are two track access points at this location. These are a vehicular access into a small yard by the Down Fast line, and a pedestrian access down a flight of steps leading to the Up Slow line.
The railway staff involved were intending to work on the Up and Down Slow lines, which were already blocked to rail traffic. However, they instead accessed the railway adjacent to the Up and Down Fast lines, which were still open to normal train services, and used the fast line access point to reverse the van on to the railway. At the time of the near miss, the van was positioned across the Down Fast line, with its rear close to the Up Fast line on which the train was travelling. There were no injuries or damage caused during the incident.
3. Cause of the incident
The incident occurred because the van was driven onto the incorrect side of the railway and parked on lines which remained open to traffic.
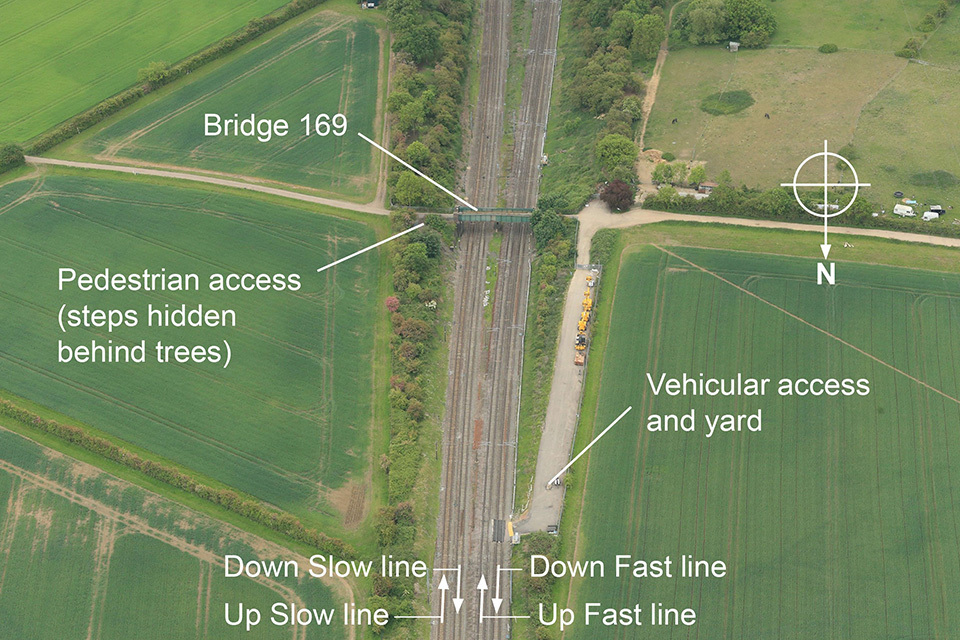
The site of the incident (courtesy of Network Rail with RAIB annotations).
At the time of the incident, the slow lines were under an engineering possession. This meant that they were blocked to normal train movements and available for maintenance work to take place. The fast lines, however, remained open to trains travelling up to the permitted linespeed of 125 mph (201 km/h). The lines available for engineering possessions typically alternate weekly, with the slow lines being available one week, and the fast lines available the following one.
The staff involved in the near miss were part of a team of ten people. These comprised:
- A person in charge (PIC) who worked for Network Rail. Under Network Rail standards, a PIC has overall accountability for supervising and overseeing works and managing operational, site and task risks. The PIC was also the designated controller of site safety (COSS) for the team, which is a common arrangement. A COSS is the person responsible for ensuring that a safe system of work is set up to protect staff from the movement of trains.
- A site warden, the driver of the van involved, who worked for Network Rail. As part of a safe system of work, a site warden is responsible for ensuring that personnel do not leave the safe working area.
- Eight track operatives, who worked for a contractor.
The team was tasked with undertaking track maintenance work, over a series of night shifts, at various locations within a work site which was established in the planned engineering possession. The work involved fixing discrete track defects by lifting the track and packing the ballast under the sleepers. There were also other teams working at different locations within the work site that night.
On the night of the incident, the team met at Network Rail’s Bedford maintenance depot, adjacent to Bedford station, at around 21:30. The PIC briefed the team on the planned work for that night, and on the contents of the safe work pack (SWP). The SWP provides details on the safety arrangements for the work, including the system of work which is to be implemented to make sure that a team is not in danger from passing trains.
The brief included details of the access arrangements, stating that the work was on the slow lines, and that the team would access the track at “water bridge” (bridge 169). The SWP incorrectly indicated that a different access point was to be used by the team at Chimney Corner, where the PIC was due to undertake another task. However, this error had been noticed and corrected by the PIC and did not affect the information that they briefed to the team.
Witness evidence suggests that the PIC planned to repeat the safety-critical elements of the brief once the team were on site, near Millbrook. After the brief was completed, the site warden and contractors loaded the site warden’s van with the tools and equipment for the night’s work.

The van involved in the near miss.
The PIC had also been tasked with assisting the engineering supervisor, a person responsible for establishing, managing and securing a work site within a possession, by placing marker boards at the limits of the work site. This had to be done before any work could start and required the PIC to drive to Chimney Corner, around 3 miles (5 km) north of bridge 169. This meant that the PIC was not initially on site when the remainder of the team arrived at the access. The intention was that the PIC would rejoin the team after placing the marker boards, before work started.
While the PIC was undertaking this task, the site warden drove their van to bridge 169, followed by the contractor’s staff in other vehicles, arriving at around 22:40. The site warden opened the access gate on the fast line side of the track and reversed their van into the yard ready to start work.
At around 23:15, the PIC was told they could place the work site marker boards at Chimney Corner. At around 23:33, before driving to bridge 169 to rejoin the team, the PIC called the site warden to inform them that the work site was in place. The PIC asked the site warden to get the van into position ready to start the work. Witness evidence suggests that the PIC’s intention was for the van to be positioned alongside the pedestrian access gate on the slow line side, ready to unload the equipment so it could then be carried down the steps.
After this call, the site warden reversed the van down to the access point adjacent to the fast lines, with the intention of unloading the equipment directly onto the track. This access point has a permanent road-rail access point (RRAP) installed on the Down Fast line, to allow heavy rail plant to access the track. The site warden reversed the van onto this RRAP, so that it was positioned directly on the Down Fast line, perpendicular to the rails. At least two of the contractor’s staff were walking alongside the van, assisting with the manoeuvre.
At around 23:34, a passenger train travelling at 108 mph (174 km/h) passed the site on the Up Fast line, heading towards London. Forward-facing CCTV from the train shows that the van was stationary on the RRAP, and that the rear of the van was very close to the passing train. The train driver was unaware of the van and so did not sound the train’s horn as it approached the RRAP. Witness evidence suggests that the train was “between 1 and 2 feet” from the van. The site warden, who was still in the van, stated that they did not see or hear the passing train. Witness evidence is that the contractor’s staff told the site warden to move the van clear, after seeing the near miss.
At around 23:35, the PIC was driving back from Chimney Corner. As they did so, they drove over a road bridge that crosses the railway around 400 metres north of the access point. As they crossed the bridge, they saw the van on the RRAP. Realising that the van was on a line which was still open to traffic, the COSS immediately stopped and called the site warden to tell them to get clear of the line. This happened around the same time as the contractor’s staff told the site warden to get the van clear. Once the van was clear of the railway, the incident was immediately reported by the PIC to the railway’s control room, and the team was stood down.
Network Rail’s standard RT 3170 ‘The Guide to your Personal Track Safety’ states that ‘The COSS must be with the work group from when you access the infrastructure, while working up to when you leave the infrastructure’. In addition, the Rule Book, Handbook 7 ‘General duties of a controller of site safety’ states that a COSS must stay with any group that is on or near the line to personally observe and advise their actions.
Witness evidence is that the telephone conversation between the PIC and the site warden led to a misunderstanding by the latter as to the intent of the PIC’s instructions. This resulted in the site warden believing that they had authority to unload equipment onto the track, and this then led to them entering the railway without the presence of the PIC, who was the designated COSS. This occurred even though the site warden themself had recently qualified as a COSS. This decision to access the track without the COSS being present was not challenged by the other staff present.
Both the PIC and the site warden were familiar with the site, access points, and general area and they had previously worked on both the fast and slow lines at this location. The details of the work, including that the team was working on the slow lines, had also been briefed to the team in the depot before they loaded the tools. Both access points at bridge 169 have lineside signage detailing the site access arrangements, including line identities and speeds.
RAIB has not been able to determine exactly what led to the site warden confusing the two access points on the night of the incident.

The vehicular access point and (inset) close up of the sign detailing the access point arrangements.
4. Previous similar occurrences
Many incidents and accidents involving track workers have been investigated by RAIB. These resulted in fatalities or had the potential to do so. Those with similarities to the incident at Millbrook include:
- In 2017, RAIB published a class investigation into accidents and near misses involving trains and track workers outside possessions (RAIB report 07/2017). The common causal factors included members of work groups not challenging deviations from the safe system of work, and poor communications.
- In December 2018, a near miss occurred between a train and two track workers at Sundon, Bedfordshire (RAIB safety digest 05/2019). The track workers involved had unintentionally accessed the railway at the wrong location, onto the open fast lines, instead of the blocked slow lines. The staff were not familiar with the location, and the access point they used did not have any signage that showed they were at the wrong location.
- In July 2022, two track workers narrowly avoided being struck by a train while working close to Penkridge station (RAIB report 09/2023). At the time the train passed, the track workers believed that the line they were standing on was blocked to the passage of trains, while the PIC believed that they were standing away from the track in a position of safety, and had allowed the line blockage to be removed without warning them.
- In March 2024, a near miss occurred between a train and a track worker near to Euxton Junction on the West Coast Main Line (RAIB safety digest 05/2024). This incident occurred because the COSS misidentified which of the railway lines at the location had been blocked to the passage of trains. Although signage at one of the access points used by the team correctly showed the layout of the track, the COSS did not spot the error. The error was also not challenged by the other member of the team during a briefing given by the COSS.
RAIB’s website includes a summary of learning relating to the protection of track workers from moving trains. This includes further examples of similar incidents and accidents.