
Derailment of a tram near Highbury Vale tram stop, Nottingham, 30 September 2022
Published 13 February 2023

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/safety-digest-012023-highbury-vale/derailment-of-a-tram-near-highbury-vale-tram-stop-nottingham-30-september-2022
1. Important safety messages
This accident demonstrates the importance of:
-
recognising that working on assets in degraded conditions can mean that normal technical and operational risk controls may no longer be present
-
taking the time to understand the risks that reactive work, such as responding to faults, may bring to the staff on site, to safety-critical systems and to vehicles using the infrastructure
-
staff dealing with safety-critical equipment working within their competencies and taking appropriate action when they recognise that they are not.
2. Summary of the accident
At around 07:17 hrs, Nottingham Express Transit (NET) tram number 219 was travelling northwards on a journey from Nottingham City Centre to the Phoenix Park terminus. Trams travelling north can be routed towards either Phoenix Park or towards Hucknall using a set of points located between David Lane and Highbury Vale tram stops (numbered ‘HVP3’ points). The leading wheelset of tram 219 encountered these points in an intermediate position, where they were not set correctly for either route. This caused the tram to derail.
The tram was travelling at approximately 11 km/h (7 mph) at the time of the derailment. Although the tram was in passenger service at the time of the derailment, only the driver was onboard. There were no injuries as a result of the derailment, but some minor damage was caused to the tram and to the infrastructure.
Before the accident, HVP3 points had been reported as defective. A team of NET technicians had been despatched to the location as soon as they reported for duty that morning. The tramway control room had notified all drivers via a general radio broadcast that these points had failed and that there were maintenance technicians on site.
At 07:14:39 hrs, tram 219 arrived at David Lane tram stop. The driver saw that the points position indicator (PPI) repeater (located at David Lane tram stop) for HVP3 points indicated that the points were in an intermediate position. Having heard the earlier control room broadcast, the driver correctly attributed this to the maintenance team. He expected to find the team working on the points, which are approximately 700 metres north of David Lane tram stop.

Image taken from the forward-facing CCTV of tram 219 as it arrived at David Lane tram stop with the points position indicator (repeater) for HVP3 points showing them to be in an intermediate position (left image) and later set for Phoenix Park (right image).
Before departing from David Lane, tram drivers need to use their in-cab controls to command HVP3 points to move to the desired route (that is, either to Phoenix Park or Hucknall). While stationary at David Lane tram stop, the driver of tram 219 selected the left-hand route towards Phoenix Park at 07:14:48 hrs. He then saw the PPI repeater show that this route was correctly set.
After the driver had selected the route to Phoenix Park, the technicians working on the failure used the points controller adjacent to HVP3 points to ‘swing’ the points between various positions. Between 07:14:57 and 07:15:08 they did this four times, with the PPI repeater showing the positions briefly during this time. However, when tram 219 departed David Lane tram stop at 07:16:17 hrs, forward-facing CCTV (FFCCTV) images confirm that the PPI repeater at the tram stop was showing that HVP3 points were set for the route to Phoenix Park and that it had been doing so for over a minute before the tram departed.
There was fog in the area which reduced visibility, and the tram driver was aware that the maintenance team may have been working close to the line ahead of him. Consequently, the driver decided to approach the points at a lower speed of 11 km/h (7 mph) instead of 25 km/h (16 mph) permitted, for the route towards Phoenix Park.
At 07:16:41 hrs, tram 236, the next northbound service, arrived at the platform at David Lane. The intended route for tram 236 was towards Hucknall.
A second PPI is located in close proximity to HVP3 points. Forward-facing CCTV images from tram 219 show that this second PPI was correctly indicating that HVP3 points were set to the left (for Phoenix Park), and the driver of tram 219 continued, in the knowledge that the correct route was set.
Having seen tram 219 depart from David Lane, the driver of tram 236 intended to leave enough time for tram 219 to pass over the junction before calling the alternative route. However, the fog meant that tram 219 was not visible to the driver of tram 236 as it neared the junction. Tram 219 reached the toe of HVP3 points at approximately 07:17:21 hrs. Less than one second before the derailment, and after both the PPI and the point blades themselves had passed from the view of the driver of tram 219, the driver of tram 236 at David Lane called points HVP3 to swing to the right, towards Hucknall.
Calling the points towards Hucknall meant that the points moved and the front wheelset of tram 219 encountered them in an intermediate position, causing the derailment. In normal operation, the movement of the points with an approaching tram in this position would have been inhibited by the control system.
3. Cause of the accident
This derailment was caused because tram 236 was able to call HVP3 points and change their position as the leading wheelset of tram 219 was about to pass over them.
The tram drivers involved in the accident were working according to normal operational procedures and their actions were not a factor in the derailment.
In normal operation, trams travelling north towards HVP3 points from David Lane are detected by a track circuit located on the approach to the points. Trams are then subsequently detected by a mass detector located at the junction. This detection should inhibit further operation of the points and ensure that they are not moved while a tram is passing over them. Once trams clear the track circuit and then the mass detector (in the correct sequence) the points are released to accept a new route for following trams.
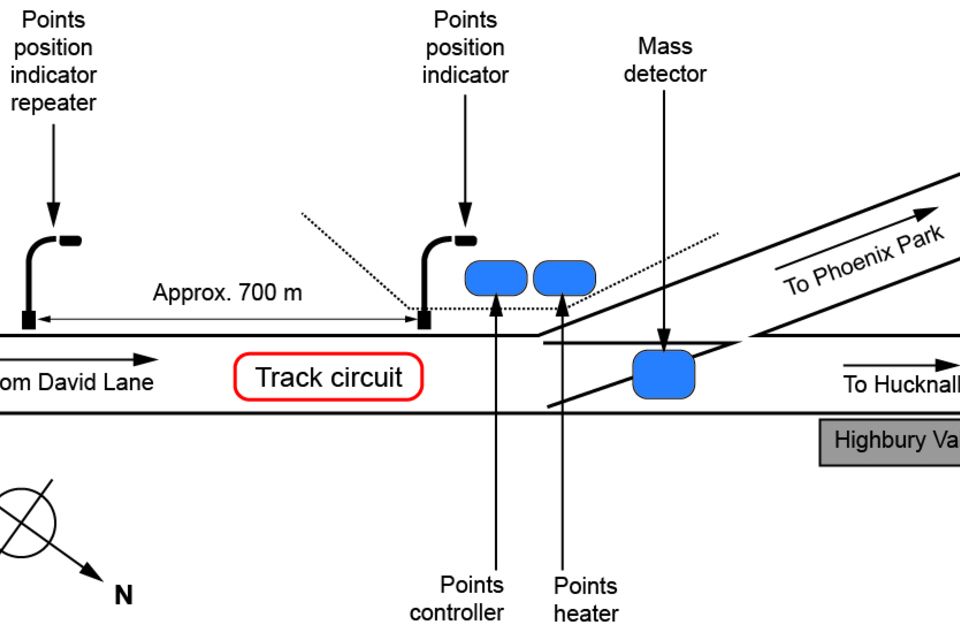
Sketch map showing layout of the accident location and relevant infrastructure.
Investigations showed that before the accident, the track circuit on approach to HVP3 points had not been operating correctly. This meant that the points control system was registering the presence of a tram through the mass detector without the track circuit having first detected the tram’s approach. As this was contrary to the expected sequence, the control system generated an ‘out of sequence’ alarm and prevented the points from moving as a ‘fail-safe’ measure.
The technicians who responded to this failure noted that the lineside points controller unit was displaying fault code ‘FL02’. However, they were unaware of the meaning of this fault code. A laminated sheet in the points control cabinet stated that one possible cause of an ‘FL02’ fault is a ‘sequence error’.
Although the technicians were unaware of the nature of the fault, they discovered that they could clear the ‘FL02’ fault code from the points controller by either turning the controller off and on again or by using the buttons within the points controller cabinet to swing the points manually. To allow trams to continue operating while the technicians were investigating the fault, they adopted an improvised method of work. This involved clearing the fault code to allow approaching trams to call the points into the position required for their route. Once the route was called, the technicians then stopped work and waited for northbound trams to depart from David Lane tram stop and to clear the junction before restarting work.
In line with this improvised system of work, the technicians stopped working on the points controller as tram 219 approached from David Lane, in the knowledge that the fault had been cleared and that the tram could continue on the set route.
However, the technicians were unaware that by resetting the controller, the stored route request from (in this case) tram 219 was removed from the points control unit. This meant that the controller would accept, and act on, a subsequent call (from another tram) for the points to move. The absence of the protection provided by the track circuit meant that the points could, in such circumstances, swing with a tram approaching them.
In these circumstances, the last opportunity to avoid the derailment would be a tram driver observing that the PPI immediately before the points was showing an incorrect indication and observing the point blades themselves, as required by NET procedures. However, in the case of this accident, the points moved after both the PPI and the point blades had passed out of the view of the driver of tram 219.
NET explained that there is no written plan for dealing with the ‘FL02 sequence error’ identified on HVP3 points. However, NET procedure QP/ENG/GEN/0003 requires staff working on or near the tramway to undertake a Worksite Safety Assessment (WSA) where written plans for the work to be carried out do not already exist. The staff attending the site in response to the fault did not create a WSA, nor was any other plan devised to help understand the risks that their improvised system of work might inadvertently create. Consequently, they did not adopt suitable mitigations against the risks created by working on the points while trams were running.
4. Previous similar occurrences
RAIB has previously investigated a number of occurrences on the mainline railway which highlight the importance of staff following the correct process when working on safety-critical equipment. More recent examples are a slow speed passenger train collision at Waterloo (RAIB report 19/2018) and an empty passenger train derailment at Dalwhinnie (RAIB report 10/2022). Although these accidents took place on Network Rail infrastructure (and staff actions are therefore mandated by the relevant Network Rail standards and handbooks), these accidents illustrate the importance of following established procedures when working with such systems.
On 29 June 2017 the driver of a passenger train approaching Canterbury West station saw road vehicles crossing the track at Broad Oak level crossing that the train had been signalled to proceed over. RAIB Safety Digest 13/2017 describes how the crossing was under local control for maintenance at the time and should have been closed to road traffic. This digest reminded the railway industry about the importance of following procedures when arranging to carry out work that will affect the normal operation of railway assets. While also a mainline incident, the primary safety learning is similar to that from the Highbury Vale derailment.