Laboratory confirmed cases of pertussis reported to the enhanced pertussis surveillance programme in England: annual report for 2013
Published 2 May 2014

© Crown copyright 2014
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/pertussis-enhanced-surveillance-laboratory-confirmed-cases-in-england-in-2013/laboratory-confirmed-cases-of-pertussis-reported-to-the-enhanced-pertussis-surveillance-programme-in-england-annual-report-for-2013
In England there were 4623 laboratory confirmed cases of pertussis (culture, PCR, serology or oral fluid) reported to the Public Health England pertussis enhanced surveillance programme in 2013 (table1) and 212 cases reported in Wales. Over a third (35%; 1625/4623) of all confirmed cases in England in 2013 were reported in the first quarter (January to March).
Numbers of confirmed cases in England in 2013 were 51% lower than the 9367 cases reported in 2012. While the number of confirmed cases decreased in 2013 in comparison to 2012, confirmed cases were more than four-fold higher than the 1053 reported in 2011. In infants under a year, however, pertussis cases were lower in 2013 (116) than in 2012 (407) and 2011 (207). The national incidence for all age groups, based on laboratory confirmations in England and 2011 population estimates [1], was 2 cases of pertussis per 100,000 population in 2011, 18 per 100,000 in 2012 and 9 per 100,000 in 2013.
Pertussis is a cyclical disease with increases occurring every 3 to 4 years. Typically pertussis activity peaks in quarter 3 and then declines, as observed in previous years (figure 1). The continued increase observed in each successive quarter between the first quarter of 2011 and third quarter of 2012 was unusual and was largely due to the increase in the numbers of confirmed cases in individuals aged 15 years and older. A changing epidemiological pattern continued in 2013 with peak disease levels in the first quarter followed by an overall decrease in pertussis cases through the year after the exceptional activity observed in 2012.
A national outbreak of pertussis (level 3 incident [2]) was declared by the HPA in April 2012 and, as a response to the ongoing outbreak, the Department of Health announced the introduction of a temporary immunisation programme for pregnant women on 28 September 2012 [3]. The most recent PHE figures report that the proportion of mothers due to give birth between January 2013 and December 2013 who had been immunised with a pertussis containing vaccine in pregnancy in England ranged from 49.8% to 61.5% [4,5].
As was seen in 2012 the majority (85%; 3912/4623) of laboratory confirmed cases in England in 2013 occurred in individuals aged 15 years and older. Confirmed cases in this age group decreased by 50% between 2012 and 2013; from 7775 in 2012 (incidence of 18/100,000) to 3912 in 2013 (incidence of 9/100,000) (figure 2). Whilst disease incidence continued to be highest in infants <3 months, confirmed cases in this age group were 79% lower in 2013 (85 cases) than in 2012 (407 cases) and 49% lower than the 166 cases in 2011. The incidence of laboratory confirmed cases in infants less than 3 months, who are at most risk of serious disease and too young to be fully vaccinated, was 50 per 100,000 in 2013 compared with 240 per 100,000 in 2012 (figure 2). Three pertussis related infant deaths were reported for infants with pertussis confirmed in 2013 compared to 14 deaths in 2012. All infants were too young to be protected by the vaccine and none of the infants’ mothers were vaccinated during pregnancy. No pertussis related infant deaths were reported in Wales in 2013. These early data in young infants following the introduction of a programme to immunise pregnant women are encouraging. It is important to be aware, however, that raised levels of pertussis persist in older age groups. Women should continue to be encouraged to be immunised against pertussis during pregnancy in order to protect their babies from birth.
Since mid-2006 there has been greater use of serology testing compared to previous years due to increasing clinical awareness of pertussis in older children and adults [6] and increased awareness of the availability of this diagnostic method [7]. In 2013, serology confirmed cases accounted for the greatest proportion (94%; 4364/4623) of total laboratory confirmations, and account for 99% of all confirmed cases of pertussis in older age groups (table2). All but 2 infants under 1 year of age with confirmed pertussis in 2013 were tested using culture and PCR methods. From January 2013 oral fluid (OF) testing was offered for children aged 8 to <17 years and for children aged 5 to <17 years from October 2013. In 2013, 97 cases (2.1%) tested positive for a recent pertussis infection by OF testing only.
The choice of laboratory testing method is dependent on the age of the patient and the stage of the illness; this is reflected in the distribution of testing methods summarised in table 2. Culture has high specificity but loses sensitivity with increasing time from the onset of illness. PCR testing is offered for acutely ill infants aged less than 1 year old hospitalised with respiratory illness compatible with pertussis [8]. In contrast, serology testing is routinely offered for older children/adults who have been unwell with a cough for more than 2 weeks. However, as recent pertussis vaccination (primary and pre-school booster vaccination) can confound the serology and OF results, these investigations are not usually recommended for infants or children within 1 year of receiving the pertussis vaccine (primary or pre-school booster).
PCR, serology and OF testing services are provided by the Respiratory and Vaccine Preventable Bacteria Reference Unit (RVPBRU) at Public Health England Microbiology Services Division Colindale. For the PCR service for hospitalised infants under 1 year, either a pernasal swab or nasopharyngeal aspirate should be sent as soon as possible after onset; for the pertussis serology service for older children and adults it is advised that not less than 400 µl of separated serum at least 2 to 3 weeks post-onset of cough should be sent. OF testing kits are available from local health protection teams for children aged between 5 and 16. Further information is available in the PHE Bacteriology Reference Department user manual at: http://www.hpa.org.uk/cfi/rsil/bordetella.htm.
| Quarter | Culture | PCR | Serology | OF only | Total |
|---|---|---|---|---|---|
| Jan-Mar | 18 | 21 | 1553 | 33 | 1625 |
| Apr-Jun | 27 | 21 | 1047 | 25 | 1120 |
| Jul-Sep | 23 | 31 | 1050 | 25 | 1129 |
| Oct-Dec | 12 | 9 | 714 | 14 | 749 |
| Total | 80 | 82 | 4364 | 97 | 4623 |
Table 1. Laboratory-confirmed cases of pertussis by quarter and test method in England: 2013
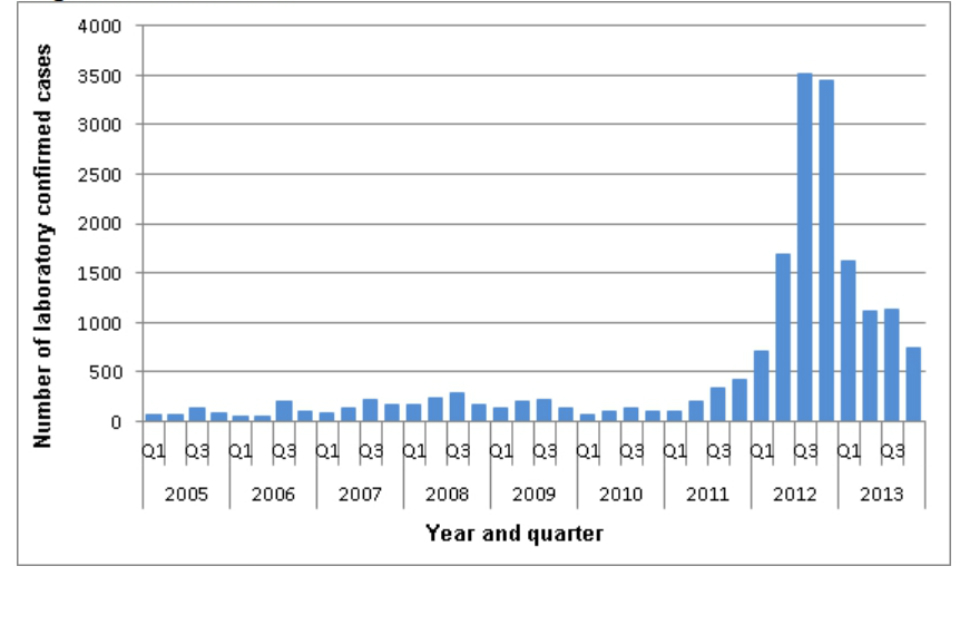
Figure 1. Total number of laboratory-confirmed pertussis cases per evaluation quarter in England: 2005 to 2013
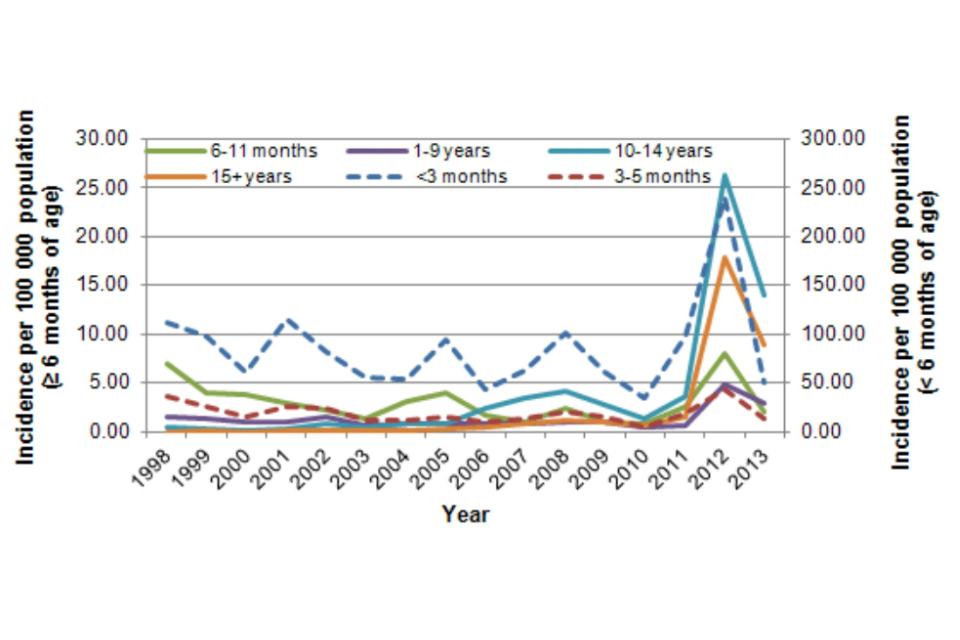
Figure 2. Incidence of laboratory-confirmed pertussis cases by age group in England: 1998 to 2013
| Age group | Culture* | PCR | Serology | OF | Total |
|---|---|---|---|---|---|
| <3 months | 39 | 46 | – | – | 85 |
| 3-5 months | 10 | 13 | 1 | – | 24 |
| 6-11 months | 2 | 4 | 1 | – | 7 |
| 1-4 years | 5 | 4 | 55 | 2 | 66 |
| 5-9 years | – | – | 86 | 14 | 100 |
| 10-14 years | 7 | 1 | 361 | 60 | 429 |
| 15+ years | 17 | 14 | 3860 | 21 | 3912 |
| Total | 80 | 82 | 4364 | 97 | 4623 |
Table 2. Age distribution of laboratory-confirmed cases of pertussis in England: 2013
* Culture confirmed cases may additionally have tested positive using other methods. Submission of all presumptive B. pertussis isolates is encouraged for confirmation of identity and to allow further characterisation for epidemiological purposes.
1. References
- Office for National Statistics – 2011 Census population estimates: http://www.ons.gov.uk/ons/taxonomy/index.html?scl=Population+Estimates
- Health Protection Report Vol. 6 No 15 (13 April 2012)
- Department of Health https://www.gov.uk/government/news/pregnant-women-to-be-offered-whooping-cough-vaccination
- Public Health England: https://www.gov.uk/government/publications/pertussis-vaccine-uptake-in-pregnant-women-october-2012-to-september-2013
- Health Protection Report Vol. 8 No 17 (02 May 2014)
- Harnden A, Grant C, Harrison TG, Perera R, Brueggemann AB , Mayon-White R, Mant D. Whooping cough in school age children with persistent cough: prospective cohort study in primary care. BMJ. 2006; 333: 174-7.
- Fry NK, Tzivra O, Li YT, McNiff A, Doshi N, Maple PA, Crowcroft NS, Miller E, George RC, Harrison TG. Laboratory diagnosis of pertussis infections: the role of PCR and serology. J Med Microbiol. 2004; 53: 519-25.
- Fry NK, Duncan J, Wagner K, Tzivra O, Doshi N, Litt DJ, Crowcroft N, Miller E, George RC, Harrison TG (2008). Role of PCR in the diagnosis of pertussis infection in infants: 5 years’ experience of provision of a same-day real-time PCR service in England and Wales from 2002 to 2007; J Med Microbiol; 58, 1023-29.
This report was published in Health Protection Report volume 8 issue 17.