Critical risk assessment report: use of UK plasma for the manufacture of immunoglobulins and vCJD risk
Published 21 April 2021

© Crown copyright 2021
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/critical-risk-assessment-report-use-of-uk-plasma-for-the-manufacture-of-immunoglobulins-and-vcjd-risk/critical-risk-assessment-report-use-of-uk-plasma-for-the-manufacture-of-immunoglobulins-and-vcjd-risk
Lay summary
Human blood and, in particular, plasma derived from human blood, is used as a starting component for the manufacture of a number of medicinal products, for example, coagulation factors for use in haemophilia or albumin for use in maintenance of blood volume. This differs from the use of blood or blood components in transfusion, which uses the blood of one person to be transfused into one other, whereas the manufacture of medicinal products from plasma involves pooling blood donations from numerous donors to extract sufficient amounts of a particular component. The pooling of blood introduces the risk of a pathogen present in the blood of one donor affecting the entire pool, and consequently all individual medicinal products made from that pool.
The majority of pathogens and toxins that can be transmitted through blood are successfully eliminated by modern manufacturing procedures, but some, such as prions, remain a risk. Prions are misfolded proteins that can cause similar proteins in the human body to misfold and lose their normal function. They cause a number of illnesses in animals, such as scrapie in sheep, chronic wasting disease in deer and bovine spongiform encephalopathy (BSE) in cattle (commonly known as “mad cow disease”). In humans, prions are the cause of Creutzfeldt–Jakob disease (CJD) and its variant (vCJD).
In 1999, in response to the emergence of the vCJD epidemic in the UK associated with the consumption of meat products from BSE-affected cattle, the Government introduced a ban on the use of UK human blood plasma for the manufacture of all plasma-derived medicinal products. Since the introduction of the ban, plasma for the manufacture of such products used in the UK has had to be imported. The main source of plasma for these products at present is the USA.
Due to limitations in the supply of immunoglobulin products caused by the need to import plasma in the UK, long term measures had to be implemented in the NHS to prioritise supply of these products to patients with the highest clinical need. The COVID-19 pandemic is placing further pressures on supply due to the increased need for blood plasma in the development of new COVID-19 medicines, and the falling numbers of blood plasma donations due to pandemic related restrictions.
An initial review was conducted by the MHRA in March 2020 and considered lifting the ban for the manufacture of hyperimmune immunoglobulin from COVID-19 convalescent patients for the treatment of COVID-19. The Commission on Human Medicines (CHM) recommended deferring full consideration until more information relating to the risk and benefits of the products became available from the ongoing clinical trials.
Subsequently, the MHRA undertook a comprehensive review of the evidence on the safety of UK blood plasma if used for manufacturing immunoglobulin medicinal products. Evidence for the review was gathered through stakeholder consultation (which included manufacturers, patient associations, government organisations, and prion experts) and mathematical modelling of the risk. This evidence was presented to the CHM in October 2020.
The stakeholder consultation showed general agreement that the decline of vCJD cases in the UK population had been more rapid than was initially predicted. Whilst all academics consulted recognised the time was right to conduct a review of the vCJD risk from the use of UK plasma, they advised a cautious approach given the remaining uncertainties around the number of asymptomatic carriers of vCJD, who might potentially transmit the infection via transfusion or other iatrogenic routes. However, most prion experts estimated the risk of vCJD transmission associated with blood products is likely to be very low, and certainly lower than what was predicted 20 years ago.
The mathematical modelling, previously developed to estimate vCJD transmission risk through transfusion of blood components, was adapted to make it applicable to immunoglobulins. This modelling estimated that, for 23 different immunoglobulin products when used at their maximum doses, the risk of infection ranges from 0.000005 to 324 infections per million administered doses. The use of leucodepletion, a procedure to remove leucocytes (white blood cells) from blood components, as a risk minimisation measure, further decreases the risk of infection by a factor of 5. Importantly, no cases of vCJD have been observed as a result of blood component transfusions since the introduction of leucodepletion in 1998. The mathematical modelling predicted that, in the worst-case scenario, assuming that 30,000 patients are treated for at least 33 years at a dose of 1000g of immunoglobulin annually, 24 clinical vCJD cases might be expected to occur in the UK. This is comparable to the risk already accepted for the transmission of vCJD arising from transfusions of fresh frozen blood plasma, which was estimated at a maximum of 15 clinical cases over the next 50 years.
On 8 October 2020, the CHM deliberated on whether the removal of the ban would pose a risk of increased transmissions and clinical cases of vCJD. The CHM concluded that the risk of vCJD cases arising from the use of UK plasma for the manufacture of immunoglobulin medicinal products would be negligible. The CHM also noted the clinical need for immunoglobulin products for patients with immunodeficiency and certain autoimmune conditions.
The CHM advised that UK-sourced plasma is acceptably safe for the manufacture of immunoglobulin medicinal products provided the following risk-mitigation measures are adhered to:
- All relevant risk-mitigation measures already in place for blood components for transfusion (the use of leucodepletion, deferral of high-risk donors and traceability between donor and recipient) should be applied to UK-sourced plasma for the manufacture of immunoglobulins.
- Manufacturers should be required to submit an application to vary the terms of their existing licences to introduce the use of UK-sourced plasma. The product-specific risk assessment and an evaluation of the prion reduction capacity of the product manufacturing process, will be required. Each product will need to be individually reviewed and evaluated by the MHRA, and advice sought from the CHM’s Clinical Trials, Biologicals and Vaccines Expert Advisory Group and CHM.
Executive summary
- There is an increased need for certain plasma-derived products but, at present, there is a ban, introduced since 1999, on the use of UK plasma to manufacture such products due to the risk of vCJD transmission. This paper discusses whether removing this ban would pose a risk of an increase in vCJD cases.
- A consultation with stakeholders (manufacturers, patient associations, government organisations) as well as prion experts has been conducted. There is general agreement that it is time to consider whether the ban is still necessary given that the vCJD risk from plasma products appears to be significantly lower than when it was implemented.
- However, prion experts recommend a cautious approach given the remaining uncertainties around the disease, especially the significance of asymptomatic carriers of the disease that would be able to transmit it.
- The mathematical model developed by the Department of Health and Social Care to estimate the vCJD risk of blood components was modified to apply it to immunoglobulins taking account of data provided by the manufacturers, i.e., the donor plasma pool size, the batch size and the prion reduction factor.
- The risk of vCJD infection and of clinical case was estimated for 17 normal Immunoglobulins and 6 hyperimmune Immunoglobulins. If using non-leucodepleted plasma and depending on the products, the risk of infection expressed per million of single maximum doses ranges from 0.0007 to 324 and the risk of clinical case ranges from 0.00005 to 24, for normal Igs; the risk of infection ranges from 0.0000045 to 0.0009 and the risk of clinical infection ranges from 0.0000003 to 0.00007, for hyperimmune Igs.
- Leucodepletion decreases the risk of infection by a factor of ~5 and the risk of clinical case by a factor of ~3.5, so for the lowest risk products, the impact of leucodepletion is negligible while it may be slightly more significant for the highest risk products.
- As two thirds of normal Ig treatments are long-term treatments, the risk for these patients is increased. This has been taken into account with highly precautionary dosing and patient exposure assumptions. As a result, the number of vCJD clinical cases expected to occur in the future is estimated to be fewer than 1-2 cases for most products assessed; for the others, it is of the same order of magnitude as the 15 clinical cases predicted for fresh frozen plasma transfusions over the next 50 years (SaBTO report, March 2019). This level of risk was already considered acceptable for fresh frozen plasma transfusion and the risk reduction measures previously in place for fresh frozen plasma have been subsequently withdrawn.
- In conclusion, based on external consultation and mathematical modelling, it is considered that the use of plasma from UK donors for the manufacture of human Ig products would expose the target patient population to no or minimal additional risk of vCJD in the future.
List of abbreviations
- ACDP: Advisory Committee on Dangerous Pathogens
- ATD: adult therapeutic dose
- BSE: bovine spongiform encephalopathy
- CHMP: Committee for Medicinal Products for Human use
- CI: credible interval
- CIPD: chronic inflammatory demyelinating polyradiculoneuropathy
- CJD: Creutzfeldt-Jakob disease
- CLL: chronic lymphocytic leukaemia
- DDA: direct detection assay
- DH: Department of Health
- DHSC: Department of Health and Social care
- EMA: European Medicines Agency
- FDA: Food and Drug Administration
- FFP: fresh frozen plasma
- HAV: hepatitis A virus
- HIV: human immunodeficiency virus
- HSCT: hematopoietic stem cell transplantation
- IBTS: Irish Blood Transfusion Service
- ID: infective dose
- Ig: immunoglobulin
- IVIG: intravenous immunoglobulin
- MAA: marketing authorisation application
- MM: multiple myeloma
- MMN: multifocal motor neuropathy
- MRC: Medical Research Council
- NCJDRSU: National CJD Research & Surveillance Unit
- NHSBT: National Health Service Blood and Transplant
- NIBSC: National Institute for Biological Standards and Control
- PDMP: Plasma-derived medicinal products
- PHE: Public health England
- PID: primary immunodeficiency syndromes
- PMCA: protein misfolding cyclical amplification
- PPTA: Plasma Protein Therapeutics Association
- PRF: prion reduction factor
- PRNP: prion protein gene
- PrP: prion protein
- PrPSc: prion protein scrapie
- PSSC: Pathogen Safety Steering Committee
- RBC: red blood cell
- SaBTO: Safety of Blood, Tissues and Organs
- SCIG: subcutaneous immunoglobulin
- sCJD: sporadic Creutzfeldt-Jakob disease
- SID: secondary immunodeficiencies
- SmPC: Summary of Product Characteristics
- TSE: transmissible spongiform encephalopathies
- TTP: thrombotic thrombocytopenic purpura
- UCL: University College London
- UKHCDO: United Kingdom Haemophilia Centre Doctors’ Organisation
- UKPA: UK Plasma Action
- UKPIPS: UK Primary Immune-deficiency Patient Support
- vCJD: variant Creutzfeldt-Jakob disease
1. Introduction
1.1. Background
Directives 2001/83/EC and 2002/98/EC encourage EU Member States to take all measures to achieve self-sufficiency for blood and plasma through voluntary unpaid donations and self-sufficiency has been achieved for blood components in most EU countries. The UK had followed the principle of self-sufficiency until the development of bovine spongiform encephalopathy (BSE) and the prion disease variant Creutzfeldt-Jakob disease (vCJD), which was first identified in the UK in 1996. As a result, since 1999, where plasma coagulation factors and other plasma-derived products are used, these have been fractionated from plasma imported from the United States. Fresh Frozen Plasma (FFP) used for children and certain groups of adults needing frequent transfusions has also been imported. From 2004 onward, recipients of blood components have been excluded from donating blood, in order to prevent vCJD - or potentially other infections - being “recycled” within the population.
In 2019, the advisory committee on the Safety of Blood, Tissues and Organs (SaBTO) evaluated if these risk reduction measures should be maintained. The modelling conducted by DHSC and reviewed by independent experts on the Advisory Committee on Dangerous Pathogens - Transmissible Spongiform Encephalopathies (ACDP TSE) Sub Group showed that the impact of these measures was small. If these risk reduction measures were not in place, a further 1-2 clinical cases may occur due to plasma transfusions that take place over the next 50 years (worst case 15 extra cases). This means that the additional risk of death from transfusion-acquired vCJD would on average be 1 in every 5.2 million units of UK-plasma transfused (SaBTO report, March 2019). As a result, these measures were withdrawn. Other risk reduction measures such as leucodepletion remain in place.
There are now concerns regarding the availability of normal immunoglobulins due to increasing demand, reliance on international product supply and a global decrease in the number of blood donations. This paper examines whether the risk of possible vCJD transmission has reduced sufficiently to allow the use of UK-sourced plasma for the manufacture of human immunoglobulins.
1.2. Patient need
The use of immunoglobulins has been steadily increasing since 2000 and various measures have been taken to ensure rational use and prevent product shortages. For example, the Department of Health appointed an immunoglobulin Expert Working Group in August 2006 to formulate the national Demand Management Programme. The clinical guidelines on immunoglobulin use are periodically revised to ensure scientifically justified use and adequate supply.
1.3. Epidemiological data
There are 4 forms of CJD: sporadic (sCJD), variant (vCJD), familial (genetic), iatrogenic. Causative agents of CJD are prions, composed of misfolded prion proteins (PrPSc), which form aggregates in neurological tissue leading to progressive brain damage and characteristic signs and symptoms of the disease.
Patients with vCJD have prominent psychiatric (frequently depression, anxiety and withdrawal) or sensory symptoms and delayed onset of neurologic abnormalities, including ataxia within weeks or months, and dementia and myoclonus late in the illness. The disease always progresses to death. Disease duration is 14 months on average. The definite diagnosis of vCJD requires post-mortem examination of brain tissue. vCJD is more contagious than CJD, presumably due to the causative prion being present in peripheral tissue. Most reported vCJD cases appear to have been infected through the consumption of bovine meat products contaminated with the agent of BSE. The incubation period after food borne exposure is thought to be around 10 years, possibly shorter than CJD.
Since 1995, 178 patients with definite and probable vCJD have been reported in the UK, the last of whom died in 2016.
Table 1: CJD in the UK
This can be accessed on the National CJD Research & Surveillance Unit website
Individual risk factors
There is individual variation in susceptibility to infection, with possible influences including age and the prion protein gene (PRNP) genotype. Compared to CJD, which tends to affect middle-aged and elderly individuals, vCJD predominantly affects younger individuals, with an average age of onset of around 28 years and median age at death of 28 years.
Transmission
Cases of transmission of vCJD from blood transfusion have only been reported in the UK. A total of five people died following transmission of vCJD from blood donors who later developed vCJD; two of them died from another cause with no symptoms of brain disease but were found to have evidence of vCJD in their spleen, which could represent a pre-clinical form of the disease (Peden, 2010). All the recipients infected by blood transfusion had received red cells that had not been leucodepleted. There have been no reports of vCJD transmission from plasma or platelet transfusion.
No evidence of vCJD iatrogenic transmission by any form of surgery, dentistry, endoscopy, organ transplantation or childbirth has been identified unlike iatrogenic transmission of CJD (from patients with either sporadic or genetic forms of CJD), which has been reported in many countries including the UK, particularly in recipients of human pituitary-derived growth hormone or human dura mater grafts, or following neurosurgery.
Subclinical disease
Unlike sporadic CJD, the variant form is associated with the accumulation of misfolded prion protein (PrP) in the lymphoreticular system (lymph nodes, tonsils, spleen and lymphoid follicles in intestinal organs. Two appendectomy sample surveys estimated the prevalence of abnormal prion protein (PrP) in the British population exposed to BSE to be 237 per million and 493 per million, respectively. A third survey was recommended to measure the prevalence of abnormal PrP in population groups thought to have been unexposed to BSE. None of the seven positive samples found were from appendices removed before 1977, or in patients born after 2000 and none came from individuals diagnosed with vCJD. Two interpretations are possible. Either there is a low background prevalence of abnormal PrP in human lymphoid tissues that may not progress to vCJD. Alternatively, all positive specimens are attributable to BSE exposure, a finding that would necessitate human exposure having begun in the late 1970s and continuing through the late 1990s. The contrast between the prevalence of abnormal PrP and the number of clinical vCJD cases seen to date strongly suggests that possibly none of those in whom abnormal PrP is detected through an ante-mortem lymphoid tissue survey will develop any symptoms of prion disease (Gill et al., 2020).
2. Description of immunoglobulin products
Immunoglobulins are a subset of medicinal products that can be derived from human (and animal) blood. The two types of immunoglobulin products included in this review are referred to as “normal” immunoglobulin and “hyperimmune” immunoglobulin.
2.1. Products and indications
2.1.1. Normal Ig products
Normal immunoglobulin products are cocktails of antibodies to a wide variety of antigens, circulating in human blood. They confer passive immunity to individuals who may be immunodeficient. There are two product formulations of normal Ig – for subcutaneous (SCIG) and intravenous (IVIG) administration. Different products differ in their pharmaceutical properties but the active ingredient of all of the products is the same. SCIG and IVIG have different pharmacokinetics, whereas IVIG usually requires administration every 3 or 4 weeks, SCIG infusions are typically administered more frequently (biweekly, weekly and even daily based on patient need (Ness S., 2019)).
The indications of normal Ig products include i) replacement therapy in primary and secondary immunodeficiency syndromes with impaired antibody production and ii) immunomodulation in primary immune thrombocytopenia and other auto-immune diseases. In addition, some SCIGs have indications in hepatitis A prophylaxis due to high content of anti-HAV antibodies.
2.1.2. Hyperimmune Ig products
Hyperimmune Ig products target a more specific indication or deficiency. They are usually isolated from individuals who are specifically immunised with or selected according to the antigen of interest with the objective to harvest the antibodies of interest. The key factor is that hyperimmune products offer a higher titre of antibodies for specific indications, as compared to normal immunoglobulin. Hyperimmune products currently manufactured from human blood are for prevention of infectious diseases (cytomegalovirus, hepatitis B, rabies, tetanus and varicella zoster) and of rhesus D isoimmunisation.
2.2. Usage data in the UK
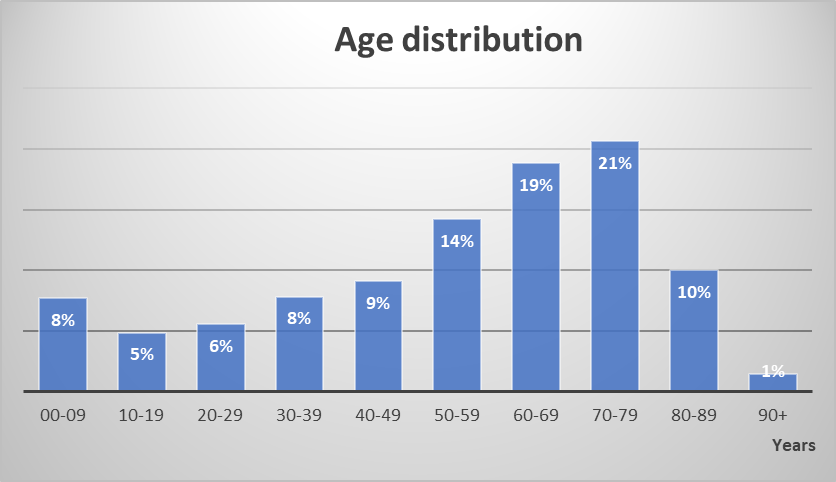
An annual report from the NHS Immunoglobulin Database (for England and Northern Ireland) is publicly available and additional data have been obtained from MD/SAS, which is monitoring the database. In 2018/2019, 17,720 patients received 5,868,858 g of normal Igs. Almost two thirds of these patients are under long-term treatment with an average dose of 36 g per administration. The average dose for short-term treatment is slightly lower (32 g). The age distribution of the patient population is represented in Figure 1; half of the patients are ≥ 60 years old.
{kind=link}
In 2018/2019, intravenous products accounted for 80% of the total volume of normal Igs. In terms of indications, almost equal proportions of the total volume of normal Igs were used in immune deficiencies (45%) and neurologic diseases (43%), e.g. chronic inflammatory demyelinating polyradiculoneuropathy or multifocal motor neuropathy, followed by haematologic diseases (6%), mainly immune thrombocytopenic purpura. A similar database exists for Scotland, which recorded in 2018/2019 the treatment of 1,585 patients for a volume of 479,320 g of normal Igs.
Finally, the use of hyperimmune Igs is extremely limited when compared to normal Igs. Information was obtained from Public health England (PHE) that in 2019, 364 vials of anti-hepatitis B Ig and 1304 vials of anti-varicella zoster Ig were purchased.
Figure 1. Age distribution of patient population that received normal Igs in 2018/2019
3. Risk evaluation
Two approaches have been used to address the risk of possible vCJD transmission by administering Igs manufactured from UK-sourced plasma: an external expert consultation and a modelling of the risk for various human Ig products authorised in the UK.
3.1. MHRA external consultation
The MHRA carried out an external consultation with a wide range of stakeholders including plasma product manufacturers, academic scientists specialising in prion diseases, relevant government organisations, and patient/medical professional organisations with the following objectives.
Manufacturers presented an overview of the changes in scientific knowledge that support the conclusion that the risk of vCJD transmission by plasma products is significantly lower than initially estimated. They further discussed the ability of some manufacturing processes to clear prion protein and reduce infectivity.
Patient associations emphasised the striking contrast between past predictions and actual vCJD figures. They highlighted the results of the long-term surveillance of UK haemophilia patients and those who received immunoglobulin. No cases of vCJD have occurred in the 75 Primary Immunodeficiency patients exposed to UK-sourced immunoglobulin between 1997 and 2000 (Helbert et al, 2016). Finally, they proposed that the vCJD risk should be compared to the potential harm to patients because of plasma product supply difficulties.
There is a consensus among prion experts that transmission of vCJD through blood products is possible. However, most infectivity is associated with cells with lower levels in the plasma. Furthermore, very few cases (3 clinical cases and 2 subclinical cases) of actual transmission have been identified by a reliable set of surveillance systems and importantly, none for some time as the last died in 2008. Of these 5 cases, four were related to (non-leucodepleted) red blood cells transfusion and only one subclinical case was possibly related to Factor VIII products.
The overall vCJD risk from plasma products appears to be significantly lower than when the ban on UK plasma was implemented. Most experts acknowledge the methodologies for the reduction/elimination of both PrPSc and prion infectivity during plasma processing, which indicates that any prion infectivity present in the original plasma is highly unlikely to carry through to the final protein products and the Medical Research Council (MRC) Prion Unit evaluates the risk from zero to very small. However, a validated specific vCJD inactivation step in the fractionation process and a reliable test for vCJD in donors/potential carriers are yet to be developed.
There is also a consensus that the decline of vCJD cases in the general UK population has been more rapid than predicted but there is still significant uncertainty over the number of asymptomatic carriers of infection, who have the potential to transmit the infection via transfusion or other iatrogenic routes. Nevertheless, the contrast between the prevalence of abnormal PrP in the appendectomy sample surveys and the number of clinical vCJD cases seen to date strongly suggests that possibly none of those in whom abnormal PrP is detected will develop any symptoms of prion disease. Also, given the estimated number of people with asymptomatic infection, what is known and what is assumed about infection risks, it is very notable that so few transmissions via transfusion have been identified, and thus, the overall risk must be considerably lower than originally feared.
At the outset of the vCJD outbreak, all patients were found to be homozygous MM at codon 129 of the PRNP gene. Experts generally agree that a second wave of vCJD has started for individuals heterozygous at codon 129 who appear less susceptible to prion diseases and have long incubation times. Therefore, vigilance should be maintained although the MRC Prion Unit expects this second wave to involve zero to a small number of annual cases. Several experts are concerned that some cases of vCJD are misdiagnosed as sporadic CJD, especially in the elderly. This has been considered by NCJDRSU and an ongoing DH-funded study is being conducted in the elderly. Therefore, post-mortem examination of suspected CJD cases should be encouraged to reverse the declining trend that has been observed in recent years.
In conclusion, most experts acknowledge that there are arguments for changing the present plasma policy but that given the remaining uncertainties, a cautious approach should be adopted with continued or even enhanced surveillance of vCJD cases and risk mitigation strategies with an emphasis on the development of highly sensitive and specific markers of infection. Still, most estimate that the risk associated with blood product transmission is very low and definitely lower than initially expected 20 years ago.
3.2. Mathematical modelling of risk
3.2.1. Method
The risk assessment modelling was based on modifications of the model that was developed by DHSC, in conjunction with Clinical Operational Research Unit (CORU) University College London, to evaluate the risk of blood components.
Data were obtained from manufacturers of immunoglobulins on the volume of plasma to manufacture a batch, the batch size (weight of protein), and the prion reduction factor achieved by the manufacturing process. Donor exposure was calculated by dividing the volume of plasma to manufacture a batch by the average volume of FFP extracted from a single whole blood donation (263 ml).
The results are presented as the risk of infection and the risk of clinical case per million of single maximum doses as the risk is proportional to the dose. For normal Igs, the maximum of 140 g is based on the product information of normal Igs (2 g * 70 kg for an adult). For hyperimmune Igs, the maximum dose is based on the product information of the specific products. The risks are presented for the use of leucodepleted and non-leucodepleted plasma in the manufacturing process.
The calculated risks relate to the year 2020, subsequent years will have a lower risk due to the decline in dietary BSE exposure in the donor population. Risk of infection over time decreases roughly linearly by 3% a year until 2050. The risk of infection does not vary by age, however the risk of an infection developing into a clinical case will depend on the age of the patients. The age of a patient in receipt of a donation is not considered in the model.
The assumptions of the model, which were reviewed for the blood components model by the ACDP TSE subgroup, are considered highly precautionary. These include in particular the prevalence of infection in the donor population, the prion infectious load in blood donation, no plasmapheresis considered, the susceptibility of recipients and their normal life expectancy. This last assumption is clearly overconservative as in 2019, 51% of the normal Ig recipients is 60 years or older whereas this proportion is only 16% in the general UK population. Even the declining risk in the donor population may accommodate for a “second wave” of vCJD, which the MRC Prion Unit experts expect to be very low. As the calibration of the model is also highly precautionary, it is likely that the estimated number of infections and clinical cases of vCJD represent an overestimate and so will be lower in reality.
3.2.2. Results
3.2.2.1. Risks per dose
The risk of vCJD infection and clinical case was estimated for 17 normal Igs and 6 hyperimmune Igs for which data were provided by manufacturers.
The median risk of infection/clinical case was estimated from three separate models based on the pool size and batch weight data provided by manufacturers. The numerical values of the risks shown below are those of the upper limit of the 95% credible confidence interval for the median in the model with the highest risk value, which means that they correspond to the worst-case scenario and should be considered very cautiously. The maximum risk of infection and clinical case per million of maximum doses is presented for the various Ig products in decreasing order of risk and by leucodepletion status (Tables 2 to 9). Risk quintiles (range: 1-5) were derived based on using for each product the model with the highest upper limit of the 95% credibility interval for the risk value.
If using non-leucodepleted plasma, the risk of infection for normal Igs, expressed per million of single maximum doses (140 g), decreases from 324 to 0.0007 and the risk of a clinical case from 24 to 0.00005 depending on the products. Approximately 1 out of 10 infections is expected to lead to a clinical case. If using leucodepleted plasma, the risk of infection decreases from 67 to 0.00015 and the risk of a clinical case from 7 to 0.000015 depending on the products. As expected, leucodepletion reduces the risk of infection and clinical case, but for products with a very low risk, the impact of leucodepletion is negligible.
The risk of infection and clinical case has been ranked for the various products in descending order and it appears that this ranking corresponds exactly to the ascending ranking of the prion reduction factor (PRF). This observation confirms that the risk is closely and inversely correlated to the prion reduction factor.
All hyperimmune Igs studied have a high PRF (> 7). The risk of infection, using leucodepleted plasma, is less than 2 in 10 billion maximum doses for all products; the risk of clinical case is less than 2 in 100 billion maximum doses. For these products, the impact of plasma leucodepletion is negligible. The reason why hyperimmune Igs show lower risk than normal Igs with the same PRF is mainly due to the much smaller doses used (the maximum dose for the products assessed ranges between 38 and 1333 mg compared to 140 g for normal Igs). It is also noted that the donor exposure (pool size) is significantly smaller for hyperimmune Igs than for normal Igs. Overall, the risk of infection and clinical case appears extremely low for hyperimmune Igs.
Table 2. Risk of infection per million maximum doses: normal immunoglobulins –
leucodepleted plasma
Normal Igs / Leucodeplete
| Product ID | Maximum risk of infection per million doses of 140 g* | Risk quintile | Range | Prion reduction factor (log10) |
|---|---|---|---|---|
| 5 | 67 | 5 | 5.75-67 | 4.8 |
| 7 | 18.7 | 5 | 18.7-66.8 | 5.66 |
| 8 | 18.7 | 5 | 18.7-66.8 | 5.66 |
| 4 | 6.29 | 4 | 5-91-6.29 | 5.85 |
| 9 | 5.91 | 4 | 5.91-6.29 | 6.16 |
| 15 | 3.75 | 4 | 3.75-3.75 | 6.4 |
| 16 | 3.75 | 4 | 3.75-3.75 | 6.4 |
| 17 | 3.75 | 4 | 3.75-3.75 | 6.4 |
| 3 | 0.848 | 3 | 0.6084-2.63 | 6.8 |
| 12 | 0.0772 | 2 | 0.0608-0.0772 | 7.9 |
| 6 | 0.0608 | 2 | 0.0608-0.0772 | 8.26 |
| 1 | 0.00213 | 2 | 0.0213-0.0505 | 9.4 |
| 2 | 0.00213 | 2 | 0.0213-0.0505 | 9.4 |
| 10 | 0.000246 | 1 | 0.000119-0.00179 | 10.4 |
| 13 | 0.000184 | 1 | 0.000134-0.000184 | 10.3 |
| 14 | 0.00018 | 1 | 0.000134-0.000184 | 10.3 |
| 11 | 0.000147 | 1 | 0.000147-0.00191 | 10.5 |
*Risk represents the upper limit of the 95% credible confidence interval for the median from the model with the highest risk value
Table 3. Risk of infection per million maximum doses: normal immunoglobulins -
non-leucodepleted plasma
Normal Igs / Non-Leucodepleted
| Product ID | Maximum risk of infection per million doses of 140 g * | Risk quintile | Range | Prion reduction factor (log10) |
|---|---|---|---|---|
| 5 | 324 | 5 | 27.9-324 | 4.8 |
| 7 | 90.5 | 5 | 90.5-323 | 5.66 |
| 8 | 90.5 | 5 | 90.5-323 | 5.66 |
| 4 | 30.5 | 4 | 28.6-30.5 | 5.85 |
| 9 | 28.6 | 4 | 28.6-30.5 | 6.16 |
| 15 | 18.2 | 4 | 18.2-18.2 | 6.4 |
| 16 | 18.2 | 4 | 18.2-18.2 | 6.4 |
| 17 | 18.2 | 4 | 18.2-18.2 | 6.4 |
| 3 | 4.11 | 3 | 0.331-12.7 | 6.8 |
| 12 | 0.374 | 2 | 0.295-0.374 | 7.9 |
| 6 | 0.295 | 2 | 0.295-0.374 | 8.26 |
| 1 | 0.0103 | 2 | 0.0103-0.244 | 9.4 |
| 2 | 0.0103 | 2 | 0.0103-0.244 | 9.4 |
| 10 | 0.00119 | 1 | 0.000577-0.00866 | 10.4 |
| 13 | 0.000889 | 1 | 0.00065-0.000889 | 10.3 |
| 14 | 0.000872 | 1 | 0.00065-0.000889 | 10.3 |
| 11 | 0.000711 | 1 | 0.000711-0.00925 | 10.5 |
*Risk represents the upper limit of the 95% credible confidence interval for the median from the model with the highest risk value
Table 4. Risk of clinical case per million maximum doses: normal immunoglobulins –
leucodepleted plasma
Normal Igs / Leucodepleted
| Product ID | Maximum risk of clinical case per million doses of 140 g | Risk quintile | Range | Prion reduction factor (log10) |
|---|---|---|---|---|
| 5 | 6.65 | 5 | 0.571-6.25 | 4.8 |
| 7 | 1.86 | 5 | 1.86-6.63 | 5.66 |
| 8 | 1.86 | 5 | 1.86-6.63 | 5.66 |
| 4 | 0.624 | 4 | 0.587-0.624 | 5.85 |
| 9 | 0.587 | 4 | 0.587-0.624 | 6.16 |
| 15 | 0.372 | 4 | 0.372-0.372 | 6.4 |
| 16 | 0.372 | 4 | 0.372-0.372 | 6.4 |
| 17 | 0.372 | 4 | 0.372-0.372 | 6.4 |
| 3 | 0.0842 | 3 | 0.00679-0.261 | 6.8 |
| 12 | 0.00766 | 2 | 0.00604-0.00766 | 7.9 |
| 6 | 0.00604 | 2 | 0.00604-0.00766 | 8.26 |
| 1 | 0.000212 | 2 | 0.000212-0.00501 | 9.4 |
| 2 | 0.000212 | 2 | 0.000212-0.00501 | 9.4 |
| 10 | 0.000024 | 1 | 0.0000118-0.000177 | 10.4 |
| 13 | 0.000018 | 1 | 0.0000133-0.0000182 | 10.3 |
| 14 | 0.000018 | 1 | 0.0000133-0.0000182 | 10.3 |
| 11 | 0.000015 | 1 | 0.0000146-0.00019 | 10.5 |
*Risk represents the upper limit of the 95% credible confidence interval for the median from the model with the highest risk value
Table 5. Risk of clinical case per million maximum doses: normal immunoglobulins –
non-leucodepleted plasma
Normal Igs / Non-leucodepleted
| ID | Maximum risk of clinical case per million doses of 140 g | Risk quintile | Range | Prion reduction factor (log10) |
|---|---|---|---|---|
| 5 | 23.6 | 5 | 2.03-23.6 | 4.8 |
| 7 | 6.58 | 5 | 6.58-23.5 | 5.66 |
| 8 | 6.58 | 5 | 6.58-23.5 | 5.66 |
| 4 | 2.22 | 4 | 2.08-2.22 | 5.85 |
| 9 | 2.08 | 4 | 2.08-2.22 | 6.16 |
| 15 | 1.32 | 4 | 1.32-1.32 | 6.4 |
| 16 | 1.32 | 4 | 1.32-1.32 | 6.4 |
| 17 | 1.32 | 4 | 1.32-1.32 | 6.4 |
| 3 | 0.299 | 3 | 0.0241-0.927 | 6.8 |
| 12 | 0.0272 | 2 | 0.0214-0.0272 | 7.9 |
| 6 | 0.0214 | 2 | 0.0214-0.0272 | 8.26 |
| 1 | 0.000751 | 2 | 0.000751-0.0178 | 9.4 |
| 2 | 0.000751 | 2 | 0.000751-0.0178 | 9.4 |
| 10 | 0.000087 | 1 | 0.000042-0.00063 | 10.4 |
| 13 | 0.000065 | 1 | 0.0000473-0.0000646 | 10.3 |
| 14 | 0.000063 | 1 | 0.0000473-0.0000646 | 10.3 |
| 11 | 0.000052 | 1 | 0.0000517-0.000673 | 10.5 |
*Risk represents the upper limit of the 95% credible confidence interval for the median from the model with the highest risk value
Table 6. Risk of infection per million maximum doses: hyperimmune immunoglobulins – leucodepleted plasma
Hyperimmune Igs / Leucodepleted
| Product ID | Maximum risk of infection per million doses | Risk quintile | Range* | Prion reduction factor (log10) |
|---|---|---|---|---|
| 23 | 0.000192 | 5 | 7.3 | |
| 19 | 0.000033 | 5 | 9.4 | |
| 22 | 0.000025 | 4 | 9.4 | |
| 20 | 0.000015 | 3 | 9.4 | |
| 18 | 0.0000061 | 2 | 9.4 | |
| 21 | 0.00000093 | 1 | 9.4 |
*No range as there was only 1 value per quintile
Table 7. Risk of infection per million maximum doses: hyperimmune immunoglobulins – non-leucodepleted plasma
Hyperimmune Igs / Non-leucodepleted
| Product ID | Maximum risk of infection per million doses | Risk quintile | Range* | Prion reduction factor (log10) |
|---|---|---|---|---|
| 23 | 0.000932 | 5 | 7.3 | |
| 19 | 0.000159 | 5 | 9.4 | |
| 22 | 0.000119 | 4 | 9.4 | |
| 20 | 0.000071 | 3 | 9.4 | |
| 18 | 0.00003 | 2 | 9.4 | |
| 21 | 0.0000045 | 1 | 9.4 |
*No range as there was only 1 value per quintile
Table 8. Risk of clinical case per million maximum doses: hyperimmune immunoglobulins – leucodepleted plasma
Hyperimmune Igs / Leucodepleted
| Product ID | Maximum risk of clinical case per million doses | Risk quintile | Range* | Prion reduction factor (log10) |
|---|---|---|---|---|
| 23 | 0.000019 | 5 | 7.3 | |
| 19 | 0.0000032 | 5 | 9.4 | |
| 22 | 0.0000024 | 4 | 9.4 | |
| 20 | 0.0000015 | 3 | 9.4 | |
| 18 | 0.00000061 | 2 | 9.4 | |
| 21 | 0.000000093 | 1 | 9.4 |
*No range as there was only 1 value per quintile
Table 9. Risk of clinical case per million maximum doses: hyperimmune immunoglobulins – non-leucodepleted plasma
Hyperimmune Igs / Non-leucodepleted
| Product ID | Maximum risk of clinical case per million doses | Risk quintile | Range* | Prion reduction factor (log10) |
|---|---|---|---|---|
| 23 | 0.000068 | 5 | 7.3 | |
| 19 | 0.000012 | 5 | 9.4 | |
| 22 | 0.0000087 | 4 | 9.4 | |
| 20 | 0.0000052 | 3 | 9.4 | |
| 18 | 0.0000022 | 2 | 9.4 | |
| 21 | 0.00000033 | 1 | 9.4 |
*No range as there was only 1 value per quintile
3.2.2.2. Risks with long-term treatment
Patients treated with normal Igs are unlikely to receive only one single dose of treatment, and therefore, it is important to estimate the risk of repeated administrations, the worst-case scenario being a life-time treatment at the maximum dose.
The risk from each dose is assumed to be independent and therefore the cumulative risk from multiple doses was calculated using the binomial distribution. Given the order of magnitude of the estimated risk values the risk from multiple doses is approximately additive. Calculations were performed using the upper limit of the 95% credibility interval of the median modelled risk using the highest risk value (as previously described).
The risk over time was calculated based on the assumption of a maximum yearly dose of 1000 g. This yearly dose is derived from the NHSE database, which provides the yearly Ig volume by indication with the number of patients affected; on average, the highest yearly dose was reported to be 917 g for the treatment of multifocal motor neuropathy.
The highest risk value was calculated for a year of treatment and then a cumulative risk over 33 years of treatment was calculated. This duration derives from the assumption that the risk of infection of blood donations decreases by 3% every year, so that after 33 years, it becomes null and therefore, the risk does not increase beyond this duration (i.e., after 2053). The risk of infection was estimated with or without adjustment for a 3% yearly decline, and likewise, the risk of clinical infection. It is acknowledged that there may still be clinical cases after this date due to previous transmissions, but there is no risk of a new infection beyond this point that leads to a clinical case.
Based on this risk, the average number of patients treated for 33 years at the maximum yearly dose for 1 infection or 1 clinical case to occur was estimated and, assuming an exposure to normal Igs of 30,000 patients per year, the expected number of infections/clinical cases in the population was calculated. The risk of clinical case is presented for the various products in decreasing order by leucodepletion status (adjusting for decreasing risk over time) (Tables 10 and 11).
The average number of patients to be treated for one clinical case to occur shows a wide range, spanning between ~ 500 million for products with a high PRF and a few thousand for products with a lower PRF. These numbers are obtained using leucodepleted plasma and adjusting for decreasing vCJD incidence over time. Finally, treating a cohort of 30,000 patients for at least 33 years at the maximum dose may potentially result in less than 1 clinical case for products with a high PRF and 24 cases for the product with the lowest PRF.
To contextualise these results, which have been obtained with extreme exposure assumptions, it is helpful to compare them with those estimated for FFP transfusion. Based on the data provided by the manufacturers, a single dose of 140 g has a lower risk of secondary vCJD infection than transfusion of a single unit of FFP. Nevertheless, as the risk for normal Igs increases with long-term treatment, it should be judged in light of the risk of clinical cases estimated for FFP in the DHSC model that was used by the SaBTO committee to recommend the withdrawal of risk reduction measures in place.
The model estimated that the worst case would be 15 clinical cases due to plasma transfusions over the next 50 years (SaBTO report, March 2019). Based on the numerical values previously mentioned, it appears that for the majority of normal Ig products assessed, the expectation would be a much lower number of cases than with FPP. Only for the products with a low PRF would the number of cases be of the same order of magnitude as estimated for FFP. Furthermore, for these products, the impact of plasma leucodepletion becomes noticeable as the number of clinical cases is multiplied by a factor of ~3.5 if using non-leucodepleted plasma.
Table 10. Maximum risk of clinical case after 33 years: normal immunoglobulins – leucodepleted plasma
Normal Igs
| Leucodepleted | Adjusting for decrease in risk over time | ||
|---|---|---|---|
| Product ID | Maximum risk of clinical case per 33 years of treatment | Average number of patients treated for 33 years for 1 clinical case | Expected number of clinical cases in 30, 000 patients treated for 33 years |
| 5 | 8.14E-04 | 1,228 | 24 |
| 8 | 2.27E-04 | 4,398 | 7 |
| 7 | 2.27E-04 | 4,398 | 7 |
| 4 | 7.65E-05 | 13,067 | 2 |
| 9 | 7.19E-05 | 13,906 | 2 |
| 15 | 4.56E-05 | 21,916 | 1 |
| 16 | 4.56E-05 | 21,916 | 1 |
| 17 | 4.56E-05 | 21,916 | 1 |
| 3 | 1.03E-05 | 96,861 | 0.31 |
| 12 | 9.39E-07 | 1,065,120 | 0.028 |
| 6 | 7.40E-07 | 1,350,828 | 0.022 |
| 2 | 2.59E-08 | 38,560,670 | 0.001 |
| 1 | 2.59E-08 | 38,560,670 | 0.001 |
| 10 | 2.99E-09 | 334,084,692 | 0.0001 |
| 13 | 2.23E-09 | 447,764,830 | 0.0001 |
| 14 | 2.19E-09 | 456,319,149 | 0.0001 |
| 11 | 1.79E-09 | 559,961,439 | 0.0001 |
Table 11. Maximum risk of clinical case after 33 years: normal immunoglobulins –
non-leucodepleted plasma
| Normal Igs | |||
|---|---|---|---|
| non-leucodepleted | Adjusting for decrease in risk over time | ||
| Product ID | Maximum risk of infection in 33 years of treatment | Average number of patients treated for 33 years for 1 clinical case | Expected number of infections in 30,000 patients treated for 33 years |
| 5 | 2.89E-03 | 346 | 87 |
| 8 | 8.07E-04 | 1,240 | 24 |
| 7 | 8.07E-04 | 1,240 | 24 |
| 4 | 2.72E-04 | 3,683 | 8 |
| 9 | 2.55E-04 | 3,919 | 8 |
| 15 | 1.62E-04 | 6,177 | 5 |
| 16 | 1.62E-04 | 6,177 | 5 |
| 17 | 1.62E-04 | 6,177 | 5 |
| 3 | 3.66E-05 | 27,298 | 1 |
| 12 | 3.33E-06 | 300,174 | 0.10 |
| 6 | 2.63E-06 | 380,693 | 0.079 |
| 1 | 9.20E-08 | 10,867,228 | 0.003 |
| 2 | 9.20E-08 | 10,867,228 | 0.003 |
| 10 | 1.06E-08 | 94,152,239 | 0.0003 |
| 13 | 7.92E-09 | 126,189,791 | 0.0002 |
| 14 | 7.78E-09 | 128,600,525 | 0.0002 |
| 11 | 6.34E-09 | 157,809,152 | 0.0002 |
4. Possible risk mitigation measures
There are two main approaches that could be used to further reduce the risk of vCJD transmission by plasma-derived medicinal products: controlling the quality of the starting material to ensure that only low-risk material enters the manufacturing process, and controlling the manufacturing process to ensure that it provides a sufficient level of safety to accommodate the use of UK-sourced plasma.
The first approach could include donor deferral (e.g. based on medical history, age) or starting material/pool testing (if a suitable test becomes available). The second approach could include mandating leucodepletion, the use of prion or nano-filters, specific combinations of numbers of donations and prion reduction factor to ensure an acceptable risk. Additional measures could relate to traceability of the sourced plasma and effective methods for cleaning manufacturing equipment.
5. Overall discussion
There is an increased need for plasma-derived products but, at present, there is a ban on the use of UK plasma to make such products. Two approaches have been taken to evaluate the risk of allowing for the use of UK plasma in the manufacture of immunoglobulins (normal and hyperimmune Igs).
A consultation with stakeholders (manufacturers, patient associations, government organisations) as well as prion experts has been conducted. There is a general consensus that the decline of vCJD cases in the general UK population has been more rapid than initially predicted. Manufacturers of human immunoglobulins as well as patient representatives argue for wider plasma resources due to increasing demand for treatments in face of decreasing blood donations worldwide, including in the US, due to the COVID-19 pandemic. Although all academics recognise that it is timely to conduct a review of the vCJD risk from the use of UK plasma, their approach is understandably cautious as there is still significant uncertainty over the number of asymptomatic carriers, who have the potential to transmit the infection via transfusion or other iatrogenic routes. Still, most prion experts estimate that the risk associated with blood product transmission is very low and definitely lower than initially expected 20 years ago.
The risk assessment based on the modified DHSC model predicts that there will be no additional vCJD cases or only a very small number of cases in the future if allowing for the use of leucodepleted plasma from UK donors in the manufacture of normal Igs. In the examined worst-case scenario, the number of clinical cases related to long-term treatment with normal Igs would be of the same order of magnitude as the number previously predicted if extending the use of UK FFP to the whole population. This risk level was considered acceptable and prompted the SaBTO committee to recommend that, based only on vCJD risk, the risk reduction measures for individuals born on or after 1st January 1996 be withdrawn.
The use of non-leucodepleted plasma has a marginal impact on products with high PRF but may become relevant for the products with the lowest PRF although, as emphasised throughout the whole report, the actual risks are likely to be much smaller than the estimated risks due to the highly precautionary approach of all assumptions and calibrations.
No additional risk is predicted for hyperimmune Igs as their use is mainly occasional and their doses are much lower compared to normal Igs.
The need for risk mitigation measures and their nature is dependent upon the level of risk that is considered as acceptable. Any additional safety measures that may be recommended may have profound impact on manufacturers and should therefore be carefully considered.
6. Overall conclusion
On the basis of current scientific knowledge, it is considered that the use of plasma from UK donors for the manufacture of human Ig products would expose the target patient population to no or minimal additional risk of vCJD in the future. In the worst-case scenario, this risk is estimated to be of the same order of magnitude as the risk considered acceptable by the SaBTO committee in 2019 for the administration of FFP.
7. List of references
- Gill ON et al. Prevalence in Britain of abnormal prion protein in human appendices before and after exposure to the cattle BSE epizootic. Acta Neuropathol 2020; 139: 965–976.
- National Creutzfeldt-Jakob Disease Research & Surveillance Unit Data
- Ness S. Differentiating characteristics and evaluating intravenous and subcutaneous immunoglobulin. Am J Manag Care. 2019 Jun;25(6 Suppl):S98-S104.
- NHS Immunoglobulin Database Annual Reports
- Peden A et al. Variant CJD infection in the spleen of a neurologically asymptomatic UK adult patient with haemophilia. Haemophilia 2010; 16: 296–304.
- SaBTO: Advisory Committee on the Safety of Blood, Tissues and Organs. Paediatric Components Working Group Report: Importation of plasma and use of apheresis platelets as risk reduction measures for variant Creutzfeldt-Jakob Disease. 2019
- Department of Health and Social Care: Technical Report - Risk assessment of the transmission of vCJD by blood components. 2019. vCJD transmission by blood components: risk assessment.