COVID-19 Ethnicity subgroup: Interpreting differential health outcomes among minority ethnic groups in wave 1 and 2, 24 March 2021
Updated 13 May 2022

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/covid-19-ethnicity-subgroup-interpreting-differential-health-outcomes-among-minority-ethnic-groups-in-wave-1-and-2-24-march-2021/covid-19-ethnicity-subgroup-interpreting-differential-health-outcomes-among-minority-ethnic-groups-in-wave-1-and-2-24-march-2021
Executive summary
1. It is clear from ONS quantitative studies that all minority ethnic groups in the UK have been at higher risk of mortality throughout the COVID-19 pandemic (high confidence). Data on wave 2 (1 September 2020 to 31 January 2021) shows a particular intensity in this pattern of differential mortality among Bangladeshi and Pakistani groups (high confidence).
2. This paper draws on qualitative and sociological evidence to understand trends highlighted by the ONS data and suggests that the mortality rates in Bangladeshi and Pakistani groups are due to the amplifying interaction of: I) health inequities; II) disadvantages associated with occupation and household circumstances; III) barriers to accessing health care; and IV) potential influence of policy and practice on COVID-19 health-seeking behaviour (high confidence).
I) Health inequities
3. Pakistani and Bangladeshi groups suffer severe, debilitating underlying conditions at a younger age and more often than other minority ethnic groups due to health inequalities. They are more likely to have 2 or more health conditions that interact to produce greater risk of death from COVID-19 (high confidence).
4. Long-standing health inequities across the life course explain, in part, the persistently high levels of mortality among these groups in wave 2 (high confidence).
II) Disadvantages associated with occupation and household circumstances
5. Occupation: Pakistani and Bangladeshi communities are more likely to be involved in: work that carries risks of exposure (such as retail, hospitality, taxi driving); precarious work where it is more difficult to negotiate safe working conditions or absence for sickness; and small-scale self-employment with a restricted safety net and high risk of business collapse (high confidence). By comparison, Black African and Black Caribbean groups who work more widely in health and social care roles were likely not fully protected in wave one, but consistent access to workplace PPE and new safe practices and regulations in wave 2 in health and social care settings may have produced comparatively less transmission in this group (low confidence).
6. Household circumstances among Bangladeshi and Pakistani families amplify disadvantage due to higher numbers of multigenerational households, family members with chronic, disabling illness (at a younger age) and women involved in care work for family or others (medium confidence). [See SAGE Ethnicity Subgroup, 2020b.]
III) Barriers to accessing health care
7. Stigma: All minority groups face stigma. Bangladeshi and Pakistani groups face intersecting forms of stigma and racism relating to their ethnic and their religious identity, and triggering events intensify experiences of stigma, including media coverage and central government COVID-19 interventions, for instance introducing restrictions during celebrations such as Eid and Ramadan. Stigma can cause health inequalities, drive morbidity and mortality, and undermine access to health services (medium confidence).
8. Over-burdened health services: The regions in which Bangladeshi and Pakistani communities live – such as in London and the Northwest – have faced high COVID-19 hospitalisations over a longer period of time, with greater strains on GP services (high confidence).
9. Practical difficulties of access: it is more difficult for minority ethnic groups to access NHS Track and Trace services due to testing site locations, difficulties taking time off from work for testing, and concerns about loss of livelihood if required to self-isolate (medium confidence).
IV) Potential influence of policy practice on COVID-19 health-seeking behaviour
10. Financial support: Furlough, self-employment and business support schemes have helped thriving businesses and better-off self-employed people the most, rather than those in the most hard-pressed situations (high confidence).
11. Communications and community support: The Black Lives Matter movement increased solidarity within and between Black African and Black Caribbean groups. Additionally, culturally appropriate approaches to delivering health education may have increased knowledge of COVID-19 in Black communities in the UK (medium confidence). By contrast, British Pakistani and Bangladeshi communities have been stigmatised by media narratives around multigenerational households and religious festivals, which can result in barriers to seeking help and contribute to more severe health problems (medium confidence).
Key findings
A range of steps have the potential to deliver greater health equity and aid recovery from COVID-19 impacts:
For immediate consideration
I) Health equity
a. MHCLG funded Community champion schemes are an effective means to reach minority ethnic communities, including Bangladeshi and Pakistani groups. There is scope to use these schemes in the future to target communications and support. In doing so, it would be important to include non-stigmatizing advice in relevant languages on multi-morbidities and COVID-19 risks, vaccination access, the importance of lateral flow testing in schools, and workplace risks and mitigations.
b. Evidence shows that vaccine access has been improved through provision in faith institutions. Inclusion of workplaces that are at risk for COVID-19 transmission, including factories, hospitality and retail may help increase uptake further among disadvantaged groups. [See SAGE Ethnicity Subgroup, 2020c.]
c. Unaffordability of taking unpaid time off, or concerns about the effect of absences on job security are likely to be significant contributory factors to low vaccination rates among low paid individuals, including ethnic minorities. UK employment law does not currently require employers to allow paid time off for vaccination (Hanif et al, 2020; CDC, 2021).
II) Occupation and household
d. Uptake of testing and adherence to self-isolation among groups who feel less able to do so given possible financial implications for themselves and their families should be incentivised. Evidence suggests that greater support for those who are socio-economically disadvantaged, including Bangladeshi and Pakistani groups (who predominantly work in precarious occupations), will enable them to adhere to the test, trace and isolate system (Bodas and Peleg, 2020 ,SPI-B, 2020b).
e. Other forms of practical help for those self-isolating, including accommodation outside the household and assistance from subsidised carers and with supplies of food and other provisions, would also likely increase adherence.
f. To improve testing uptake in disadvantaged and minority community areas, a focused health promotion campaign is needed to explain the importance of lateral flow testing in schools for the prevention of transmission to multigenerational households – as is providing easier access to lateral flow testing, for example by increasing the number of testing sites.
III) Accessing healthcare
g. Given evidence that Pakistani and Bangladeshi groups in particular have felt that communications in the context of COVID-19 have reinforced stigma, it is important to avoid stigmatising communications about vaccine uptake or in relation to local interventions, such as surge testing for variants in particular neighbourhoods or local restrictions. This might involve, for example, training and advice in the NHS and in Public Health Teams on the impact of stigma on health outcomes and on how to de-stigmatise interactions and communications.
IV) Communications
h. If it is necessary to restrict minority celebrations, explanations could emphasise that affected communities are hardworking and have faced exposure through occupations that serve and benefit the whole country.
i. Messaging should focus on testing equity and vaccine equity rather than testing or vaccine hesitancy.
j. Mass media communications can reduce stigma by promoting collective identity and social cohesion.
k. Effective community engagement is more likely to have an impact if it recognises within-group, inter-generational and gender differences. This requires working with diverse authority figures perceived to be locally legitimate. [See also SAGE Ethnicity Subgroup 2020a.]
For consideration over the medium term
l. Targeted investment in improving housing stock in overcrowded areas could help to alleviate increased transmission and risk in Bangladeshi and Pakistani communities based on evidence [showing that these groups have higher rates of living in crowded housing, which a driver of increased mortality and morbidity].
m. Improvements in the provision of COVID-safe formal elder care and childcare in socio-economically deprived and minority settings may help in reducing COVID-19 risks in these settings.
Further research should be considered in the following areas
n. On impacts of COVID-19 on all religious minorities and precarious migrant groups, such as those with no recourse to public funds.
o. On the impact of social cooperation (like that associated with the Black Lives Matter movement) on response to government COVID-19 public health initiatives.
p. On the amplifying intersections between employment, household and family structure that cause chronic COVID-19 transmission and higher mortality rates among minority groups.
q. On the long-term COVID-19 health effects (Long-Covid) for and socio-economic recovery among ethnic and religious minority groups.
r. On improving data quality throughout government on ethnicity and health inequality, including for subgroups of religion, gender and age.
I. Context and background
It is clear from quantitative studies that all minority ethnic groups in the UK have been at higher risk of mortality throughout the COVID-19 pandemic (high confidence). If we look at the existing data on wave 2 (1 September 2020 to 31 January 2021) we see a particular intensity in this pattern of differential mortality among Bangladeshi and Pakistani groups (high confidence). In this paper we concentrate on qualitative explanations for this pattern. However, further disaggregation of differential mortality among all minority ethnic groups is required, along with concerted policy attention to preventing unequal outcomes. Research-led policy is essential to prevent endemic COVID-19 related health disparities continuing during and after the vaccine roll-out.
In wave one (24 January to 31 August 2020) people from all minority ethnic groups were at greater risk of death from COVID-19 compared to White British groups (high confidence; OpenSAFELY, QResearch, Nafilyan 2021). Highest risk of mortality was evidenced among people from Black African ethnic backgrounds. In wave 2, risks among Black African and Black Caribbean groups compared with people of White British ethnicity still remained high but attenuated somewhat (medium confidence). However, this emerging data should be treated with caution, as it does not chart the full course of the pandemic in the UK. In addition, during wave 2, men and women from Bangladeshi and Pakistani ethnic groups were at a considerably higher risk of death involving COVID-19 compared with those of White British ethnicity (high confidence; ONS 2021). Rates were by far the highest among men and women from Bangladeshi backgrounds. They were closely followed by those from Pakistani backgrounds. Indian ethnic groups showed slightly less elevated levels above Black African and Caribbean groups. These patterns raise 3 important questions:
- Why is the risk of death highest for people from Bangladeshi and Pakistani groups in wave 2?
- What interventions could be made to support Bangladeshi and Pakistani communities to overcome these unequal outcomes?
- What policy measures could help to mitigate disparities in health outcomes among minority ethnic groups?
This paper draws on existing qualitative evidence to address these questions. However, further quantitative and qualitative research is required to prevent persistent, or even, rising health inequalities.
Differential health outcomes are the result of intersecting forms of disadvantage experienced by members of social groups over their life-course. Political, economic and social factors contribute to differing COVID-19 mortality rates, including structural inequalities faced by specific communities. As these factors combine, they can produce exponential impacts on social groups, increasing the transmission and severity of COVID-19, which are captured in statistics under an ethnicity identifier. The elevated mortality risk for Bangladeshi and Pakistani men and women in wave 2 data so far likely results from multiple socio-economic factors amplifying each other, rather than being due to a single aspect of their social or cultural circumstances (high confidence).
To explain such group effects, we need to look at the matrix of social relationships that produce mortality impacts. Therefore, in this paper we focus on:
I. health equity issues faced by minority ethnic groups
II. disadvantages produced by occupation and household circumstances
III. barriers to accessing health care
IV. potential influence of policy and practice on COVID-19 health-seeking behaviour
The interaction of I to IV generates elevated risk of illness and mortality from COVID-19. In distinct groups and their subgroups (of religion, age, gender, place and time of migration), different social inequalities may have greater or lesser impacts. It is particularly important to consider these intersections as we move into the next phase of the pandemic in the UK, including vaccination rollouts and Long-Covid support, or disparities will likely persist, and the pandemic may become a source of permanent health inequality.
I. Health equity
Ethnic minorities did not enter the pandemic on an equal footing in relation to their underlying health. It is well known that socio-economic inequality produces effects on physical health and the process of ageing (Nazroo, 2015). Underlying conditions can contribute to disease severity, thereby contributing to the persistently high levels of mortality among Pakistani and Bangladeshi groups (medium confidence).
Pakistani and Bangladeshi groups experience severe, debilitating conditions earlier and more often than other minority ethnic groups. This contributes to a process of weathering, or biological ageing, whereby disadvantages accumulate over the life course, producing increased risk of age-related conditions (Nazroo, 2015). In wave one, individuals from South Asian groups with COVID-19 infection experienced more severe health outcomes than those from other groups (Public Health England, 2020).
Additionally, according to the Health Survey for England, the level of reporting fair or bad health for White English people aged 61 to 70 years is equivalent to that of Black Caribbean and Indian people aged 46 to 50 years, Pakistani people aged 36 to 40 years and Bangladeshi people aged 26 to 30 years (Chouhan and Nazroo, 2020). British Pakistani and Bangladeshi men and women have the highest levels of self-reported poor health of all ethnic groups. This divergence appears at age 30 years, becoming steadily more marked among older age groups (Nazroo, 2015; Nazroo and Williams, 2006). The high levels of pre-existing chronic health conditions among Pakistani and Bangladeshi minorities (Platt and Warwick, 2020) create increased risk of severe complications from COVID-19 if infected (medium confidence).
Many of the co-morbidities associated with severe COVID-19 are more prevalent among British Pakistani and Bangladeshi groups than others (for example diabetes, ischaemic heart disease: Prats-Uribe et al. 2020). Additionally, they are more likely to have multimorbidity, that is, 2 or more long-term health conditions (Salway et al. 2007 cf. Zimedikun et al. 2018; Watkinson et al. 2021). Multimorbidity creates additional health needs beyond those from each individual condition. British Pakistani and Bangladeshi people with long-term health conditions are disproportionately likely to report activity limitations as a result (Salway et al. 2007, p.20-1). Self-reporting as disabled is a high risk factor for COVID-19, above risks associated with each individual health condition (ONS 2020).
Long-standing health inequalities across the life-course, and chronic health inequalities likely contribute to persistently high levels of mortality among Bangladeshi and Pakistani groups (medium confidence). These effects are likely to have been amplified by household members being disproportionately exposed to COVID-19, due to disadvantages associated with occupational and household settings (Section II).
II. Disadvantages Produced by Occupation and Household Circumstances
Exposure to and transmission of COVID-19 can be intensified through interconnections between risky working environments and household circumstances (high confidence). Here we define risky working environments in 3 ways:
a. they involve work that carries risks of exposure (the ONS definition)
b. they are precarious work in which it is difficult to negotiate safe working conditions or leaves of absence for sickness; or
c. they are small-scale self-employment with a restricted safety net and risk of business collapse
Occupational risks of exposure
Occupations that have greater exposure to virus (for example; health workers, social care, close contact workers, construction and warehouse workers) are associated with greater risk of infection (Hiironen et al. 2020) and death (ONS 2020a) (high confidence). Jobs associated with higher death risks are also those in which ethnic minorities are clustered (high confidence). For example, Black African men and women are particularly heavily concentrated in social care roles (ONS, 2014; Platt and Warwick, 2020) and ethnic minorities (including migrant workers) are heavily concentrated among security guards and cleaners. Men from Asian and Asian British groups are highly concentrated in jobs in the hospitality and in the wholesale and retail trade with over a third (36 per cent) of Bangladeshi men working in this sector. Pakistani and Bangladeshi women are over-represented among sales workers (Platt, forthcoming 2021). Additionally, in the Midlands, South Asian men and women are often employed in small-scale textile and other industrial or food production units. Alongside this they predominate in taxi driving (for example around 21 per cent of foreign-born Pakistani men are taxi drivers, as are 8 per cent of UK born Pakistani men) (Platt, forthcoming 2021).
These differences in occupation are likely to have contributed to differential exposure in wave 2 for distinct ethnic groups. During wave one, the workplaces of some Black African and Black Caribbean groups, for example those working in health and social care, were not yet fully protected (Community Cares 2021), but in wave 2 PPE and new safe practices and regulations may have produced less transmission in this group (low confidence). By contrast, Pakistani and Bangladeshi groups are likely to have continued to be at the same level of risk in their workplaces as it is unlikely that new COVID-19 secure practices were introduced (medium confidence).
The occupational risks for Bangladeshi and Pakistani groups may even have increased in the lead up to wave 2. In late September into October 2020, when case numbers were rising rapidly across most UK regions, hospitality and non-essential retail was kept open, exposing workers to risk of infection. When the UK entered a national lockdown on 5 November, essential retail remained open along with takeaway services even as numbers of cases rose steeply. At this point the relatively more transmissible variant emerged (B.1.1.7), creating a potentially greater risk of exposure for Pakistani and Bangladeshi groups who remained unable to work from home.
Precarity of work
Pakistani and Bangladeshi groups are also more likely to work in precarious work (short-term, contractual work, usually without union protection (high confidence). In this situation it is difficult to negotiate sick-leave, and if sick-leave is taken employees may be dismissed or penalised with shorter hours. Figures from the 2011 census that report that over half (54 per cent) of Bangladeshi men and women (56 per cent) worked part-time along with over half of Pakistani women (52 per cent) (ONS 2011). Part-time work is more likely to be precarious and associated with zero-hours contracts. The extent of zero-hours contracts across minority groups, and especially Pakistani workers, was also an issue addressed in the Women and Equalities Committee report on unequal impacts of the pandemic (House of Commons Women and Equalities Committee, 2020; Bowyer and Henderson, 2020).
Self-employment and risk of business collapse
Self-employment – where incomes may be especially uncertain – is also more prevalent amongst Pakistani and Bangladeshi men (high confidence). Pakistani men are over 70 per cent more likely to be self-employed than White British men (Platt and Warwick 2020); this presents distinct difficulties in reducing the risk of exposure or self-isolating in the event of symptoms, as most self-employed work among Pakistani men involves contact with the public. Non-attendance at work would risk business’ viability, in part because government measures only offered one-off loans to small businesses and initially did not support the self-employed (see below).
Household amplifications of disadvantage
Some deaths are direct consequences of exposure through employment, but it is likely that occupational exposure and severity of infection are amplified by household transmission. Recent work has illustrated how larger or multigenerational households are associated with risks of infection and death (high confidence; SAGE Ethnicity Subgroup, 2020b). This is due to several factors:
a. poor quality and dense housing stock, which creates high risk for transmission (SPI-B, EMG, 2020; SPI-B 2020c)
b. age structure of multigenerational households, which place older family members at risk of exposure from younger family members
c. caring for family members, social support and care networks that link households, particularly involving middle aged and older women; or
d. concentration of time within the home due to national restrictions, school closures and job losses, allowing prolonged exposure to viral loads within the home
While Black African and Black Caribbean households also have a multigenerational structure and will have been affected by job losses and school closures and face poor housing stock, these factors are amplified among Pakistani and especially Bangladeshi communities. Multigenerational households in Bangladeshi and Pakistani families contain family members with chronic, disabling illness at a younger age. Rates of age-adjusted disability are known to differ across ethnic groups, with those for Bangladeshi men historically being particularly high. Reported rates among Black Africans are, by contrast, markedly lower and there may be different responses to disability across ethnic groups (Salway et al. 2007). For example, long-term sick Pakistani and Bangladeshi people – especially in contexts of low labour demand – were likely to retreat from active participation in labour markets (Salway et al. 2007, p. 32; Gardner 2002), which suggests that long-term sick adults in these groups may be disproportionately exposed to household transmission (medium confidence).
This risk of household transmission may be exacerbated through an interaction between economic disadvantage and the multigenerational household (medium confidence). The economic downturn is likely to have affected Bangladeshi and Pakistani communities disproportionately especially because of their profile of precarious work and self-employment. The disproportionate impact could mean potential exposure to COVID-19 at home from younger family members spending more time with older, chronically ill members. Impacts could be expected to be exacerbated by increased stress which generates suppressed immune responses (Segerstrom and Miller, 2004; Algren et al., 2018).
The risk to family members with long-term health issues may also be increased through transmission from schoolchildren attending education in areas with high levels of community transmission (medium confidence). Family size differs substantially by ethnic group, and it is likely that multiple-child families would face greater risks than single-child households. In addition, recent research from Born in Bradford (Bingham et al., 2021) suggests that during school closures, there were substantial ethnic differences in the extent to which children spent time outside the home by ethnic group, with Pakistani children much less likely than White UK children to leave the home. Children previously exposed to transmission in schools or the community could then potentially be more likely to transmit to older family members within the home. This could occur despite the careful protective practices reported in recent research on British Pakistani families (Atiya Kamal, unpublished research), given the poor quality, dense housing stock that Bangladeshi and Pakistani families live in.
Multigenerational households are also ‘highly networked’ to the wider community through ties of social support and care-work which are especially important to maintain when formal services are closed, inaccessible or too expensive (Bear et al 2020, SPI-B Wellbeing and Household Connection). For many ethnic minority groups, these ties are often held together through the work of women, especially middle age and older women. The ONS reported from the 2011 census that the highest proportion of women who reported carrying out unpaid care work were Bangladeshi (54 per cent) and Pakistani (52 per cent) of all communities in the UK. Preliminary qualitative research indicates British Pakistani families in large and multigenerational households have implemented several control measures to reduce the risk of COVID-19 including limiting contact with wider networks, particularly where family members are identified as having increased risk due to age or co-morbidities (Atiya Kamal, unpublished research). However, it is likely that women carrying out paid and unpaid care labour may be at higher risk than the family members being cared for (medium confidence). There is some suggestion that this is the case from a recent paper and we should carry out further qualitative and quantitative research to address this (SAGE Ethnicity Subgroup, 2020b).
Overall, it is important to note that the multigenerational household in itself is not a single risk factor producing differential mortality effects. Instead, it is because of the amplifying effects of household stock, high density of family members, underlying health and disability, age structure, social support networks and occupational and school risks that we see persistently high mortality rates in Bangladeshi and Pakistani groups (high confidence).
It is notable that little quantitative or qualitative analysis to date has been able to examine how far household level factors interact with ethnicity and occupation for different minority groups. We need further research on this across all minority groups as mortality rates are inequitably high for all of them. We also need to immediately address the acute issues for all such groups.
III. Barriers to health
Stigma
Stigmatisation is the process of stereotyping, labelling, separation, status loss and discrimination, which can arise through media representations and in institutional and community settings. Evidence suggests that stigma including racism is a fundamental cause of health inequalities, and a driver of morbidity and mortality (Hatzenbuehler et al, 2013) which undermines access to housing, employment and health treatment (high confidence).
Stigma disrupts social relationships and creates behavioural or psychological responses among individuals and groups, generating physiological stress. All minority ethnic communities face stigma, affecting medical treatment, and responses to central government public health measures (Link and Phelan, 2001; Metzl and Roberts, 2014). Bangladeshi and Pakistani groups face intersecting forms of stigma and racism that relate to their ethnic and their religious identity (Samari et al., 2018).
A history of experiencing stigma can directly impact on individuals’ health, creating physiological effects including long-term health conditions, and preventing people from accessing health care and other public institutions (Karlsen and Nazroo, 2002; Karlsen and Nazroo, 2004; Wallace et al., 2016). Imbalances of power, inappropriate cultural idioms and lack of sympathy are longer-term experiences within health and social settings for minority groups in the UK (Memon et al, 2016). These experiences are increased by hostile environments and policies such as Prevent, which can lead to ethnic and religious minorities experiencing more difficulty trusting in, and seeking help from, healthcare and other institutions (Fazil et al., 2002; Laird et al., 2007).
Policy environments and events can intensify or decrease the experience of stigma and racism in institutions and workplaces, leading to changes in community norms, interpersonal relations and individual capacities (Stangl et al, 2019). The COVID-19 pandemic in the UK has intensified uncertainty and social distrust, and at times, stigmatisation of minority groups (Bear et al., 2020; Major and O’Brien, 2005). Recent research suggests that some central government COVID-19 interventions have unintentionally increased stigma against Muslim groups (medium confidence). In particular, the introduction of restrictions before Ramadan and Eid celebrations fuelled disproportionate public emphasis on transmission within this religious group, leading to direct effects on social cohesion (Abrams et al, 2020; Bliuc et al, 2019). Additionally, press and political coverage has often singled out multigenerational households in ethnically diverse neighbourhoods as a particular source of transmission. This has fuelled social division, hostility and stress for groups such as Pakistani and Bangladeshi communities. This is particularly problematic as levels of adherence to government regulations are high across all social groups, and research shows that South Asian families follow social restriction rules more than other groups overall (Bingham et al., 2021; Nandi and Platt, 2020). Such flashpoints of singling out communities can threaten individuals’ identities, widely reported in the stigma research literature, which intensifies historical experiences of exclusion, leads to greater psychological stress and more difficulty engaging with health initiatives (Major and O’Brien, 2004; Holzemer et al, 2007). Pakistani and Bangladeshi groups have therefore likely been adversely affected due to their public visibility during the local interventions in 2020, with potential physiological effects and undermining health seeking and engagement with institutional settings relating to COVID-19 (medium confidence).
It is essential that the public environment changes, particularly during the vaccination roll out and with the implementation of local interventions to prevent local transmission or surge-testing in areas where new variants emerge. If COVID-19 becomes endemic in a local area, public communications and media should clearly state this is due to the structural driver of socio-economic disadvantage, and supportive messages should be given to avoid compounding stigma and exclusion, and thereby worsening health outcomes from COVID-19. Unfortunately, the media emphasis on ‘BAME’ communities having low vaccine uptake may also unintentionally contribute to the process of stigmatisation, if not handled correctly. Similarly, if surge testing is carried out in a particular area, local public health teams and the national government must be considered in their communications about this to prevent singling out particular minority or religious groups.
Over-burdened health services and practical difficulties of access
Regions in London and the Midlands where many Bangladeshi and Pakistani communities live have had high COVID-19 hospitalisation rates over a longer period of time, along with greater strains on GP services, than other areas. There are also disparities in access to testing sites, with free taxi rides provided in some areas by charities, but not others, and difficulty accessing testing locations by public transport.
Barriers to health in relation to NHS Track and Trace
It is likely that there are barriers to testing among Black African, Black Caribbean, Pakistani and Bangladeshi groups (SPI-B, 2020d; Kamal et al., in prep). This likely reflects physical barriers (distance, lack of transport), occupational barriers (not being able to take time off work) and concerns about loss of livelihood for individuals, their family and community networks through a positive test (which would force self-isolation), and experiences of stigma. However, qualitative research to understand the reasons for delayed test-seeking is warranted.
Overall, this section suggests that stigma and racism affects health outcomes for all minority ethnic and religious groups, including during the COVID-19 pandemic, and its current effects require further research, However, due to public media attention to Muslims during Eid and Ramadan this has intensified between wave one and wave 2 for people of this faith including for Muslims in Bangladeshi and Pakistani groups. This may have contributed to more barriers to accessing health services. It is important that politicians, media, civil servants and local public health teams seek actively to reduce stigmatising practices and representations inside and outside of institutions, including in public communications around targeted variant surge testing, vaccines uptake and local interventions to prevent transmission.
IV. Potential influence of policy and practice on COVID-19 health-seeking behaviour
Rather than defining specific groups as ‘hard to reach communities’, it is more effective to address why certain social groups might find it difficult to protect themselves from COVID-19 exposure and how they might be supported to do this. Policies should therefore address questions of inequality alongside issues of trust and communication. In the sections that follow we will examine how insufficient financial and practical support, community engagement and communications may have produced persistently high levels of mortality in Bangladeshi and Pakistani groups in wave one and wave 2 (medium confidence).
Financial and practical support
Since Bangladeshi and Pakistani communities are disproportionately employed in precarious work or businesses, measures addressing their economic situation and workplace rights will help decrease COVID-19 exposure and transmission. The pressures to attend work even during local and national social restrictions were particularly intense for these communities (TUC, 2020; Matilla-Santander; 2021; Discover Society, 2020). In addition, precarious workers in textile factories, food production or retail and hospitality have little scope to not attend work if they are unwell (TUC, 2019). It may be that further regulations for COVID-safe workplaces would help with these situation of exposure along with regular inspections in environments that are known to be risky. Furlough, self-employment and business support schemes rolled out by the government have been shown to have benefited already thriving businesses and better-off self-employed people the most (Bear et al., 2020). Since Bangladeshi and Pakistani groups rely centrally on lower-rated businesses or lower income self-employed work they may have felt greater pressure to continue working during the second national lockdown. This was the crucial period in October to November when transmission through exposure would have been most risky and which contributed to the second peak in December 2020 to January 2021.
In addition, evidence shows that increased self-isolation payments would assist all low paid workers and therefore minority ethnic groups as well (SPI-B 2020b, Smith et al 2020, Bodas and Peleg 2020). Furthermore, while some localised support has been offered by local authorities to assist families to self-isolate should multiple members become unwell, which is particularly important for multigenerational household (SAGE Ethnicity Subgroup, 2020b), further support through food delivery, paid care workers and paid for accommodation outside the home may be required.
Looking to the present situation of vaccination roll-out, there is currently no legal or financial support for time off work to attend appointments. For precarious workers it is very difficult to ask for leaves of absence. Introducing workplace vaccination schemes in high risk workplaces including retail and hospitality, along with factories, and incentivising, or legally requiring, employers to give time-off for vaccination, along with a payment of a usual days wages to the employees, could enable more people in precarious and low-income work to get vaccinated (medium confidence; CDC, 2021).
ONS analysis for wave 2 mortality figures should also include mortality rates for ‘non-residents’ for all ethnic minority communities, as it is likely that recent migrants and people with no recourse to public funds are omitted from our public health measures and policy support (Bear et al., 2020).
Communications and community support
As many of the factors that relate to increased risk in minority ethnic groups are structural, such as occupation, the impact of health messages can be limited (SAGE ethnicity sub-group, 2020). However, health communication can support dissemination of public health information but must use culturally accessible language, be shared via trusted sources and tailored to reflect personal circumstances (SPI-B, 2020a).
Ongoing primary research has shown that during wave one, health messages were not reaching all Black, Bangladeshi and Pakistani groups due to inaccessible language, modes of delivery and mistrust towards formal organisations that were sharing the messages (Kamal, unpublished research; TSIP, 2020; medium confidence). This resulted in adopting a more strategic, co-designed approach to health messaging with a strong focus on community engagement (GOV.UK Press Release, 2021). In addition national communications in wave 2 occurred against the backdrop of a national anti-racist movement, Black Lives Matters (BLM), which began in June and continued through August 2020 and may have created greater empowerment. During the same period stigmatising communications towards some Bangladeshi and Pakistani groups increased (as outlined above). This hypothesis has not been tested and requires further research (hence low confidence). However, understanding the process of community engagement at the local level, and how it has been different for diverse ethnic and religious minority groups, may offer insights into different health disparity outcomes in wave one and wave 2.
The BLM movement has fostered greater empowerment within the Black African and Black Caribbean community and enabled these groups to express their frustrations of many years (medium confidence). This new empowerment may have created a sense of optimism and facilitated open dialogue which increased knowledge and contributed to greater use of cultural, religious and collaborative approaches to reducing risk and transmission of COVID-19 in Black communities in the UK (medium confidence) (Kamal and Bear, ongoing research). Strategies include sharing videos of elders having the vaccine and hosting a COVID-19 vaccine event to address misinformation stemming from historic issues of unethical scientific research and religious beliefs (Caribbean and African Health Network, 2021).
In contrast, recent and ongoing research shows that Bangladeshi and Pakistani groups have not reported similar feelings of empowerment (Kamal and Bear, ongoing research; Bear et al, 2020). While there is increased use of cultural, religious and collaborative approaches for these communities, access to evaluation data is limited. Stigmatising communications are known to disempower communities (Public Health Wales, 2019) and stigma can result in mistrust towards formal organisations and contribute to more severe health problems (Gronholm et al, 2021). Although community engagement efforts are now underway with MHCLG funded Community Champions schemes running in several parts of the UK, establishing and/or rebuilding trust may take longer, particularly for Bangladeshi and Pakistani groups in the absence of a national movement such as BLM. Some groups may feel more wary or sceptical of community engagement activities based on their experiences of wave 1 communications (Kamal et al 2020) (medium confidence). Effective community engagement will also involve recognising within-group, inter-generational and gender differences to ensure health messages do not treat minority ethnic groups as homogenous. Health messages should also be tailored to the lived experiences of these groups. Communications should avoid attaching locations and ethnicity to COVID-19 to minimise stigmatising attitudes towards specific groups and mass media strategies should be used as a platform for anti-stigma communications to promote social cohesion and collective identity (Gronholm et al, 2021) at a national and local level.
Annex: The case of Leicester
Laura Bear, Lucinda Platt and Nikita Simpson.
Here we illustrate how occupational, household disadvantage and stigma intersect through a case study of Leicester to produce a chronic situation of COVID-19 transmission. While Pakistani and Bangladeshi communities are not the largest minority group in this city, which is highly diverse, this example illustrates how socio-economic factors intersect to produce ethnic health disparities. We first set out the context and patterns of infections and deaths before drawing on ethnographic work to explain COVID-19 health outcomes.
With a population of a little over 0.5 million people, Leicester has a large Indian population, but also has substantial shares of Black African and Pakistani ethnic groups, compared to their representation in the population as a whole. Importantly, it has faced relatively high death rates in the aftermath of the first period of national restrictions from March to May 2020. It has also experienced specific local interventions since the end of June 2020 as well as substantial media attention, leading to stigmatisation. It has never had restrictions lifted and yet has experienced a chronic situation of COVID-19 transmission and mortality. Therefore from the patterns here we can pick up directly on underlying socio-economic interactions that generate disproportionate impact on minority ethnic groups.
Occupational disadvantage
Occupational distributions are distinctive in Leicester with large numbers of people working in risky and lower-paid occupations. Looking at the three-digit occupational level for the years 2015 to 2017 (ONS, no date), Leicester has markedly higher shares of Process Operatives, Transport Drivers, Assemblers and Routine Operators, Elementary Process Plant Occupations and Elementary Storage Occupations than for Great Britain as a whole. On the other hand, it has lower shares of various professional occupations including teaching and business professionals. While any occupational group has just a small percentage of all workers (a few per cent), the somewhat distinctive occupational profile nevertheless is of interest for the extent to which it may lead to greater risks – especially if the distribution among such occupations is uneven across the population. It is worth noting that in the ONS analysis of occupations, process plant operatives and elementary process operatives were among the occupations with higher risks of death (ONS, 2020). In fact all elementary occupations were associated with higher risks for men compared to the average, comparable to caring and service occupations. Working conditions have been flagged as more at the root of the greater risks for these occupations, compared to the greater chances of coming in contact with someone infected in health and social care occupations (POST, 2020). In addition, as argued in the main paper, these forms of work have greater precarity than others, making it hard for people to self-isolate because they are pressured by employers or cannot risk their livelihoods. It is important to note for example that deprivation among Indians is rather greater in Leicester than it is in other cities (Zuccotti and Platt 2017).
Locational and household disadvantage
The greatest housing and occupation disadvantage in Leicester (according to the 2011 census) is in the North-East and East, followed by the West and North-West districts. This ranking also captures ethnic differences, with minority groups living in the greatest numbers in the North-East, East and West of Leicester (Leicester City Council, 2011).
The central district of Leicester is relatively affluent and occupied by 2 university campuses and business and retail premises, with residential areas for students and skilled or professional occupations. It is predominantly of white ethnicity (49.7 per cent) with 4.3 per cent reporting as long-term sick or disabled. In the North-west (Beaumant Leys, Mowmacre Hill, Stocking Farm, Abbey Rise and New Parks) older housing estates are occupied by 65.3 per cent White Ethnicity, with an equal mix of retail, service, care, education, manufacturing and professional occupations. Overcrowding is at 12.1 per cent. 10 per cent are long-term sick or disabled.
In the North-East (Northfields and Tailby estates and the Golden Mile Shopping District) 52.8 per cent of the residents are Asian British: Indian with 24.9 per cent White British. Overcrowding is at a higher level of 14.7 per cent and the area is less affluent with 40.5 per cent working in retail or manufacturing with only 10 per cent in professional occupations. 9.5 per cent are long-term sick or disabled.
The East area of the city (St Matthews and St Peters Thurnby Lodge) includes the oldest housing stock in Leicester in the district known as Highfields. 46.9 per cent of the residents here are Asian British Indian with 20.8 per cent White British. Overcrowding is at an even higher level of 17.8 per cent. Job profiles are more deprived as well with 40 percent working in retail or manufacturing with 17.1 per cent in Elementary occupations and 11.9 per cent in Sales and Service sector. 9.9 per cent are long-term sick and disabled.
The South district is more suburban, white ethnicity and professional (Aylestone and Knighton, the Eyres Monsell estate, Aylestone Park, Saffron Lane, Knighton Fields, West Knighton and the Stoneygate Conservation Area). White ethnicity residents are 72 per cent with overcrowding at a low rate of 9 per cent. 60 per cent of people in this area are in professional, skilled, administrative and caring occupations. There are 7.4 per cent reporting as long term sick or disabled.
The West part of Leicester presents a more mixed picture with close packed terracing, council estates and a garden city estate (Braunstone, West End, Newfoundpool, Danes Hill and Fosse). 63.4 per cent are White ethnicity, with 10.8 per cent other white groups and 5.7 per cent Black African and Black Caribbean, and 9.9 per cent Indian. Overcrowding is high at 13.4 per cent and long term disability at 7.5 per cent. Professional profiles are similarly split with thirty percent in elementary or manufacturing process jobs, while 34 per cent are in skilled, service and professional trades.
Overall we see most of Leicester’s minority ethnic populations distributed in the following way within the most crowded, most socio-economically disadvantaged wards (Leicester City Council, 2011) Indian groups in -Spinney Hills, St Matthews, Highfields, Belgrave, North Evington, Leicester City, Rushey Mead, Latimer, Coleman; Black African groups in St Matthews (Somali especially), Beaumont and Braunstone’; Bangladeshi groups in Highfields, Spinney Hills and North Evington; and Pakistani groups in Spinney Hills, Highfields and Washbrook (Leicester City Council, 2011).
Patterns of infections and deaths
By 1 March, Leicester had experienced 34064 COVID-19 cases, a rate of 9616 per 100,000.
Figure 1 shows hose those infection rates evolved over time since 13 March 2020, though of course part of this is to do with the increase in testing.
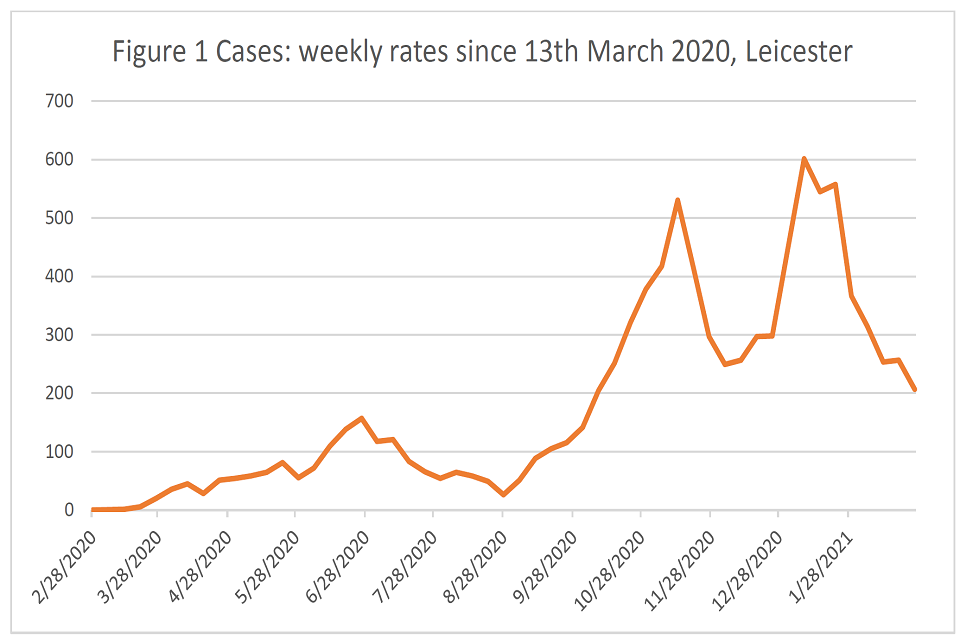
Line graph plotting weekly case rates (y-axis, ranging from 0 to 700) from 28 February 2020 to 28 January 2021 (x-axis, labels given in monthly intervals). The axes have a single trendline, coloured orange.
Figure 1: Cases: Weekly rates since 13 March 2020, Leicester. Source: derived from data downloaded from UK Coronavirus Dashboard on 2 March 2021.
Hospital admissions (Figure 1a) tend to follow the pattern for cases in the more recent period. In the earlier period cases only tended to be identified in hospital, hence the peak for hospitalisations is not reflected in the case rate for wave one.
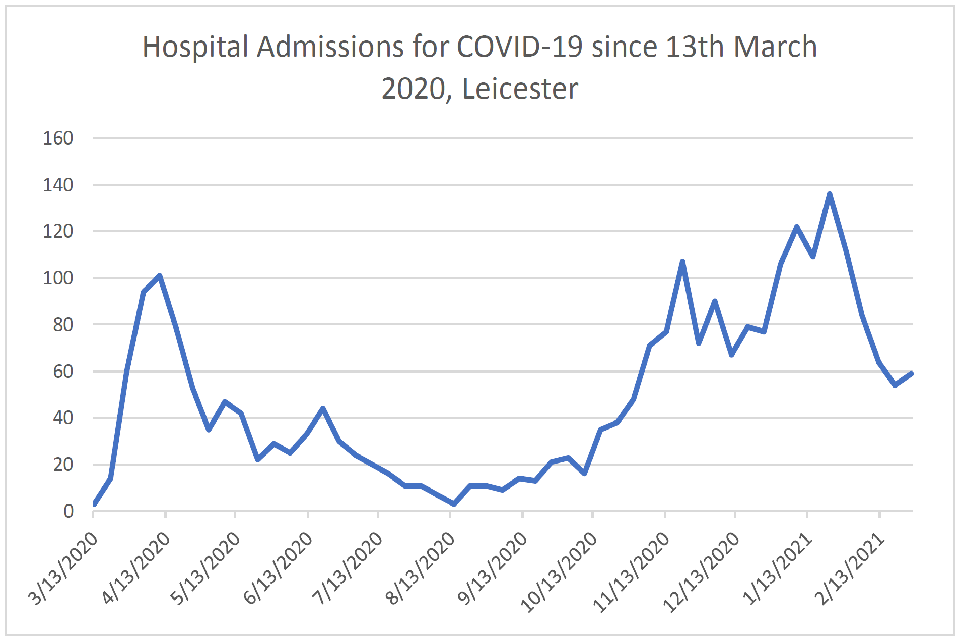
Line graph plotting hospital admissions for COVID-19 (y-axis, ranging from 0 to 160) from 13 March 2020 to 13 February 2021 (x-axis, labels given in monthly intervals). The axes have a single trendline, coloured blue.
Figure 1a: Hospital Admissions for COVID-19 since 13 March 2020, Leicester. Source: derived from data downloaded from: UK Coronavirus Dashboard on 2 March 2021.
There had been 731 COVID-19 deaths by 1 March 2021. Figure 2 shows how the cumulative total evolved over time. And for comparison, Figure 3 shows the cumulative rate (per 100,000 population) compared to Hackney, which makes it clear that the cumulative rate for Leicester overtook that for Hackney in May 2020. We have chosen to compare with Hackney because it is an area that has a diverse inner-city population too, but with a different occupational make-up, strong connections between the local authority and third sector and mutual aid groups and a greater amount of black African and Caribbean residents than Leicester. This comparison merits much further investigation than it is possible to complete here, including data from the end of the second wave in Hackney.
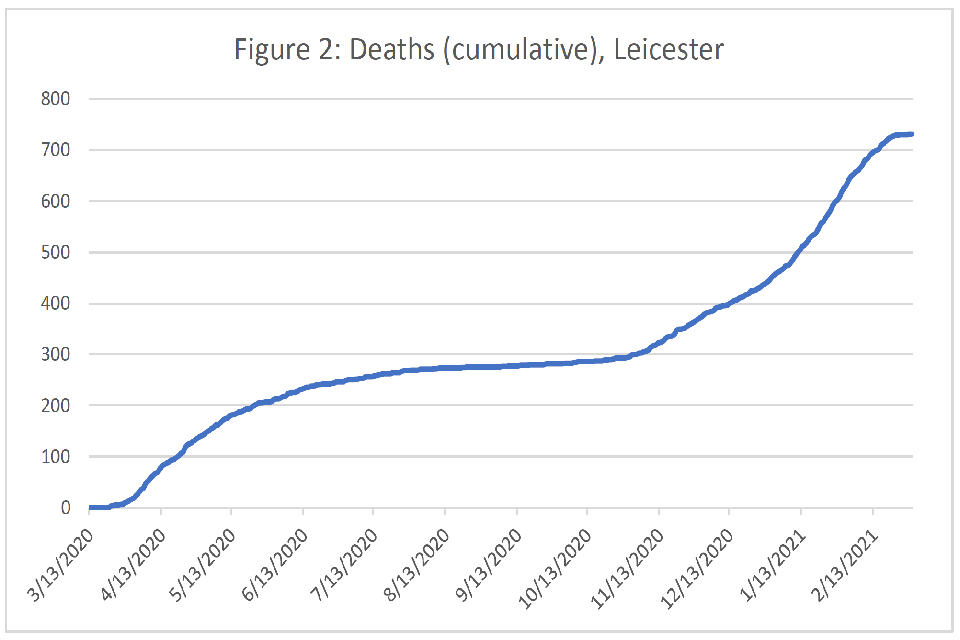
Line graph plotting cumulative deaths (y-axis, ranging from 0 to 800) from 13 March 2020 to 13 February 2021 (x-axis, labels given in monthly intervals). The axes have a single trendline, coloured blue.
Figure 2: Deaths (cumulative), Leicester. Source: derived from data downloaded from: UK Coronavirus Dashboard on 2 March 2021.
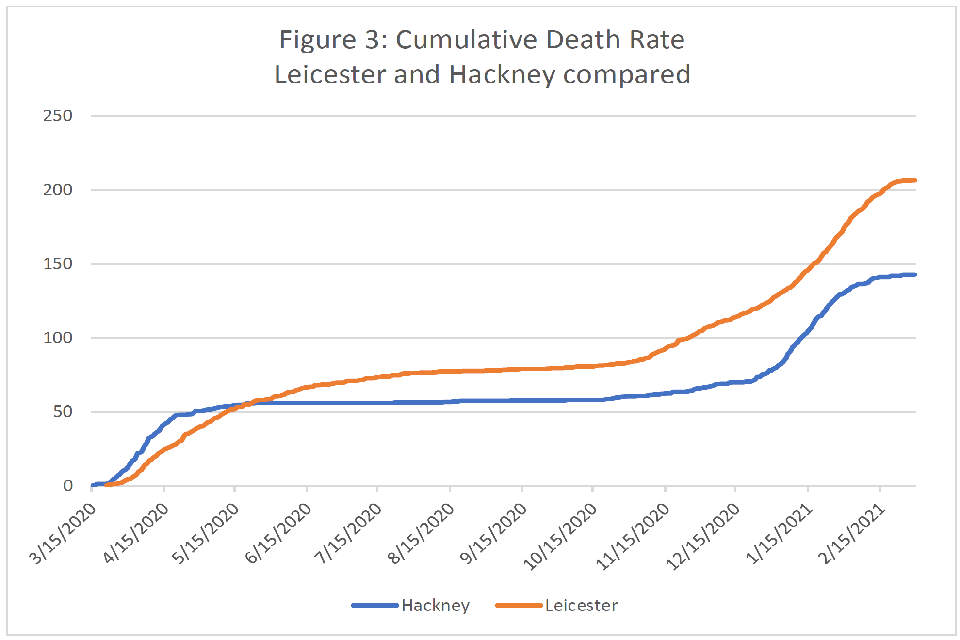
Line graph plotting cumulative death rate (y-axis) from 15 March 2020 to 15 February 2021 (x-axis). Graph compares data seen for Hackney (blue trendline) and Leicester (orange trendline).
Figure 3: Cumulative Death Rate Leicester and Hackney compared. Source: derived from data downloaded from: UK Coronavirus Dashboard on 2 March 2021.
Figure 4, rather than looking at the cumulative total, looks at the rolling death rate (namely the rolling 7-day average). This shows how the rate in the more recent period exceeded that for the earlier period. Again, a comparison with Hackney shows how the patterns across the 2 areas differ. The England rolling rate is also included for reference. The rate in Leicester is clearly to the right of that for Hackney with a lower initial peak but slower decline, including some upticks. Note that Leicester was put into lockdown on 26 June, by which time its rolling rate had been above that for England for a few weeks. Leicester experienced a higher second peak than Hackney and then a later third peak.
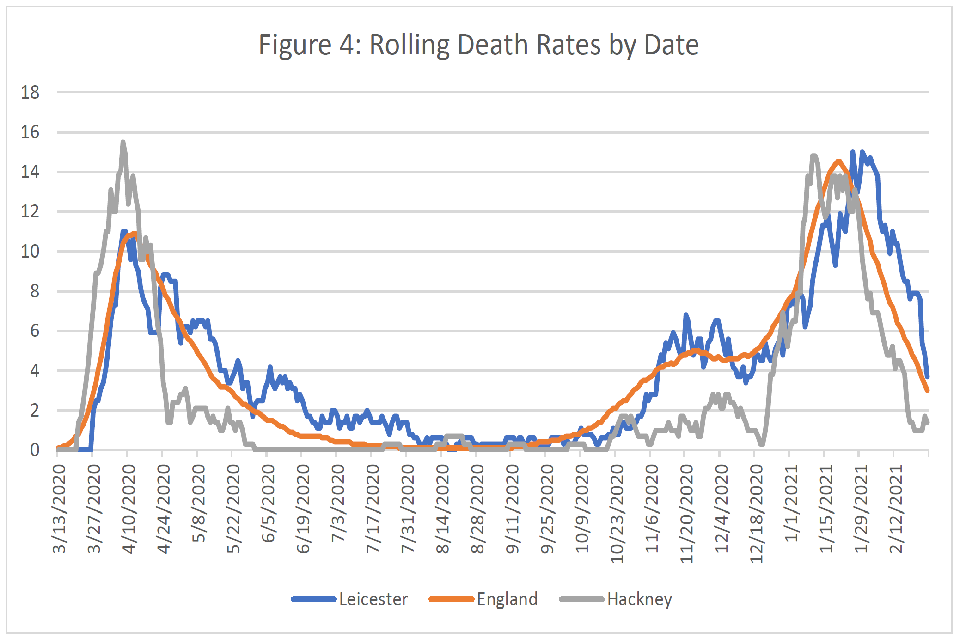
Line graph plotting rolling death rates (y-axis) from 13 March 2020 to 12 February 2021 (x-axis). Three trendlines are plotted on the axes: data from Leicester, England and Hackney are represented respectively as blue, orange and grey lines.
Figure 4: Rolling Death Rates by Date. Source: derived from data downloaded from: UK Coronavirus Dashboard on 2 March 2021.
Finally, Figure 5 digs a bit deeper to look at variation in case rates by ward within Leicester. For this information there is just the week ending 26 February.
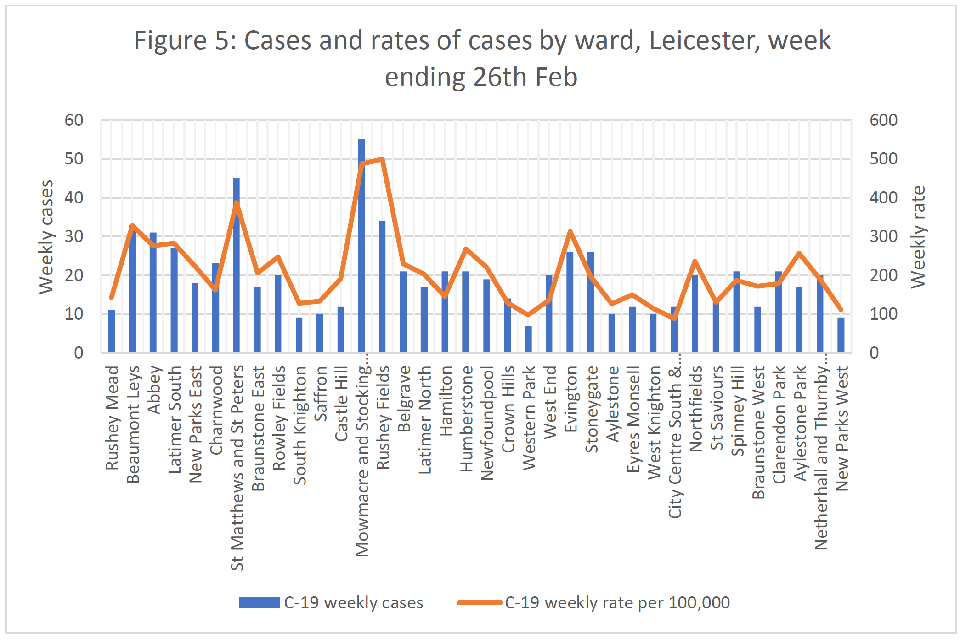
Dual axis chart. Data is plotted for 36 wards of England (x-axis). COVID-19 weekly cases are shown as a bar-chart in blue. COVID-19 weekly rate per 100,000 people shown as line graph, with an orange trendline superimposed on the bar chart.
Figure 5: Cases and rates of cases by ward, Leicester, week ending 26 February. Source: derived from data downloaded from: Open Leicester on 2 March 2021.
In addition we have plotted local public health case date per week per 1000 according wards in Leicester from 20 April to 21 January.
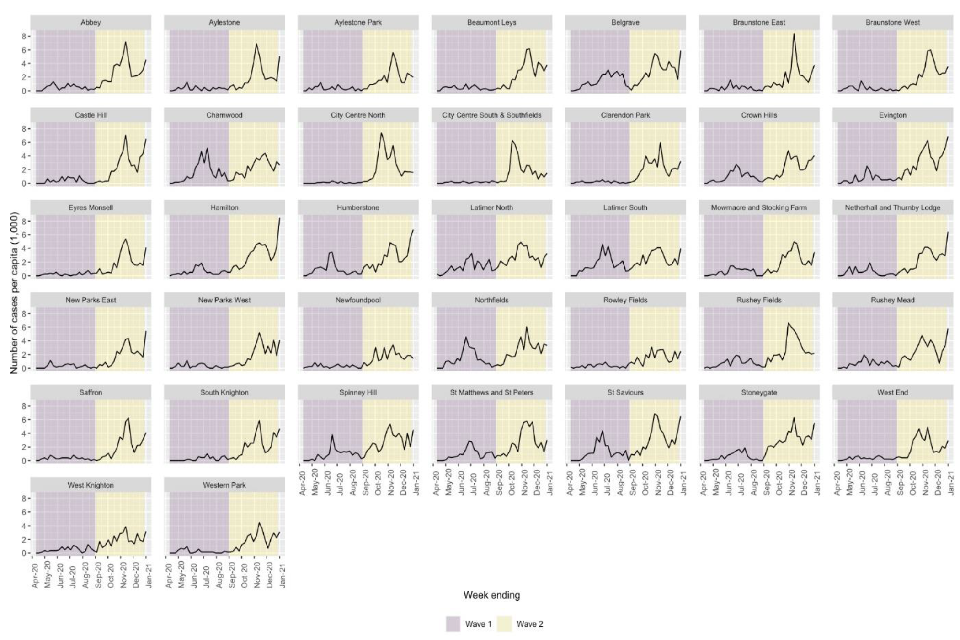
37 line graphs, each representing a ward in England. Y-axes show case numbers per capita; x-axes plot from April 2020 to January 2021. Left- and right-hand sides of each graph are respectively purple and yellow coloured, representing waves one and two.
These graphs indicate that mortality and case loads across Leicester have been chronic, and COVID-19 is endemic in some areas in spite of restrictions. In addition there has been a particularly high case load clustered in the area East and adjacent to the city centre that includes Spinney Hills, Evington, Mowmacre, Rushey Fields, Charnwood, St Matthews and St Peters, Northfields and Stoneygate. This is mainly South Asian, and densely populated. It is the area where many textile factories are (especially Evington and Spinney Hills) and where those who work there live. This has had chronically high transmission rates through the whole year with especially high transmission rates in the Summer and Autumn. It seems likely that these spikes represent the interactions of disadvantages of occupation and household circumstances. Or in other words high case loads due to people working in precarious work in which they cannot negotiate sick-leave and living in multigenerational households containing members with reduced health in densely packed neighbourhoods. It is clear too that the people engaged in these occupations would have still had to go to work during local interventions. The disproportionate ethnicity effect of this is visible in the following graphs.
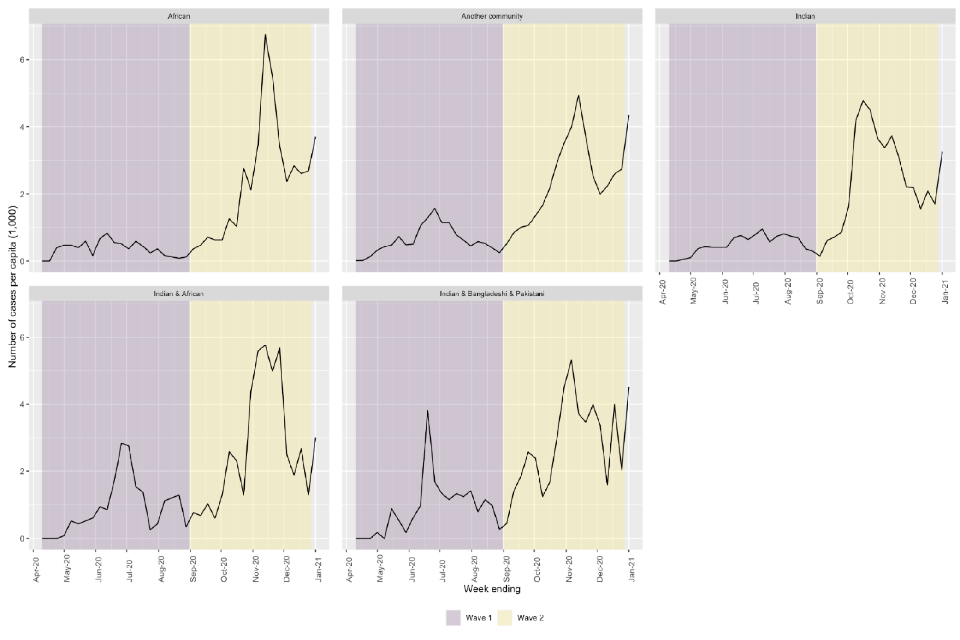
5 line graphs, each representing an ethnic group. Y-axes: case numbers per capita. X-axes plot from April 2020 to January 2021. From top right, clockwise: African; Another community; Indian; Indian and African; and Indian, Bangladeshi and Pakistani.
Stigma and amplifications of health disparity
It is clear that the dense housing and occupations among minority ethnic groups in Leicester have caused a chronic situation of exposure to and transmission of COVID-19, along with a heavy death toll. This situation is likely to have been amplified by long-standing experiences of stigma that have intensified during the trigger event of a local intervention in June 2020 and the prevention of celebrations during Eid. However, attention to these issues by the local authority, community organisations and trade unions has somewhat reduced these effects, which points a way forward for other national and local institutions. All the following data comes from LSE Anthropology’s ongoing study on COVID-19 and Care in the UK.
When the local interventions were first introduced it produced fears that Leicester’s residents were the ‘Lepers of Leicester.’ Initially within non-white ethnic groups, local garment workers and Muslim groups were blamed for spread, along with young people. White residents attributed transmission to all non-white ethnic groups living in dense neighbourhoods and multigenerational households. However local authority, Public Health England, community groups and trade union interventions have greatly helped showing the value of confronting the problem of stigma. The stigma against garment workers in ‘illegal’ factories has lessened in intensity as local groups (unions, employment rights services, local authority) have mobilised to provide new support services and regulation for these groups.
However divides still remain. These continue within ethnic groups between wealthier and less wealthy members and across ethnic divides. There is also a persistent stigma against young people, who are perceived to be non-compliant with regulations especially young men. In addition there remains a suspicion across all communities that business in factories has gone on as usual despite the wave 2 national social intervention.
People who live in densely populated neighbourhoods in the city centre (especially St Matthews, Highfields) are concerned about ongoing narratives of transmission related to housing conditions, intergenerational living arrangements and urban environments. Indeed, people who live in suburban or semi-rural areas actively avoid the city centre for this reason, and avoid forming relationship, visiting or allowing into their homes those who live there.
This has opened up new class divides within ethnic minority groups, where older links of care provision between family or friends who live in the city versus those who live beyond its limits have been truncated as a result of fear of transmission. This places a greater care burden on the less well of members of minority ethnic groups, which may lead to their greater exposure as well.
In addition long-standing barriers to access to care have continued, and perhaps increased. Formal care services are finding it difficult to reach out to communities who are not digitally connected, have poor English skills or literacy barriers. This contributes to the idea among policy makers that such communities are bounded and ‘hard to reach’. There is a reluctance on the part of some communities to access hospital service as they fear “people go in but they don’t come out”. There is a perception that unconscious bias is part of the healthcare workers decisions in care provision in situations of crisis, meaning people from Black communities are not prioritised for care. This perception is refuted by ethnic minority healthcare professionals themselves, who see care provision as equal especially in wave 2 where strong protocols and better resourcing has resulted in less of a crisis situation. There are fears of miscommunication and misrepresentation for people who don’t speak English or who are perceived to come from an immigrant background. There is a perception that such people will not be provided with adequate or even standard care, especially in the provision of pain medication and follow up.
Overall the qualitative evidence shows that the local intervention in Leicester initially led to a peak in stigmatisation, division and isolation between and among different ethnic groups. This was reduced by careful and informed outreach by the local authority, community, third sector and trade unions. However given the chronic COVID-19 transmission within Leicester uncertainty and divides have persisted. These are likely to contribute to health barriers and access to care unless they are further addressed through communications, investment in healthcare and outreach, along with concerted efforts to address the underlying disadvantages of occupation and household circumstance faced by minority groups in Leicester.
Conclusion
The quantitative and qualitative evidence presented here shows that multifaceted policy is necessary to overcome disproportionate transmission and mortality among minority groups. This is likely to require a combination of financial support for precarious groups, self-isolation payments, investment in healthcare and inspection of workplaces as well as a concerted effort to address the issues of stigma faced by minority groups in the context of COVID-19.
References
Abrams, Dominic and Lalot, Fanny and Broadwood, Jo and Platts-Dunn, Isobel (2020) Beyond Us and Them: Perception of Covid-19 and Social Cohesion. Project report. University of Kent. DOI: 10.22024/UniKent/01.02.84111.
Algren, M.H., Ekholm, O., Nielsen, L., Ersbøll, A.K., Bak, C.K. and Andersen, P.T. (2018). Associations between perceived stress, socioeconomic status, and health-risk behaviour in deprived neighbourhoods in Denmark: a cross-sectional study. BMC Publ Health. 18(1)
Bear, L., et al. (2020). A Right to Care [online]. Accessed [08 March 2021].
Bingham, D. et al. (2021). Covid-19 lockdown: Ethnic differences in children’s self-reported physical activity and the importance of leaving the home environment. A longitudinal and cross-sectional study from the Born in Bradford birth cohort study [online]. MedRXiv. Accessed [08 March 2021].
Bliuc, A.M., Betts, J., Vergani, M., Iqbal, M., & Dunn, K. (2019). Collective identity changes in far-right online communities: The role of offline intergroup conflict. New Media & Society, 21(8), 1770–1786.
Bodas, Moran, and Kobi Peleg. (2020). Income assurances are a crucial factor in determining public compliance with self-isolation regulations during the COVID-19 outbreak–cohort study in Israel. Israel Journal of Health Policy Research 9.1, 1-10.
Bowyer, G. and Henderson, M. (2020). Race Inequality in the Workforce: Exploring connections between work, ethnicity and mental health [online]. London: Carnegie UK Trust, UCL Centre for Longitudinal Studies and Operation Black Vote. Accessed [08 March 2021].
Bristol Somali Youth Voice & Bristol Somali Forum (2020). Impact of COVID-19 on Somali Community in Bristol.
Caribbean and African Health Network (2021). COVID-19 Vaccines and the Caribbean and African Community.
Center for Disease Control and Prevention (CDC) (2021). Workplace Vaccination Program.
Chouhan, K. and Nazroo, J. Y. (2020) Health inequalities. In Byrne et al (Eds.) Ethnicity, Race and Inequality in the UK. State of the Nation. Policy Press. p76.
Community Care (2021). Social care failed by lack of PPE during first wave of pandemic, say MPs.
Discover Society (2020). Precarity, precarious work and Covid-19: insights from Nottingham [online]. Accessed [08 March 2021].
Fazil, Q., et al. (2002). Disadvantage and discrimination compounded: the experience of Pakistani and Bangladeshi parents of disabled children in the UK. Disability & Society. 17.3: 237-253.
GOV.UK Press Release (2021). Community Champions to give COVID-19 vaccine advice and boost take up. Accessed [08 March 2021].
Gronholm P. et al (2021) . Reducing stigma and discrimination associated with COVID-19: early stage pandemic rapid review and practical recommendations. Epidemiology and psychiatric sciences. 28 January 2021:1-23.
Hanif, W. et al (2020). Cultural competence in Covid-19 vaccine rollout. BMJ 2020; 371: m4845. https://doi.org/10.1136/bmj.m4845
Hatzenbuehler, M. et al (2013). Stigma as a Fundamental Cause of Population Health Inequalities. American Journal of Public Health 103: 813-821, https://doi.org/10.2105/AJPH.2012.301069.
Hiironen, I. et al. (2020). Occupational exposures associated with being a COVID-19 case; evidence from three case-controls studies [online]. MedRXiv. Accessed [08 March 2021].
Holzemer, W. et al (2007). A conceptual model of HIV AIDS stigma from five African countries. Journal of Advanced Nursing, 58: 541-551. https://doi.org/10.1111/j.1365-2648.2007.04244.x
House of Commons Women and Equalities Committee (2020) Unequal Impact? Coronavirus and BAME People. Third Report of Session 2019–21 [online]. London: House of Commons. Accessed [08 March 2021].
Kamal, A. and Bear L. (2021). Ongoing research not yet published.
Kamal, A, Gibson E, Mahmood H, Knowles N. (2020). Report for the LRF BAME engagement cell: Recommendations for developing culturally competent health messages. July.
Karlsen, S. and Nazroo, J.Y. (2002). The relationship between racial discrimination, social class and health among ethnic minority groups. American Journal of Public Health 92, 4, 624-31.
Karlsen, S. and Nazroo, J.Y. (2004). Fear of racism and health. Journal of Epidemiology and Community Health 58, 1017-1018.
Laird, L. D., et al. (2007). Muslim patients and health disparities in the UK and the US. Archives of disease in childhood. 92.10: 922-926.
Leicester City Council (2011). Compendium of key statistics: Leicester.
Link, B. and J. Phelan (2001). Conceptualizing Stigma. Annual Review of Sociology 27:1, 363-385.
Matilla-Santander et al. (2021). COVID-19 and Precarious Employment: Consequences of the Evolving Crisis. International Journal of Health Services. https://doi.org/10.1177/0020731420986694.
Major, B., and O’Brien, L. T. (2005). The social psychology of stigma. Annual Review of Psychology. 56, 393-421.
Memon A, et al (2016). Perceived barriers to accessing mental health services among black and minority ethnic (BME) communities: a qualitative study in Southeast England. BMJ Open 6:e012337. doi: 10.1136/bmjopen-2016-012337
Metzl, J. M., and Roberts. D. E. (2014). Structural competency meets structural racism: race, politics, and the structure of medical knowledge. AMA Journal of Ethics. 16.9: 674-690.
MHCLG (2020). Overcrowded households: Ethnicity facts and figures.
Nafilyan, V. et al (2021). Ethnic differences in COVID-19 mortality during the first two waves of the Coronavirus Pandemic: a nationwide cohort study of 29 million adults in England. Pre-print.
Nafilyan, V., Islam, N., Mathur, R. (2021) Ethnic differences in COVID-19 mortality during the first two waves of the Coronavirus Pandemic: a nationwide cohort study of 29 million adults in England. medRxiv 2021.02.03.21251004; doi: https://doi.org/10.112021.02.03.21251004.
Nandi, A. and Platt, L. (2020) Ethnic differences in effects of COVID-19: household and local context. Understanding Society Briefing Note 2020-14 [online]. Accessed [08 March 2021].
Nazroo, J. Y., and Williams, D. R. (2006). The social determination of ethnic/racial inequalities in health. Social determinants of health. 2. 238-266.
Nazroo, J., (2015). Addressing inequalities in healthy life expectancy. Government Office for Science [online]. Accessed [08 March 2021].
ONS (2014). 2011 Census analysis: Ethnicity and the Labour Market, England and Wales [online]. Accessed [08 March 2021]. Available at: 2011 Census analysis - Office for National Statistics (ons.gov.uk).
ONS (2020). Updated estimates of coronavirus (COVID-19) related deaths by disability status, England: 24 January to 20 November 2020 [online]. Accessed [08 March 2021].
ONS (not dated) ONS Summary of analysis: Tables looking at Occupational Employment at UK regional, NUTS3 and Local Authority Level, JD15-JD17. Tables derived by ONS from the Annual Population Survey, in response to ad hoc request.
Parliamentary Office on Science and Technology (POST) (2020). Covid-19 and occupational risk
Platt, L. (forthcoming 2021) COVID-19 and ethnic inequalities in England. LSE Public Policy Review.
Platt, L. and Warwick, R. (2020). COVID-19 and Ethnic Inequalities in England and Wales. Fiscal Studies. 41(2): 259-289.
Prats-Uribe, A., Paredes, R. and Prieto-Alhambra, D. (2020) Ethnicity, comorbidity, socioeconomic status, and their associations with COVID-19 infection in England: a cohort analysis of UK Biobank data [online]. MedRXiv. Accessed [08 March 2021].
Public Health England, (2020). Disparities in the risk and outcomes of COVID-19 [online]. Accessed [08 March 2021].
Public Health Wales (2019) Principles of Community Engagement for Empowerment.
SAGE Ethnicity Subgroup. (2020a). Evidence summary of impacts of public health communication for minority ethnic groups. [online]. Accessed [08 March 2021].
SAGE Ethnicity Subgroup. (2020b). Housing, household transmission and ethnicity.
SAGE Ethnicity Subgroup. (2020c). Factors influencing COVID-19 vaccine uptake among minority ethnic groups.
Salway, S., Platt, L., Chowbey, P., Harriss, K., and Bayliss, E. (2007). Long-term ill health, poverty and ethnicity. Policy Press.
Samari, G., Alcalá, H. E., and Sharif, M. Z. (2018). Islamophobia, health, and public health: a systematic literature review. American journal of public health. 108.6: e1-e9.
Segerstrom, S.C., Miller, G.E. (2004) Psychological stress and the human immune system: a meta-analytic study of 30 Years of inquiry. Psychol Bull. 601–630.
Smith, L. E. et al. (2020). Adherence to the test, trace and isolate system: results from a time series of 21 nationally representative surveys in the UK (the COVID-19 Rapid Survey of Adherence to Interventions and Responses [CORSAIR] study). MedRxiv.
SPI-B (2020a). Public Health Messaging for Communities from Different Cultural Backgrounds.
SPI-B (2020b). Impact of financial and other targeted support on rates of self-isolation or quarantine.
SPI-B (2020c). SPI-B Evidence Review for MHCLG Housing Impacts Paper.
SPI-B (2020d). How important is symptom recognition in leading people to seek a test for COVID-19? Unpublished paper.
SPI-B and EMG (2020). COVID-19 housing impacts.
Stangl, A. et al. (2019). The Health Stigma and Discrimination Framework: a global, crosscutting framework to inform research, intervention development, and policy on health-related stigmas. BMC Med 17, 31. Available at: https://doi.org/10.1186/s12916-019-1271-3.
Trade Union Congress. (2019). BME workers far more likely to be trapped in insecure work [online]. Accessed [08 March 2021].
TUC (2020). Dying on the job - Racism and risk at work [online]. Accessed [08 March 2021].
TSIP (2020). An equitable recovery from Covid-19: Insights from Lambeth [online]. Accessed [08 March 2021].
Wallace, S., Nazroo, J.Y. and Bécares, L. (2016). Cumulative exposure to racial discrimination across time and domains: exploring racism’s long-term impact on the mental health of ethnic minority people in the UK. American Journal of Public Health 106, 7,1294-1300, doi: 10.2105/AJPH.2016.303121.
Watkinson, R. E., Sutton, M., and Turner, A. J. (2021). Ethnic inequalities in health-related quality of life among older adults in England: secondary analysis of a national cross-sectional survey. The Lancet Public Health. 6(3).
Zemedikun, D. et al. (2018). Patterns of multimorbidity in middle-aged and older adults: an analysis of the UK Biobank data. Mayo Clinic Proceedings. 93 (7), pp. 857-866