Breastfeeding and dental health
Updated 30 January 2019

© Crown copyright 2019
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/breastfeeding-and-dental-health/breastfeeding-and-dental-health
1. Summary
- dental teams should continue to support and encourage mothers to breastfeed
- not being breastfed is associated with an increased risk of infectious morbidity (for example gastroenteritis, respiratory infections, middle-ear infections)
- breastfeeding up to 12 months of age is associated with a decreased risk of tooth decay
- exclusive breastfeeding is recommended for around the first 6 months of life − complementary foods should be introduced from around 6 months of age alongside continued breastfeeding
- the prevalence of breastfeeding in UK is low, with 34% of mothers still breastfeeding their child at 6 months and only 1% exclusively breastfeeding
- further advice for dental teams can be found in Health Matters: Child Dental Health and Delivering Better Oral Health (2014)
Breastfeeding is the physiological norm against which other behaviours are compared; therefore dental teams should promote breastfeeding and include in their advice the risks of not breastfeeding to general and oral health.
Policy advice with regard to breastfeeding and dental health has not changed. Dentists and their teams should support evidence-based guidelines from the World Health Organization (WHO) and the UK government.
Since 2001 the WHO has recommended that mothers worldwide exclusively breastfeed infants for the first 6 months to achieve optimal growth, development and health. Thereafter, they should be given nutritious complementary foods as breastfeeding continues up to the age of 2 years or beyond. These guidelines were reiterated in the WHO’s Global Strategy (WHO, 2003)[footnote 1] and endorsed by the Scientific Advisory Committee on Nutrition (SACN) in 2003.
In 2018, the Scientific Advisory Committee on Nutrition (SACN) published its report on ‘Feeding in the first year of life’ [footnote 2] as a result policy advice with regard to breastfeeding has not changed. With regard to oral health it concluded that breastfeeding up to 12 months of age is associated with a decreased risk of dental caries.
Healthcare professionals including dentists and their teams should support evidence-based guidelines from the World Health Organization (WHO) and the UK government.
2. Breastfeeding and dental health
Despite this advice, breastfeeding rates in the UK remain low with the Infant Feeding Survey 2010[footnote 3] reporting that just over a third (34%) of mothers were still breastfeeding their child at 6 months with only 1% exclusively breastfeeding as recommended.
Current advice from PHE with regard to oral health and breastfeeding can be found in Delivering Better Oral Health[footnote 4] and Health Matters: Child dental health[footnote 5] and is summarised in the infographic below:
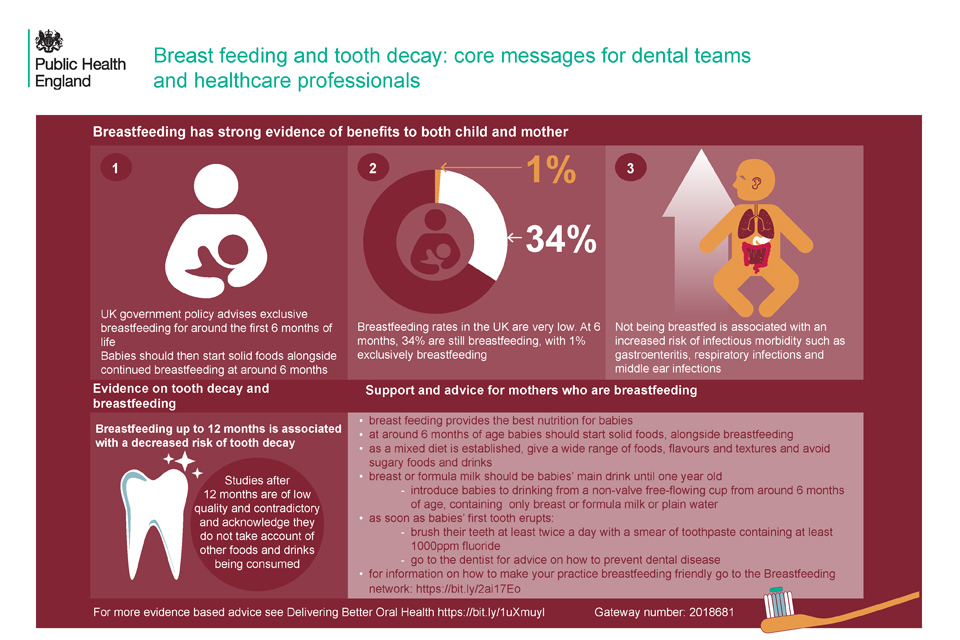
Breast feeding and tooth decay: core messages for dental teams and healthcare professionals
This image is available for download.
Health Matters: Child Dental Health (2017) states [footnote 5]:
“Health professionals, such as midwives and health visitors, should support and encourage women to breastfeed. Creating the right environment to promote this is crucial. The UNICEF Baby Friendly Initiative provides a robust evidence-based framework to develop a whole-systems approach to breastfeeding.
“The UK government recommends exclusive breastfeeding for around the first 6 months of life. Complementary foods should be introduced into the infant’s diet from around 6 months of age alongside continued breastfeeding (or infant formula if the mother chooses).
“Not being breastfed is associated with an increased risk of infectious morbidity (for example gastroenteritis, respiratory infections, middle-ear infections), and current evidence suggests that breastfeeding up to 12 months of age is associated with a decreased risk of tooth decay.”
Delivering Better Oral Health (PHE, 2014 updated content 2017)[footnote 4] recommends that:
- breast milk is the only food or drink babies need for around the first 6 months of their life, first formula milk is the only suitable alternative to breast milk
- bottle-fed babies should be introduced to drinking from a free-flow cup from the age of 6 months and bottle feeding should be discouraged from 12 months old
- only breast or formula milk or cooled, boiled water should be given in bottles
- only milk or water should be drunk between meals and adding sugar to foods or drinks should be avoided
Recent systematic reviews such as that by Tham and others (2015)[footnote 6] included studies where children were breastfed beyond 12 months. When infants are no longer exclusively breast or formula fed, confounding factors, such as the consumption of potentially cariogenic drinks and foods and tooth brushing practices (with fluoride toothpaste), need to be taken into account when investigating the impact of infant feeding practices on caries development. Tham and others (2015) noted that several of the studies did not consider these factors and concluded that with regard to associations between breastfeeding over 12 months and dental caries “further research with careful control of pertinent confounding factors is needed to elucidate this issue and better inform infant feeding guidelines”. Good quality evidence on breastfeeding and oral health is an area with significant methodological challenges which have been outlined by Peres and others (2018)[footnote 7].
In 2017 a birth cohort study in Brazil was published by Peres and co-authors[footnote 8]. This study is notable in that it has used marginal structural modelling in an attempt to estimate the controlled direct effect of breastfeeding on dental caries and address some of the methodological challenges. The study reported that in comparison with children breastfed up to 12 months, those breastfed from 13 to 23 months (that is over 1 year) there was no effect on dental caries, but those breastfed for over 2 years (24 months) had a higher number of decayed missing and filled surfaces. However, the authors recognise the study’s limitations in that:
- no information was collected on other potentially cariogenic sources and the frequency of nocturnal breastfeeding, which may have led to residual confounding
- the absence of information on dental caries experience before the age of 5 years did not permit a better understanding of the long-term effect of breastfeeding on dental caries experience in the earlier stages
- another limitation is related to the period when information regarding sugar consumption was collected (in the study it began at 24 months) as patterns of consumption are established in early childhood
This single study adds to the body of evidence that will be reviewed shortly by SACN when they commence work on a report for children aged 12 to 60 months.
3. References
-
World Health Organization and UNICEF. ‘Global strategy for infant and young child feeding’ World Health Organization, Geneva 2003 (viewed on 31 October 2018) ↩
-
Scientific Advisory Committee on Nutrition. ‘Feeding in the First Year of Life’ 2018 (cited 19 September 2018) ↩
-
NHS Digital. ‘Infant Feeding Survey - UK, 2010’ 2012 (viewed on 19 September 2018) ↩
-
Public Health England. ‘Delivering Better Oral Health: An Evidence-Based Toolkit for Prevention’ 2014 (viewed on 3 August 2018) ↩ ↩2
-
Public Health England. ‘Health Matters: Child Oral Health’ 2017 (viewed on 19 September 2018) ↩ ↩2
-
Tham R and others. ‘Breastfeeding and the risk of dental caries: a systematic review and meta‐analysis’ Acta Paediatrica 2015: volume 104(S467), pages 62 to 84 ↩
-
Peres K and others. ‘Breastfeeding and Oral Health: Evidence and Methodological Challenges’ Journal of Dental Research 2018: volume 97(3), pages 251 to 258 ↩
-
Peres K and others. ‘Impact of Prolonged Breastfeeding on Dental Caries: A Population-Based Birth Cohort Study’ Pediatrics 2017: volume 140(1), pages 2,016 to 2,943 ↩