
Discussion paper on the effects of excess Vitamin E on maternal health
Published 6 July 2026

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/14th-july-2026-committee-on-toxicity-meeting/discussion-paper-on-the-effects-of-excess-vitamin-e-on-maternal-health
This is a paper for discussion. This does not represent the views of the Committee and should not be cited.
Introduction
1. The Scientific Advisory Committee on Nutrition (SACN) last considered maternal diet and nutrition in relation to offspring health in its reports on ‘The influence of maternal, fetal and child nutrition on the development of chronic disease in later life’ (SACN, 2011) and on ‘Feeding in the first year of life’ (SACN, 2018). In the latter report, the impact of breastfeeding on maternal health was also considered.
2. In 2019, SACN agreed to conduct a risk assessment on nutrition and maternal health focusing on maternal outcomes during pregnancy, childbirth and up to 24 months after delivery; this would include the effects of chemical contaminants and excess nutrients in the diet. The assessment would also consider infant outcomes, but only where they relate to the neonatal period. The neonatal period was normally considered to be up to 28 days after birth, but the relevant time window for neonatal effects would be determined on a case-by-case basis.
3. SACN agreed that, where appropriate, other expert Committees would be consulted and asked to complete relevant risk assessments e.g. in the area of food safety advice. This subject was initially discussed during the horizon scanning item at the January 2020 meeting with a scoping paper being presented to the Committee in July 2020. This included background information on the provisional list of chemicals proposed by SACN. It was noted that the provisional list of chemicals was subject to change following discussion by COT who would be guiding the toxicological risk assessment process: candidate chemicals or chemical classes can be added or removed as the COT considered appropriate. The list was brought back to the COT with additional information in September 2020: [ARCHIVED CONTENT]. Following a discussion at the COT meeting in September 2020, it was agreed that papers on a number of components should be prioritised and to this end, papers on iodine, vitamin D and dietary supplements have been or will be presented to the Committee. The remaining list of compounds were to be triaged on the basis of toxicity and exposure. The current paper presents information intended to aid this process.
4. Following discussion of the first prioritisation paper [ARCHIVED CONTENT] on substances to be considered for risk assessment by the COT, the Committee decided that Vitamin E should be considered in a specific paper.
Current UK Government and International advice
5. UK Government advice as given on the national health service (NHS) NHS.uk website lists good sources of vitamin E as plant oils (such as rapeseed (vegetable oil), sunflower, soya, corn and olive oil), wheatgerm (found in cereals and cereal product), nuts and seeds (NHS, 2020).
6. UK Government dietary advice, as given on the NHS website, does not have specific recommendations concerning pregnant women consuming Vitamin E and states that ‘a healthy, varied diet’ should provide sufficient vitamin intake during pregnancy, unless stated otherwise.
7. The World Health Organisation (WHO) reports that the current evidence does not support the routine use of vitamin E supplementation during pregnancy. The WHO’s recommendations are considered in more detail in paragraph 18.
Background
Structure and sources
8. Vitamin E is the collective name for a group of eight structurally similar compounds consisting of four tocopherols and four tocotrienols (α (alpha), β (beta), γ (gamma), and δ (delta) forms) (Szewcyyk, et al. 2025). α-tocopherol is recognised as the only essential form of Vitamin E (EFSA, 2024).
9. Vitamin E activity is expressed as d-α-tocopherol equivalents. Where activity is given as International Units (IU), 1 IU of d-α-tocopherol (RRR-α-tocopherol) is equivalent to 0.67 mg. If the vitamin E is present in the form of dl-α-tocopherol (all-rac-α-tocopherol), then 0.91 mg is equivalent to 1 IU.
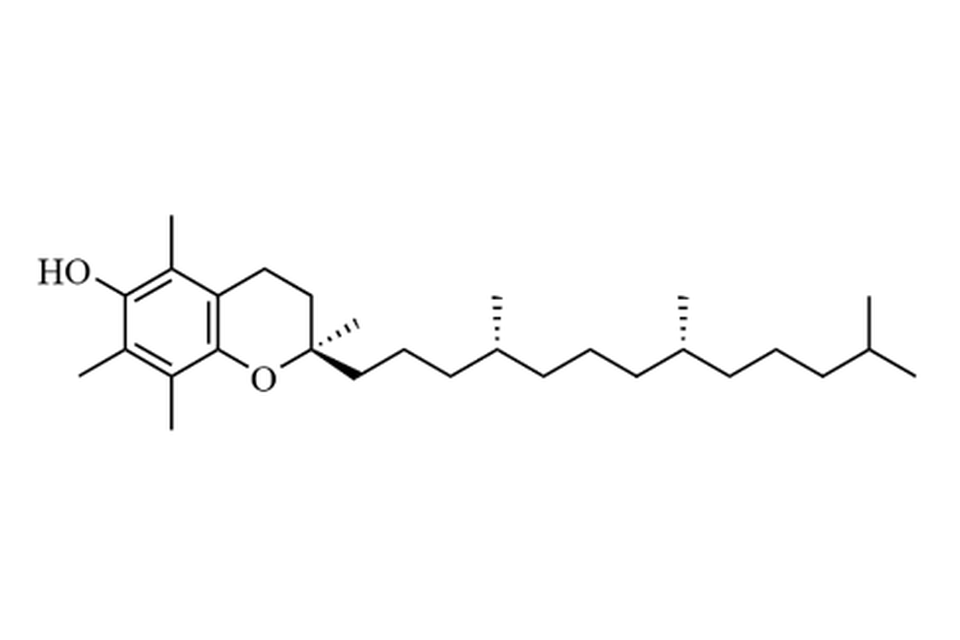
Figure 1: Chemical structure of natural α-tocopherol (i.e. RRR-α-tocopherol). RRR refers to R- conformation at the 2,4 and 8 positions.
10. Vitamin E in the diet is essential for health in general and vitamin E deficiency in pregnant women is known to compromise fetal development and increase the risk of miscarriage, pre-eclampsia, and premature delivery (Gagné, et al., 2009).
11. Vitamin E is synthesized by plants and is primarily found in dietary sources such as vegetable oils, seeds, kernels, and nuts (Szewcyyk, et al. 2025). Animal tissues generally have a low concentration of vitamin E, with accumulation occurring in fatty tissues depending on intake.
12. Plant oils are the main dietary sources of vitamin E (560-1600 mg/kg in soybean oil, 530-1620 mg/kg in corn oil and 50-150 mg/kg in olive oil), with meat (0.5-1.6 mg/kg), poultry (1.6-4.0 mg/kg) and dairy products (0.4-10.0 mg/kg) providing only moderate amounts. The Expert Committee on Vitamins and Minerals (EVM) (2003) states that vitamin E is present in a variety of dietary supplements at doses of up to 268 mg/day in multi-constituent products and 670 mg/day in single constituent products (EVM, 2003). Recent data from market analysis of vitamin E supplements (vitamin E only or multi-ingredient dietary supplements (MIDS)) showed a daily dose of 4-536 mg of vitamin E.
Population estimates
13. In developing countries around the world, there are issues with vitamin E deficiency in vulnerable populations through limited intake of food sources containing vitamin E and a higher prevalence of oxidative stressors such as malaria and HIV infection, which accelerate its depletion (Dror and Allen, 2011). Vitamin E deficiency in pregnant women can cause miscarriage, preterm birth, preeclampsia, and intrauterine growth restriction (Gagné, et al, 2009).
Previous evaluations
14.Previous evaluations of vitamin E have been carried out by the European food safety authority (EFSAa, 2015; EFSAb, 2015; EFSA, 2024), EVM (2003), the Scientific Committee on Food (SCF) (2003), and the WHO (Rumbold, et al. 2015).
15. The SCF (2003) set a Tolerable Upper Intake Level (TUL) for vitamin E of 280 mg/day for adults, rounded to 300 mg/day using an uncertainty factor of 2, based on the effect on blood clotting and the increased risk of bleeding from a study by Meydani et al. (1998). The same TUL was applied to pregnant and lactating women.
16. The EVM established a Safe Upper Level (SUL) of 540 mg (800 IU) for supplemental Vitamin E, equivalent to 9 mg/kg bw/day in a 60 kg adult (EVM, 2003). This was based on 3 key studies (Gillilan et al. (1977); Meydani et al. (1996); Stephens et al. (1996)) which are discussed in more detail in paragraph 113. In the studies by Gillilan et al. (1977) and Meydani et al. (1996), the biochemical and physiological effects of vitamin E were investigated and the findings indicated that supplemental doses of 800 to 1600 IU/day were without apparent adverse effect. The results were derived from small groups that may not be representative, therefore the EVM considered that an additional uncertainty factor could be applied to account for inter-individual variation. However, the results of the larger CHAOS trial (Stephens et al., 1996) supported the view that 800 IU/day supplemental vitamin E would not result in any adverse effects and, taking the three studies together, the EVM concluded that no further uncertainty factors were necessary (EVM, 2003).
17. In 2015, EFSA adopted the TULs for vitamin E from all dietary sources retained for all population groups in line with the SCF of 300 mg/day for adults, including pregnant and lactating women. In 2024, EFSA reviewed the TUL of α-tocopherol previously established by the SCF, and found no basis to change the TUL, therefore retaining the TUL of 300 mg α-tocopherol/day for adults. This TUL also applies to pregnant and lactating women as no new evidence was found regarding specific adverse effects or different susceptibility in these groups (EFSA, 2024).
18. The WHO’s systematic review of vitamin E supplementation in pregnancy found that the evidence ‘does not support the routine use of vitamin E supplementation in pregnancy for the prevention of fetal or neonatal death, preterm birth, preeclampsia, or intrauterine growth restriction for women with or without a high risk of adverse pregnancy outcomes. While vitamin E supplementation reduced the risk of placental abruption, an increased risk of term [premature rupture of membranes] PROM and the side effect of abdominal pain was also found among women receiving vitamin E’ (WHO, date not given; Rumbold, et al. 2015).
Functions
19. Vitamin E is often considered the main lipophilic antioxidant of the body due to its important role in counteracting oxidative stress. Free (non-esterified) vitamin E functions as an antioxidant and deactivates reactive oxygen species (ROS). Vitamin E’s antioxidant activity is mostly directed at cellular membrane lipids, where it protects against ROS‑mediated lipid peroxidation by preventing and terminating reactions that produce peroxide, which act as secondary ROS (Rutkowski and Grzegorczyk, 2012).
20. Secondary functions such as gene transcription and expression have also been suggested for alpha-tocopherol (EVM, 2003).
Mechanisms of action
Antioxidant effects
21. The mechanism of action for most of vitamin E’s effects are currently still unknown (Brigelius-Flohe, 2009). α-tocopherol is an antioxidant that binds free radicals, protecting cellular components from oxidative damage (EVM, 2003, Okebukola, Kansra and Barrett, 2017).
22. A mechanism of vitamin E’s antioxidant effect is in the termination of lipid peroxidation. The vitamin reacts with unstable lipid radicals, which produces stable lipids and a relatively stable vitamin E radical. This radical is then reduced back to stable vitamin E by reacting with ascorbate or glutathione (EVM, 2003, Herrera and Barbas, 2001).
Mechanisms of toxicity
23. The most established mechanism of toxicity of vitamin E is its interference with vitamin K metabolism and function, leading to impaired blood coagulation particularly in susceptible individuals (EVM, 2003; Meydani, et al. 1998; Megavitamin E Supplementation and Vitamin K-Dependent Carboxylation. 1983; Corrigan and Marcus, 1974; and Yue, and Jansson. 2001).
24. The mechanism of this interference is uncertain, but it has been suggested that competitive inhibition between tocopheryl quinone and vitamin K, which are both structurally similar, for the enzyme vitamin K-dependent carboxylase. This enzyme is essential for converting specific residues in certain proteins into functional clotting factors (Booth, 2004). Another proposed mechanism is competitive redox reaction between tocopherol quinone and the reduced form of vitamin K, vitamin K hydroquinone, which would result in a depletion of the cofactor for the vitamin K-dependent carboxylase (Tovar, 2006).
ADME
25. α-tocopherol is absorbed from the small intestine by non-saturable passive diffusion. Tocotrienol esters are hydrolysed first by pancreatic esterase, and then absorption occurs mostly in the upper and middle of the small intestine. The absorption efficiency of tocopherol and its esters are generally considered variable (EFSA, 2024). EVM (2003) stated that human studies reported that absorption of alpha-tocopherol and its acetate ester is in the region of 21-86% over 24 hours. EFSA (2024) considered that the average α-tocopherol absorption from a usual diet would be about 75% (EFSAa, 2015).
26. Vitamin E has not been found to have a specific carrier protein in plasma (EVM, 2003). There are currently no data to suggest that any tissue serves as a storage site for α-tocopherol for its release on demand. Thus, tissues acquire α- tocopherol by non-specific lipid- or lipoprotein-dependent mechanisms that also deliver peroxidisable fats, but it is not known how the tissues release or secrete α-tocopherol (EFSA, 2024). α-tocopherol is absorbed by the liver and released in low density lipoprotein. Most absorbed tocopherols are transported unchanged to the tissues. Kinetic studies have indicated that the human body has two collections of Vitamin E. One is ‘labile’ that turns over rapidly and one is ‘fixed’ that turns over slowly. The labile collection predominates in tissues such as plasma and liver because tocopherol is depleted rapidly in those tissues under conditions of vitamin E deprivation (EVM, 2003). In contrast, the fixed collection appears to predominately reside in the bulk lipid phase as adipose vitamin E (EFSA, 2024; EVM, 2003).
- The presence of α-tocopherol transfer protein (α-TTP) in the placenta has been shown (Kaempf-Rotzoll et al., 2003; Muller-Schmehl et al., 2004). Based on immunohistochemical localisation of α-TTP and estimated staining intensity, it was found that α-TTP expression in the placenta doubled from the first trimester (six to eight weeks) to term (Rotzoll et al., 2008).
28. EFSA (2024) noted that, in humans, although some α-tocopherol catabolism takes place in the intestine or the kidney, more than 90% of α-tocopherol catabolism takes place in the liver, where α-tocopherol is catabolised to long-chain carboxy-catabolites and, ultimately, α-carboxyethyl hydroxychroman (α-CEHC) (EFSA, 2024; Traber et al., 2019). α-CEHC is then excreted in the urine, bile and faeces (EFSA, 2024; EVM, 2003). EVM (2003) stated that 30–70% of vitamin E is excreted in the faeces via the bile, whereas less than 1% is excreted in the urine (EVM, 2003).
Acute toxicity
29. Vitamin E is largely considered safe compared to other fat-soluble vitamins (Tappel, 1972) and vitamin E toxicity is almost exclusively associated with high-dose supplementation. Overall, EFSAb (2015), EVM (2003) and SCF (2003) all consistently consider the acute oral toxicity of α-tocopherol to be very low, commonly citing an acute toxicity study conducted by Krasavage and Terhaar (1977). In this study, mature CD rats (10 animals/sex/group) were fasted for 16 hours before being given either d-α-tocopheryl poly(ethylene glycol) 1000 succinate, polyethylene glycol 1000 or d-α-tocopheryl acid succinate at 7000 mg/kg bw. All animals were observed for clinical signs of toxicity for 14 days, after which, gross necropsies were conducted. Six of the 60 animals died within 48 hours of treatment; all deaths were attributed to dosing errors. After an initial transient 24-hour period of listlessness and diarrhoea, no further adverse effects were observed. The LD50 values for all three test substances were greater than 7000 mg/kg bw.
30. Acute clinical effects of vitamin E toxicity in humans are gastrointestinal upset, including nausea and diarrhoea, fatigue, muscle weakness, and anticoagulant effects caused by detrimental effects on vitamin K activity (Kappus and Diplock. 1992).
Short term and subchronic toxicity
31. The effects of tocopherols (primarily α-tocopherol) following repeated exposures in short-term and subchronic studies have been previously reviewed (EFSAb 2015; EVM, 2003; SCF, 2003). The key studies (Krasavage and Terhaar, 1977; Abdo et al., 1986) cited in these reviews are summarised in the following paragraphs.
32. Krasavage and Terhaar (1977) conducted a 90-day dietary study, where CD weanling rats fed diets containing 0, 0.002, 0.2 or 2 % d-α-tocopheryl poly(ethylene glycol) 1000 succinate (calculated by the study authors to be 0, 0.5, 50 or 500 mg/kg bw/day vitamin E, respectively). The rats were observed for clinical signs of toxicity, and body weights were recorded prior to treatment, and haematology and clinical chemistry parameters were measured on days 42 and 84 (15 rats/sex from the control and highest dose group). These rats were then killed on day 91 and histopathological examinations were conducted. There were no adverse findings in this study. Blood clotting parameters, such as prothrombin time, were not measured; however, there were no reports of excessive bleeding or haemorrhages (Krasavage and Terhaar, 1977). The EFSA ANS (2015) panel concluded that the NOAEL for this study is ≥ 500 mg/kg bw/day d-α-tocopheryl poly(ethylene glycol) 1000 succinate.
33. Abdo et al. (1986) carried out a 13-week oral gavage study, conducted in accordance with a protocol that is comparable with OECD TG 408 (OECD, 1998a). Weanling Fischer 344 rats (10 animals/sex/group) were dosed with 0, 125, 500 or 2 000 mg/kg bw/day d-α-tocopherol acetate in corn oil. The untreated controls were dosed with corn oil only. Body weights and food consumption were recorded on a weekly basis and rats were observed for clinical signs of toxicity throughout the study. Blood samples for haematology and blood chemistry determination were taken from 10 rats from each group on days 5, 45 and 90 of treatment. A complete necropsy was performed on all rats after scheduled sacrifice on day 90. Deaths occurred in male rats that had received the highest dose only (7 out of 10 male rats in this group died); these deaths were attributed to internal haemorrhage. Signs of toxicity observed in the male rats that had received the highest dose were diarrhoea, tachypnoea, nose bleeds, dark faeces and red crusts around the eyes. There were no adverse effects on body weight or food consumption. Statistically significant increase of the liver-to body-weight ratios of females in the 500 and 2000 mg/kg bw/day groups (p < 0.05) was observed. There was a significant dose-related trend (p < 0.02) for increased thromboplastin time, activated partial thromboplastin time, fibrinogen, and reticulocyte, white blood cell, lymphocyte and segmented neutrophil counts (statistically significant at 90 days, p < 0.05) in males. There was also a decrease in haematocrit, red blood cell count and haemoglobin concentrations after 90 days (statistically significant at 90 days, p < 0.05) in males. Activated partial thromboplastin time was also increased in the 500 mg/kg bw/day group at 90 days (p < 0.05). In females, statistically significantly increased reticulocyte counts, decreased red blood cell counts and haemoglobin concentrations (p-values not given) were observed but there was no dose-dependent trend. There was, however, a dose-dependent increase in activated partial thromboplastin time in females at 90 days. There were statistically significant increases in serum chloride and γ-glutamyl transpeptide concentrations in males of the highest dose group, but the change was not dose-dependent (p-value not stated). Thyroid stimulating hormone was statistically significantly increased in all treated male and female rats at 90 days (p < 0.05). Haemorrhagic diathesis (haemorrhage or haemorrhagic inflammation in the nose, oesophagus, salivary gland, trachea, mediastinum, epididymis or meninges of the brain) occurred in 7 out of 10 males and in 2 out of 10 females in the 2000 mg/kg bw/day group. Increased extramedullary erythropoiesis of the spleen was observed in highest dose males (4/10 rats). Adenomatous hyperplasia and chronic interstitial inflammation of the lung were observed in all vitamin E-treated rats; the incidence and severity increased in a dose-dependent manner (Abdo et al., 1986). In the SCF opinion (SCF, 2003), the NOAEL derived for this study was 125 mg/kg bw/day, based on the serum chemistry and the effects on the liver that indicated hepatotoxicity.
34. Gianello et al., 2007 carried out a 90-day dietary study conducted in accordance with OECD TG 408 (OECD, 1998a) and GLP. The test substance was mixed tocopheryl phosphates, which is a mixture of d-α-tocopheryl phosphate and d-α-di-tocopheryl phosphate (together constituting 72 % of the mixture) and d-α-tocopherol (13 % of the mixture), plus water and phosphonic acid. Sprague–Dawley rats (10 animals/sex/group) were fed diets containing 0, 1, 3 or 5 % (calculated by study authors to be approximately 0, 600, 1900 and 3 200 mg/kg bw/day, respectively) mixed tocopheryl phosphates for 90 days. Blood clotting parameters, such as prothrombin times, were not determined in this study. Histopathological examinations revealed changes in the mesenteric lymph nodes and small intestines of treated male and female rats. There was a dose-related appearance of macrophages containing crystal-like foreign material in both tissues. The authors noted that “In the lymph nodes, sinus histiocytosis increased with dose, but the severity was similar between the control and low dose groups. Foreign-body granulomatous inflammation, associated with Maltese-cross birefringence of the crystals was seen in the mid- and high-dose rats, but not in the low-dose rats. Similarly, the small intestine showed increasing amounts of foreign material and inflammation in the mid- and high-dose”. Therefore, the authors of this study concluded that the NOAEL was a 1 % concentration (approximately 600 mg/kg bw/day) of mixed tocopheryl phosphates (Gianello et al., 2007). However, they noted that the crystals in the lymph nodes and small intestine were likely to be tocopheryl phosphate, probably in the polymerised state. Therefore, the EFSA ANS panel (2015) concluded that these findings were not relevant to the tocopherols covered by their re-evaluation. Because of the availability of other good quality studies on the tocopherols, and the fact that studies on the mixed tocopheryl phosphates give toxicological findings that are not relevant to this re-evaluation, additional studies on mixed tocopheryl phosphates were not included herein (EFSAb, 2015).
Additionally, in the 1994 Alpha-Tocopherol, Beta-Carotene (ATBC) study, vitamin E supplementation was associated with an increased risk of mortality from haemorrhagic stroke. The 1996 Cambridge Heart Antioxidant Study (CHAOS) obverse a small excess of cardiovascular deaths in the vitamin E supplemented group (EVM, 2003).
Interactions – Vitamin K
36. Studies in animals have shown that high dietary α-tocopherol can lead to impaired coagulation (Frank et al., 1997). Specifically, fatal haemorrhaging was associated with excess dietary vitamin E (Takahashi et al., 1990) and was prevented with vitamin K supplementation (Frank et al., 1997).
37. EFSA (2024) discussed how it is well established that high doses of α-tocopherol increase the risk of bleeding, as observed in animal studies (Abdo et al., 1986; EFSAb, 2015; Frank et al., 1997; Helson, 1984; March et al., 1973; Takahashi et al., 1990; Wheldon et al., 1983; Woolley, 1945). An increased risk of haemorrhage and prolonged prothrombin times and activated partial thromboplastin times have been observed upon oral administration of high doses of α-tocopherol to chicks, rodents and mini-pigs (EFSAb, 2015; IOM, 2001). In vitro, ex vivo and in vivo data suggest that the mechanisms by which α-tocopherol could impair blood clotting could be similar in animals and humans.
38. Different mechanisms were proposed by which high α-tocopherol intakes could increase the risk of bleeding in humans. First, α-tocopherol appeared to impair vitamin K absorption, hepatic metabolism and status. In animals, fatal haemorrhages associated with excess dietary α-tocopherol were prevented with vitamin K supplementation (Frank et al., 1997; Helson, 1984; Wheldon et al., 1983). In healthy humans, high-dose α-tocopherol supplements (1000 mg/day RRR- α-tocopherol) for 12 weeks increased concentrations of the inactive under-γ-carboxylated forms of prothrombin to levels indicative of poor vitamin K status (Booth et al., 2004). Second, α-tocopherol was found to inhibit platelet aggregation in vitro (Kakishita et al., 1990; Srivastava, 1986) and reduced platelet adhesion was observed in individuals taking α-tocopherol supplements (Jandak et al., 1989; Steiner, 1983). The exact mechanism for the effect was unknown but was thought to be mediated by the inhibition of protein kinase C, a major regulator of platelet granule secretion, integrin activation and platelet aggregation (Freedman et al., 1996; Steiner, 1999). Finally, α-tocopherol at high doses could potentiate the effect of antiplatelet and anticoagulant medications through different mechanisms (Podszun & Frank, 2014). In this context, the SCF considered the effect of α-tocopherol on blood clotting as the critical endpoint to derive a TUL for vitamin E (SCF, 2003).
39. EVM (2003) stated that ‘Vitamin E may exacerbate the effects of vitamin K deficiency, thus affecting blood coagulation. This has been reported in animal studies and in case reports of humans taking large doses the basis for the interaction is unclear. Vitamin E may also interfere with vitamin A absorption.’
EFSA ANS 2015 discussion of vitamin E and pregnant or lactating women
40. In EFSA 2015, the Panel on Food Additives and Nutrient Sources added to Food (ANS) re-evaluated the safety of tocopherol-rich extract (E 306), α-tocopherol (E 307), γ-tocopherol (E 308) and δ-tocopherol (E 309) as food additives (EFSAb, 2015). There was no concern that tocopherols were genotoxic or carcinogenic. Data were considered insufficient to address the reproductive and developmental toxicity. The Panel considered prolonged coagulation time as the critical adverse effect.
Reproductive toxicity
41. Boskovic et al. (2004) investigated prospectively the safety of high doses of vitamin E supplementation during the first trimester of pregnancy in 82 pregnant women exposed to 400-1200 IU/day vitamin E. Pregnancy outcomes were compared with a control group of women (n = 130) who were counselled on non-teratogenic exposure. The women were then followed up until 2–6 months after their expected dates of delivery. For one out of the 82 women in the vitamin E group, versus none of the 130 women in the control group, a major malformation was reported (details not stated). The mean birth weight of the vitamin E group was statistically significantly lower than the control group (3173 ± 467 g versus 3417 ± 565 g; p < 0.0015). There were no statistically significant differences in live birth rates, premature births, miscarriages or stillbirths (Boskovic et al., 2004; no further details).
42. Scholl et al. (2006) used a cohort of 1 231 pregnant women (from a population susceptible to poor diet) to examine the relationship between maternal plasma concentrations of α- and γ-tocopherols and fetal growth. Samples of blood were taken from the women at 16 and 28 weeks of pregnancy and concentrations of the tocopherols were determined after adjustment for total cholesterol. In this study, the concentrations of both tocopherols increased significantly (p < 0.0001) between 16 and 28 weeks of pregnancy: α-tocopherol by 20.5 % (11.37 compared with 13.70 µg/mL) and γ-tocopherol by 9.9 % (1.92 compared with 2.11 µg/mL). After adjustment for confounding variables, such as age and smoking status, α-tocopherol showed a positive linear relationship with birth weight, but there was no such relationship with γ-tocopherol. The relationship with fetal growth was also observed in a study conducted by Masters et al., (2007), which showed that maternal vitamin E is essential for normal growth and development of the human fetus. In this study, babies born to mothers with low plasma concentrations of α-tocopherol (<500 µg/dL) weighed less and had a smaller head circumference.
43. Intra-cytoplasmic sperm injection (ICSI), an in vitro fertilisation procedure, involves injection of a single sperm into an egg in order to fertilise it. Poor implantation and pregnancy rates have been reported when the sperm have elevated DNA fragmentation (Greco et al., 2005). Therefore, Greco et al. (2005) conducted a study in order to investigate the potential benefit of antioxidant treatment prior to collection of spermatozoa. Following one failed attempt at ICSI, 38 men with elevated (at least 15 %) DNA-fragmented spermatozoa were treated with antioxidants (1 g each of vitamin C and E) for two months. Treatment led to a decrease in DNA-fragmented spermatozoa in 76 % of men. In a second attempt at ICSI, fertilisation was not affected by treatment, but the pregnancy rates increased from 6.9 % to 48.2 %, and implantation increased from 2.2 % to 19.6 % in the treated group, compared with the pre-treated rates. It is not clear from these results which of the vitamins, or if both, had the beneficial effect. The Panel noted that this study may point to a protective role for vitamin E in male fertility.
44. EFSA ANS (2015) stated that although the study conducted by Boskovic et al. (2004) indicated that vitamin E supplements lead to reduced birth weights in humans, this result was not representative of the data as a whole. Overall, EFSA ANS (2015) considered that the data from human studies do not suggest that the tocopherols have an adverse effect on reproduction and development, and instead are essential for normal fetal growth and male fertility.
EFSA NDA 2015 discussion of vitamin E and pregnant or lactating women
45. In EFSA 2015, the Panel on Dietetic Products, Nutrition, and Allergies (NDA) were requested to derive Dietary Reference Values for vitamin E (EFSAa, 2015). The Panel’s discussion on the effects of vitamin E on pregnant and lactating women is included below.
Pregnancy
46. Four prospective cohort studies investigated the association between maternal ‘vitamin E’ intake from foods and supplements during pregnancy and the risk of wheeze, asthma, eczema and/or hay fever (Martindale et al., 2005; Devereux et al., 2006; Litonjua et al., 2006; Allan et al., 2015) in children at various ages over the first 10 years with, overall, inconsistent results.
47. In a randomised controlled trial (Pressman et al., 2003), pregnant women received from week 35 of gestation onwards a daily prenatal vitamin C- and ‘vitamin E’-containing supplement (containing 120 mg vitamin C and 30 IU ‘vitamin E’, which would be equivalent to 20.1 mg/day of α-tocopherol), either with or without additional 500 mg vitamin C and ‘vitamin E’ (400 IU, which would be equivalent to 268 mg/day of α-tocopherol). Mean maternal plasma α-tocopherol concentrations were 31.3 µmol/L and 50.4 µmol/L at delivery in each group (without and with supplementation, respectively), while cord plasma α-tocopherol at delivery was only 6.97 µmol/L in both groups (differences between groups not statistically significant). In addition, maternal plasma and chorioamnion α-tocopherol concentrations were correlated (r = 0.87, p < 0.001).
48. An observational study followed 19 pregnant women with α-tocopherol intakes (mean (range)) of 8.1 (1.4–22.7) mg/day from foods and consuming ‘vitamin E’ supplements (mean of 30 IU/day, range of 11–100 IU/day, which would be equivalent to about 20 (7.4–67) mg/day of α-tocopherol) (Didenco et al., 2011). Mean (± SD) maternal α-tocopherol concentration measured during the course of pregnancy (exact period not specified) was significantly higher than mean α-tocopherol cord blood concentration (33.4 ± 7.7 µmol/L vs. 6.7 ± 2.5 µmol/L, p < 0.001). The author stated that this suggests that insufficient placenta transfer is a factor that limits α-tocopherol transfer to the fetus (Didenco et al., 2011). There was no significant correlation between maternal and cord blood α-tocopherol concentrations, but a significant correlation was observed between maternal and cord blood α-CEHC concentrations (r = 0.70, log transformed α-CEHC, p < 0.002). Mean concentration of umbilical cord blood α-CEHC (30.2 ± 28.9 nmol/L) was not significantly different from maternal α-CEHC concentration. The author of the study speculated that, based on these results, a higher intake of vitamin E during pregnancy results in elevated metabolite concentrations in the fetal blood, without increasing the fetal blood vitamin E. However, the source of the metabolite was not determined, and could have been maternal liver, fetal liver or placenta. Therefore, if vitamin E supplements are taken during pregnancy to increase fetal stores, in reality there might be an increase in metabolites, rather than increasing circulating tocopherol (Didenco et al., 2011).
49. In 26 mothers at delivery, mean (± SE) maternal plasma α-tocopherol concentration was significantly higher than mean cord plasma α-tocopherol concentration, expressed as µmol/L (26.1 ± 1.1 vs. 5.5 ± 0.4 µmol/L, p = 0.0001) or µmol/mol total lipids (2.6 ± 0.1 vs. 1.9 ± 0.1 µmol/mol, p = 0.0001). Maternal plasma and cord plasma α-tocopherol concentrations were significantly correlated after adjustment for total lipids (r = 0.54, p = 0.007), but not when expressed as µmol/L (r = 0.09, p = 0.64) (Jain et al., 1996).
50. In another study on 66 mothers and 40 samples of umbilical cord blood of full-term newborns, mean (± SD) α-tocopherol concentration in maternal blood measured between 10 and 20 weeks of gestation was significantly higher than cord blood α-tocopherol at delivery (20.6 ± 4.0 µmol/L vs. 7.2 ± 1.9 µmol/L, p < 0.02) (Kiely et al., 1999). There was no correlation between maternal and cord blood α-tocopherol concentrations as well as lipid-adjusted α-tocopherol concentrations (Kiely et al., 1999).
51. Fifteen pregnant women were supplemented with 30 mg/day of all-rac-α-tocopheryl acetate during pregnancy, and with different doses (15, 30, 75, 150 or 300 mg/day, n = 3 per dose) of D3-RRR-α-tocopheryl acetate and D6-all-rac-α-tocopheryl acetate (1:1 by weight, n = 3 per dose) within five to nine days before delivery (Acuff et al., 1998). Maternal plasma total (i.e. deuterated or not) α-tocopherol concentrations of the five groups at delivery (mean ± SEM) were between 39.35 ± 2.86 µmol/L and 59.03 ± 0.73 µmol/L, while corresponding mean total α-tocopherol concentrations in cord blood were between 6.71 ± 0.49 µmol/L and 9.52 ± 0.90 µmol/L. Maternal plasma and cord plasma at delivery had significantly higher concentrations of D3-RRR-α-tocopherol than D6-all-rac-α-tocopherol (p < 0.05), whatever the dose received. Maternal D3-RRR-α-tocopherol concentrations were significantly higher with the two highest doses (150 and 300 mg/day) than with the three lowest, and cord plasma D3-RRR-α-tocopherol concentrations were significantly higher with the two highest doses than with the lowest (15 mg/day) (p < 0.05).
52. Placental transfer was investigated by analysis of α-tocopherol concentration according to gestational age, in 52 fetal blood samples (umbilical cord) and maternal blood (Abbasi et al., 1990). Mean α-tocopherol concentration was 9.2 ± 3.3 µmol/L in samples from 13 fetuses with a gestational age up to 22 weeks, 9.2 ± 4.9 µmol/L in 12 fetuses at 23–27 weeks of gestation and 8.6 ± 4.2 µmol/L in 27 fetuses with a gestational age of 28–38 weeks. Maternal plasma α-tocopherol concentrations were measured in six mothers at ≤ 22 weeks and also at 23–27 weeks of gestation, and in 20 mothers at ≥ 28 weeks of gestation. Maternal plasma α-tocopherol concentrations correlated significantly with those in the fetus (r = 0.551, p < 0.002). There were no significant differences in plasma α-tocopherol concentrations in samples from early, mid or late gestation in either the mother or the fetus. This study suggests that placental transfer of α-tocopherol is relatively constant throughout gestation.
53. Overall, the Panel noted that, despite the presence of α-TTP in the placenta and the existence of a correlation between maternal plasma and chorioamnion α-tocopherol concentrations, the α-tocopherol concentration of cord blood is much lower than that of maternal blood. In addition, maternal ‘vitamin E’ supplementation increases maternal but not cord plasma α-tocopherol concentrations. The Panel also noted that placental transfer of α-tocopherol is relatively constant throughout gestation.
EFSA 2024 core studies discussing Vitamin E and pregnancy and lactation
54. Rumbold et al. (2015) published a systematic review of randomised control trails to evaluate the safety of ‘vitamin E’ supplementation during pregnancy. A total of 21 trials were eligible for that review, of which only three trials administered supplemented ‘vitamin E’ alone versus placebo (Anthony et al., 1996; Sawhney et al., 2003; Shahraki, 2006). Two of those were available as conference abstracts and did not report the dose and form of ‘vitamin E’ used (Anthony et al., 1996; Sawhney et al., 2003). Shahraki (2006) aimed to assess the effect of 100 mg/day ‘vitamin E’ supplementation (form not specified) for 45 days on leg cramps. The study found that Vitamin E supplementation reduced mean cramp duration and overall did not report adverse effects of α-tocopherol under the conditions of the intervention.
- EFSA (2024) identified two additional RCTs on α-tocopherol supplementation that were not included in the review by Rumbold et al. (2015). Bastani et al. (2011) randomised pregnant women to receive 296 mg/day α-tocopherol (400 IU/day RRR- α-tocopheryl acetate) or a placebo from week 14 of gestation to the end of pregnancy (n = 104 in the intervention group) and assessed the risk of preeclampsia, birth weight and Apgar score. Wangkheimayum et al. (2011) reported the effects of 2-weeks of supplementation of 400 IU/day as α-tocopheryl acetate (source not specified) versus a placebo in women with pre-eclampsia (n = 24 in treatment group) on plasma concentrations of soluble P-selectin. These studies did not indicate adverse effects of α-tocopherol under the conditions of the interventions.
56. The Panel notes that available RCTs do not indicate adverse effects of α-tocopherol under the conditions of the interventions. However, data are scarce and provide limited relevant information for the safety assessment.
57. The Panel considered that the available evidence on the relationship between α-tocopherol intake and pregnancy-related outcomes could not be used for establishing a TUL for vitamin E (α-tocopherol).
Updated literature search for the reproductive effects of vitamin E
58. The following literature review covers studies published between 1st January 2024 to 14th May 2026. This time period was chosen to cover literature published after the latest EFSA Opinion in 2024. Parameters used for the literature review can be found in Annex A.
Animal studies
Damodarn, Yahaya and Mordi (2025)
59. Damodarn, Yahaya and Mordi (2025) carried out a study combining in silico modelling with an in vivo zebrafish embryo assay to evaluate the developmental toxicity of a tocotrienol-rich fraction (TRF), a form of vitamin E derived from palm oil.
60. The study included a negative control (system water), a solvent control (0.1% DMSO), and a positive control (3,4‑dichloroaniline) and TRF treated groups. Embryos were exposed to a range of TRF concentrations (62.5, 125, 250, 500, 1,000, 2,000 μg/mL) for up to 96 hours post-fertilisation. The test substance was a TRF containing approximately 75% tocotrienols and 25% α‑tocopherol, supplied as a liquid formulation. The mixture was diluted in 0.1% DMSO for administration and the zebrafish embryos were exposed via immersion in solution. Adverse effects were assessed following OECD Test Guideline 236 for fish embryo toxicity using a combination of lethal and sub-lethal endpoints (including mortality, developmental endpoints, morphological malformations, pigmentation changes and growth parameters). These endpoints were evaluated at 24, 48, 72, and 96 hours.
61. At lower concentrations (≤250 μg/mL), no significant morphological abnormalities were observed in the Zebrafish embryos. However, at higher concentrations (≥500 μg/mL), embryos exhibited developmental toxicity, including pericardial edema, yolk sac edema, and spinal deformities. At concentrations ≥1,000 μg/mL, additional adverse effects were observed, including reduced heart rate, delayed hatching, hypopigmentation, and increased mortality, with complete mortality at a concentration of 2,000 μg/mL. The calculated teratogenicity index (TI ≥2) suggests that TRF has teratogenic potential, even at doses that do not immediately cause death.
62. In silico toxicity predictions were also incorporated, which suggested generally favourable pharmacokinetic properties but identified potential human ether a-go-go-related gene (hERG) channel inhibition, a known mechanism associated with cardiotoxicity. This was consistent with the observed reduction in embryonic heart rate at high doses.
63. The authors concluded that TRF from palm oil was likely safe at concentrations below 500 μg/mL during zebrafish embryonic development.
Rabiee et al 2026
64. Rabiee et al. (2026) investigated the effects of different levels of vitamin E supplementation on ovarian physiology, redox balance, and reproductive outcomes.
65. 150 female mice (4 weeks old) were randomly allocated to six groups (n = 25 per group): a control group, two sham groups (water and olive oil), and three vitamin E treatment groups receiving a dose (1,000 mg/kg), an overdose (2,000 mg/kg), or a severe overdose (4,000 mg/kg). The mice received the supplementation treatment via gavage for 30 days. Following treatment, 15 animals per group were used for biochemical and histological analyses, and 10 were mated to assess fertility outcomes.
66. In both the overdose and severe overdose of vitamin E significant reductions in pregnancy rates (approximately 50% and 40%, respectively), litter size, and oocyte development capacity compared to the other groups, was noted. Oocyte development was also impaired in both these groups. The number of germinal vesicle oocytes recovered per animal, blastocyst formation rates, and total blastocyst cell numbers were all significantly reduced in the overdose treatment groups, indicating compromised oocyte quality and embryonic development.
67. In both overdose groups, impaired folliculogenesis, with reduced numbers of antral follicles and corpora lutea, and increased numbers of atretic follicles was observed. The severe overdose group also resulted in a reduction in primary follicles and significant thinning of the endometrium.
68. In contrast, the optimal dose of vitamin E did not adversely affect reproductive outcomes compared with controls and was associated with a modest increase in endometrial thickness, suggesting a potential benefit at physiological levels.
69. The overdose and severe overdose groups exhibited significantly increased GSH/GSSG ratios, indicating reductive stress, alongside increased ROS levels in granulosa cells, particularly in the severe overdose group.
70. Additionally, vitamin E overdose was associated with a reduction in the Bax/Bcl2 ratio, which indicated suppressed apoptosis in ovarian tissue.
- Serum vitamin E concentrations only increased significantly in the severe overdose group, suggesting that systemic levels may not reflect tissue-level accumulation or effects, and that reproductive tissues may be particularly sensitive to local changes in vitamin E exposure.
72. The authors concluded that excessive vitamin E intake induces reductive stress, disrupts ovarian physiology, and significantly compromises fertility in mice.
Gomez et al. 2025
73. Gómez et al. (2025) investigated how maternal vitamin E and/or hydroxytyrosol (HXT) supplementation during late gestation and lactation affects ovarian development in offspring. Fifty pregnant sows (Iberian pigs) were fed a controlled diet in the pre-experiment period (until day 85 of pregnancy). At day 85 of pregnancy, sows were allocated into four supplement groups: group 1 (30 mg of α-tocopheryl acetate/kg feed (control group)), group 2 (100 mg of α-tocopheryl acetate/kg feed), group 3 (30 mg of α-tocopheryl acetate/kg feed and 1.5 HXT/kg feed), group 4 (100 mg of α-tocopheryl acetate/kg feed and 1.5 HXT/kg feed).
74. At 110 ± 5 days old, 45 female offspring of similar birth weight were weighed, and blood samples and ovarian tissues taken. Oxidative stress markers, ovarian morphology, hormonal levels and gene expression (e.g. IGF1, RUNX1, FSHR, HSD17B7) were all measured.
75. This study found that high doses of Vitamin E supplementation increased markers of oxidative stress in offspring, including higher malondialdehyde and lower superoxide dismutase activity. The authors noted that this was unexpected as vitamin E was typically considered an antioxidant, suggesting that higher doses may disrupt redox balance or reflect altered physiological states. High doses of Vitamin E supplementation also resulted in increased ovarian surface area, lower follicle density, and a greater proportion of medium and large follicles. The authors noted that these findings indicated accelerated follicular development, which suggested that these offspring may have been closer to puberty. This was supported by the finding of increased expression of gene HSD17B7, which is involved in estrogen synthesis and suggested increased late-stage steroidogenic pathway activity.
76. No significant differences were found in offspring overall body weight or hormone levels, indicating that structural and molecular changes occurred without major systemic hormonal shifts at this stage.
77. The authors concluded that maternal antioxidant supplementation, particularly high‑dose vitamin E, can influence offspring ovarian development, and while higher vitamin E intake may promote ovarian maturation, it may also increase oxidative stress.
Human studies
Pippen et al. (2025)
78. Pippen et al. (2025) carried out a secondary analysis of a large, randomized, double-blind, placebo-controlled trial of prenatal vitamin C and E supplementation to prevent preeclampsia in low-risk nulliparous participants.
79. A total of 198 maternal–neonatal pairs were included in the analysis (98 in the vitamin group and 100 in the placebo group). Participants were randomised to receive either a fixed daily oral dose of antioxidant supplementation (1,000 mg vitamin C and 400 IU vitamin E (RRR‑α‑tocopherol)) or placebo (mineral oil capsules). Dosage continued from enrolment (9–16 weeks gestation) until delivery, resulting in an exposure duration of approximately 27–28 weeks.
80. Plasma of participants (pregnant women, 24.4 ± 4.3 years old) at time of randomization (9–16 weeks gestation) and delivery, and neonatal cord blood were analysed for adiponectin concentration. Pippen et al. (2025) found that for participants with high baseline adiponectin concentration, vitamin C and E supplementation was associated with higher adiponectin concentration at delivery. Conversely, vitamin supplementation was associated with lower cord adiponectin concentration among participants with low baseline adiponectin concentration.
81. Only participants with >80% compliance (based on adherence records rather than biomarkers) were included in the analysis. Participants were generally healthy as individuals with pre-existing hypertension, proteinuria, diabetes, in vitro fertilisation pregnancies, or known fetal anomalies were excluded. As such, the findings are most applicable to healthy pregnant populations and may not extend to higher-risk groups.
82. The chemical form of vitamin E (RRR‑α‑tocopherol) was specified, however, no further information was provided regarding product purity, composition, or potential contaminants. Additionally, participants were permitted to take standard prenatal vitamins, which may have contained variable amounts of vitamin E and other micronutrients. This introduces potential confounding and variability in baseline exposure that was not fully controlled.
83. This study focused on biochemical endpoints, specifically maternal and neonatal adiponectin concentrations measured in blood samples collected at baseline (early pregnancy), at delivery, and from umbilical cord blood. There was no structured collection of other data, such as clinical adverse events, maternal complications, or neonatal morbidity.
84. The authors considered that the reduction in neonatal adiponectin could be interpreted as a potentially adverse metabolic effect, although the clinical significance of this biomarker change was not established. It should be noted that no differences were observed in key clinical neonatal outcomes, including birth weight or gestational age at delivery.
85. Co-administration of vitamin C alongside vitamin E makes it difficult to attribute observed effects specifically to vitamin E. Pippen et al. (2025) argues that vitamin C likely does not influence adiponectin, but this cannot be fully verified within the study design.
86. The authors concluded that for participants with high baseline adiponectin concentration, vitamin C and E supplementation was associated with higher adiponectin concentration at delivery. Conversely, vitamin supplementation was associated with lower cord blood adiponectin concentration among participants with low baseline adiponectin concentration.
Atazadegan et al. (2024)
87. Atazadegan et al. (2024) carried out a cross-sectional observational study on 138 primiparous pregnant women between 6–10 weeks of gestation to evaluate the association between nutritional status and insulin sensitivity in early pregnancy.
88. This study additionally investigated maternal weight, pregravid BMI, total physical activity, job activity, and household income compared with insulin sensitivity, however as they are outside the scope of this paper, they have not been further discussed.
89. A researcher-made questionnaire was used to record participant characteristics. Nutrient intake was estimated based on the 72-hour dietary recall by Nutritionist 4 software. Insulin sensitivity was evaluated using the quantitative insulin sensitivity check index (QUICKI), calculated from fasting glucose and insulin concentrations measurements. Only dietary vitamin E exposure was recorded with no information given on supplement intake.
90. Participants were healthy, with no indication of pre-existing disease, and the study aimed to characterise metabolic variation in a low-risk early-pregnancy population. This study did not monitor clinical outcomes, side effects, or maternal or fetal complications, and focused solely on a metabolic biomarker (insulin sensitivity).
91. Higher dietary vitamin E intake was associated with lower insulin sensitivity, as measured by QUICKI. For every one unit increase in vitamin E, insulin sensitivity decreased by 0.003 unit. In contrast, carbohydrate and vitamin C intake was associated with increased insulin sensitivity. The authors suggested that higher vitamin E intake, at least within the range observed in diet, may be associated with reduced insulin sensitivity in early pregnancy.
92. While the authors concluded that nutritional factors influence insulin sensitivity and highlight weight management as a preventive strategy for gestational diabetes, the specific finding that vitamin E intake was associated with reduced insulin sensitivity was not emphasised as a potential adverse effect. Additionally, because of the cross-sectional nature of the data, it was not clear whether vitamin E intake led to reduced insulin sensitivity or whether individuals with lower insulin sensitivity have different dietary patterns.
Li et al. 2026
93. Li, et al. (2026) carried out a retrospective cross-sectional analysis to examine the associations between maternal fat-soluble vitamin status (vitamins D, A, and E), meteorological factors, and delivery and neonatal outcomes in a large cohort of pregnant women in central China.
94. Participants were healthy, as women with pre-existing chronic diseases affecting vitamin metabolism, fetal anomalies, or preterm delivery were excluded. They noted that the cohort therefore represented a relatively low-risk population, although no placebo or control group was included.
95. This study included 10,824 third-trimester women (31.2 ± 3.6 years old) who delivered at ≥37 weeks gestation between 2020 and 2023. Vitamin concentrations were measured once in late pregnancy (37–40 weeks gestation) using high-performance liquid chromatography. Vitamin D, A, and E were classified into deficiency, insufficiency, sufficient, and (for vitamin E only) excess categories. However, no information was provided on dietary intake or supplement use.
96. Meteorological exposure was assessed by assigning daily temperature, humidity, precipitation, and wind speed values to each participant based on the date of blood collection. Clinical outcomes were extracted from electronic medical records and included delivery outcomes (fetal distress, meconium-stained amniotic fluid, and premature rupture of membranes) and neonatal outcomes (low birth weight and macrosomia).
97. Vitamin D deficiency was observed in 30.2% of women, vitamin A deficiency in 5.5%, and vitamin E excess in 41.8%, with no cases of deficiency reported for vitamin E.
98. Temperature was identified as the strongest meteorological determinant of vitamin status. Each 1°C increase in ambient temperature was associated with decreased odds of vitamin D deficiency (adjusted odds ratio (aOR) 0.970) and vitamin A deficiency (aOR 0.976). Significant interaction effects between temperature and other meteorological variables (e.g. humidity and wind speed) were also reported, suggesting that environmental factors act in combination rather than independently.
99. Restricted cubic spline analyses demonstrated that higher concentrations of vitamin E were associated with 60% increased likelihood of macrosomia (aOR 3.14).
Yang et al. 2025
100. Yang et al. (2025) carried out a prospective cohort study within the Jiangsu Birth Cohort to investigate the association between maternal vitamin E intake during early pregnancy and the risk of developing gestational hypertension (GH) and preeclampsia (PE) in women undergoing assisted reproductive technology (ART).
101. This study included 3,587 women who conceived via ART and had pregnancies progressing to ≥20 weeks gestation. Participants were recruited in the first trimester and monitored throughout pregnancy. Women with chronic hypertension were excluded, and diagnoses of GH and PE were obtained from medical records using established clinical criteria. The cohort was therefore specific to women undergoing ART, who may represent a higher-risk group for hypertensive disorders compared to the general pregnant population.
102. Exposure to vitamin E was assessed using a semi-quantitative food frequency questionnaire during the first trimester. Dietary vitamin E intake was estimated from reported food consumption, while vitamin E supplementation was self-reported and recorded separately, including dose, duration, and cumulative intake.
103. Blood samples were also taken from 1,103 participants during the first trimester for metabolomic analysis. Vitamin E-related metabolites, particularly α-tocopherol and its downstream metabolites, were measured to provide a biomarker of exposure.
104. Dietary vitamin E intake (mean 37.4 mg/day) alone was not associated with GH/PE risk, even at higher intake levels. However, vitamin E supplementation exceeding 100 mg/day in early pregnancy was significantly associated with increased risk of GH/PE (odds ratio 1.68), particularly when vitamin E supplement intake was >2 months or >12,000 mg.
105. Among women with low dietary vitamin E intake, increased risk was observed only at higher supplementation doses (>100 mg/day). However, among women with high dietary vitamin E intake, both low-dose (≤100 mg/day) and high-dose (>100 mg/day) supplementation were associated with increased risk of GH/PE.
106. Metabolomic analyses found that higher concentrations of α-tocopherol metabolites, particularly α-carboxyethyl hydroxychroman sulfate, were associated with increased risk of GH/PE (aOR 2.09 for high vs low levels). Elevated α-isomer metabolites were associated with a 55% increase in risk of GH/PE (aOR 1.55).
107. The authors concluded that due to increased risk of GH/PE, the overuse of Vitamin E supplementation during pregnancy should be cautioned.
Yang et al. 2024
-
Yang et al. (2024) investigated the association between vitamin E with fetal growth and lipids. This study recruited 146 mother–infant pairs from a hospital in China, comprising of 62 infants classified as small for their gestational age (SGA) and 84 as appropriate for gestational age (AGA). Only term, singleton pregnancies without major maternal complications were included.
-
Cord blood vitamin E was measured using high‑performance liquid chromatography–mass spectrometry. Lipid parameters in cord blood, including triglycerides (TG), total cholesterol (TC), low‑density lipoprotein (LDL), and high‑density lipoprotein (HDL), were also measured. Dietary vitamin E intake and supplementation were not recorded.
110. The study mainly focused on impact of fetal growth status, specifically whether the infant was SGA (birth weight <10th percentile for gestational age) versus AGA.
111. Higher cord blood vitamin E levels were associated with an increased risk of SGA, with an adjusted odds ratio of 2.24 (95% CI 1.21–4.74). Vitamin E levels were inversely related to birth weight, indicating that higher cord vitamin E was linked with poorer fetal growth. Vitamin E was also positively correlated with multiple lipid measures (LDL, HDL, TC, and TG) in cord blood, suggesting that vitamin E may influence fetal lipid metabolism, which in turn could affect fetal growth and development. The authors also noted that vitamin E has known roles in regulating glucose and lipid metabolism, and disturbances in these pathways could contribute to altered fetal growth patterns.
112. The authors noted that these findings contradict findings of previous studies (no citation provided) that showed higher maternal vitamin E linked to increased fetal growth, suggesting that maternal versus fetal (cord blood) vitamin E may have different relationships with growth outcomes.
113. The authors concluded that higher cord blood vitamin E concentrations are associated with increased risk of small‑for‑gestational‑age birth and are positively linked to lipid levels, suggesting a potential role for vitamin E in fetal lipid metabolism.
Mou et al. 2026
14. Mou et al. (2026) carried out an observational birth cohort study to investigate how fat‑soluble vitamins influence transplacental transfer of per‑ and polyfluoroalkyl substances (PFAS) and how these interactions relate to neonatal outcomes.
115. The study measured 23 PFAS concentrations in paired maternal and cord serum, as well as fat‑soluble vitamins (A, D, E, and K₁) in cord serum from 227 mother–infant pairs recruited at a single hospital in Guangzhou, China. Participants were pregnant women ≥18 years with singleton pregnancies and no major complications such as gestational diabetes or occupational pollutant exposure. Maternal blood samples were collected during late pregnancy, and cord blood was collected at delivery. Maternal diet and supplementation data were not collected.
116. The study also derived transplacental transfer efficiency (TTE), defined as the ratio of PFAS concentration in cord blood relative to maternal blood, to quantify fetal exposure.
117. Neonatal anthropometric outcomes (including birth weight, birth length, and head circumference) were measured and standardised as z‑scores using international growth standards.
118. The study found vitamin E was negatively associated with the transplacental transfer efficiencies of perfluoroheptanoic acid and perfluorododecanoic acid, suggesting reduced placental transfer with higher vitamin E levels.
119. PFAS were largely detectable in both maternal and cord serum, with moderate maternal–fetal correlation (Spearman r ≈ 0.67), indicating substantial but incomplete placental transfer.
120. Mou et al. (2026) proposed that vitamin E may influence PFAS transfer through its role as an antioxidant and stabiliser of cell membranes, potentially enhancing placental barrier integrity and reducing PFAS permeability. Additionally, both PFAS and fat‑soluble vitamins bind to plasma proteins and lipoproteins, raising the possibility of competition or interaction in transport pathways that could alter PFAS distribution and transfer.
121. The study found that vitamin E effected the relationship between perfluorononanoic acid and birth weight and length, with higher vitamin E associated with more negative associations (i.e. potentially stronger adverse effects).
122. The authors concluded that fat‑soluble vitamins, especially vitamin E and K₁, are associated with the placental transfer of PFAS and may modify how these environmental exposures relate to neonatal growth.
Health-based guidance values (tolerable upper intake levels (TULs)/safe upper limits (SULs))
123. EVM (2003) considered key studies (Gillilan et al. (1977); Meydani et al. (1998); Stephens et al. (1996)) to determine a NOAEL of 800-1600 IU/day (540 – 970 mg d-α-tocopherol equivalents/day) with an uncertainty factor of 1. The Gillilan et al. (1977) and Meydani et al. (1998) studies were derived from small groups that may not be representative, thus an additional uncertainty factor could be applied to account for inter individual variation. However, the results of the larger CHAOS trial (Stephens et al., 1996) support the view that 800 IU/day supplemental vitamin E would not result in any adverse effects and, taking the three studies together, no further uncertainty factors are necessary. EVM (2003) discussed a study in male smokers has suggested that 55 IU/day vitamin E (equivalent to 37 mg d-α-tocopherol equivalents/day) may increase the risk of mortality from haemorrhagic stroke in hypertensive subjects who smoked. Although biologically plausible, the significance of this finding is uncertain. It has not been repeated in other studies in subjects at high risk of cardiovascular events treated with higher doses of vitamin E (up to 600 mg/day); however, if it is an effect related to smoking there may have been too few smokers in these studies for any effect to be apparent. In addition, a large observational study of male health professionals did not report this association. The EVM concluded that “a Safe Upper Level of 800 IU/day (540 mg d–tocopherol equivalents/day) supplemental vitamin E is recommended. This is equivalent to 9.0 mg/kg bw/day for a 60 kg adult. Assuming an intake of 18 mg/day from food, a total intake of 560 mg d–tocopherol equivalents/day would not be expected to result in any adverse effect. This is equivalent to 12.4 mg/kg bw/day.”
124. In order to set a Tolerable Upper Intake Level (TUL), SCF (2003) considered the impact on blood clotting as the critical adverse effect. This was based on a study by Meydani et al. (1998) in which 88 healthy subjects over 65 received either a placebo or doses of 40, 134 or 537 mg α-TE/day for four months. It was stated that no side effects were reported. Supplementation had no adverse effects on plasma concentration of other anti-oxidant vitamins and minerals, glutathione peroxidase, superoxide dismutase or total cysteine. There was no significant effect of vitamin E on serum non-specific immunoglobulin concentrations or anti-DNA and anti-thyroglobulin antibodies. The cytotoxic ability of neutrophils against Candida albicans was not compromised. Vitamin E had no effect on body weight, plasma total proteins, albumin, glucose, plasma lipids or the lipoprotein profile, total bilirubin, serum liver enzymes, blood count, platelet number, bleeding time, haemoglobin, haematocrit, urinary or serum creatine levels. The study concluded that supplementation had no detrimental effect on health (Meydani et al. 1998; EVM, 2003).
125. Based on the Meydani et al. (1998) study, SCF (2003) identified a No Observed Adverse Effect Level (NOAEL) of 540 mg α-TE/day (800 IU/day). SCF (2003) concluded that ‘an uncertainty factor (UF) of 2 would adequately cover interindividual differences in sensitivity. A larger UF was not considered necessary because data from a number of other older but less well controlled studies showed no adverse effects at considerably higher intakes.’ SCF (2003) established a TUL of 280 mg/day for adults, rounded to 300 mg/day using an uncertainty factor of 2. The same TUL was applied to pregnant and lactating women. TULs for children and adolescents were extrapolated from the TUL for adults based on body surface area 0.75 (allometric scaling). No TUL was established for infants (< 1- year old).
126. In 2015, EFSA adopted the TUL for vitamin E in line with the SCF of 300 mg/day for adults, including pregnant and lactating women. In 2024, EFSA reviewed the TUL of α-tocopherol previously established by the SCF, and found no basis to change the TUL, therefore retaining the TUL of 300 mg α-tocopherol/day for adults. This TUL also applies to pregnant and lactating women as no new evidence was found regarding specific adverse effects or different susceptibility in these groups (EFSA, 2024). EFSA further noted that two additional human intervention studies, which were not previously considered by the SCF, confirmed this conclusion. Also, in line with the SCF conclusions, EFSA considered the effect on blood clotting, and the increased risk of bleeding is the critical effect to establish a TUL for vitamin E (α-tocopherol) for the general population (EFSA, 2024).
Exposure
Vitamin E in the diet and in supplements
127. Vitamin E occurs naturally in a large variety of foods; main sources of vitamin E in the diet include plant oils (such as rapeseed oil (vegetable oil), sunflower oil, soya bean oil, corn oil and olive oil), nuts and seeds, wheatgerm (found in cereals and cereal products), fortified cereals, avocados, spinach, eggs, tuna, herring, swiss chard, tomatoes and broccoli (NHS, 2023; Huizen, 2023).
128. A summary of the vitamin E content of some common foods is presented in Table 1. This information is based on data UK where possible. This information is presented for information only as the exposure assessment for vitamin E has been performed using a nutrient assessment.
129. A nutrient assessment utilises the UK Nutrient Databank (NDB) using NDB and National Diet and Nutrition Survey (NDNS) years 1-11 data. The NDB contains extensive information on the nutrient content of foods, including vitamin E, and can be used with the NDNS food consumption data to estimate dietary exposure to specific nutrients.
130. Information on supplements that contain vitamin E and are available on the UK market was gathered from online research. Details of the supplements identified from the online research and that were subsequently used in this exposure assessment are presented in Annex B (in Annex B, Table 1). Where the vitamin E content of the supplement was provided on the packaging and/ or website, calculations have been performed to estimate the maximum daily exposure to vitamin E from that supplement.
131. A number of vitamin E containing drinks were identified in the online research; these were marketed as being beneficial to health as multivitamin drinks, metabolism boosting, or similar. Some meal replacements drinks which also contain vitamin E were identified. These drinks were not included in the exposure assessment as they are not considered to be either vitamin E supplements or MIDS.
Table 1. Summary of the typical vitamin E content in foods reported to be main dietary sources of vitamin E.
| Food type | Food | Typical vitamin E content (mg /100 g)* | Reference |
|---|---|---|---|
| Oils | Rapeseed oil | 22 | Nutridex |
| Oils | Wheatgerm oil | 140 | Nutridex |
| Oils | Olive oil | 5.1 | Nutridex |
| Oils | Sunflower oil | 49 | Nutridex |
| Oils | Corn oil | 17 | Nutridex |
| Oils | Soybean oil | 16 | Nutridex |
| Nuts, seeds | Sunflower seeds | 38 | Nutridex |
| Nuts, seeds | Almonds (whole kernels) | 26 | Nutridex |
| Nuts, seeds | Peanuts (dry roasted) | 1.1 | Nutridex |
| Cereals and cereal products (including Wheatgerm) | Breakfast cereal, fruit and fibre type, fortified | 1.4 | Nutridex |
| Cereals and cereal products (including Wheatgerm) | Breakfast cereal, wheat biscuits, Weetabix type, fortified | 1.5 | Nutridex |
| Cereals and cereal products (including Wheatgerm) | Breakfast cereal, oat, instant, plain, fortified, cooked, made up with semi-skimmed milk | 0.14 | Nutridex |
| Cereals and cereal products (including Wheatgerm) | Breakfast cereal, cornflakes, fortified | 0.14 | Nutridex |
| Cereals and cereal products (including Wheatgerm) | Breakfast cereal, rice, toasted/crisp, fortified | 0.16 | Nutridex |
| Cereals and cereal products (including Wheatgerm) | Bran, wheat | 1.0 | Nutridex |
| Cereals and cereal products (including Wheatgerm) | Bread, wheatgerm | 0.48 | Nutridex |
| Cereals and cereal products (including Wheatgerm) | Bread, white, average | 0.080 | Nutridex |
| Cereals and cereal products (including Wheatgerm) | Bread, brown, average | 0.010 | Nutridex |
| Cereals and cereal products (including Wheatgerm) | Bread, wholemeal, average | 0.28 | Nutridex |
| Vegetables | Broccoli | 1.7 | Nutridex |
| Vegetables | Spinach | 1.7 | Nutridex |
| Vegetables | Tomatoes | 0.52 | Nutridex |
| Vegetables | Swiss chard | 1.9 | 10 best foods high in vitamin E |
| Fruits | Avocado | 2.2 | Nutridex |
| Eggs | Egg | 1.3 | Nutridex |
| Fish | Tuna: Canned in brine | 0.42 | Nutridex |
| Fish | Tuna: Canned in sunflower oil | 2.8 | Nutridex |
| Fish | Tuna: Fresh | 0.13 | Nutridex |
| Fish | Herring: Pickled | 0.64 | Nutridex |
| Fish | Herring: Fresh | 0.76 | Nutridex |
| Fish | Kipper | 0.47 | Nutridex |
- Rounded to 2 significant figures.
UK Vitamin E intake – Supplements
132. The exposure assessment for supplements assumes that a woman of childbearing age (16-49 years) would consume only one type of supplement and would follow the instructions on either the packaging or the website for the dosage (whichever reports the highest dosage).
133. The daily vitamin E dose resulting from the consumption of the supplements identified for the exposure assessment is summarised in Table 2. Estimated daily doses are between 4 and 536 mg of vitamin E per day. Generally, MIDS resulted in lower doses than specific vitamin E supplements, particularly for those aimed at pregnant or breastfeeding women, or those looking to conceive.
134. Based on the range of recommended daily doses (4 -536 mg of vitamin E), an exposure assessment has been performed using the average bodyweight of women of childbearing age from the NDNS years 1-11 (70.3kg); this is presented in Table 2.
135. The resulting range of estimated exposure is 0.057 – 7.6 mg/kg bw/day. These values have been rounded to 2 significant figures.
Table 2: Exposure estimates for women of childbearing age (16-49 years) to vitamin E from supplements (vitamin E only and MIDS), identified by online research of UK retailers at the time of the assessment.
| Supplement name | Supplement type | Vitamin E content in a daily serving (maximum serving size) (mg) | Exposure to Vitamin E (maximum daily serving*) (mg/kg bw/day)** |
|---|---|---|---|
| Vitamin E 400iu Softgel Capsules | Capsules – Vitamin E only | 536 | 7.6 |
| Holland and Barrett Vitamin E capsules | Capsules – Vitamin E only | 268 | 3.8 |
| Boots Skin Formula Vitamin E | Capsules – Vitamin E only | 268 | 3.8 |
| Cytoplan Vitamin E as tocopherols and tocotrienols | Capsules – Vitamin E only | 300 | 4.3 |
| Bulk vitamin E softgels | Capsules – Vitamin E only | 268 | 3.8 |
| NOW Foods, Vitamin E-Oil, Antioxidant Protection, 170 mg | Liquid – Vitamin E only | 170 | 2.4 |
| Marney’s Vita Help Natural Vitamin E | Liquid – Vitamin E only | 12 | 0.17 |
| Vitabiotics Pregnacare Him & Her Conception | Tablet - MIDS | 4 | 0.057 |
| Vitabiotics Pregnacare Original | Tablet - MIDS | 4 | 0.057 |
| Vitabiotics Pregnacare Max | Tablet - MIDS | 4 | 0.057 |
| Vitabiotics Pregnacare Gummies | Gummies - MIDS | 3 | 0.043 |
| Vitabiotics Pregnacare Liquid Pregnancy Vitamins | Liquid - MIDS | 4 | 0.057 |
| Vitabiotics Wellwoman Multivitamin Gummies for Women | Gummies - MIDS | 24 | 0.34 |
| Vitabiotics Wellwoman Original Multivitamin for Women | Capsule - MIDS | 30 | 0.43 |
| Vitabiotics Wellwoman Plus | Tablet - MIDS | 36.6 | 0.52 |
| Vitabiotics Wellwoman Max | Tablet - MIDS | 20 | 0.28 |
| Centrum women | Tablet - MIDS | 16 | 0.23 |
| Inessa advanced multivitamin | Tablet - MIDS | 12 | 0.17 |
| Cytoplan women’s wholefood multivitamin capsules | Capsules - MIDS | 30 | 0.43 |
| Seven Seas Omega-3 and multivitamins | Tablet - MIDS | 18 | 0.26 |
| Boots a-z vitamins and minerals | Tablet - MIDS | 12 | 0.17 |
| Purolabs multivitamin | Capsules- MIDS | 25 | 0.36 |
| Nutravita multivitamins | Tablet - MIDS | 12 | 0.17 |
| Swallow multivitamin | Tablets - MIDS | 12 | 0.17 |
| Holland and Barrett Ultra woman | Caplet - MIDS | 22 | 0.31 |
| Weightworld multivitamin and mineral | Tablet - MIDS | 12 | 0.17 |
-
Maximum serving assumes the maximum amount recommended on the packaging or website of the supplement is consumed. E.g. if recommended to take 1-2 capsules per day, this table assumes 2 capsules would be taken. Another example is if the website suggests a serving of 2 capsules a day, but the packaging suggests 3, then the highest suggestion has been used.
-
Rounded to 2 significant figures.
UK Vitamin E exposure – Dietary
136. A nutrient assessment was performed using the National Diet and Nutrition Survey (NDNS) and the UK Nutrient Databank (NDB). This assessment used food groups based on those established for the 2014 Total Diet Study (TDS) for metals and other elements (FSA, 2014) with NDNS years 1-11 consumption data. Mean and 97.5th percentile exposure estimates have been provided on a chronic basis, using a population-based approach for women of childbearing age (16-49 years).
137. The exposure estimates for women of childbearing age to vitamin E from the diet are presented in Table 3 for each food group and all food groups (referred to as “All” in Table 3). It should be noted, that where all food groups does not refer to the sum of exposures from individual food groups, but is an exposure estimate from the distribution of exposures to vitamin E from all foods when considered together.
138. Based on the consumption of all food groups the mean dietary exposure to vitamin E for women of childbearing age is 9.0 mg/ person/ day or 0.13 mg/ kg bw/day. The high level (97.5th percentile) dietary exposure to vitamin E for women of childbearing age is 18 mg/ person /day or 0.28 mg/ kg bw/day.
Table 3. Chronic exposure to vitamin E from the diet for women of childbearing age (16-49 years) (NDNS years 1-11)
| Food groups | Consumers exposed to vitamin E from the food group | Mean (mg/ person/ day*) | P97.5 (mg/ person/ day*) | Mean (mg/ kg bw/day*) | P97.5 (mg/ kg bw/day*) |
|---|---|---|---|---|---|
| Bread | 2402 | 0.25 | 1.2 | 0.0038 | 0.017 |
| Misc cereals | 2500 | 1.2 | 3.9 | 0.018 | 0.062 |
| Milk | 2154 | 0.11 | 0.41 | 0.0016 | 0.0059 |
| Carcase meat | 1102 | 0.014 | 0.090 | 0.00020 | 0.0013 |
| Meat products | 1721 | 0.23 | 1.2 | 0.0033 | 0.018 |
| Fish and seafood | 1322 | 0.45 | 2.3 | 0.0068 | 0.037 |
| Canned vegetables | 1552 | 0.25 | 1.4 | 0.0037 | 0.022 |
| Other vegetables | 2378 | 0.59 | 2.4 | 0.0088 | 0.039 |
| Green vegetables | 2020 | 0.21 | 1.1 | 0.0032 | 0.017 |
| Potatoes | 2005 | 0.58 | 2.7 | 0.0086 | 0.043 |
| Fresh fruit | 1858 | 0.27 | 1.5 | 0.0041 | 0.023 |
| Sugars and confectionary | 1334 | 0.17 | 1.1 | 0.0026 | 0.017 |
| Non-alcoholic beverages | 564 | 0.029 | 0.24 | 0.00043 | 0.0036 |
| Fruit products | 1204 | 0.14 | 0.85 | 0.0022 | 0.014 |
| Alcoholic beverages# | 25 | 0.0022 | 0 | 0.000033 | 0 |
| Condiments | 2351 | 1.1 | 5.2 | 0.016 | 0.081 |
| Poultry | 1994 | 0.38 | 2.1 | 0.0055 | 0.035 |
| Nuts and seeds | 734 | 0.32 | 2.7 | 0.0049 | 0.044 |
| Snacks | 1452 | 0.50 | 2.3 | 0.0074 | 0.038 |
| Fats and oils | 2378 | 1.5 | 6.1 | 0.022 | 0.094 |
| Eggs | 1367 | 0.33 | 1.6 | 0.0049 | 0.024 |
| Dairy products | 2203 | 0.28 | 1.5 | 0.0042 | 0.022 |
| Desserts | 840 | 0.092 | 0.79 | 0.0014 | 0.012 |
| Meat alternatives | 137 | 0.025 | 0.31 | 0.00037 | 0.0045 |
| Offal | 86 | 0.0029 | 0.038 | 0.000042 | 0.00054 |
| **All | 2556 | 9.0 | 18 | 0.13 | 0.28 |
- Rounded to 2 significant figures.
- This is not a sum of all the individual groups.
There are very few consumers exposed to vitamin E from the alcoholic beverage food group as the large majority of the products within the group do not contain vitamin E. For this reason, there are very few consumption events where consumers of alcoholic beverages are exposed to vitamin E from these foods, compared with the total number of consumption events. Therefore, it is possible for the 97.5th percentile to be 0 in this case.
Combined exposure assessment scenarios
139. It is possible that women of childbearing age may take a supplement containing vitamin E at varying dosages and that this exposure occurs in addition to their dietary intake of vitamin E. The scenarios included in this section aim to estimate the combined exposure to vitamin E from supplements and the diet. These scenarios are listed below.
140. Scenario 1: Average estimate – combines the range of exposure estimates for vitamin E intake from supplements with the mean dietary exposure estimate for vitamin E (‘All’ in Table 3) for women of childbearing age
141. Scenario 2: High-level estimate– combines the high-level exposure estimate for vitamin E intake from supplements (highest recommended dose) and the high-level dietary exposure estimate (97.5th percentile) for vitamin E (‘All’ in Table 3), for women of childbearing age.
142. The exposure estimates for these scenarios are presented in Table 4.
Table 4. Exposure estimates for scenarios 1 and 2 (combining dietary exposure estimates to vitamin E with exposure estimates from supplements)
| Scenario | Exposure estimates (mg/ person/ day*) | Exposure estimates (mg/ kg bw/day*) |
|---|---|---|
| Scenario 1: Average estimate (range of supplementation and mean dietary exposure ) | 13-550 | 0.19-7.7 |
| Scenario 2: High-level estimate (highest supplementation and high level (97.5th percentile) dietary exposure) | 550 | 7.9 |
- Rounded to 2 significant figures.
Uncertainties and assumptions
143. Some assumptions have been made where dosage recommendations are varied. In cases where the dosage is given as a range (e.g. 1-3 capsules per day), the highest recommended amount has been assumed to be consumed (e.g. 3 capsules per day). Also, where there is a discrepancy between the packaging image and website instructions, the highest dosage has been assumed e.g. if the website suggests a serving of 2 capsules a day, but the packaging suggests 3, then the highest suggestion has been used.
144. For many of the supplements listed, the warnings provided on the website/ packaging recommend that pregnant or breastfeeding women consult a doctor/ healthcare professional before taking them. It is possible that a health care professional may advise against taking certain supplements or advise a different dosage. Actual vitamin E intakes from supplements may therefore vary depending on individual circumstances.
145. The NDNS does not include pregnant or breastfeeding women and so the nutrient assessment has been performed for women aged 16-49 (women of childbearing age). The diet of this population group may not be fully representative of the maternal diet.
146. The “Alcoholic beverages” food group has been included in the assessment as the exposure assessment uses women of childbearing ages as a proxy and this consumption may differ to those who are pregnant or trying to conceive.
147. In NDNS there is a reported 30% energy intake underestimation. There are many possible reasons for this, resulting from both misreporting and the survey design. However, exposure assessments at the 97.5th percentile are undertaken to ensure that high consumers are accounted for in the assessment, including those who may have mis-reported their energy intake.
Risk Characterisation
148. EFSA (2024) reviewed the TUL of α-tocopherol from all dietary source and found no basis to change the TUL previously established by the SCF, therefore retaining the TUL of 300 mg α- tocopherol/day for adults, including pregnant and lactating women from all dietary sources. The EVM (2003) recommended a SUL of 800 IU/day (540 mg d–tocopherol equivalents/day) supplemental vitamin E. Assuming an intake of 18 mg/day from food, a total intake of 560 mg d–tocopherol equivalents/day would not be expected to result in any adverse effect. (EVM, 2003).
149. Based on the TUL of 300 mg/day and taking women of childbearing age as a whole, the dietary intake of vitamin E from food sources is well below the TUL and therefore would not be a concern for their health or for fetal development. Vitamin E is widely distributed in common foods such as vegetable oils, nuts, seeds and cereals, and typical dietary patterns do not result in excessive intakes.
150. However, use of high-dose vitamin E supplements may result in intakes exceeding the EFSA TUL. Individuals consuming the highest-level supplements of α-tocopherol in combination with a high-level dietary exposure estimate (97.5th percentile) have calculated intakes of 550 mg/day (shown in Table 4), exceeding the EFSA TUL.
151. Using a more conservative approach and considering that the TUL set by EFSA accounts for all dietary sources, the TUL of 300 mg/day is used to characterise the risk to health from intake of Vitamin E during pregnancy. Therefore, there may be an increased risk of impaired blood clotting or haemorrhagic effects, particularly in susceptible individuals or those taking anticoagulant medication. However, it should be noted that evidence for adverse effects at these intake levels remain limited and inconsistent.
152. Considering the use of high-dose vitamin E supplements, particularly in pregnancy or individuals with conditions affecting blood coagulation, individuals would be advised seek advice from their medical practitioner prior to taking high-dose supplements to reduce potential risk associated with excessive vitamin E intake.
Discussion and conclusions
153. Vitamin E in the diet is essential for health in general and vitamin E deficiency in pregnant women is known to compromise fetal development and increase the risk of miscarriage, pre-eclampsia, and premature delivery (Gagné, et al., 2009).
154. Vitamin E functions as an antioxidant and deactivates ROS, mostly directed at cellular membrane lipids where it protects against ROS‑mediated lipid peroxidation by preventing and terminating reactions that produce peroxide, which act as secondary ROS.
155. Excessive vitamin E intake has been associated with a range of potential adverse effects, including increased risk of gestational hypertension, pre-eclampsia, and macrosomia. Also, elevated cord blood vitamin E levels have been associated with increased risk of small‑for‑gestational‑age (SGA) births and reduced birth weight.
156. Higher dietary vitamin E intake in early pregnancy has been associated with reduced insulin sensitivity, which may indicate a potential adverse effect on glucose metabolism.
157. Vitamin E has also been found to interfere with vitamin K absorption and metabolism, reducing the production of vitamin K-dependant clotting factors, resulting in increased risk of prolonged bleeding. This interaction was identified as a critical endpoint for establishing the TUL, and although direct evidence in pregnant women is very limited, it remains a concern that such effects could have adverse effects during pregnancy and childbirth. This is a greater concern in the context of high-dose supplements, which may result in total vitamin E intakes exceeding the TUL when combined with dietary exposure.
158. Evidence reviewed by the World Health Organization indicates that vitamin E supplementation during pregnancy may increase the risk of premature rupture of membranes (PROM) and abdominal pain, despite potential reductions in placental abruption. This highlights uncertainty regarding the overall benefit–risk balance of vitamin E supplementation during pregnancy.
159. Results from large-scale observational human studies have been limited and inconsistent, however these studies were often not designed to detect adverse effects, were reliant on self-reporting, or did not record vitamin E supplementation.
160. Animal studies found that high-dose vitamin E supplementation was associated with reduced fertility, impaired oocyte development, and altered ovarian physiology, potentially mediated through oxidative or reductive stress pathways. While the relevance of these findings relating to humans is uncertain, they are consistent with the hypothesis that excessive antioxidant exposure may disrupt normal redox balance, with downstream effects on reproductive health.
161. Dietary vitamin E is generally well below established upper intake levels and is unlikely to pose a risk. High-dose supplementation can lead to total intakes exceeding the EFSA TUL of 300 mg/day. Overall, evidence is inconsistent with limitations, however a consistent finding across studies is that adverse effects are more likely to occur in the context of high-dose vitamin E supplementation rather than habitual dietary intake.
The Committee is asked to consider the following questions:
a) Does the Committee have any comments on the discussion paper?
b) Does the Committee agree on the use of the more conservative EFSA 2024 TUL or the previous EVM SUL?
c) Does the Committee agree with contents and structure of the discussion paper?
d) Does the Committee have any other comments?
Abbreviations
| Abbreviation | Definition | |
|---|---|---|
| α-CEHC | α-Carboxyethyl Hydroxychromanol | |
| α-TTP | α-tocopherol transfer protein | |
| AGA | Appropriate for Gestational Age | |
| aOR | Adjusted Odds Ratio | |
| ART | Assisted Reproductive Technology | |
| ATBC | Alpha-Tocopherol Beta-Carotene | |
| CHAOS | Cambridge Heart Antioxidant Study | |
| COT | Committee on Toxicity | |
| EAT | Exposure and Trade Team | |
| EFSA | European Food Safety Authority | |
| EU | European Union | |
| FSA | Food Standards Agency | |
| FSS | Food Standards Scotland | |
| GH | Gestational Hypertension | |
| hERG | Human Ether-à-go-go-Related Gene | |
| HDL | High-Density Lipoprotein | |
| HXT | Hydroxytyrosol | |
| IU | International Units | |
| LDL | Low-Density Lipoprotein | |
| NDNS | National Diet and Nutrition Survey | |
| NHS | National Health Service | |
| NOAEL | No Observed Adverse Effect Level | |
| PE | Preeclampsia | |
| PFAS | Per- and Polyfluoroalkyl Substances | |
| PROM | Premature Rupture of Membranes | |
| QUICKI | Quantitative Insulin Sensitivity Check Index | |
| ROS | Reactive Oxygen Species | |
| SACN | Scientific Advisory Committee on Nutrition | |
| SGA | Small for Gestational Age | |
| SUL | Safe Upper Level | |
| TC | Total Cholesterol | |
| TDS | Total Diet Study | |
| TG | Triglycerides | |
| TRF | Tocotrienol-Rich Fraction | |
| TTE | Transplacental Transfer Efficiency | |
| TUL | Tolerable Upper Intake Level | |
| UF | Uncertainty Factor | |
| WHO | World Health Organisation |
References
Abdo, K. M., Rao, G., Montgomery, C. A., Dinowitz, M., & Kanagalingam, K. 1986. Thirteen- week toxicity study of d- alpha- tocopheryl acetate (vitamin E) in Fischer 344 rats. Food and Chemical Toxicology, 24, 1043–1050. Thirteen-week toxicity study of d-α-tocopheryl acetate (vitamin E) in Fischer 344 rats - ScienceDirect
Allan KM, Prabhu N, Craig LC, McNeill G, Kirby B, McLay J, Helms PJ, Ayres JG, Seaton A, Turner SW and Devereux G, 2015. Maternal vitamin D and E intakes during pregnancy are associated with asthma in children. European Respiratory Journal, 45, 1027-1036.
Anthony, J., Smith, P., Mantel, G., & Johanson, R. 1996. A randomised controlled trial of vitamin E supplementation in conservatively managed pre- eclamptic patients. Proceedings of the 10th world congress of the International Society for the Study of hypertension in pregnancy; 1996 August 4–8 (p. 193). Seattle, USA.
Atazadegan, M.A., Yazdi, M., Biabanaki-Goortani, A. and Goodarzi-Khoigani, M., 2024. Is Nutritional Status Associated with Quantitative Insulin Sensitivity Check Index in the First Trimester of Gestation?. Journal of Kerman University of Medical Sciences, 31(5).
Bastani, P., Hamdi, K., Abasalizadeh, F., & Navali, N. 2011. Effects of vitamin E supplementation on some pregnancy health indices: A randomized clinical trial. International Journal of General Medicine, 4, 461–464. 10.2147/IJGM.S20107
Bates, B.; Lennox, A.; Prentice, A.; Bates, C.; Page, P.; Nicholson, S.; Swan, G. 2014. National Diet and Nutrition Survey Results from Years 1, 2, 3 and 4 (combined) of the Rolling Programme (2008/2009 – 2011/2012) Main heading
Bates, B.; Cox, L.; Nicholson, S.; Page, P.; Prentice, A.; Steer, T.; Swan, G. 2016. National Diet and Nutrition Survey Results from Years 5 and 6 (combined) of the Rolling Programme (2012/2013 – 2013/2014) Main heading
Bates, B.; Collins, D.; Jones, K.; Page, P.; Roberts, C.; Steer, T.; Swan, G. 2020. National Diet and Nutrition Survey Results from years 9, 10 and 11 (combined) of the Rolling Programme (2016/2017 to 2018/2019) National Diet and Nutrition Survey
Booth, S. L., Golly, I., Sacheck, J. M., Roubenoff, R., Dallal, G. E., Hamada, K., & Blumberg, J. B. 2004. Effect of vitamin E supplementation on vitamin K status in adults with normal coagulation status. The American Journal of Clinical Nutrition, 80, 143–148. 10.1093/ajcn/80.1.143
Boots. 2025. A-Z multivitamins. Boots A-Z 180 Tablets (6 month supply) - Boots. Viewed 24/11/2025.
Boots. 2025. Boots skin formula Vitamin E, 400iu capsules. Boots Skin Formula Vitamin E, 90 Capsules - Boots. Viewed 21/11/2025
Boskovic R, Gargaun L, Oren D, Djulus J, Koren G. Pregnancy outcome following high doses of Vitamin E supplementation. Reprod Toxicol. 2005 May-Jun;20(1):85-8. doi: 10.1016/j.reprotox.2005.01.003. PMID: 15808790.
Brigelius-Flohe R: Vitamin E: the shrew waiting to be tamed. Free Radic Biol Med. 2009.;46(5):543-54. doi: 10.1016/j.freeradbiomed.2008.12.007
Bulk. 2025. Vitamin E softgels, 400iu. Vitamin E Softgels 400 IU Pure Vitamin E Bulk™. Viewed 21/11/2025.
Butte NF, Lopez-Alarcon MG and Garza C, 2002. Nutrient adequacy of exclusive breastfeeding for the term infant during the first six months of life. World Health Organization, 57 pp.
Corrigan, J.J. and Marcus, F.I., 1974. Coagulopathy associated with vitamin E ingestion. Jama, 230(9), pp.1300-1301.
Cytoplan 2025. Vitamin E as tocopherol and tocotrienols. Tocopherols & Tocotrienols Complex Vitamin E Cytoplan. Viewed 21/11/2025
Cytoplan 2025. Women’s wholefood multi with Iron . Women’s Wholefood Multi Award-Winning Multivitamin Capsules. Viewed 24/11/2025
Damodaran, T., Yahaya, N.S. and Mordi, M.N., 2025. Integrative toxicity assessment of tocotrienol-rich fraction from palm oil using in silico methods and zebrafish embryotoxicity model. Toxicology in Vitro, 107, p.106062.
Devereux G, Turner SW, Craig LC, McNeill G, Martindale S, Harbour PJ, Helms PJ and Seaton A, 2006. Low maternal vitamin E intake during pregnancy is associated with asthma in 5-year-old children. American Journal of Respiratory and Critical Care Medicine, 174, 499-507.
Didenco, S., Gillingham, M. B., Go, M. D., Leonard, S. W., Traber, M. G., & McEvoy, C. T. 2011. Increased vitamin E intake is associated with higher alpha- tocopherol concentration in the maternal circulation but higher alpha- carboxyethyl hydroxychroman concentration in the fetal circulation. The American Journal of Clinical Nutrition, 93, 368–373. 10.3945/ajcn.110.008367
Dror, D.K. and Allen, L.H., 2011. Vitamin E deficiency in developing countries. Food and nutrition bulletin, 32(2), pp.124-143.
EFSAa (EFSA Panel on Dietetic Products, Nutrition and Allergies), 2015. Scientific Opinion on Dietary Reference Values for vitamin E as α‐tocopherol. EFSA Journal, 13(7), p.4149.
EFSAb (EFSA Panel on Food Additives and Nutrient Sources added to Food). 2015. Scientific Opinion on the re- evaluation of tocopherol- rich extract (E 306), α- tocopherol (E 307), γ- tocopherol (E 308) and δ- tocopherol (E 309) as food additives. EFSA Journal, 13(9), 4247. https:// doi. org/ 10. 2903/j. efsa. 2015. 4247
EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies), 2009. Scientific Opinion on the appropriate age for introduction of complementary feeding of infants. EFSA Journal 2009;7(12):1423, 38 pp. doi:10.2903/j.efsa.2009.1423
EFSA NDA Panel (Panel on Nutrition, Novel Foods and Food Allergens), Turck, D., Bohn, T., Castenmiller, J., de Henauw, S., Hirsch‐Ernst, K.I., Knutsen, H.K., Maciuk, A., Mangelsdorf, I., McArdle, H.J. and Pentieva, K., 2024. Scientific opinion on the tolerable upper intake level for vitamin E. EFSA Journal, 22(8), p.e8953.
Elise Kelly, Simon Sinclair. 2025. Nutridex. Nutridex
Expert Group on Vitamins and Minerals (EVM). 2003. Safe Upper Levels for Vitamins and Minerals. [ARCHIVED CONTENT] Expert Group on Vitamins and Minerals (2003) Safe Upper Levels for Vitamins and Minerals Food Standards Agency
FAO/WHO/UNU (Food and Agriculture Organization of the United Nations/World Health Organization/United Nations University), 2004. Human energy requirements. Report of a Joint FAO/WHO/UNU Expert Consultation: Rome, 17–24 October 2001. FAO food and nutrition technical report series, 103 pp.
Farrell, P.M. and Bieri, J.G., 1975. Megavitamin E supplementation in man. The American Journal of Clinical Nutrition, 28(12), pp.1381-1386.
Frank, J., Weiser, H., & Biesalski, H. K. 1997. Interaction of vitamins E and K: Effect of high dietary vitamin E on phylloquinone activity in chicks. International Journal for Vitamin and Nutrition Research, 67, 242–247.
Freedman, J. E., Farhat, J. H., Loscalzo, J., & Keaney, J. F., Jr. 1996. Alpha- tocopherol inhibits aggregation of human platelets by a protein kinase C- dependent mechanism. Circulation, 94, 2434–2440. https://doi.org/10.1161/01.CIR.94.10.2434
FoodPlus. 2025. Dr Witt Premium metabolism green multivitamin drink. Dr Witt Premium Metabolism Green Multivitamin Drink 1l Food Plus Shop online. Viewed 24/11/2025.
Food Standard Agency. 2014. Total diet study: Metals and other elements. View PDF
Gagné, A., Wei, S.Q., Fraser, W.D. and Julien, P., 2009. Absorption, transport, and bioavailability of vitamin e and its role in pregnant women. Journal of Obstetrics and Gynaecology Canada, 31(3), pp.210-217.
Gianello, R., Hall, W.C., Kennepohl, E., Libinaki, R. and Ogru, E., 2007. Subchronic oral toxicity study of mixed tocopheryl phosphates in rats. International journal of toxicology, 26(5), pp.475-490.
Gillilan, R. E., Mondell, B., & Warbasse, J. R. 1977. Quantitative evaluation of vitamin E in the treatment of angina pectoris. American Heart Journal, 93, 444–449. 10.1016/s0002-8703(77)80406-7
Gómez, G., Heras-Molina, A., Núñez, Y., Sánchez-Esquiliche, F., Gómez-Carballar, F., Olivares, Á., González-Bulnes, A., Rey, A.I., Óvilo, C., García-Casco, J.M. and Muñoz, M., 2025. Impact of maternal antioxidant supplementation on ovarian development in prepuberal Iberian pig offspring. Translational Animal Science, 9, p.txaf078.
Greco E, Romano S, Iacobelli M, Ferrero S, Baroni E, Minasi MG, Ubaldi F, Rienzi L and Tesarik J, 2005. ICSI in cases of sperm DNA damage: beneficial effect of oral antioxidant treatment. Human Reproduction, 20, 2590–2594.
Greenblatt, I.J., 1957, January. Use of massive doses of vitamin-E in humans and rabbits to reduce blood lipids. In Circulation (Vol. 16, No. 3, pp. 508-508). 227 East Washington SQ, Philadelphia, PA 19106: Lippincott Williams & Wilkins.
Helson, L. 1984. The effect of intravenous vitamin E and menadiol sodium diphosphate on vitamin K dependent clotting factors. Thrombosis Research, 35, 11–18. 10.1016/0049-3848(84)90308-6
Herrera E, Barbas C. Vitamin E: action, metabolism and perspectives. J Physiol Biochem. 2001. Mar;57(2):43-56. PMID: 11579997. Vitamin E: action, metabolism and perspectives - PubMed
Holland and Barett. 2025. Centrum women. Centrum Women (60 Tablets) H&B. viewed 24/11/2025.
Holland and Barett. 2025. Multivitamins and minerals, Ultra woman. Holland & Barrett Ultra Woman Tablets 3 Months Supply Bundle H&B. viewed 24/11/2025.
Holland and Barett. 2025. SevenSeas Omega-3 and multivitamins (woman). Omega-3 & Multivitamins Woman Duo Pack Seven Seas H&B. viewed 24/11/2025.
Holland and Barett. 2025. Vitamin E 400iu capsules. Holland & Barrett Vitamin E 400iu 30 Capsules H&B. Viewed 21/11/2025
Huel. 2025. Ready-to-drink On-the-go meal shakes. Ready-To-Drink Meal Replacement Shakes Huel. Viewed 24/11/2025.
iHerb. 2025. NOW Foods, Vitamin E-Oil, 170mg (253 iu). NOW Foods, Vitamin E-Oil, Antioxidant Protection, 170 mg (253 IU), 1 fl oz (30 ml). Viewed 21/11/2025.
Inessa. 2025. Advanced multivitamin. Inessa Advanced Multivitamin. Viewed 24/11/2025.
IOM (Institute of Medicine). 2001. Dietary reference intakes for vitamin C, vitamin E, selenium, and carotenoids (p. 531). Food and Nutrition Board. National Academy Press.
Jandak, J., Steiner, M., & Richardson, P. D. 1989. Alpha- tocopherol, an effective inhibitor of platelet adhesion. Blood, 73, 141–149. https:// doi. org/ 10. 1182/ blood. V73.1. 141. 141
Jennifer Huizen. 2023. 10 foods rich in vitamin E. The 10 best foods high in vitamin E
Kappus, H. and Diplock, A.T., 1992. Tolerance and safety of vitamin E: a toxicological position report. Free Radical Biology and Medicine, 13(1), pp.55-74.
Kaempf-Rotzoll DE, Horiguchi M, Hashiguchi K, Aoki J, Tamai H, Linderkamp O and Arai H, 2003. Human placental trophoblast cells express alpha-tocopherol transfer protein. Placenta, 24, 439-444.
Kakishita, E., Suehiro, A., Oura, Y., & Nagai, K. 1990. Inhibitory effect of vitamin E (alpha- tocopherol) on spontaneous platelet aggregation in whole blood. Thrombosis Research, 60, 489–499.
Klein EA, Thompson IM, Jr., Tangen CM, Crowley JJ, Lucia MS, Goodman PJ, Minasian LM, Ford LG, Parnes HL, Gaziano JM, Karp DD, Lieber MM, Walther PJ, Klotz L, Parsons JK, Chin JL, Darke AK, Lippman SM, Goodman GE, Meyskens FL, Jr. and Baker LH, 2011. Vitamin E and the risk of prostate cancer: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). Journal of the American Medical Association, 306, 1549-1556.
Krasavage, W.J. and Terhaar, C.J., 1977. d-. alpha.-Tocopheryl poly (ethylene glycol) 1000 succinate: acute toxicity, subchronic feeding, reproduction, and teratologic studies in the rat. Journal of Agricultural and Food Chemistry, 25(2), pp.273-278.
Li, C., Deng, S., Zhou, P., Rao, J., Xiang, Y., Xi, L. and Wang, X., 2026. Beyond deficiency prevention: meteorological determinants and nonlinear associations of maternal vitamins D, A, and E with perinatal outcomes in 10,824 Chinese pregnancies. Frontiers in Nutrition, 13, p.1737197.
Litonjua AA, Rifas-Shiman SL, Ly NP, Tantisira KG, Rich-Edwards JW, Camargo CA, Jr., Weiss ST, Gillman MW and Gold DR, 2006. Maternal antioxidant intake in pregnancy and wheezing illnesses in children at 2 y of age. American Journal of Clinical Nutrition, 84, 903-911.
Marneys. 2025. Liquid Vitamin E VITAHELP. Liquid Vitamin E MARNYS. Viewed 21/11/2025
March, B. E., Wong, E., Seier, L., Sim, J., & Biely, J. 1973. Hypervitaminosis E in the chick. The Journal of Nutrition, 103, 371–377. https://doi.org/10.1093/jn/103.3.371
Martindale S, McNeill G, Devereux G, Campbell D, Russell G and Seaton A, 2005. Antioxidant intake in pregnancy in relation to wheeze and eczema in the first two years of life. American Journal of Respiratory & Critical Care Medicine, 171, 121-128.
Megavitamin E Supplementation and Vitamin K-Dependent Carboxylation, Nutrition Reviews, Volume 41, Issue 9, September 1983, Pages 268–270, https://doi.org/10.1111/j.1753-4887.1983.tb07197.x
Meydani, S. N., Meydani, M., Blumberg, J.B., Leka, L.S., Pedrosa, M., Diamond, R., Schaefer, E.J. 1998. Assessment of the safety of supplementation with different amounts of vitamin E in healthy older adults. American Journal of Clinical Nutrition 68, 311-318.
Miller, D.R. and Hayes, K.C., 2012. Vitamin excess and toxicity. Nutritional toxicology, 1, pp.81-133.
Mou, Z., He, J., Zhou, S., Deng, F., Peng, R., Yuan, J., Wei, Y. and Tan, L., 2026. Fat-Soluble Vitamins Modulate Transplacental Transfer Efficiencies of Per-and Polyfluoroalkyl Substances and Their Association with Neonatal Anthropometric Measurements. Journal of Hazardous Materials, p.142232.
Muller-Schmehl K, Beninde J, Finckh B, Florian S, Dudenhausen JW, Brigelius-Flohe R and Schuelke M, 2004. Localization of alpha-tocopherol transfer protein in trophoblast, fetal capillaries’ endothelium and amnion epithelium of human term placenta. Free Radical Research, 38, 413-420.
NHS. 2023. Vitamin E-Vitamins and minerals. Vitamins and minerals - Vitamin E - NHS
NHS (2020). NHS advice on vitamins and minerals: Vitamin E. Last reviewed, August 2020 Vitamins and minerals - Vitamin E – NHS
Nutravita. 2025. Multivitamins and minerals. Multivitamin Minerals - Vegan & Vegetarian Multivitamins - Nutravita Nutravita. Viewed 24/11/2025
Nutritionvalu.org. 2025. Beverages fortified acai berry drink. Beverages, fortified, Acai berry drink nutrition facts and analysis. viewed 24/11/2025
OECD (Organisation for Economic Co-operation and Development), 1998a. OECD Guideline for testing of chemicals. Test No. 408: Repeated Dose 90-day Oral Toxicity Study in Rodents. Adopted 21 September 1998. Test No. 408: Repeated Dose 90‑Day Oral Toxicity Study in Rodents OECD
Okebukola PO, Kansra S, Barrett J: Vitamin E supplementation in people with cystic fibrosis. Cochrane Database Syst Rev. 2017 Mar 6;3:CD009422. 10.1002/14651858.CD009422.pub3
Pippen, J.L., McGee, P., Roberts, J.M., Myatt, L., Varner, M.W., Tita, A.T., Wapner, R.J., Thorp Jr, J.M., Mercer, B.M., Plunkett, B.A. and Blackwell, S.C., 2025. The Effect of Maternal Antioxidant Vitamin Supplementation on Maternal and Cord Blood Adiponectin Concentrations. American journal of perinatology, 42(11), pp.1469-1476.
Podszun, M., & Frank, J. 2014. Vitamin E- drug interactions: Molecular basis and clinical relevance. Nutrition Research Reviews, 27, 215–231. 10.1017/S0954422414000146
Pressman EK, Cavanaugh JL, Mingione M, Norkus EP and Woods JR, 2003. Effects of maternal antioxidant supplementation on maternal and fetal antioxidant levels: A randomized, double-blind study. American Journal of Obstetrics and Gynecology, 189, 1720-1725.
ProteinPackage. 2025. Vitamin Well Vitamin Drinks. Vitamin Well Vitamin Drinks 12x500ml Protein Package Protein Package. Viewed 24/11/2025.
Purolabs. 2025. Puro vegan Multivitamin. Vegan Multivitamin Multivitamins Purolabs. Viewed 24/11/2025.
Rabiee, F., Fattahi, M., Iranzad, M., Rahimi Andani, M., Jafarpour, F., Sanei, M.H., Drevet, J.R. and Nasr-Esfahani, M.H., 2026. Excessive Vitamin E Supplementation: Implications for Ovarian Physiology and Reproductive Health. Oxidative Medicine and Cellular Longevity, 2026(1), p.1330508.
Roberts, C.; Steer, T.; Maplethorpe, N.; Cox, L.; Meadows, S.; Page, P.; Nicholson, S.; Swan, G. 2018. National Diet and Nutrition Survey Results from Years 7 and 8 (combined) of the Rolling Programme (2014/2015 – 2015/2016) National Diet and Nutrition Survey
Rotzoll, D.E., Scherling, R., Etzl, R., Stepan, H., Horn, L.C. and Pöschl, J.M., 2008. Immunohistochemical localization of α-tocopherol transfer protein and lipoperoxidation products in human first-trimester and term placenta. European Journal of Obstetrics & Gynecology and Reproductive Biology, 140(2), pp.183-191.
Rumbold, A., Ota, E., Hori, H., Miyazaki, C., & Crowther, C. A. 2015. Vitamin E supplementation in pregnancy. Cochrane Database of Systematic Reviews, 2015, CD004069. 10.1002/14651858.CD004069.pub3
Rutkowski, M., Grzegorczyk, K. 2012. Adverse effects of antioxidative vitamins. International Journal of Occupational Medicine and Environmental Health. 25, 105–121. pdf-2262-2130
Sawhney, H., Singhal, S., Vasishta, K., & Majumbar, S. 2003. Effect of vitamin E supplementation on lipid peroxide levels in preeclampsia. International Journal of Gynecology & Obstetrics, 70, E31. https:// doi. org/ 10. 1016/ S0020- 7292(00) 82441- 8
SCF (Scientific Committee on Food), 2003. Opinion of the Scientific Committee on Food on the Tolerable Upper Intake Levels of vitamin E. SCF/CS/NUT/UPPLEV/39 Final, 10 pp.
Scholl TO, Chen X, Sims M and Stein TP, 2006. Vitamin E: maternal concentrations are associated with fetal growth. American Journal of Clinical Nutrition, 84, 1442–1448.
Shahraki, A. D. 2006. Effects of vitamin E, calcium carbonate and milk of magnesium on muscular cramps in pregnant women. Journal of Medical Sciences, 6, 979–983. https://doi.org/10.3923/jms.2006.979.983
Srivastava, K. C. 1986. Vitamin E exerts antiaggregatory effects without inhibiting the enzymes of the arachidonic acid cascade in platelets. Prostaglandins, Leukotrienes, and Medicine, 21, 177–185. https:// doi. org/ 10. 1016/ 0262- 1746(86) 90151- 4
Steiner, M. 1983. Effect of alpha- tocopherol administration on platelet function in man. Thrombosis and Haemostasis, 49, 73–77. Effect of alpha-tocopherol administration on platelet function in man - PubMed
Steiner, M. 1999. Vitamin E, a modifier of platelet function: Rationale and use in cardiovascular and cerebrovascular disease. Nutrition Reviews, 57, 306–309. 10.1111/j.1753-4887.1999.tb06903.x
Stephens, N. G., Parsons, A., Schofield, P. M., Kelly, F., Cheeseman, K., & Mitchinson, M. J. 1996. Randomised controlled trial of vitamin E in patients with coronary disease: Cambridge heart antioxidant study (CHAOS). Lancet, 347, 781–786. https:// doi. org/ 10. 1016/ s0140- 6736(96) 90866- 1
Supplemented. 2025. Vitamin E 400iu softgel capsules. Vitamin E 400iu Softgel Capsules – Supplemented. Viewed 21/11/2025
Swallow. 2025. Daily multivitamin. Daily Multivitamin Tablets for Women and Men - High Dose – The Swallow Co. viewed 24/11/2025.
Szewczyk, K., Bryś, J., Brzezińska, R. and Górnicka, M., 2025. Nutritional status of vitamin E and its association with metabolic health in adults. Nutrients, 17(3), p.408.
Takahashi, O., Ichikawa, H., & Sasaki, M. 1990. Hemorrhagic toxicity of d- alpha- tocopherol in the rat. Toxicology, 63, 157–165. https://doi.org/10.1016/0300-483X(90)90039-J
Tappel, A. 1972. Vitamin E and free radical peroxidation of lipids. Ann. N. Y. Acad. Sci. 203(1):12-28.
The Alpha-Tocopherol Beta Carotene Cancer Prevention Study Group, 1994. The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. New England Journal of Medicine, 330, 1029-1035.
Tovar, A., Ameho, C.K., Blumberg, J.B., Peterson, J.W., Smith, D. and Booth, S.L., 2006. Extrahepatic tissue concentrations of vitamin K are lower in rats fed a high vitamin E diet. Nutrition & Metabolism, 3(1), p.29.
Tsai, A.C., Kelley, J.J., Peng, B. and Cook, N., 1978. Study on the effect of megavitamin E supplementation in man. The American Journal of Clinical Nutrition, 31(5), pp.831-837.
Verve. 2025. Transparent Greens V80 Powder. V80 Greens Powder from Verve - Boost Your Nutrition. Viewed 24/11/2025
Vitabiotics. 2025. Pregnacare him and her conception tablets. Pregnacare® Him & Her Conception Tablets By Vitabiotics. Viewed 21/11/2025.
Vitabiotics. 2025. Pregnacare original tablets. Pregnacare® Original Pregnancy Supplement Vitabiotics. Viewed 21/11/2025
Vitabiotics. 2025. Pregnacare max. Pregnacare® Max Pregnancy Vitamins By Vitabiotics. Viewed 21/11/2025
Vitabiotics. 2025. Pregnacare gummies. Pregnacare® Gummies Pregnancy Gummies Vitabiotics. Viewed 21/11/2025
Vitabiotics. 2025. Pregnacare liquid. Pregnacare® Liquid Pregnancy Vitamins Vitabiotics. Viewed 21/11/2025
Vitabiotics. 2025. Wellwoman multivitamin gummies. Wellwoman® Multi - Vitamin Gummies For Women. Viewed 24/11/2025.
Vitabiotics. 2025. Wellwoman original. Wellwoman Original Multivitamin For Women Vitabiotics®. Viewed 24/11/2025.
Vitabiotics. 2025. Wellwoman plus. Wellwoman® Plus Omega 3-6-9 By Vitabiotics. Viewed 24/11/2025.
Vitabiotics. 2025. Wellwoman Max. Wellwoman® Max Supplement For Women By Vitabiotics. Viewed 24/11/2025.
Wangkheimayum, S., Kumar, S., & Suri, V. (2011). Effect of vitamin E on sP- selectin levels in pre- eclampsia. Indian Journal of Clinical Biochemistry, 26, 169–171. Effect of Vitamin E on sP-Selectin Levels in Pre-Eclampsia Indian Journal of Clinical Biochemistry Springer Nature Link
WeightWorld. 2025. Multivitamins and Minerals tablets. Multivitamin and Mineral Tablets 400 Tablets WeightWorld. Viewed 24/11/2025.
Wheldon, G. H., Bhatt, A., Keller, P., & Hummler, H. (1983). d,1- alpha- Tocopheryl acetate (vitamin E): A long term toxicity and carcinogenicity study in rats. International Journal for Vitamin and Nutrition Research, 53, 287–296.
WHO. (no date given). Vitamin E supplementation in pregnancy. [Online]. World Health Organisation. Vitamin E supplementation in pregnancy [Accessed 2 July 2026].
Woolley, D. W. (1945). Some biological effects produced by α- tocopherol quinone. Journal of Biological Chemistry, 159, 59–66. https:// doi. org/ 10. 1016/ S0021- 9258(19) 51301- 1
Yang, G., Wang, N., Liu, H., Si, L. and Zhao, Y., 2024. Cord blood vitamin E and lipids in infants born small for gestational age. European Journal of Pediatrics, 183(10), pp.4397-4402.
Yang, X., Dou, Y., Hu, L., Zhang, X., Pang, L., Jiang, Y., Lv, H., You, L., Lei, S., Ke, K. and Sun, T., 2025. Vitamin E supplementation and increased risk of gestational hypertension and preeclampsia in women undergoing assisted reproductive technologies. Chinese Medical Journal, 138(24), pp.3467-3478.
Yue, Q.Y. and Jansson, K., 2001. Herbal drug curbicin and anticoagulant effect with and without warfarin: possibly related to the vitamin E component. J Am Geriatr Soc, 49(6), p.838.
TOX/2026/25 Annex A
Literature search
The literature search parameters included papers published between 1st January 2024 to 14th May 2026.
The following terms were input into LitFetch (which is a tool that preforms key word searches on the PubMed, Scopus, Springer, and Ebsco (Food Science Source) and the relevant papers found as well as references therein were cited in this paper:
Vitamin E AND maternal health
preconception
conception
pregnancy
postnatal
fetus OR foetus
teratogen*
abortion
absorption
distribution
metabolism
excretion
toxicity
repro*
interactions
beta carotene
preeclampsia
cancer
TOX/2026/25 Annex B
Vitamin E supplement Information
1. Table 1 provides the summary of dosage information for vitamin E supplements (vitamin E only and multi-ingredient dietary supplements (MIDS)) listed in no particular order. Where the vitamin E content was provided on the packaging and/or website, calculations have been performed to estimate the maximum daily exposure to vitamin E from the supplement in mg per person per day. Depending on information on the product label, the maximum daily serving was calculated based on the assumption that the supplement is consumed at the maximum recommended daily intake.
2. A internet search was conducted using the term ‘bestselling Vitamin E supplements in the UK’ to perform market analysis of the commercially available vitamin E supplements on sale in the UK only. Table 2 provides the full list of vitamin E supplements (vitamin E only supplements and MIDS) with source information on supplement name, type, retailer, dose information, recommendation for use, composition, and additional information and warnings.
3. There are also a number of drinks available for sale which are marketed as beneficial to health because they are multivitamin drinks, metabolism boosting or similar which contain vitamin E. Some meal replacements drinks also contain vitamin E. These have not been included in the supplements section as they are not considered vitamin E or MIDS supplements. For additional information only, a summary of Vitamin E containing drinks with source information was provided in Table 3.
Table 1. Dosage information for vitamin E Supplements (Vitamin E only and MIDS), as sold in UK online retailers at the time of the assessment.
| Supplement name | Supplement type | Maximum recommended daily serving | Vitamin E content per unit (capsule/ tablet/ scoop etc) (mg) | Vitamin E intake from a daily serving (maximum serving size*) (mg) |
|---|---|---|---|---|
| Vitamin E 400iu Softgel Capsules | Capsules – Vitamin E only | 2 capsules | 268 | 536 |
| Holland and Barrett Vitamin E capsules | Capsules – Vitamin E only | 1 capsule | 268 | 268 |
| Boots Skin Formula Vitamin E | Capsules – Vitamin E only | 1 capsule | 268 | 268 |
| Cytoplan Vitamin E as tocopherols and tocotrienols | Capsules – Vitamin E only | 1 capsule | 300 | 300 |
| Bulk vitamin E softgels | Capsules – Vitamin E only | 1 capsule | 268 | 268 |
| NOW Foods, Vitamin E-Oil, Antioxidant Protection, 170 mg (253 IU) | Liquid – Vitamin E only | 8 drops (0.32ml) | 170 | 170 |
| Marney’s Vita Help Natural Vitamin E | Liquid – Vitamin E only | 0.5ml | 12 | 12 |
| Vitabiotics Pregnacare Him & Her Conception | Tablet - MIDS | 1 tablet | 4 | 4 |
| Vitabiotics Pregnacare Original | Tablet - MIDS | 1 tablet | 4 | 4 |
| Vitabiotics Pregnacare Max | Tablet - MIDS | 2 tablets | 2 | 4 |
| Vitabiotics Pregnacare Gummies | Gummies - MIDS | 2 gummies | 1.5 | 3 |
| Vitabiotics Pregnacare Liquid Pregnancy Vitamins | Liquid - MIDS | Two 5ml teaspoonfuls per day (10mls). | 2 (per 5ml) | 4 |
| Vitabiotics Wellwoman Multivitamin Gummies for Women | Gummies - MIDS | 3 gummies | 8 | 24 |
| Vitabiotics Wellwoman Original Multivitamin for Women | Capsule - MIDS | 1 capsule | 30 | 30 |
| Vitabiotics Wellwoman Plus | Tablet - MIDS | 1 tablet (micronutrient tablet) + 1 Omega 3-6-7 capsule | 30 (micronutrient tablet) + 6.6 (Omega 3-6-7 capsules) | 36.6 |
| Vitabiotics Wellwoman Max | Tablet - MIDS | 1 tablet | 20 | 20 |
| Centrum women | Tablet - MIDS | 1 tablet | 16 | 16 |
| Inessa advanced multivitamin | Tablet - MIDS | 1 tablet | 12 | 12 |
| Cytoplan women’s wholefood multivitamin capsules | Capsules - MIDS | 2 capsules | 15 | 30 |
| Seven Seas Omega-3 and multivitamins | Tablet - MIDS | 1 tablet | 18 | 18 |
| Boots a-z vitamins and minerals | Tablet - MIDS | 1 tablet | 12 | 12 |
| Purolabs multivitamin | Capsules- MIDS | 1 capsule | 25 | 25 |
| Nutravita multivitamins | Tablet - MIDS | 1 tablet | 12 | 12 |
| Swallow multivitamin | Tablets - MIDS | 2 tablets | 6 | 12 |
| Holland and Barrett Ultra woman | Caplet - MIDS | 1 caplet | 22 | 22 |
| Weightworld multivitamin and mineral | Tablet - MIDS | 1 tablet | 12 | 12 |
- Maximum serving assumes the maximum amount recommended on the packaging or website of the supplement. E.g. if recommended to take 1-2 capsules per day, this table assumes 2 capsules would be taken. Another example is if the website suggests a serving of 2 capsules a day, but the packaging suggests 3, then the highest suggestion has been used.
Table 2. Full list of vitamin E Supplements (vitamin E only supplements and MIDS) with source of information
| Supplement name | Website link/retailer | Supplement type | Recommendations for use | Dosage information | Composition | Additional information and warnings |
|---|---|---|---|---|---|---|
| Vitamin E 400iu Softgel Capsules | Vitamin E 400iu Softgel Capsules – Supplemented | Capsules – Vitamin E only | Take two capsules daily. Take one hour before bedtime as a food supplement or as directed by a healthcare professional. | 536 mg daily (268mg per capsule) | Vitamin E 400iu. (2680% RDA) dl-alpha-tocopherol, Soybean oil,Gelatin, Glycerine, Purified Water. | Not intended for persons under 18 years. If under medical supervision, taking medication, pregnant or lactating consult a doctor before. Packaging states 1 capsule, website states 2. |
| Holland and Barrett Vitamin E capsules | Holland & Barrett Vitamin E 400iu 30 Capsules H&B | Capsules– Vitamin E only | Take 1 capsule per day, preferably with a meal. Do not exceed stated dose. | 268 mg daily (268mg per capsule) | Vitamin E (DL-Alpha-Tocopherol Acetate), Capsule Shell (Gelatine), Humectant (Glycerol), Sunflower Seed Oil. | If you are pregnant, breastfeeding, taking any medications or under medical supervision, please consult a doctor or healthcare professional before use. Discontinue use and consult a doctor if adverse reactions occur. Keep out of sight and reach of young children. Do not use if seal under cap is broken or missing. |
| Boots Skin Formula Vitamin E | Boots Skin Formula Vitamin E, 90 Capsules | Capsules – Vitamin E only | Take 1 capsule a day with plenty of liquid. Do not exceed the daily dose. | 268 mg daily (268mg per capsule) | Vitamin E, tapioca starch, Glycerine | Suitable for adults and children aged 12 years and over. Not suitable for Vegetarians. Food Supplements are intended to supplement the diet and should not be regarded as a substitute for a balanced and varied diet or a healthy lifestyle. Not suitable for children under 12. Before taking this product, please consult your doctor or pharmacist if you are taking any medication, have any medical condition, are pregnant or breastfeeding. |
| Cytoplan Vitamin E as tocopherols and tocotrienol | Tocopherols & Tocotrienols Complex Vitamin E Cytoplan | Capsules – Vitamin E only | Take 1 capsule daily with food, or as recommended by a practitioner. | 300 mg daily (300mg per capsule) | Vitamin E (as mixed tocopherols and tocotrienols), anti-caking agent (microcrystalline cellulose, silicon dioxide), plant cellulose (capsule shell). | If you are taking any medications, consult your doctor before use. |
| Bulk vitamin E softgels | Vitamin E Softgels 400 IU Pure Vitamin E Bulk™ | Capsules – Vitamin E only | Take 1 softgel per day, with food. | 268 mg daily (268 per capsule) | Vitamin E (DL Alpha Tocopheryl Acetate), Softgel (Gelatin, Glycerine, Water). | Food supplements are not intended to replace a varied and balanced diet and a healthy lifestyle. Do not exceed the recommended usage. Keep out of reach of children. Although every care has been taken to keep product information up to date on our website, please always read the information provided on product label or packaging before use. The actual results of consuming dietary supplements may differ from those implied. Individuals may respond differently, and the suggested results presume appropriate nutrition and training plan. |
| NOW Foods, Vitamin E-Oil, Antioxidant Protection, 170 mg (253 IU) | NOW Foods, Vitamin E-Oil, Antioxidant Protection, 170 mg (253 IU), 1 fl oz (30 ml) | Liquid – Vitamin E only | Take 8 drops (0.32ml) daily with a meal. | 170 mg daily (170mg per 8 drop (0.32ml) serving) | Other ingredients: Organic extra virgin olive oil. Contains soy (vitamin E from non-GMO soy). Not manufactured with wheat, gluten, milk, egg, fish, shellfish, or tree nut ingredients. Produced in a GMP facility that processes other ingredients containing these allergens. | For adults only. Consult physician if pregnant/nursing, taking medication, or have a medical condition. Keep out of reach of children. |
| Marney’s Vita Help Natural Vitamin E | Liquid Vitamin E MARNYS | Liquid – Vitamin E only | Take 0.5ml a day, preferably in the morning. | 12 mg daily (12mg per 0.5ml serving) | Vitamin E in an extra virgin olive oil base. | Food supplements should not be used as a substitute for a balanced nutrition. It is recommended to keep a varied and balanced diet and healthy lifestyle. Do not exceed the recommended daily dose. |
| Keep away from children. Do not store at a temperature above 30ºC. | ||||||
| Vitabiotics Pregnacare Him & Her Conception | Pregnacare® Him & Her Conception Tablets By Vitabiotics | Tablet - MIDS | Women: one tablet per day, with your main meal (pink blister). Swallow with water or a cold drink. | 4 mg daily (4 mg per tablet) | Maltodextrin, Bulking Agent: Microcrystalline Cellulose, Vitamin C (Ascorbic Acid), Magnesium Oxide, L-Carnitine Tartrate, Inositol, Vitamin E (D-Alpha Tocopheryl Acid Succinate) (from Soya), Maca Extract, Zinc Sulphate, Tablet Coating (Hydroxypropylmethylcellulose, Glycerin, Colours [Iron Oxides]), Crosslinked Cellulose Gum, Pine Bark Extract, Anti-Caking Agents: Stearic Acid, Magnesium Stearate & Silicon Dioxide, Thiamine (Vitamin B1 as Mononitrate), Niacin (as Nicotinamide), Ferrous Fumarate, Citrus Bioflavonoids, Pantothenic Acid (as Calcium Salt), Vitamin B6 (Pyridoxine HCl), L-Arginine, Vitamin A (as Acetate, Antioxidants: DL-Alpha Tocopherol), Vitamin D3 (Cholecalciferol, Antioxidant: DL-Alpha Tocopherol), Siberian Ginseng Extract, Riboflavin, Octacosanol (Rice Bran), Copper Sulphate, L-Glutathione, Coenzyme Q10, Manganese Sulphate, Lycopene Extract, Folic Acid (as Pteroylmonoglutamic Acid), Sodium Selenate, Chromium Trichloride, Biotin, Vitamin B12 (Cyanocobalamin). | Not to be chewed. Do not exceed recommended intake. To be taken only on a full stomach. Not suitable for children. Pregnacare® Conception is a nutrient based, scientifically researched formula without any drugs or hormones. It contains no ingredients known to cause irregularity in the monthly cycle. Some women have reported a delay in their monthly cycle while using this product. If you experience a delay or change in your monthly cycle, this may not necessarily mean you are pregnant and it is advised to take a pregnancy test and speak to your doctor or health professional. |
| Vitabiotics Pregnacare Original | Pregnacare® Original Pregnancy Supplement Vitabiotics | Tablets - MIDS | Take one tablet per day with your main meal. Swallow with water or cold drink with main meal (to be taken with full stomach). | 4 mg daily (4 mg per tablet) | Maltodextrin, Magnesium Oxide, Bulking Agent: Microcrystalline Cellulose, Vitamin C (Ascorbic Acid), Ferrous Fumarate, Zinc Sulphate, Tablet Coating (Hydroxypropylmethylcellulose, Polydextrose, Medium Chain Triglycerides, Glycerin, Talc, Colours [Calcium Carbonate, Iron Oxides]), Anti-Caking Agents: Silicon Dioxide, Stearic Acid & Magnesium Stearate, Niacin (as Nicotinamide), Vitamin B6 (Pyridoxine HCl), Betacarotene, Pantothenic Acid (as Calcium Salt), Vitamin B12 (Cyanocobalamin), Vitamin E (D-Alpha Tocopheryl Acid Succinate) (from Soya), Vitamin D3 (Cholecalciferol), Thiamin (Vitamin B1 as Mononitrate), Riboflavin, Copper Sulphate, Vitamin K (Vitamin K1), Folic Acid (as Pteroylmonoglutamic Acid), Potassium Iodide, Biotin, Sodium Selenate. | Not to be chewed. Do not exceed recommended intake. You can take Pregnacare during all stages of your pregnancy. This comprehensive formula replaces other Pregnacare multivitamins. There is no need to take an additional multivitamin. |
| Vitabiotics Pregnacare Max | Pregnacare® Max Pregnancy Vitamins By Vitabiotics | Tablet - MIDS | Two (2) pregnacare® max tablets per day, plus one (1) omega-3 capsule per day, with your main meal. Swallow with water or cold drink with main meal (to be taken with full stomach). | 4 mg daily (4 mg per 2 tablets) | Calcium Carbonate, Magnesium Oxide, Maltodextrin, Bulking Agent: Microcrystalline Cellulose, L-Arginine, Vitamin C (Ascorbic Acid), Tablet Coating (Hydroxypropylmethylcellulose, Colours: [Calcium Carbonate, Iron Oxide Yellow & Copper Chlorophyllin (Natural Source)], Polydextrose, Medium Chain Triglycerides, Glycerin), Inositol, Anti-Caking Agents: Silicon Dioxide, Stearic Acid & Magnesium Stearate, N-Acetyl Cysteine, Ferrous Fumarate, Zinc Sulphate, Niacin (as Nicotinamide), Vitamin B6 (Pyridoxine HCl), Vitamin B12 (Cyanocobalamin), Betacarotene (Antioxidant: DL-Alpha Tocopherol), Thiamin (Vitamin B1 as Mononitrate), Pantothenic Acid (as Calcium Salt), Vitamin E (D-Alpha Tocopheryl Acid Succinate (from Soya), Vitamin D3 (Cholecalciferol, Antioxidant: DL-Alpha Tocopherol), Copper Sulphate, Riboflavin, Vitamin K (Vitamin K1), Manganese Sulphate, Folic Acid (as Pteroylmonoglutamic Acid & Calcium-L-Methylfolate), Potassium Iodide, Biotin, Sodium Selenate. | Not to be chewed. Do not exceed recommended intake. Pregnacare Max can be started at any point during pregnancy. This comprehensive formula replaces other Pregnacare® multivitamins. There is no need to take an additional multivitamin. |
| Vitabiotics Pregnacare Gummies | Pregnacare® Gummies Pregnancy Gummies Vitabiotics | Gummies - MIDS | Chew 2 gummies per day with your main meal. | 3 mg daily (3mg per two gummies) | Glucose Syrup, Granulated Sugar, Water, Gelling Agent (Pectins), Acidity Regulators (Citric Acid, Sodium Citrate), Suspending Agent (Vegetable Fat), Vitamin C (L-Ascorbic Acid), Medium Chain Triglycerides, Zinc Citrate, Purple Black Carrot & Apple Concentrate, Nicotinamide, Ferrous Fumarate, Natural Flavourings, Emulsifier (Sunflower Lecithin), Pantothenic Acid, Vitamin B12 (Cyanocobalamin), Sodium Selenite, Vitamin E (D Alpha Tocopherol), Beta-carotene, Vitamin B6 (Pyridoxine Hydrochloride), Vitamin B1 (as Thiamin Nitrate), Riboflavin, Vitamin K1, Vitamin D3 (as Cholecalciferol), Folic Acid (Pteroylmonoglutamic Acid), Biotin, Potassium Iodide, Glazing Agent (Modified Corn Starch). | Do not exceed the recommended intake. Pregnacare can be taken all stages of pregnancy. This comprehensive formula replaces other Pregnacare multivitamins. There is no need to take an additional multivitamin. |
| Vitabiotics Pregnacare Liquid Pregnancy Vitamins | Pregnacare® Liquid Pregnancy Vitamins Vitabiotics | Liquid - MIDS | Two 5ml teaspoonsful per day. One teaspoonful = approx. 5ml 5ml spoon included. Pregnacare Liquid should not be taken on an empty stomach. Ideally taken with a main meal. | 4 mg daily (4 mg per 10 ml serving) | Purified Water, Raw Cane Sugar, Sweetener: Maltitol Syrup, Magnesium Gluconate, Glycerin, Vitamin C (Ascorbic Acid), Ferrous Sulphate, Betacarotene (Vegetable Glycerin, Polysorbate 80, Vegetable Oil, Rosemary Extract, Antioxidant: Mixed Tocopherols), Zinc Gluconate, Acidity Regulators: Citric Acid & Sodium Hydroxide, Stabiliser: Xanthan Gum, Niacin (as Nicotinamide), Vitamin B6 (Pyridoxine HCl), Natural Flavouring: Orange Oil, Preservative: Potassium Sorbate, Pantothenic Acid (D-Panthenol), Vitamin E (DL-Alpha Tocopheryl Acetate), Thiamin (Vitamin B1 as Hydrochloride), Copper Sulphate, Riboflavin, Folic Acid (as Pteroylmonoglutamic Acid), Potassium Iodide, D-Biotin, Vitamin K, Sodium Selenate, Antioxidant: Butylated Hydroxyanisole, Vitamin D3 (Cholecalciferol), Vitamin B12 (Cyanocobalamin). | Pregnacare liquid should not be taken on an empty stomach. Ideally taken with a main meal. Do not exceed the recommended intake. Excessive consumption may produce laxative effects. You can take Pregnacare during all stages of your pregnancy. This comprehensive formula replaces other Pregnacare multivitamins. There is no need to take an additional multivitamin. |
| Vitabiotics Wellwoman Multivitamin Gummies for Women | Wellwoman® Multi - Vitamin Gummies For Women | Gummies - MIDS | Chew 3 gummies per day with your main meal. | 24 mg daily (24 mg per 3 gummies) | Wheat Glucose Syrup, Sugar, Fructooligosaccharides, Gelling Agent: Fruit Pectin, Vitamin and Nutrient Blend (Citrus Bioflavonoids, Niacin [as Nicotinamide], Ferric Pyrophosphate, Sodium Selenite, Zinc Citrate, Pantothenic Acid, Potassium Iodide, Vitamin D3 [Cholecalciferol (Vegan)], Vitamin B6 [as Pyridoxine HCl], Vitamin B1 [as Thiamin HCl], Riboflavin, Vitamin B12 [as Cyanocobalamin], Vitamin K [as Vitamin K1], Copper Citrate, Folic Acid, Chromium Picolinate, Biotin), Acidity Regulators: Citric Acid & Sodium Citrate, Vitamin C [Ascorbic Acid], Black Carrot Juice Concentrate, Vitamin E [as D-Alpha Tocopheryl Acetate], Starflower Oil, Evening Primrose Oil, Blueberry Flavouring, Strawberry Flavouring, Antioxidant: Mixed Tocopherols, Coating: Vegetable Oils (Coconut Oil, Rape Seed Oil), Glazing Agent (Carnauba Wax) and Antioxidant (Alpha Tocopherol), Betacarotene. | Do not exceed the recommended intake. This comprehensive formula replaces other Wellwoman multivitamins. There is no need to take an additional multivitamin. Not suitable for children. As this product contains vitamin K, if you are taking anticoagulants (blood thinners) do not take these gummies except on the advice of a doctor. Not to be taken on an empty stomach. This product contains iron, which if taken in excess, may be harmful to very young children. Food supplements must not replace a varied and balanced diet and a healthy lifestyle. As with other food supplements, consult your doctor or pharmacist before using if you are under medical supervision, pregnant, breast-feeding, have epilepsy, a thyroid condition, haemochromatosis, suffer from food allergies, or are allergic to any of the ingredients. |
| Vitabiotics Wellwoman Original Multivitamin for Women | [Wellwoman Original Multivitamin For Women Vitabiotics® (https://www.vitabiotics.com/products/wellwoman-original-tablets) | Capsules -MIDS | One capsule per day with your main meal. Not to be chewed. Swallow with water/cold drink. | 30 mg daily (30 mg per capsule) | Capsule Shell (Pharmaceutical Grade Gelatin [Halal Bovine Source], Glycerin, Colour [Iron Oxides], Orange Flavour), Soya Bean Oil (from Soya), Magnesium Oxide, Evening Primrose Oil, Starflower Oil, Vitamin C (Ascorbic Acid), Vitamin E (DL-Alpha Tocopheryl Acetate), Niacin (as Nicotinamide), Ferrous Fumarate, Zinc Sulphate, Para Amino Benzoic Acid, Lecithin (from Soya), Citrus Bioflavonoids, Thiamin (Vitamin B1 as Mononitrate), Flavouring: Natural Orange Oil, Vitamin B6 (as HCl), Pantothenic Acid (Calcium Salt), Manganese Sulphate, Betacarotene (Antioxidant: DL-Alpha Tocopherol), Riboflavin (Vitamin B2), Copper Sulphate, Thickener: Beeswax, Vitamin D3 (Cholecalciferol [Antioxidant: DL-Alpha Tocopherol]), Folic Acid (as Pteroylmonoglutamic Acid), Chromium Trichloride, Selenium (Sodium Selenite), Vitamin K, Biotin, Vitamin B12 (as Cyanocobalamin). | Do not exceed the recommended intake. To be taken on a full stomach. This comprehensive formula replaces other Wellwoman® multivitamins. There is no need to take an additional multivitamin. As with other food supplements, consult your doctor or pharmacist before using if you are under medical supervision, pregnant, breast-feeding, have epilepsy, haemochromatosis, suffer from food allergies, or are allergic to any of the ingredients. Not suitable for children. |
| Vitabiotics Wellwoman Plus | Wellwoman® Plus Omega 3-6-9 By Vitabiotics | Tablets - MIDS | One tablet (purple blister) plus one capsule (aqua blister) per day with your main meal. Not to be chewed. Swallow with water/cold drink. | 36.6 mg daily (30 mg per tablet; 6.6 mg per capsule) | Bulking Agents: Dibasic Calcium Phosphate & Microcrystalline Cellulose, Magnesium Oxide, Vitamin C (Ascorbic Acid), Tablet Coating: (Hydroxypropylmethylcellulose, Glycerin, Colours: Calcium Carbonate & Copper Chlorophyllin [Natural Source]), Vitamin E (D-Alpha Tocopheryl Acid Succinate) (from Soya), Ferrous Fumarate, Zinc Sulphate, Niacin (Nicotinamide), Hydroxypropylcellulose, Para Amino Benzoic Acid, Vitamin B12 (Cyanocobalamin), Citrus Bioflavonoids, Anti-Caking Agents: Stearic Acid, Silicon Dioxide & Magnesium Stearate, Thiamin (Vitamin B1 as Mononitrate), Vitamin B6 (Pyridoxine HCl), Betacarotene, Vitamin D3 (Cholecalciferol), Pantothenic Acid (as Calcium Salt), Polyvinylpyrrolidone, Riboflavin, Manganese Sulphate, Copper Sulphate, Vitamin K1 (Phytomenadione), Folic Acid (as Pteroylmonoglutamic Acid), Sodium Selenate, Chromium Trichloride, Biotin. | Do not exceed the recommended intake. To be taken on a full stomach. This comprehensive formula replaces other Wellwoman® multivitamins. There is no need to take an additional multivitamin. As with other food supplements, consult your doctor or pharmacist before using if you are under medical supervision, pregnant, breast-feeding, have epilepsy, haemochromatosis, suffer from food allergies, or are allergic to any of the ingredients. Not suitable for children |
| Vitabiotics Wellwoman Max | Wellwoman® Max Supplement For Women By Vitabiotics | Tablets - MIDS | Take with your main meal: one max tablet (purple blister), plus one omega 3-6-9 capsule (green blister), plus one calcium tablet (blue blister). Swallow each with water or a cold drink. | 20 daily (20 mg per tablet) | Bulking Agents: Microcrystalline Cellulose, Starch (Pregelatinised Maize Starch) & Potato Starch, Magnesium Oxide, Vitamin C (Ascorbic Acid), Tablet Coating (Hydroxypropylmethylcellulose, Polydextrose, Talc, Medium Chain Triglyceride, Colours [Iron Oxides & Calcium Carbonate]), L-Carnitine Tartrate, Niacin (as Nicotinamide), Ferrous Fumarate, Zinc Sulphate, L-Methionine, N-Acetyl Cysteine, Vitamin E (D Alpha Tocopheryl Acid Succinate) (from Soya), Anti-Caking Agents: Magnesium Stearate, Stearic Acid, Silicon Dioxide & Purified Talc, Polyvinylpolypyrrolidone, Guarana Extract, Thiamin (Vitamin B1 as Mononitrate), Citrus Bioflavonoids, Ethyl Cellulose, Vitamin B6 (Pyridoxine HCl), Betacarotene, Pantothenic Acid (as Calcium Salt), Vitamin D3 (Cholecalciferol), Manganese Sulphate, Vitamin B12 (Cyanocobalamin), Riboflavin, Green Tea Extract, Copper Sulphate, Vitamin K1 (Phytomenadione), Coenzyme Q10, Folic Acid (as Pteroylmonoglutamic Acid), Chromium Trichloride, Sodium Selenate, Potassium Iodide, Biotin | Not to be chewed. Do not exceed the recommended intake. To be taken on a full stomach. This comprehensive formula replaces other Wellwoman multivitamins. There is no need to take an additional multivitamin. As with other food supplements, consult your doctor or pharmacist before using if you are under medical supervision, pregnant, breast-feeding, have epilepsy, haemochromatosis, suffer from food allergies, or are allergic to any of the ingredients. Not suitable for children. |
| Centrum women | Centrum Women (60 Tablets) H&B | Tablets - MIDS | Take one tablet a day with water, preferably with food | 16 mg daily (16 mg per tablet) | Dicalcium phosphate; Calcium carbonate; Magnesium oxide; Bulking agents: E 460, E 464, E 1200; L-ascorbic acid; Anticaking agents: E 468, E 551, E 553b, E 470b; Ferrous fumarate; DL-alpha tocopheryl acetate; Nicotinamide; Calcium D-pantothenate; Zinc oxide; Pyridoxine hydrochloride; Riboflavin; Thiamine mononitrate; Vegetable oil (Coconut, Palm kernel); Beta-carotene; Cupric sulphate; Retinyl acetate; Pteroylmonoglutamic acid; Chromium III chloride; Sodium molybdate; Potassium iodide; Sodium selenate; D-biotin; Phylloquinone; Cholecalciferol; Cyanocobalamin; Colours: E 120, E 133. | Food Supplements are intended to supplement the diet and should not be regarded as a substitute for a balanced and varied diet or a healthy lifestyle. |
| Inessa advanced multivitamin | Inessa Advanced Multivitamin | Tablets - MIDS | Reach your daily nutrition goals with the world’s most comprehensive one-a-day multivitamin. | 12 mg daily (12 mg per tablet) | Plant fibre (Microcrystalline Cellulose), Vitamin C (Ascorbic Acid), Dicalcium Phosphate Dihydrate, Vitamin B1 (Thiamine HCl), Zinc Citrate, Vitamin K2, Co Enzyme Q10, Vitamin B5 (Calcium-D-Pantothenate), Vitamin B2 (Riboflavin), Vitamin B3 (Nicotinamide), Lutein, Inositol, Vitamin D3 (Cholecalciferol), Stearic Acid, Coating (Hydroxy Propyl Methyl Cellulose [plant fibre], Glycerol), Vitamin E (D-alpha Tocopherol Succinate), Vitamin B6 (Pyridoxal 5’ Phosphate), Beta-Carotene (Dunliella Salina), L-Methionine, Silicon Dioxide, Manganese Citrate, Boron (Di-Sodium Tetraborate), Vitamin A (Retinyl Acetate), Riboflavin 5 Phosphate, Chromium Polynicotinate, 5-Methyltetrahyrdrofolate, Methylcobalamine, D-Biotin, Potassium Iodide, Sodium Molybdate. | Not provided. |
| Cytoplan women’s wholefood multivitamin capsules | Women’s Wholefood Multi Award-Winning Multivitamin Capsules | Capsules - MIDS | 1 to 2 capsules daily. Take with food or as directed by a practitioner. | 30mg daily (30 mg per two capsules) | Broccoli powder (brassica oleracea), calcium ascorbate (providing vitamin C), magnesium (from citrate), chromium (from yeast), vitamin B5 (as calcium D-pantothenate), iron (as ferrous citrate), vitamin E (as d-alpha tocopherol succinate), spirulina powder (arthrospira platensis), carrot powder (daucus carota), zinc (from citrate), selenium (as selenomethionine), kelp extract (laminaria japonica) providing iodine, vitamin B1 (as thiamin hcl), vitamin B2 (as riboflavin), vitamin B3 (as nicotinamide), vegan D3 (cholecalciferol) preparation (mct oil, arabic gum, maltodextrin, ascorbic acid, d-alpha tocopherol, beta carotene (daucus carota), vitamin B6 (as P5P), acai berry (euterpe oleracea), acerola cherry extract (malpighia emarginata), copper (as glycinate), vitamin K2 (MK-7), boron (as sodium borate), manganese (as citrate), folic acid (as L-5-methyltetrahtdrofolate calcium), vitamin B12 (as methylcobalamin), molybdenum (as sodium molybdate), biotin, plant cellulose (capsule shell). | Do not exceed the recommended daily intake. This product should not be used as a substitute for a varied balance diet and lifestyle. |
| Seven Seas Omega-3 and Multivitamins | Omega-3 & Multivitamins Woman Duo Pack Seven Seas H&B | Tablets - MIDS | Adults (18+): Take one Vitamin and Mineral tablet (pink blister) and one Omega‑3 Fish Oil capsule (red blister) a day with a glass of cold water; take during or immediately after a meal. | 18 mg daily (18 mg per tablet) | Capsule: Fish Oil; Beef Gelatin; Humectant: Glycerol; Antioxidant: Tocopherol Tablet: Calcium carbonate; Bulking agent: Microcrystalline Cellulose; Magnesium oxide; L-ascorbic acid; Ferrous fumarate; Maltodextrin; Nicotinamide; Modified starch; DL-alpha-tocopheryl acetate; Riboflavin; Bulking agents: Dicalcium phosphate, Cross-linked sodium carboxymethylcellulose; Thiamine mononitrate; Zinc oxide; Calcium D-pantothenate; Glazing agents: Hydroxypropyl methyl cellulose, Talc; Pyridoxine hydrochloride; Anti-caking agents: Silicon dioxide, Magnesium salts of fatty acids, Fatty acids; Carrier: Acacia gum; Sugar; Starch; Glucose syrup; Manganese sulphate; Copper sulphate; Retinyl acetate; Pteroylmonoglutamic acid; D-biotin; Chromium chloride; Potassium iodide; Sodium selenite; Phytomenadione; Cyanocobalamin; Cholecalciferol | Do not exceed the recommended daily dose. Food supplements are not intended as a substitute for a varied and balanced diet and a healthy lifestyle. Contains iron, which, if taken in excess, may be harmful to very young children. Keep out of sight and reach of young children. If you are pregnant, intending to become pregnant, breastfeeding or postmenopausal, have any concerns or questions, are taking any other food supplements or medication, including warfarin or other blood thinning medicines, or have an existing health condition, please talk to your healthcare professional before taking this product. |
| Boots a-z Vitamins and minerals | Boots A-Z 180 Tablets (6 month supply) - Boots | Tablets - MIDS | Take 1 tablet a day with plenty of liquid. Do not exceed the daily dose. | 12 mg daily (12 mg per tablet) | Calcium Carbonate, Magnesium Oxide, Ascorbic Acid, Cellulose, Maltodextrin, Ferrous Fumarate, Dicalcium Phosphate, Vitamin E Acetate, Nicotinamide, Hydroxypropylmethylcellulose, Zinc Oxide, Cross-linked Sodium Carboxymethylcellulose, Silicon Dioxide, Magnesium Stearate, Calcium Pantothenate, Manganese Sulphate, Copper Sulphate, Pyridoxine Hydrochloride, Thiamine Mononitrate, Riboflavin, Vitamin A Acetate, Antioxidants (DL Alpha Tocopherol, Tartaric Acid, Sodium Ascorbate), Folic Acid, Potassium Iodide, Chromium Chloride, Sodium Molybdate, Sodium Selenite, Talc, Vitamin K1, Biotin, Vitamin D3 (Cholecalciferol), Methylcobalamin. | Suitable for Adults and children aged 12 years and over. Food Supplements are intended to supplement the diet and should not be regarded as a substitute for a balanced and varied diet or a healthy lifestyle. Keep out of sight and reach of children. In case of overdose seek medical attention. Before taking this product, please consult your doctor or pharmacist if you are taking any medication, or are taking warfarin or other blood thinning medications, have any medical condition, have diabetes, or are pregnant, trying to become pregnant or breastfeeding. |
| Purolabs multivitamin | Vegan Multivitamin Multivitamins Purolabs | Capsules - MIDS | Take1 capsule per day. Take consistently with water or food for the best results. | 25 mg daily (25 mg per capsule) | Vegetable Cellulose (HPMC), Magnesium Ascorbate, Brown Rice Flour, Nicotinamide (Niacin), Vitamin E Acetate, Calcium Carbonate DC (Contains Starch), Pantothenic Acid (D-Calcium Pantothenic), Magnesium Citrate, Choline Bitartrate, Zinc Citrate, L-Seleno Methionine (Selenium), Bamboo Silica, Rice Extract Blend, Pyridoxine Hydrochloride (Vitamin B6), Thiamine Hydrochloride (Vitamin B1), Olive Leaf Extract, Vitamin B2 (Riboflavin), Inositol, Para Aminobenzoic Acid (PABA), Ferrous Fumarate, Manganese Citrate, Sodium Tetraborate Anhydrous (Boron), Co-Enzyme Q10 Powder (Ubiquinone), Vitamin A Acetate (Contains Starch), Lutein (Contains Starch), Vitamin D2 (Ergocalciferol), Sodium Molybdate (Molybdenum), Cupric Sulphate (Copper), Chromium Picolinate, Bilberry Extract, Folic Acid, Biotin, Beta Carotene, Potassium Iodide, Vitamin B12 (Cyanocobalamin). | If you are taking medication or under medical supervision, please consult your healthcare practitioner before taking any food supplement. Store in a cool, dry place away from direct sunlight. Keep out of reach of children. Food supplements are not to be used as a substitute for a varied, balanced diet and healthy lifestyle. |
| Nutravita multivitamins | Multivitamin Minerals - Vegan & Vegetarian Multivitamins - Nutravita Nutravita | Tablets -MIDS | Take one tablet a day with a full glass of water preferably with breakfast. | 12 mg daily (12 mg per tablet) | Bulking Agents (Dicalcium Phosphate, Microcrystalline Cellulose), Magnesium Oxide, Calcium Carbonate (Maltodextrin), Vitamin C (Ascorbic Acid) (HydroxyPropylMethyl Cellulose), Potassium Chloride, Ferrous Fumarate, Vitamin E Acetate (Modified Food Starch, Silicon Dioxide), Vitamin B3 (Nicotinamide), Zinc Oxide, Glazing Agents (HydroxyPropyl MethylCellulose, Glycerin, Carnauba Wax) Vitamin A (Retinyl Palmitate) (Maltodextrin, Arabix Gum, Corn Starch, Vegetable Oil, Tocopherol), Anti-Caking Agents (Magnesium Stearate, Silicon Dioxide), Vitamin B5 (D-Calcium Pantothenate), Manganese Sulphate, Sodium Selenite (Microcrystalline Cellulose), Copper Sulphate, Vitamin B12 (Cyanocobalamin) (Maltodextrin), Vitamin B6 (Pyridoxine Hydrochloride), Vitamin K1 ( Maltodextrin), Vitamin B2 (Riboflavin), Vitamin B1 (Thiamine Hydrochloride), Chromium Picolinate, Folic Acid, Potassium Iodide, Sodium Molybdate, Vitamin D (Cholecalciferol) ( Maltodextrin, Sugar, Ascorbyl Palmitate), Biotin | Food supplements must not be used as a substitute for a varied and balanced diet and a healthy lifestyle. If you are pregnant, breastfeeding, taking any medications or under medical supervision, please consult a doctor or healthcare professional before use. |
| Swallow multivitamin | Daily Multivitamin Tablets for Women and Men - High Dose – The Swallow Co | Tablets - MIDS | Take 2 tablets a day, with a drink or food. Ideally, take one in the morning and one in the evening. Do not exceed the stated dose. | 12 mg daily (12 mgs per 2 tablets) | Magnesium Bisglycinate, Dicalcium Phosphate, Vitamin-C (PureWay-C®), Iron (Ferrous Bisglycinate), Coenzyme Q10 (Ubiquinone), Glazing Agent (HydroxyPropylMethylCellulose, Glycerol), Zinc Citrate, Rice Extract Blend, Nicotinamide, Vitamin E (D-Alpha Tocopheryl Succinate), Bulking Agent (Microcrystalline Cellulose), Thiamine Hydrochloride, Manganese Bisglycinate, L-Selenomethionine, Retinol Acetate, Calcium Pantothenate, Lutein Ester, Copper Gluconate, Vitamin K2 MK7, Vitamin B6 (Pyridoxal 5-Phosphate), Vitamin D3 (from Algae), Riboflavin 5-Phosphate Sodium (R5P), Chromium Picolinate, L-5-Methyletetrahydrofolate MTHF, Potassium Iodide, D-Biotin, Methylcobalamin (methylated Vitamin B12). | If you are pregnant, breastfeeding, taking medication or due for surgery it is advisable to consult a GP prior to taking any supplements. Not intended for use by persons under the age of 18 years old |
| Holland and Barrett Ultra woman | Holland & Barrett Ultra Woman Tablets 3 Months Supply Bundle H&B | Caplets - MIDS | Take one caplet daily, preferably with a meal. Do not exceed stated dose. | 22mg daily (22mg per caplet) | Calcium Carbonate, Bulking Agent (Microcrystalline Cellulose), Magnesium Oxide, Potassium Chloride, Vitamin C (as Ascorbic Acid), Dicalcium Phosphate, Iron Fumarate, Citrus Sinensis Extract, Glazing Agents (Hydroxypropylmethyl Cellulose, Glycerine, Hydroxypropyl Cellulose), Vitamin E (as d-Alpha Tocopheryl Acid Succinate), Emulsifiers (Cross-linked Sodium Carboxymethylcellulose, Sodium Carboxymethylcellulose), Beta-Carotene, Anti-Caking Agents (Magnesium Stearate, Silicon Dioxide), Manganese Gluconate, Pantothenic Acid (as d-Calcium Pantothenate), Niacin (as Nicotinamide), Copper Gluconate, Zinc Oxide, Vitamin D3 (as Cholecalciferol), Vitamin B6 (as Pyridoxine Hydrochloride), Vitamin B12 (as Cyanocobalamin), Pomegranate Extract, Vitamin B1 (as Thiamin Mononitrate), Vitamin B2 (as Riboflavin), Chromium Picolinate, Grapeseed Extract, Cranberry Extract, Flaxseed Powder, Sodium Borate, Bilberry Fruit Extract, Vitamin K1 (as Phylloquinone), Folic Acid (as Pteroylmonoglutamic Acid), Sodium Selenite, Potassium Iodide, Sodium Molybdate, Biotin (as d-Biotin), Lycopene, Lutein, Zeaxanthin, Coenzyme Q10 (as Ubiquinine). | Food supplements must not be used as a substitute for a varied and balanced diet and a healthy lifestyle. If you are pregnant, breastfeeding, taking any medications or under medical supervision, please consult a doctor or healthcare professional before use. |
| WeightWorld Multivitamin and Mineral | Multivitamin and Mineral Tablets 400 Tablets WeightWorld | Tablets - MIDS | Take 1 tablet daily with a full glass of water, preferably with a main meal. You can take the tablet during the day, at noon or at night, whatever you prefer. For optimal results, it is recommended that you take the tablet at approximately the same time every day. | 12mg daily (12 mg per tablet) | Vitamin C (as L-Ascorbic acid), Magnesium (as magnesium oxide), potassium (as Potassium Chloride), Vitamin E (as DL-Alpha Tocopherol Acetate), Vitamin B3 (as Nicotinamide), Iron (as Ferrous Fumarate), Zinc (as Zinc Citrate), Calcium (as Calcium Carbonate), Vitamin B5 (as Pantothenic Acid), Manganese (as Manganese Citrate), Vitamin B2 (as Riboflavin), Vitamin B6 (as Pyridoxine Hydrochloride), Vitamin B1 (as Thiamin Mononitrate), Copper (as Copper Gluconate), Vitamin A (as Retinyl Acetate), Selenium (as L-Selenomethionine), Sodium (as Sodium Chloride), Vitamin B9 (as Folic Acid), Iodine (as Potassium Iodide), Vitamin B12 (as Cyanocobalamin), Vitamin B7 (as D-Biotin), Chromium (as Chromium Chloride), Boron (as Boric Acid), Cholin (as Cholin Bitartrate), Molybdenum (as Sodium Molybdate), Vitamin D3 (as Cholecalciferol), Vitamin K2 MK7 (as Menoquinone). | Do not exceed the recommended daily dose. Food supplements must not be used as a substitute for a varied and balanced diet and a healthy lifestyle. If you are pregnant, breastfeeding, taking any medications or are under medical supervision, please consult a healthcare professional before use. Discontinue use if any adverse reactions occur. Not intended for use by persons under the age of 18. |
Table 3: Summary of drinks products marketed as meal replacements and/ or beneficial to health which contain vitamin E with source information
| Product | Website/ retailer | Product type | Recommendations for use | Vitamin E content | Composition | Additional information and warnings |
|---|---|---|---|---|---|---|
| Huel Ready-to-drink On-the-go complete meal | Huel Ready-to-drink On-the-go complete meal | Drink – meal replacement shake. | Each bottle contains one portion and is considered a meal replacement. | 3.0-3.2 mg (highest, banana flavour) | Varied based on flavour, example: Water, Pea protein, Tapioca starch, gluten-free oat flour, rapeseed oil, cocoa powder (1.5%), ground flaxseed, soluble vegetable fibre (chicory, corm), medium-chain triglyceride powder (from coconut), micronutrient blend (Minerals: potassium, chloride, calcium, magnesium, phosphorus, copper, zinc, iodine, chromium; Vitamins:C, K, E, A, Niacin, D, B12, Pantothenic acid, biotin, B6, B2, B1, folate; Cholin), natural flavourings, brown rice flour, coconut sugar, sunflower lecithin, gellan gum, sea salt, sucralose | We recommend one serving a day if you are pregnant or breastfeeding. |
| Verve Transparent Greens V80 Powder | V80 Greens Powder from Verve - Boost Your Nutrition | Drink – powder. | Add one heaped 10g scoop to 300ml of water, shake and enjoy. Best taken in the morning on an empty stomach. | 12 mg per 10g serving | Spirula, Pea protein, sugar beet oligofructose soluble fibre powder, kiwi pear powder, barley grass, chlorella, wheat grass, alfalfa, potassium phosphate, flaxseed extract, broccoli powder, inulin, bamboo extract, calcium (as calcium citrate), strawberry. | Not provided. |
| Vitamin Well vitamin drinks | Vitamin Well Vitamin Drinks 12x500ml Protein Package | Drink – flavoured soft drink. | Not provided. | 6 – 7.2 mg per 500ml bottle (depends on type/ flavour) | Water, Fructose, Acidity Regulators (Citric Acid, Calcium Carbonate), Vitamins (Vitamin D3, Vitamin E, Niacin, Folic Acid, Vitamin B12, Biotin, Pantothenic Acid), Minerals (Magnesium, Zinc, Selenium), Flavouring. | Not provided. |
| Dr Witt Premium Metabolism Green Multivitamin Drink | Dr Witt Premium Metabolism Green Multivitamin Drink 1 Food Plus Shop online | Drink – flavoured soft drink. | Not provided. | 1.8 mg (assumed to be per L bottle) | water, apple juice from apple juice concentrate 20%, sugar, juices from juice concentrates: lime juice from juice concentrate 0,1%, pineapple juice from concentrated juice 0,1%, grape juice from juice concentrate 0,1%, kiwi juice from juice concentrate 0,05%, acidity regulators: citric acid and sodium citrates, stabilisers: guar gum and xanthan gum, colourings – carotenes, copper complexes of chlorophylls and chlorophyllin, flavourings, zinc, Vitamins: E, C, niacin, B6, folic acid, B12, biotin, pantothenic acid, sweetener – sucralose | Not provided. |
| Beverages, fortified, Acai berry drink | Beverages, fortified, Acai berry drink nutrition facts and analysis. | Drink – flavoured soft drink. | Not provided. | 29.55 mg | Not provided. |