Risk of severe harm from use of incorrect giving (administration) set for blood transfusion (DSI/2026/003)
There is a potential for serious harm to patients if an intravenous (IV) infusion giving set is used instead of a blood transfusion giving set to deliver a transfusion of blood or blood components.
Summary
There is a potential for serious harm to patients if an intravenous (IV) infusion giving set is used instead of a blood transfusion giving set to deliver a transfusion of blood or blood components (see Annex 1). Use of an IV infusion giving set instead of a blood transfusion giving set may result in under-infusion of blood or destruction of red blood cells (haemolysis) which can lead to serious patient injury.
Advice for Healthcare Professionals:
Advice for coordinators:
- ensure staff who may carry out IV therapy and transfusions and non-clinical staff who handle the sets can identify the differences between IV infusion and blood transfusion giving sets
- ensure blood transfusion giving sets are stored in clearly labelled containers, in their original packaging, separate from IV infusion giving sets to prevent selection of the wrong type
Advice for individual healthcare professionals:
- always use a blood transfusion giving set for a blood transfusion
- be aware that using an IV infusion giving set for a blood transfusion can result in under-infusion of blood or haemolysis with potentially serious consequences for the patient
How to identify a blood transfusion giving set:
![]()
- blood transfusion giving sets (see image 1) contain a large filter (pore size ~170-200 µm). This is to allow larger blood components to pass through. Note: some blood transfusion giving sets have 2 chambers, see annex 2 for examples.
- IV infusion giving sets (see image 2) contain a very small filter (pore size ~15 µm) to remove particulate matter
- if you cannot see a filter, check the packaging to ensure that you are using the correct type of set
- the packaging of a blood transfusion giving set should include the following:
- an indication that the product is for blood transfusion
- filter size ~170-200µm (whereas for an IV infusion it is ~15µm). The size of filter may be denoted using the below graphic

- be aware that manufacturers have not all used the same colour coding for packaging and giving set components to denote between sets for IV infusion and sets for blood transfusion. It is important users check that they have selected the correct set prior to use
Before starting a transfusion of blood or blood components:
- check that you are using a blood transfusion giving set
- check that the pump settings (if used) are correct
- a pre-transfusion checklist such as the Serious Hazards of Transfusion (SHOT) Transfusion checklist should be completed prior to starting a transfusion as recommended in 2017 through CAS alert CEM/COM/2017/005
Advice for Healthcare Professionals to Provide to Patients:
- Serious Hazards of Transfusion (SHOT) have developed resources for patients including the My Transfusion app which provides useful information for patients who are likely to receive a blood transfusion
Explanation of identified safety issue
Choice of giving set is important because IV infusion and blood transfusion sets use different filters.
- An IV infusion giving set has a small ~15 μm pore size filter to trap any particulate matter so that it is not infused
- A blood transfusion giving set has a much larger ~170-200 μm pore size filter to remove clots and particulate matter but allow larger blood components such as red blood cells and platelets to pass
If an IV infusion giving set is used instead of a blood transfusion giving set, blood can be restricted by the smaller pore size in the filter which will reduce the transfusion rate. This can cause under-infusion of blood within the desired time and may cause serious harm to the patient.
Use of the incorrect giving set for a blood transfusion can also result in mechanical damage to red blood cells resulting in haemolysis.
Harm associated with identified safety issue
The MHRA has been made aware of a case in which an incorrect giving set was used for a blood transfusion, which contributed to severe brain damage to a baby.
The baby underwent an exchange blood transfusion, where blood is removed from a person and replaced within a short timeframe with donor blood or blood components, to treat jaundice. Instead of a blood transfusion giving set, an IV infusion giving set was used with a volumetric pump to deliver replacement blood. Due to the incorrect choice of giving set, the pump did not deliver the required volume of blood at the required speed, leading to blood being removed faster than it could be replaced.
The baby suffered a cardiac arrest, potentially due to hypovolaemia, as a result of inadequate blood volume replacement, and was later diagnosed with severe brain injury.
This case was investigated by the Maternity and Newborn Safety Investigations programme, and has been the subject of a Safety Spotlight publication. The British Association of Perinatal Medicine have also published an alert on this issue, with additional recommendations for safe practice in neonatal blood transfusions.
The risk is greatest for neonates being treated with blood transfusions due to the small volumes involved. Serious Hazards of Transfusion (SHOT) have highlighted neonatal exchange transfusion as being an area of concern including in the 2024 paediatric chapter.
Annual reports published by SHOT indicate that there are between 20 and 30 events involving use of the incorrect type of giving set to administer blood transfusions reported each year. Although the evidence available suggests that harm is rare, this case highlights the potential for significant harm.
This error in choice of set can impact any brand of giving set. However, the potential for this error may be greater when a site uses both blood transfusion and IV infusion giving sets supplied under the same brand (for example, for use with a specific infusion pump), as these can have similar branded packaging.
SHOT have published a suite of guidance for healthcare professionals to raise awareness of the issue and provide guidance on how to minimise the risk.
Actions being taken by industry
The MHRA is committed to working with manufacturers to improve the usability of these products to help users make the correct choice when selecting a giving set. Examples of products currently on the market can be found in Annex 2.
Updates include:
- changes to the packaging of blood transfusion giving sets to easily differentiate from IV infusion giving sets
- addition of colour coded clamps to the line of blood transfusion giving sets to differentiate from IV infusion giving sets. Be aware that not all manufacturers have followed the same colour coding system. Users should always check the packaging and labelling prior to use
Work is ongoing with infusion pump manufacturers around the potential for automatic recognition and alert if the type of giving set selected is incorrect for the intended type of infusion.
Reporting advice
Healthcare professionals should report incidents involving medical devices:
- in England and Wales to the Yellow Card website or via the Yellow Card app
- in Scotland to Incident Reporting & Investigation Centre (IRIC) and their local incident recording system
- in Northern Ireland to the Yellow Card website in accordance with your organisation’s medical device policies and procedures
Healthcare professionals should also report incidents involving blood and blood components to Serious Hazards of Transfusion (SHOT) via the SABRE portal.
Download Document
Annex
Annex 1
-
In this document, ‘blood’ and ‘blood components’ refers to red cells, platelets, fresh frozen plasma (FFP), granulocytes and cryoprecipitate
- In this document, ‘IV infusion giving set’ is synonymous with the following:
- Fluid administration set, IV solution administration set, IV solution giving set, General purpose administration set, General purpose giving set, Standard giving set
- In this document, the term ‘blood transfusion giving set’ is synonymous with:
- Blood set, Blood giving set, Blood administration set, Blood transfusion administration set, Transfusion set, Transfusion administration set, Transfusion giving set, Transfusion specific set
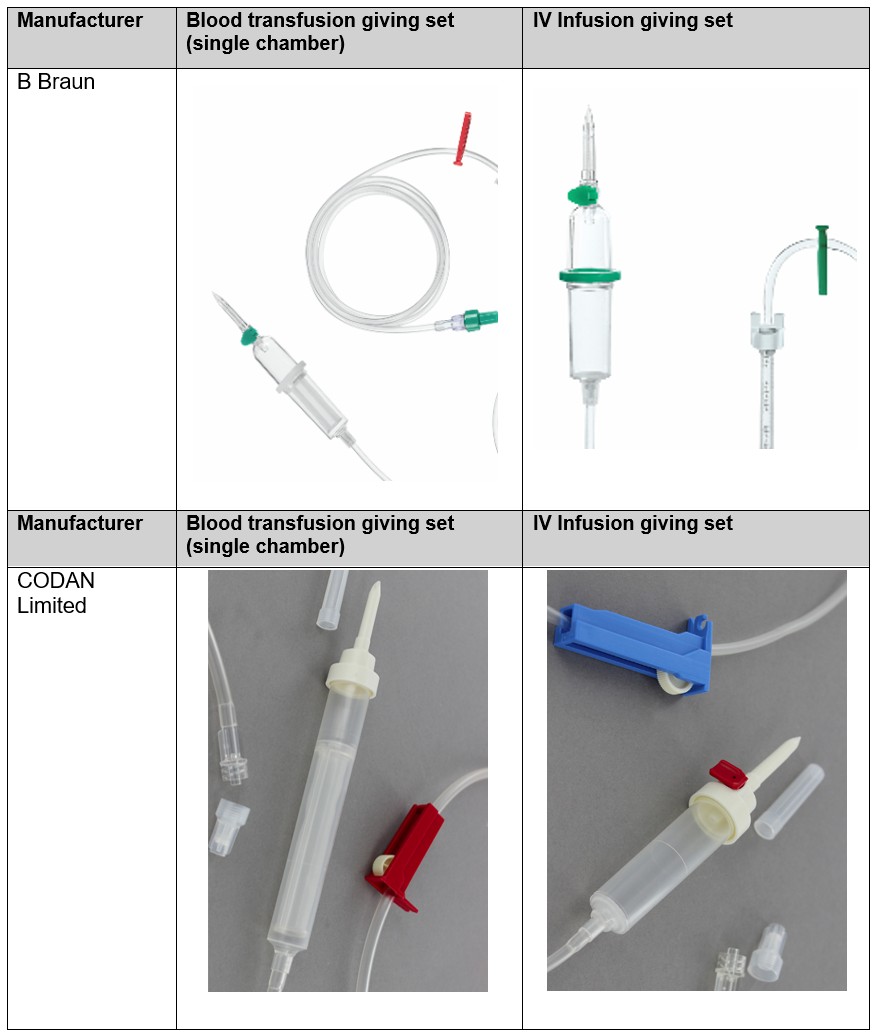
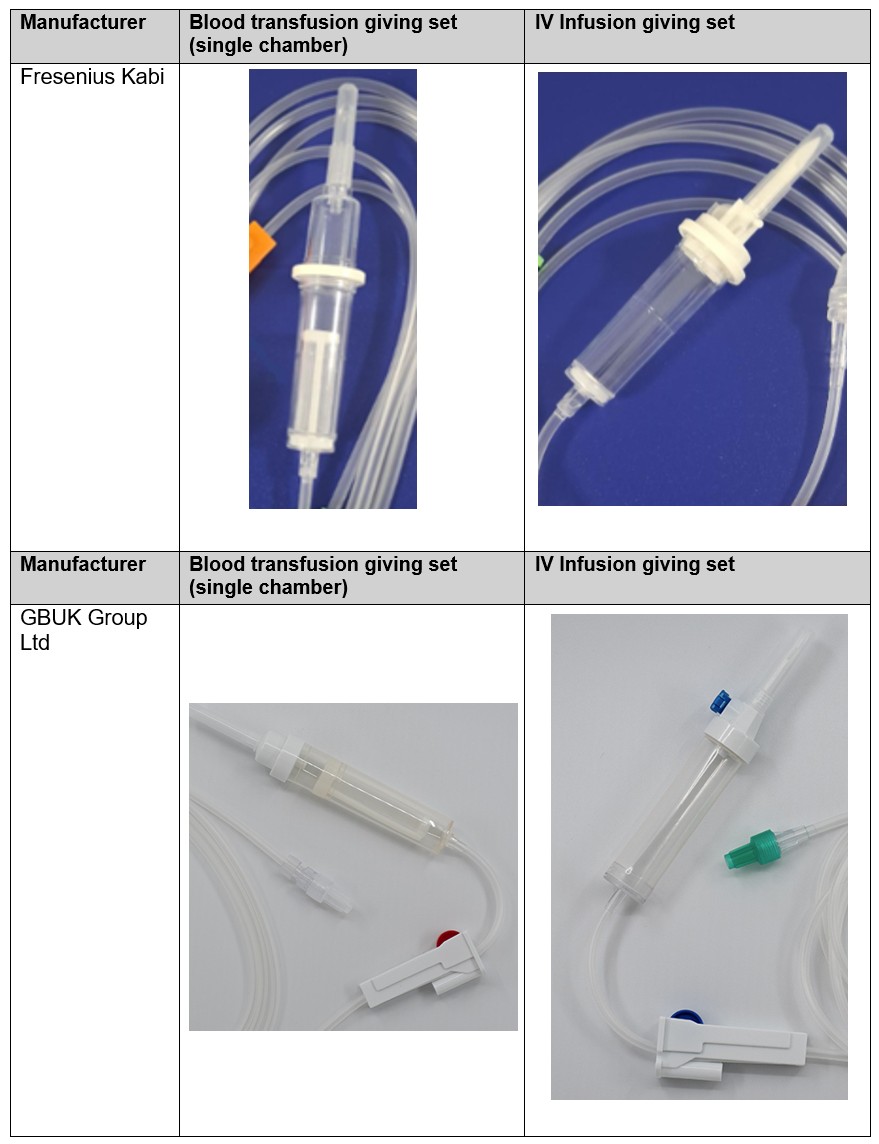
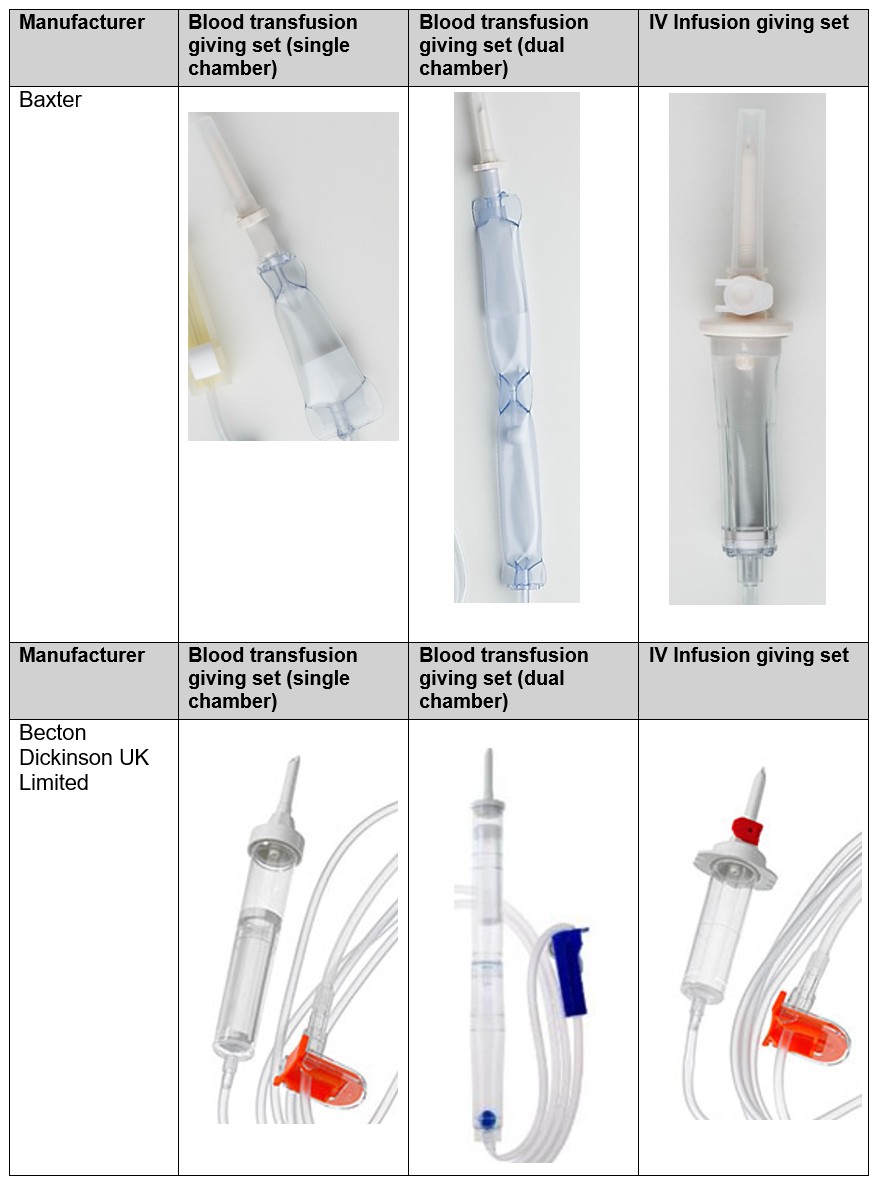
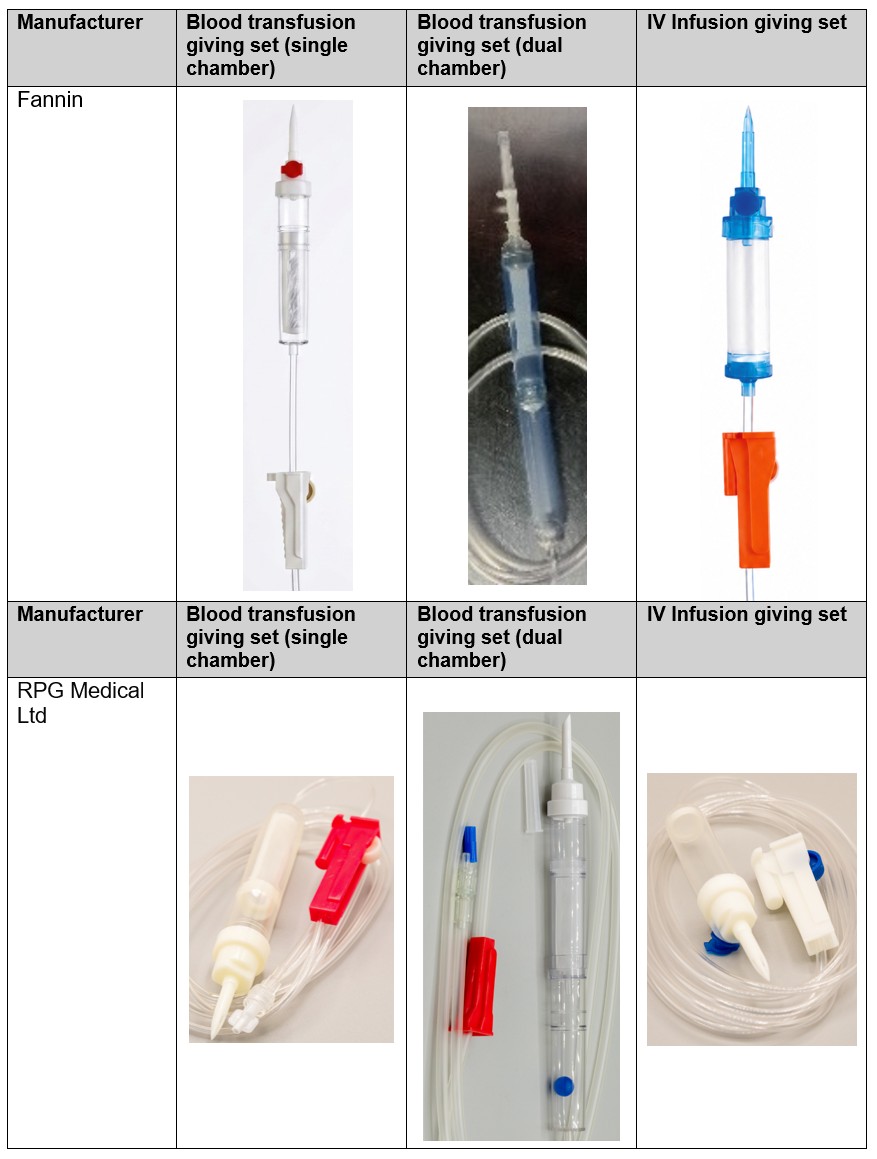
Annex 2
Examples of products currently on the market can be found below for information (not an exhaustive list). Note the difference in size between the filters in each case. Where there is no photo provided, there are no devices fitting this description in the current product portfolio.
Additional information
You can sign up to receive email updates on alerts and device safety information from the MHRA.
You can sign up to receive our monthly roundup of safety communications.
For any enquiries, please contact info@mhra.gov.uk
Stakeholder engagement:
- Maternity and Newborn Safety Investigations (MNSI) programme
- Serious Hazards of Transfusion (SHOT)
- NHS England Patient Safety Team
- Incident Reporting & Investigation Centre (IRIC) for Scotland
- NHS Wales
- Department of Health (NI)
- B Braun
- Baxter
- Becton Dickinson UK Limited
- CODAN
- Fannin
- GBUK Group Ltd
- RPG Medical Ltd