Exploring loneliness stigma through qualitative interviews and focus groups
Published 12 June 2023

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/research-exploring-the-stigma-associated-with-loneliness/exploring-loneliness-stigma-through-qualitative-interviews-and-focus-groups
Executive summary
Overview of the research
This report presents the findings from a qualitative study exploring loneliness stigma. Previous research has highlighted that both self- and social stigma can present barriers to sharing and overcoming feelings of loneliness. For the purpose of this research, loneliness and stigma are defined as follows:[1]
-
Loneliness: “A subjective, unwelcome feeling of lack or loss of companionship. It happens when we have a mismatch between the quantity and quality of social relationships that we have, and those that we want.”[2]
-
Social stigma: Negative attitudes or beliefs towards an individual or group, based on experiences or characteristics which are seen to distinguish them from other people (in this case, experiences of loneliness). This results in the person or group being devalued and/or suffering discrimination.[3],[4] This research explores actual and perceived social stigma.
-
Self-stigma: Feeling shame around a personal characteristic or experience and being inclined to conceal it from others. [5]
-
Stigma: Covers both social and self-stigma.
The Department for Culture, Media and Sport (DCMS) commissioned this study to explore loneliness stigma and address evidence gaps identified in reviews of the literature. The Tackling Loneliness evidence review (published on 26th January 2022) critically examined the existing literature on loneliness, identifying that little was known about loneliness stigma. The Loneliness Stigma evidence review was subsequently commissioned to explore existing research on loneliness stigma. This review identified specific evidence gaps around how loneliness stigma is experienced and how it can be tackled, subsequently recommending further qualitative research to explore the drivers of loneliness stigma across different population groups, along with how interventions could effectively tackle such stigma.
This research aimed to explore:
-
Understandings and expressions of loneliness.
-
Barriers that prevent people from taking actions to overcome their loneliness.
-
The experience of loneliness stigma, and strategies for reducing this stigma.
-
How these issues are experienced across different population groups.
The report draws on findings from:
-
Six interviews with professionals with experience tackling loneliness stigma (“stakeholders”).
-
Forty in-depth interviews and diaries completed by participants experiencing loneliness regularly (“interviewees”). These participants were recruited based on their age/life stage (young adults (age 16-30); parents of young children (age 27-35); middle-aged (age 40-60); retired people age 65+).
-
Three focus groups with participants with little or no recent experience of loneliness (“focus group participants”) to explore wider societal understandings of loneliness. Each focus group contained participants from one age group (16-34; 35-64; 65+).
Key findings
Understandings and expressions of loneliness
As detailed in the Government definition of loneliness above, this research found that experiences of loneliness are related to negative feelings about quantity (i.e., number) and/or quality of social connections. Spending time alone could drive feelings of loneliness for interviewees, regardless of the number of social connections they had. For those with a higher quantity of day-to-day connections, experiences of loneliness were also driven by negative feelings about the quality of their connections. This included feeling disconnected from others and/or wanting specific additional connections, such as a romantic partner.
The Government definition gives equal weight to experiences of loneliness which are driven by negative feelings about quantity or quality of social connections. However, there was a view presented by some interviewees and focus group participants that more “serious” loneliness relates to the quantity of connection and is experienced by people who are socially isolated. This view was contested by other interviewees and focus group participants, with some interviewees highlighting that their most difficult experiences of loneliness were driven by feelings of disconnection (i.e., quality of connection). Interviewees attributed their feelings of loneliness to a variety of life experiences, including health conditions, life events and commitments (e.g., parenthood). These experiences caused physical and emotional barriers to connecting with others. A common view across the interviews and focus groups (i.e., those with regular and little/no recent experience of loneliness) was that everyone is likely to experience some form of loneliness at some point in their lives. However, some interviewees felt that loneliness within certain population groups was harder for society to understand. For example, both young people and new parents felt that their experiences were dismissed (or not recognised at all) due to assumptions that their needs for social connection were met by those around them. While focus group participants perceived that loneliness could be experienced at any age, one perspective (raised across all three groups) was that older people might experience a more severe form of loneliness due to having fewer opportunities for connection.
Interviewees had mixed perspectives on whether their experiences of loneliness were driven by circumstance, their actions and/or the actions of others. Where interviewees linked their loneliness to their own actions, this tended to be driven by feelings that they should be doing more to seek out and develop connection with others. When discussing the causes of loneliness in others (i.e., outside personal experiences), both interviewees and focus group participants demonstrated consideration and sympathy. However, some of these participants attributed loneliness in others to internal causes (e.g., lack of confidence) or felt that others could do more to control or overcome their experience.
Barriers to managing and overcoming loneliness
Interviewees felt that sharing feelings of loneliness helped them feel less alone and more able to manage their experience. However, some interviewees had little experience of talking about how they felt. Barriers that made it more difficult to share feelings of loneliness included:
-
Past responses to sharing feelings of loneliness. These responses included limited experiences of negative reactions (e.g., experiences being dismissed and assumptions of blame) and wider responses that interviewees considered unhelpful (e.g., offering unwanted advice or attempts at distraction).
-
Fear of how others might react. Interviewees also refrained from sharing experiences due to concerns about being judged, pitied or perceived differently. While some interviewees had negative experiences of sharing their feelings, others felt these fears stemmed from their own assumptions or internal thought processes (e.g., anxiety).
-
Fear of burdening others. This fear was experienced across all interviewee groups, but specifically applied to those who identified some form of care and support responsibility (e.g., for family or friends). In some cases, this fear was driven by cultural or gender stereotypes around caring.
-
Lack of opportunity or means to discuss loneliness. While some interviewees described themselves as “private” or struggled to express their feelings, there was also a more general sentiment that there is a lack of language around loneliness. This perspective was echoed by some focus group participants (not experiencing loneliness), who lacked the language and tools to discuss loneliness with people experiencing it and help identify solutions.
Interviewees also identified wider actions which they had taken to overcome loneliness, including joining groups and learning to enjoy time alone - this included taking steps to do enjoyable activities alone (e.g., hobbies or holidays). There were a number of barriers to taking these actions – which often overlapped with causes of loneliness – including lack of time, financial and emotional barriers to connection and accessibility concerns.
Loneliness stigma
The findings in this report demonstrate perceived social stigma and self-stigma, with some (limited) evidence of actual social stigma.
-
Exploring actual social stigma involved examining attitudes towards those who experience loneliness, to understand the extent of negative perceptions. This report has paid particular attention to whether opinions ascribe blame to those who feel lonely, as this emerged as a driving factor of social stigma in the Loneliness Stigma evidence review. Some interviewees had experienced negative responses when sharing feelings of loneliness. In some cases, these responses could be considered stigmatising (in line with the definitions used in this research), for instance where jokes were made, or responses assumed blame. However, many responses interviewees considered unhelpful (e.g., “glossing over” their feelings) were not necessarily suggestive of negative beliefs around loneliness. Some focus group participants and interviewees perceived that loneliness in others could be caused by individual traits and actions, such as low confidence and self-isolation. However, only in some cases did these opinions lead to responsibility being ascribed to those experiencing loneliness. Generally, these opinions were presented with sensitivity and understanding (e.g., an understanding that some people may self-isolate due to health issues). Both interviewees and focus group participants were open to reflecting on their views and proactively questioned some of the more “stereotypical” views that they presented (e.g., loneliness being common among older people).
-
Exploring perceived social stigma involved examining whether people who feel lonely perceive that others hold negative opinions about loneliness. This was considered separately to experiences of actual social stigma (see above). There was a perception of social stigma among interviewees. This included perceptions that loneliness is seen as a weakness and those who feel lonely are seen as “odd”, “sad” or blamed for their experience. While participants tended to believe that everyone experiences loneliness, some interviewees felt that the stigma they perceived was driven by a societal lack of understanding about who experiences loneliness and what causes it.
-
Exploring self-stigma involved considering whether people experiencing loneliness felt embarrassment or shame around their experience and were inclined to conceal their feelings. While some interviewees had shared feelings of loneliness, others did conceal their experiences due to embarrassment or shame. These feelings were driven by factors such as self-blame or feeling that they “shouldn’t” be lonely. As well as having concerns about what others might think, interviewees worried that sharing would impact how they felt about themselves. This included worries about feeling “needy” or vulnerable. While some fears appeared to be driven by experiences or perceptions of social stigma (rather than actual social stigma), other participants felt that their concerns were driven by internal thought processes (e.g., internal anxiety about how they presented themselves to others).
Recommendations to tackle loneliness stigma
This research indicates that the following actions would help reduce social stigma (perceived and actual) and self-stigma around loneliness:
-
Use of national campaigns to normalise loneliness. It was suggested that promoting loneliness as a normal and universal emotion would help those experiencing it to feel part of the majority, rather than the minority (thereby reducing self-stigma). It is recommended that campaign design considers the following:
-
Recognising a diverse range of experiences of loneliness. As well as ensuring that all campaign imagery is inclusive and diverse, stakeholders suggested focusing on the variety of drivers of loneliness, including life events and/or circumstances, such as parenthood, health and employment changes.
-
Reframing loneliness to remove some of the negative connotations. Given the findings in this report, it may also be helpful for campaigns to consider messaging which targets blame around loneliness or fears of being burdensome to address both self- and (perceived and actual) social stigma.
-
Making campaigns accessible to different population groups. Tailoring campaign messaging to different target population groups was proposed to ensure that messaging is accessible and relevant to all.
-
Taking more direct steps to support people to discuss experiences of loneliness. Wider actions could mitigate loneliness stigma, such as encouraging group discussions around experiences of loneliness, signposting to loneliness-specific services and supporting other services to identify and support people experiencing loneliness. Schools, workplaces and other organisations can all play a role in normalising day-to-day discussion of loneliness.
A number of enablers could support organisations to address stigma through national campaigns and direct support mechanisms. In particular:
-
Considering the language around loneliness. In service delivery and campaigns, the language used around loneliness needs to be carefully constructed, so as to not perpetuate stigma. This could include avoiding negative words like ‘tackle” and using a range of terms to describe support/services (including more positive terminology such as “connecting,” and “building relationships”).
-
Coordinating across organisations. Collaborating with partner organisations who work “on the ground” could help ensure services and campaign messaging considers diverse lived experience and reaches wide-ranging groups. Stakeholders also suggested that further coordination of campaign activity across relevant organisations could ensure year-round messaging.
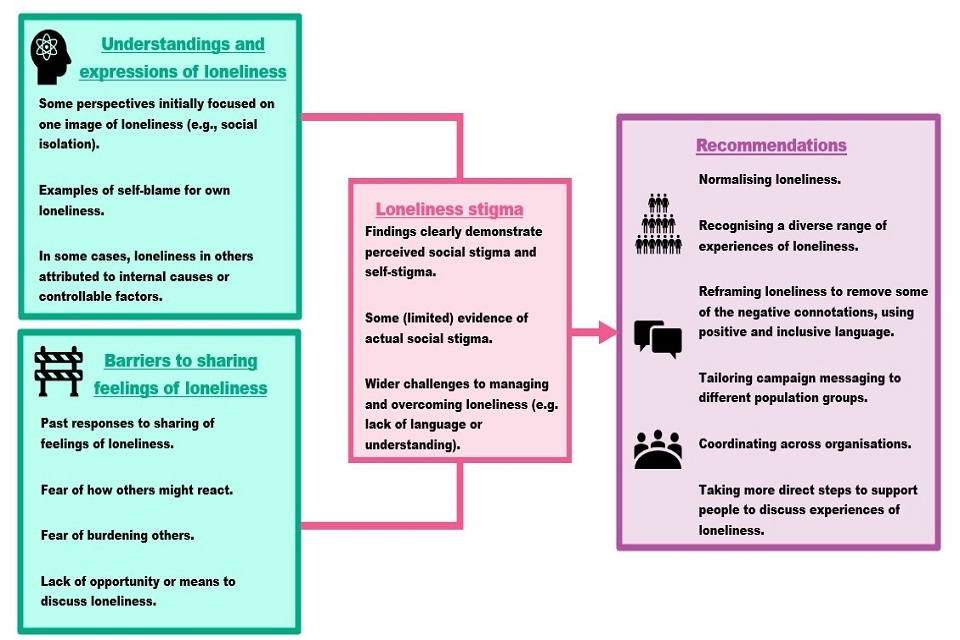
This research demonstrates that normalising loneliness, tackling negative associations and encouraging conversations would help people experiencing loneliness feel less alone, help remove associated internal shame (i.e., self-stigma) and anticipate more positive reactions from sharing their feelings (thereby reducing perceived social stigma). There is also the potential for these actions to address actual social stigma by addressing some of the more “stereotypical” or negative perceptions of loneliness. There are wider barriers to overcoming loneliness which would need to be addressed alongside stigma (e.g., practical challenges to socialising such as lack of childcare, local groups or free time). However, this research suggests that these actions still have the potential to help people feel less alone and more able to manage their experience, even where the experience of loneliness cannot be completely overcome. Please see below for an illustration of the key findings:
Figure 1. Key findings
[1] These definitions align with recent academic papers on loneliness stigma (e.g., Barreto et al., 2022 which reports on the BBC Loneliness Experiment).
[2] Drawing on Perlman and used in the UK Government’s Loneliness Strategy (2018), D. and Peplau, L. A. (1981) Toward a Social Psychology of Loneliness. In R. Gilmour & S. Duck (Eds.), Personal Relationships: 3. Relationships in Disorder (pp. 31-56). London.
[3] Drawing on Link, B. & Phelan, J. (2001). Conceptualizing Stigma. Annu Rev Sociol, 27, 363–85.
[4] Drawing on Barreto, M., van Breen, J., Victor, C., Hammond, C., Eccles, A., Richins, M. T., & Qualter, P. (2022). Exploring the nature and variation of the stigma associated with loneliness. Journal of Social and Personal Relationships, 39(9), 2658–2679.
[5] Drawing on Barreto, M., van Breen, J., Victor, C., Hammond, C., Eccles, A., Richins, M. T., & Qualter, P. (2022). Exploring the nature and variation of the stigma associated with loneliness. Journal of Social and Personal Relationships, 39(9), 2658–2679.
Glossary and abbreviations
DCMS - The Department for Culture, Media and Sport.
Evidence review - A research method which locates and synthesises existing evidence on a particular topic or issue.
Focus group participants - Participants with little recent experience of loneliness who took part in focus groups (n=24).
Framework / Framework method - A method for extracting and analysing data, whereby each row represents one paper, and each column represents a research question or sub-question.
Intersectional approach - An intersectional approach recognises that different facets of a person’s identity ‘intersect’ to shape the lived experience of the individual.
Interviewees - Participants experiencing loneliness regularly who completed interviews and diary entries (n=40)
Loneliness - “A subjective, unwelcome feeling of lack or loss of companionship. It happens when we have a mismatch between the quantity and quality of social relationships that we have, and those that we want.”[1]
Rapid Evidence Assessment (REA) - A type of evidence review (see definition above) which seeks to understand the existing evidence on a particular topic within a short period of time.
Self-stigma - Feeling shame or embarrassment around a personal characteristic or experience and being inclined to conceal it from others.[2]
Social stigma - Negative attitudes or beliefs towards an individual or group, based on experiences or characteristics which are seen to distinguish them from other people (in this case, experiences of loneliness). This results in the person or group being devalued and/or suffering discrimination.[3],[4] This review explores actual and perceived social stigma.
Stigma - Covers both social and self-stigma.
Stakeholders - Professionals with experience tackling loneliness stigma who took part in interviews (n=6).
Qualitative research - The collection and analysis of non-numerical data (e.g., data from interviews).
[1] Drawing on Perlman, D. and Peplau, L. A. (1981) Toward a Social Psychology of Loneliness. In R. Gilmour & S. Duck (Eds.), Personal Relationships: 3. Relationships in Disorder (pp. 31-56). London.
[2] Drawing on Barreto, M., van Breen, J., Victor, C., Hammond, C., Eccles, A., Richins, M. T., & Qualter, P. (2022). Exploring the nature and variation of the stigma associated with loneliness. Journal of Social and Personal Relationships, 39(9), 2658–2679.
[3] Drawing on Link, B. & Phelan, J. (2001). Conceptualizing Stigma. Annu Rev Sociol, 27, 363–85.
[4] Drawing on Barreto, M., van Breen, J., Victor, C., Hammond, C., Eccles, A., Richins, M. T., & Qualter, P. (2022). Exploring the nature and variation of the stigma associated with loneliness. Journal of Social and Personal Relationships, 39(9), 2658–2679.
1. Introduction
1.1 Background
Long-term feelings of loneliness are associated with higher rates of mortality and poorer physical health outcomes.[1] Furthermore, loneliness can predict the onset of common mental disorders, such as depression and anxiety.[2],[3] The UK Government’s tackling loneliness strategy sets out the approach to tackling loneliness in England. The goals set out within this strategy include “reducing the stigma attached to loneliness so that people feel better equipped to talk about their social wellbeing” (pg. 9). However, as demonstrated through the Tackling Loneliness evidence review there are gaps in the evidence base around loneliness stigma.
In 2022, DCMS commissioned The National Centre for Social Research (NatCen) to undertake a Rapid Evidence Assessment (REA) of existing research on loneliness stigma (“the Loneliness Stigma evidence review”). The full report identified 36 relevant papers. Although evidence of self- and social stigma was found, national and international surveys indicated that social stigma may not be widespread. It was also demonstrated that self-stigma and the perception of social stigma can present barriers to discussing and overcoming loneliness. However, evidence gaps were identified around how loneliness stigma is experienced and how it can be tackled. The Loneliness Stigma evidence review accordingly recommended further research to explore the drivers of loneliness stigma across different population groups, along with how interventions could effectively tackle such stigma.
1.2 Research aims
To further develop the evidence-base around loneliness stigma, DCMS commissioned NatCen and RSM UK Consulting (RSM) to explore the following research questions:
-
How do different demographic groups understand and express loneliness?
-
What are the barriers that prevent people from taking actions to try and overcome their loneliness, and do these differ across demographic groups?
-
Do different demographic groups experience stigma around loneliness? If so, how?
-
How do you reduce the stigma experienced by people experiencing loneliness?
-
Could reducing stigma alleviate loneliness and, if so, in what ways?
-
How could a national campaign to reduce stigma be effective, and for whom?
1.3 Methods and participants
This research consisted of three parts: interviews with stakeholders, in-depth interviews and diaries with participants experiencing loneliness regularly and focus groups with participants with little or no recent experience of loneliness. For more details of the sample, methodological approach and ethical considerations, please see Appendix A.
Stakeholder interviews
Six interviews were conducted with stakeholders with professional experience in tackling loneliness stigma. These interviews provided expert insights into interventions and strategies to overcome loneliness stigma.
Interviews and diaries with interviewees
Forty in-depth interviews were conducted with participants who reported regular feelings of loneliness and loneliness stigma. Participants were sampled based on their life stage (young adults; parents of young children; middle-aged; retired). Secondary sampling criteria (e.g., ethnicity, disability and relationship status) were also monitored to ensure that the research captured a diverse range of experiences. Over two weeks prior to the interview, participants completed online diary entries documenting their connections with others, experiences of loneliness and whether they had discussed their feelings. Interviewers drew on entries to facilitate the discussion and generate richer insights into day-to-day experiences of loneliness.
Focus groups
Three focus groups, each with eight participants, were conducted to explore societal perspectives of loneliness in others. Participants reported little or no recent experience of loneliness. Each focus group contained participants from one age group (16-34; 35-64; 65+).
Analysis and interpretation of findings
Interviews and focus groups were transcribed and analysed using the Framework approach,[4] whereby each row represented one interview or focus group and each column represented a topic of relevance. Relevant information from each interview or focus group was written into the corresponding cell. This grouped information around each research question, enabling the research team to assess the relevant evidence. Findings have been integrated across the three work strands and are presented thematically.
This report does not provide numerical findings, since qualitative research cannot support numerical analysis. Instead, the qualitative findings provide in-depth insights into the diverse range of views and experiences of participants and verbatim quotes are used to illustrate these. Experiences of interviewees were informed by a range of factors, including demographics and life circumstances, which culminated in unique experiences for each individual. While this report comments on the impact of demographics and wider factors, this focuses on qualitative insights (i.e., how and why demographics impact experiences) rather than making quantitative claims that certain experiences are more or less common in different groups.
1.4 Structure
This report is divided into the following sections:
-
Chapter 2 explores expressions and understandings of loneliness
-
Chapter 3 discusses barriers to sharing and managing experiences of loneliness
-
Chapter 4 explores experiences of loneliness stigma. This Chapter also contains illustrations of how experiences of loneliness and loneliness stigma can be shaped by demographic factors
-
Chapter 5 makes recommendations for how stigma can be tackled and considers the likely impact of these interventions.
[1] Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social relationships and mortality risk: a meta-analytic review. PLoS medicine, 7(7)
[2] Mann, F., Wang, J., Pearce, E., Ma, R., Schleif, M., Lloyd-Evans, B. and Johnson, S. (2021). Loneliness and the onset of new mental health problems in the general population: A systematic review. MedRxiv.
[3] Nuyen, J., Tuithof, M., de Graaf, R., Van Dorsselaer, S., Kleinjan, M. and Have, M.T. (2020). The bidirectional relationship between loneliness and common mental disorders in adults: findings from a longitudinal population-based cohort study. Social psychiatry and psychiatric epidemiology, 55(10)
[4] Ritchie, J., Lewis, J., Nicholls, C.M. and Ormston, R. eds., 2013. Qualitative research practice: A guide for social science students and researchers. Sage.
2. Expressions and understandings of loneliness
This Chapter explores how different population groups understand and express loneliness by drawing on insights from interviewees (i.e., those experiencing loneliness regularly) and focus groups (i.e., those with little or no recent experience of loneliness).
2.1 Personal expressions of loneliness
This section explores how interviewees described their experience of loneliness and the factors driving it. Section 2.2 will then consider broader perceptions of loneliness, and how these perceptions align with lived experience.
2.1.1 The experience of loneliness
Interviewees’ experiences of loneliness were related to negative feelings about their quantity or quality of social connection. For some participants, feelings of loneliness were driven by having very little day-to-day connection with other people (e.g., not speaking to many other people daily). This caused consistent negative and unwelcome feelings such as isolation, a sense of loss and emptiness.
“I don’t have any family and I don’t have any close friends really, so I am a bit bereft of that type of family connection, and also they’ve [extended family and friends] got children and grandchildren, and they’ve got their own lives that I’m not connected with, really” – Interviewee (40-60 age group)
However, loneliness was also experienced by those with higher day-to-day levels of social connection, including those with strong relationships. In these cases, feelings of loneliness were driven by three factors:
- Physically spending time alone due to circumstances (rather than active choice). These feelings were experienced by interviewees who did not live with other adults, but were also triggered by doing activities alone which the interviewee would prefer to do with others. For some parents, this included time spent with small children but without other adults. These activities were specific to each individual and included entertainment outside the house (e.g., going to the cinema) and day-to-day chores. When physically spending time alone, participants explained that they missed companionship and the “little things”, such as the physical presence of another person.
“When I’ve done my night-time chores and I sit alone in my flat. The feelings of lack of companionship overwhelm me” – Diary entry (parent)
-
Feeling disconnected from others. In some cases, disconnection was driven by the interviewee feeling different from those around them. This led interviewees to feel that they were not understood or created a barrier to finding commonality or shared interests. For others, disconnection related to the quality or strength of their relationships. One interviewee described having only “surface level” relationships while others were unable to have meaningful conversations with family and friends. Feelings of disconnection could be experienced when interviewees were alone or spending time with others that they did not feel connected to.
-
Missing particular connections. Some participants felt that while they had meaningful relationships, particular connections were “missing” from their lives. This included particular relationships (e.g., a partner) and particular people (e.g., friends and family who lived far away).
As illustrated in section 2.1.2 below, these factors can be experienced alone or simultaneously.
2.1.2 Causes and drivers of loneliness
Interviewees attributed their feelings to different life experiences. As described below, they felt that these experiences led to loneliness by – directly or indirectly – reducing the quantity and/or quality of their connections.
Health and disability
Some participants felt that their experience of loneliness was attributable to physical or mental health conditions including disability, cancer, depression and anxiety. Older people tended to attribute their loneliness to physical health while younger people were more likely to discuss the impacts of their mental health.[1] One younger interviewee felt that mental health was a key driver of loneliness among their peer group. Health challenges and disability were felt to cause loneliness in the following ways:
-
Physical health barriers to social connection. In some cases, interviewees struggled to socialise due to their health condition or disability, which resulted in them spending time alone. Physical health challenges and pain made it difficult for interviewees to leave the house or socialise face-to-face. In some cases, interviewees in the 40-60 and 65+ age groups spoke about how poor health prevented them engaging in activities which had previously been important in their social life (e.g., sports clubs). Some people living with health conditions or disabilities had experienced very difficult periods of loneliness at times when they were physically prevented from seeing others (e.g., during hospital stays).
-
Emotional barriers to social connection. Interviewees living with a health condition or disability also felt that their experiences had led to emotional barriers to connecting with others. Some felt that poor mental health was a barrier to connecting with others because they found socialising difficult, particularly in times of low mood or heightened anxiety. Others described how physical health conditions (e.g., cancer) caused them to lose confidence or emotionally withdraw from friends and family. In some cases, the COVID-19 pandemic had prompted or exacerbated mental and physical health anxieties which continued to drive worries about socialising. Feelings of disconnection could also arise for interviewees with a health condition or disability due to a lack of shared experience. For example, an interviewee living with a disability could not do the “normal stuff” that his friends could (e.g., playing football) and had experiences of hospitalisation that his friends could not relate to. Some interviewees with a health condition or disability highlighted the role of others in creating or perpetuating these emotional barriers to connection. For example, one interviewee attributed their “fear of rejection” to first-hand experiences of stigmatising views around disability. However, others focused on their own actions and mindset, such as whether they took proactive steps to socialise and were open to new connections. In some cases, this led to interviewees feeling accountable for their experiences of loneliness.
“It’s like a rejection type thing. I think it’s just me, got this mindset that thinks that other people, they’re always going to be busy and not to bother or trouble them type thing. Yes, I think it’s down to me really.” – Interviewee (40-60 age group)
Life circumstances and experiences
Some experiences of loneliness were caused by life events and commitments which reduced social connection. This included:
-
Retirement, unemployment or other working changes (e.g., working from home) that reduced day-to-day social connection.
-
Parenting commitments that reduced time for socialising or prompted lifestyle changes, which resulted in interviewees spending less time with other adults.
-
Death of a partner or other relative, with interviewees missing the close connection and companionship they previously enjoyed with that person. One interviewee who had lost his wife explained “it’s been a big like culture change of doing everything together, then, all of a sudden, you’re on your own”.
-
Other changes to relationships, such as friends or family moving away. Similarly, divorce or relationship break- down led to some interviewees feeling lonely due to spending more time alone. However, these interviewees also tended to describe feelings of loneliness or disconnection within their relationship, with some describing these were worse than the feelings they experienced post-break up.
The life events discussed above had immediate impacts on interviewees’ social connections. However, in some cases there were also long-term impacts on loneliness. This could occur when experiences (e.g., bereavement, divorce or working away from home) forced interviewees into a routine of spending time alone, which then felt hard to break.
As well as impacting the quantity of social connection, life events and circumstances could prompt feelings of disconnection from others who did not share the same experiences. This was due to interviewees not feeling understood or wanting empathy (even if those around were supporting and sympathetic).
“Motherhood is a very lonely thing, especially if you’re going through struggles…It was a really lonely time, because no one was going through quite what I was around me. There’s only so much people can sympathise.” – Interviewee (parent)
Non-working interviewees also experienced disconnection because they did not have experiences of work or socialising to contribute to discussions with others. One interviewee felt that working “gives you something to talk about”. Similarly, parenthood caused some interviewees to feel a reduced level of connection with their partners because the focus of the relationship had changed.
When discussing these types of life events, interviewees had mixed perspectives on whether their experience of loneliness was driven by their actions, by the actions of others or by circumstance (e.g., getting older, family moving away). Some interviewees described the impact of their own actions or choices in reducing their level of social contact. For example, one retired interviewee felt that changes to their self-image, which accompanied retirement, caused them to withdraw from others. Another experience was that of parents with little time to socialise, who described how they took decisions to prioritise spending time with family over socialising with others.
“I suffer from a lot of mum guilt…So I exclude myself from social activities, and actually putting myself out there, and taking the time to actually meet people and be in networks where I’m able to establish relationships, friendships, any kind of companionship that would be open to me, had I not had the guilt.” – Interviewee (parent)
However, some interviewees had considered the role of others in their experiences of loneliness. For example, some people who had been through a life change (e.g., serious illness, retirement or parenthood) felt that those around them made fewer efforts to connect with them than before.
“You notice that people don’t bother inviting you anymore. You then get that little bit older, then they might have children, so then they’re focused on that. That again dwindles your circle down… It’s just what happens.” – Interviewee (parent)
2.2 Societal understandings of loneliness
This section explores how loneliness is understood from a societal perspective, drawing on findings from focus groups (i.e., those with no/little recent experience of loneliness) and interviews with people experiencing loneliness.
2.2.1 Understandings of the experience of loneliness
Across the interviews and focus groups, there were mixed perceptions about how loneliness (outside personal experiences) related to quantity and/or quality of social connection. Some participants initially perceived that loneliness only related to the quantity of connections. For example, the word ‘loneliness’ prompted some interviewees and focus group participants to think about images of social isolation or a person with few connections.
“I think for me, [the image of loneliness is] no friends or family and no contact with anybody that they could have conversation with or contact.” – Focus group participant (65+ age group)
However, interviewees and focus group participants who reflected on these views tended to ultimately perceive that experiences of loneliness could be driven by negative feelings about both quantity and quality of connections.
Some focus group participants perceived that loneliness was “less about” the quantity of connections, suggesting that someone could be physically surrounded by others and/or have long-term relationships but still experience loneliness if they felt disconnected or if their needs were not being met. These participants did not disagree that some experiences of loneliness were caused by a low quantity of social contact. Instead, their perspective was that quality of connection was a more useful measure to understand loneliness because it captured a wider range of experiences. Similar comments were made by interviewees, particularly those with higher levels of day-to-day connection.
There were mixed understandings as to which factors were important in distinguishing severity of loneliness. The Government definition gives equal weight to experiences of loneliness driven by negative feelings about quality or quantity of social connection. However, some interviewees believed that severity of loneliness was linked to the level of social isolation (i.e., quantity of social connection). One perspective was that “really serious loneliness” was being totally isolated and alone. The impact of this was that although interviewees regularly felt lonely, some did not believe that they could experience the most serious type of loneliness because they had friends and family. Conversely, some interviewees with more social contact felt that others did not understand how serious feelings of loneliness in their situation could be. An interviewee in the 16-30 age group stressed that loneliness was a really serious issue among young people despite some perceptions to the contrary, and that young people really “feel it” – this suggests that it is more important to understand how the experience impacts the person, rather than how it appears from the outside. Altogether, interviewees who discussed the severity of loneliness tended to relate this to the intensity of their current experience, rather than the length of time they had felt this way. When thinking about imagery of loneliness, focus group participants (with little/no recent experience of loneliness) found it difficult to distinguish between long-term and transient loneliness, given the variety of factors (e.g., life events and wider circumstances) which could lead to loneliness. However (as explained below) some focus group participants perceived that certain factors (e.g., old age and low confidence) could lead to more frequent feelings of loneliness.
2.2.2 Causes and drivers of loneliness
Understandings of the experience of loneliness across the life course
Interviewees and focus group participants felt that everyone is likely to experience some form of loneliness at some point in their lives. It was perceived that some experience of loneliness is almost inevitable at some point in the life course due to the connection with certain life events (e.g., changing jobs, divorce or widowhood). As explained above, focus groups did not generally distinguish particular experiences as long term or transient loneliness, perceiving that experiences of loneliness were likely to vary depending on individual factors.
“I think there’s probably people that are more prone to it than others, I’d have thought. Everyone’s got other things going on in their lives and everyone processes things in different ways, so I’d imagine there’s probably people that are more prone to feeling lonely or depressed, or things like that than others. I’d be surprised if there was anyone that ever could say that they’ve never felt lonely.” – Focus group participant (16-34 age group)
On the basis of personal experience, some interviewees felt that loneliness within certain groups was harder for society to understand. For example, both younger people and new parents felt that loneliness within their peer group was dismissed (or not recognised at all) due to assumptions that their needs were met by those around them. One interviewee in the 16-30 age group also questioned how common loneliness was in their peer group due to a perception that most people spent a lot of time socialising. In comparison, interviewees felt that loneliness among older people was well recognised, particularly in the media.
“They expect you to be bubbly…You’re at uni, you’re going out clubbing, you’re drinking, you’ve got all your friends from school…I do think they dismiss it [loneliness] because…you can do all that.” – Interviewee (16-30 age group)
One perspective from an older interviewee was that younger people may not understand their experience of loneliness. This appeared to relate to a perception held by the interviewee that younger people are less likely to face the same barriers to social connection as older people (e.g., living alone or physical health barriers) and therefore would not be able to understand why loneliness could not be overcome.
While focus groups recognised that loneliness could be experienced at any age, there was a common perception (contrary to the Government definition of loneliness) that older people were susceptible to a more severe or frequent experience of loneliness, due to being socially isolated and not having distractions to remove them from the feelings.
“My old neighbour…she’s not really going to change the way that she feels loneliness-wise. She may have very short periods where she’s reading or she’s doing something, but I think those are very few and far between. Whereas I think children or young adults, they have to have some sort of interaction with adults or schools or whatever, so they are getting some form of contact. I think that an elderly group is going to feel that loneliness more than a child or a young adult.” – Focus group participant (65+ age group)
However, perceptions were often stated in terms such as “the automatic thing to say is it’s older people”. This image was questioned by participants, who reflected that other age groups can experience loneliness or highlighted examples of retired friends or family who “love every minute of it”. However, despite this self-reflection, the regularity with which this group was mentioned indicates that society continues to view loneliness as being inextricably linked with old age.
Interviewees and focus group participants drew on personal experiences when discussing how they understood loneliness. Focus group participants were sampled on the basis that they had not recently experienced regular feelings of loneliness. However, some had felt lonely themselves at some point, had friends or family who had experienced loneliness or had encountered loneliness in the course of their work.[2] Focus group participants recounted specific examples in their lives, such as a friend who could not leave the house, an elderly neighbour or young people they had worked with. Older focus group participants also spoke about their experiences during the life course, which guided their views on loneliness among younger age groups. Interviewees and focus group participants also felt that the media, including TV, film and books, may have influenced some of their views. While some felt that media focus tended towards older people living alone - “it’s shown as elderly people that live alone-type situation” - coverage around the COVID-19 pandemic was felt to have highlighted broader experiences of loneliness.
Understanding of causes of loneliness
As explained in section 2.1, interviewees tended to focus on individual causes when describing their own experiences of loneliness (e.g., health conditions and life experiences). Within each focus group, participants (with little/no recent experience of loneliness) recognised that these experiences could drive feelings of loneliness, referencing similar examples of life events leading to feelings of loneliness for friends or loved ones. In this respect, focus group participants did not attribute feelings of loneliness to being within the control of the individual or place blame for loneliness on those experiencing it.
Focus group participants perceived that certain traits (e.g., confidence and resilience) may drive people to proactively seek social connection. Some interviewees also felt that loneliness could be caused by the actions of the individual. While some interviewees only raised this perspective in the context of their own experiences (see section 2.1.2 for findings about self-blame), others felt that other people isolated themselves. In some cases, it was acknowledged that self-isolation was driven by circumstantial factors (e.g., old age and health problems). However, there was also a perception that some people could do more to seek out connection.
“I would say that certain people do feel lonely quite often. I think confidence has a big impact…I’ve known people in the past and now who aren’t very confident in themselves, so they isolate themselves away, or don’t know how to get involved, which, obviously, in itself creates being alone and not in the mix with people, which I would class as being lonely.” – Focus group participant (35-64 age group)
“I think you can control it. You can make yourself isolated and lonely. You’ve got to put effort in yourself, and if you don’t, there’s no guarantee that other people will, so I think you can. Certain people can create their own loneliness where they cut themselves off, but then I feel for me, my loneliness has gone how things have changed as my friends and everyone have got older, families, grandchildren.” – Interviewee (40-60 age group)
When considering the causes of loneliness in society, both focus group participants and interviewees attributed loneliness to a range of societal factors, including social media and virtual communication.
Younger focus group participants (age 16-34) suggested that social media use could lead to feelings of “not fitting in” or being “left out”. Younger interviewees confirmed that social media exacerbated their feelings of loneliness, by causing them to compare themselves negatively to others they saw online.
“I do think social media has a really big influence on it. I think it’s very easy to post things and then, as a viewer, watching this, thinking, how do these people get to - these people have got loads of friends, and they’re always out and about, and they have money to do these things. Why can’t I? That can make you feel quite lonely and isolated.” – Interviewee (16-30 age group)
Focus group participants (with little/no recent experience of loneliness) also perceived that loneliness was driven by a lack of physical contact, caused by the increased use of virtual communication methods, such as social media or Zoom (in work contexts). These participants suggested that virtual communications do not satisfy the need for human connection and promote less meaningful interactions. To some extent, this perspective was reflected in the first-hand experiences of interviewees. For example, some older interviewees felt that phone calls and face-to-face contact had decreased, being replaced by text messages, which they felt exacerbated experiences of loneliness. Younger and older interviewees who spoke about the impact of virtual communication on their own experiences discussed this as a societal issue and an external driver for loneliness, rather than something they could control. However, there was a perception (particularly among older focus group participants and interviewees) that some younger people felt lonely because they prioritised screen time or social media over face-to-face or deeper connections. For example, some older focus group participants (age 65+) perceived that many young people are more concerned with how many “Facebook friends” they have, rather than building closer relationships with their family and friends. It should be noted that this suggestion was not supported by data collected from young interviewees. While some young interviewees acknowledged social media as a societal driver of their loneliness (see above), they did not suggest that their lonely feelings resulted from a choice to prioritise social media over face-to-face connection. Therefore, this can be considered (see Chapter 4) as a potentially stigmatising view of loneliness.
“I think social media plays a very, very big part in loneliness. Maybe I’m wrong in saying that, but that’s the feeling I get from people who are on the screens all the time. It’s okay being on the screens if you’re doing something productive, but that’s just my feeling about the internet.” – Focus group participant (65+ age group)
It is important to note that some interviewees had positive experiences of using social media to overcome feelings of loneliness. This included experiences of joining online groups or talking to friends and family who they struggled to see face-to-face. While younger and older interviewees highlighted the importance of face-to-face contact, virtual communication provided a way to connect when face-to-face connection was not possible.
Some focus group participants and interviewees perceived that loneliness may have increased due to a decline in community and neighbourly relations. It was felt that people were too busy and “wrapped up in their own worlds”, therefore less likely to check in on those around them. In particular, the older focus group (age 65+) perceived that both families and communities could do more to support people who may be at risk of loneliness.
“I think family could help a lot more than they do. I think the trouble is they’re very busy these days.” – Focus group participant (65+ age group)
Some interviewees recounted experiences of others not reaching out to them during difficult or transitional periods in their lives. However, others spoke positively of friends and family. While some interviewees felt they would like to see family more, they did not blame their experiences on those around them.
[1] This finding should not be assumed to be representative of the wider population (given the qualitative methodology and sampling). However, it can help guide interpretation of the findings below.
[2] As research has demonstrated, it is likely that most people experience some form of loneliness at some point in their lives. Therefore, it is likely that any composition of focus group will have experiences of loneliness (even if these are not chronic experiences).
3. Barriers to managing and overcoming feelings of loneliness
This Chapter explores actions taken to manage and overcome loneliness, along with barriers to taking these actions. This primarily draws on views from interviewees (i.e., those experiencing loneliness regularly), as well as with some insights from stakeholders and focus groups (i.e., those with little/no recent experience of loneliness).
3.1 Overview of approaches to managing and overcoming feelings of loneliness
The Loneliness Stigma evidence review found that stigma prevents people from talking about loneliness and accessing support. However, the review also identified wider barriers to talking about loneliness which may or may not be linked to stigma. It was suggested that further research could explore the range of barriers which prevent those experiencing loneliness from accessing support, and the impact of tackling stigma in this context.
Interviewees shared examples of actions they had taken (or wanted to take) to overcome feelings of loneliness. However, others felt that their experiences were not something they could or should “overcome”. This was particularly the case for those who attributed their loneliness to circumstances, such as caring or work commitments, that they could not “fix”. Therefore, this Chapter will discuss barriers to overcoming and managing feelings of loneliness. While there was some consistency across interviewees, some factors driving these barriers related to demographics or wider life experiences. These factors are set out throughout this Chapter. Please also see Chapter 4 for illustrations of how lived experiences are shaped by gender, age and health.
3.2 Sharing feelings of loneliness
While some interviewees had shared their feelings of loneliness with other people, others had little experience of talking about how they felt. Interviewees typically shared lonely feelings with those close to them or where there was trust and/or mutual understanding. As discussed in Chapter 2, some interviewees attributed loneliness to specific life experiences. These individuals valued talking to others with similar experiences who could understand their feelings in context. For instance, some mothers felt able to share their feelings with “mum friends”, whereas others felt comfortable sharing experiences at groups for people with similar health conditions. In some cases, interviewees had sought support from professionals about feelings of loneliness, including GPs and Samaritans. This action was taken when feelings of loneliness had become severe or where interviewees did not feel comfortable talking to those close to them.
3.3 Barriers to sharing feelings of loneliness
Interviewees identified several barriers to sharing feelings of loneliness, which are set out below (please see Chapter 4 for a discussion of the role of stigma in these barriers):
Past responses to sharing feelings of loneliness
Some interviewees who shared their feelings reported positive responses. This included empathy and appropriate action being taken, such as friends and family visiting or facilitating opportunities to socialise. Knowing that others cared made participants feel more able to share feelings of loneliness going forward. This was particularly the case when others were able to empathise with their experience.
“I feel like then I don’t feel stupid for the way I feel sometimes because other people feel like that as well, it’s not just me.” – Interviewee (parent)
However, not all well-intentioned reactions left interviewees feeling comfortable to share future experiences of loneliness. Some interviewees received unwanted advice, including suggestions to “go out more” or take other steps to socialise (e.g., join clubs). In cases where the interviewee did not take the recommended action, because they were unable or did not want to, they felt less comfortable sharing with these people in future. This was driven by a fear that friends and family might be frustrated that their earlier advice had seemingly been ignored. Other interviewees felt patronised by advice they received from professionals (e.g., counsellors), who suggested they take up unsuitable activities to leave the house. Another unhelpful response involved others trying to distract interviewees from how they were feeling. While this response was well-intentioned, some interviewees would have preferred space to discuss their feelings.
“Some people when you say, ‘Oh, I’m feeling a bit lonely,’ they just go, ‘Oh, make yourself busy then. Make plans. Have you tried messaging someone? Have you tried ringing someone?… but it’s not always as simple as just ringing someone or just making yourself busy.” – Interviewee (16-30 age group)
“I just sometimes might want to vent, and I just think I don’t want people to try and start problem-solving for me.” – Interviewee (parent and 16-30 age group)
Some interviewees received responses which were felt to be less well-meaning, including “shrugging off” or “glossing over” loneliness. Other reactions implied blame. For example, one parent was told that their experience of loneliness was a result of their life choices. After sharing feelings, some interviewees received no “follow-up” offers of support or checking in. Other interviewees were cautious about sharing their experience because they had experienced situations where their feelings – or the feelings of others – had become “gossip”.
Fear of how others might react
As well as reactions already received, anticipated or feared reactions were a barrier to sharing feelings of loneliness. Interviewees worried that sharing experiences of loneliness could be perceived negatively as “moaning” or being “miserable”. Interviewees feared that expressing negativity would cause others to view them as “sad” or “boring” and distance themselves. Instead, interviewees wanted to view themselves, and have others view them, in a more positive light. This concern was particularly relevant for those experiencing wider challenges (e.g., health issues), who worried about sounding like a “broken record”. Interviewees struggled to pinpoint the cause of their fears and spoke about their worries being assumptions rather than based on the attitudes or actions of others.
Interviewees also feared judgement from others, particularly those who did not share similar life experiences. Some mothers feared being judged as ungrateful and avoided discussing their experiences so as not to appear that they did not enjoy motherhood. Other interviewees were concerned that people would blame them for their experience. In some cases this stemmed from perceptions about societal assumptions, while others were unsure where this fear came from. Another view was that others without shared experiences (e.g., parenting) would not judge, but their lack of understanding would render them unable to offer an appropriate response.
“I wouldn’t tell my friends as they just don’t get it. They have never been in this position so don’t understand.” – Interviewee (40-60 age group)
Fear of pity was also a barrier to sharing feelings. Interviewees did not want to feel that people were engaging with them just because they felt sorry for them, but because they enjoyed their company. This feeling was expressed across all age groups, but was particularly key for older adults in respect of their grown-up children. This concern was often cited along with a fear of burdening others (see below) but specifically related to how the interviewee was perceived – by themselves and others – rather than the impact on others.
Fear of burdening others
Fear of burdening others prevented interviewees from sharing feelings of loneliness with certain people. For example, some older people refrained from sharing with their adult children to avoid worrying them. A similar explanation was provided by those whose close friends and family had “a lot on their plate”, such as physical or mental health needs. In these cases, interviewees felt that they had to remain emotionally “strong” for others, which entailed not sharing their own struggles. For some, wanting to avoid burdening others was explicitly linked to their prescribed role as dictated by gender and/or culture. Parents felt that their caring role meant they were not meant to seek support from their children. One mother did not feel comfortable sharing feelings of loneliness due to a cultural expectation of strength, related to her gender and caring role – “in my culture they just say that women just have to stay strong and carry on with whatever they are feeling and things will get better”.[1] While fears about burdening others were influenced by societal expectations, interviewees did not feel that these feelings were driven by specific first-hand experiences. Interviewees acknowledged that they did not personally feel burdened when others had opened up to them about their struggles. However, the fear of being a burden remained a strong barrier to instigating conversations about experiences of loneliness.
“Everyone has been really helpful, but again I guess it’s my mindset where I think that I’m loading them up with my problems all the time and dragging them… I think it’s just me that thinks that really.” – Interviewee (40-60 age group)
Lack of means or opportunity to discuss loneliness
Some interviewees had not shared experiences of loneliness because they did not feel able to express their feelings effectively. Some interviewees described themselves in terms such as “private” and explained that sharing any personal matter did not come naturally.
“I just think I struggle with saying my emotions out loud to other people and communicating them the way I mean them.” – Interviewee (16-30 age group)
While these experiences were expressed across all age groups, some older interviewees felt that their generation did not share personal feelings. In other cases, interviewees whose experience of loneliness was tied to a life experience (e.g., bereavement) explained that discussing their feelings would raise wider experiences that they did not feel able to talk about. In some cases, interviewees also struggled to express what support they wanted from others or could not foresee a response that could “fix” their feelings. Stakeholders highlighted that older people may be more likely to hide their feelings due to a societal perspective that loneliness is particularly common among this generation (as highlighted in Chapter 2). In the experience of stakeholders, this perception prevented some older people from seeking support because they assumed that loneliness should be accepted as a consequence of ageing.
Other interviewees wanted to share their experiences, but had not had the opportunity to do so. This tended to be because the interviewee did not feel comfortable initiating the conversation and it was never raised by others. Some felt that others feared upsetting them, particularly where feelings of loneliness stemmed from a difficult life experience, such as the death of a partner. In other cases, it was felt that society generally lacks the language and understanding to have conversations about loneliness.
Focus group participants (with little/no recent experience of loneliness) supported the above, whereby some felt unsure how to best initiate and manage discussions about loneliness. Despite wanting to provide support, some participants felt that concerns about upsetting or embarrassing others prevented them from raising the topic. These concerns were driven by a number of factors. Some participants felt that they lacked the understanding and language to sensitively find out if someone felt lonely and create an environment where they could discuss their feelings. The biggest challenge for focus group participants appeared to be asking direct questions around loneliness. In contrast, participants felt they would be more comfortable providing broader support (e.g., inviting others to socialise). In some cases, participants linked their discomfort to not having personally experienced loneliness, leading to concerns around providing the right comfort and/or solutions. Participants also worried about making assumptions that others feel lonely, particularly where they had a higher level of social connection than the person concerned.
“I wouldn’t really know how to go about getting information out of someone about loneliness and getting them to open up and talk about it. I wouldn’t know how to elicit that information without perhaps upsetting or embarrassing them.” – Focus group participant (65+ age group)
“I don’t even think asking someone if they’re lonely is even really in our language.” – Focus group participant (35-64 age group)
Despite the challenges raised, some focus group participants felt comfortable discussing loneliness and had done so with family, friends, and neighbours who felt lonely. For these participants, a key enabler was having professionally developed communication skills (e.g., through customer/service user facing roles). In some cases, this included professional experience in conducting sensitive conversations (e.g., working in schools or the emergency services).
3.4 Other actions taken to manage or overcome loneliness
Interviewees reported several strategies for managing loneliness in addition to, or instead of, talking about their feelings with others. This included actions to increase their level of social interaction, for example by joining groups to meet others with shared interests. While these activities provide opportunities for relationships to develop, thereby improving social connection, they could also provide a welcome distraction from feelings of loneliness. Similarly, interviewees described focusing time on their own interests (e.g., attending to an allotment, knitting or playing music) as a “release” from loneliness. Rather than increasing their level of social connection, some interviewees wanted to change how they felt by becoming more content in their own company - this included taking steps to do enjoyable activities alone (e.g., hobbies or holidays).
Barriers
Interviewees identified a number of barriers to taking these actions, which often overlapped with causes of loneliness (see Chapter 2):
-
Lack of time. Practical considerations, such as work and caring responsibilities, meant that some interviewees had no time to take actions to manage or overcome feelings of loneliness. This was particularly true for interviewees in the 16-30; parents and 40-60 age groups who were in employment. The combination of work and childcare constraints also posed a barrier for parents.
-
Financial barriers. Financial concerns were a practical barrier to managing loneliness. Some interviewees could not afford to socialise as much as they would like, or did not have time to because they have had to increase their working hours to ensure their financial security. Some made references to the recent rise in the cost of living as exacerbating this barrier.
-
Exhaustion. A combination of the factors outlined above led some interviewees to feeling tired consistently. This prevented them from doing activities that helped manage feelings of loneliness when they arose, such as socialising or playing video games.
-
Emotional barriers. Some interviewees felt that emotional barriers, such as low self-confidence or fear of rejection, prevented them from taking action to connect with others. Some felt more comfortable being alone when feeling lonely. Feelings of low self-esteem led some to feel like they did not have anything to offer those around them, which made them less confident in reaching out to others. To some extent, these emotional barriers were widespread across interviewees. However, in some cases interviewees felt these were driven by mental health challenges or wider experiences (see Chapter 2 for more details).
“When I feel lonely, as well, my self-esteem can tell me to just stay on my own.” – Interviewee (40-60 age group)
- Availability and accessibility of options. Some interviewees had looked for opportunities to make connections, but struggled to find anything of interest in their local area. In some cases, interviewees assumed that this was because their area was rural or “quiet”. Others had considered attending local events or groups, but found travelling to the event to be tiring or anxiety-inducing. In some cases, labelling or first-hand experience of groups had stopped interviewees attending. For example, one interviewee in the age 65+ group who did not feel “older” avoided groups targeted at “older people”, perceiving them as irrelevant and uninteresting. One parent also described how they did not want to join local mother and baby groups, because they felt that the groups were exclusionary to mothers with lower incomes.
[1] The culture of the interviewee is not provided here because this finding represents one experience and should not be taken to be common across that culture. However, when understood with wider findings in this paragraph it does indicate that cultural expectations can drive barriers to sharing feelings of loneliness.
4. Experiences of loneliness
This Chapter draws the findings from Chapters 2 and 3 and wider insights from stakeholders, interviewees (i.e.,those experiencing loneliness regularly) and focus group participants (i.e.,those with little/no recent experience of loneliness) to examine how loneliness stigma is understood and experienced.
4.1 Defining loneliness stigma
The definitions of stigma used in this research were developed through the Loneliness Stigma evidence review. This section discusses the findings from this research in the context of the literature identified in this review.
-
Social stigma: Negative attitudes or beliefs towards an individual or group, based on experiences or characteristics which are seen to distinguish them from other people (in this case, experiences of loneliness). This results in the person or group being devalued and/or suffering discrimination.[1],[2]
-
Self-stigma: Feeling shame around a personal characteristic or experience and being inclined to conceal it from others.[3]
Stakeholders defined stigma in similar terms, and were guided by the literature when expressing their views. However, wider reflections from interviewees and stakeholders could broaden the definition of social stigma in future research. Both groups spoke more broadly about stigma as a general negativity around loneliness. Some interviewees struggled to pinpoint specific attitudes or beliefs but still felt this negativity, with one describing stigma as “like a negative thing that’s stuck onto it [loneliness]”.
4.2 Experiences and perceptions of social stigma
Actual social stigma
The Loneliness Stigma evidence review found that some people do hold stigmatising views of loneliness. However, these are not universal and tend to be grounded in stereotypes of people who feel lonely (e.g., assumptions that people are responsible for their experience). It was suggested that further research could explore the extent of societal assumptions around loneliness and whether (and how) people who feel lonely have experienced stigmatising views from others.
Exploring actual social stigma involved examining attitudes towards those who experience loneliness, to understand the extent of negative opinions. This report has paid particular attention to whether opinions ascribe blame to those who feel lonely, as this emerged as a driving factor of social stigma in the Loneliness Stigma evidence review.
As discussed in Chapter 3, some interviewees had experienced negative or unhelpful responses when sharing feelings of loneliness. In some cases, these responses could be considered stigmatising (in line with the definitions used in research), for instance where jokes were made which portrayed the interviewee in a negative light or comments were made that loneliness was caused by their own life choices. One interviewee in the 16-30 age group spoke of first-hand experiences of stigmatising views during conversations at school, whereby students linked loneliness with social isolation (i.e.,someone without friends). In this situation, the interviewee felt that the tone of the discussion was that “there’s got to be something wrong with you”. However, many responses that interviewees considered unhelpful were not necessarily stigmatising or suggestive of negative beliefs around loneliness. For example, reactions such as “glossing over” experiences of loneliness or offering oversimplified solutions may be driven by the types of issues discussed in Chapters 2 and 3 rather than negative perceptions of those experiencing loneliness. This could include perceptions that more “serious” loneliness tends to impact older people and/or the confidant not feeling confident discussing loneliness.
Focus group participants generally did not discuss views of loneliness which were explicitly negative or blame those experiencing loneliness. This related to a strong view that feelings of loneliness are a normal part of life, and an understanding that these can be driven by a wide variety of life events and circumstances. As explained in Chapter 2, some focus group participants were informed by their own personal experiences of loneliness and experiences of loneliness among friends and family.
Chapter 2 described some perceptions among focus group participants and interviewees that loneliness could be linked to individual factors such as a lack of confidence, resilience and self-isolation.
“I would say that certain people do feel lonely quite often. I think confidence has a big impact…I’ve known people in the past and now who aren’t very confident in themselves, so they isolate themselves away, or don’t know how to get involved, which, obviously, in itself creates being alone and not in the mix with people, which I would class as being lonely.” – Focus group participant (35-64 age group)
For the most part, the degree to which these views are stigmatising is debatable. For example, one focus group perception was that loneliness could be attributed to individual factors such as low confidence and resilience. It was also perceived that some people self-isolate due to various circumstantial reasons (e.g., ill-health). However, these participants did not speak negatively about people experiencing loneliness or make assumptions that factors such as low self-confidence were controllable or should be viewed as a failing.[4] It is also notable that (as set out in Chapter 2) interviewees described their experiences of loneliness using similar language around self-confidence and self-isolation. However, other perceptions (from both interviewees and focus group participants) that placed a certain degree of responsibility on those experiencing loneliness could be seen as more stigmatising. In particular, there was a perception among older interviewees and focus group participants that young people may experience loneliness because they prioritise virtual, less meaningful connections (e.g., ‘Facebook friends’) above more meaningful relationships. Some interviewees and focus group participants also used stigmatising language around self-isolation (e.g., “certain people can create their own loneliness where they cut themselves off”).
When discussing imagery of loneliness, the first reaction of some focus group participants was to think of people experiencing loneliness as appearing in a certain way (examples included thinking of someone who was “sad” or thinking of an isolated older person). However, as the discussion in each group progressed, it was recognised that people experiencing loneliness did not fall within one group or image. Interviewees and focus group participants were open to reflecting on their views and proactively questioned some of the more “stereotypical” views that they presented (e.g., loneliness being common among older people).
Perceived social stigma
The Loneliness Stigma evidence review found that some people who feel lonely spoke directly about a social stigma, however stigma was spoken about in a general sense with no specific examples of social stigma provided. Other people experiencing loneliness described fears of being judged or rejected. While these people did not speak directly about loneliness stigma, their views indicated a perception of such stigma. However, in the BBC Loneliness Experiment, the average participant (including those who did and did not experience loneliness) did not perceive much social stigma in the community.[5] It was suggested that further research could explore perceptions of social stigma to better understand the nature and impacts of these perceptions.
Exploring perceived social stigma involved examining whether people who feel lonely perceive that others hold negative opinions about loneliness. Some interviewees (who had and had not experienced stigmatising views) perceived that there was a social stigma around loneliness. While some used this term, others spoke of expectations that if they shared feelings of loneliness, others might think negatively of them. For example, interviewees worried about being seen as “sad”, “boring” or “weak”, or being blamed for their experience. In some cases, these fears aligned with the interviewee’s experience of self-stigma (i.e.,feeling internally that their loneliness was a sign of weakness). However, other interviewees did not hold these negative views about their own experiences but felt that others would.
“Yes, sad, get out and get a life, basically! That’s probably what they’d be thinking.” – Interview participant (40-60 age group)
Some interviewees felt that this perceived stigma was driven by a lack of understanding about who experiences loneliness and what causes it. This was particularly the case for interviewees who felt that their experience of loneliness was not well recognised. In particular, these interviewees felt that they may be blamed because of assumptions that these feelings are due to their own actions. On the contrary (as shown in Chapter 2) loneliness is driven by a variety of life circumstances and experiences which can impact anyone. While concerns about blame were present across all age groups, some younger people felt that – because of their age and circumstances – others must assume that they had ample opportunity to socialise if they wanted to. One interviewee linked these concerns to a broader feeling that society views those who spend time alone in a negative light, particularly when this is felt to be by choice.
“I think people just assume because you’re lonely, you don’t have any friends and you don’t, and then they think, why doesn’t she have any friends? She must be weird or she must be, there must be something wrong with her, or she might be not nice or… It’s that kind of thing.” – Interviewee (parent)
As mentioned in section 4.1, some interviewees perceived a general negativity around loneliness or commented that it was seen as “not normal” but struggled to identify more specific negative attitudes. Some interviewees felt that society did not view those experiencing loneliness negatively, but still viewed loneliness as a “bad thing” which raised negative emotions (e.g., talking about loneliness makes people feel “sad”). Others did not have strong views – or found it difficult to comment – on how others view loneliness. In some cases, this was because they had no experience of discussions around this topic.
3.3 Experiences of self-stigma
The Loneliness Stigma evidence review found that loneliness can be accompanied by feelings of embarrassment or shame. However, there was little evidence for how people who feel lonely come to hold negative perceptions about their loneliness. It was suggested that further research could explore which factors are influential in how people feel about their own loneliness.
Exploring self-stigma involved considering whether people experiencing loneliness felt embarrassment or shame around their experience and were inclined to conceal their feelings. Some interviewees were reluctant to share their experiences of loneliness due to feelings of embarrassment and shame. Not all interviewees were able to pin-point where these feelings came from, however this was often linked with the barriers to sharing loneliness documented in Chapter 3 (i.e.,actual or perceived reactions of others or fear of burdening loved ones). In some cases, embarrassment came from the feelings of self-blame explained in Chapter 2 (e.g., interviewees feeling that they could do more to socialise). This embarrassment was exacerbated when interviewees had been encouraged by friends and family to take more steps to socialise, and had not acted on the advice. In other cases, embarrassment was driven by a feeling that the interviewee “shouldn’t” feel lonely. This was particularly apparent among interviewees who had family and friends, and was thought to be exacerbated by some of the perceived misunderstandings about loneliness explained in Chapter 2 (e.g., loneliness being linked to social isolation and not being common among certain groups).
“You feel like you’re a grown-up, you shouldn’t be feeling lonely, you’ve got a child, you work, so I feel like that’s what makes you feel a bit embarrassed, telling someone that you’re lonely.” – Interviewee (parent)
Feelings of self-stigma were driven both by concerns about how others would perceive the interviewee (relating to perceptions of social stigma) and how they would perceive themselves. Interviewees wanted to be perceived in a positive light by others (e.g., as “happy”), as well as feel independent and capable of coping by themselves. They feared that sharing their feelings would make them feel “needy” or vulnerable, or that they would be perceived as “a chore”. Some stakeholders and interviewees related these feelings to a perception that society expects people to be sociable and independent.
“I don’t want people to think I need them more than they need me – it feels needy and embarrassing. I would never say such things to a friend who was feeling the same way as I do, but internally I feel a great deal of embarrassment for not being able to make it on my own.” – Diary entry (16-30 age group)
While some fears about what others would think were driven by general or specific perceptions of social stigma (see section 4.2 above), other interviewees were confident that they would not receive stigmatising responses and felt that internal thought processes must be driving their concerns. In some cases, interviewees felt these processes were compounded by wider mental health challenges (e.g., anxiety and self-esteem).
“No one’s ever going to say, ‘That’s so weird that you feel lonely. I think that’s such a strange thing to say.’… but I think that’s what anxiety does, it makes the idea of something far scarier than the thing itself.” – Interview participant (parent and 16-30 age group)
3.4 The impact of demographics on experiences of loneliness and loneliness stigma
The Loneliness Stigma evidence review found limited consideration of loneliness stigma across different demographic groups. It was suggested that future qualitative research could further explore stigma across different groups.
This section brings together findings from Chapters 2-4 to illustrate how demographics and life experiences can shape understandings of loneliness and loneliness stigma, before briefly outlining some thoughts on the benefits of taking an intersectional approach to understanding loneliness and the stigma around it.
Illustrations of how gender[6] can shape understandings of loneliness and loneliness stigma
- Comfort discussing sensitive issues such as loneliness. While some men had positive experiences of discussing loneliness with male friends and family, others had experience of male friends making light of their feelings. Some male interviewees and focus group participants felt that men were less comfortable talking about their feelings generally. This made some male interviewees more likely to seek support from women in their lives. These concerns were particularly apparent among younger men.
“I don’t think males get involved with it that much. I think they sort of get on with it, just block it out a bit. When you’re talking to people about it, you’ll have a minute or two-minute conversation and then they get you on to something else. I don’t think they find it comfortable to talk about really.” – Male interview participant (16-30 age group)
- The impact of gender stereotypes. Both male and female interviewees identified gender stereotypes which acted as a barrier to sharing feelings of loneliness. For example, some male interviewees expressed that feeling lonely and sharing emotions did not fit into society’s perception of masculinity (e.g., being “strong”) and felt that men could be perceived as “soft” for publicly sharing their experiences. However, some interviewees felt that this damaging view of masculinity was less prevalent than it used to be, making it easier for men to express their feelings. Gender stereotypes can also drive women to hide feelings of loneliness. While some men suggested that women were comfortable sharing these feelings, female interviewees described hiding these experiences due to fears of burdening others or concerns about how others would perceive them. It was particularly apparent that cultural roles and stereotypes ascribed to motherhood caused some women to hide feelings of loneliness. Some mothers perceived an expectation that they should feel satisfied by the connection they had with their children and worried that expressing feelings of loneliness would be seen as “ungrateful”. Mothers also felt that they were expected to focus on the needs of their children, rather than their own emotional needs. Both mothers and fathers chose not to share feelings of loneliness with grown-up children to maintain their role as the care giver.
Illustrations of how age can shape understandings of loneliness and loneliness stigma
-
Interviewees in the 16-30, parent and 40-60 age groups felt that loneliness was not recognised as being common among their age group. There were examples of participants receiving or anticipating surprise in response to sharing experiences of loneliness. Some younger interviewees felt that they “shouldn’t” feel lonely because they had other people around them and opportunities to socialise. This perceived lack of understanding made them less likely to share their feelings due to concerns that these would not be understood or would be dismissed. While focus group participants and interviewees recognised loneliness across all age groups, both groups also spoke about the “stereotypical” lonely person being older and physically alone. There was also a contested view that more constant loneliness – attached to social isolation – may be more common among older people, as younger people are more likely to have day-to-day contact with others.
-
In contrast, it was generally felt that loneliness among older people was well recognised, particularly in the media. However, older interviewees faced similar barriers to sharing feelings of loneliness as younger interviewees (e.g., concerns about the perceptions of others or feeling burdensome). Stakeholders also highlighted that the perception that loneliness is commonplace among older people can discourage this generation from seeking support due to a feeling that they should accept their experience.
-
Younger interviewees described social media as a societal driver of their loneliness, acknowledging its impact in enabling comparisons with others and decreasing face-to-face contact. However, there was a (stigmatising) perception among some focus group participants and older interviewees that younger people may feel lonely because they are too focused on social media and virtual (rather than face-to-face) communication.
Illustrations of how health and disability can shape understandings of loneliness and loneliness stigma
-
Some interviewees described their disability or health condition driving their experience of loneliness. As described in Chapter 2, experiences of living with a health condition or disability could lead to physical and emotional barriers to connecting with others. This included previous experiences of stigmatising views around disability, which led one interviewee to fear rejection from others.
-
Similarly, some interviewees highlighted their experiences of living with a health condition or disability as driving barriers to overcoming loneliness. It was often difficult for interviewees to separate out talking about loneliness with talking about the drivers of loneliness (e.g., health challenges). If the interviewee was not comfortable talking about their health, this also impacted the extent to which they felt able to talk about loneliness. This also caused some people in this situation to feel like a “broken record”, in that they were often speaking to friends and family about various negative experiences (e.g., health, loneliness, other challenges). Other interviewees living with mental health conditions felt that their condition made them more anxious about sharing feelings with others.
-
As highlighted in Chapter 3, interviewees often felt most comfortable talking about loneliness among those with similar experiences. For some interviewees, groups which brought together people with similar health experiences were safe places where issues like loneliness could be discussed openly and without fear of judgement.
Stakeholders and interviewees explained that in some cases, loneliness stigma can intersect with other stigmas or challenges to the detriment of people experiencing loneliness. For example, one stakeholder highlighted that among older people, factors such as sexuality, disability and employment history can exacerbate the impacts of loneliness stigma by creating additional challenges to connecting with others and sharing feelings. Some interviewees also explained how different facets of their lived experience (e.g., relationship breakdown, unemployment or disability) attracted a stigma which generally made it harder to talk about personal matters.
“Everybody here has a husband. I’m a single mum, so that automatically puts my back up because I’m going to get judged because I’m a single mum.” – Interviewee (parent)
The impact of these types of intersecting factors can be seen across Chapters 2-4. Altogether, this demonstrates the importance of applying an intersectional approach to viewing experiences of loneliness and loneliness stigma, rather than only concentrating on siloed groups (e.g., young people vs older people).
4.5 The impact of loneliness stigma
The key impact of both social (actual and perceived) and self-stigma, as reported by stakeholders and interviewees, is that it prevents individuals from wanting to talk about their feelings or seek help. Interviewees also commented that stigma, and the perceived impacts of stigma (i.e.,a lack of visibility around loneliness generally) could make them feel more alone in their experience.
Some participants felt that the social stigma around loneliness was gradually decreasing. Some stakeholders and interviewees suggested that the COVID-19 pandemic contributed to a reduction in loneliness stigma as social isolation increased for everyone – subsequently loneliness was presented as something that was more common. Focus group participants and interviewees also made comparisons between discussions of mental health, which were previously considered taboo, and the current conversation about loneliness. This gave participants hope that talking about loneliness would follow a similar trajectory. However, stakeholders, interviewees and focus group participants felt that despite progress being made, more needs to be done to address loneliness stigma. Steps that could be taken to reduce loneliness stigma are discussed in Chapter 5.
[1] Drawing on Link, B. & Phelan, J. (2001). Conceptualizing Stigma. Annu Rev Sociol, 27, 363–85.
[2] Drawing on Barreto, M., van Breen, J., Victor, C., Hammond, C., Eccles, A., Richins, M. T., & Qualter, P. (2022). Exploring the nature and variation of the stigma associated with loneliness. Journal of Social and Personal Relationships, 39(9), 2658–2679.
[3] Drawing on Barreto, M., van Breen, J., Victor, C., Hammond, C., Eccles, A., Richins, M. T., & Qualter, P. (2022). Exploring the nature and variation of the stigma associated with loneliness. Journal of Social and Personal Relationships, 39(9), 2658–2679.
[4] It should also be noted that participants may feel that societal expectations prevented them from sharing stigmatising views in a focus group setting, despite findings being reported anonymously. However, a number of measures were put in place to mitigate the risk of this bias. For example, group sizes were kept small, participants were prompted to discuss a variety of views and ground rules were put in place to create a safe space for discussion.
[5] The BBC Loneliness Experiment was a worldwide survey of 55,000 people aged 16 years and over, led by the BBC and the University of Manchester. More information about the survey can be found on the study webpage.
[6] Interview participants identified as either male or female. To the knowledge of the research team, no other gender identities (e.g., nonbinary) were represented within this research. Therefore, it should be recognized that these interviews may not capture the full breadth of views relating to gender.
5 Recommendations for tackling loneliness stigma
This section draws on perspectives of stakeholders (i.e.,professionals with experience tackling loneliness and loneliness stigma) and interviewees (i.e.,those experiencing loneliness regularly) to explore what can be done to tackle loneliness stigma.
The Loneliness Stigma evidence review identified that tackling loneliness stigma has involved action being taken at the national level to normalise loneliness. The review also found that those working directly with people experiencing loneliness had aimed to address self-stigma (i.e.,embarrassment or shame around loneliness) by carefully framing and targeting interventions, using sensitive language and providing the opportunity for open discussions around loneliness. However, the review identified no published evaluation of the impact of initiatives or approaches to tackle loneliness stigma, or evidence on whether (and how) normalising loneliness reduces stigma or enables more open conversations. It was suggested that further research could seek to better understand how interventions (including campaigns) can reduce stigma and explore how to capture impact going forward.
The approaches discussed in this Chapter build on the findings in the Loneliness Stigma evidence review, by exploring how campaigns (section 5.1) and wider actions to support discussions around loneliness (section 5.2) could tackle social (actual and perceived) and self-stigma. This Chapter also discusses a number of enablers and barriers to addressing stigma which apply to both campaigning and wider approaches. These include co-ordination between organisations and the language used around loneliness. The approaches and enablers to tackling stigma addressed in this Chapter are not mutually exclusive and can be used together to enhance efficacy.
5.1 National campaigning and messaging
Normalising loneliness
All participant groups suggested that it was important to highlight that loneliness is a normal emotion which can be felt by anyone. One stakeholder felt that normalising loneliness as something that everyone is likely to experience, even if some people experience less serious or transient loneliness, could help everyone who experiences loneliness feel less alone and less ashamed. This is because people experiencing loneliness would feel part of a large group, rather than a small minority. The stakeholder explained that this approach was grounded in research on mental health, which suggests that society will tend to focus on the most extreme form of emotions, leading to perceptions that the emotion is uncommon (i.e.,because only a small group suffer from the most extreme form of emotion). To counteract these perceptions, some mental health campaigns highlight that certain emotions (e.g., anxiety) operate on a spectrum to demonstrate that most people will have some experience of this emotion, but to varying degrees.
While focus group participants and interviewees discussed diverse and common experiences of loneliness, initial perceptions of loneliness can sometimes tend towards more “stereotypical” images which focus on smaller groups of people (e.g., those who are isolated). Interviewees also discussed feeling alone in their experience of loneliness. Even where these interviewees believed that feeling lonely was a common experience, the lack of visibility and recognition around loneliness led to them feeling alone and made it harder to share their feelings. Altogether, this demonstrates the need to normalise loneliness as a common experience.
While interviewees felt that it would be helpful to normalise loneliness generally (as above), some particularly felt that their experience of loneliness was not understood. This led interviewees to hide their feelings (see Chapters 2 and 3). Pertinently, it was expressed that seeing familiar examples of people who experienced loneliness would be helpful (e.g., people of the same age or with similar life circumstances). In particular, this should include examples of people who feel lonely despite having regular connection with others. Views of interviewees also suggest that campaigning should not make assumptions about which experiences of loneliness were most difficult or needed support.
“Just letting people be aware that it’s a thing - It’s okay to feel lonely when you’ve got people around you or when you’ve not got people around you.” – Interviewee (16-30 age group)
As well as ensuring that campaign imagery is inclusive and diverse, stakeholders suggested that life circumstances could be captured by focusing on the drivers of loneliness. For instance, emphasising the connection between loneliness and a variety of life events and circumstances, such as parenthood, health or employment changes.
Case study
A Co-op Foundation online campaign asked young people to share similar experiences of loneliness, so participants could easily engage with stories that may be relevant to them. For example, one online space was for stories of those who felt different from their peers, while another was for those who did not have the financial means to socialise. This campaign received a positive reception and was thought to be successful because it acknowledged the linked drivers of loneliness and enabled young people to talk about the specifics of their experience. This included highlighting some sub-group experiences among young people. For example, the space for those who felt different from their peers attracted a lot of stories from the LGBTQIA+ community. This type of action has potential for addressing some of the concerns highlighted by interviewees in Chapter 2, relating to how their particular experiences of loneliness are not understood (e.g., parents), along with normalising loneliness more broadly.
Interviewees felt that normalising all experiences of loneliness would help them feel less alone in their experience, help to remove internal shame associated with loneliness and lead them to anticipate more positive reactions from others. This demonstrates that normalising loneliness has the potential to tackle both self-stigma and perceived social stigma. Normalising loneliness also has the potential to target some of the more “stereotypical” perceptions of loneliness presented in this research (e.g., perceived links between loneliness and old age or social isolation), thereby tackling actual social stigma.
“It removes the shame, it removes the taboo, because you understand that you’re not on your own feeling about it. If no one talks about it, you don’t know how many people feel that way, so you feel like it’s only you, and you feel like others might laugh at you, judge you, think you’re strange, think you’re weak, all of these things, whereas if you know that so many other people are feeling that way, it removes that shame… You think, oh, actually, it wasn’t just me, and I don’t think those horrible things about that person who’s just admitted that. I think that’s really brave that they did that” – Interviewee (parent)
“If I said to someone, ‘I’m lonely’, they wouldn’t automatically think, she’s got no friends. Why has she got no friends…They would think, I hope she’s all right.” – Interviewee (parent)
Reducing the negativity around loneliness
As explained in Chapters 3 and 4, interviewees felt embarrassment and shame around loneliness. This was due to negative perceptions about their loneliness, both internally and from other people. Interviewees and stakeholders suggested that future campaigns needed to demonstrate that loneliness could happen to high status (e.g., celebrities) and successful people (e.g., workforce leaders). It was felt that a key impact of this would be to challenge internal negative perceptions about loneliness (i.e.,self-stigma), particularly around self-blame and associations between loneliness and negative characteristics. Stakeholders felt that campaigning on mental health (e.g., involvement of celebrities) provided good evidence that these types of strategies would work well to help normalise loneliness.
As explained in Chapter 4, interviewees perceived a general negativity around loneliness. Presenting loneliness as “normal” and removing negativity around these feelings would help people to manage this experience, in the way(s) best for them, without shame or embarrassment. It is important to recognise that removing the negativity around loneliness does not mean accepting loneliness as something that cannot be supported, managed and/or overcome. Interviewees who felt that loneliness should be perceived as a normal emotion still felt that more actions could (and should) be taken to support those experiencing it. Similarly, stakeholders reflected that normalising loneliness was the first step in encouraging people to speak up and ask for support. Depending on the individual’s needs and wants, interviewees suggested that this support be focused on increasing social connection or managing feelings of loneliness.
“I think more people would know it’s ok then…I think it would be positive, to show people that life isn’t as rosy as people try and make it out. People do have bad days and it’s not bad if you feel like that sometimes.” – Interviewee (parent)
Given the perceptions identified in Chapters 2 and 3 (of those with regular and little/no recent experience of loneliness), other considerations for national messaging involve avoiding narratives which are blaming or suggesting that loneliness is easily overcome. This could help tackle actual and perceived social stigma and self-stigma. Messaging which either tackles the stigma around feeling burdensome or highlights alternative forms of support (i.e.,professional services rather than friends and family) could also support people to share feelings of loneliness, as this was raised as a concern across all age groups.
Targeting and tailoring campaigns
While it was felt that campaigning should be inclusive of different experiences of loneliness, interviewees and stakeholders suggested targeting or tailoring campaigns in the following ways:
-
Stakeholders suggested that there would be a need to target groups who are less likely to be reached by mainstream campaigning. In particular, those who are less likely to have regular access to digital technologies (e.g., older people and those living in areas of higher deprivation). One stakeholder used billboards and school workshops in areas of higher deprivation to complement digital campaign work.
-
Stakeholders also suggested that given the breadth of experiences, campaigns will need to be targeted and tailored to ensure that the messaging is relevant to people with different experiences of loneliness. This approach would require recognising that (as explained in Chapter 4) loneliness and loneliness stigma can be driven by different factors even within one demographic group (e.g., older people). One example of how this can be done is the campaign for younger people referenced above, which highlighted different drivers of loneliness (e.g., feeling different from others and financial barriers).
5.2 Creating safe environments to discuss experiences of loneliness
Discussing loneliness with peers
As well as using campaigns to target loneliness stigma, wider actions could mitigate the impact of this stigma by supporting people to discuss their experiences. In particular, interviewees felt it would be useful to have more environments where they could discuss loneliness with others who experienced it. One suggestion was that local support groups could bring people together and provide a non-judgmental space to discuss experiences of loneliness.
“If I had to speak about my loneliness in a group discussion, I feel like I would be happy to do that, because there’s other people feeling a certain way and they would explain their feelings and how we can tackle that together” – Interviewee (parent)
However, there was a difference of opinion as to what form of group would best serve people’s needs. Some interviewees felt it was important to ensure these groups were inclusive of a range of people, including all age groups. In particular, one view was that groups targeted at older or retired people were off-putting as individuals did not always identify with the stereotypes associated with those labels (e.g., identifying as being ‘older’). However, as highlighted in Chapter 3, other interviewees felt most comfortable discussing experiences of loneliness with others in a similar context (e.g., due to health conditions or parenthood). In these cases, interviewees felt they were more inclined to attend a group with others with similar life experiences. For example, one interviewee felt that a cancer support group environment allowed them to be more open and honest about their experiences, as others would empathise rather than offering less-welcome reactions (such as pity).
“You’re not pitying each other, you’re just talking about it, and it’s a relief when someone else gets it without having to explain” – Interviewee (parent)
Stakeholders suggested that encouraging conversations around loneliness within organisations and institutions could help people to discuss their feelings and further normalise the experience of loneliness, thereby reducing actual and perceived social stigma and self-stigma. Some stakeholders felt whilst public communication about loneliness (e.g., campaigning) was important, taking steps to translate this messaging into everyday connections and conversations was really key to overcoming stigma. Drawing on learnings from actions taken to normalise mental health discussions, it was suggested that two key steps should be taken to encourage openness around loneliness:
-
Encouraging workplace conversations about loneliness. One stakeholder suggested that conversations about loneliness in the workplace could be encouraged by leadership teams promoting openness around the subject and speaking about their own experiences of loneliness.
-
Promoting conversations about loneliness in schools. Both stakeholders and interviewees (from all age groups) felt that encouraging discussion of loneliness in schools was important to help to normalise these conversations from a very young age and provide children with the tools to discuss their experiences. No interviewees mentioned experiences of discussing loneliness in the classroom.[1] However, one young interviewee had experience of discussing/learning about mental health in a classroom setting, and felt that similar actions would be helpful to encourage conversations around loneliness.
Discussing loneliness with professionals
Stakeholders and interviewees felt that because loneliness was not normalised, there was a lack of easily accessible information on support. For example, some interviewees were unsure whether their GP could help or signpost them to support. It was felt that national campaigning could help signpost relevant options, ideally through a centralised website or service. Stakeholders also suggested that healthcare practitioners and wider services (e.g., GPs and Job Centre Plus) should be encouraged to provide or refer individuals for loneliness support to increase the type of organisations involved in identifying and referring those who were feeling lonely to available services. This research suggests that involvement of wider organisations may require national support and training in the following areas:
-
Approaching discussions of loneliness. Interviewees suggested that training might help professionals to identify loneliness and offer the appropriate support, especially to those who do not feel comfortable asking for it. As explained in section 5.3, some support organisations have tried and tested methods of approaching these types of conversations, which could inform the work of wider services.
-
Advice for people experiencing loneliness. Services should consider the advice being given to service users to ensure this is person-led, flexible to individual needs and does not perpetuate stigma. As explained in Chapter 3, advice about overcoming loneliness can be perceived as unhelpful. Furthermore, it can prevent the individual reaching out again if it is overly simplistic or does not consider the person’s needs and circumstances. In some cases, people will want support to improve their level of social connection. However, others may need a space to discuss their feelings without fear of shame or judgement. Interviewees also felt there was a strong need for clarity around the distinction between loneliness and mental health problems, as conflating the two could result in the wrong type of support being sought or provided. For example, one new mum felt that her loneliness was misdiagnosed as postnatal depression by healthcare professionals. Another interviewee felt that proposed solutions often failed to recognise that loneliness was not just about being physically alone, suggesting that support tended to focus on the number of social connections rather than managing other feelings (e.g., disconnection).
5.3 Enablers and barriers to addressing loneliness stigma through campaigning or wider approaches
The language around loneliness
It is important that those involved in campaigning and providing support services carefully consider the language used around loneliness. There were mixed views among stakeholders about how the term ‘loneliness’ should be used. Some stakeholders felt that the term was only suitable in a policy and research context, suggesting that a softer term with less negative connotations should be used in a service environment. These stakeholders felt that people were more comfortable sharing their experience if they were not directly asked about loneliness. Ideally, it was expressed that service staff should aim to use the language used by the service user. Other stakeholders felt the word ‘loneliness’ needed to be used to normalise the experience. However, these stakeholders still felt that the topic of loneliness needed to be approached sensitively. This could be done in two ways:
- Not leading with questions about loneliness. Some stakeholders felt that it was helpful to start the conversation with wider questions on social needs and building relationships, rather than directly asking someone if they were feeling lonely at the first point of interaction. The types of wider question included “Who would you reach out to if you needed help?” or “Would you like support to connect with your community?”.
“We’ve got anecdotal evidence from […] services that it takes a long time for people to feel confident to say, ‘Yes, I’m lonely’. There is a place for the word ‘lonely’, but I don’t think it should be headline stuff. I think it’s almost like it’s a bit further down the narrative, so that people don’t get bombarded with that negativity immediately.” – Stakeholder
- Using the word loneliness as part of a wider narrative. One stakeholder provided an example of a scheme which was marketed using the word ‘loneliness’. The marketing successfully attracted service users, however the stakeholder suggested that it was important that they also used a range of words like “connect”, “relationships” and “support networks”. This approach recognised that different people are likely to identify with different language around loneliness. Another stakeholder suggested using the term ‘loneliness’ in campaigns but breaking it down into smaller concepts or messages that people can engage with, rather talking about loneliness as a broad concept.
As highlighted in Chapter 3, some interviewees and focus group participants felt they did not have the language to discuss loneliness. Some of these participants felt that normalising loneliness would naturally increase discussions around this topic, making it easier to have these conversations. However, it was notable that focus group participants (with little/no recent experience of loneliness) who did feel comfortable discussing loneliness often had some prior professional experiences which had developed their communications skills around sensitive topics. Altogether, this suggests that those organising campaigns or supporting peer to peer discussions may want to provide some tools and language for those who want to discuss their experiences or support others.
Stakeholders also felt that the language used to talk about loneliness by campaigns and support services needs to be considered to ensure it does not perpetuate negative associations, and therefore stigma. Stakeholders suggested avoiding terms, such as ‘tackle’ and ‘eradicate’, when referring to loneliness. By doing so, loneliness is presented as a negative emotion, rather than something that is experienced by everyone at some point. Interviewees also felt that messaging to normalise loneliness should emphasise that “it’s okay” to feel lonely.
“Tackle’ is a negative word – this word needs softening to take the stigma away from it.” – Stakeholder
Coordination across organisations to enable sustained effort
Stakeholders reflected on the positive outcomes of the Government’s loneliness campaigns so far, which they felt had encouraged people to talk about loneliness. However, it was suggested that a longer and sustained effort was required to achieve a lasting impact. For example, stakeholders referred to the long-term efforts and impacts of mental health campaigning, in particular the Time to Change campaign. Stakeholders highlighted that campaigns around loneliness tend to take place during the winter, because loneliness is commonly associated with the colder months. While stakeholders felt that this was necessary, they also suggested that sustained effort throughout the year would be required to change societal attitudes. Stakeholders acknowledged the challenges involved in long-term campaigning, such as costs and maintaining the consistency of the messaging. One suggestion to keep the messaging sustained throughout the year was for the sector to coordinate campaign activity, to ensure that different campaigns took place throughout the year. While not suggested by stakeholders, further coordination could also ensure that messaging is similarly focused and consistent.
“You need sustained efforts, that’s the biggest barrier. Government’s campaign is probably the longest one, which is brilliant, but it’s not like everyone’s seeing it or the targeted people are constantly seeing these messages.” – Stakeholder
Stakeholders also highlighted wider opportunities for coordination between organisations. This included working closely with partners “on the ground” to design campaigns and support with accessible and compelling messaging. For example, one stakeholder received support to design a campaign for young people from a partner with strong links with youth workers across the UK. This provided helpful insights into how to best tailor the content and mode of delivery to the target group. As explained above, a range of different demographic factors and life experiences intersect to inform individual lived experiences of loneliness. Organisations who work closely with particular groups will be best placed to identify different needs and experiences within each group. These may be the types of factors highlighted in this report (i.e.,gender, age, health and disability), or may be informed by more specific knowledge about the group in question. For example, one stakeholder provided examples of groups of older people whose experience of loneliness and stigma may require tailored messaging, including older carers, veterans and LGBTQIA+ groups. These considerations could apply to those looking to support discussions around loneliness (e.g., through peer groups) as well as campaigning. As well as coordination at the national level, stakeholders and interviewees suggested that coordination with more local organisations (e.g., workplaces, schools and media outlets) would help to expose everyone to messaging about loneliness, therefore normalising loneliness in different everyday areas of life and subsequently reducing social and self-stigma.
Measuring and demonstrating the impact of loneliness campaigns and other services
As highlighted above, stakeholders had found it challenging to evidence the impact of campaigning and other initiatives. In particular, stakeholders found it difficult to measure changes in loneliness linked to service provision and attribute any changes in loneliness to particular campaigns.
Stakeholders noted that inherent challenges with national measures of loneliness and stigma made it difficult to monitor changes in experiences of loneliness. While some stakeholders used standard approaches such as the ONS measures (consisting of the UCLA measures and/or the direct measures of loneliness) with service users, others felt that these types of questions (e.g., “how often do you feel isolated?”) were too negative and/or intrusive. This tended to be guided by the opinions of frontline staff, some of whom were not comfortable asking the ONS questions.
“I think, nationally, we’re not very good at collecting data. There are loneliness scales, which aren’t diagnostic tools, but frontline staff are really reluctant to use them because of the stigma attached to asking about loneliness. We generally don’t know how people are. We have anecdotal softer data, but we don’t have population-wide measures in place, and that’s not just our organisation. I’d say that’s collectively. There’s no commonality in how organisations collect data.” – Stakeholder
In these cases, stakeholders reported using self-developed measures to identify potential service users. These self-developed measures aimed to be less intrusive and use more positive language. For one stakeholder, this included questions which focused on how people would respond to feeling lonely, such as “When you’ve felt lonely, have you talked about it?”. Another stakeholder referred to measures developed by the Campaign to End Loneliness which used more positive language (e.g., “do you feel included?”; “do you feel that you have companionship?”).
There were additional challenges associated with measuring the impact of national campaigns. Some stakeholders had collected qualitative feedback from their target audiences (e.g., through interviews or conversations) or were able to measure the level of engagement with the campaign (e.g., number of responses submitted to an interactive campaign). However, it was felt that robustly measuring national campaign success would require more widespread quantitative data collection involving people who viewed the campaign to understand changes in feelings of loneliness over time. It was also felt this type of quantitative research would need to be carried out alongside in-depth qualitative research which explored why and how any changes occurred.
5.4 Could reducing stigma reduce loneliness?
As explained above, tackling loneliness stigma would require action to normalise loneliness and remove negative associations at a national level, while people experiencing loneliness are also supported to share their experiences (with peers and professionals). Altogether, it was felt that these actions could help people experiencing loneliness feel less alone and more able to share their feelings and seek support, if this is something they want to do. In particular, stakeholders hoped that these actions could help people seek support earlier before feelings of loneliness become overwhelming.
“If it’s taught that it’s okay, we would start to be okay in a weird way because we know we’re not alone; that people do feel that” – Interviewee (16-30 age group)
“If you reduce stigma, you will reduce loneliness, because more people would be willing to ask for help, whether that’s their friends and family or services, before they enter a crisis point” – Stakeholder
However, as discussed in Chapter 3, stigma is not the only barrier to overcoming feelings of loneliness. Even if stigma were reduced, practical challenges to socialising would exist (e.g., cost, health barriers and childcare). Similarly, stakeholders highlighted that service provision (e.g., befriending services) may need to be extended if significantly higher volumes of people were to access support, which would have cost implications. However, this research suggests that the actions above still have the potential to help people feel less alone and more able to manage their experience of loneliness, even where it cannot be overcome.
5.5 Overview of recommendations to tackle loneliness stigma
This research has explored how people understand loneliness from an individual and societal perspective, as well as the barriers to overcoming and managing this experience. This has demonstrated how loneliness stigma (actual and perceived social stigma and self-stigma) can present a direct barrier to managing loneliness, which is experienced alongside wider challenges for those who would like to share and/or seek support for their feelings (e.g., a lack of language around loneliness). These findings have led to six recommendations, which are summarised in the graphic below and the Executive Summary of this report.
[1] Loneliness was included on the curriculum in 2018, and therefore would only have been experienced by the youngest interviewees (if at all).
Appendix A
Methodology
Given the exploratory and sensitive nature of the research aims, the study used a qualitative approach. This included:
-
Six scoping interviews with professional expert stakeholders
-
Forty in-depth interviews with interviewees and loneliness stigma. All in-depth interviewees also completed up to five online diary entries over the course of two weeks prior to the interview
-
Three focus groups each comprised of eight participants who had little or no recent experience of loneliness
Sampling
As is the quality standard in qualitative research, the aim was not to be statistically representative of the wider population, but to sample the range and diversity of experiences and circumstances relevant to research aims within the target population.
In-depth interviews and diary entries
Participants were selected based on the following primary sampling criteria:
-
Regular recent experience of loneliness (based on the participant’s score on the ONS loneliness measures) [1]
-
Experience of loneliness stigma (based on a score developed for the BBC Loneliness study)[2]
-
Key life stages identified in prior research linked with loneliness (young adults (16-30 years old), parents of young children, middle age, retired)
-
Gender
Secondary selection criteria, which we also monitored, involved: ethnicity, socioeconomic status, disability, and relationship status and household composition.
Focus groups
Participants were selected based on the following primary sampling criteria:
-
Little or no recent experience of loneliness (based on the participant’s score on the ONS loneliness measures)[3]
-
Age and life stage, (16-34 years old, 35-64 years old, 65+ years old)
-
Gender
Secondary selection criteria, which were also monitored, involved: ethnicity and socioeconomic status.
Recruitment
Professional stakeholders
A list of possible expert stakeholders or organisations were identified by NatCen and RSM, based on the findings from the Loneliness Stigma Evidence Review. Some contact details were provided by DCMS, while other organisations were approached independently by RSM.
Fieldwork with participants experiencing loneliness
Research participants were recruited via a trusted recruitment agency - Criteria. Criteria contacted potential participants from their databases and conducted a screening process to ensure that participants were eligible to be included in the research. These participants were invited to take part in an interview and complete diary entries.
Focus groups
Research participants were recruited in the same way as interviewees by Criteria and were selected following a screening process. These participants were invited to take part in one of the focus groups.
Achieved sample
The achieved sample against primary section criteria for interviews and focus groups are shown in table A.1 below.
| Criteria | Interviews and diary | Focus group | |
|---|---|---|---|
| Life stage | Young adults | 11 | - |
| Parents of young children | 10 | - | |
| Middle-aged | 12 | - | |
| Retired and 65+ | 10 | - | |
| Age | 16-34 | - | 8 |
| 35-64 | - | 8 | |
| 65+ | - | 8 | |
| Gender | Male | 17 | 12 |
| Female | 23 | 12 |
Fieldwork
Interviews with professional stakeholders were conducted in February and March 2023 and each lasted up to 45 minutes.
Interviews and diary entries for interviewees were also conducted between February and March 2023 and each lasted up to 60 minutes. These participants also completed an online diary over a two-week period prior to their interview. Participants were provided with a personal web link to their diary and guidance suggesting they concentrated on the interactions they had during the day, any experiences of loneliness and their inclination to share those feelings with others. The diary provided participants with an opportunity to self-reflect on their experiences prior to the interview and were used to stimulate discussion and understand day-to-day experiences.
Focus groups were conducted in March 2023. Focus groups lasted up to 60 minutes and were conducted online with an experienced facilitator and additional staff for technical support.
Interviews and focus groups were carried out by telephone or online, using topic guides agreed with DCMS.
Ethics
Ethical approval was sought via NatCen’s ethics committee, which complies with UK Research and Innovation[5], Government Social Research[6] and Social Research Association[7] guidelines and standards. Particular attention was paid to:
-
Informed consent to take part. All research participants were made aware of the nature of the study and the type of topics to be covered before being asked to agree to take part. At all stages it was stressed in writing and verbally that participation was voluntary. For the fieldwork with members of the public, participants received a study information sheet, which set out the purposes of the research along with an explanation of what taking part would involve. Potential participants for the interviews and focus groups were screened by our recruitment agency to ensure they met criteria for inclusion and were happy to take part. For interviewees, consent to take part was also audio recorded following reiteration of key information about the research prior to the start of the interview. Participants asked at the end of the interview if they were happy to be quoted in the report.
-
Sensitive handling of the topics. The nature of the topic meant that there was a risk that participants would find the interview or diary process upsetting. This was particularly the case for the interviews and diary entries with participants experiencing loneliness. The study was conducted by experienced researchers who met prior to the start of the fieldwork to discuss potentially upsetting parts of the interview and how these should be handled. Researchers were led by participants and diary entries in terms of the language used to describe ‘loneliness’. Participants were told they did not have to talk about topics they did not want to, could take a break, reconvene the interview at another time or could withdraw from the interview. They were also told they could have someone with them during the interview to support them if they wanted. All participants were sent a leaflet after the interview listing helplines and organisations they could contact if the interview had raised difficult issues for them. Interviews were generally not conducted on a Friday, allowing the participants to access support if needed on the following day, as some support organisations tend to be closed during weekends.
-
Disclosure. Participants were advised that the research team may have to disclose information from the interview, diary entry or focus group to someone else if we believed they or someone else close to them was at risk of serious harm (in line with NatCen’s Disclosure policy).
-
Ensuring inclusivity of participation. In addition to sampling a diverse group of participants, every effort was made to ensure that participants could take part in ways most suitable and convenient for them. They were given the opportunity to take part by phone or video interview using MS Teams. Interviews took place during daytime and evenings. An incentive was offered for the interview and the focus group as a thank you and a recognition of the participant’s time. An additional incentive was offered for online diary entries, recognising the additional work involved. Participants who struggled to complete all five diary entries were given the option of completing fewer entries or were allowed more time to complete them.
Analysis
Interviews and focus groups were recorded (with consent) and transcribed. We used NatCen’s framework approach to analyse the interviews and focus group data. This approach facilitates robust qualitative data management and analysis by case (i.e.,interview or focus group) and theme. In the framework each row represented one interview or focus group and each column represented a topic of relevance to the research questions. Relevant information from each interview or focus groups was written into the corresponding cell. This grouped information around each research question, enabling the research team to assess the evidence relevant to each question. Findings have been integrated across the three work strands described above and are presented thematically.
[1] ONS. (2018). Measuring loneliness: guidance for use of the national indicators on surveys.
The ONS loneliness guidance includes both direct and indirect measures of loneliness. Participants were asked to rate how often they lacked companionship, felt left out or felt isolated from others on a scale of 1-3 as an indirect measure of loneliness. We screened in participants who scored more than 6. We also asked them how often they felt lonely as a direct measure of loneliness and screened out those who answered “never” to this question.
[2] Barreto, M., van Breen, J., Victor, C., Hammond, C., Eccles, A., Richins, M. T., & Qualter, P. (2022). Exploring the nature and variation of the stigma associated with loneliness. Journal of Social and Personal Relationships, 39(9), 2658–2679.
We used this study to identify participants who experienced or perceived loneliness stigma. Participants were asked to rate on a scale 1-7 how strongly they agreed with feeling ashamed, being too embarrassed to admit to others or not wanting to talk to other people about feeling lonely. They were also asked if they thought society held negative views about people who are lonely. Participants with an average score over 4 on questions 1-3 and/or a score of 5 or above on question 4 were included.
[3] For the focus group, we included participants with a score of 3 and under to the questions on how often they lacked companionship, felt left out or felt isolated from others. We also excluded participants who answered “often/always” and “some of the time” to describe how often they felt lonely.
[4] Please note that the total numbers in this column exceed 40 because some interviewees are both young adults and parents
[5] UK Research and Innovation (2022). Policy on the Governance of Good Research Practice.
[6] Government Social Research (2021). Ethical Assurance for Social and Behavioural Research in Government.
[7] Social Research Association (2021). Research Ethics Guidance.