Key findings from analysis of domestic homicide reviews: October 2019 to September 2020 (accessible)
Updated 31 October 2024

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/key-findings-from-analysis-of-domestic-homicide-reviews/key-findings-from-analysis-of-domestic-homicide-reviews
September 2021
Prepared for the Home Office by Analytics Cambridge and QE Assessments Ltd
Responsible author: Richard Potter, Independent Researcher, B.Sc., M.Phil., at Analytics Cambridge Contact: info@analyticscambridge.co.uk
Reviewed by: Davina James-Hanman, OBE, Independent Consultant at DJH Associates; Simon Kerss, Lecturer in Criminology, Anglia Ruskin University; Gaynor Mears OBE, MA, BA (Hons), AASW, Dip SW
Note: Some figures in the pdf version of this document have not been transferred into html. When this has happened, the information has been added to lists or tables.
1. Executive summary
Statistics from domestic homicide reviews
This report summarises information from domestic homicide reviews (DHRs) for the 12 months from October 2019. DHRs are multi-agency reviews, commissioned by community safety partnerships, into the deaths [footnote 1] of adults which may have resulted from violence, abuse, or neglect; by a person to whom they were related or with whom they had an intimate relationship, or where they were a member of the same household.
This document is intended to make available key information and share learning. It summarises areas which reviews identify can be improved and also their recommendations.
Overview
- This report presents key information from 124 DHRs which were reviewed by the Home Office quality assurance process for the 12 months from October 2019.
- Close to three quarters of these are deaths which occurred in 2017 or 2018.
- Across all the reviews there have been 127 victims (of which 14 were, or appeared to be, victims of domestic abuse who died by suicide).
- The age of victims was from under 18 to 94 (the average was 41 years old). The oldest perpetrator was aged 89, and the average age was 40).
- Eighty percent of the victims were female and 20% were male. For perpetrators, 83% were male and 17% female.
- There were dependent children in 52% of the households where the victim was aged under 60.
- Analysing the relationships between the victims and perpetrators shows that for 73% of the victims the perpetrator was a partner or ex-partner. For 27% of the victims there was a family relationship between the victim and perpetrator.
Victims
- Sixty-one percent of victims had a vulnerability, with 34% having one vulnerability and 27% having more than one.
- Of the vulnerabilities, 34% were mental ill-health, 28% were problem alcohol use and 22% were illicit drug use.
- For 26% of those with a mental health vulnerability this was depression, 16% had suicidal thoughts. Fourteen percent had attempted to take their life by suicide and, with 14% also, the vulnerability was low mood or anxiety.
- Forty-six percent of the victims had been the target of a perpetrator previously, almost always their previous partner.
- In 64% of the DHRs aggravating factors were identified, with coercive control being the most common.
Perpetrators
- Seventy-one percent of the perpetrators were considered to have a vulnerability and the most common were: illicit drug use, mental ill-health, and problematic alcohol use.
- Thirty one percent of perpetrators were affected by mental health issues and for 23% this was depression and 21% were suicidal thoughts.
- Approximately 60% of perpetrators were indicated to have a previous offending history. Of these three quarters had abused previous partners and one third family members. This includes a small proportion who had abused both previous partners and family members.
- Of the court verdicts, 62 perpetrators were sentenced for murder and 25 for manslaughter. Thirteen were deemed to have diminished responsibility or be unfit to plead.
Key themes
This project has analysed in more detail a sample of 50 of the DHRs. The areas identified for improvement are:
- contact: the need for greater contact with victims and recognition that the perpetrator can control the victim’s contacts with agencies
- assessment: the need to improve risk assessments, carer’s assessments, or mental health assessments
- records: information can be missing and not shared between agencies
- support: for staff whose work involved cases of domestic abuse and cases where support for victim was not identified or, where the need for support was identified, but there was no plan to provide it
- information: the need to improve information sharing between agencies, to hold accurate information and then use it effectively to manage risk
- risk: the right risk level needs to be identified, with information held by other agencies included.
- referrals: are not always made when needed
- training: the need to update training and make it accessible
- policy: occasions when action taken was not in line with policy and there were agencies without a domestic abuse policy
Recommendations in domestic homicide reviews
- From the recommendations in the DHRs, 25% were for partnerships (typically community safety partnerships), 24% for health organisations (including clinical commissioning groups, GPs, hospitals, and mental health trusts) and 13% for the police.
- Twenty-eight percent of the recommendations were to review existing practice.
- Twenty-six percent of the recommendations were to raise awareness, of which 72% were recommending raising awareness about domestic abuse to staff.
- Sixteen percent of the recommendations concerned information: including the quality of information and sharing information between agencies.
2. Introduction
1. This report summarises key findings from the domestic homicide reviews (DHRs) to inform policy development and provide learning in preventing domestic homicide.
2. A DHR is a multi-agency review, commissioned by a community safety partnership, of the circumstances in which the death of a person aged 16 or over has, or appears to have, resulted from violence, abuse or neglect by a person to whom they were related or with whom they were, or had been, in an intimate personal relationship, or a member of the same household. The purpose of a DHR [footnote 2] is to:
- establish lessons to be learned from the domestic homicide for the way local professionals and organisations can work individually and together to safeguard victims
- identify lessons both within and between agencies, how and within what timescales they will be acted on, and what is expected to change as a result
- apply the lessons to service responses
- prevent domestic violence and homicide and improve service responses for all domestic violence and abuse victims and their children by developing a co-ordinated multi-agency approach to ensure that abuse is identified and responded to effectively at the earliest opportunity
- contribute to a better understanding of the nature of domestic violence and abuse
- highlight good practice
3. The review process does not take the place of the criminal or coroner’s court.
4. This report is of 124 domestic homicide reviews (DHRs) which have been through the quality assurance process set out by the Home Office [footnote 3] between October 2019 and the end of September 2020. The identification of themes and summary of recommendations is from 50 randomly selected DHRs from this total.
5. The complex nature surrounding domestic homicide is reflected in the 124 reviews. Within these there are 127 victims: in two reviews there is more than one victim. [footnote 4] The term victim here refers to those who have died - though the impact of domestic homicide is greater than only the victims who have died as it extends to family members, children, friends and colleagues.
6. Of the 127 victims 14 are people who died by suicide.
7. In the reviews there are 109 perpetrators, [footnote 5] of these 11 died by suicide after the homicide.
8. The report is structured to give:
a) information on trends, location, age and gender of victims and perpetrators
b) characteristics or experience of victims in terms of their vulnerability, mental health and whether they had been the target of an abuser before
c) characteristics or experience of perpetrators, including vulnerabilities and mental health, any previous offending history, and details of criminal charges
d) themes highlighting areas for improvement
e) a summary of recommendations made in the reviews
f) contributions from and support for families in the DHR process
g) the most common reasons for the Home Office Quality Assurance Panel requiring DHRs to be resubmitted
9. The main source of information is the management information reports (MIRs) that reviewers were required to complete. The questions for these are shown in Appendix 1. There is variation in the amount and quality of information from the MIRs and also from the domestic homicide reviews. As a consequence, work has been carried out to maximise the information for analysis, more detail is given in Appendix 2. Appendix 3 shows the number of answers for each question and also the number “not known”: unless stated otherwise the percentages given are of the total known. Where information was missing from the MIR the DHRs were searched for this information.
10. The chapters on the themes and recommendations are based on a random sample of 50 reviews (Appendix 4 gives more information).
11. This report is a successor and refresh of that published in December 2016. [footnote 6] Where possible, this review has employed the same method to capture and analyse the data.
3. Domestic homicide reviews: trends, location, and demography
12. This chapter shows national trends in domestic homicides. It then describes information from the domestic homicide reviews on the dates of death, and the time between the death and when the reviews were submitted to the Home Office. This is followed with the number of reviews in each region. The chapter then provides information on the victims and the perpetrators including their age, gender and relationships.
Trends in domestic homicides in England and Wales, 2009/10 to 2019/20
13. For context, Figure 1 shows the number of victims of domestic homicide from 2009/10 to 2019/20. This has fallen from 152 in 2009/10 to 114 in 2019/20.
Figure 1 Number of domestic homicides in England and Wales: 2009/10 to 2019/20
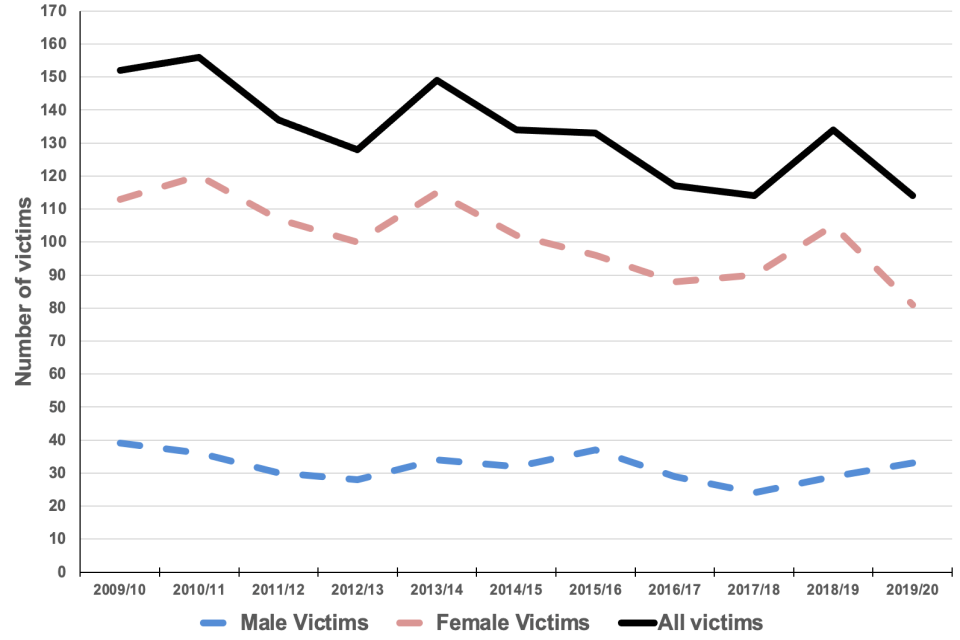
Figure 1 Number of domestic homicides in England and Wales: 2009/10 to 2019/20
Source: Homicide in England and Wales: year ending March 2020. Office for National Statistics, appendix tables Table 12A, where domestic homicide is a category used.
Domestic homicide reviews: date of death of victim
14. The DHRs in this report are those which have been reviewed by the Home Office Quality Assurance Panel from October 2019 to the end of September 2020. The time between the date of the victim’s death and the completion of the review is influenced by a range of factors:
- contact with family members and others to enable them to contribute to the review
- completion of the criminal trial
- community safety partnership meetings; report sign off and submission to Home Office
- the coroner’s inquest
- the quality assurance process through Home Office
15. Figure 2 shows the years in which the victims died, showing that almost three quarters of the deaths in this report were in 2017 and 2018. Reflecting on this, the average time between the date of death and submission of report to the Home Office Quality Assurance Panel is two years. [footnote 7] Seventy-two percent of the reports have been submitted within two years or less from when the death occurred.
Figure 2 Year of death of victims in DHRs
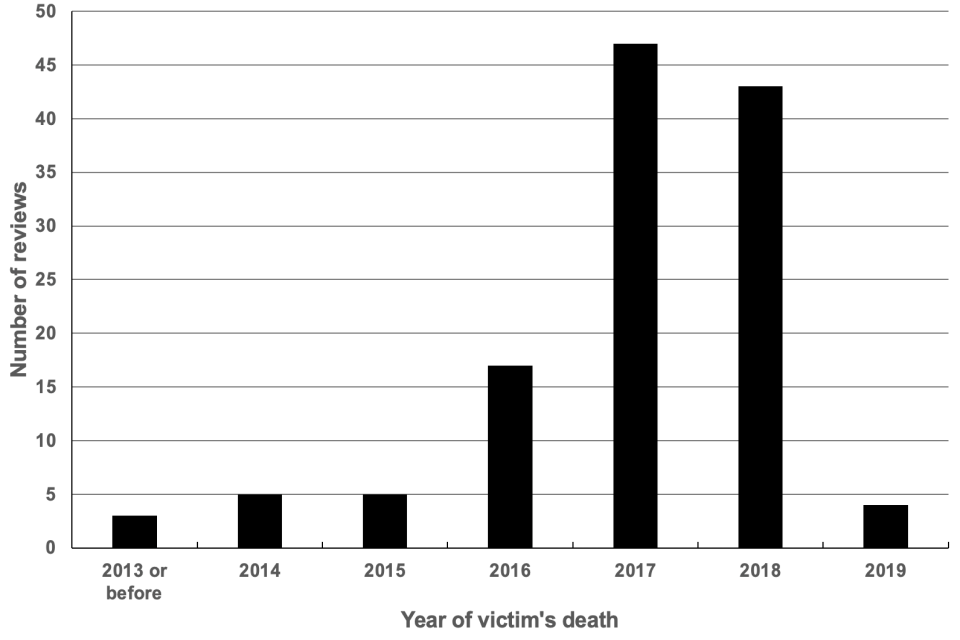
Figure 2 Year of death of victims in DHRs
Location of the deaths of victims
16. The death of the victims took place in 88 local authorities [footnote 8] in England and seven in Wales. Of the 88 local authorities in England there were six with three reviews, 14 with two reviews and 68 with one review. In Wales there was one local authority with two reviews and six with one review each.
17. For the place where the death occurred, in 83% this was the victim’s home and for four percent the location was the place where the perpetrator lived. Other locations included roads, hospitals, and open space.
18. Table 1 shows where the deaths of victims in the DHRs occurred by region in England and in Wales. [footnote 9]
Table 1 Number of domestic homicide reviews by region or nation
| Region / Nation | Number of reviews |
|---|---|
| North East | 6 |
| North West | 9 |
| Yorkshire and the Humber | 12 |
| East Midlands | 12 |
| West Midlands | 12 |
| East | 13 |
| London | 23 |
| South East | 15 |
| South West | 14 |
| England | 116 |
| Wales | 8 |
| England and Wales | 124 |
Note: It is likely that the differing numbers of reviews is influenced by the differing population sizes: the South-East and London are the two largest (as given by 2018 ONS mid-year estimates).
Age of victims and perpetrators
19. The average [footnote 10] age of victims was 41 years old, close to the average age of perpetrators [footnote 11] which was 40. There were two victims aged under 18 and the oldest was aged 94. The oldest perpetrator was aged 89.
20. Figure 3 shows the proportions of victims and perpetrators in different age groups. For victims, 26% were aged 30 to 39. There are two age groups in which there are 18% of victims: 18 to 29, 40 to 49.
21. The age group with the highest proportion of perpetrators is also 30-39 (33%). The group aged 50-59 has the second highest proportion: 25%.
Figure 3 Percentage of victims and perpetrators by age
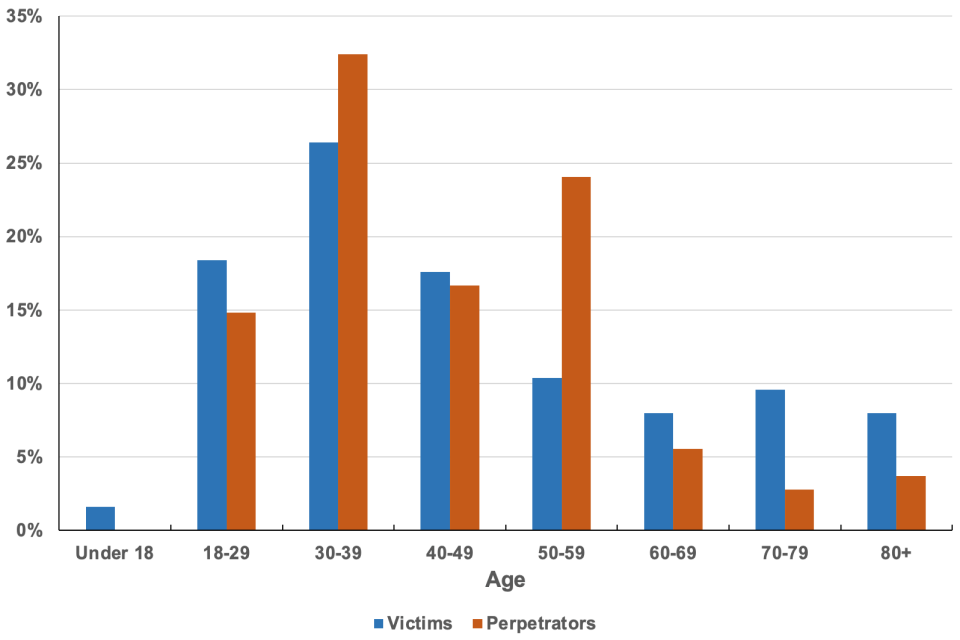
Figure 3 Percentage of victims and perpetrators by age
22. There are similar numbers of reviews where the age of the preparator is older than the victim to those where the victim is older than the perpetrator. [footnote 12]
23. Examining age and relationships: in one in five of the domestic homicide reviews [footnote 13] the victim was 20 (or more) years older than the perpetrator. Table 2 shows the relationships in these cases, with the perpetrator being the son of the victim in 56% of these. There are three cases where the perpetrator was at least 20 years older than the victim.
Table 2: DHRs where victim was 20 or more years older than the perpetrator
| Relationship of perpetrator to victim | Number of perpetrators | Percentage |
|---|---|---|
| Son | 10 | 56% |
| Daughter | 4 | 22% |
| Grandchild | 2 | 11% |
| Other | 2 | 11% |
| Total | 18 |
Notes: the relationship categories son and daughter include son-in-law and step-daughter.
24. Where the victim and the perpetrator were partners, or had been partners, the age of the victim ranged from 19 to 88. For these the age of the perpetrator was similar to that of the victim: in 55% the age difference was less than five years.
Gender of victims and perpetrators
25. In the DHRs, 80% of the victims were female and 20% male. For perpetrators, 83% were male and 17% female.
Ethnicity
26. The proportion of victims and perpetrators by ethnicity from the DHRs and for all homicides are shown in Table 3 and Table 4.
Table 3 Ethnicity of victims
| Ethnicity | Percent of DHR victims | Percent of all homicides |
|---|---|---|
| Asian / Asian British | 8% | 9% |
| Black /African / Caribbean / Black British | 5% | 14% |
| Other or multiple ethnic group | 7% | 3% |
| White | 80% | 74% |
Source: for all homicide victims and all homicide suspects is Office for National Statistics, Homicide in England and Wales Articles. Principal suspects convicted of homicide, by ethnic appearance of victim and principal suspect. Homicide in England and Wales: year ending March 2019, Appendix Table 27 and Homicide in England and Wales: year ending March 2020, Appendix Table 28.
Notes: For DHR victims (and perpetrators) the terms used for types of ethnicity are from the Government guidelines on categories. For the data from ONS the ethnicity categories are Asian (Indian sub-continent), black, white and other. Proportions for all percentages are of those where ethnicity is known. The percentages may not add to 100 as they are rounded to the nearest whole number.
Table 4 Ethnicity of perpetrators
| Ethnicity | Percent of DHR perpetrators | Percent of all homicide suspects |
|---|---|---|
| Asian / Asian British | 11% | 9% |
| Black /African / Caribbean / Black British | 13% | 19% |
| Other or multiple ethnic group | 5% | 3% |
| White | 71% | 69% |
Source and notes: as for table 3.
Nationality
27. For the victims, where nationality was recorded, 86% were British. Other victims, who may have been living in the UK for a number of years, had nationality from 12 different countries.
28. Nationality, where recorded, for perpetrators revealed 85% were British. And for those where nationality was not British there were 11 other nationalities recorded.
Religion
29. A question asked of the reviews (for both the victims and perpetrators) included “Is religion a relevant factor?”. There were no reviews where it was recorded as a relevant factor.
30. There were six DHRs where culture (for example, the country where the victim or perpetrator was raised) was mentioned as potentially a contributory factor. One example is: “…it seems likely that, despite her determination to change her circumstances, she was under enormous pressure to conform to gender and cultural norms, in particular, to accept the authority of the males in her life: a divorced husband and an uncle”.
Dependent children
31. In 41% of the reviews there were dependent children (aged under 18) living in the household at the time of the homicide. The total number of children in the households was 89. [footnote 14]
32. For the DHRs where the victim was aged under 60, the proportion with dependent children in the household increased to 52%.
33. In 12 DHRs children were subject to child protection procedures due to domestic abuse. In 10 DHRs it was indicated that some children had been removed into the care of the local authority, and in six of these children were subject to child protection procedures.
Relationships between victims and perpetrators
34. Information on the relationship between victims and perpetrators was given in 113 DHRs. For 73% of the victims the perpetrator was a partner or ex-partner. In 9% of these cases it was indicated that separation had taken place or was taking place.
35. In 27% of the 113 DHRs the relationship can be described as familial (within family). Within the familial relationships, half of these were where the victim was the parent of the perpetrator. There was a wide a range of other familial relationships (10) including, for example, grandparent, brother, sister.
Method of killing
36. The domestic homicide reviews included the method of killing. Close to half the killings are from a sharp instrument or stabbing with a knife, 24% by strangulation, [footnote 15] and 8% by blunt force trauma (see Table 5).
Table 5 Method of killing in domestic homicide reviews
| Method of killing | Percent |
|---|---|
| Blunt force trauma | 8% |
| Firearm | 1% |
| Other | 17% |
| Stabbing knife | 49% |
| Strangulation | 25% |
Notes: The methods of killing categorised as “other” fall into two main categories: a generalised description e.g. “pro-longed, sustained assault”, or a more detailed description e.g. “most likely cause of death was one of cocaine toxicity rather than the injuries sustained”.
4. Characteristics of victims
37. This chapter summarises further information on the 127 victims in the domestic homicide reviews, examining vulnerabilities and mental health issues. It then looks at whether the victim was a carer or had a life limiting illness. This is followed by whether the victim had been the target of an abuser before and whether they had been referred to a multi-agency risk assessment conference (MARAC).
There is a summary of aggravating factors that the victim experienced. It finishes with the number of victims whose death was by suicide.
Vulnerability
38. The DHRs were asked to consider the vulnerabilities that victims may have had, in terms of:
- illicit drug use
- learning disability
- mental ill-health
- physical disability
- problem alcohol use
39. Sixty-one percent of the victims were recorded with at least one vulnerability [footnote 16]. Thirty-four percent of victims have been recorded with one vulnerability, 16% with two and 11% with three vulnerabilities [footnote 17] .
40. Where a vulnerability was recorded Figure 4 shows those most often noted. Of the victims, for 34% a vulnerability was mental ill-health, for 28% there was problematic alcohol use, and for 22% illicit drug use. For 12% of the victims, physical disability was assessed as a vulnerability and for 5% a learning disability.
Figure 4 Vulnerabilities of victims: where a vulnerability was noted
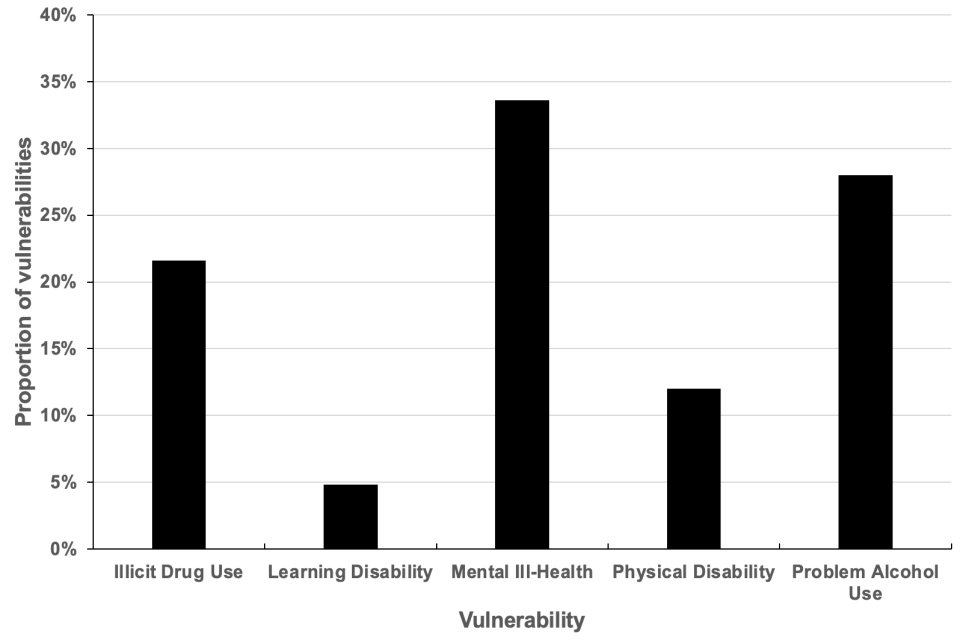
Vulnerabilities of victims: where a vulnerability was noted
Mental health
41. Reviews also identified mental health issues diagnosed or recorded for the victim. [footnote 18] The following categories were used:
- adjustment disorder
- anxiety
- dementia or Alzheimer’s
- depression
- low mood / anxiety
- panic attacks
- psychosis
- post-traumatic stress disorder (PTSD)
- self-harm
- suicidal thoughts
- suicide attempts
- not specified
42. Mental health issues were recorded for 48% of the victims. [footnote 19] The mental health issues do not differentiate between those which existed prior to their experiences of domestic abuse and those which are directly related to the experience of being abused. For 16% there was only one of the issues listed above, for 13% there were two mental health issues, and for 8% it was three issues. There were 11% of victims where more than three mental health issues were identified.
43. Figure 5 shows that of the mental health issues noted depression is most often found (26% of the issues recorded). Sixteen percent of victims had had suicidal thoughts and 14% had attempted to take their life by suicide. [footnote 20] Low mood / anxiety was also a mental health issue impacting on 14% of victims. The other mental health issues noted include anxiety, dementia or Alzheimer’s, panic attacks, psychosis, PTSD, and self-harm.
Figure 5 Mental health of victims: where reported
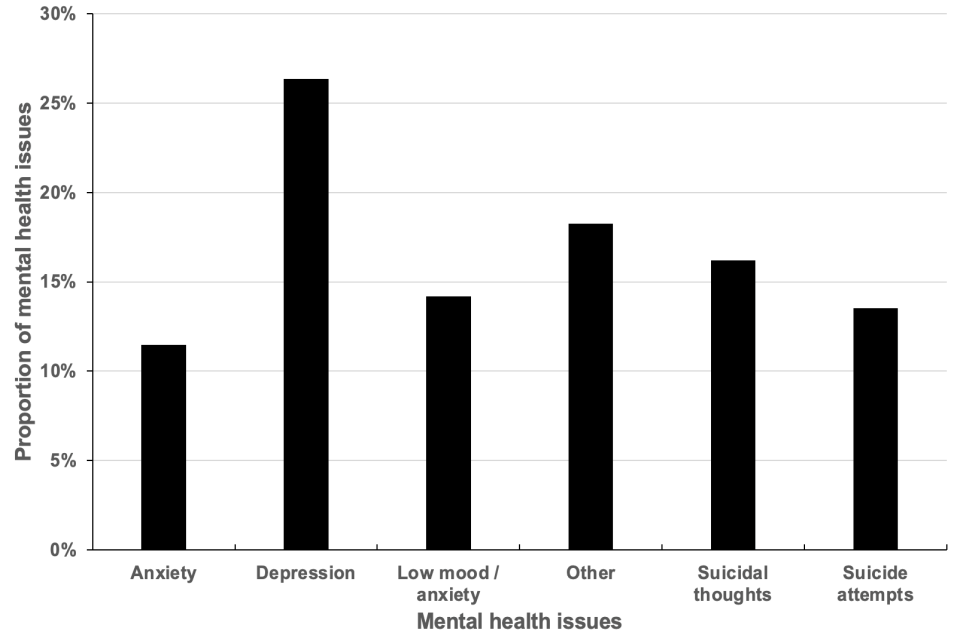
Figure 5 Mental health of victims: where reported
Carer
44. The DHRs indicate that 8% of the victims were carers. [footnote 21] In 60% of these cases the homicide was carried out by a person being cared for. None of the victims with a caring role had received a carer’s assessment of their support needs connected with their role as a carer.
Life limiting illness
45. The DHR information is asked to record if victims had a life limiting illness [footnote 22] and 14% had a condition judged to fulfil this definition. The average age of the victims with life-limiting illness was 68. The youngest four were aged under 40 and the oldest four were aged 79 or over.
Target of abuser before
46. DHRs determined whether the victim had been the target of a perpetrator previously. [footnote 23] For 46% it was recorded that the victim had previously experienced domestic abuse: in nearly every occasion this was by a previous partner.
MARAC
47. In 20% of the DHRs the victim had been referred to a multi-agency risk assessment conference (MARAC). For the victims referred to a MARAC, in 84% of these the cases were heard before the victim’s death.
Aggravating factors
48. The DHRs were required to identify a range of aggravating factors experienced by victims [footnote 24] and, where recorded, these were noted in 64% DHRs. Figure 6 shows these factors, with coercive control identified in 65% of these DHRs. The MIRs also requested additional comments on aggravating factors, and seven included this information. In these, four referred to financial abuse.
Suicide
49. Fourteen of the victims in 124 reviews died by suicide. Eleven were female and three were male. Their average age was 36. [footnote 25]
Figure 6 Occurrence of aggravating factors
| Aggravating factor | Percent |
|---|---|
| Coercive control | 65% |
| Physical stalking | 18% |
| Digital stalking | 8% |
| Immigration issues | 6% |
| Other | 4% |
5. Characteristics of perpetrators
50. This chapter summarises information on 109 perpetrators in the domestic homicide reviews. [footnote 26] The vulnerabilities and mental health issues considered are the same as those for victims. Information is then summarised on whether the perpetrator had abused previous partners or family members and whether this was known to agencies. The chapter provides the number of perpetrators with a previous offending history and then reviews the court verdicts where a criminal trial had taken place.
Vulnerability
51. DHRs were also asked to consider the vulnerabilities of perpetrators and 71% had been recorded with at least one vulnerability [footnote 27] (which is a larger proportion than the 61% of victims).
52. In examining the type of vulnerability (see Figure 7), illicit drug use, problematic alcohol use and mental ill-health were the largest proportions (30% to 33%).
Figure 7 Vulnerabilities of perpetrators: where a vulnerability was noted
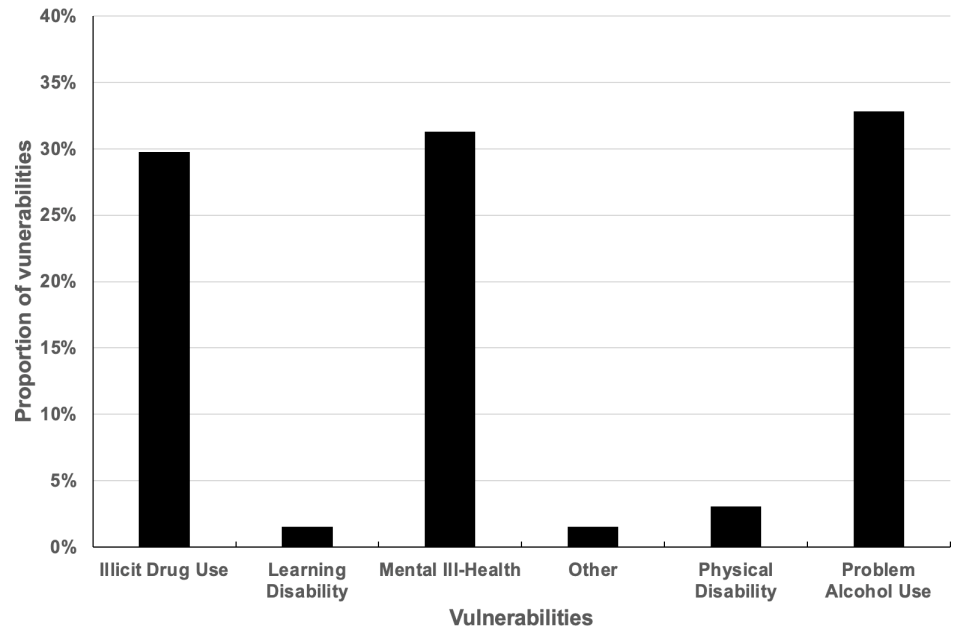
Figure 7 Vulnerabilities of perpetrators: where a vulnerability was noted
Mental health
53. The DHRs identify mental health issues which affected perpetrators. [footnote 28] These were reported for 31% of perpetrators, [footnote 29] similar to the proportion of victims (34%). For 36% of perpetrators more than one mental health vulnerability was recorded.
54. For the mental health issues which were recorded, Figure 8 shows that 23% of the perpetrators were noted to experience depression and 21% reported suicidal thoughts. These were the most common two issues also for victims, but, for victims, suicidal thoughts were a smaller proportion (16%). The largest difference in mental health issues for perpetrators compared to victims was psychosis, which formed 10% of the issues for perpetrators and 4% for victims. The mental health issues which have been grouped together as “other” are: adjustment disorder, dementia or Alzheimer’s, low mood / anxiety, panic attacks, PTSD and self-harm.
Figure 8 Mental health issues of perpetrators: where reported
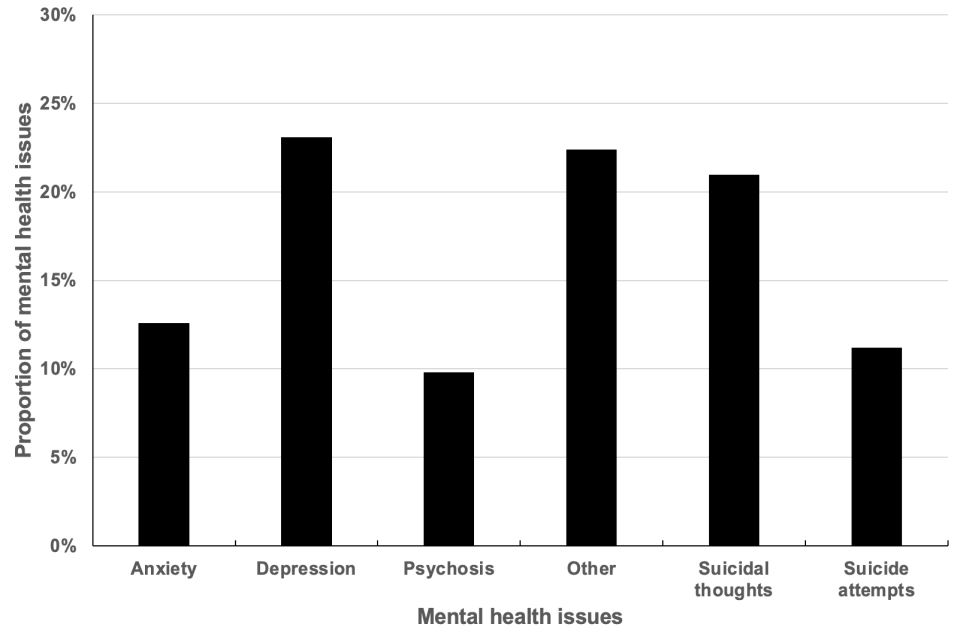
Figure 8 Mental health issues of perpetrators: where reported
Life limiting illness
55. Eleven percent of the perpetrators had a life limiting illness.
Carer
56. Thirteen percent of perpetrators were carers. Only one perpetrator had received a carer’s assessment under the Care Act 2014.
Previous offending history, previous history of abuse and whether the perpetrator was known to agencies
57. The DHRs show that 51 perpetrators were recorded to have a previous offending history. This can be taken as approximately 60%. [footnote 30] [footnote 31]
58. DHRs were also asked to note whether the perpetrator had abused previous partner/s or family members: approximately 60% are indicated to have had a having done this. While this percentage is the same as the offenders with a previous offending history, there is not an exact match in terms of individuals. Where previous offending history has been given as “No” there are three perpetrators noted as having abused previous partners or family members. For the 51 perpetrators where previous offending history has been given as “Yes” there are four where abuse of previous partners or family members is given as “No”.
59. More detail is given on nine out of ten of the perpetrators who have abused previous partner/s or family members. With three quarters of perpetrators the abuse involved previous partners and for one third the abuse included family members (these proportions include perpetrators who have abused both previous partners and also family members).
60. In the DHRs it was noted that half the perpetrators were known to agencies as an abuser. [footnote 32]
61. When the perpetrators were known to agencies, in 50% of the reviews this was just one agency, in 25% it was two agencies, and in 25% of the DHRs the perpetrator was known to three agencies or more.
62. In terms of the agencies where the perpetrator was known ( Figure 9), for 52% the police were the agency. 10% of the perpetrators were known to children’s social services and health agencies. [footnote 33]
Figure 9 Proportion of agencies to which perpetrator was known
| Agency | Percent |
|---|---|
| Police | 52% |
| Children’s social services | 12% |
| Health | 11% |
| Other | 10% |
| Probation | 7% |
| Social services | 5% |
| Housing | 3% |
Notes: the agencies used are those described in the DHRs and DHR management information reports. Children’s social services was referred to 11 times and social services five times. No assumption has been made that the term social services refers to children’s social services as it is possible it might refer to social services for adults (including older people).
Was the perpetrator being managed or supervised?
63. The MIRs were asked to report whether the perpetrator was being supervised or managed by either drug and alcohol services, multi-agency public protection arrangements (MAPPA), mental health services, a probation service or were attending or had attended a perpetrator programme. From this question 16 perpetrators were recorded as supervised or managed by at least one of these services. [footnote 34] Eight were being supervised by probation and seven were being managed and supported by a mental health service. [footnote 35] Some perpetrators were being managed or supervised by more than one service: for example, of the seven being supervised by probation two were also being supervised or managed by mental health services.
Court verdict and sentence
64. Table 6 shows the court verdicts for perpetrators. Within these 13 perpetrators were sentenced to hospital orders under the Mental Health Act 1983.
65. The perpetrators (shown in the table below) can be associated with more than one verdict. For example, the 25 perpetrators where the verdict is manslaughter includes eight with diminished responsibility. Of the four perpetrators where the information provided on the court verdict includes unfit to plead, for two both manslaughter and diminished responsibility are recorded.
Table 6 Details of court verdicts for perpetrators
| Court verdict | Number of perpetrators |
|---|---|
| Murder | 62 |
| Manslaughter | 25 |
| Diminished responsibility | 9 |
| Other offence | 9 |
| Unfit to plead | 4 |
Note: with the term verdict, as used here, there can be more than one verdict in relation to the homicide under review. For example, in one review the court verdict is manslaughter, diminished responsibility and unfit to plead.
66. The MIRs were required to provide “details of sentence AND sentence tariff”. The sentences and the information provided about them, can be complex. To give two examples: for one perpetrator the verdict was “guilty of manslaughter (diminished responsibility) and benefit fraud and prevention of a lawful burial”. Another perpetrator was found guilty of murder and arson. The information given on the sentence is “found guilty of both offences and sentenced to life imprisonment with seven years to run concurrently for the arson offence, to serve a minimum term of 25 years.” Within this context, Table 7 provides a simple summary of the information that has been provided.
Table 7 Summary information on length of sentences (years)
| Court verdict | Maximum | Average | Minimum |
|---|---|---|---|
| Manslaughter | 21 | 11 | 3 |
| Murder | 40 | 21 | 11 |
Homicide / suicide
67. In 11 DHRs the perpetrator died by suicide following the homicide of the victim(s), 10 of these perpetrators were male.
6. Themes in domestic homicide reviews
68. This chapter highlights learning from DHRs to contribute to the development of policy and practice to assist the prevention of domestic homicide. DHRs have been explored to identify key themes and areas which can be improved.
69. To draw out themes a randomly selected sample of 50 DHRs was examined in detail. [footnote 36] Themes were chosen through a selection of words and a search of the frequency they occurred. The themes are shown in Figure 10 ordered by the number of associated DHRs.
70. This chapter looks at these themes in terms of the agencies associated with them and topics within the theme. For links between agency and theme, agencies are counted only once in each DHR where there is a link. For example, if in one DHR, the word “risk” is associated with police more than once it is only counted once for that DHR.
71. The term “agency” is used to mean the function involved. For police the association between agency and the function provided is direct. For housing the term agency has been used to indicate providers of housing services - housing can be delivered in different ways and through differing types of agency, both direct and indirect.
72. For each theme the associations are then grouped into topics with examples. The examples can include the names in the DHRs. Adhering to the guidance on anonymisation these are not the names of the victims or perpetrator.
Figure 10 Themes in DHRs
| Theme | Number of DHRS in sample in which theme occurs |
|---|---|
| Contact | 42 |
| Assessment | 41 |
| Record | 40 |
| Support | 39 |
| Information | 38 |
| Risk | 36 |
| Referral | 35 |
| Training | 35 |
| Policy | 30 |
Note; Number of DHRs in sample: 50.
73. There are some overlaps between the themes since individual words can be used together. For example, “risk assessments” are words counted as risk and also assessment. Records and information also overlap. And training relating to other themes could be identified as needed e.g., training in risk assessment.
74. This chapter concludes with examples of good practice and a comparison with the themes in the 2016 report. [footnote 37]
Cases where contact was highlighted as an issue
75. In 42 of the 50 DHRs there are 122 instances of referencing an agency and contact. The list below indicates the type of agency referred to.
Frequency of agencies mentioned in relation to contact
- health: 38 (within health there are references to GPs (16), mental health services (9), and hospitals (4)), 31%
- police: 26, 21%
- housing: 11, 9%
- children’s social care: 9, 7%
- adult social care: 7, 6%
- domestic abuse support: 7, 6%
- many (more than one agency [footnote 38] ): 6, 5%
- other: 18 (including: environmental health, school/nursery, substance misuse services, victim support), 15%
Common issues related to contact
76. The issues related to contact have been grouped into four categories:
- services achieving or maintaining contact with the victim
- the perpetrator interfering in information provided by the victim
- a lack of contact between agencies
- domestic abuse not noted when the victim has been in contact with agencies
77. In relation to contact, 14 DHRs refer to achieving or maintaining the contact needed, for example:
the social worker recorded that there had been no contact by email or telephone by Olivia within the requested 14-day period. As there had been multiple attempts to contact with no response, Olivia’s case was closed.
78. A number of DHRs (13) noted the interference of the perpetrator in information provided by the victim, for example:
Adult B was also possessive and would check his wife’s mobile phone regarding her contacts and had stated to his pastor that his wife would be ‘in the gutter ‘if it wasn’t for him.
79. Twelve DHRs made reference to a lack of sufficient contact between agencies, for example:
The histories of Tigre and Canada illustrate the wide range of agencies and staff roles in contact with them, all with a need to collaborate with each other and with the potential to identify domestic abuse.
80. In five DHRs while the victim had been in contact with agencies, domestic abuse had not been noted, for example:
at times the practitioners and agencies coming into contact with Shelly and Mike demonstrated a real lack of professional curiosity.
Cases where assessment was highlighted as an issue
81. In 41 of the 50 DHRs there are 120 instances of referencing an agency and assessment. The list below indicates the type of agency referred to:
Frequency of agencies mentioned in relation to assessment
- health: 42 (within health there are references to mental health services (15), GPs (12), and hospitals (11)), 35%
- police: 25, 21%
- children’s social care: 14, 12%
- housing: 10, 8%
- adult social care: 9, 7%
- probation, community rehabilitation: 6, 5%
- other: 14 (including: domestic abuse support, environmental health, school/nursery, substance misuse services, victim support), 12%
Common issues related to assessment
82. For assessment, the terms risk assessment occurs in 23 DHRs, carer’s assessment in seven and mental health assessment in four.
83. The issues related to assessment have been connected with risk and mental health assessment; the sharing or risk assessments between agencies; the need for training in risk assessment; and that risk assessment is carried out at the right time.
84. The biggest theme relating to assessment in the DHRs was through 45 instances when they were not carried out or where some information was missing, for example:
There has been a regular absence of the use of DASH risk assessments and professional curiosity which may have improved the care and support provided to victim
The GP practice did not offer David’s mother a carer’s assessment; she was not recognised as a carer
The documented safeguarding is minimal. The entries are brief, lack detail and any rationale. For example, the enhanced risk assessment is completed but part B (safety plan) and part C (risk management plan) are left blank
85. In 10 DHRs there was reference to when a risk assessment carried out by one agency was not available to another. There are also instances where the lack of sharing occurred within agencies i.e. one department or team may not communicate an assessment to another department or team within the organisation, for example:
David’s risk assessment at the GP practice was not informed by information from other agencies.
The risk assessment present in Catherine’s notes did not cite the previous attempts and numerous presentations at A&E, nor consider the previous triggers to suicide attempts such as incidents of domestic abuse with her husband.
86. Other references with regard to assessment make reference to: training needs (5 DHRs), and the need for assessments to be carried out at the right time (4 DHRs) for example:
However, most of the Trust staff involved had not, at the time, completed the safeguarding training that covered domestic abuse risks assessment.
Once an initial risk assessment had been completed it should have been kept under review and updated once per 6 months and/or where there were significant events. Although there were significant events in this case, after the case had been transferred, further risk assessments were not completed. A significant factor in this was staffing capacity. Long term sickness and vacancies within teams had impacted assessment times and the size of staff caseloads.
Cases where record(s) were highlighted as an issue
87. In 40 DHRs there were 123 instances of referencing an agency and record(s). The list below indicates the type of agency referred to.
Frequency of agencies mentioned in relation to record(s)
- health: 51 (within health there are references to GPs (19), mental health services (10) and hospitals (7)), 41%
- police: 28, 23%
- children’s social care: 12, 10%
- housing: 8, 6%
- adult social care: 7, 6%
- probation, community rehabilitation: 5, 4%
- other: 12 (including: domestic abuse support, school/nursery, substance misuse services, victim support), 10%
Common issues related to record(s)
88. Examples within the theme of record(s) have been grouped into five categories. These are that records might not include all the information needed; information in records not being transferred between agencies; the need to improve aspects of record keeping; the need to improve minutes of meetings; and the need to improve the systems that hold information.
89. In 17 DHRs there were references to records which have information missing or do not contain all the relevant information, for example:
The … record uses only the ambiguous phrase “his history of abuse”, which does not show whether he was the perpetrator or victim.
A joint visit was planned by Environmental Health with the Police, but it took the panel some time to identify what had actually happened in response because of inadequate record keeping.
90. Ten DHRs referenced a lack of records affecting information transfer between agencies, for example:
There was no record made of any physical check of the child or provide any account of their views, wishes and feelings. Because there was no sharing of information with children’s services for example, there was no opportunity to establish if the family were already known.
There is no record of correspondence having been received from the secondary mental health service, and it is of note that no such correspondence was ever received on any occasion.
91. In seven DHRs there were references to instances where record keeping could be improved, for example:
Records maintained by primary services must ensure that they contain clear and unambiguous information to prevent manipulative patients from circumventing the system.
92. In four DHRs there was reference to the minutes of meetings not recording suitable information, particularly action to be taken, for example:
… must agree a process that ensures all MARAC meetings are accurately minuted and that the allocation and implementation of actions are recorded.
The contact … appears to have been discussed at a MARAC meeting although none of the services have a written record other than no further action was required.
93. Three DHRs noted that recording forms, or systems used to record information, needed improvement to hold all the required information, for example:
The assessment is more a contract management database recording what the GP does with a patient rather than an aid to GP assessment. Indeed, one GP commented “we serve it, not it serving us”. As a tool to assess risk, particularly to others, it is the view of the panel that the current mental health assessment for GPs does not support busy doctors in their decision making and is totally inadequate.
Cases where support was highlighted as an issue
94. In 39 DHRs there are 128 instances of referencing an agency and support. The list below indicates the type of agency referred to.
Frequency of agencies mentioned in relation to support
- health: 49 (within health there are references to GPs (16), mental health services (15) and hospitals (7)), 38%
- police: 19, 15%
- children’s social care: 11, 9%
- housing: 11, 9%
- domestic abuse support: 9, 7%
- adult social Care: 7, 5%
- other: 22 (including: community group, drugs or alcohol service, local authority, prison, probation, school / nursery, victim support), 17%
Common issues related to support
95. The theme of support has a wide range of aspects which have been grouped into six themes: not identifying the type or amount needed; the need for staff to be supported; instances where the victim declined support; the need for greater awareness of available support; support for carers; and the risk when support is accessed.
96. In 25 DHRs the theme of support for the victim can be broken down into: firstly, not identifying that support was needed or recording the need for support, secondly, not creating a plan for support and, thirdly, the lack of the correct type or amount of support for the victim. For example:
There was no assessment of Betty’s support needs as a carer for Adult A.
While Father was not at home and both men had time to reflect, services could have worked with each of them to address their reluctance to accept help and perhaps create a workable and acceptable plan of support for when Father was discharged.
The IMR states: ‘Potentially if he had received the appropriate support as a carer he may not have assaulted his mother.
97. In 16 DHRs there was reference to the need to support staff whose work involved cases of domestic abuse, for example:
There is no evidence in the record or supervision notes [of] any additional support and guidance in managing cases where there are DA and safeguarding concerns .. provided.
98. There are 15 cases where the victim declined support, for example:
Olivia declined the offer of support but did agree to a text being sent that contained the telephone number of the Victim Assessment and Referral Centre should she ever change her mind.
In these there are three which directly refer to the perpetrator acting to prevent the victim from being aware of support.
Tracey was suffering domestic abuse or coercive control and remained unaware of the support that was available to her.
99. Within 15 DHRs the analysis found a lack of awareness regarding which support might be available. There are references to victims and communities in this respect, for example:
… suffering domestic abuse or coercive control and remained unaware of the support that was available to her.
Whilst in hindsight her [work] colleagues realised she may have been subject to abuse; they did not believe they had the evidence or confidence to broach the subject directly with her or know what to do or who to refer to for help and support.
Asylum seekers and newly arriving communities will usually be unfamiliar with criminal justice and support systems available to them in the UK to keep them safe from domestic abuse. Practitioners will usually need to work especially hard to overcome barriers to help- seeking amongst asylum seeking women.
100. Two other aspects of support which DHRs raise are:
- The need for support to a victim or perpetrator if they have the role of carer.
The victim would have benefited from a carer’s assessment, a structured support package and respite care. However, many carers are reluctant to accept help for themselves and just want the person that they care for to receive the help that they need. Practitioners need to be promoting the carers assessment as a means for the family unit to strengthen its resilience.
- The need for support to be available at the right time and the attendant risk which occurs when support is accessed.
The need for real-time response is evidenced in the very nature of domestic abuse. The risk to a family increases when sources of potential support are accessed, in this case a report to the police.
Cases where information was highlighted as an issue
101. In 38 DHRs there are 129 instances of referencing an agency and information. The list below indicates the type of agency referred to.
Frequency of agencies mentioned in relation to information
- health: 46 (within health there are references to GPs (21), mental health services (9) and hospitals (7)), 36%
- police: 23, 18%
- children’s social care: 11, 8%
- adult social care: 9, 7%
- housing: 7, 5%
- many (more than one agency): 6, 5%
- school: 6, 5%
- domestic abuse support: 5, 4%
- drugs or alcohol service: 5, 4%
- other: 11 (including: community groups, local authority, prison, probation or community rehabilitation, victim support), 8%
Common issues related to information
102. Examples within the theme of information have been grouped into five types. These are:
- the importance of sharing information
- holding insufficient information
- using the information held
- improving the information for the victim or family
- that the victim can be unwilling to provide information
103. In 23 DHRs there is reference to the importance of improving the sharing of information between agencies, for example:
An information marker which highlighted concerns of domestic abuse was added to the intelligence system however, there is no information that any liaison took place with support agencies in relation to the concerns expressed.
The impact of the GP practice and the Mental Health Service not having the information concerning the incidents which involved the Police contact with David undoubtedly impeded the effective treatment and management of his behaviour and his health.
104. In 19 DHRs there is reference to sufficient information not being held, for example:
There is no information on the file to indicate that Jane disclosed or was asked directly about domestic abuse.
The IMR identified that historical information is however crucial, particularly in cases where there are indicators of domestic abuse.
105. In 11 DHRs the issue was that information was not being used or used well enough, for example:
When the initial call was made to MASH [multiagency safeguarding hub], insufficient pertinent facts were gathered. Even so, the information that was recorded and passed on appeared to be have been diluted leading to essential concerns not being highlighted and acted upon as they should have been.
106. In 6 DHRs there was reference to improvements which could be made in providing information to the victim or family, for example:
The ‘Get Help’ page lists support services alphabetically, including both specialist domestic and sexual abuse services, as well as other more generic services. While this is a useful resource, for a victim or survivor, the quantity of information may be overwhelming.
107. Five DHRs referred to either the victim being unwilling to provide information or the manipulation of information by the perpetrator, for example:
Adults and particularly children are often reluctant to disclose matters of neglect and abuse and it is crucial that those encountering such situations remain open minded and gather as much information as possible, and then share what they have discovered with other agencies.
The point needs to be made that manipulative and determined perpetrators may seek to hijack agencies systems with misleading information to paint themselves as the aggrieved party.
Cases where risk was highlighted as an issue
108. In 36 DHRs there were 93 instances of referencing an agency and risk. The list below indicates the type of agency referred to.
Frequency of agencies mentioned in relation to risk
- health: 30 (within health there are references to GPs (9), hospitals (7), and mental health services), 32%
- police: 28, 30%
- children’s social care: 10, 11%
- housing: 7, 8%
- domestic abuse support: 5, 5%
- probation: 5, 5%
- other: 8 (including: adult social care, fire and rescue, local authority, school/nursery, substance misuse service), 9%
Common issues related to risk
109. Issues related to risk include risk assessment not being carried out or the risk not being assessed as high enough. There is also the need to consider repeat individual risk assessments together rather than by individual incident; that risk assessment might have been downgraded; and the need for training in risk assessment.
110. The two most common issues concerning risk (each identified in 13 DHRs) were risk assessment not being carried out or the risk not being assessed as high enough, for example:
In health services, there was no documentation of questioning around domestic abuse and no assessment or identification of risk when Shelly attended at the GP Practice or A&E, despite presenting with injuries consistent with physical abuse, and despite staff being alerted to the number of previous A&E presentations through access to electronic systems.
111. The following examples also show the issue that the risk assessment would have been different if information from previous individual risk assessments was assessed overall or that risk assessments were shared between agencies (noted in 6 DHRs), for example:
Each risk assessment appeared to be based solely on the incident reported and did not take a holistic view of previous contacts with police, which may have impacted on the grading.
David’s risk assessment at the GP practice was not informed by information from other agencies.
112. Five DHRs gave examples of when risk had been downgraded, for example:
This is one of the very few occasions when a medium assessment was made. Then the police were called again on 24th February and the risk was assessed as standard. Given that Catherine had called the police on three occasions in the intervening weeks it would appear that the risk assessment should have remained medium.
113. Four of the DHRs noted the importance of training on appropriately assessing risk, for example:
In the Community Mental Health Team as a whole, while 98% had undertaken basic safeguarding training by July 2017, only 17% of those required to had undertaken the Level 3 training. Completion of the training would have provided a better understanding of domestic abuse, and of the systems in place within the Trust, which could have supported the efforts of Trust staff to identify and address the risks.
Cases where referral was highlighted as an issue
114. In 35 DHRs there were 126 instances of referencing an agency and referral. The list below indicates the type of agency referred to.
Frequency of agencies mentioned in relation to referral
- health: 48 (GPs (19), mental health services (14), and hospitals (8)), 38%
- police: 22, 17%
- adult social care: 11, 9%
- children’s social care: 11, 9%
- domestic abuse support: 10, 8%
- substance misuse service: 6, 5%
- school: 5, 4%
- other: 13 (including: Department for Work and Pensions, housing, prison, probation or community rehabilitation, victim support, Youth Offending Service), 10%
Common issues related to referral
115. The issues related to referral include examples of where a referral was not made; where the victim declined being referred; referrals which should have contained more information; and pathways identified in referrals which were not enacted.
116. The largest issue (in 21 DHRs) within the theme of referral was when a referral was not made, for example:
The review is concerned that given the history of excessive alcohol use, mental illness and a history of domestic abuse a referral to a longer-term treating team … was not considered. It is considered that this is a missed opportunity.
Nevertheless, there were missed opportunities for the GP practice to make referrals to adult social care for a carer’s assessment for Angela.
117. In eight DHRs there were references to the victim declining referral, for example:
The victim experienced male violence and abuse throughout most of her life and her substance misuse and mental ill-health could well have been as a consequence and means of coping with this abuse. At times she felt able to reach out for help but always retreated again from onwards referrals to specialist services.
118. Six DHRs made references that referrals should have contained more information, for example:
The letter did not give any background history concerning David’s 6-year involvement with the service, or guidance on what level of concern might constitute a threshold for re-referral.
119. Six DHRs also gave examples where referral pathways were not enacted, or previous referrals were not considered, for example:
Children’s social care missed the opportunity to utilise information contained within previous referrals and their impact on the current referral being made.
Cases where training was highlighted as an issue
120. In 35 DHRs there are 84 references to training. The list below shows the type of agency referred to.
Frequency of agencies mentioned in relation to training
- health: 40 (within health there are references to GPs (11), hospitals (8), and mental health services (7)), 48%
- police: 9, 11%
- adult social care: 8, 9%
- children’s social care: 7, 8%
- housing: 7, 8%
- local authority [footnote 39]: 5, 6%
- other: 8 (including probation, substance misuse services, victim support), 10%
Common issues related to training
121. Within the 35 DHRs where training was an issue the following represent the main characteristics. These include examples of where training needs to be modified; the need to provide more training - including refresher training; that more staff should be trained; the need to see that the training is effective; that training needed should take place; that mandatory training should be taken; and trained staff should carry out particular types of work.
122. Fifteen DHRS referred to the need to modify existing training, for example to address features from the DHR, or in the use of new or modified systems to record additional relevant information for example.
all safeguarding training to include a section on coercive control, intergenerational and familial abuse.
these issues will only ever be identified when systems are in place that link such information and when practitioners either have the training and knowledge/confidence to apply professional curiosity so that they have a satisfactory sense of who they are dealing with and what their needs are and how they have got there.
123. In 12 DHRs training was raised through the need to provide more training opportunities. Refresher training is an example given.
additional refresher training … should be considered by the schools involved.
124. Ten DHRs referred to the need to train more staff, in some this was training staff who had not receive relevant training in their roles, and for some DHRs the issue was given as training a greater proportion of staff, for example:
While Evie and her child were receiving care from her GP the practice did not have a domestic violence and abuse policy in place, and staff had not received any specific training.
125. Seven DHRs included the benefits from auditing existing training to ensure it was effective, for example:
GP safeguarding leads to audit the effectiveness of the … training for GPs including the number of GP referrals… and appropriate referrals to MARAC as well as the outcomes for clients referred.
126. Seven DHRs also referred to carrying out training needs assessment, which could enable a plan for training to be implemented, for example:
the current head teacher … has identified the school needed to strengthen its resources together with training, knowledge, and skills of staff to support vulnerable children’s emotional wellbeing in school.
127. In six DHRs there was reference to the need to ensure that mandatory training was undertaken by staff, for example:
To continue to ensure all professionals complete required mandatory training enabling them to play a key role in the early identification and response to domestic abuse and coercive and controlling behaviour.
128. Four DHRs referred to the need for trained staff to carry out particular aspects of work, for example in assessing risk level associated with incidents.
A more thorough risk / needs assessment is best undertaken by those with specialist training.
Cases where issues on the theme policy were highlighted
129. In 30 DHRs there are 53 references to policy in the analysis sections. The list below shows the type of agency referred to.
Frequency of agencies mentioned in relation to policy
- police: 17, 32%
- health: 16 (within health there are references to GPs (4), hospitals (3) and mental health services (2)), 30%
- housing: 5, 10%
- other: 15 (including: adult social care, central government, children’s social care, domestic abuse support, drugs or alcohol service, local authority, many organisations or partnerships, probation, school / nursery, victim support, Youth Offending Service), 28%
Common issues related to policy
130. Within the theme of policy there are four main types of example: having a suitable policy; actions not taken in line with policy; lack of knowledge of policy, and no policy existed.
131. In 16 DHRs the references were to a suitable policy, and action being taken in line with such a policy, for example:
The Review is satisfied that these two incidents were recorded as domestic abuse in accordance with … Police Domestic Abuse Policy and Home Office Crime Recording standards.
132. In 10 DHRs there was mention that a policy had been changed or is being changed, for example:
Their policy and procedure had recently been reviewed following another domestic homicide review and the panel felt assured that this reflected all of the latest guidance, research and legislation.
133. Nine DHRs reported instances when the need for action was not checked against policy or did not happen, for example:
Neither the nurse nor doctor were familiar with the … domestic abuse policy. Additionally, as a locum, the doctor could not access the intranet and therefore could not access any … policies. Furthermore, the consultant did not advise locum of non-obstetric care guidelines.
134. Five DHRs gave examples of agencies not having a policy, for example:
We have seen that the nursery concerned had no domestic abuse policy or procedures contained within its safeguarding policies and staff were not trained or supported on domestic abuse which is the most common safeguarding and child protection issue.
Cases of good practice
135. In order to provide a count and examples of good practice the sample of 50 DHRs were searched in full – not just the sections relating to analysis. In 32 DHRs there were 69 examples of good practice. The list below shows the type of agency referred to.
Frequency of agencies mentioned in relation to good practice
- health: 26 (within health there are references to GPs (10), hospitals (5) and mental health services (4)), 38%
- police: 18, 26%
- children’s social care: 5, 7%
- other: 20 (including: adult social care, domestic abuse support, drugs or alcohol service, housing, local authority, probation, school / nursery, victim support), 29%
Main areas of good practice
136. The DHRs made reference to 64 examples of good practice. These have been grouped into three types: agencies working together; the way in which the victim was asked about their experience of domestic abuse; the timely nature of assessment.
137. Twenty-eight percent of these are on the issue of one agency working with or referring the victim to another, for example:
The xx Safeguarding Adults Board has representation from the housing sector in all of the Board’s subgroups.
When Omar presented with mental health problems, a doctor at the GP surgery asked questions about his family and the broader social context of Bilqiis and Omar and made family-focused referrals as a result. This acknowledged the wider impact of Omar’s mental ill health, Bilqiis’s history of mental ill health and the family’s likely need for wider support.
138. Seventeen percent of the examples can be grouped as the ways in which victims are asked about their experience of domestic abuse for example:
The xx policy that has been adopted since 2017, is that maternity services require pregnant women to be asked about potential domestic abuse three times during their care. The outcomes of this policy are regularly audited and reported upon. This is now being audited quarterly.
139. Nine percent of the examples of good practice were on the timely nature of assessment or action for example:
The immediate contact by the clinical lead following the on-line self-referral on the 27th January 2014 was good practice.
Additional examples of good practice
140. Other examples of good practice have been identified during the quality assurance process for the Home Office.
- Identifying risk management of patient’s care and the need for practice and policy changes, for example:
William continued to obtain the repeat prescription (for an opiate based medication) until he was taken to hospital following an overdose. The prescription policy of the practice was identified by the agency review as an area of learning along with encouraging the good practice of reviewing the household medication when notified of a member of the household with a substance abuse problem… It is good medical and health care practice to keep under active review the prescription of opiate-based medications, including households where there may be multiple prescriptions for related medication, and to treat all new patient registrations, including those who are returning to a GP practice, as new patients and confirm the validity and appropriateness of any request for medication.
- Risk assessment, for example:
xx Housing use a risk assessment framework when considering whether tenants are at risk of domestic violence, abuse or neglect. They are also signed up to the Chartered Society of Housing, Make a Stand Initiative, to address domestic abuse in housing authorities, and have domestic abuse and safeguarding champions to support their workforce.
- Inter-agency information sharing and identification of risk, for example:
the children’s school raised concerns as Stephan had dropped one of his daughters at school, which was unusual. When the daughter had been spoken to, she had provided differing accounts; that Marcia had gone to London and was very tired and that Marcia had got a job. The same day, school rang the police and raised their concerns for Marcia’s safety and that she had last been seen four days earlier.
- Good practice relating to training, for example:
good practice by xx CCG. They had committed to a rolling programme of mandatory 3.5 hour Level III Child Safeguarding Training which included learning from DHRs/SCRs and a 1.5 hour case study on domestic abuse indicators and ‘asking the question.
Comparing themes with 2016
141. This report is an update on the previous Home Office (2016) report [footnote 40] describing key findings from analysis of domestic homicide reviews.
142. Five themes – policy, record keeping, referral, risk, and training – appear in both the 2016 and 2021 reports. For record keeping the aspect of where records were not kept or shared occurs in both reports. In this report there are also examples where the records did not contain information required.
143. Although the remaining four themes in this report are not replicated by name there are links.
Assessment
The term assessment in the 2016 report is widely used under the heading risk assessment. It also occurs under themes of organisational policy; multi-agency working practices; professional and practitioner competence; and training.
This report provides examples of risk assessment, and also carers’ assessments and mental health assessments.
Contact
In the 2016 report there is no heading or theme labelled contact. However, examples of contact were given under the themes of multi-agency working practices; competence, knowledge and skills; and public awareness.
Information
The theme communication/information sharing between agencies was a theme in the 2016 report. In the 2021 report this is the largest theme under the heading information. Other aspects which are noted are sufficient and accurate information not being held, the need for improvements in information sharing and victims being unable or constrained from providing information.
Support
Support was not a separate theme in 2016 but was noted within risk assessment; multi-agency working practices, competence, referrals, and public awareness.
7. Analysis of recommendations in domestic homicide reviews
144. Domestic homicide reviews should make specific, measurable, achievable, relevant, and time-bound (SMART) recommendations identifying actions to improve responses. The sample of 50 DHRs has been examined to show the agencies or organisations given responsibility and also the type of action in the recommendations.
145. The 50 reviews provided 544 recommendations for this analysis. These include those in individual management reviews (IMRs) where they appear in the DHR document. IMRs are to “allow agencies to look openly and critically at individual and organisational practice and the context within which professionals were working (culture, leadership, supervision, training) to see whether the homicide indicates that practice needs to be changed or improved to support professionals to carry out their work to the highest standards”. [footnote 41]
146. The circumstances of the domestic homicide, and whether IMRs have been included within the DHR, influence the number of recommendations. There were a small number of DHRs with no recommendations and some with 30 or more.
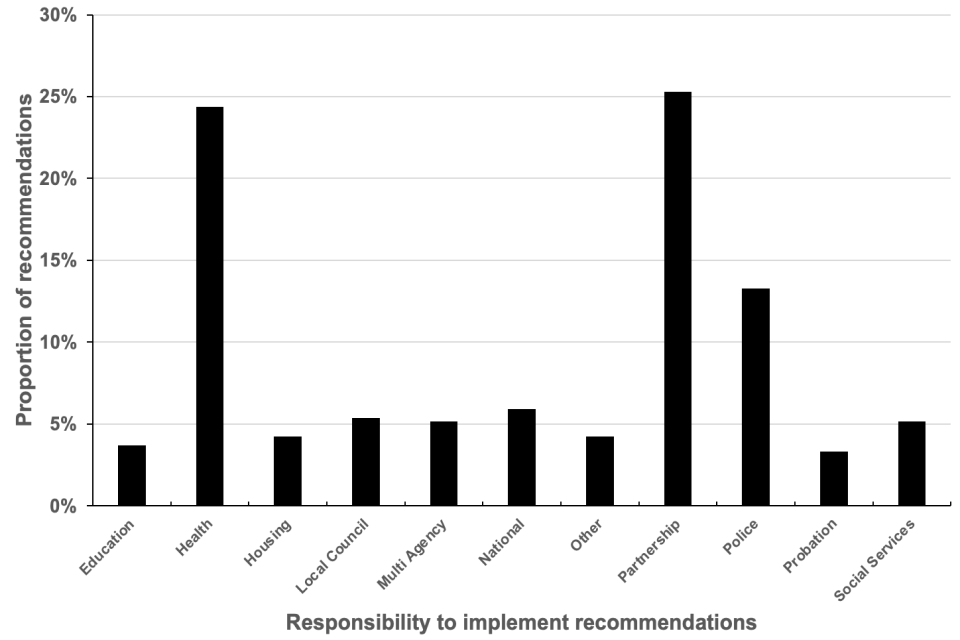
147. The recommendations in the DHRs identify the agency with responsibility for carrying out the actions to fulfil the recommendations (shown in Figure 11). Twenty-five percent of the recommendations are seen as the responsibility of Partnerships. The number is similar for organisations working in health (24% of the recommendations). The police are given responsibility for 13%.
148. There are a number of differing partnerships with responsibility. Of the total recommendations for partnerships, 69% are for the community safety partnerships and 13% are for domestic abuse boards.
149. The recommendations for health organisations are across the wide range of organisations who deliver health services e.g. hospitals, mental health services, and GPs, or those who are responsible for commissioning health services, e.g. clinical commissioning groups.
Figure 11 Responsibility to implement recommendations
Responsibility to implement recommendations
150. The recommendations indicate the type of action needed and Figure 12 summarises these.
Figure 12 Themes from DHR recommendations
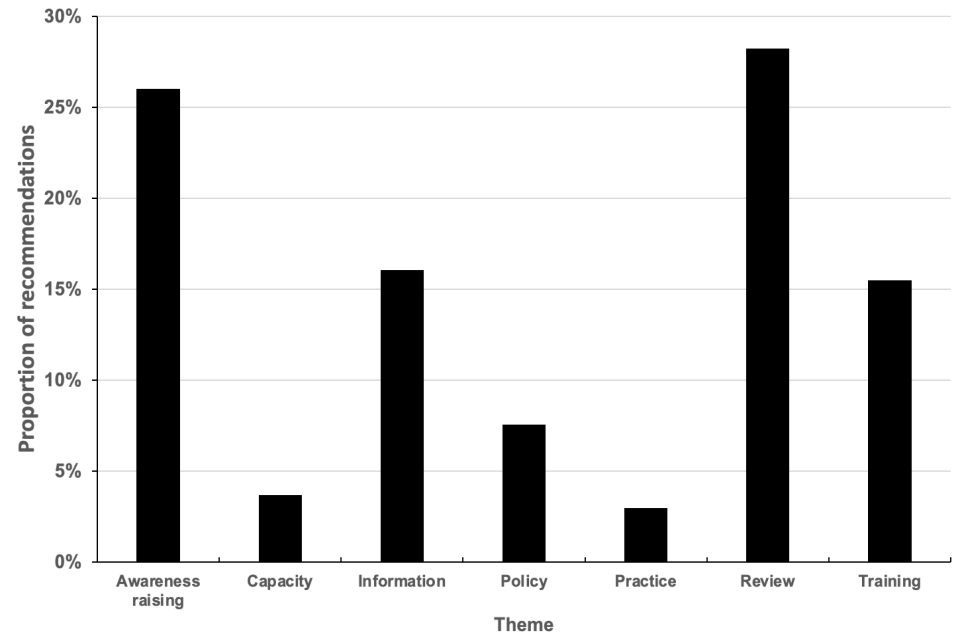
Themes from DHR recommendations
151. Twenty-eight percent of the recommendations were to review existing practice. There is variety within these between those with a wide scope - “review the services provided to victims and perpetrators” - and those which are more specific, for example:
That revisions take place to the GP Mental Health Assessment risk assessment page to provide a comprehensive list of areas to cover which includes substance misuse, domestic abuse, both as perpetrator and victim, and the quality of family relationships including any tensions.
152. A similar proportion of the recommendations (26%) were to raise awareness. The majority of these (72%) refer to raising awareness of staff or organisations, for example:
Learning from this DHR will be shared with … staff and in the wider Trust so that staff have a greater awareness of DA cases and learn from case reviews.
153. Other recommendations on raising awareness relate to the public or particular communities, for example:
Community Safety Partnership to increase levels of awareness of stalking and harassment law and the support available; to ensure that this information reaches all communities and ages..
VAWG [Violence against Women and Girls] providers to consider opportunities to promote specific targeted services to identified ethnic minority groups to improve disclosures of abuse and thus access to DA [domestic abuse] services.
154. There were 16% of the recommendations which referred to information. Of these 69% emphasise the need to improve the quality of the information held, for example:
That relevant … staff are reminded of the importance of accurate record keeping with regards to safeguarding and services provided for victims of DA.
155. Thirty nine percent of the recommendations concerning information relate to the sharing of information, frequently between agencies, for example:
Ensure that information provided by service user is checked with partner agencies.
156. Training is the subject for 15% the recommendations, for example:
Enhance their training programme to encourage frontline practitioners to demonstrate more professional curiosity when receiving disclosures of domestic abuse from patients and their families.
8. Family contribution and support through DHR process
157. The Multi-agency Statutory Guidance for the Conduct of Domestic Homicide Reviews (2016) [footnote 42] sets out how DHRs should engage with family, friends, work colleagues, neighbours and the wider community: “the review panel should recognise that the quality and accuracy of the review is likely to be significantly enhanced by family, friends and wider community involvement. Families should be given the opportunity to be integral to reviews and should be treated as a key stakeholder” (paragraph 52).
158. MIRs included questions to record family contributions: the responses for the 124 DHRs are shown below.
Did the family contribute to the DHR?
159. Seventy seven percent of the DHRs reported that families did contribute.
Were the family consulted about the terms of reference?
160. Thirty two of the DHRs noted that families were consulted about the terms of reference and 22 reported that this did not happen. With the 22 DHRs which recorded that consultation had not taken place eight gave reasons: in three the families made the choice not to contribute, and in two the family did not live in the UK.
161. In 70 of the DHRs the answer to the question was not given or found within the DHR.
Did the family have the support of an expert specialist advocate?
162. In 38 DHRs the support of an expert specialist advocate was recorded as “Yes”, for 56 the answer was “No”. Within the answers “No” in 22 DHRs it was indicated that support had been offered but not taken up.
163. In the DHRs with details on the specialist advocate support provided, in 18 this was the specialist service Advocacy After Fatal Domestic Abuse (AAFDA). Seven were victim support, and three were supported via police family liaison officers.
164. For 30 DHRs an answer had not been given or found.
Did the family receive the draft report to comment on?
165. For 56 of the DHRs it is recorded that the family received the draft report to comment on, and there were 28 where it was recorded that they did not receive the draft report – in many cases this was related to the family not engaging with the DHR process.
166. For 40 DHRs the answer is not known.
Did the family attend the DHR panel?
167. There were nine instances where members of the family attended the DHR panel, 64 cases where it was noted they did not attend. For eight of the DHRs where it was indicated that the family did not attend it was recorded that they declined the invitation.
168. No answer was given in 51 DHRs.
9. Common reasons the Home Office Quality Assurance Panel require DHRs to be resubmitted
169. The Quality Assurance Panel provides feedback to commissioning community safety partnerships in two formats. A letter approving the DHR for publication with perhaps suggestions for minor amendments prior to publication. Or feedback detailing where further amendments and analysis are requested to enable the DHR to reach a suitable standard to be published, and for the DHR to be resubmitted to the panel.
170. Analysis of the feedback given by the Quality Assurance Panel process for 36 DHRs resubmitted in the timeframe of this research reveals common themes which bring about the need for resubmission. These are shown in Table 8.
171. The purpose of this chapter is to assist DHR panels in performing their duties under the DHR Statutory Guidance Section 7(74), [footnote 43] and community safety partnerships on receiving the DHR prior to submission to the Home Office Section 7(78). [footnote 44]
172. Significant reasons why DHRs are requested to be resubmitted are:
- DHRs have not followed report templates in Statutory Guidance (Appendix 3 and 4) - this results in information required in the Guidance for DHRs being omitted and having to be requested
- insufficient probing and depth of analysis
- significant levels of typographical and grammar errors
- the need for additional anonymisation
- insufficient information about the chair / author’s background, experience and independence (Section 4(36) of Guidance)
- a lack of evidence or citing research to back up statements
173. DHRs requiring resubmission had a combination of these issues, not just one.
174. Other themes influencing the need for resubmission include:
- coercive control inadequately addressed
- equality and diversity issues inadequately addressed
- inadequate detail about family contributions as requested in guidance
- lack of perpetrator background history
- use of pseudonyms which would make DHR easier to follow
- recommendations not made or poorly worded
- victim blaming phrases or comments
Not a reason for resubmission, but a common comment to community safety partnerships to note for future DHRs concerned the DHR lacking a specialist domestic abuse agency on the DHR panel and / or specialist service for case specific areas of concern i.e. drug and alcohol services.
Table 8 Common reasons for Quality Assurance Panel requiring DHRS to be resubmitted
| Reason | Percent |
|---|---|
| Guidance templates not followed resulting in missing information | 15% |
| Insufficient probing and analysis | 15% |
| Typos and grammar | 11% |
| Chair /author’s background, training and independence lacks sufficient detail | 8% |
| Further anonymisation required | 8% |
| Lack of evidence and research cited to support statements | 7% |
| Coercive control and other specific forms of abuse not explored when relevant | 6% |
| Equality and diversity inadequately addressed | 6% |
| Inadequate detail re: family involvement including detail required in guidance | 6% |
| Recommendations not well worded or not made when learning suggests required | 6% |
| Lack of DA specialist agency on panel and / or specialist for case specific subjects | 5% |
| Victim blaming phrasing or comment | 4% |
| Use of pseudonym would make DHR easier to follow | 3% |
| Lack of perpetrator background history | 2% |
Appendix 1. Management information report questions
The following management information report (MIR) is that used for each DHR from July 2019. A number of differing forms were used before July 2019 – for these the DHRs were reviewed for answers to questions not contained within the current MIR. DHRs were also reviewed for answers not provided to July 2019 questions.
PLEASE MARK EACH BOX: IF QUESTION IS NOT APPLICABLE, PLEASE STATE: N/A IF ANSWER IS NOT KNOWN PLEASE STATE THIS OR PUT: N/K
Name of community safety partnership
Local authority
Police force area
Date of death
Postcode and location of death
Is location victim’s home address? (Y, N or N/K)
Review panel chair
Review author
Date Home Office notified of DHR
Local DHR reference
Date report completed by author
Date signed off by CSP Board
Date submitted to Home Office by CSP Board
Home Office reference number given for report
1. Victim/s
Sex of victim/s
Age at time of death
Relationship to perpetrator
Ethnicity
Nationality
Is religion a relevant factor? (Y, N or N/K)
If religion is a relevant factor please comment
Sexual orientation. Please state orientation and how known, or mark N/K
Is or was the victim a carer? (Y, N or N/K)
If Yes, had they had a carer’s assessment under the Care Act? (Y, N or N/K)
Vulnerabilities
Please mark (e.g. X) ALL that apply
Mental ill-health, illicit drug use, problem alcohol use, pregnancy, physical disability, learning disability
Mental health issue/s identified in the DHR
Please mark (e.g. X) ALL that apply
Depression, psychosis, self-harm, suicidal thoughts, suicide, low mood / anxiety (no diagnosis), panic attacks, anxiety, PTSD, adjustment disorder, dementia or Alzheimer’s disease, not specified.
Any serious or life limiting illness? (Y, N or N/K)
If Yes please describe
Has the victim been a target of an abuser before? (Y, N or N/K)
if Yes please state by whom?
2. Perpetrator
Sex of perpetrator
Age at time of fatal incident
Relationship to victim/s
Ethnicity
Nationality
Is religion a relevant factor? (Y, N or N/K)
If religion is a relevant factor please comment
Sexual orientation. Please state orientation and how known, or mark N/K
Is or was the perpetrator a carer? (Y, N or N/K)
If Yes, had they had a carer’s assessment under the Care Act? (Y, N or N/K)
Vulnerabilities
Please mark (e.g. X) ALL that apply
Mental ill-health, illicit drug use, problem alcohol use, physical disability, learning disability
Mental health Issue/s identified in the DHR. Please mark (e.g. X) ALL that apply
Depression, psychosis, self-harm, suicidal thoughts, suicide, low mood / anxiety (no diagnosis), Panic attacks, anxiety, PTSD, adjustment disorder, dementia or Alzheimer’s disease, not specified
Any serious or life limiting illness? (Y, N or N/K)
If Yes please describe
Had the perpetrator abused previous partner/s or family member before? (Y, N or N/K) If Yes please state who the victim was
Was the perpetrator known to agencies as an abuser? (Y, N or N/K) If Yes please state which agency
Has the perpetrator any previous offending history? (Y, N or N/K) If Yes please state which offences
Was the perpetrator being managed or supervised by, or attending any of the following?
Please mark (e.g. X) ALL that apply
MAPPA, National probation, mental health services, drug and alcohol services, attending or had attended a perpetrator programme
3. Crime details, MARAC and outcome of trial
Had the victim been referred to MARAC? (Y, N or N/K)
Was the case heard at MARAC before the homicide? (Y, N or N/K)
Method of killing
If relevant please state weapon used:
Firearm, stabbing knife, strangulation, blunt force trauma, other, please state
Cause of death - results from post-mortem
Details of court verdict. Please mark (e.g. X) ALL that apply:
Murder, manslaughter, diminished responsibility, unfit to plead, not guilty
Details of sentence AND sentence tariff
4. Details, if reviewing suicide or murder / suicide
Is DHR reviewing a murder and suicide? (Y or N)
If DHR is reviewing a death by suicide, please answer the following
Sex of deceased
Method of suicide
Reason suicide met threshold for DHR
5. Aggravating factors
Aggravating factors in DHR.
Please mark (e.g. X) ALL that apply
Immigration issues (V if relevant for victim and / or P if relevant for perpetrator), forced marriage, HBV, physical stalking, digital stalking, coercive control
6. Details of children if relevant (0-18yrs)
Did the parties in the DHR have parental responsibility for children? (Y, N or N/K)
If YES, please give sex of child/ren
If YES, please give age of child/ren
Were children subject to child protection procedures due to domestic abuse? (Y, N or N/K)
Any children removed into care of local authority? (Y, N or N/K)
7. Family contribution and support though DHR process
Did the family contribute to the DHR? (Y, N or N/K)
If answer is N, please comment
Were the family consulted about the terms of reference? (Y, N or N/K)
If answer is N, please comment
Did the family have the support of an expert specialist advocate? (Y, N or N/K)
If answer is Y, please specify.
Did the family receive the draft report to comment on? (Y, N or N/K)
If answer is N, please comment
Did the family attend the DHR panel? (Y, N or N/K)
If answer is N, please comment
Definitions
The following definitions were provided with the questions.
Physical disability
A person is considered to have a disability if they have a long-standing illness, disability or impairment which causes difficulty with day-to-day activities (Equality Act 2010).
Learning disability
A learning disability affects the way a person understands information, how they learn new skills, how they communicate, and in some cases whether they can cope independently. There are varying degrees of learning disability for example: Some people with a mild learning disability can talk easily and look after themselves but may need a bit longer than usual to learn new skills. Other people may not be able to communicate at all and have other disabilities as well. Some adults with a learning disability are able to live independently, while others need help with everyday tasks, such as washing and dressing, for their whole lives.
Life-limiting illness
Life-limiting illness is a term used to describe an incurable condition that will shorten a person’s life, though they may continue to live active lives for many years. There is a wide range of life-limiting illnesses, including heart failure, lung disease, neurological conditions, such as Parkinson’s and Multiple Sclerosis, and cancer that is no longer responding to treatment intended to cure.
Equality Act 2010
A person is considered to have a disability if they have a long-standing illness, disability or impairment which causes difficulty with day-to-day activities.
For ethnicity (Office for National Statistics)
White
1. English/Welsh/Scottish/Northern Irish/British
2. Irish
3. Gypsy or Irish Traveller
4. Any other White background, please describe
Mixed/Multiple ethnic groups
5. White and Black Caribbean
6. White and Black African
7. White and Asian
8. Any other Mixed/Multiple ethnic background, please describe
Asian/Asian British
9. Indian
10. Pakistani
11. Bangladeshi
12. Chinese
13. Any other Asian background, please describe
Black/ African/Caribbean/Black British
14. African
15. Caribbean
16. Any other Black/African/Caribbean background, please describe
Other ethnic group
17. Arab
18. Any other ethnic group, please describe
Appendix 2. How data was assembled for use
This report uses information from 124 Domestic Homicide Reviews which were assessed via the Home Office Quality Assurance Panel during the 12 months from October 2019. It is based on information requested through management information reports (MIR) for each DHR.
There were a number of types of MIR, with different formats and different questions, used before the one for this report was put in place.
Twenty two reviews had no MIRs. Information used has come from searching the DHRs.
Seventy seven reviews had data from earlier MIR forms. These DHRs were searched for data needed for the additional questions.
The MIRs from the remaining 25 DHRs were checked and edited as data was frequently given in a different format or way to that requested. Examples are:
-
data not as precise as requested e.g. the age of a victim might be given as “mid thirties” - for the analysis this was changed to 35 years.
-
there were a number of questions where the answer requested was Y, N or N/K (not known) but the answer was left blank - for these the DHRs were checked to see if the missing data could be found, if not found then the answer was changed from blank to not known.
To help comparisons between the answers for different questions, the percentages from DHRs are as percentages of those known i.e. the number Yes and the number No.
For the questions on vulnerabilities and mental health issues, the answer requested in the MIR was just X where these were recorded or noted. For these the number of X’s have been given as percentages of the total (victims or perpetrators). Through this there is an assumption that any answer blank means No, and so it is assumed there are no unknowns. The percentage with a vulnerability would be given as higher if some of the blanks were vulnerabilities or mental health issues which were Not Known.
Appendix 1 shows the other questions where the answer requested was simply X (i.e. not accompanied by N or N/K).
There was variation in the proportion of answers Not Known. For the question “Is location victim’s home address? (Y, N or N/K)” there are three of the 124 DHRs where this information was not given. There are questions where the number of unknowns is seen to be notably higher. In particular these are:
- had the perpetrator abused previous partner/s or family member before?
- was the perpetrator known to agencies as an abuser?
- has the perpetrator any previous offending history?
The table below shows the number of unknowns in these. It also shows the differing percentages for Yes and No depending on whether these are of the total known or the total which includes the unknown.
It is possible that there is bias in whether the unknowns might be Yes or No. For example, it may be easier to record a previous offending history (Yes) than indicate there is no pervious offending history. If this is so then the unknowns are more likely to be No than Yes. The information on these questions has been given as percentages of those which are Yes or No but the term approximate has been used to indicate there is a level of uncertainty.
Table: Known and unknowns
| Answer | Previous offending history? | Abused previous partner/s or family member? | Known to agencies as an abuser? |
|---|---|---|---|
| Yes | 51 | 45 | 49 |
| No | 34 | 30 | 49 |
| Not known | 24 | 34 | 11 |
Percentage of total known
| Answer | Previous offending history? | Abused previous partner/s or family member? | Known to agencies as an abuser? |
|---|---|---|---|
| Yes | 60% | 60% | 50% |
| No | 40% | 40% | 50% |
Percentage of total
| Answer | Previous offending history? | Abused previous partner/s or family member? | Known to agencies as an abuser? |
|---|---|---|---|
| Yes | 47% | 41% | 45% |
| No | 31% | 28% | 45% |
| Not known | 22 | 31 | 10 |
Part of the uncertainty on data quality comes from the length of the DHR reports. There is not a simple relationship between a longer report being better, and part of the length is likely to reflect the complexity of the DHR. But five of the DHR reports were less than 20 pages and eight were over 100 pages.
Appendix 3. Data from information required with DHRs
This table gives the number of answers in each management information reports (MIR). It indicates the number with data (used), the number where the MIR marks the answer as N/K (not known) and the number where the answers is left blank.
| Question | Number with data | N/K | Number blank |
|---|---|---|---|
| Date of death | 124 | - | - |
| Is location victim’s home address? | Y = 101 N= 20 |
3 | - |
| Questions on victim/s | Number with data | N/K | Number blank |
|---|---|---|---|
| Sex of victim/s | 127 | - | - |
| Age at time of death | 125 | 2 | - |
| Relationship to perpetrator | 113 | 14 | - |
| Ethnicity | 119 | 8 | - |
| Nationality | 114 | 13 | - |
| Is religion a relevant factor? (Y, N or N/K) | 111 | 16 | - |
| Sexual Orientation - state orientation and how known, or mark N/K | 110 | 17 | - |
| Is or was the victim a carer? (Y, N or N/K) | Y = 10 N=113 |
4 | - |
| If Yes, had they had a carer’s assessment under the Care Act? (Y, N or N/K) | Y = 0 N=118 |
9 | - |
| Questions on victim vulnerabilities | Number with data | N/K | Number blank |
|---|---|---|---|
| Mental ill health | 42 | - | 85 |
| Illicit drug use | 27 | - | 100 |
| Problem alcohol use | 35 | - | 92 |
| Pregnancy | 0 | - | 127 |
| Physical disability | 15 | - | 112 |
| Learning disability | 6 | - | 121 |
| Questions on victim mental health Issue/s identified in the DHR | Number with data | N/K | Number blank |
|---|---|---|---|
| Depression | 39 | - | 88 |
| Psychosis | 6 | - | 121 |
| Self-harm | 6 | - | 121 |
| Suicidal thoughts | 24 | - | 103 |
| Suicidal attempts | 20 | - | 107 |
| Low mood / anxiety (no diagnosis) | 21 | - | 106 |
| Panic attacks | 4 | - | 123 |
| Anxiety | 17 | - | 110 |
| PTSD | 4 | - | 123 |
| Adjustment Disorder | 1 | - | 126 |
| Dementia or Alzheimer’s disease | 4 | - | 123 |
| Not specified | 2 | - | 125 |
| Any serious or life limiting illness? | Y = 16 N = 97 |
14 | - |
| Has the victim been a target of an abuser before? | Y = 36 N = 43 |
48 | - |
| Questions on perpetrator/s | Number with data | N/K | Number blank |
|---|---|---|---|
| Sex of perpetrator | 109 | - | - |
| Age at time of fatal incident | 103 | 6 | - |
| Relationship to victim/s | 107 | 2 | - |
| Ethnicity | 101 | 8 | - |
| Nationality | 92 | 17 | - |
| Is religion a relevant factor? (Y, N or N/K) | N=92 | 17 | - |
| Sexual Orientation - state orientation and how known, or mark N/K | 88 | 21 | - |
| Is or was the victim a carer? (Y, N or N/K) | Y = 13 N=88 |
8 | - |
| If Yes, had they had a carer’s assessment under the Care Act? (Y, N or N/K) | Y = 1 N=8 |
2 | 98 |
| Questions on perpetrator vulnerabilities | Number with data | N/K | Number blank |
|---|---|---|---|
| Mental ill health | 41 | - | 68 |
| Illicit drug use | 39 | - | 70 |
| Problem alcohol use | 43 | - | 66 |
| Physical disability | 4 | - | 105 |
| Learning disability | 2 | - | 107 |
| Other | 2 | - | 107 |
| Questions on perpetrator mental health Issue/s identified in the DHR | Number with data | N/K | Number blank |
|---|---|---|---|
| Depression | 33 | - | 76 |
| Psychosis | 14 | - | 95 |
| Self-harm | 8 | - | 101 |
| Suicidal thoughts | 30 | - | 79 |
| Suicidal attempts | 16 | - | 93 |
| Low mood / anxiety (no diagnosis) | 13 | - | 96 |
| Panic attacks | 1 | - | 108 |
| Anxiety | 18 | - | 91 |
| PTSD | 3 | - | 106 |
| Adjustment Disorder | 1 | - | 108 |
| Dementia or Alzheimer’s disease | 0 | - | 109 |
| Other | 6 | - | 103 |
| Any serious or life limiting illness? | Y = 10 N = 77 |
22 | - |
| Had the perpetrator abused previous partner/s or family member before? (Y, N or N/K) | Y = 45 N = 30 |
34 | - |
| Was the perpetrator known to agencies as an abuser? (Y, N or N/K) | Y = 49 N = 49 |
11 | - |
| Has the perpetrator any previous offending history? (Y, N or N/K) | Y = 51 N = 34 |
24 | - |
| Was the perpetrator being managed or supervised by, or attending any of the following? | Number with data | N/K | Number blank |
|---|---|---|---|
| MAPPA | 4 | - | 105 |
| National probation | 7 | - | 101 |
| Mental health services | 7 | - | 102 |
| Drug and alcohol services | 3 | - | 106 |
| Attending or had attended a perpetrator programme | 1 | - | 108 |
| Crime details, MARAC and outcome of trial | Number with data | N/K | Number blank |
|---|---|---|---|
| Had the victim been referred to MARAC? (Y, N or N/K) | Y=25 N=99 |
- | - |
| Was the case heard at MARAC before the homicide? (Y, N or N/K) | Y=21 N=4 |
- | 99 |
| Method of killing if relevant please state weapon used | Number with data | N/K | Number blank |
|---|---|---|---|
| Firearm | 1 | - | 106 |
| Stabbing knife | 49 | - | 58 |
| Strangulation | 25 | - | 82 |
| Blunt force trauma | 8 | - | 99 |
| Other | 17 | 2 | 88 |
| Details of court verdicts | Number with data | N/K | Number blank |
|---|---|---|---|
| Murder | 62 | - | 41 |
| Manslaughter | 25 | - | 78 |
| Diminished responsibility | 9 | - | 94 |
| Unfit to plead | 4 | - | 99 |
| Not guilty | 4 | - | 103 |
| Other | 9 | - | 94 |
| Details, if reviewing suicide or murder / suicide | Number with data | N/K | Number blank |
|---|---|---|---|
| Is DHR reviewing a murder and suicide? (Y or N) | homicide and suicide 11 suicide 14 |
| If DHR is reviewing a death by suicide, please answer the following | Number with data | N/K | Number blank |
|---|---|---|---|
| Sex of deceased | 14 | - | - |
| Method of suicide | 11 | - | 3 |
| Aggravating factors | Number with data | N/K | Number blank |
|---|---|---|---|
| Immigration issues (V if relevant for victim and / or P if relevant for perpetrator) | 4 | - | 120 |
| Forced marriage | 1 | - | 123 |
| HBV | 2 | - | 122 |
| Physical stalking | 14 | - | 110 |
| Digital stalking | 6 | - | 118 |
| Coercive control | 51 | - | 73 |
| Details of children if relevant (0-18yrs) | Number with data | N/K | Number blank |
|---|---|---|---|
| Did the parties in the DHR have parental responsibility for children? (Y, N or N/K) | Y=50 N=71 |
3 | - |
| If yes, please give sex of child/ren | * | * | * |
| If yes, please give age of child/ren | * | * | * |
| Were children subject to child protection procedures due to domestic abuse? (Y, N or N/K) | Y=12 N=32 |
2 | 78 |
| Any children removed into care of local authority? (Y, N or N/K) | Y=10 N=37 |
1 | 76 |
* Considerable variation in the amount of information given
Appendix 4. Selection of themes from DHRs
The identified themes for Themes in Domestic Homicide Reviews have come from a randomly selected sample of 50 of the 124 DHRs.
The identification of themes is from the sections on analysis from the 50 DHRs. DHRs have a standard, commonly used structure:
- an introduction section looking at items such as: terms of reference (what the review is about and the time period it refers to), engagement with family, contributors to the review, and equality and diversity
- a review of the facts of the case, a chronology
- a section on analysis
- conclusions, lessons learnt, and recommendations
There is variation between DHRs in the analysis sections: in some key lessons learnt and recommendations are also included.
The selection of themes was from counts of occurrence of 32 words, derived from:
- the themes in the 2016 [footnote 45] report Key Findings from Analysis of Domestic Homicide Reviews [footnote 46]
- additional words from those most frequently occurring in the analysis sections of the (50) DHRs
- additional words from those most commonly occurring in recommendations from these DHRs, those used for chapter 7: Analysis of recommendations in Domestic Homicide Reviews. There is an overlap with the analysis sections as some recommendations occurred in these
The table below gives these 32 words and their rank from the number of times they occurred in recommendations in the sample DHRs or their analysis sections.
Following the counts of frequently occurring words some were excluded:
- those about specific agencies (e.g., health, police), as these are included in the sections on each theme in chapter 5
- the term practice, as this was frequently related to general practice(s) i.e., doctors
- words which were about the overall subject or process e.g. abuse, domestic, review, panel, violence
The occurrence of the 32 words was then ranked for each of the two sources (recommendations and analysis) and a final rank produced from these.
The themes have been identified come from the from nine words highlighted in the table below. They account for 65% of the total word counts (of the 32 words) in recommendations and 72% of the analysis sections.
Section 6, Themes in domestic homicide reviews is from the nine words in the table marked *.
| Word | Rank from recommendations | Rank from analysis sections | Final rank |
|---|---|---|---|
| *Risk | 2 | 1 | 1 |
| *Support | 3 | 2 | 2 |
| *Information | 4 | 3 | 3 |
| *Training | 1 | 8 | 4 |
| *Assessment | 6 | 4 | 5 |
| *Referral | 5 | 7 | 6 |
| *Record | 8 | 6 | 7 |
| Within | 7 | 9 | 8 |
| *Contact | 16 | 5 | 9 |
| multi | 12 | 12 | 10 |
| management | 11 | 13 | 10 |
| *Policy | 10 | 14 | 10 |
| awareness | 9 | 16 | 13 |
| between | 17 | 10 | 14 |
| procedure | 14 | 14 | 15 |
| sharing | 15 | 18 | 16 |
| public | 13 | 22 | 17 |
| partnership | 28 | 11 | 18 |
| capacity | 23 | 17 | 19 |
| organisation | 19 | 21 | 19 |
| knowledge | 21 | 20 | 21 |
| quality | 17 | 24 | 21 |
| communication | 20 | 23 | 23 |
| understanding | 26 | 19 | 24 |
| identification | 22 | 25 | 25 |
| data | 23 | 27 | 26 |
| skills | 23 | 28 | 27 |
| planning | 27 | 26 | 28 |
| competence | 28 | 29 | 29 |
| intra-agency | 28 | 30 | 30 |
The word “within” was examined but was not selected as it had a number of different uses which reduced its significance as one theme. Examples of uses of “within”:
- time: (i.e. within 24hrs)
- remit or operation of agencies i.e. within and outside the service
- the location of staff of one agency within another
- the theme of records i.e. information was within or not within records
Glossary
AAFDA: advocacy after fatal domestic abuse
DA: domestic abuse
DASH: domestic abuse, stalking and honour based violence assessment tool
DHR: domestic homicide review
GP: general practitioner (doctor)
HBV: honour based violence
IMR: individual management review
MAPPA: multi-agency public protection arrangements
MARAC: multi-agency risk assessment conference
MIR: management information report
ONS: Office for National Statistics
PTSD: post-traumatic stress disorder
Footnotes
-
The word death has been used as not all the deaths in the DHRs are proven homicides. A proportion are death by suicide. ↩
-
Home Office, (2016) Multi-agency Statutory Guidance for the Conduct of Domestic Homicide Reviews ↩
-
Home Office (2013) Terms of reference: Domestic Homicide Review Quality Assurance Panel ↩
-
In one review there are two victims killed and in another there are three victims. ↩
-
There are two DHRs where there are two perpetrators and one where four people have been included as perpetrators. ↩
-
Home Office, (2016) Domestic Homicide Reviews, Key Findings from Analysis of Domestic Homicide Reviews ↩
-
The median number is 2 years. This is from 81 of the 124 reviews where the date the report was submitted to the Home Office is available. Seven of these were asked to be resubmitted: the date used has been the original submission. The number of years between the date of death and date of submission is simply based on the year in the date rather than the full date. ↩
-
The local authorities referred to here are either, using the ONS classifications, London borough, metropolitan district, non-metropolitan district or unitary. Nine DHRs have been excluded as their locations have been given in five counties in England but no further detail that would enable the local authority district to be identified. ↩
-
The regions used are those as shown by the Office for National Statistics Detailed information on the administrative structure within England ↩
-
Average as the median age. This is of the 125 victims where the age has been given. ↩
-
The median age of 108 perpetrators where age was given. ↩
-
This is from 94 reviews where the age of both victim and perpetrator is known and where there is only one perpetrator and one victim. In 44 reviews the victim was younger, in 42 the victim was older, and in 8 reviews the ages were similar. ↩
-
These are 94 domestic homicides reviews where the ages of the victims and perpetrators was known. ↩
-
This is probably a slight underestimate. The information used is that from the management information reports and, where this is incomplete, from the DHRs. As an example of remaining missing data, in one review the MIR has no information on the number of children, however, the review states “Victim was 6 months pregnant and had two children, location unknown”. ↩
-
Words and phrases used include: asphyxiation, pressure to neck, strangulation, and suffocation. ↩
-
The management information reports were asked for information on vulnerabilities to be given as Y (yes) or N (no) – see Appendix 1. There is no request to indicate whether the vulnerability is N/K (not known). If the number of N/K were identified and the percentages were given as proportions of the totals known, then the proportions of victims with vulnerabilities would be higher. ↩
-
None was identified with four vulnerabilities. ↩
-
These can be from a variety of sources such as a GP or views given by friends or family. ↩
-
Mental health is one of the vulnerabilities ask for identification in the MIRs. This is the 34% given in Figure 4. The 48% given in this section on mental health is from the details asked in MIRs on mental health issues. As implied, there are a number of victims where a specific mental health issue is identified where the vulnerability of mental health was not indicated. ↩
-
This includes the victims who died by suicide. ↩
-
The definition of a carer in this context refers to an adult or young person who is caring for someone due to their health and social care needs. This includes mental health as well as physical health support, which would entitle the carer to a Carer’s Assessment under the Care Act 2014. The Children and Families Act 2014 also includes duties for the assessment of young carers and parent carers of children under 18. ↩
-
Life-limiting illness describes an incurable condition that will shorten a person’s life, though they may continue to live active lives for many years. There is a wide range of life-limiting illnesses, including heart failure, lung disease, neurological conditions, such as Parkinson’s and Multiple Sclerosis, and cancer that is no longer responding to treatment intended to cure. ↩
-
This includes those victims who died by suicide. ↩
-
The occurrence of immigration was noted for some perpetrators as well as victims. ↩
-
Median age. ↩
-
The number of perpetrators for this chapter relates to the DHRs in the following ways. In six DHRs the perpetrators were either not charged or not found guilty, so the information has not been included. Apart from one section in this chapter, information on the 14 DHRs where the perpetrator committed suicide was not requested in the MIRs. There are three reviews where there was more than one perpetrator and the information on all has been included. ↩
-
The potential for underestimation as given in footnote 16 also applies to vulnerabilities for perpetrators. ↩
-
The potential for underestimation as given in footnote 16 also applies with mental health issues for perpetrators. ↩
-
As noted with victims, there were a number where a detailed mental health issue was identified but where mental health had not been identified as a vulnerability. ↩
-
Some information in this section is given as numbers rather than percentages. This is because there can be larger numbers where the answer has been left blank or N/K (not known). It is possible that the answers blank or N/K may not be evenly divided between those where the answer is Yes or No Appendix 2 Methods of abstraction of data for analysis, gives more information. ↩
-
Information on whether the perpetrator had previous offending history is available for 85 and missing for 24. Sixty percent is the 51 of 89 known. It is possible that the perpetrators where the information is missing are more likely not to have previous offending history – if so then the 60% would be less (more information is given in Appendix 2). ↩
-
Half of the perpetrators where information was available. There were 11 perpetrators where the information was missing ↩
-
Health agencies referred to include Accident and Emergency, GPs and mental health. ↩
-
Four perpetrators were recorded as being supervised by two agencies and one by four agencies. ↩
-
This includes two perpetrators who were supervised/managed by both. ↩
-
Appendix 4. Selection of themes from DHRs gives more information on the approach used. ↩
-
Home Office, (2016) Domestic Homicide Reviews, Key Findings from Analysis of Domestic Homicide Reviews ↩
-
For example “the comments made would support the view of the panel that at times the practitioners and agencies coming into contact with Shelly and Mike demonstrated a real lack of professional curiosity”. ↩
-
For example, a general reference to Local Authority or a rare reference to a function such as environmental health. Housing and Social Services, adult or children, have been counted separately. ↩
-
Home Office, (2016) Domestic Homicide Reviews, Key Findings from Analysis of Domestic Homicide Reviews ↩
-
Home Office (2016) Multi-agency Statutory Guidance for the Conduct of Domestic Homicide Reviews ↩
-
Section 7(74) On being presented with the overview report and executive summary the review panel should: a) ensure that contributing organisations and individuals are satisfied that their information is fully and fairly represented in the reports; b) be satisfied that the reports accurately reflect the review panel’s findings; c) ensure that the reports have been written in accordance with this guidance; and d) be satisfied that the reports are of a sufficiently high standard for them to be submitted to the Home Office ↩
-
Section 78 (78) On receiving the documents the CSP should: a) agree the content of the overview report, executive summary and action plan, ensuring that they are fully anonymised apart from including the names of the review panel chair and members; b) make arrangements to provide feedback and debriefing to staff, family members and the media as appropriate; c) sign off the overview report, executive summary and action plan. For brevity sections (d), (e), and (f) are not included here. See guidance page 22-23. ↩
-
Home Office, (2016) Domestic Homicide Reviews, Key Findings from Analysis of Domestic Homicide Reviews ↩
-
Figure3, page 16 of that report. ↩