Newborn hearing screening standards data report 1 April 2017 to 31 March 2018
Published 23 October 2019

© Crown copyright 2019
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/newborn-hearing-screening-standards-data-report-april-2017-to-march-2018/newborn-hearing-screening-standards-data-report-1-april-2017-to-31-march-2018
This report presents data against each of the screening standards for the NHS newborn hearing screening programme (NHSP) in England from 1 April 2017 to 31 March 2018.
The data source is the NHSP national IT system, SMaRT4Hearing (S4H), which is used to collect screening and audiology data across England. Data is presented by local NHSP screening sites.
Newborn hearing screening aims to identify permanent moderate, severe and profound deafness and hearing impairment in newborn babies.
Newborn hearing screening is provided locally by a skilled workforce of hearing screening teams, working predominantly in maternity units. The teams are led by local managers and liaise closely with audiology and paediatric teams to provide a high quality, safe and effective service for the local population.
The NHSP pathway begins with the identification of babies eligible for screening and includes undertaking the relevant screening tests. It ends for babies who pass the screen or for those with screen-positive results, up to and including the point of referral to audiology and entry into audiological assessment.
National NHSP standards provide a defined set of measures that providers must meet to make sure services are safe and effective.
1. NHSP standards
There are 5 national NHSP standards, which are:
-
NHSP-S01: coverage
-
NHSP-S02: test: well babies who do not show a clear response in both ears at automated otoacoustic emission 1 (AOAE1)
-
NHSP-S03: test: referral rate to diagnostic audiological assessment
-
NHSP-S04: referral: time from screening outcome to offered appointment for diagnostic audiological assessment
-
NHSP-S05: diagnosis/intervention – time from screening outcome to attendance at an audiological assessment appointment
We produce standards data quarterly for local providers and publish it annually unless the standard is also a key performance indicator (KPI) in which case we published the data quarterly.
Two thresholds (acceptable and achievable) are specified for each standard: the acceptable threshold and achievable threshold.
Data is presented by financial year (1 April 2017 to 31 March 2018) unless stated otherwise.
2. Results
The quality and completeness of NHSP data is high. This is a result of accurate data input and effective use of S4H by every local screening and audiology service.
The data shows that most regions meet the acceptable threshold for some screening standards. However, London is the only region to meet the acceptable threshold for all 5 standards.
There are 109 local NHSP screening services in England, which screened between 1,296 and 24,866 babies during the year. There is no correlation between the size of local services and their ability to meet screening standards.
NHSP services offer either a community model, where screening does not usually start until after 10 days of age, or a hospital model, where most babies are screened by 10 days of age.
There are 6 community-based services, all in the South region. Calculations are based on the current model at the time of reporting for services that changed from community to hospital model during or after the period 1 April 2017 to 31 March 2018.
2.1 Table 1: national and regional summary
| Regional summary | NHSP-S01 (KPI NH1) (%) | NHSP-S02 hospital (%) | NHSP-S02 community (%) | NHSP-S03 hospital (%) | NHSP-S03 community (%) | NHSP-S04 (%) | NHSP-S05 (KPI NH2) (%) |
|---|---|---|---|---|---|---|---|
| Acceptable | ≥ 98.0 | ≤ 27.0 | ≤15.0 | ≤ 3.0 | ≤ 1.6 | ≥ 97.0 | ≥ 90.0 |
| Achievable | ≥ 99.5 | ≤ 22.0 | ≤13.5 | ≤ 2.0 | ≤ 1.3 | ≥ 99.0 | ≥ 95.0 |
| London | 98.5 | 22.2 | - | 2.5 | - | 97.3 | 91.2 |
| Midlands and East | 98.5 | 24.2 | - | 2.3 | - | 97.4 | 90.0 |
| North | 98.2 | 25.5 | - | 3.3 | - | 96.9 | 87.1 |
| South | 98.9 | 20.2 | 15.5 | 1.8 | 1.8 | 94.5 | 86.8 |
| England | 98.5 | 23.4 | 15.5 | 2.5 | 1.8 | 96.7 | 88.7 |
3. NHSP-S01: coverage (KPI NH1)
NHSP-S01 provides assurance that screening is offered to parents of all eligible babies and that each baby, for whom the offer is accepted, has completed screening and has an outcome.
This standard gives the proportion of babies eligible for newborn hearing screening for whom the screening process is complete by 4 weeks corrected age (hospital programmes-well babies, neonatal intensive care unit (NICU) babies) or by 5 weeks corrected age (community programmes-well babies).
There were 639,460 babies eligible for newborn hearing screening during the year. Of these, 629,920 had completed screens by 4 to 5 weeks corrected age.
Across England, 98.5% of babies eligible for screening had the screen completed by 4 to 5 weeks of age with the rate increasing to 99.3% by the age of 3 months. 0.1% of parents or carers declined the newborn hearing screen. See separate data tables spreadsheet for full NHSP-S01 data broken down by local NHSP screening service.
A regional variation can be seen. All regions met the acceptable threshold (≥ 98.0%) but none managed to meet the achievable threshold (≥ 99.5%). 90 out of 109 NHSP sites met the acceptable threshold, including 15 that met the more stringent achievable threshold. The 19 services that did not meet the acceptable threshold should investigate why the standard was not met and put in place plans to work towards improvement.
One service (West Suffolk) appears to have a much lower coverage rate than other services. This was due to babies born at the USAF Lakenheath base not being eligible for the English newborn hearing screening programme, but being included in their denominator. Re-mapping records within the NHSP national IT system will resolve this issue in the future.
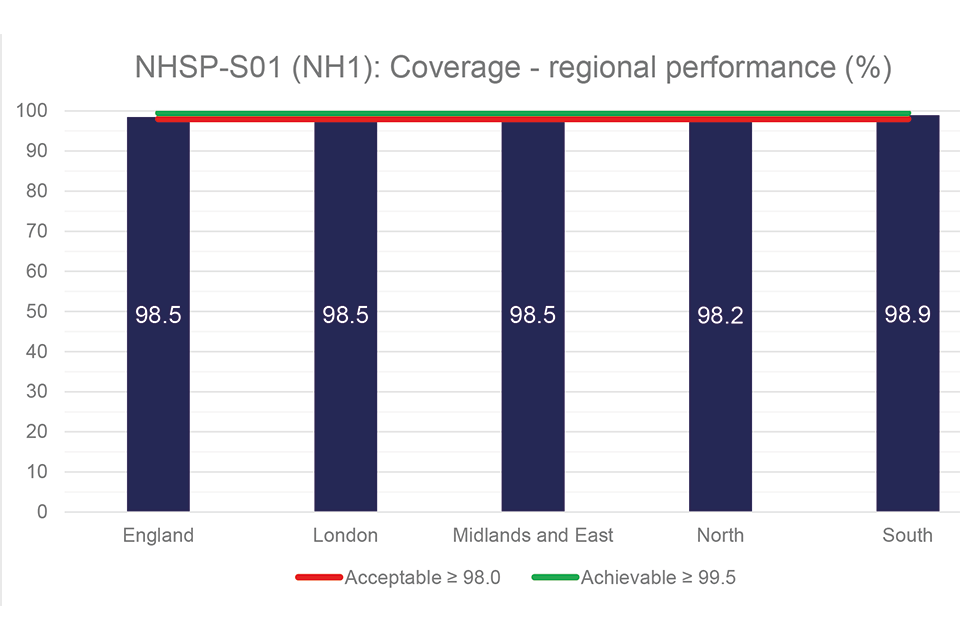
Figure 1: NHSP-S01 – coverage (KPI NH1) regional performance
4. NHSP-S02: test – well babies who do not show a clear response in both ears at automated otoacoustic emission 1 (AOAE1)
The standard NHSP-S02 is needed to monitor the performance of the screening test, minimise harm and maximise performance.
There are different thresholds for hospital and community programmes due to the older age at which most babies are tested in a community based model. Factors which may affect attainment of this standard include screener technique and test conditions (environment). NHSP sites should put staff training and assessment plans in place to help improve achievement of this standard.
In hospital-based services across England, nationally the acceptable threshold (≤ 27%) was met, with the South being the only region to meet the achievable threshold (≤ 22%). 22 out of 103 hospital services did not meet the acceptable threshold, most of which were in the Midlands and East or North regions.
A total of 34 services met the achievable threshold. It is worth noting that some of these changed from a community model during the reporting period, which may account for an apparently much lower rate than other hospital-based services.
In community programmes, 4 out of 6 services met the acceptable threshold of ≤ 15% including 2 that also met the achievable threshold of ≤ 13.5%. The remaining 2 services failed to meet the acceptable threshold. All 6 community services are within the South region, which overall does not meet the acceptable threshold.
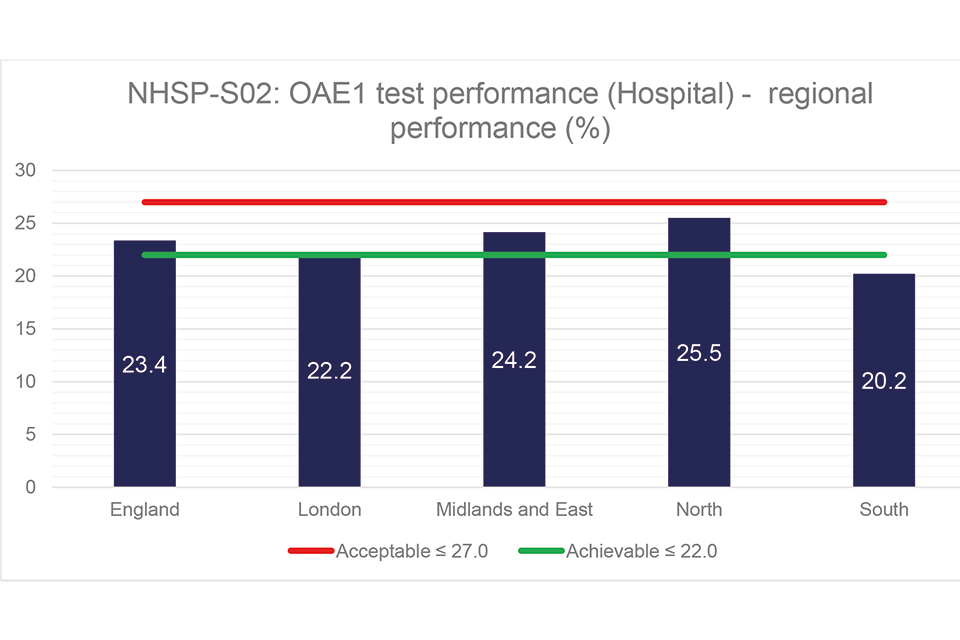
Figure 2: NHSP-S02 – regional performance (hospital)
5. NHSP-S03: test – referral rate to diagnostic audiological assessment
NHSP-S03 is needed to monitor the performance of the screening test at the final result of the screen to minimise harm and to maximise performance.
High rates of referral can be caused by poor screener technique or screening conditions. High referral rates may also lead to over-burden of resources in audiology and increased parental anxiety.
50 of the 103 hospital-based sites in England met the achievable rate of ≤ 2% of babies being referred from the screen for audiological assessment. There was a wide variation in attainment between services, with 22 not meeting the acceptable threshold of ≤ 3%, 13 of which were in the North region.
More stringent thresholds are set in community-based services because babies are screened at an older age. 3 of the 6 community services managed to meet the acceptable level of ≤1.6%.
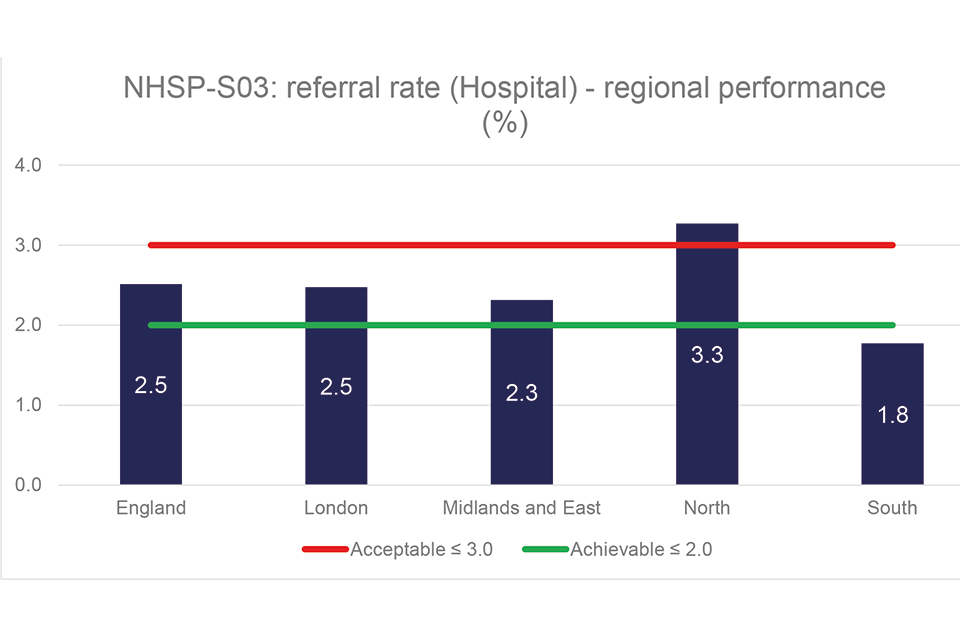
Figure 3: NHSP-S03 – regional performance (hospital)
6. NHSP-S04: referral – time from screening outcome to offered appointment for diagnostic audiological assessment
NHSP-S04 is important as it relates to the timely assessment in audiology for babies referred from the screen. If this standard is not met then it is unlikely that standard 5 will be achieved, which may lead to a delay in assessment of babies.
Nationally, the acceptable threshold of ≥ 97.0% for standard 4 was not met. Only 2 regions met the acceptable rate, and none met the achievable rate of ≥ 99.0%.
The achievable threshold was met by 28 services while 39 services did not meet the acceptable threshold, most of these being in the Midlands and East and North regions.
A review of the process for arranging and prioritising appointments in audiology for babies referred from the newborn hearing screen may help local services achieve the standard.
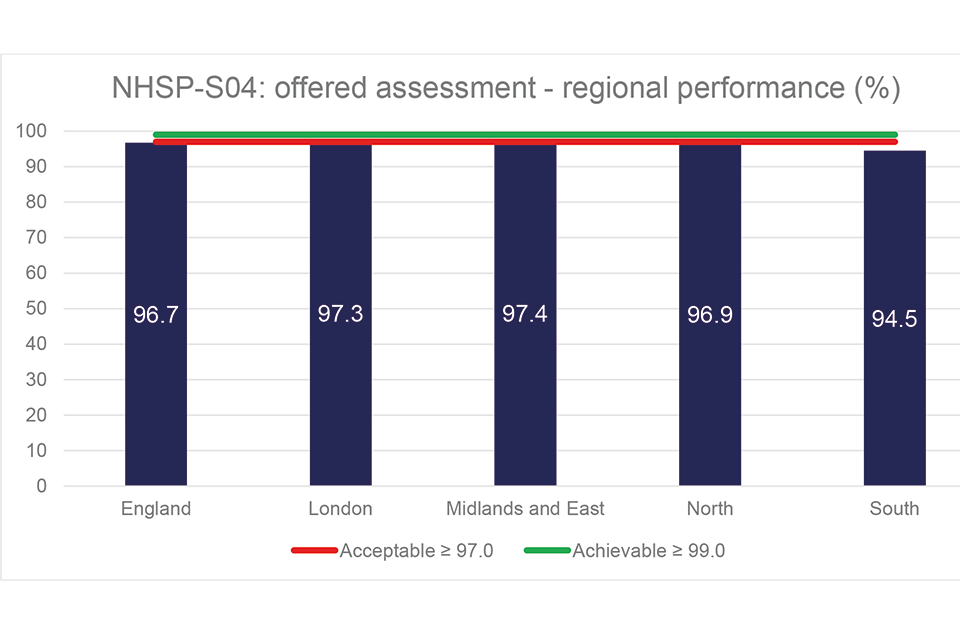
Figure 4: NHSP-S04 – regional performance
7. NHSP-S05: diagnosis/intervention – time from screening outcome to attendance at an audiological assessment appointment (KPI NH2)
NHSP-S05 has been a long-term focus for the programme and it is disappointing that some sites are still unable to meet the acceptable threshold of ≥ 90.0%.
Early identification of hearing loss is an important aim of the newborn hearing screening programme and this will not be achieved if assessment in audiology is delayed. The data shows though that attainment of the standard is not always associated with the diversity of the population or the number of babies referred because London is the only region in England able to meet the acceptable threshold.
There was a wide range in performance (range 60.9% to 100%) with some smaller services being in the lower range group. Of the 109 sites, only 18 met the achievable rate of ≥ 95.0% while 46 did not meet the acceptable threshold, most of these being located in the North.
Local services should put measures in place to review their performance and look to higher achieving services to learn from their good practice. Sites should consider basic factors such as making sure that audiology appointments are offered to parents at a time or location convenient to them and that screening teams stress the importance of attending audiology.
A report entitled Time from screening outcome to attendance at an audiological appointment (NHSP standard 5): learning from best performing sites was published in January 2018 with a checklist (see appendix 5 of the report) to help NHSP sites look at ways to improve their processes based on learning from the best performing services. The report highlighted the main factors that enable success in achieving this standard.
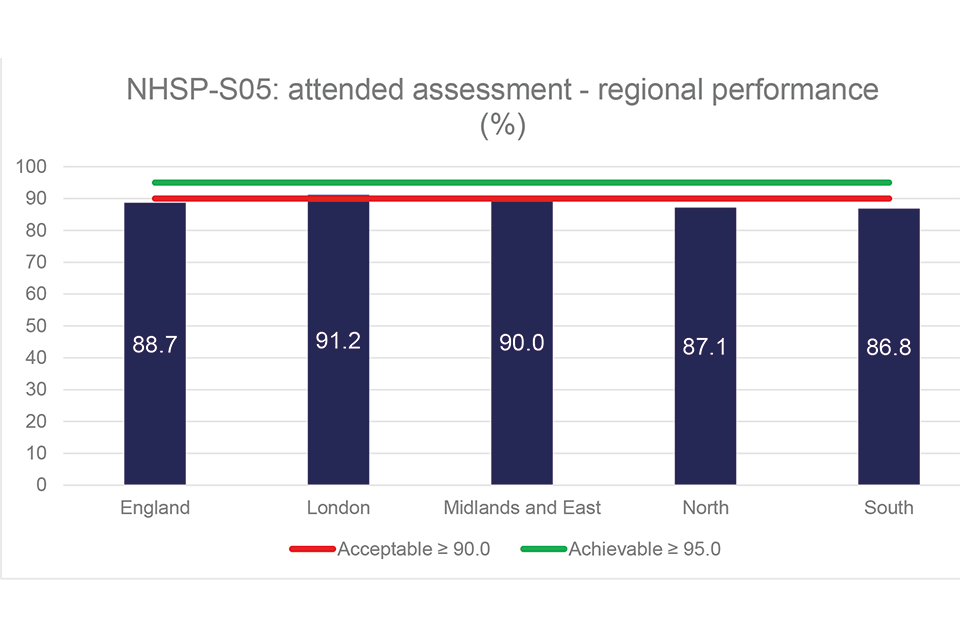
Figure 5: NHSP-S05 – regional performance