Dupuytren’s contracture: clarification of intention and amendment of the prescription
Updated 14 April 2023

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/dupuytrens-contracture-clarification-of-intention-and-amendment-of-the-prescription/dupuytrens-contracture-clarification-of-intention-and-amendment-of-the-prescription
In May 2014 the Industrial Injuries Advisory Council (IIAC) published a command paper ‘Dupuytren’s contracture due to hand-transmitted vibration’ in which recommendations were made to add Dupuytren’s contracture (DC), due to hand-transmitted vibration, to the list of Industrial Injuries Disablement Benefit (IIDB) prescribed diseases. This was initially rejected by the Minister for Disabled People, Health and Work. Following engagement by IIAC members with the minister, it was announced in the 2018 Budget Statement that Dupuytren’s would be added to the list of IIDB prescribed diseases.
The recommendations of the 2014 command paper are:
The council recommends that Dupuytren’s contracture be added to the list of prescribed diseases for which benefit is payable, when severe enough to involve fixed flexion deformity and following exposure of at least 10 years in aggregate to the tools and activities presently scheduled in relation to Prescribed Disease A12(a) (carpal tunnel syndrome).
| Disease | Occupation |
|---|---|
| Dupuytren’s contracture resulting in fixed flexion deformity of one or more digits | Any occupation involving the use of hand-held powered tools whose internal parts vibrate so as to transmit that vibration to the hand, but excluding those tools which are solely powered by hand, where the use of those tools amounts to a period or periods in aggregate of at least 10 years and where, within that period or those periods, the use of those tools amounts to at least 2 hours per day for 3 or more days per week and where the onset of the disease fell within the period or periods of use specified in this paragraph. |
In the command paper the council proposed that cases affecting only the palm and with no involvement of the fingers should be excluded from consideration; for the purposes of prescription, the disease should involve fixed flexion deformity (contracture) of one or more of the digits.
Clarification of the prescription
In 2019 Department for Work and Pensions (DWP) policy officials asked that the 2014 command paper be reviewed by the council and feedback provided to ensure the legislation was written to reflect the council’s intentions that it is the disabling condition which should be prescribed.
A group of council members with expertise in this area then considered in more detail the severity of disease that should be considered for a diagnosis under the prescription and also how to assess the severity. A member presented a paper describing the progression of the disease and information on severity staging together with illustrative diagrams. Members felt that the prescription should be worded to reflect the intention that only the disabling element of the condition should be applicable.
It was felt that the diagnosis and severity of the contracture were 2 separate issues. The 2014 command paper highlighted the Hueston table top test[footnote 1] as a useful rough guide to severity. With this test, the person places their hand on a table. If the hand lies completely flat on the table, the test is considered negative. If the hand cannot be placed completely flat on the table, leaving a space between the table and a part of the hand as big as the diameter of a ballpoint pen, the test is considered positive.
However, council members felt that the use of this test as an initial filter for claims could potentially lead to a large number of claims where there was no significant contracture (fixed flexion of a finger or thumb) and this would not attract any benefit. It was decided that the Tubiana scale for assessing severity by degrees of fixed flexion was more appropriate[footnote 2].
To reflect this scale, the council agreed that the terminology needed to be strengthened and made more explicit, so revised the recommendation of the wording of the prescription to read “ ….fixed flexion deformity of one or more interphalangeal joints of one or more of the digits”.
The revised wording of the prescription is now:
| Disease | Occupation |
|---|---|
| A. 15 Dupuytren’s contracture of the hand involving: (i) fixed flexion deformity of one or more metacarpophalangeal joints greater than 45 degrees* that developed during the period or periods set out in the second column in relation to this paragraph; or (ii) fixed flexion deformity of one or more interphalangeal joints that developed during the period or periods set out in the second column in relation to this paragraph; or (iii) fixed flexion deformity of one or more metacarpophalangeal joints greater than 45 degrees that developed after the period or periods in the second column in relation to this paragraph if there is evidence of the onset of metacarpophalangeal joint involvement or palmar changes (nodules or thickening)** during that period or periods; or (iv) fixed flexion deformity of one or more interphalangeal joints that developed after the period or periods set out in the second column in relation to this paragraph if there is evidence of the onset of metacarpophalangeal joint involvement or palmar changes (nodules or thickening) during that period or periods |
Any occupation involving the use of hand-held powered tools whose internal parts vibrate so as to transmit that vibration to the hand (but excluding those tools which are solely powered by hand) where: (a) the use of those tools amounts to a period or periods in aggregate of at least 10 years; and (b) within that period or those periods, the use of those tools amounts to at least 2 hours per day for 3 or more days per week |
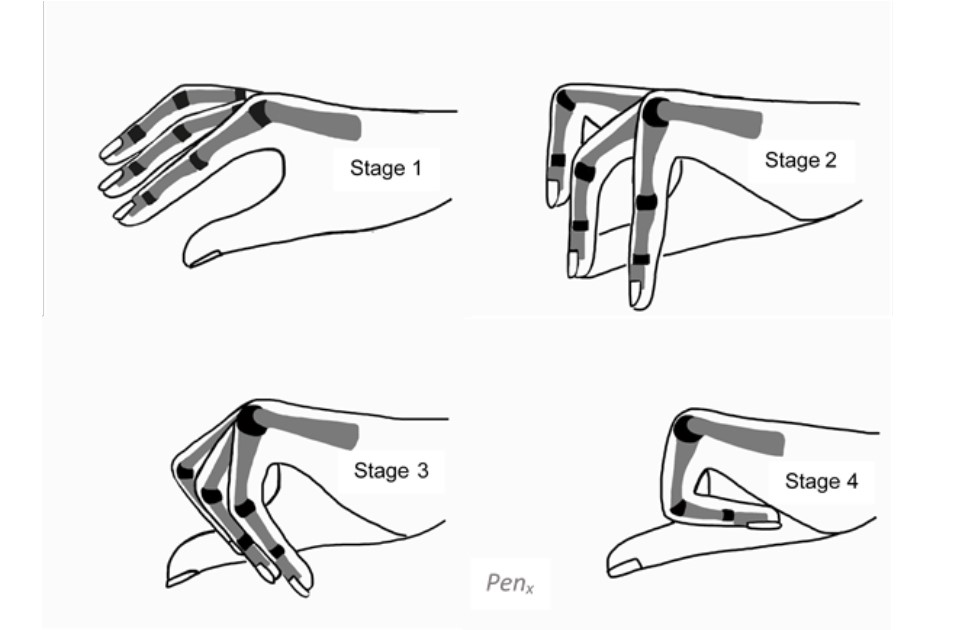
* A fixed flexion deformity is when the joints of the digit are pulled down toward the palm of the hand (see Figure 1). While that often will involve the interphalangeal joints (mostly the middle joint of the fingers, and occasionally the end joint of the fingers or thumb), assessment of fixed flexion deformity will include metacarpophalangeal deformity in the overall assessments and also will take into account cases of isolated involvement of the metacarpophalangeal joint (the joint between the digit and the palm) where the deformity is significant (see Stage 1 in Figure 1).
** Thickening, in the context of the prescription, refers to a palpable thickening of the connective tissue (called fascia) that lies beneath the skin: whilst the skin may appear thicker through pitting and puckering it is actually unaffected by Dupuytren’s disease.
Figure 1: Diagram showing various degrees and combinations of contracture at interphalangeal and metacarpophalangeal joints
Summary
The council amended the recommendation to prescribe for Dupuytren’s contracture to ensure the most disabling element of this condition is covered and to provide clarity for claimants to manage their expectations better.
The council hopes that this clarification will help to reduce the number of claims from workers who have the less disabling features of Dupuytren’s contracture.