The appointment and operation of the Patient Safety Commissioner: consultation response
Updated 6 January 2022

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/consultations/the-appointment-and-operation-of-the-patient-safety-commissioner/outcome/the-appointment-and-operation-of-the-patient-safety-commissioner-consultation-response
Background
Why a Patient Safety Commissioner is needed
Patient safety remains a top priority for the government. Enormous emphasis has been placed on patient safety and good progress has been made – for example, through the NHS Patient Safety Strategy, which at its core seeks to improve the way in which the NHS learns, involves patients and encourages staff to speak up when things go wrong.
The Patient Safety Commissioner will add to and enhance this existing work to improve patient safety by acting as a champion for patients, helping us learn more about what we can do to put patients first, and promoting the importance of the views of patients and the public in relation to the safety of medicines and medical devices.
This acts on the second recommendation of the Independent Medicines and Medical Devices Safety Review: First Do No Harm, published in July 2020 by Baroness Cumberlege, which examined the consequences of the use of Primodos, sodium valproate and pelvic mesh, and its effects on patient safety.
Legislative framework and consultation process
The Medicines and Medical Devices Act 2021 (‘the act’) received royal assent on 11 February 2021. Part 1 is about the Patient Safety Commissioner, and section 1 establishes the Commissioner position and sets out its ‘core duties’.
Under the act (paragraph 6 of schedule 1), the Secretary of State can make legislative provisions about the appointment and operation of the Commissioner, for example the terms of office, finances and other support for the Commissioner. This detail on the appointment and operation of the Commissioner is what our consultation sought feedback on, between 10 June and 5 August 2021, in line with the consultation requirement set out at section 45(1) of the act.
Once the Commissioner has been appointed, they must prepare and publish a set of principles to govern the way in which they will carry out their core duties, as detailed in schedule 1 of the act. Interested parties will therefore have further opportunities to comment on matters relating to the Commissioner beyond this specific consultation.
Summary of results
61 respondents, comprised of 34 organisations and 27 individuals, responded to this consultation.
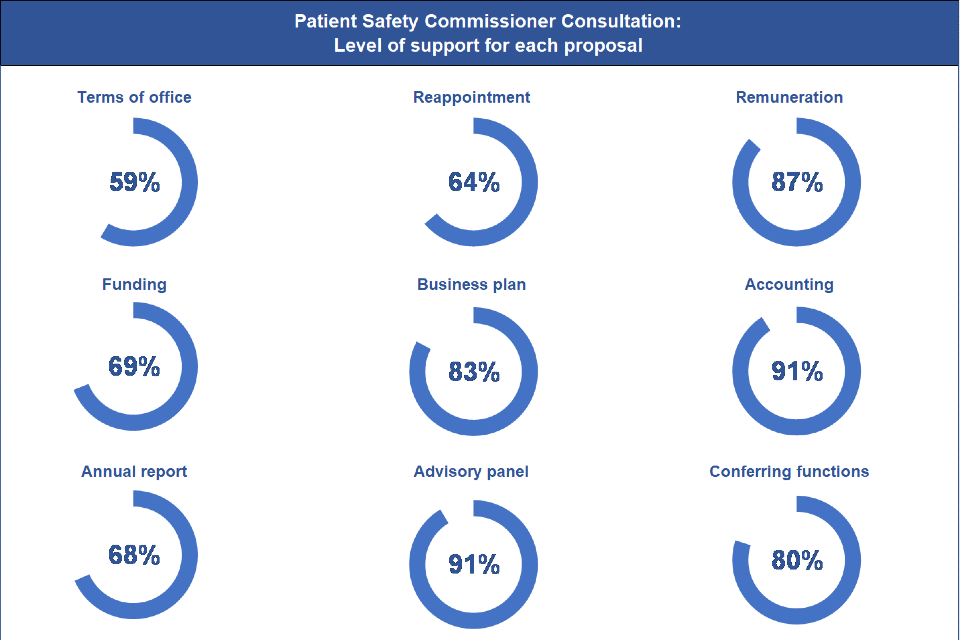
As shown in Infographic 1 below, each of the 9 proposals upon which we consulted were supported by more than half of respondents, ranging from 59% to 91% in agreement. This series of doughnut charts show that:
- 59% agreed or strongly agreed that the Commissioner should serve a term of 3 years
- 64% agreed or strongly agreed that the Commissioner should be eligible for reappointment for an additional term of 3 years and that they may resign or be removed by the Secretary of State
- 87% agreed or strongly agreed that the Commissioner should be remunerated
- 69% agreed or strongly agreed that the Secretary of State should fund the operation of the Commissioner
- 83% agreed or strongly agreed that the Commissioner should routinely publish a business plan to describe their strategic priorities for the coming year
- 91% agreed or strongly agreed that the Commissioner must keep statements of accounts each financial year and provide the Secretary of State with a copy
- 68% strongly agreed that the Commissioner should publish an annual report
- 91% agreed or strongly agreed that the Commissioner should appoint an advisory board
- 80% agreed or strongly agreed that the Commissioner should be able to delegate responsibilities to staff members within their office
Infographic 1: level of support for each proposal made in the Patient Safety Commissioner consultation
A more detailed summary of results is provided in the rest of this section, including a selection of anonymised comments which provide insight into why respondents tended to agree (or disagree) with the proposals. Where comments have been shortened for readability purposes, the omitted text is represented by an ellipsis in square brackets “[…]”. Care was taken to ensure this did not misrepresent the sentiment of the original text when read in full.
Supplementary data tables are available at the end of this report.
Terms of office
Government response
The Department of Health and Social Care (DHSC) will proceed with the proposal that the Patient Safety Commissioner will serve for an initial term of 3 years.
Summary of responses received
59% of respondents agreed or strongly agreed that this length of term was “just right” (see Table 1 in the supplementary data tables section below) with supportive comments such as:
We support this model and support the proposed term of 3 years, as a standard and appropriate duration for similar roles.
Terms of office tend to be for 3 to 4-year terms. This term of office is comparable with similar organisations and enables the Patient Safety Commission to become established in post.
Where respondents disagreed with this proposal, they were most likely to say that 3 years might be “too short” a period to establish the role and make progress against long-term strategic aims.
The Commissioner can, however, be reappointed to serve for an additional 3 years, in effect giving them up to 6 years in office. This offsets the risk, and was recognised in the comments made by several respondents:
We support the proposed 3-year term, although the ability for a Commissioner to be reappointed for a second term is a condition of this. We feel that the potential total of 6 years in post offers an adequate window for a Commissioner to achieve an impact, without allowing one individual or approach to monopolise the role.
[Three years is] Long enough to understand the role, the work needed and to start investigations. S/he can also run again to complete work started.
Reappointment
Government response
DHSC will proceed with the proposal that the Patient Safety Commissioner will be eligible for reappointment after having held office and that they may resign or be removed by the Secretary of State, if appropriate.
Summary of responses received
64% of respondents agreed or strongly agreed with this proposal (see Table 2 in the supplementary data tables section below), commenting that the ability to reappoint an effective Commissioner was important, both for continuity purposes and the ability to affect long-term change:
They [the Commissioner] should be able to be reappointed on a longer basis as long as they are doing a good job and have proved themselves a capable person for the first year. This would be important for continuity.
It is best to retain a positive change-maker longer and that option should be open. If there is a programme of change underway, this gives them the chance to ensure it is implemented and embedded into practice.
Some respondents held reservations over the Secretary of State having the sole discretion to remove the Patient Safety Commissioner from office, if this in turn led to the role becoming politicised and therefore jeopardised its independence.
The freedom to act independently and influence change will be an essential element of the role’s success. It is important that the role of PSC [Patient Safety Commissioner] encourages the right culture from government through to healthcare organisations.
Alternative proposals put forward by respondents included:
- making the role accountable to the Privy Council or Health and Select Committee
- having independent adjudicators oversee any decision to remove the Commissioner
- at the very least, ensuring that the criteria for removal is transparent and adhered to
Given that third-party involvement could create unnecessary bureaucracy, retaining the original proposal is preferable. This is the same provision that is in place for similar roles, such as the Children’s Commissioner for England. We would also expect that existing safeguards – such as the Nolan principles, which set out the ethical standards expected of public office holders – would apply and be upheld by the Patient Safety Commissioner.
Following the consultation, it is the DHSC’s intention to outline in secondary legislation the limited circumstances in which a Secretary of State has the power to remove a Commissioner, for example, if a Commissioner has:
- become unfit or unable to properly discharge their functions
- behaved in a way that is not compatible with continuing in office
Remuneration
Government response
DHSC will proceed with the proposal that the Patient Safety Commissioner shall receive remuneration.
Summary of responses received
87% of respondents agreed or strongly agreed that the Patient Safety Commissioner should be remunerated (see Table 3 in the supplementary data tables section below), both to attract appropriate candidates and to ensure they are able to commit to the role full time.
We do not believe that it will be possible to attract a sufficiently diverse pool of applicants without providing remuneration for a potentially complex and time-consuming role. If the role is not remunerated, then it will be more likely to attract applicants with independent income or require anyone applying for the role to maintain additional employment, which may not be conducive to recruiting a Commissioner who can commit sufficient time and attention to the role.
This is in line with standard practice; for example, the Victims’ Commissioner and the Children’s Commissioner are remunerated. The Patient Safety Commissioner’s salary will therefore be commensurate with equivalent roles and proportionate to the work it entails.
Funding
Government response
DHSC will proceed with the proposal that the Secretary of State will fund the operation of the Patient Safety Commissioner.
Summary of responses received
69% of respondents agreed or strongly agreed that the Secretary of State should fund the operation of the Patient Safety Commissioner (see Table 4 in the supplementary data tables section below). For the majority, this was predicated on the principle that funds will not be allocated or withheld in such a way that would unduly influence the work taken forward by the Commissioner.
As the DHSC will be the Commissioner’s sponsor department of government, we support the proposal that funding comes from the Secretary of State. It is important that the budget is sufficient for the Commissioner to perform their duties to the full. It is also essential that the Commissioner remains operationally separate from and independent of the DHSC.
Those disagreeing with the proposal suggested that the role be funded via a non-DHSC source, such as the Cabinet Office or HM Treasury, saying that this is crucial to ensuring the actual and perceived independence of the Commissioner.
[…] There must be no possibility of ministers choking off the work of a politically inconvenient Patient Safety Commissioner by reducing their operating budget arbitrarily. […]
However, the operation of many similar regulatory and investigative roles and bodies are the responsibility of the relevant Secretary of State. For example, the Children’s Commissioner is sponsored by the Department for Education and the Victim’s Commissioner by the Ministry of Justice.
Independence will necessarily be exercised in the carrying out of the Commissioner’s functions. For example, the Commissioner will have the power to make recommendations or reports to the Secretary of State, who will then be under a duty to consider and respond. The department will expect that the Commissioner makes any such reports or recommendations independently, without recourse to or clearance from the Secretary of State or DHSC.
Business plan
Government response
DHSC will proceed with the proposal that the Patient Safety Commissioner will produce an annual business plan and take reasonable steps to consult before publishing each plan.
Summary of responses received
83% of respondents agreed or strongly agreed that the Commissioner should routinely publish a business plan to describe their strategic priorities for the coming year (see Table 5 in the supplementary data tables section below), not least to ensure their work remains transparent, measurable and centred on patients. The time taken to produce an annual plan should not, however, divert a significant amount of the Commissioner’s resources away from ‘getting things done’.
We would welcome an annual business plan from the Patient Safety Commissioner, and would agree that this should be formed with consultation from relevant stakeholders, especially patients and patient groups. The success of the business plan should also be measured by a report analysing the progress made on the strategic priorities identified.
It is important for the Patient Safety Commissioner to set out on a regular basis their priorities and focus, allowing for their work to remain transparent and accountable to the public they are representing. The business plan must provide a degree of flexibility for the role, however, allowing the Commissioner to respond reactively to any key issues relating to patient safety that arise during a year.
Accounting
Government response
DHSC will proceed with the proposal that the Patient Safety Commissioner is to keep proper accounts each financial year and provide a copy to the Secretary of State.
Summary of responses received
91% of respondents agreed or strongly agreed that the Patient Safety Commissioner must keep statements of accounts each financial year and provide the Secretary of State with a copy (see Table 6 in the supplementary data tables section below), for reasons including:
This is good governance and contributes to ensuring accountability […]
This will ensure transparency concerning the Commissioner’s accounts.
Is it important for public confidence that the commissioner is seen to be appropriately using public funds.
Annual report
Government response
DHSC will proceed with the proposal that the Patient Safety Commissioner shall publish an annual report to explain the activities they have undertaken during the year in relation to their core duties, a copy of which is to be sent to the Secretary of State and laid before each House of Parliament.
Summary of responses received
68% of respondents strongly supported the proposal that the Commissioner should publish an accessible annual report detailing the ways in which they have discharged their functions, including how they have directly engaged with patients and what they have found while doing so (see Table 7 in the supplementary data tables section below).
Aside from maintaining public accountability, respondents felt this provided a critical mechanism through which patient safety issues and necessary improvements can be raised directly with those who have influence over the healthcare system.
[…] Production of an annual report is an established and effective method of providing a public record of the work undertaken during the year and informing the public/stakeholders/sponsoring body of progress made and future plans.
[…] Not only will this reflect the public accountability of the new function, but it will highlight patient safety concerns directly to the parliamentary community.
Some respondents worried that an annual report might mean patient safety concerns are not highlighted through the year when they occur. For example:
I agree, but an annual report is not enough. Patient safety concerns cannot wait for a year! For patients, this new role could make the difference between life or death, or potentially a lifetime of suffering if trends are not spotted and raised immediately. […]
[…] The functions of the PSC should be reflexive and in full sight of both public and government to gain the confidence of the public in the new role and inform government in real time of emerging safety issues. […]
DHSC can confirm that the annual report does not prevent a Patient Safety Commissioner from raising concerns when they learn of them. We would expect that any such concerns are duly considered and acted on as necessary by the Patient Safety Commissioner throughout the year, regardless of when the annual report would be published.
Advisory panel
Government response
DHSC will proceed with the proposal that the Patient Safety Commissioner may appoint an advisory board, whose members will have a broad range of relevant interests, experience and knowledge of the health system, sectors and patients.
Summary of responses received
91% of respondents agreed or strongly agreed that the Patient Safety Commissioner should appoint an advisory board to “enhance the effectiveness of the role” and bring diversity of thought and experience to the Commissioner’s work (see Table 8 in the supplementary data tables section below).
Ensuring that the Patient Safety Commissioner has good channels of communication across the health system, with an ear to the ground across all areas of health and care, is essential so they can undertake their role effectively; engagement with a wide range of voices through an advisory panel is a good step towards this.
The majority of respondents went further in flagging that the most important voice to represent on any panel would be that of patients – those with lived experiences of avoidable harm, including individuals from ‘hard to reach’ or traditionally under-represented groups.
Additional suggestions included (but were not limited to):
- patient safety groups, advocates, charities and organisations
- NHS and independent sector healthcare providers and medical professionals
- safety experts from outside the healthcare sector
- academics
- regulators
- legal professionals
[…] While the role of the Patient Safety Commissioner will be a new one, there are already a diverse range of groups […] that can provide a helpful source of knowledge, insight, information and support. By bringing these organisations into a network, the Commissioner could amplify the voices of many already actively promoting patient safety, especially patient campaigning groups and charities.
To maintain the actual and perceived impartiality of the work of the Commissioner, respondents felt that recruitment to the advisory board should be transparent and that, to attract the broadest range of relevant voices, consideration should be given to remunerating advisors for their time.
[…] an Advisory Panel must be established with full clarity of its role and remit. […]
[…] It is imperative that he/she [the Commissioner] needs to be surrounded by a team of the best advisors possible on safety issues. However, conflicts of interest must be given the highest priority. Unchecked self-declaration must not be allowed. Rigorous recruitment processes must be applied. […]
[…] To ensure the advisory panel is accessible and inclusive of all necessary views, adequate remuneration is essential. Voluntary input is likely to exclude important voices.
Conferring of functions on others
Government response
DHSC will proceed with the proposal that any staff of the Patient Safety Commissioner, so far as authorised by the Commissioner, may exercise any of the Commissioner’s functions.
Summary of responses received
80% of respondents agreed or strongly agreed that the Patient Safety Commissioner should be able to delegate responsibilities to staff members within their office (see Table 9 in the supplementary data tables section below); in essence, operating as an organisation. In the absence of this power, some felt this would limit the scope and volume of work the Commissioner could reasonably be expected to take forward, and that it is important for business continuity.
Given that the role of the Commissioner will be onerous, and involve a large number of obligations across a complex and varied field of work, we would accept that the staff of the Patient Safety Commissioner may exercise any of the Commissioner’s functions […] However, the Commissioner should remain ultimately responsible for the output of the office and staff.
Supplementary data tables
Tables 1 to 9 provide a breakdown of results to this consultation. The shorthand [c] is used where a data point would disclose confidential information (for example, the answer provided by a single respondent). This is in line with Government Statistical Service statistics disclosure control guidelines.
Table 1: respondents’ views on the proposal that the Commissioner would serve an initial term of 3 years
Total number of respondents answering this question: 58
| Answer | Count | Proportion |
|---|---|---|
| Too short | 13 | 22% |
| Just right | 34 | 59% |
| Too long | c | c |
| Don’t know | c | c |
Table 2: extent to which respondents agreed with the proposal that the Commissioner can be reappointed once, can resign and can be removed by the Secretary of State
Total number of respondents answering this question: 58
| Answer | Count | Proportion |
|---|---|---|
| Strongly disagree | c | c |
| Disagree | c | c |
| Neither agree nor disagree | 12 | 21% |
| Agree | 28 | 48% |
| Strongly agree | 9 | 16% |
Table 3: extent to which respondents agreed with the proposal that the Commissioner will receive remuneration
Total number of respondents answering this question: 53
| Answer | Count | Proportion |
|---|---|---|
| Strongly disagree | c | c |
| Disagree | c | c |
| Neither agree nor disagree | c | c |
| Agree | 21 | 40% |
| Strongly agree | 25 | 47% |
Table 4: extent to which respondents agreed with the proposal that the Secretary of State will fund the operation of the Commissioner
Total number of respondents answering this question: 55
| Answer | Count | Proportion |
|---|---|---|
| Strongly disagree | 5 | 9% |
| Disagree | 5 | 9% |
| Neither agree nor disagree | 7 | 13% |
| Agree | 26 | 47% |
| Strongly agree | 12 | 22% |
Table 5: extent to which respondents agreed with the proposal that the Commissioner should publish an annual business plan setting out their strategic priorities, having taken reasonable steps to consult relevant stakeholders beforehand
Total number of respondents answering this question: 58
| Answer | Count | Proportion |
|---|---|---|
| Strongly disagree | c | c |
| Disagree | c | c |
| Neither agree nor disagree | 5 | 9% |
| Agree | 22 | 38% |
| Strongly agree | 26 | 45% |
Table 6: extent to which respondents agreed with the proposal that the Commissioner should keep proper accounts and provide an annual financial statement to the Secretary of State
Total number of respondents answering this question: 55
| Answer | Count | Proportion |
|---|---|---|
| Strongly disagree | c | c |
| Disagree | c | c |
| Neither agree nor disagree | c | c |
| Agree | 18 | 33% |
| Strongly agree | 32 | 58% |
Table 7: extent to which respondents agreed with the proposal that the Commissioner must publish an annual report to explain the activities they have undertaken during the year in relation to their core duties
Total number of respondents answering this question: 57
| Answer | Count | Proportion |
|---|---|---|
| Strongly disagree | c | c |
| Disagree | c | c |
| Neither agree nor disagree | c | c |
| Agree | c | c |
| Strongly agree | 39 | 68% |
Table 8: extent to which respondents agreed with the proposal that the Commissioner may appoint an advisory board, whose members will have a broad range of relevant interests, experience and knowledge
Total number of respondents answering this question: 58
| Answer | Count | Proportion |
|---|---|---|
| Strongly disagree | c | c |
| Disagree | c | c |
| Neither agree nor disagree | c | c |
| Agree | 20 | 34% |
| Strongly agree | 33 | 57% |
Table 9: extent to which respondents agreed with the proposal that any staff of the Patient Safety Commissioner, so far as authorised by the Commissioner, may exercise any of the Commissioner’s functions
Total number of respondents answering this question: 55
| Answer | Count | Proportion |
|---|---|---|
| Strongly disagree | c | c |
| Disagree | c | c |
| Neither agree nor disagree | 6 | 11% |
| Agree | 33 | 60% |
| Strongly agree | 11 | 20% |