Consultation report on the future of UK seafarer medical examination (ENG1) fee 2022
Updated 11 November 2022

© Crown copyright 2022
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/consultations/consultation-on-the-future-of-the-uk-seafarer-medical-examination-eng1-fee-2022/consultation-report-on-the-future-of-uk-seafarer-medical-examination-eng1-fee-2022
Section 1. Introduction
This consultation on the future of the UK Seafarer medical examination (ENG1) fee 2022 ran from 19 May to 11 August 2022. It was intended to ask the public their opinion on whether to continue the status quo with a statutory set fee for the ENG1 or whether to remove the fee from the regulations and to allow the Maritime and Coastguard Agency (MCA) Approved Doctors (ADs) to set their own prices for the medical examinations they perform.
This was a full public consultation and all our external stakeholders including industry, unions, ship operators and ADs were notified and asked for their opinion. We are grateful for all the comments received and we acknowledge the time and effort put into the information provided to us.
Under current legislation, the ENG1 fee is limited by statute and the MCA controls the availability of ADs (for quality control purposes), which contracts the market for the provision of UK seafarer medicals. The fact that the fee is controlled by regulations has made the process of increasing the fee protracted. In recent decades this has resulted in the fee remaining unchanged for long periods, which does not allow ADs to recover their costs. The low ENG1 fee has led to problems in the recruitment and retention of ADs in some areas, with other practices reducing the availability of appointments.
Following on from a stakeholder engagement exercise conducted in February 2017, regulations came into force on 13 November 2018, and set the relevant fees as follows (depending on the date of examination):
- carried out on or after 13 November 2018 but before 13 November 2019 £95
- carried out on or after 13 November 2019 but before 13 November 2020 £105
- carried out on or after 13 November 2020 £115
The next uplift planned by the MCA for all fees is not until at least 2024, which means that the ENG1 fee will remain at the level last set in November 2020. This level is on average much lower than other industry medical prices and also much lower than doctors’ usual chargeable rates. This situation has led to seafarers benefitting over the years from lower prices for ENG1 medicals than for other comparable medicals whilst ADs are effectively being paid at an unviable rate for carrying out ENG1s meaning that they are subsidising their costs from other medical work.
1.1 Proposed changes
The aim of removing this fee from the Regulations is to ensure that there is greater flexibility to respond to changing economic circumstances affecting Approved Doctors’ (AD) costs, to ensure that ADs are properly remunerated, support the quality of the examination, help to ensure parity with other industries’ medical fees and futureproof the supply of these essential medical examinations. The MCA, in line with its commitment to attempting to minimise the impact of fee changes on industry stakeholders, has therefore consulted with stakeholders on whether the ENG1 fee could be removed from the Merchant Shipping (Fees) Regulations 2018/1104.
Section 2. Key findings
2.1 The consultation questions were:
For Question A please let us have your views on the two options presented:
Question A. Which option would you favour and why? (Option 1: Do nothing or Option 2: ENG1 fee to be set by market forces).
Question B. Are there other benefits and disbenefits which the MCA has not identified above?
Question C. Are there other models for charging that could be considered?
There were two options proposed for Question A listed below and the consultation included the benefits and disbenefits for each option:
Option 1: Do nothing - continue with set medical fee. As the fee has no more planned increases since November 2020 when it rose to £115, one option is to leave things as they are, with a statutory fee. However, the current fee continues to lag behind other comparable industry medical prices. If the issue of fee setting remains unsolved, AD recruitment and retention will continue to be affected. We have seen a recent example of an MCA AD resigning due to it not being financially viable to continue carrying out seafarer medicals at current pricing levels. In our last consultation running from 14 September 2016 to 26 October 2016, we received responses from 49 respondents who were concerned with the capping of the ENG1 fee.
Option 2: ENG1 fee to be set by market forces (preferred option).
Most occupational medical examination fees are not set by legislation, for example the Health and Safety Executive does not set fees for divers’ medical examinations, nor does the renewables industry. In other industries such as aviation and rail, the medical fees are not capped, so this policy will align Maritime with other UK transport sectors.
As the ENG1 fee is paid directly by the seafarer or their employer to the AD, it is an anomaly that the fee is set in statute. Removing the statutory fee would allow companies to negotiate contracts to supply medical services, including the statutory seafarer medical examinations, with ADs at mutually agreed rates, which could result in improved services for seafarers. In the larger ports as well as some remote areas, there is evidence that ADs consider their role as providing a community service and so would be unlikely to take advantage of an unregulated fee to increase their charges beyond “the going rate”.
Section 3. Summary of responses
3.1 The MCA findings are based on qualitative analysis, where survey responses were systematically categorised to allow themes and patterns to emerge. A ‘code’ was created each time a new theme emerged in response to a question. This process is called inductive coding.
- There were 84 consultation responses in total, 79 of which answered question A, which was whether to continue the status quo (Option 1) with a statutory set ENG1 fee or whether to remove the ENG1 fee from the regulations in order to allow the MCA Approved Doctors set their own prices for these medicals (option 2). Not all respondents for Question A gave an answer to the choice between Option 1 and Option 2.
- The headline figure is that of the 79 responses to question A, 47% (37 respondents) said they would prefer option 1 and 53% (42 respondents) would prefer option 2. This was closer in numbers than we predicted.
- As a percentage of the total replies to Question A, 72% were from medical professionals (Approved Doctors “ADs”, medical referees and former ADs) and 28% from Industry sectors (including seafarers, ship operators, Unions, the Chamber of Shipping).
3.2 Analysis of the consultation responses outlined a number of key points
The MCA could have expected that all Maritime Industry responses were in favour of Option 1, and that all ADs would be in favour of Option 2 however responses were more mixed:
Of the responses to Question A:
- of those choosing Option 1, 59% were medical professionals and 41% were from the Industry sector.
- of those choosing Option 2, 83% were medical professionals and 17% were from the Industry sector
There was a good range of opinions and types of people in each sector. From ADs, foreign ADs, former ADs and medical referees in the medical sector to seafarers, unions, ship operators in the industry sector.
3.3 Question A major themes emerging from the 37 responses supporting Option 1 continue with set medical fee
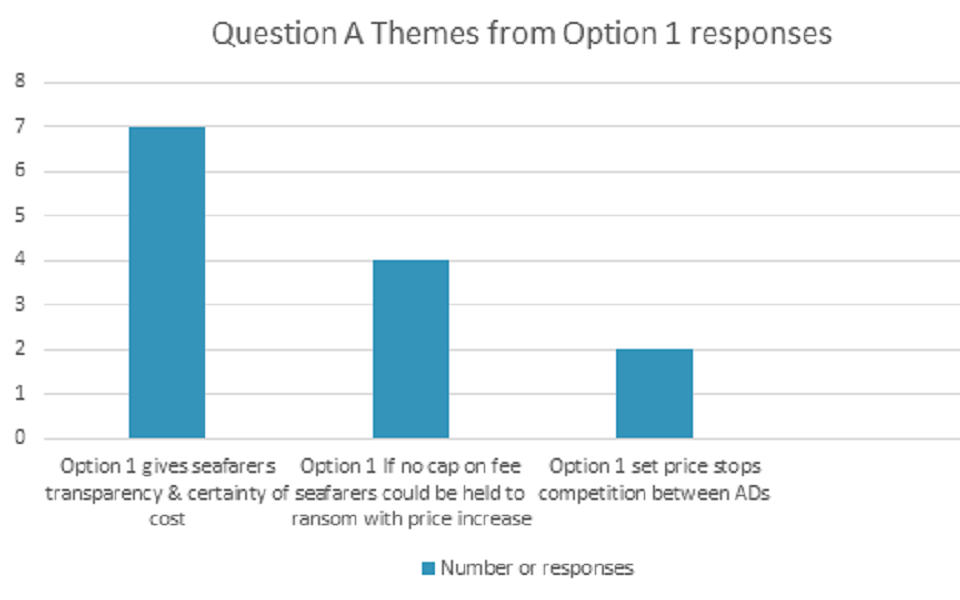
The primary justification for selecting Option 1 in response to Question A was transparency and certainty of cost for seafarers (N=7). Concern that seafarers could be “held to ransom” over fees, thereby being put in a position where they must pay whatever the cost in order to secure their mandatory certification, was the second most common theme that emerged from responses to question A (N=4).
3.4 Question A major themes emerging from the 42 responses supporting Option 2 take the medical fee out of Fees Regulations
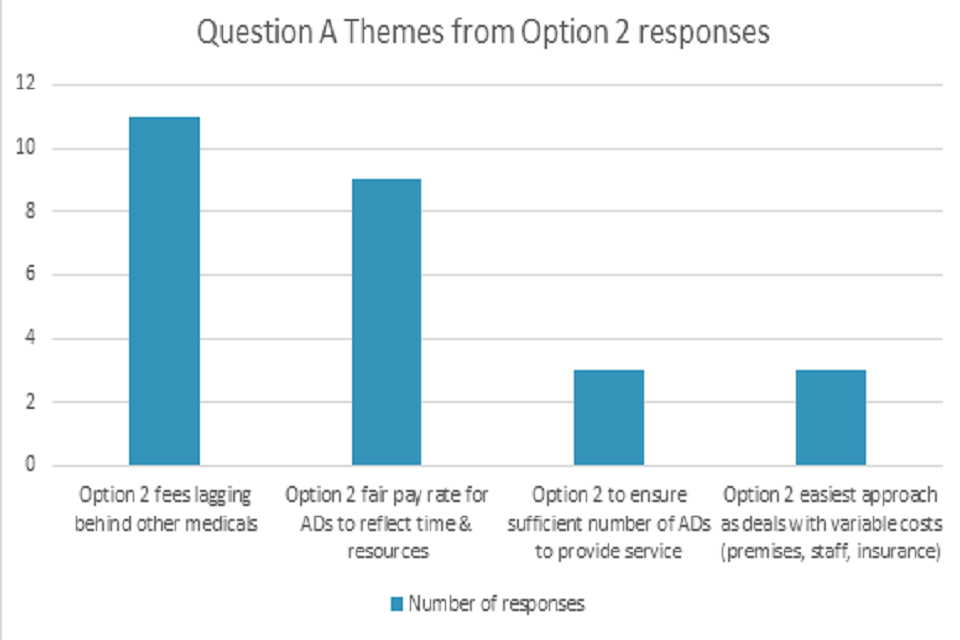
The primary justification for selecting Option 2 in response to Question A was that fees lagged behind other medicals (N=11), with the need for a fair pay rate for AD’s second (N=9).
3.5 Question A sample of Quotes reflecting different views from consultation responses
The below table gives an indication of how responses differ by industry.
(Where D is an AD or medical professional, S is a seafarer, U is a union, SO is a ship operator, I is Industry sector, numbers denote different respondent’s answers)
| Response sector | Option 1 quote (status quo) | Response sector | Option 2 quote (remove ENG1 fee from regulations) |
|---|---|---|---|
| D1 | I think the current fee of £115 is a fair cost. It reflects the time involved pretty well. Having a set price stops competition between ADs and gives all seafarers transparency about the service | D2 | I agree with Option 2. I had decided that before I read the “Preferred option”. It will pay the doctors the rate they should be charging without also setting rates over and above |
| D3 | I would be in favour of Option 1 do nothing as I think the current statutory fee system works well and allows everyone involved to be clear and transparent about the financial aspects of the medical process | D4 | I favour Option 2, for the reasons clearly explained in the consultation document. I have been offering medicals for commercial divers and offshore workers for many years, the content of which is very similar to the ENG1 seafarer assessment. The fees for these medicals are in the region of £150-£200, in my area (London) |
| S1 | It is already very expensive for seafarers to obtain an ENG1, and most have to pay out of their own pocket to have said Medical. If doctors are allowed to charge what they want without a cap, then seafarers will be held to ransom for the price they will have to pay in order to work at sea | I1 | From the two options presented Option 2 is preferred based on the need to ensure the number of ADs is sufficient to service the need. |
| S2 | The ENG1 fee should be set by statute as a fixed fee in consultation with accredited ADs. The proposal to allow market forces to set the fee for the ENG1 is absurd | S3 | Option 2 is what I would favour, I fully agree with argument and benefits that are laid out in consultation document |
| SO1 | Option 1 – whilst we can see this is established in other sectors, we feel that this may cause costs to spiral, especially in the current climate | SO2 | Whilst we appreciate the benefits that option 2 might create (especially the part about improving the retention and recruitment of ADs), we also have concerns. Our main concern is being able to manage our budget for ENG1s. |
| U1 | Whilst we believe that it is entirely reasonable to keep the level of the ENG1 fee under review to ensure that approved doctors’ expenses are covered, we do not support the proposed removal of the cap, which could result in significant variance in fees being charged for medicals. This variance would limit companies’ ability to budget for medical fees and also impose increased financial burden on those seafarers who pay for their own medical. | SO3 | I would say looking at the pros and cons that Option 2 would probably be suitable. I understand the reasons why this is being suggested. However, the worry I would have is that being no cap as such on fees, any doctor could charge whatever the liked and although you state that many doctors would stay in line with a reasonable cost, surely, we must be aware that some may view this as a money spinner |
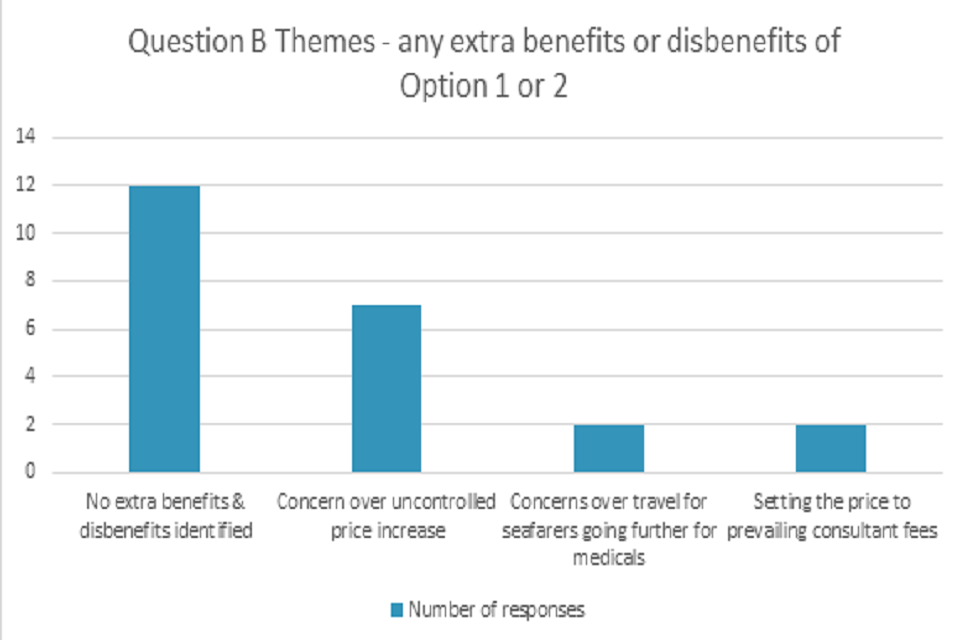
3.6 Question B Major themes emerging from the 30 responses
3.7 Question B sample of Quotes reflecting different views from consultation responses
(Where D is an AD or medical professional, S is a seafarer, U is a union, SO is a ship operator, I is Industry Sector, numbers denote different respondent’s answers)
| Response sector | Are there any other benefits or disbenefits that the MCA has not identified? |
|---|---|
| S1 | Removing the statutory fee will result in a limiting of choice for seafarers due to the unregulated cost |
| S2 | A fee clearly has to be paid but it is essential that seafarers and employers are not exploited by medical practitioners. |
| D1 | Set fee takes away uncertainty about what to charge and easier to explain to seafarer. Global economic uncertainty will be difficult for businesses, so this does provide some stability when other things are having increasing costs. |
| D2 | I believe the main benefits and disadvantages are laid out in the consultation document. In particular, costs associated with delivering these services vary considerably depending on geography (staff, premises, utilities, insurance). The profitability of undertaking ENG1s will therefore also vary considerably depending on local forces |
| I 1 | No extra benefits or disbenefits that I can see. |
| I2 | The largest disbenefit is the very real risk of the cost of the ENG1 increasing, which will disproportionately affect the Small Commercial Vessel sector. This sector sees most seafarers paying for their own medicals, and in many cases the individuals carry out their seafaring as a volunteer or part-time/occasional work. |
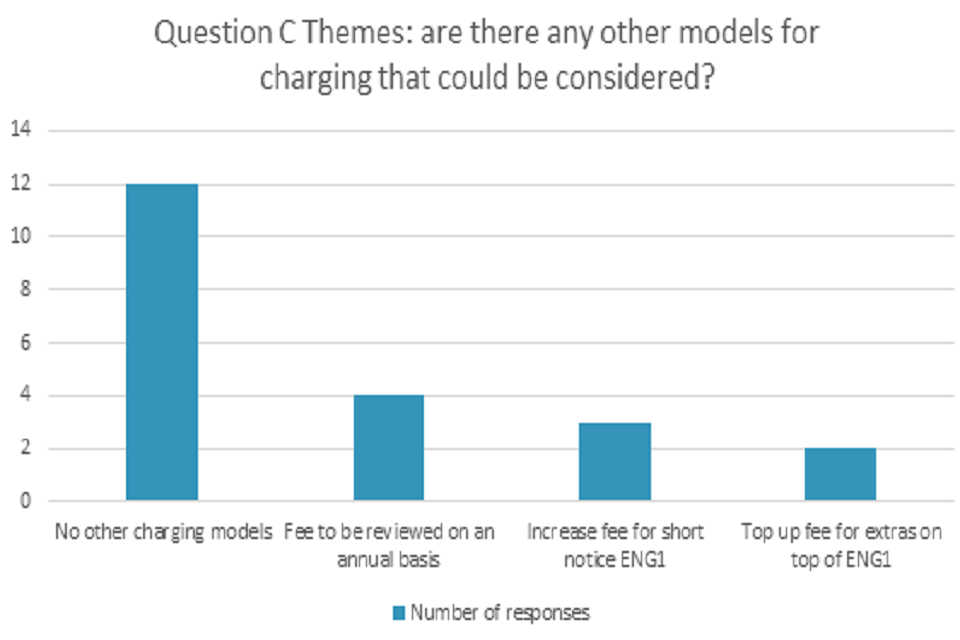
3.8 Question C major themes emerging from the 34 responses
3.9 Question C sample of Quotes reflecting different views from consultation responses
(Where D is an AD or medical professional, S is a seafarer, U is a union, SO is a ship operator, I is Industry Sector, numbers denote different respondent’s answers)
| Response sector | Are there other models for charging that could be considered? |
|---|---|
| SO1 | Setting a committee with a range of people from the medical profession. |
| SO2 | Establish a cost range. This gives some flexibility to the ADs and would remove the chance of areas with no competition setting unreasonable prices. |
| I1 | It would be preferrable to set a rate or band that covers the costs and is reviewed on an ongoing basis against the market rate either annually or biennially |
| I2 | Nil |
| D1 | Increase fee if short notice/urgent. Fees should be reviewed on annual basis with CPI increase |
| D2 | Setting a fee by time taken and hourly rate appropriate to training and seniority. |
| D3 | Not that I know of |
| S1 | The fee must be set by responsible legislation in consultation with responsible medical professionals. |
| S2 | If the seafarer is paying for the medical directly, look into option of spreading the cost over a number of months e.g., Buy now/pay later |
3.10 Extra Comments from Consultation (outside responses to Questions A.B and C)
(Where D is an AD or medical professional, S is a seafarer, U is a union, SO is a ship operator, I is Industry Sector, numbers denote different respondent’s answers)
| Response sector | Any other comments? |
|---|---|
| S1 | Possibility of combining the ENG1 with the Oil & Gas medical (OGUK) should be investigated. It is often a requirement for a seafarer to hold both medicals to work in offshore industry. It is additional cost obtaining 2 medicals often issued by same doctor for a similar kind of medical. Other option is for 2 industries to accept each other’s medical i.e., ENG1 should be accepted as the Offshore Oil and Gas Industry and vice versa. |
| D1 | The launch of the ADIS system has brought many advantages, but it does take time to become familiar with the process and even with familiarity some doctors may take longer to process an ENG1 with the online system. This could encourage some doctors to resign their appointment, whereas a flexible fee structure would enable paid time to be allocated as needed and relieve pressure around the financial viability of the process. |
| D2 | There is high demand for access to ENG1 appointments and I am unable to fully meet local demand in my area. I am aware that there are some seafarers who self-fund the examination fees, but this is not the case for the large majority, and the medical fee remains small in proportion to training fees and other expenses. |
| D3 | The point regarding large employers being able to contract with occupational health providers to deliver ENG medicals is an agreeable rate is quite correct. There will be scope for economies of scale for big employers with rate-setting by the market |
| D4 | The main problem is for seafarers is the lack of approved Drs in their area. I regularly see clients from London or Even Essex/Cambridge who travel to Hampshire to renew their ENG1. I think it would be reasonable to allow more approved Drs to be registered at a particular clinic or even to allow Approved Drs to consult in other locations. I know this is something the MCA has been against. Although the reasons for this are not clear to me |
Section 4. MCA response
4.1 Response to Question A, whether to keep with a set statutory fee for the ENG1 or whether to remove the fee from the 2018 Fees Regulations allowing for ADs to set their own fee
4.1.2 The majority of answers from those respondents who want to continue with a set fee justified this choice by arguing against option two which could result in possible price rises for ENG1s once ADs can set their own prices. However, this is not guaranteed, as the Impact Assessment has shown, there is a possibility for price increase or decrease as the market for such medicals would regulate itself and competition came into effect. One respondent agreed that there could be the possibility of companies who obtain medicals for their crew to arrange beneficial prices with an AD. The MCA accepts that this would not be the case for individuals seeking to arrange and pay for their own medical.
4.1.3 The MCA had explained in the consultation document why there is a need to change the way that the Seafarer medical fee is set. Many responses recognised the need for change (both from Industry and ADs) in terms of ensuring the resilience of the AD network. The historically low ENG1 fee has meant that the work for ADs has become more financially unviable, placing the AD network at risk. Indeed, vacancies for ADs exist around the coast and there are difficulties with recruitment. The MCA is concerned if the fee remains set in statute, then the fee will continue to increase slowly and will continue to lag behind other occupational health medical prices.
4.1.4 One response that came from a respondent about concern for price increases did make the MCA acknowledge that there could be other impacts for individuals if they have to travel further for a medical, in terms of environmental impact. The Impact Assessment will be updated accordingly.
4.1.5 One response asked about the implications for VAT charging if the ENG1 fee was no longer set in statute. The MCA verified with the BMA that there would seem to be no reason to charge VAT if this change came in to force.
4.1.6 Some Industry bodies expressed concern about potential price rises if the ENG1 fee were to be set by ADs and MCA has engaged with Industry over the past few years to explain why this proposed change is necessary. As the Impact Assessment states, prices may go up or down dependent on local market conditions.
4.2 Response to Question B, Are there other benefits and disbenefits which the MCA has not identified above?
4.2.1 Some respondents were concerned about the limiting of choice for seafarers if the cost for ENG1 medicals became unregulated, however there should be a choice as all ADs will display their prices and a seafarer, fishermen or ship operator will be able to research where they would like to go to obtain their medicals. Many ADs expressed their agreement with setting their own fees in terms of better reflecting their costs for the ENG1 medical.
4.2.2 Some respondents, mostly ship operators, but also some ADs felt that the set fee continues to provide transparency and stability for seafarers and fishers and the MCA acknowledges that this has been the case for some years. Shipping companies and seafarers have raised concerns about the economic impact at this time, so we are considering how to balance those concerns against the pressures faced by ADs offering the service at an uneconomic fee.
4.3 Response to Question C, Are there other models for charging that could be considered?
4.3.1 Some respondents preferred for the ENG1 fee to be linked to inflation rates or set with a minimum or maximum “cap”. This is not possible to do within MCA regulations as has been described in the Impact Assessment, we can either have a set fee or no set fee. Some respondents suggested a yearly set fee, but as explained in the consultation document, the MCA does not have the ability to change regulations yearly, this is not a possible timeline to meet. 33% of the responses to this question agreed that there were no other fee charging models to be considered.
4.4 Response to Comments in consultation response document
4.4.1 One response mentioned the possibility to combine ENG1 and offshore medicals. The offshore medical is an industry standard, whereas the ENG1 is a statutory medical meeting the standards of international Conventions, so this is not a viable option. Some respondents were encouraged by the potential for ADs to set their own fees as they were unable to meet local demand, and this should encourage AD recruitment and retention.
4.4.2 One AD responded that ADs should be able to consult in other locations where there are shortages, in the interests of fair and open competition, and for audit and administrative reasons, ADs are only approved to carry out medical examinations at the address to which they are appointed. However, approval may be given to carry out medicals at a subsidiary address of the same surgery if in close proximity to the main surgery. The appointment is not transferable to any other location or practice without the approval of the MCA.
4.4.3 Although some seafarers and unions expressed concerns at potential price rises of unregulated ENG1 prices for themselves or their members, one AD said that the majority of seafarers don’t pay for their own medical costs. As all fee charging is done by ADs, MCA has no evidence to provide to show how many seafarers or fishermen pay for their own ENG1 medicals.
Section 5. Who responded
The MCA would like to thank the following organisations and individuals for taking the time to comment on this consultation.
- MCA Approved Doctors
- Stena
- Blue Funnel Cruises
- Heathrow Medical
- Individual Seafarers
- Red Funnel
- Marine Scotland
- Chamber of Shipping
- Wightlink
- Zodiac Maritime Agency
- Western Ferries
- National Union of Rail, Maritime and Transport Workers (RMT)
- Maritime Craft Service (Clyde)
- Nautilus International
- RYA
- Hon Co Master Mariners
- Scottish Fishing Federation
- Seafish
- MAIB
- Evergreen Marine
- Ozra Shipping Agency
- British Medical Association
The table does not reflect the number of responses received.