Appendices: assessing fitness to drive
Appendix to the assessing fitness to drive guide for medical professionals.
Appendix A: The legal basis for the medical standards
The Secretary of State for Transport, acting through DVLA, has the responsibility of ensuring all licence holders are fit to drive.
The legal basis of fitness to drive in the UK lies in the following legislation:
- The Road Traffic Act 1988
- The Motor Vehicles (Driving Licences) Regulations 1999 (as amended)
According to Section 92 of the Road Traffic Act 1988:
- A relevant disability is any condition which is either prescribed in regulations or any other disability where driving is likely to be a source of danger to the public. A driver who is suffering from a relevant disability must not be licensed, but there are some prescribed disabilities where licensing is permitted provided certain conditions are met.
- Prospective disabilities are any medical conditions that, because of their progressive or intermittent nature, may develop into relevant disabilities in time. Examples are Parkinson’s disease and early dementia. A driver with a prospective disability may be granted a driving licence for up to 5 years, after which renewal requires further medical review.
Sections 92 and 94 of the Road Traffic Act 1988 also cover drivers with physical disabilities who require adaptations to their vehicles to ensure safe control. These adaptations must be coded and shown on the licence. See Appendix F, disabilities and vehicle adaptations and Appendix G, Mobility Centres and Driving Assessment Centres.
‘Serious neurological disorders’
The law requires that driving licences shall not be issued to, nor renewed for, applicants with serious neurological disorders, unless supported by the applicant’s doctor.
A serious neurological disorder is defined for the purposes of driver licensing as any condition of the central or peripheral nervous system that has led, or may lead, to functional deficiency (sensory, including special senses, motor, and/or cognitive deficiency), and that could affect ability to drive.
When DVLA evaluates the licensing of these applicants, it will consider the functional status and risk of progression. A short-term licence for renewal after medical review is generally issued whenever there is a risk of progression.
Further information relating to specific functional criteria is found in the following chapters:
- Chapter 1, neurological disorders
- Chapter 4, psychiatric disorders
- Chapter 6, visual disorders
- Chapter 8, miscellaneous conditions – excessive sleepiness
Appendix B: Epilepsy and seizure rules and further guidance
The legislation governing drivers who experience a seizure
The following 2 boxes extract the paragraphs from regulations 72 and 73 of the Motor Vehicle (Driving Licences) Regulations 1999 (as amended) that govern the way in which epilepsy is ‘prescribed’ as a ‘relevant’ disability for Group 1 or Group 2 drivers (also see Appendix A, the legal basis for the medical standards).
Group 1 car and motorcycle
Regulation 72
(2) Epilepsy is prescribed for the purposes of section 92(2) of the Traffic Act 1988 as a relevant disability in relation to an applicant for, or a holder of, a Group 1 licence who has had 2 or more epileptic seizures during the previous 5 year period.
(2A) Epilepsy is prescribed for the purposes of section 92(4)(b) of the Traffic Act 1988 in relation to an applicant for a Group 1 licence who satisfies the conditions set out in paragraph (2F) below and who has either:
(a) been free from any unprovoked seizure during the period of one year immediately preceding the date when the licence is granted
or
(b) during that one year period has suffered no unprovoked seizure other than a permitted seizure.
(2B) A permitted seizure for the purposes of paragraph (2A)(b) is:
(a) a seizure – which can include a medication-adjustment seizure – falling within only one of the permitted patterns of seizure, or
(b) a medication-adjustment seizure, where:
(i) that medication-adjustment seizure does not fall within a permitted pattern of seizure
(ii) previously effective medication has been reinstated for at least 6 months immediately preceding the date when the licence is granted
(iii) that seizure occurred more than 6 months before the date when the licence is granted, and
(iv) there have been no other unprovoked seizures since that seizure
or
(c) a seizure occurring before a medication-adjustment seizure permitted under sub-paragraph (b) where:
(i) that earlier seizure has, to that point, formed part of only one permitted pattern of seizure and had occurred prior to any medication-adjustment seizure not falling within the same permitted pattern
or
(ii) it is a medication-adjustment seizure, which was not followed by any other type of unprovoked seizure, except for another medication-adjustment seizure.
(2C) A permitted pattern of seizure for the purposes of paragraph (2B) is a pattern of seizures:
(a) occurring during sleep, where:
(i) there has been a seizure while asleep more than one year before the date when the licence is granted
(ii) there have been seizures only while asleep between the date of that seizure while asleep and the date the licence is granted
and
(iii) there has never been an unprovoked seizure while awake
or
(b) occurring during sleep, where:
(i) there has been a seizure while asleep more than 3 years before the date when the licence is granted
(ii) there have been seizures only while asleep between the date of that seizure while asleep and the date the licence is granted
and
(iii) there is also a history of unprovoked seizure while awake, the last of which occurred more than 3 years before the date when the licence is granted
or
(c) without influence on consciousness or the ability to act, where:
(i) such a seizure has occurred more than one year before the date when the licence is granted
(ii) there have only been such seizures between the date of that seizure and the date when the licence is granted
and
(iii) there has never been any other type of unprovoked seizure.
(2D) An isolated seizure is prescribed for the purposes of section 92(2) of the Traffic Act 1988 as a relevant disability in relation to an applicant for, or a holder of, a Group 1 licence.
(a) in a case where there is an underlying causative factor that may increase future risk, where such a seizure has occurred during the previous one year period
and
(b) in any other case, where such a seizure has occurred during the previous 6 month period.
(2E) An isolated seizure is prescribed for the purposes of section 92(4)(b) of the Traffic Act 1988 in relation to an applicant for a Group 1 licence, who:
(a)
(i) in a case where there is an underlying causative factor that may increase future risk, has had such a seizure more than one year immediately before the date when the licence is granted
and
(ii) in any other case, has had such a seizure more than 6 months immediately before the date when the licence is granted
(b) has had no other unprovoked seizure since that seizure
and
(c) satisfies the condition set out in paragraph (2F).
(2F) The conditions are that:
(a) so far as is predictable, the applicant complies with the directions regarding treatment for epilepsy or isolated seizure, including directions as to regular medical check-ups made as part of that treatment, which may from time to time be given by a registered medical practitioner or one of the clinical team working under the supervision of that registered medical practitioner
(b) if required to do so by the Secretary of State, the applicant has provided a signed declaration agreeing to observe the condition in sub-paragraph (a)
(c) if required by the Secretary of State, there has been an appropriate medical assessment by a registered medical practitioner
and
(d) the Secretary of State is satisfied that the driving of a vehicle by the applicant in accordance with the licence is not likely to be a source of danger to the public.
Group 2 bus and lorry
Regulation 73
(8) Epilepsy is prescribed for the purposes of section 92(2) of the Traffic Act as a relevant disability in relation to an applicant for, or a holder of, a Group 2 licence, where two or more epileptic seizures have occurred, or that person has been prescribed medication to treat epilepsy, during the previous ten year period.
(8A) Epilepsy is prescribed for the purposes of section 92(4)(b) of the Traffic Act 1988 in relation to an applicant for a group 2 licence who:
(a) in the case of a person whose last epileptic seizure was an isolated seizure satisfies the conditions in paragraph (8C) and (8D)
or
(b) in any other case, satisfies the conditions set out in paragraph (8D) and who, for a period of at least 10 years immediately preceding the date when the licence is granted has:
(i) been free from any epileptic seizure
and
(ii) has not been prescribed any medication to treat epilepsy.
(8B) An isolated seizure is prescribed for the purposes of section 92(2) of the Traffic Act 1988 as a relevant disability, in relation to an applicant for, or a holder of, a Group 2 licence, where during the previous 5 year period, such a seizure has occurred, or that person has been prescribed medication to treat epilepsy or a seizure.
(8C) An isolated seizure is prescribed for the purposes of section 92(4)(b) of the Traffic Act 1988 in relation to an applicant for a Group 2 licence who satisfies the conditions set out in paragraph (8D) and who, for a period of at least 5 years immediately preceding the date when the licence is granted:
(a) has been free from any unprovoked seizure
and
(b) has not been prescribed medication to treat epilepsy or a seizure.
(8D) The conditions are that:
(a) if required by the Secretary of State, there has been an appropriate medical assessment by a neurologist
and
(b) the Secretary of State is satisfied that the driving of a vehicle by the applicant, in accordance with the licence, is not likely to be a source of danger to the public.
Withdrawal of epilepsy medication
This guidance relates only to epilepsy treatment.
During the therapeutic procedure of epilepsy medication being withdrawn by a medical practitioner, the risk of further epileptic seizures should be noted from a medicolegal point of view.
If an epileptic seizure does occur, the patient will need to meet the medical standards before resuming driving and will need to be counselled accordingly.
It is clearly recognised that withdrawal of epilepsy medication is associated with a risk of seizure recurrence. A number of studies have shown this, including a randomised study of withdrawal in patients in remission conducted by the Medical Research Council’s study group on epilepsy drug withdrawal. This study showed a 40% increased risk of seizure associated with the first year of withdrawal compared with continued treatment.
The Secretary of State for Transport’s Honorary Medical Advisory Panel on Driving and Disorders of the Nervous System states that patients should be warned of the risk they run, both of losing their driving licence and of having a seizure that could result in a road traffic accident.
The Advisory Panel states that drivers should usually be advised not to drive from the start of the withdrawal period and for 6 months after treatment cessation – it considers that a person remains as much at risk of seizure during the withdrawal as during the following 6 months.
This advice may not be appropriate in every case, however. One specific example is withdrawal of anticonvulsant medication when there is a well-established history of seizures only while asleep.
In such cases, any restriction on driving is best determined by the physicians concerned, after considering the history. It is the patient’s legal duty to comply with medical advice on driving.
It is important to remember that the driver licensing rules remain relevant in cases of medication being omitted as opposed to withdrawn, such as on admission to hospital.
For changes of medication, for example due to side effect profiles, the following general advice is applicable.
- When changing from one medication to another and both would be reasonably expected to be equally efficacious, then no period of time off driving is recommended.
- When the new medication is felt to be less efficacious than the previous medication, the 6 months off driving period is recommended. This time period would start from the end of the change over period.
Provoked seizures
To be considered a provoked seizure, the seizure must be attributable solely to a recognisable provoking cause and that causative factor must be reliably avoidable. It should be clear that the seizure has been provoked by a stimulus which is unlikely to be repeated. Driving will usually need to cease for 6 months (group 1) (in the absence of previous unprovoked seizures or existing cerebral pathology) or up to 5 years (group 2) following a provoked seizure.
Doctors may wish to advise patients that the likely total period of time they will be required by DVLA not to drive will be extended if there is a previous history of unprovoked seizure or evidence of pre-existing cerebral pathology (e.g. longstanding cerebral lesion, epileptic activity on EEG or evidence of fixed neurological deficit), that increases the risk of further seizures.
The following seizures may be treated as provoked:
- true seizures associated with cardiovascular syncope (convulsive syncope is not considered to be a seizure and the relevant syncope standard must be met)
- seizure in the first week following a head injury
- seizure in the first week following a stroke, TIA or spontaneous acute subdural haematoma
- seizure during, or in the first week following, intracranial surgery
- seizure associated with severe electrolyte or biochemical disturbance (including hypoglycaemia) documented within 24 hours of specific biochemical or haematologic abnormalities
- seizure associated with drug or alcohol intoxication or withdrawal, or exposure to well-defined epileptogenic drugs
The following provoked seizures are excepted and do not require driving to cease, although the relevant medical standards for the underlying condition will have to be met:
- seizures occurring at the very moment of impact of a head injury
- eclamptic seizures
- seizures provoked by electroconvulsive therapy
Appendix C: Cardiovascular considerations
Group 2 bus and lorry entitlement only
Licence duration
A bus or lorry (Group 2) licence issued after cardiac assessment for established cardiovascular disease will usually be short-term, for a maximum licence duration of 3 years, and licence renewal will require satisfactory medical reports.
Exercise tolerance testing
The preferred functional test to assess fitness to drive is an exercise tolerance test.
The requirements for exercise evaluation to assess fitness for Group 2 licensing are:
- Discontinuation of anti-anginal medication (i.e., nitrates, beta blockers, calcium channel blockers, nicorandil, ivabradine, and ranolazine) prior to exercise tolerance testing is not required.
- The default test should be a treadmill exercise test with the Bruce protocol.
- Bicycle ergometry is a suitable alternative when the individual cannot use the treadmill.
- The customer should be able to safely complete 3 stages (9 minutes) of the standard Bruce protocol (or cycle for 10 minutes with 20 W per minute increments, to a total of 200 W) without signs of cardiovascular dysfunction, such as:
- angina pectoris
- syncope
- fall in systolic blood pressure of 20mmHg or more
- arrhythmia that requires intervention or premature termination of the exercise test
- There must be no electrocardiographic ST segment deviation that is interpreted by a cardiologist to be indicative of inducible myocardial ischaemia (usually defined as at least 2 mm horizontal or down-sloping ST-segment depression or 2mm ST-segment elevation), either during exercise or the recovery period.
- When exercise testing is undertaken as part of medical enquiries regarding aortic stenosis, hypertrophic cardiomyopathy or cardiac transplantation, pre-existing ST segment abnormality may confound interpretation of any exercise-induced ST-segment deviation. In such cases, the test is undertaken to assess the haemodynamic response to exercise and as a marker of exercise capacity.
- Should atrial fibrillation develop de novo during exercise testing, the supervising clinician should determine whether it is appropriate to complete the test. If the test is completed and the DVLA exercise tolerance test criteria above are met, licensing will be subject to echocardiographic confirmation that left ventricular ejection fraction is at least 40% and the licensing requirements for individuals with pre-existing atrial fibrillation (see Arrhythmias section in ‘Assessing fitness to drive: guide for medical professionals’).
- If there is established coronary heart disease, DVLA will require exercise or other functional evaluation at regular intervals not to exceed 3 years.
Stress myocardial perfusion scan or stress echocardiography
A functional imaging test (radionuclide stress myocardial perfusion imaging, stress echocardiography, or stress cardiac MRI) can be considered as an alternative to exercise testing for customers with:
- left bundle branch block (LBBB)
- right bundle branch block with QRS exceeding 120 ms
- paced rhythm
- musculoskeletal or other disability that prevents exercise on a treadmill or cycle ergometer
If the exercise standard cannot be met because of lack of fitness or other non-cardiac reasons, a report may be requested from the supervising clinician before a functional imaging test is commissioned.
The licensing standards for functional imaging tests are:
- no more than 10% of the left ventricular myocardium is affected by reversible ischaemic change on myocardial perfusion imaging
or
- no more than one segment is affected by reversible ischaemic change on stress echocardiography
Left ventricular ejection fraction
Group 2 licencing requires a resting left ventricular ejection fraction of at least 40%. The preferred methods for assessment of left ventricular function are echocardiography or cardiac magnetic resonance imaging.
Full DVLA protocol requirements for these tests are available on request (see contact details).
Coronary angiography
For licensing purposes in individuals with coronary artery disease, DVLA considers non-invasive functional assessment to be more important than angiographic assessment of coronary artery disease severity.
For this reason, coronary angiography is not commissioned by DVLA. Exercise tolerance testing and, where necessary, myocardial perfusion imaging or stress echocardiography are the investigations of relevance (outlined above) with the standards as indicated to be applied.
If there is a conflict between the results of a non-invasive functional test and recent (within 6 months) coronary angiography, the case will be considered individually. This assessment will take account of angiographic evidence of obstructive and non-obstructive coronary artery disease, and any evidence of functional coronary artery abnormality.
Marfan syndrome: aortic root surgery
Group 2 licencing after aortic surgery for Marfan syndrome will require individual assessment.
A bus or lorry licence for annual review may be issued after elective aortic root replacement surgery provided:
- surgery is successful without complications
- there is satisfactory regular specialist follow-up
- there is no evidence of suture-line aneurysm postoperatively and on 2-yearly MRI or CT surveillance
Group 2 licensing following elective external aortic support procedures will require individual consideration. Continued licensing thereafter will require regular clinical review, including MRI imaging one year after surgery and every 3 years thereafter.
Aortic stenosis (to include sub-aortic and supravalvular stenosis)
Aortic stenosis severity should be assessed from clinical, echocardiographic and biomarker parameters, in line with recommendations in 2021 ESC/EACTS guidelines for the management of valvular heart disease.
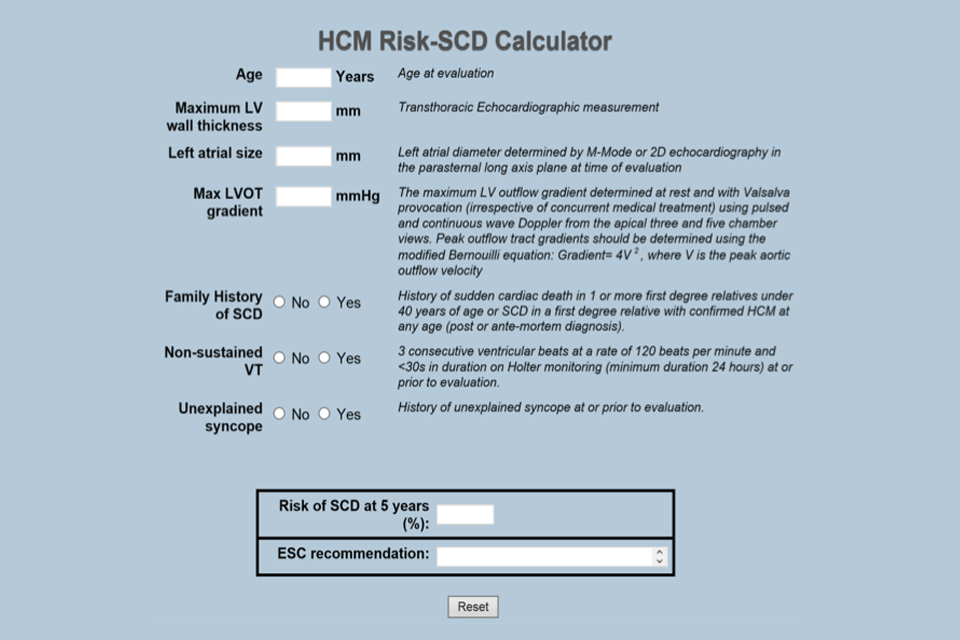
ESC Hypertrophic Cardiomyopathy Risk-SCD Calculator
This calculator is recommended by the European Society of Cardiology to assess sudden cardiac death (SCD) risk in individuals with hypertrophic cardiomyopathy. The calculator assigns individuals with hypertrophic cardiomyopathy to low risk (5-year risk of SCD less than 4%), intermediate risk (5-year risk of SCD 4 to 6%), or high risk (5-year risk of SCD equal to or greater than 6%) categories.
An online version of the calculator is available.
Congenital heart disease
Complexity of congenital heart disease can be classified as mild, moderate or severe. Refer to table 4 in the 2020 European Society of Cardiology guidelines for the management of adult congenital heart disease.
Appendix D: INF188/2 leaflet
Information for drivers with diabetes, including the INF294 leaflet.
Appendix E: Important notes concerning psychiatric disorders
All mental health symptoms must be considered
Any psychiatric condition that does not fit neatly into the classifications in Chapter 4 will need to be reported to DVLA if it is causing or is considered likely to cause symptoms that would affect driving.
Such symptoms include, for example:
- any impairment of consciousness or awareness
- any increased liability to distraction
- or any other symptoms affecting the safe operation of the vehicle
The patient should be advised to declare both the condition and the symptoms of concern.
It is the relationship of symptoms to driving that is of importance.
The law sets out the minimum medical standards of fitness to drive and the requirements for mental health in broad terms state that:
- there is a clear distinction between the standards for Group 1 car and motorcycle, and Group 2 bus and lorry licensing. The standards for the latter are more stringent because of the size of the vehicles and the greater amounts of time spent at the wheel by occupational drivers
- severe mental disorder is a prescribed disability for the purposes of section 92 of the Road Traffic Act 1988. Regulations define “severe mental disorder” as including mental illness, arrested or incomplete development of the mind, psychopathic disorder, and severe impairment of intelligence or social functioning
- the standards of fitness to drive must reflect, not only the need for an improvement in the mental state, but also a period of stability, such that the risk of relapse can be assessed should the patient fail to recognise any deterioration
- misuse of or dependence on alcohol or drugs are cases that require consideration of the standards in Chapter 5 in addition to those for psychiatric disorders in Chapter 4
Medications
Section 4 of the Road Traffic Act 1988 does not differentiate between illicit and prescribed drugs.
Any person driving or attempting to drive on a public highway or other public place while unfit due to any drug is liable for prosecution.
- All drugs with an action on the central nervous system can impair alertness, concentration and driving performance.
- This is of particular relevance at the initiation of treatment, or soon after, and also when dosage is being increased. Anyone who is adversely affected must not drive.
- It should be taken into account when planning the treatment of a patient who is a professional driver that the older tricyclic antidepressants can have pronounced anticholinergic and antihistaminic effects, which may impair driving, whereas the more recently developed antidepressants may have fewer such effects.
- Antipsychotic drugs, including depot preparations, can cause motor or extrapyramidal effects as well as sedation or poor concentration. These effects, either alone or in combination, may be sufficient to impair driving, and careful clinical assessment is required.
- The epileptogenic potential of psychotropic medication should be given particular consideration in patients who are professional drivers.
- Benzodiazepines are the psychotropic medications most likely to impair driving performance – the long-acting compounds in particular – and alcohol will potentiate effects.
- Doctors have a duty of care to advise their patients of the potential dangers of adverse effects from medications and their interactions with other substances, especially alcohol.
Electroconvulsive therapy
The likely severity of the underlying condition requiring electroconvulsive therapy (ECT) means the driver should be advised that they must notify DVLA.
Electroconvulsive therapy is usually employed in the context of an acute intervention for a severe depressive illness or, less commonly, as longer-term maintenance therapy.
In both courses, it is the severity of the underlying mental health condition that is of prime importance to the determination of whether driving may be permitted.
A seizure induced by ECT is regarded as provoked for the purposes of fitness to drive and is not a bar to licensing and driving – under both Group 1 car and motorcycle, and Group 2 bus and lorry.
The concerns for driving are:
- severity of the underlying illness requiring ECT treatment
- potential cognitive or memory disturbances associated with both the underlying depression and the ECT therapy
Driving must stop during an acute course of treatment with ECT and is not permitted until the relevant medical standards and observation periods associated with underlying conditions have been met, as set out in Chapter 4 and with respect to any other mental health symptoms or psychiatric conditions that do not fit neatly into classifications.
Again, this guidance must stress that the underlying condition and response to treatment are what determine licensing and driving.
Where ECT is used as maintenance treatment with a single treatment sometimes given weeks apart there may be minimal or no symptoms. This would not affect driving or licensing providing there is no relapse of the underlying condition.
Driving must stop for 48 hours following the administration of an anaesthetic agent.
Appendix F: Disabilities and vehicle adaptations
Group 1 car and motorcycle
Driving often remains possible with certain adjustments for a disability, whether for a static and progressive disorder or a relapsing one. These vehicle modifications may be needed for:
- permanent limb and spinal disabilities – for example, amputation, hemiplegia, cerebral palsy, ankylosing spondylitis, or severe arthritis (especially with pain)
- chronic neurological disorders – for example, multiple sclerosis, Parkinson’s disease, motor neurone disease, or peripheral neuropathy
Vehicle adaptations range from simple automatic transmission for many disorders, to sophisticated modifications such as joysticks and infrared controls for people with severe disabilities.
DVLA will need to know about a disability and whether any controls require modification, and will ask the patient to complete a simple questionnaire.
The driving licence is coded to reflect any vehicle modifications.
Assessment centres offer people advice about driving with a disability (these are listed in Appendix G).
Note that a person in receipt of the mobility component of Personal Independence Payment (PIP) can hold a driving licence from 16 years of age. (A person can’t apply for PIP until their 16th birthday.)
Group 2 bus and lorry
Some disabilities, if mild and non-progressive, may be compatible with driving large vehicles. DVLA needs to be notified and will require an individual assessment.
Mobility scooters and powered wheelchairs
Users of Class 2 or 3 mobility vehicles – which are limited to 4 mph or 8 mph respectively – are not required to hold a driving licence, and they do not need to meet the medical standards for driving motor vehicles. DVLA recommends the following, however:
- individuals with a medical condition that may affect their ability to drive these mobility vehicles should consult their GP first
- users should be able to read a car number plate from a distance of 12.3 metres
For more information, see Mobility scooters and powered wheelchairs: the rules.
Appendix G: Mobility Centres and Driving Assessment Centres
Find a centre on the Driving Mobility website.
Last updated 15 January 2024 + show all updates
-
Minor grammar changes to Appendix A. Clarification of the provoked seizure paragraphs in Appendix B. Significant changes to Appendix C for cardiovascular considerations, including exercise tolerance testing, stress myocardial perfusion scanning, coronary angiography, marfan syndrome, aortic stenosis and congenital heart disease. To note there have been no changes to the standards, the wording and testing requirements have been clarified.
-
Hypertrophic cardiomyopathy – interpretation of ECG changes during exercise testing (Appendix C). Congenital heart disease – referencing of classification of complexity of congenital heart disease (Appendix C).
-
Changes to the style of the text.
-
Clarification regarding provoked seizures, including confirmation that eclamptic seizures do not require time from driving.
-
Appendix G: list of mobility centres and driving assessment centres replaced with new search tool on the Driving Mobility website.
-
Panel updates.
-
Panel updates.
-
Appendix B - Rewritten section on provoked seizures. Appendix C - Inclusion of the European Society of Cardiology Risk of Sudden Cardiac Death calculator.
-
First published.