Harnessing technology for the long-term sustainability of the UK’s healthcare system: report
Published 23 August 2021

© Crown copyright 2021
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/harnessing-technology-for-the-long-term-sustainability-of-the-uks-healthcare-system/harnessing-technology-for-the-long-term-sustainability-of-the-uks-healthcare-system-report
Background and context
The challenge
Changing environments and lifestyles, an ageing population and an increased need for managing chronic and multiple long-term conditions in the UK will challenge our health system and increase healthcare costs.[footnote 1][footnote 2] Often those people most in need of healthcare (such as older, rural and socially deprived populations) have the most difficulty accessing service delivery centres. In some cases, there is also a variation in quality and quantity of healthcare provision. Such healthcare inequalities are driving disparities in health outcomes within and between regions.
There are challenges within the system itself. Structural silos exist at several levels; within the medical field there is a division into specialisms, within the National Health Service (NHS) there is an administrative and financial division into trusts, worsened by a lack of interoperability, and across the wider system there is a separation of health from social care and public health services. These structures reduce the ease with which information from one part of the system can be shared with other parts, can complicate a patient’s journey through the system, and may waste time and resources. Taken together, these barriers to flow of information affect the quality and integration of care.[footnote 3] Furthermore, the composition and distribution of the healthcare workforce is changing, with difficulties such as staff shortages[footnote 4] serving to compound the strain on service delivery.
The COVID-19 pandemic has further exposed the limitations of the current system, highlighting health inequalities, the challenges to integrated health and social care and the shortcomings in our approach to public and population health. It has also led to further pressures on the system, with a backlog of treatment requirements that may take considerable time to clear.
As currently structured, spending on the NHS would need to increase to maintain long term sustainability of the service. Under the current system, a continued drive for health service efficiency and cost reductions could further reduce resilience to emerging crises and further increase inequalities. As the government’s white paper[footnote 5] on health and social care recognises, a change in approach is needed.
The opportunity
As part of this change in approach, application of a wide range of technologies presents the possibility to transform health systems and create a more person-centred service. Successful integration of existing healthcare technologies could enable health system leaders to radically reshape the model of health and care delivery. These innovations are also the key to rebalancing our healthcare system, to shift our focus from acute intervention to early-stage prevention and maintenance of good health. This is vital to relieve demands on frontline services, secure a sustainable future for our NHS and to empower people to take greater control over their health and access to health services. The Box below provides some examples.
Box 1: Example technology applications in health care[footnote 6]
Individual-centred information
There is a huge range of technology that can provide information about an individual’s current health status and potential future risk. Examples include digitally connected sensors (such as Technology Integrated Health Management[footnote 7] for dementia) allowing real-time remote monitoring of markers of health and disease, imaging, genetic testing. Advances in miniaturisation and design can allow individuals to use these in the home or community setting without direct medical supervision. For example, ‘Hospital at home’ provides intensive hospital-level care for acute conditions in a patient’s home, using technology to monitor conditions through multidisciplinary healthcare teams and reducing strain on hospital admissions. Access to these technologies means individuals and those caring for them can be more aware of their health information than ever before and provide new approaches to delivery of prevention, early diagnosis and care.
Insight to support health professionals
The increasing availability and breadth of information about patients increases the importance of tools to help individuals and health professionals make sense of this and support evidence and risk-based choices on what care to offer. UK strengths in cohort studies, the success of the 100,000-genome project and development of the UK Biobank allow greater understanding of risk factors across the population and help refine diagnostic accuracy. Advances in natural language processing (NLP) can help turn rough notes in electronic patient health records into machine readable data. Artificial intelligence (AI)-enabled digital radiology and pathology helps to reduce demands on radiology services.[footnote 8] Clinically trained machine learning systems ensure patients spend less time waiting to be treated and can help to flag ‘at risk’ individuals for health professional’s attention.
Planning services and interventions to improve health outcomes
Patient and practitioner access to data held in patient records not only improves a citizen’s engagement with and understanding of their health and healthcare, and help inform choices about screening and care, it also helps the health and care system to plan local services. Technologies to support organisational design and identify efficiencies are already being applied, such as computational modelling[footnote 9] to optimise care pathways and to plan staffing and infrastructure needs.
Trusted, interoperable technical infrastructures
As increasing amounts of information about a person is captured, technologies for security, privacy and interoperability become even more important to enable optimal use of health data, to build trust in the system and enable people to control access to their own data. Cloud systems can support secure data storage and access by multiple users. AI platforms can facilitate connection on data sets and interoperability. Differential privacy algorithms and blockchain approaches can enable controlled access to anonymised data.
Develop new treatments and insights on interventions
Developments in science and technology are helping to support development of new treatments, therapies and insights into care. The response to the COVID-19 outbreak illustrates this: from machine learning for rapid identification of potential new drugs to rapid sequencing of virus strains and development of vaccines.
Data can also be made available to researchers and innovators to enable them to find out more about diseases, their causes and risks. This will enable more informed decision-making for all, and better-enable researchers and innovators to develop new treatments or design new interventions for prevention and early diagnosis.
In the longer term, further benefits could be realised by accelerating the integration of curative therapies as permanent correction for health conditions. Thanks to ongoing investment in the R&D infrastructure, the UK has world-leading research in several areas (such as genomics,[footnote 10] gene therapy and gene editing,[footnote 11] regenerative medicine, and immune manipulation in cancer and autoimmunity) which offer potential for cures to disease. This could enable individuals to be economically and socially active for longer and have significant implications for future health services.
There have been multiple attempts to drive improvement and innovation in the health system previously and there are some good structures already in place to bring research into the NHS, including UK Research and Innovation (UKRI), National Institute of Health Research (NIHR) and the Academic Health Science Networks (AHSNs). Establishment of the Accelerated Access Collaborative (AAC), hosted by NHS England and NHS Improvement, has been a major step forward in building the partnerships to streamline health innovation across the NHS. The AAC was instrumental in helping to establish the ‘RAPID C-19’ initiative[footnote 12] as part of the UK COVID-19 response, enabling safe and timely patient access to effective treatments. From 2019 to 2020, AAC programmes have saved the NHS an estimated £50 million.[footnote 13] However, to bring about systemic change, we must build on these initiatives, take a whole-systems approach, and enable radical new approaches to address unwarranted variation, bolster uptake of proven cost-effective innovations and support better health outcomes for patients across the UK.
The uptake and adoption of digital technologies in the health system is perceived to be low and slow.[footnote 14] Barriers include emerging technologies not working with current systems and/or with one another and lack of staff capacity and skills to integrate technologies effectively. The lack of interoperability leads to datasets being fragmented, data being virtually inaccessible to other relevant professionals, and ultimately not being used for optimum benefit. The problems of access and interoperability of data were evident early in the Covid pandemic.
The absence of an adequate integrated digital service delivery and infrastructure presents challenges to creating a more collaborative and coordinated health system and wastes staff time. There are additional challenges to using digital technologies and data most effectively, many of which are being considered in plans for the NHSX Data Strategy for Health and Social Care[footnote 15] and the Goldacre Review.[footnote 16] These challenges include building a workforce able to design systems and interpret/use the data in a clinical setting (and in service planning) and establishing approaches to data stewardship, governance and use that engender public trust.
Why now?
The government’s white paper on health and social care gives more flexibility to local leaders to plan around the needs of their local population and to better integrate health and care services. Realising this vision of empowered local health system leadership will mean harnessing the power of data to inform planning, identifying where new approaches could be deployed to achieve the best outcomes for the population you serve, and shaping a health professional workforce that is enabled by technology.
There is a wide range of technologies available now which are ripe for adoption and the combination of biomedical and digital technologies has huge potential. The unprecedented adoption of remote consultation and online information sharing (such as the summary care record) that has occurred, necessitated by the COVID-19 pandemic, shows the potential for rapid and widespread adoption, system change and transformation of services through innovation.[footnote 17] We must ensure that the system has the capacity to adopt and use these technologies to their full potential. The COVID-19 pandemic also highlighted the capability of the NHS for flexibility and agility, as well as building the impetus for a shift in focus towards early detection, prevention, community care and health resilience.
Now is the time to build on this momentum and unleash the power of technology and systems thinking to support better outcomes for patients, the workforce and the nation. The recommendations below must be considered as one part of a suite of measures, needed both within the NHS and across the widest possible range of public bodies to promote healthy living and build a sustainable health system in the long term. Technology alone cannot overcome the inequalities that lead to disparities in health outcomes and increase demand for healthcare resources. Indeed, poor implementation of technological innovations can risk increasing inequality. An important measure of success will be a system that offers integrated support and improves health outcomes for all.
In constructing this report, we have reflected on what is already known to identify the biggest opportunities where technology uptake should be targeted (priorities for change) and propose actions to realise these opportunities. We have seen the innovation already underway within the healthcare system and have heard from academics, innovators, and those working within the system. We have also considered previous reports to identify key principles and direct our recommendations to areas most relevant to increasing the impact of technology on health outcomes. Additionally, as health and social care are devolved matters, we have focussed our report predominantly on England. However, some recommendations are likely to be relevant to devolved administrations and some issues highlighted (such as harmonising data collection across public healthcare settings or sharing expertise) would greatly benefit from a four nations approach.
This report presents recommendations aimed at creating system change to improve outcomes for patients and support healthcare professionals. The recommendations focus on:
-
This report presents recommendations aimed at creating system change to improve outcomes for patients and support healthcare professionals. The recommendations focus on:
- a) fostering an environment for positive change across the whole system, to support current innovation and encourage more
- b) using lessons learned from other sectors, where digital technology adoption has been a success, to understand how to better harness technology in the health system for the benefit of all citizens, to improve outcomes for patients, to support and enable staff, and to improve the long-term sustainability of the system
- c) encouraging healthcare leaders to transform the way they work by incorporating technology and the ways in which members of the public access and engage with the system in the future
- d) promoting the key principles for successful use of technology in healthcare. These include creating a clear evidence base, engaging with potential users during development and implementation, and building widespread capacity in using new technology
- e) targeting investment in the infrastructure and capabilities that will enable development of a more adaptable and resilient healthcare system, to make the most of available technologies and to future proof the health system for emerging challenges
Priorities for change
System-wide adoption of technology can enable transformative change that will benefit the health and wellbeing of our nation and promote economic growth. We have outlined two areas of opportunity for the UK below, looking across public sector systems for health, including public health and the NHS.
Priority 1: Supporting a step-change to improve and maintain population health, centred around new ways of engaging and supporting individuals and communities, enabled by data and evidence
We welcome the White Paper’s focus on preventative healthcare and addressing inequalities, including the recently announced Office for Health Promotion (OHP). A systems approach to improving population health should start with looking across how national and local government policies shape the places where we live and work (and the choices open to us) and encourage working together to support a ‘Health in All Policies’ approach.
Appropriate implementation of technology within the healthcare system could create widespread public health benefits. We suggest four areas where science and technology can play a role for health promotion.
-
Monitoring population health risk factors: As technology (such as mobile phones and associated apps) becomes increasingly ubiquitous, there is a huge opportunity to combine this with ‘smart’ equipment that can give feedback to the user and information to providers of medical care and other support. Technology can also help to identify populations at risk (for example, through tracking internet searching of symptoms, deriving risk algorithms from analysis of big data and health records, monitoring air quality and environmental indicators, genome screening). Whether self-reported through an app or tracked through various monitoring methods, this data can provide information to health system planners to help them better understand risk factors and what works to address the needs of different communities in their local population.
-
Enable informed choices: Technology can be a route for providing information and enabling choice as part of health promotion or to targeted groups as part of wider initiatives to prevent illness and reduce chronic disease. The UK has the chance to lead the world in health technologies. We have world-class tech companies and academic institutes and, the world’s largest health service organisation, the NHS. Tools are increasingly available for individuals to monitor their own health. We have new tools and online pathways for monitoring care of chronic diseases (such as diabetes and hypertension) and there are a range of digital technologies[footnote 19] from remote monitoring to the Couch To 5K app[footnote 20] which support healthy behaviours. Technology could play a role in giving individuals key information and feedback that could improve their knowledge and engage them in making informed decisions about their health.[footnote 21] In a future where more information will be available to individuals about their current health status and risks to future health, government may wish to encourage discussion about what expectations on citizens are appropriate to understand and manage their own health and improve access to services, what support needs to be available through education, community and healthcare services and the implications for standards and regulation.
-
Digital engagement for improving health literacy:[footnote 22]: Health literacy is recognised as a social determinant of health, with poor health literacy being linked to poor education, poverty, low socioeconomic status, and unemployment. Low health literacy can also be found in affluent communities, especially in the face of a new risk to health.[footnote 23] Technologies that help individuals and communities to access, understand, and act upon health information have the potential to improve health literacy across the board. Digital media gives new opportunities to improve access to health information and the capacity of individuals to use the information effectively[footnote 24]. This is already happening outside formal health systems. For example, social media can play a role in informing the cultural beliefs, attitudes and behaviours (social norms) around health such as vaccine hesitancy. There are also online platforms offering peer-to-peer support between people with similar health conditions. Use of digital technologies for public health interventions is still in its infancy with the evidence base still being built on how technology-based interventions are received by individuals and what impact this has on behaviour.[footnote 25][footnote 27]
-
Designing user-centred approaches to improve services: There may be an opportunity to harness digital tools for the health service to reach and engage with hard-to-reach or vulnerable groups in new ways, such as through new prevention and treatment modes (for example, remote monitoring of self-administered medication)[footnote 28]. Technology used in this way could provide more cost-effective and accessible means of therapy for hard-to-reach people. This offers more convenience and choice to patients who cannot, or may not want to, engage with health practitioners in-person. To be fully inclusive, healthcare professionals must also recognise when the use of technology is not appropriate for individuals.[footnote 29]
Digital tools for health should be accessible to all. There is a strong association between groups that are digitally excluded and those that are at greater risk of poor health. Without addressing the ‘digital divide’, such tools have the potential to exacerbate health inequalities. To successfully address health inequalities, support for those from disadvantaged groups to improve their digital literacy and/or confidence in using digital tools and equitable access to online services needs to be placed at the heart of the system. This must include coproduction with relevant communities to ensure any technology developed considers their social, cultural and linguistic needs.
Priority 2: Re-engineering the health system to support integrated ‘pathways’ for prevention, treatment and care and better outcomes for individuals
Digital consultation tools, diagnostics and advances in remote monitoring and increased use of hospital at home allow more treatment and care to be delivered in the community,[footnote 30][footnote 31] minimising the necessity for hospital attendances and can enable the development of large representative health data sets across the population. More cost-effective and convenient remote technologies for continuous monitoring, routine testing of individuals and more sophisticated decision support tools can speed up screening and triage. This can free up the time of healthcare professionals to work in multi-disciplinary teams and enable cross-team work to streamline the patient pathway from presentation with symptoms to implementing an appropriate intervention and resolution of symptoms. Use of digital tools can also free up clinicians’ time to ensure face-to-face consultation for most complex cases or those who are digitally excluded (who may also be the most disadvantaged or have more complex needs).
Related to this, technology offers the opportunity to make health checks more accessible. Technological solutions, such as remote access to specialist advice and cheaper mobile imaging equipment, could allow more routine monitoring of health indicators so that interventions can be used to prevent conditions developing or Manage[footnote 32] chronic conditions. These solutions also have the potential to make health services easily available to elderly and vulnerable individuals who are often in the greatest need but may struggle to access (due to geography, lack of transport or other logistical issues) traditional centres of healthcare delivery. Technology can help to combat this ‘place disadvantage’ by providing services which are more accessible to these groups (such as community screening, telemedicine and diagnostics). For example, advances in diagnostics have enabled mobile CT and MRI scanner units that can be placed in local pharmacies, community or health centres, which would reduce journeys to hospitals, reduce waiting lists, shorten healthcare pathways (by reducing the number of separate appointments) and make healthcare more easily accessible to a wider range of people.
Recommendations to government
-
To ensure that the opportunities outlined above are fully exploited, we highlight several key interfaces where improving the digital infrastructure and flow of data could have significant impact on enabling uptake of technologies. These include:
- a) the individual and their own data
- b) the individual and the primary care team
- c) primary care and secondary care
- d) remote monitoring and secondary care
- e) health and care system planners’ access to data
The key to successfully redesigning the system around the interfaces is proper integration of technologies in a consistent way across healthcare delivery services. We also recognise the importance of additional interfaces, such as the flow of information between health services and social care or between the public healthcare and private industries. Further integration between health and social care is likely to be an ingredient for success in any healthcare initiatives. However, these are beyond the scope of this report.
We welcome the government’s plan for an NHS Data Strategy and to legislate to ensure more effective data sharing across the health and care system. The long-term success of the Integrated Care System (ICS) approach will depend on enabling flow of information between these interfaces that will inform health system leaders to plan and deliver services but also improve outcomes for patients and address concerns about privacy. We suggest the following actions to first demonstrate what works in system redesign and build capability before scaling up to enact wider change in the future.
Recommendation 1: The government should set up at least two significant scale Demonstrators to test the system-wide application of healthcare technologies
The NHS Long Term Plan and the recent White Paper on health and social care both outline the government’s aim to get innovative technology to patients faster. The White Paper proposes changes to the system in the longer term to incentivise the use of technology to deliver improved outcomes and experiences for people and their families. This builds on the rapid adoption of remote communications approaches seen during the COVID-19 pandemic.
Proposal and rationale
To support this aim, we propose the establishment of at least two technology Demonstrators. The purpose would be to test ‘whole system’ introduction of a range of innovative health technologies at scale, across the full breadth of services. This will encompass the whole health system (including hospitals, GP surgeries et cetera) within a given region and trial system re-engineering, allowing for a range of solutions to be tested at once, quickly learn from failures and iteration to develop improvements before being applied to the whole UK health system. This would run for sufficient duration (5 to 10 years) to learn about ‘what works’, to test how the parts are assembled, and explore the challenges and opportunities relevant to adoption across the NHS. These would build on existing initiatives (such as the Long-Term Plan commitment to develop regional Test Bed clusters[footnote 33] and the support for AI-enabled technologies under the £140 million AI Health and Care Award) and be a vital step towards wholescale system change. Annex A provides an overview of some of the changes the Demonstrators could explore.
Demonstrators should focus on rapid deployment and real-world testing of established and emerging technologies to learn how to deploy them for maximum benefit, rather than research and development (R&D) for new concepts. Some of these technologies are already being applied in pockets across the UK health system which must be tested at scale. Demonstrators should be deliberately structured to enable translation and adoption of innovative approaches and technologies, to identify and address many barriers to innovation and technology uptake in one place. Integrating the technology across uses in single areas is likely to create more opportunities for synergies (and to spot unexpected consequences) than piecemeal introduction of individual technologies across the whole system.
Demonstrators should encompass as wide a part of the whole healthcare system as possible because each technology only delivers its impact in the context of the whole. Demonstrators should span public health as well as health service operations, including data collection to understand the spread of needs in that population to inform healthcare planning. Demonstrators should explore technologies that support flow of information and system redesign around the interfaces outlined in Annex B.
Many different technologies are being developed by various companies. While the MedTech funding mandate will support adoption of National Institute for Health and Care (NICE)-recommended devices and products, innovators face the challenge of gathering evidence to demonstrate which tools and care pathways lead to better outcomes. More real-world evidence is needed on how available technologies might be integrated into the system to maximises the benefits for the patient and the healthcare professions. The Demonstrators could provide a focal point for private sector innovators to work in partnership with local health system innovators to test new approaches enabled by technology and to gather know how and evidence of efficacy in a clinical setting.
Principles for successful Demonstrators
The following principles should be built into the Demonstrator programme. These are discussed in further detail in Annex C.
-
Clear objectives: Demonstrators should agree a clear set of outcomes from the beginning, linked to the needs of the local population, which can be used to determine success within a given timescale of the Demonstrators running. What excellent healthcare looks like should also be defined as well as how progress will be measured to build in data collection for evaluation from the start. A transparent approach to advertising proposed areas of focus could allow related development requests to be combined and also help potential partners propose collaborations on solutions.
-
Build a learning system with evaluation embedded from the start: This should be an iterative process, building in time for evaluation and scaling of specific technologies based on the achievement of clear objectives. Demonstrators should have an explicit focus on experimentation and comparison of solutions, aided by analysis of health outcomes data. Funding should allow for a sufficient risk appetite. Demonstrators should take a phased approach to allow for failure, evaluation, and iteration to capture learning.
-
Training: Demonstrators should allow specific workforce skills requirements to be identified at a manageable scale, allowing time to develop and test appropriate training. Demonstrators will provide opportunities for capacity building and skills development for leading innovation, working with a wide range of expertise from engineers and technology specialists to clinicians, patients or citizens using the technology. It will be important to ensure staff have time to develop skills and to invest in transformational change.
-
Governance and management: Demonstrators should be linked to an ICS and will need a strong and respected leader who is responsible for progress, with the authority to build collaborations with partners and lead changes to integrate technologies across the whole system. This single-point leader should be accountable, empowered and appropriately risk-taking.
-
Focus on building system resilience: This requires an iterative approach to systems design to architect solutions that ensure all elements are robust, adaptable or flexible, and that agile processes are put in place to deliver solutions that remain fit for purpose in the face of future shock or change.
-
Partnership with industry: Demonstrator leaders should involve healthcare and community stakeholders in shaping priorities and approaches. Demonstrators should involve industry from the outset and provide a clear point of contact to test their products in the ICS. Industry should be encouraged to view the Demonstrators as partners as opposed to customers/gatekeepers to the system. Demonstrators will need to draw on a variety of expertise medical, behavioural, data and computing, social scientists and ethicists to inform planning. They should also link closely to the local AHSN and other regional support networks that already exist to facilitate adoption of technology within the NHS and ensure that health professionals who will be users of the technologies are involved from an early stage.
-
Scale and duration: Demonstrators should be sufficiently ambitious in scale and duration, incorporating lessons learned from previous initiatives, including the NHS Test Beds Programme. The cluster model set out in the NHS Long-Term Plan and the work of the AI Health and Care Award provide useful models to build on. The Demonstrators should be designed to run for 5 to 10 years, to maximise their impact, learning and build in sufficient time for evaluation and iteration, and during this time will continuously generate learning for the wider NHS to assess and adopt. In effect they should be long-term ‘living labs’ to explore how to best harness the benefits of new technologies for the local population.
What this could deliver
If we get this right, we will be able to improve population health and wellbeing through a greater focus on prevention and efficient service delivery, but most importantly improve experience of individuals seeking diagnosis, treatment and care. The Demonstrators are not just an attempt to deliver a technologically enabled ‘hospital of the future’ but will improve how the overall system delivers outcomes for the future, with success resulting in a revolution in primary care, easy and early access to diagnostics, preventive services, leadership to manage an integrated system, more efficient workflows, arrested decline of degenerative conditions, improved indicators of overall population health (such as lower levels of obesity, smoking, diabetes or better sexual health) and reduced inequality of access, experience and outcomes.
There is a challenge around how we ensure older people and those who are socio-economically disadvantaged, who often have greatest demand for healthcare services, are not excluded from using digital services. In addition, the pandemic has highlighted different challenges for healthcare across the UK depending on demographic or hospital infrastructure. A system-wide Demonstrator could allow the individual needs of different communities in different places (and how they are changing) to be explored. The Demonstrator programme could encourage innovation on health challenges and specifically encourage consideration of the needs of ‘hard-to-reach’ groups in all projects, including whether and how they can reduce inequalities. Demonstrators should not necessarily be in areas that are already leading the way in delivering integrated care and adopting innovation. Instead, priority should be given to ICSs hosting the Demonstrators in areas with the greatest population health challenges, to work with local governments to support ambitions for ‘levelling up’ in certain areas of the country.
The first step for a Demonstrator would be to characterise the system or data to help understand issues and evaluate success, including:
a) understanding the experience of an individual navigating the health system and the care pathway they experience so you can measure the impact of changes on things that citizens care about. This would not just be costs and waiting times but also efficiency of ‘flow’ of individuals through the system, length of stay in hospital, time off work through ill health, and the ability of individuals to navigate the system and play an active role in decision-making and self-management of their health.
b) understanding the health challenges for the local population by gathering population health data covering all the major parameters. In addition to bringing together existing data sets and measuring morbidity/mortality outcomes, this could be an opportunity to work with patient and community groups to test new approaches to citizen engagement to define what is and is not working, such as apps to generate data, as has been seen with the use of the ZOE COVID Symptom Study.[footnote 34] In this way, citizens can direct the strategy and priorities of the Demonstrators by inputting health data and enable monitoring the impact of interventions put in place. This data can also be used to target interventions and learn more about which interventions and engagement works with different communities.
Essential infrastructure for the Demonstrators
Key to success will be establishing data standards for interoperability of NHS clinical information systems.
As reflected in the consultation around the Data Strategy for Health and Social Care, the way data is captured, stored, distributed, processed and shared will need to change.[footnote 35] Data quality should be treated with the same governance and scrutiny as care delivery. Key to success will be a re-examination of the legal and regulatory frameworks governing data, in conjunction with adoption of new and emerging technology. This needs to be delivered at a national level and should aim to enable and simplify.
A system-wide re-engineering of the healthcare system will require a new data infrastructure within ICSs, based upon a national approach for basic standards for interoperability and operational systems. The Demonstrators will be vital for testing a system update at scale, building a platform of technologies that bridges different parts of the system so patient health records are linked seamlessly. The contribution from Demonstrators could include the following.
-
Addressing needs: providing a focal point for investment in (and testing of) practical solutions (such as software) to reduce inefficiencies for routine jobs for healthcare professionals in recording, accessing and sharing information that supports patients. Demonstrators offer the opportunity to identify ‘gaps’ that technologies could fill and barriers to their deployment, to test practical solutions and understand different data requirements
-
Insight: designing a system that supports professionals to generate useful insights that inform future approaches, such as using data to quantify and improve ‘patient experience’ by measurement of processes end-to-end (from referral; to evaluation; admission; treatment; discharge; and out into the community) to understand performance across the system. Demonstrators can test new approaches in using data to quantify patient experience and inform policy
-
Data interoperability: at a national level, ICSs will need to be supported by standards for storing and sharing information that will form the foundations for future development and procurement guidelines that help ICSs ensure all technology suppliers understand and comply with the need for interoperability. Demonstrators could support development of standards by providing a forum for real work application and testing before national standards are confirmed. Interoperability with other providers of health and social care will also be an important consideration, building on the new Health and Social Care Network
Suggestions for where to focus
-
Successful implementation of new technologies is likely to require widescale support from users (whether staff or patients). To mitigate unexpected harms caused by inadequate implementation of new technologies, the government should establish a programme of public co-production of health support. Consultation and co-production should be at the heart of technology adoption to ensure that any digital tools developed meet the needs of their intended audience and are acceptable and accessible to them.
- a) New technologies and applications should be developed in collaboration with intended users and build expertise in bringing culture and social context to technology and systems design, delivery, and support. It is vital that adequate research and consultation is done to ensure that all digital tools proposed are user-friendly and accessible to all.
- b) The programme should allow innovators of technology to engage with the Demonstrators, to allow existing technologies to be tailored to the needs of groups experiencing health inequalities and to and learn about user needs, priorities, preferences, opportunity, and capabilities. It could also inform efforts to support health literacy and digital literacy. Not only would this benefit the health of our nation but also make the UK the easiest place in the world to co-create, test and implement personal health technologies.
- c) This programme should be representative of the UK population but with specific attention paid to hard-to-reach or vulnerable communities to ensure that the diversity of views are taken into account, there is adequate understanding of which interventions work for specific communities, and to target health promotion within these communities.
- d) While technology alone cannot overcome the inequalities that lead to disparity in health outcomes, data gathering and continuous evaluation can be used to identify gaps and groups where the campaign is not reaching. This will be vital to inform policy making within local authorities to support interventions to make a difference to these groups.
Distinction between this and below
-
The system-change will be more effective if techniques from behavioural and social science are used at every stage of the health technology design, implementation, and assessment processes through:
- a) making formal changes to regulations, research and development funding, and public and healthcare incentives
- b) ensuring individuals are supported in looking after their own health through health literacy initiatives that support them throughout their life course
- c) engaging with a wide range of stakeholders in the most effective ways to ensure that technologies are developed and implemented for the user in a manner that is widely accepted. For example, public consultation may be required for using certain datasets or introducing certain technologies, as there may be ethical and privacy concerns around some monitoring programmes or around the use of AI in decision-making
Box 2: Combining preventative and therapeutic approaches
Within the Demonstrator areas, we suggest the government could create a campaign focused on one chronic disease, to support individuals in better engaging with and managing their own health and health care by communicating information about how to best access and use services, as well as how lifestyle and other changes can modify their risk. This has potential to be managed by the Office for Health Promotion and could be trialled and evaluated in the Demonstrator areas. The goal would be to encourage and support the use of technologies to monitor progress in adopting and maintaining healthier lifestyles. This could improve treatment and care outcomes and should have clear milestones for success to allow evaluation of impact within the Demonstrators before scaling up to system-wide change. Importantly, the campaign should ensure these potential benefits reach across society by focusing on improving health literacy (especially in disadvantaged groups) through providing education and access to digital healthcare tools in community settings.
Type 2 diabetes[footnote 36] would make an excellent choice for this. It is a chronic disease which in some cases can be reversed by diet and exercise; it impacts Asian minorities approximately six times more than other groups; it is strongly correlated with obesity; it frequently leads to loss of sight, nerve damage and amputation; it is extremely costly to the NHS; and its prevalence is rising steadily in the UK and elsewhere. If public health and prevention services could be co-designed and delivered in a new way, supported by technology, to alleviate the burden of this disease, the UK could become a world leader in having developed a system based around health, not sickness. One of the best ways to improve diabetic management is careful follow-up to ensure a combined preventative and therapeutic approach, using ‘big data’ and electronic monitoring,[footnote 36] and so this could be an excellent example for the Demonstrators to showcase the impacts of technology on primary, secondary and tertiary prevention.
Recommendation 2: The government should establish a ‘National Centre for Health System Improvement’ to build capacity and skills for system transformation
This Centre must be multi-disciplinary and should engage people with a mixture of backgrounds and origins from inside and outside the medical profession and give them the skills and opportunities to lead transformation. Contributors should include, but not be limited to clinicians, data scientists, engineers, systems design specialists, clinical trialists, regulators, behavioural and social scientists, ethicists, and local community stakeholder representatives. Building on existing structures such as the Accelerated Access Collaborative (AAC), the centre should provide oversight of the Demonstrators and support innovation and integration of technologies within them. The centre should also focus on the overall potential ‘systems’ that can be captured, measured through clinical and economic evaluation and then improved within the NHS as a whole. It would serve two complementary purposes, explored below.
First, it should work closely with the Demonstrators to advise, design and evaluate system changes:
a) this could involve creating a repository of consistent measures of baseline performance and improvement across the whole healthcare system (ideally also incorporating a four nations approach). Demonstrators could liaise and share learnings with NHS England’s Sustainable Improvement Team to assist initiatives in being scaled up in the future
b) to support better targeting of improvements, modelling and decision support tools such as digital twins[footnote 38] could be established to capitalise on the data available and evaluate the effectiveness of innovative approaches to reshaping the healthcare system, including exploring ‘what if’ scenarios looking at potential impacts on various clinical, behavioural and social measures. The Centre could work with the Demonstrators to identify areas where there is a willingness to explore the use of digital twins, where there is clarity about current decision-making processes (the baseline), and there is the possibility of comparing current decision making (the control) with the use of a digital twin
c) regulation is an important enabler of innovation. Technological innovation such as digitally-enabled care pathways or diagnostic and clinical algorithms (for example, machine reading of mammograms) present new challenges for regulators. The Centre should work alongside regulatory bodies such as NICE, Medicines and Healthcare products Regulatory Agency (MHRA) and the Regulatory Horizons Council to bring together sandbox initiatives, capture learning and provide a focus point for evidence to inform regulatory change. The NHSX AI lab[footnote 39] provides a helpful model to build on
Second, the Centre should work to build capability and capacity for technology-driven improvements into the healthcare system. Whole-scale system change has implications for the healthcare workforce, including staff training in digital and remote care, pathways, use of data, clinical algorithms and generation/use of evidence of clinical validity for new pathways. A key barrier to widespread adoption and uptake of technologies is a lack of staff time to develop skills and invest in transformational change, and a lack of healthcare leaders and managers who have been able to develop expertise to manage this change. Within the areas for exploration for the Demonstrators set out above, we have set out principles to invest in skills, opportunities and networks for healthcare professionals and provide incentives for them to lead technology integration for service improvement. Many of these ideas are embodied in the recommendations of the Topol Review (2019)[footnote 40] and the government should strengthen its efforts to implement the measures outlined in this review in Demonstrator areas. We have identified the following ways that the Centre could support healthcare professionals to integrate technology into their work.
-
Training in use of new systems and technologies: training should be evidence-based, practical and engage the expertise of computer scientists, engineers, and remote diagnostics and technology industries in public health, behavioural, and social science research. Training should also be tailored to the needs of the individual. For example, support for health system leaders could include training on tools and techniques to visualise their areas of responsibility as well as analysing where interventions might be targeted to best effect.[footnote 41] Meanwhile, within the health practitioner workforce, training might focus on developing teams of adopters who have the skills to support testing and evaluation of new technologies and lead collaborations to refine and integrate technology-enabled approaches to drive innovation in their local health economy. Some existing roles in the NHS may change. For example, digitally enabled care pathways could mean that the General Practitioner (GP) plays a much more central role in the system in supporting individuals. A set of specifically tailored educational courses should also be designed to enable the practical benefits of Demonstrators to be achieved. These should be incorporated into clinical training and continuous professional development.
-
Training in systems thinking: although systems thinking is covered in some NHS management training, we suggest this is built into NHS training for all clinical and research leaders. For example, the NIHR Academy’s national programme for clinical research training[footnote 42] and the Health Education England[footnote 43] online learning resources could incorporate units on systems training which would mean training many future clinical leaders across all disciplines. The proposed new National Centre for Health System improvement could help develop suitable training modules relevant to different professional groups. Widespread understanding of systems thinking would enable staff at all levels to contribute to improving processes and the use of technology within healthcare.
-
Supporting existing systems engineering courses: there is a lack of Systems Engineers with experience of healthcare. The Centre could therefore play an important role in building capability within the system by supporting existing systems engineering courses, providing specialist healthcare systems training, and equipping health professionals and health system leaders or managers with the skills to manage change and deliver resilient improvement. The Centre should also award professional qualifications in these areas to allow recognition of these skills across disciplines.
-
Supporting initiatives for protected learning time: in line with the argument made in the recent Academy of Medical Sciences report on integrating the NHS and academia[footnote 44], there is a case for investing in schemes and initiatives which allow healthcare professionals to take time from their ‘day job’ without external workload pressures to upskill in these areas. This would not only lead to greater job satisfaction and staff retention but also bring better outcomes for patients, as the upskilled workforce will be drive system change and ensure this is implemented properly. Some of this work is already being undertaken by the Royal College of Physicians in Wales[footnote 45] and the Health Foundation.[footnote 46] Their continued involvement in this process alongside others is critical.
There is a breadth of insight and skills required to inform transformation in the NHS. The systems thinking and technological insights required will need to draw on expertise to be found outside the NHS, including from the medical technology sector, and the latest thinking in systems and technology leadership, in addition to health and care practice. Government should consider establishing the National Centre as an independent body that can tap into this broader expertise and offer advice and disruptive thinking on opportunities for transformation and the processes required to deliver them. Having a clear, strong, and experienced leader will be critical to the success of the Centre, with appropriate advisory and governance structures to maintain links with the Department of Health and Social Care and NHS leadership to focus their strategic agenda and maximise inter-disciplinary capability, while retaining this independence of operation.
Recommendation 3: The government should work with NICE, regulators and the research community to promote the development of an evidence base to underpin effective use of digital health technologies as part of care pathways
A wide range of digital tools (particularly health apps) are currently available and new products come onto the market regularly. However, there is a need to improve innovation metrics on how well-received these tech-enabled approaches are by users and healthcare professionals, how the tech is used by these individuals and whether it leads to better outcomes.[footnote 47][footnote 48][footnote 49] There is a need to build this evidence base, regulate technologies used by public bodies[footnote 50] and ensure individuals and health and care professionals understand how such technologies can be used most effectively. This has been effectively implemented for medicines, and now that the potential for the positive impact of technology is understood, the same should be done for technology.
To inform strategy for the development of promising areas of technology and experimental medicine, we need a clear understanding of the benefits they offer and how they can fit into future healthcare. A key factor in successfully integrating innovations is ensuring that appropriate resource is invested to support validation and demonstration in the clinical environment to understand the implications for widespread uptake. The government should ensure robust initial clinical evaluation and rigorous user testing supports implementation of every health technology that is adopted into the system (including apps and technologies for individuals to remotely monitor their own health). The evidence collected should be made available to healthcare professionals and the public. Evaluation and user testing could be linked into current infrastructures under the NHS Accelerated Access Collaborative, to ensure a consistent approach being adopted across the system.
To complement this, the government, working in collaboration with research and professional bodies, should develop common standards around what evidence is needed before the rollout of a technology into the health system to ensure the right tools are implemented, expanding upon the ‘Digital Technology Assessment Criteria for Health and Social Care’,[footnote 51] developed by NHSX alongside NICE. This would have the added benefit of making the UK an attractive place for small to medium-sized enterprises to implement their products, as well as large corporates. Regulation (for example, by MHRA) should build on what is set out in the Medicines and Medical Devices Act 2021, which aims to ensure the UK leads the way in developing pioneering health technology. The Demonstrators should also work with NICE to enable some exemption from the standard (and sometimes lengthy) processes of NICE approval. The goal would be to enable the Demonstrators to trial novel technologies, while still ensuring patient safety.
Annex A – Visualisation of the Demonstrator
{kind=link}
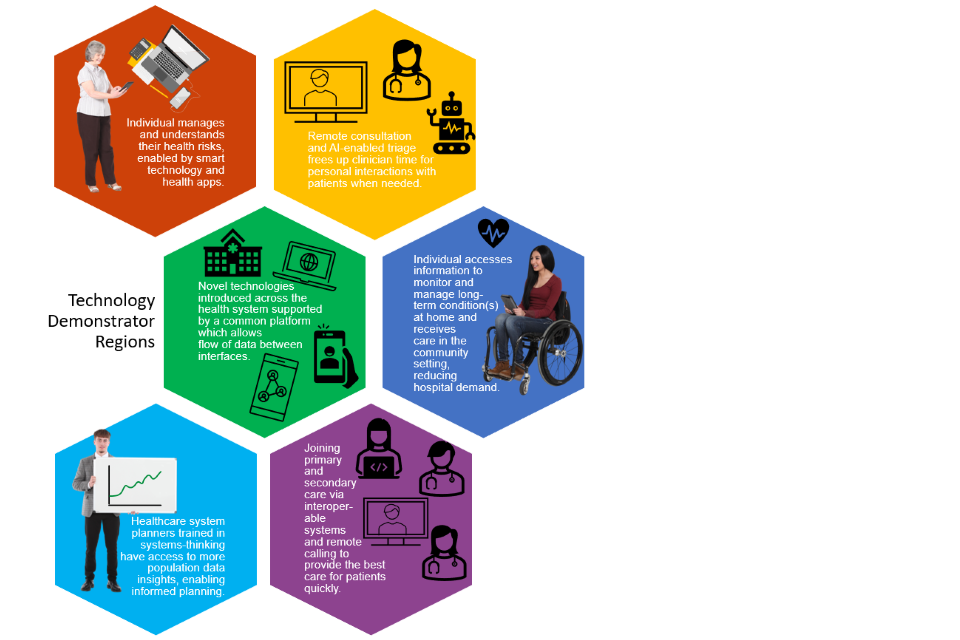
Technology Demonstrator Regions:
- individual manages and understands their health risks, enabled by smart technology and health apps.
- remote consultation and AI-enabled triage frees up clinician time for personal interactions with patients when needed
- novel technologies introduced across the health system supported by a common platform which allows flow of data between interfaces
- individual accesses information to monitor and manage long-term condition(s) at home and receives care in the community setting, reducing hospital demand
- healthcare system planners trained in systems-thinking have access to more population data insights, enabling informed planning
Annex B – Interfaces
Interfaces 1: The individual and their own data
Those with modifiable conditions, such as high blood pressure or obesity, are at higher risk of developing diseases like diabetes and cardiovascular disease. The lack of early identification and treatment of these and other preventable causes of death and morbidity result in a significant demand on health service resources.
Accessible digital platforms could enable individuals to access, understand and own or control their data (electronic health record or integrated care record), and help them understand and, where possible, modify their risk. For example, women with gestational diabetes test their blood glucose more regularly when asked to log and monitor readings in an app.[footnote 52] Evidence suggests that wearable technology (such as smartwatches) may also change behaviour, including through increased physical activity and better monitoring of heart health indicators.[footnote 53] Digital tools may also support individuals and healthcare professionals in making informed choices about treatment or non-pharmaceutical interventions that could improve their health, and their health literacy. Standards for interoperability could allow this information to flow through the health system, following a patient through their care pathway.
Individuals could also have greater control over their data including oversight of who is accessing their data, when, and for what purpose, and the ability to withdraw permission for some purposes.[footnote 54] For example, instead of giving repeated permission to different parts of healthcare organisations to access and share their file, individuals could have the process and organisational roles explained from the outset and choose to give blanket permission or to carry on giving unique permission for access to each part of the system as desired.[footnote 55] The ability to provide blanket permission and to see who has been accessing their data and when would decrease bottle-necks when permission must be requested and granted, and help to identify which parts of the system still need to engage.
Interface 2: The individual and the primary care team
The first step to accessing healthcare is often through a slow (and sometimes frustrating) primary care triage process. There are large demands on GPs’ time, since they act as the main point of entry for an individual into the current system.
Access to primary care services could be increased through online consultation, or via chatbots. This could be complemented with an AI triage system to recommend follow-up where needed through a multi-disciplinary primary care team, helping to make better use of the skills of practice nurses, physical therapists, and community pharmacists. By decreasing the number of services requiring initial GP involvement, their role would convert from that of a ‘gatekeeper’ to that of a care-coordinator: with more time to manage complex cases, guide individuals through care pathways, and provide support for more complex cases as well as self-management of conditions through technology-enabled self-testing and self-monitoring.
Interface 3: Primary care and secondary care
Patients are often required to recall aspects of their medical treatment or history for multiple people working in different parts of the system because information is not shared between them. It often falls to the GP to follow up on progress of a patient through the system. Lack of consistent information sharing between primary and secondary care is a major challenge, increasing bureaucracy and costs while undermining quality of care.[footnote 56]
Access to adequate and appropriate diagnostics capacity in different settings built into validated clinical pathways (supported by digital infrastructure) will be crucial in underpinning effective management of the referral. Online interactions and sharing patient data through interconnected platforms could enable more effective linkages between primary and secondary healthcare professionals. Ensuring clinical data and results from different services are available to primary and secondary care teams, could improve communication and clinical care coordination. The primary care team could then use video-conferencing technology to rapidly consult a specialist remotely.
As more care for long-term or complex conditions can be delivered remotely, multi-disciplinary care teams[footnote 57] could be brought together more easily, with one healthcare professional (such as the patient’s GP) coordinating the team and overseeing the care. Through online meetings, the patient, primary care team and hospital-based consultant can come together to plan management of the patient’s condition and, where necessary, admission to hospital and management after discharge. Equal access to medical records and care plans (for patients and all those involved in delivering the care) would provide better oversight and accountability, allowing easier identification of delays or problems in the patient journey.
Interface 4: Remote monitoring and secondary care
Those with complex or multiple long-term conditions are often required to make trips to primary care and hospital for routine tests, monitoring and treatments. The time invested by patients, medical staff and carers (both informal and professional) in these trips is then not available for other, potentially more productive, activities.
Remote sensor and monitoring technologies can record changes in an individual’s condition and supporting data platforms can log and analyse change over time. They can also allow simultaneous access to the information by specialist healthcare professionals to support remote device reprogramming and risk assessments to inform clinical decision-making. This enables a shared approach to care pathways, including the hand-over of care between different services, to improve quality and integration of care and reduce duplication for patients and healthcare professionals.
These technologies could enable the centre of gravity of the healthcare system to shift as more care is delivered in the community, minimising the hospital footprint and speeding up journeys through the system. Healthcare professionals would use their full set of skills and work in multi-disciplinary teams to guide individuals through care pathways with greater capacity to focus on higher risk or more complex cases.[footnote 58]
Interface 5: Health and care system planners’ access to data
Data about individuals can be brought together at a population level to help health and care system leaders understand issues, anticipate need for care and plan services or target interventions, either at a neighbourhood, place or system level, or specific groups in the population.
Experience from the pandemic illustrates how important timely access to quality data is to inform public health approaches. Data pertaining to individual citizens and their daily activities needs to be anonymized, aggregated and statistically calibrated to provide meaningful metrics for robust decision making while managing concerns about individual privacy or business value.[footnote 59]
Insights do not just come from patient health records. New approaches to monitoring service capacity can help predict bottlenecks and inform planning to better serve the needs of the local population. Longitudinal studies of population health can be interrogated for insights about which groups in the population are at high risk, to understand what drives these risks and inform interventions.[footnote 60]
The pervasive use of digital technologies across all aspects of our life is creating opportunities for insights on drivers of health, such as understanding behaviours that affect health.
The challenge is to successfully identify, access and combine data sets to generate insights for health system planning.
Annex C – Principles for the development of a Demonstrator
Principle 1: Establish a regulated, unified data strategy that delivers for individuals, the Health Service and innovation
A key barrier to harnessing the benefits of technologies is the coordinated flow of data and information between the system interfaces that will enable technologies to be adopted and used to best effect. In addition, processes for capturing information electronically in the healthcare system are not straightforward and often do not utilise technology effectively (or in some cases, at all) with healthcare professionals often relying on handwritten notes to record information.
- We welcome the plans for a Data Strategy for Health and Social Care and highlight the following areas to address to enable digital technologies and data to support innovation in the health system:
- a) interoperability, to connect the myriad of different systems currently used across different NHS services and by patients themselves
- b) reliability and integrity, to ensure data is fit to serve the intended use
- c) accessibility for patients and healthcare professionals across the whole care pathway and in all settings, from clinic, to home, to roadside emergency
- d) security, with protection from unauthorised access or access denial, and of patient privacy
- e) building public and patient trust
- f) sustainability, with clear principles on ownership and storage
- g) support for the provision of user-consumable and relevant summaries
- h) future proofing to support data mining using tools that are yet to be invented, to answer questions that have not yet been posed
In building such an ecosystem, it is important to acknowledge that there are conflicting demands and therefore trade-offs will need to be made.[footnote 61] As the landscape changes, trade-offs will need to be reviewed and amended regularly, by a team and structure that draws relevant knowledge from varied groups (patient representatives, clinicians, data experts) to a) define these trade-offs and b) monitor it over time.
- Establishing a robust and coherent data strategy is essential for Demonstrators to be a success. Measures could include:
- a) empowering people to take control of their own care and data
- i) free data usage for access to digital health services, coupled with local technology hubs providing access to devices through which to engage with services
- ii) or, more broadly, designating broadband as an essential utility to facilitate systems improvements (this links to CST advice on education and levelling up)
- b) giving healthcare professionals what they need to give the best possible care
- c) supporting local and national decision makers with data
- d) giving researchers access to what they need to develop new treatments and insights
- e) helping developers and innovators to improve healthcare
- f) defining and implementing information systems that support proactive identification and management of population needs as well as the 8 requirements (a to h) above
- i) building on the summary care record to drive implementation of a complete Electronic Health Record (EHR) accessible across primary, secondary and tertiary care
- ii) determining common, government-approved standards for information exchange in line with internationally agreed methodology
- g) introducing an economic model for assigning value to data and governing its use by internal and external groups. This will cover both the regulatory framework required to ensure common standards are upheld and that appropriate value is extracted when data is used by others (for example for research or commercial innovation), building on the work of Health Data Research UK[footnote 62] and the Centre of Improving Data Collaboration in this area. Regulation is required to protect individuals and their data, and a stable framework will attract innovators and allow the health service to derive consistent and continuous value from the data it collects
- a) empowering people to take control of their own care and data
Principle 2: Invest in skills, opportunities and networks to support healthcare professionals to lead technology integration for service improvement
Another key barrier to widespread adoption and uptake of technologies is a lack of staff time to develop skills and invest in transformational change, and a lack of support for future clinical and healthcare leaders to develop expertise to manage this change. A healthcare system for the 21st century may also include new types of skills or roles within the health and care professions, but key to success will be allowing different members of the workforce to communicate effectively and avoid working in silos.
- To address this, measures for health professionals should include:
- a) establishing, strengthening and training a new cohort of public health professionals in the context of ongoing public health, NHS and social care reform. They should be enabled to engage with the ICS in population-based planning and delivery of health improvement, protection and care services, directed at improving population health and reducing health inequalities through interventions within and outside the health system
- b) incorporating training in the use of digital technologies (everything from data dashboards from personal devices to data driven diagnostic support systems or robotic assistive technologies) in medical and nursing curricula as well as across the wider healthcare profession
- c) providing upskilling in digital technologies through evidence-based continued professional development (CPD) programmes for existing staff working in the health service
- d) innovative training programmes to create novel healthcare practitioners should be designed and piloted in selected exemplar health economies; these might include digitally trained community nurses and care pathway navigators
- e) putting training in place to develop a cohort of design or engineers with expertise in adopting a system approach to care pathway redesign. These individuals are the future leaders who can pass on best practice to others when successful initiatives are scaled up
Time for training and CPD is an investment. The government will need to give serious consideration to how to ensure individuals are able to take this time, in the context of the continuing staff shortfalls.
Many of the ideas above are embodied in the recommendations of the Topol Review (2019).[footnote 63] We recommend that the government strengthens its efforts to implement the measures outlined in this review to fully embed this principle into a redesigned system and expand training to include all professionals working within healthcare.
Principle 3: Ensure robust evaluation of technology occurs alongside implementation and support knowledge translation to underpin adoption and spread. This will require strengthening research systems to establish the efficacy of new technology-enabled approaches for prevention and care.
The evidence base that a particular digital tool will lead to better health outcomes is often weak.
Technology-enabled approaches must be well-evidenced before they are rolled out and robust initial evaluation should support implementation. Research is essential to understand the safety and effectiveness of use of devices in different settings (including virtual clinics and home use) to understand the clinical support needed to optimise service models and referral pathways and ensure technologies benefit the patient and can be successfully adopted into the system.
This could be embedded into current infrastructures such as the NHS Accelerated Access Collaborative, NIHR Applied Research Collaboratives, or the Academic Health Science Networks. The Medicines and Medical Devices Act 2021, which recently received Royal Assent is also key to this and aims to ensure the UK leads the way in developing pioneering health technology.
With crucial input from MHRA and NICE, common standards around what evidence is needed before the rollout of a technology into the health system should be developed to ensure the right tools are implemented, expanding upon the ‘Digital Technology Assessment Criteria for Health and Social Care (DTAC)’, developed by NHSX alongside NICE. This would have the added benefit of making the UK an attractive place for small-to-medium enterprises (SMEs) to implement their products, as well as large corporates.
A mechanism to allow ‘pre-approval testing’ (equivalent to Beta testing) should be established in the healthcare system Demonstrators. This may be attractive to manufacturers before they go through the time and expense of full regulatory approval and would enable the Demonstrators access to technologies ‘ahead of the curve’ of the rest of the NHS.
There is also a need to ensure that the innovation pipeline is fully understood through horizon scanning and that innovation is stimulated in areas of unmet need. From home monitoring devices that give false reassurance on brown or black skin[footnote 64] to gender bias in medical implant design,[footnote 65] the government needs to challenge the industry to design innovative technologies that benefit the whole population. While existing initiatives such as the NIHR and NHS Accelerated Access Collaborative help signal demand to innovators, more work is needed to enable communities to say what they need and to develop solutions in partnership with innovators. Related to this, it will be important to ensure that horizon scanning and regulatory processes are aligned, to allow for preparation of new regulatory pathways in a timely manner.
Principle 4: Leadership
The Demonstrator regions will require single-point, accountable, empowered leadership. This leader should be responsible for progress, with the authority to take appropriate risks and invest despite this risk.
Principle 5: Sustainability
Our final principle is to ensure financial sustainability of Demonstrators over the duration of their operation. It is generally accepted that successful businesses tend to have a higher intensity of investment in innovation and robust innovation management processes. This is not just R&D, it includes investment in machinery, equipment, software and skills needed to understand, design and develop tailored solutions to what their customers or users need. The Demonstrators will need a predictable, ring-fenced budget over several years to be able to make the strategic investments in system wide innovation. Assuming the Demonstrator is closely aligned to the local ICS, cost savings generated by the Demonstrators should be reinvested by the local ICS in a Local Health Innovation Fund to support continued innovation in subsequent years. This would be in line with the White Paper’s proposals to devolve more power to local ICS leaders and give a strong incentive to enable workforce innovation activity across the system and achieve improved health outcomes.
References
-
Two-thirds of adults over 65 are forecast to be living with multiple long-term conditions by 2035. NIHR, 2018, ‘Multi-morbidity predicted to increase in the UK over the next 20 years’ ↩
-
Projections of multi-morbidity in the older population in England to 2035: estimates from the Population Ageing and Care Simulation (PACSim) model, Age and Ageing, Volume 47, Issue 3, May 2018, Pages 374–380 ↩
-
These barriers are well known and outlined in: AAR, 2016, Accelerated Access Review: final report ↩
-
In 2019, the NHS had a workforce shortage of more than 100,000 staff with a shortfall in training of nurses and GPs and an increasing reliance on international recruitment. Buchan J, Gershlick B, Charlesworth A, Seccombe I, Falling short: the NHS workforce challenge. Health Foundation; 2019 ↩
-
DHSC, 2021, Working together to improve health and social care for all ↩
-
Summary of technologies highlighted in members discussions with fellows of the Royal Academy of Engineering (RAEng) and Academy of Medical Sciences (AMS) including the AMS 2020 annual forum and the 2019 Topol review ‘Preparing the healthcare workforce to deliver the digital future’ ↩
-
Technology Integrated Health Management (TIHM) for dementia is a pioneering Internet of Things study – devices in the home that can connect to the internet and each other, which enable clinicians to remotely monitor the health of people with dementia living at home: Technology helps clinicians monitor the health of dementia patients in their homes ↩
-
This has been supported by £100 million from the UK government. HDR UK, 2018, New centres of excellence in medical imaging and digital pathology ↩
-
For example, the Model Health System currently being developed uses data to support NHS improvements. ↩
-
For example, the UK already has strengths in genetic testing for health care and genome sequencing for research. Last year, the government published ‘Genome UK: the future of healthcare’ setting out the vision to extend the UK’s leadership in genomic healthcare and research. ↩
-
The UK now home to 12% of total global cell and gene therapy trials. Cell and Gene Therapy Catapult, 2020, UK accounts for over 12% of global cell and gene therapy clinical trials ↩
-
NICE, Research to access pathway for investigational drugs for COVID-19 (RAPID C-19) ↩
-
NHS, 2021, Accelerated Access Collaborative: Our year in focus 2019/20 ↩
-
Deloitte Centre for Health Solutions, 2019, Closing the digital gap: Shaping the future of UK healthcare ↩
-
DCMS, 2020, UK National Data Strategy ↩
-
DHSC, 2021, New review into use of health data for research and analysis ↩
-
Significant work has been done to identify the beneficial changes brought about by COVID and opportunities to embed these into business as usual, including through the AAC and NHSE beneficial changes network: Frontier Economics, Health and social care innovation, research and collaboration in response to Covid-19 ↩
-
NICE, 2020, Behaviour change: digital and mobile health interventions ↩
-
Heleen M.E. van Agt, Ida J. Korfage, Marie-Louise Essink-Bot, Interventions to enhance informed choices among invitees of screening programmes—a systematic review, European Journal of Public Health, Volume 24, Issue 5, October 2014, Pages 789–801 ↩
-
Health literacy is ‘the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions. Health literate individuals can access, read, understand written resources, and to use these resources effectively. ↩
-
Spring H., 2020, Health literacy and COVID-19 ↩
-
These may include, but are not limited to, minority ethnic groups, people with disabilities, those experiencing homelessness, looked-after children, people with English as an additional language, and traveller and Gypsy populations. ↩
-
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)32993-3/fulltext ↩
-
For example, individuals with certain mental health conditions or physical disabilities may not be able to engage with some technologies. ↩
-
https://www.england.nhs.uk/2020/10/nhs-to-introduce-one-stop-shops-in-the-community-for-life-saving-checks/ ↩
-
https://www.england.nhs.uk/publication/terms-of-reference-review-national-cancer-screening-programmes-england/ ↩
-
Freestyle Libre for type 1 diabetes is a good example: https://www.nhs.uk/conditions/type-1-diabetes/flash-monitoring-freestyle-libre/ ↩
-
https://www.longtermplan.nhs.uk/online-version/chapter-3-further-progress-on-care-quality-and-outcomes/better-care-for-major-health-conditions/research-and-innovation-to-drive-future-outcomes-improvement/ ↩
-
https://www.kcl.ac.uk/news/daily-data-covid-app-predicts-local-incidence-prevalence-virus ZOE COVID Symptom Study is an app with over 4 million users globally (2.8 million in England) which has been found by researchers at Kings College London to provide accurate estimates of COVID-19 prevalence and incidence, based on daily assessments logged by users. ↩
-
https://www.gov.uk/government/publications/uk-national-data-strategy/national-data-strategy ↩
-
The digital stream of the NHS Diabetes Prevention Programme goes some way towards this: https://www.england.nhs.uk/diabetes/digital-innovations-to-support-diabetes-outcomes/nhs-diabetes-prevention-programme-digital-stream/ ↩ ↩2
-
A digital twin is a digital representation of a system which updates with real-time data and uses tools (such as simulation or machine learning) to aid decision-making. For example, a ward could have a ‘digital twin’ which uses live data on occupancy and current on-duty staff to make decisions about staffing needs. ↩
-
https://www.nhsx.nhs.uk/ai-lab/ai-lab-programmes/regulating-the-ai-ecosystem/ ↩
-
The Topol Review: Preparing the healthcare workforce to deliver the digital future (2019) ↩
-
We envisage this would build on existing communities of practice such as the NICE tools and resources for sustainability and transformation ↩
-
AMS Report: ‘Transforming health through innovation: Integrating the NHS and academia’, (January 2020) ↩
-
Time for research - Delivering innovative patient care in Wales Royal College of Physicians (July 2019) ↩
-
‘Quality improvement in general practice: what do GPs and practice managers think?’ Health Foundation (December 2019) ↩
-
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0101312 ↩
-
For example, through implementation of adoption of NHSX’s Digital Technology Assessment Criteria: https://www.nhsx.nhs.uk/key-tools-and-info/digital-technology-assessment-criteria-dtac/ ↩
-
https://www.nhsx.nhs.uk/key-tools-and-info/digital-technology-assessment-criteria-dtac/ ↩
-
https://link.springer.com/article/10.1007/s11883-020-00889-x ↩
-
This would be consistent with the rights laid out in General Data Protection Regulation, including those of portability (giving individuals the ability to move, copy or transfer personal data easily) and access (giving individuals the ability to access and receive a copy of the personal data an organisation has stored on them). ↩
-
One individual, for example, may wish to grant permission for their data to be used by any research studies being carried out for their conditions. Another may want to give blanket permission for developers to be able to analyse their use of a technology to support improvements. Another may wish to give approval for all beneficial uses of their data. ↩
-
https://www.bma.org.uk/media/3334/bma-supporting-effective-collaboration-between-primary-secondary-care-covid-19-oct-2020.pdf ↩
-
For example, comprising nurse practitioners, pharmacists, a range of professionals allied to medicine including occupational therapists, psychological therapists, social care practitioners and social prescribers and physiotherapists. ↩
-
We recognise that there are situations where a wholly digital pathway may not be suitable (such as for individuals with serious mental illness; individuals who cannot access online services). System redesign around the interfaces we have highlighted would also support these patients in enabling the health service to release resources. ↩
-
The DELVE Initiative (2020), Data Readiness: Lessons from an Emergency. DELVE Report No. 7. Published 24 November 2020. Available from https://rs-delve.github.io/reports/2020/11/24/data-readiness-lessons-from-an-emergency.html ↩
-
https://www.hdruk.ac.uk/news/data-through-our-lifetimes-harnessing-the-power-of-longitudinal-studies-for-health/ ↩
-
The Royal Academy of Engineering has produced a ‘Data Sharing Checklist’ that may be a useful tool when considering trade-offs: http://reports.raeng.org.uk/datasharing/data-sharing-checklist/ ↩
-
‘HDR UK seeks views from health data users on data standards’ (January 2021) ↩
-
The Topol Review: Preparing the healthcare workforce to deliver the digital future (2019) ↩
-
https://www.pslhub.org/learn/patient-safety-in-health-and-care/womens-health/dangerous-exclusions-the-risk-to-patient-safety-of-sex-and-gender-bias-patient-safety-learning-march-2021-r4154/ ↩